RESUMO
Morfometria baseada em voxel (MBV) é uma abordagem útil para investigar mudanças neuroestruturais no cérebro em demência. Revisamos sistematicamente estudos de MBV de doença de Alzheimer (DA) e comprometimento cognitivo leve (CCL), focando especificamente na atrofia de matéria cinzenta (MC) no lobo frontal.
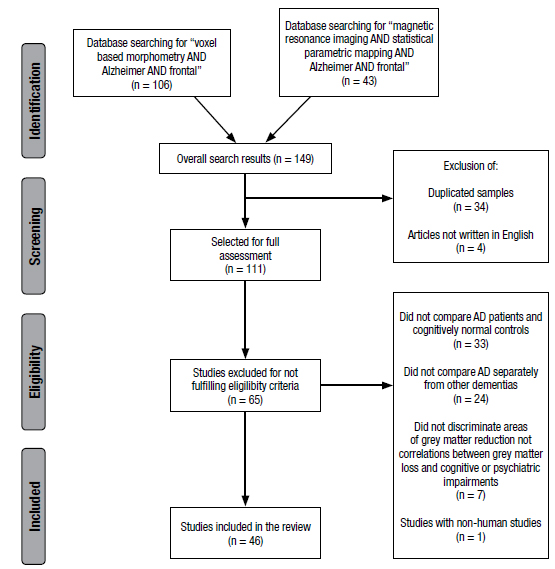
Métodos: Duas pesquisas foram realizadas na base de dados do Pubmed. Critérios de exclusão foram utilizados para assegurar a seleção somente de estudos de MBV que investigassem diretamente anormalidades de volume de MC em pacientes com DA e/ou CCL comparados com controles de cognição normal.
Resultados: De um total de 46 artigos selecionados, 35 estudos de MBV reportaram reduções de volume de MC no lobo frontal. As sub-regiões frontais em que a maioria das reduções de volume foram encontradas incluem os giros frontais inferior, superior e médio, bem como o giro do cíngulo anterior. Também acharam-se perdas de MC em pacientes com CCL que desenvolveram DA. Uma menor parte dos estudos investigou correlações entre volumes de MC frontal e mudanças comportamentais ou déficits cognitivos em DA, com achados variáveis.
Conclusão: Os resultados de estudos de MBV indicam que o lobo frontal deve ser visto como uma importante área cerebral quando da investigação de déficits de volume de MC em associação com DA. Perda de MC frontal pode não ser uma característica apenas de DA tardia. Estudos de MBV futuros com grandes amostras de pacientes com DA são necessários para investigar mais a fundo a relação entre déficits de volume frontal e sintomas de comprometimento cognitivo e neuropsiquiátricos.
Palavras-chave:
doença de Alzheimer; comprometimento cognitivo leve; morfometria baseada em voxel; lobo frontal