Abstracts
Salivary gland carcinosarcoma is a rare neoplasm in which both stromal and epithelial components meet the microscopic criteria for malignancy. Seventy-four cases have been reported in English-language literature to date. In this study, we describe the case of an 81-year-old male patient with parotid gland carcinosarcoma featuring foci of undifferentiated carcinoma and sarcomatous components such as chondrosarcoma, high-grade undifferentiated sarcoma, and malignant giant cell tumor. We reviewed and discussed this rare occurrence of salivary gland carcinosarcoma with areas of malignant giant cell tumor, which had been reported only twice previously.
Parotid gland; Parotid neoplasms; Carcinosarcoma; Glândula parótida; Tumores da parótida; Carcinossarcoma
O carcinossarcoma de glândulas salivares é uma neoplasia rara na qual os componentes epitelial e estromal apresentam critérios microscópicos de malignidade. Setenta e quatro casos já foram relatados até o momento. Neste relato, descrevemos o caso de um paciente do sexo masculino, 81 anos, com carcinossarcoma da parótida, exibindo áreas de carcinoma indiferenciado e componente sarcomatoso constituído por condrossarcoma, sarcoma de alto grau e tumor de células gigantes. Revisamos e discutimos essa rara observação de carcinossarcoma de glândula salivar exibindo focos de tumor de células gigantes, descrito apenas em dois casos prévios.
CASE REPORT RELATO DE CASO
Carcinosarcoma of the parotid gland featuring foci of malignant giant cell tumor
Carcinossarcoma da glândula parótida com áreas de tumor de células gigantes
José Castro Geraldes FilhoI; Larissa G. M. CarvalhoII; Nathanael F. Pinheiro JuniorIII; Luiz Antonio R. de FreitasIV; Paulo Roberto Fontes AthanazioV; Daniel Abensur AthanazioVI
ICirurgião de Cabeça e Pescoço do Hospital Espanhol, Salvador-BA
IIGraduanda em Medicina pela Universidade Federal da Bahia (UFBA)
IIIMestre em Patologia; patologista do Laboratório de Anatomia Patológica Imagepat, Salvador-BA
IVPhD em Patologia; pesquisador da Fundação Oswaldo Cruz e da UFBA
VMestre em Patolgia; patologista do Laboratório de Anatomia Patológica Imagepat no Hospital Espanhol, Salvador-BA
VIPhD em Patologia; professor da UFBA
Mailing address Mailing address Daniel Abensur Athanazio Universidade Federal da Bahia Instituto de Ciências da Saúde Av. Reitor Miguel Calmon s/n Vale do Canela CEP: 40110-100 Salvador-BA Tel.: (71) 3283-8885 ramal 41 Fax: (71) 3240-4194 e-mail: daa@ufba.br
ABSTRACT
Salivary gland carcinosarcoma is a rare neoplasm in which both stromal and epithelial components meet the microscopic criteria for malignancy. Seventy-four cases have been reported in English-language literature to date. In this study, we describe the case of an 81-year-old male patient with parotid gland carcinosarcoma featuring foci of undifferentiated carcinoma and sarcomatous components such as chondrosarcoma, high-grade undifferentiated sarcoma, and malignant giant cell tumor. We reviewed and discussed this rare occurrence of salivary gland carcinosarcoma with areas of malignant giant cell tumor, which had been reported only twice previously.
Key words: Parotid gland, Parotid neoplasms, Carcinosarcoma
RESUMO
O carcinossarcoma de glândulas salivares é uma neoplasia rara na qual os componentes epitelial e estromal apresentam critérios microscópicos de malignidade. Setenta e quatro casos já foram relatados até o momento. Neste relato, descrevemos o caso de um paciente do sexo masculino, 81 anos, com carcinossarcoma da parótida, exibindo áreas de carcinoma indiferenciado e componente sarcomatoso constituído por condrossarcoma, sarcoma de alto grau e tumor de células gigantes. Revisamos e discutimos essa rara observação de carcinossarcoma de glândula salivar exibindo focos de tumor de células gigantes, descrito apenas em dois casos prévios.
Unitermos: Glândula parótida, Tumores da parótida, Carcinossarcoma
Introduction
Malignant mixed tumor represents less than 2% of all mixed tumors of the salivary glands. They have been classified into three different morphological types: carcinoma ex pleomorphic adenoma (99% of all cases), metastasizing pleomorphic adenoma and carcinosarcoma. Carcinosarcoma is a rare neoplasm in which both the stromal and epithelial components meet the microscopic criteria for malignancy, accounting for less than 0.2% of all salivary gland tumors(13).
In an extensive English-language literature review, 71 cases of carcinosarcoma of the salivary glands were reported prior to 2007(13) and three additional cases were found thereafter(6, 11, 14). Data were available for 59 of those cases, of which 30 (51%) exhibited preexistence or coexistence of pleomorphic adenoma. In four of those cases, carcinosarcoma occurred after the irradiation of a pleomorphic adenoma. The interval between irradiation and the subsequent development of carcinosarcoma ranged from one to 36 years(13). Two-thirds of all salivary gland carcinosarcomas occurs in the parotid gland, 19% of cases occur in the submandibular glands, and 14% occur in the minor salivary glands of the palate(2).
This case report discusses the rare observation of a parotid gland carcinosarcoma featuring foci resembling malignant giant cell tumors of bone and soft tissue.
Case report
An 81-year-old male patient sought medical assistance due to a painless mass in his left parotid region that was present for two months. A needle-aspiration biopsy was performed, leading to the diagnosis of pleomorphic adenoma. Four months later, the patient developed localized pain, ipsilateral facial paralysis and painful swallowing. Computerized tomography revealed a heterogeneous mass in the parotid region (Figure 1). An incisional biopsy was performed. After the diagnosis of carcinosarcoma, the patient underwent left radical parotidectomy and cervical lymph node dissection. During surgery, the tumor was noted to involve the superficial and deep lobes of the parotid gland, and was also attached to the masseter muscle and the coronoid process of the mandible. The tumor was excised en bloc.
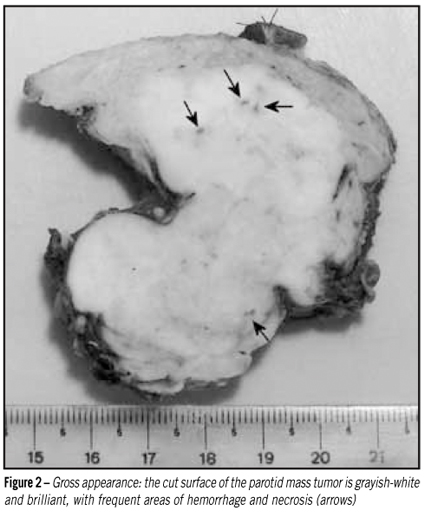
Gross examination of the surgical specimen revealed a tumor weighing 116 g and measuring 7 × 6 × 5.5 cm, infiltrating the overlying skin and adjacent salivary gland tissue. The cut surface of the tumor was grayish-white and glistening, with areas of hemorrhage and necrosis (Figure 2). Microscopy exhibited well-defined tumor margins (Figure 3), with infiltration of the dermis and adjacent salivary gland tissue in some areas.
The tumor featured a biphasic pattern with small and sparse foci of undifferentiated carcinoma, in addition to largely predominant sarcomatous areas (Figure 4A). Most of the sarcomatous component exhibited chondroid (Figure 4B) and chondromyxoid differentiation (60% of the total tumoral area), with areas of high-grade undifferentiated sarcoma (30%) and small foci of malignant giant cell tumor. These findings resembled their bone and soft tissue counterparts. These foci were composed of numerous multinucleated giant cells in a background of sheets of mononuclear cells. These cells had round or ovoid shapes, large nuclei and indistinct nucleoli, characteristics similar to the nuclei of scattered giant cells (Figure 4C). In areas with chondroid features, dimorphic histological patterns of low-grade chondrosarcoma and hypercellular areas with small, uniform and undifferentiated cells were observed, resembling mesenchymal chondrosarcoma. Areas of osteoid formation with atypical stromal cells (osteosarcoma-like) were also seen. Extensive sampling did not show any signs of preexisting pleomorphic adenoma.

Immunohistochemical analysis was performed to confirm the epithelial nature of the small areas thought to be undifferentiated carcinoma. Those areas stained focally positive for cytokeratin (AE1/AE3, DAKO, M3515) (Figure 5A), while preexisting ducts within the tumor were strongly positive (Figure 5B). Carcinoembryonic antigen (CEA) (polyclonal, DAKO, A0115) and epithelial membrane antigen (EMA) (E29, DAKO, M0613) (Figure 5C) were also expressed in areas of undifferentiated carcinoma. Stromal areas of the tumor expressed vimentin and smooth muscle actin (SMA) (1A4, DAKO, M0851). Positive staining for the S-100 protein (polyclonal, ZYMED, 18-0046) was noted in areas of chondroid differentiation. Giant cells from areas identified as malignant giant cell tumor were positive for CD68 (KP1, DAKO, M0814) (Figure 5D), in contrast to the bizarre/atypical giant cells of the high-grade sarcomatous component, which were CD68-negative. The tyrosine kinase receptor KIT (CD117; polyclonal, DAKO, A4502) was not expressed within the tumor, with the exception of scattered giant cells within the malignant giant cell tumor component. Tumor cells did not express desmin (D33, DAKO, M0760) or CD34 (QBEnd10, DAKO, M7165).

The specimen also included the product of the left cervical dissection, in which 16 lymph nodes found to be were free of tumor. The left submandibular gland, the coronoid process of the mandible and the margins were also uninvolved. The patient developed a local recurrence (measuring 3.5 cm) two months after surgery. Over the following two months, the localized pain worsened, accompanied by extreme dysphagia that led to severe malnutrition and dehydration. During hospitalization, the neck mass rapidly increased in size with ulceration and severe bleeding. The patient evolved with anemia, hypoalbuminemia and renal failure, and eventually died four months after surgery.
Discussion
The characteristic feature of carcinosarcoma is the presence of malignant epithelial and stromal components. Detailed descriptions of microscopic features are available for 29 salivary gland carcinosarcomas arising de novo (with no remnant area of pleomorphic adenoma)(13). In most cases, the carcinomatous element is a high-grade adenocarcinoma not otherwise specified (NOS) (13 cases). However, other types of carcinoma have been noted (three cases of undifferentiated carcinoma, three cases of squamous-cell carcinoma, two cases of adenoid-cystic carcinoma, two cases of salivary-duct carcinoma, one case of basaloid carcinoma and one case of large-cell neuroendocrine carcinoma). Chondrosarcoma is the most common sarcomatous component, present in 11 cases, followed by osteosarcoma (eight cases). Other malignant mesenchymal components that have been reported are fibrosarcoma (five cases), myxoid sarcoma (two cases), malignant spindle-cell sarcoma (two cases), undifferentiated sarcoma (one case), rhabdomyosarcoma (one case) and follicular dendritic cell sarcoma (one case)(13).
The literature describes 60 cases of true malignant mixed tumors of the salivary gland (de novo or ex-pleomorphic adenoma), with the most common carcinoma being squamous-cell carcinoma or adenocarcinoma, whereas the most common sarcoma was chondrosarcoma. Other sarcomas that have been reported include fibrosarcoma, leiomyosarcoma, osteosarcoma and, in rare cases, liposarcoma or any combination of these sarcomas(7).
To the best of our knowledge, only two cases of carcinosarcoma of the parotid gland featuring areas of malignant giant cell tumor resembling their counterparts in the bone and soft tissue have been reported(5, 8). The first case was a 66-year-old female patient with a 5 cm parotid mass, in which 80% of the tumor was c omprised of malignant giant cell tumor, while a minor portion consisted of salivary duct carcinoma with foci of osteosarcoma(5). In the second report, a 60-year-old female patient presented a 5 cm parotid mass with four microscopic patterns: undifferentiated carcinoma, undifferentiated sarcoma, osteosarcoma and malignant giant cell tumor(8).
Another rare finding in the pathology of the parotid gland is the osteoclast-like giant cell tumor. Only 16 cases have been reported in the English-language literature, and nine of those cases were reported to coexist with a carcinomatous component(3). These tumors were not classified as carcinosarcoma, and it is questionable whether extensive sampling would allow for the identification of carcinomatous foci in these cases of parotid gland osteoclast-like giant cell tumor. It is not clear to what extent carcinosarcoma and osteoclast-like giant cell tumor of the parotid (with or without coexistent carcinoma) are related. To date, osteoclast-like giant cell tumors are not listed as a distinct salivary gland tumor in the World Health Organization's classification(2). In contrast to the giant cell tumor of the bone, which is believed to be of histiocytic origin, the mononuclear cells of salivary gland osteoclast-like giant cell tumors exhibit an epithelial immunophenotype(3). In at least one case of coexistent malignant giant cell tumor and carcinosarcoma, the tumor cells (either giant cells or mononuclear cells) did not express cytokeratin(5). This result is in accordance with our observations, which indicated that CD68-positive giant cells were negative for cytokeratin. These findings suggest that giant cells from these two entities (salivary gland osteoclast-like giant cell tumor and carcinosarcoma) have different immunophenotypes, and are therefore unrelated. Further studies with a larger series of cases should be carried out to test this hypothesis.
KIT expression is well-documented in uterine carcinosarcoma(10, 12), and has been reported to occur in one salivary gland carcinosarcoma(1). In our case, only scattered multinucleated giant cells were KIT-positive.
Pleomorphic adenoma, and presumably its malignant counterpart, is classified as mixed tumor assuming their epithelial nature with metaplastic features and/or a broad range of morphological appearance in the spectrum of myoepithelial differentiation. In this context, immunohistochemistry (IHQ) will be of limited value and usually are not required for the diagnosis which relies on recognition of epithelial and mesenchymal differentiation(4, 9, 13). Distinction from pleomorfic adenoma and carcinosarcoma depends on architectural and cytologic criteria of malignancy. In the present case, however, the use of anti-cytokeratin antibodies was useful to identify areas of undifferentiated carcinoma, the only epithelial component of the tumor. Without detection of carcinomatous areas (Figure 5) a differential diagnosis with primary or metastatic sarcoma would be imperative. Both the use of IHQ and extensively sampling were important to correctly identify carcinosarcoma in the present case.
The recommended treatment of parotid carcinosarcoma is wide surgical excision combined with radiotherapy. Almost 60% of patients die of local recurrence and/or metastatic disease (in the lungs, bones and central nervous system), usually within a 30-month period(2). In the present case, the disease progressed rapidly after surgery, with local recurrence leading to severe complications, including painful swallowing, ulceration and bleeding of the parotid mass and eventually malnutrition, dehydration, anemia, hypoalbuminemia, renal failure and death.
Carcinosarcoma is a rare salivary gland neoplasm that may exhibit a broad range of morphological presentations that pose difficulties for the surgical pathologist, especially when dealing with small biopsies or smears from fine-needle aspiration. This case highlights the occurrence of a giant cell tumor component, which may be indistinguishable from its counterparts in the bone and soft tissues and may lead to the diagnosis of salivary gland osteoclast-like giant cell tumor. Extensive sampling may be crucial to correctly identify carcinosarcoma in such cases.
Primeira submissão em 12/07/11
Última submissão em 19/11/11
Aceito para publicação em 29/12/11
Publicado em 20/04/12
- 1. ANDREADIS, D. et al. Detection of C-KIT (CD117) molecule in benign and malignant salivary gland tumours. Oral Oncol, v. 42, n. 1, p. 57-65, 2006.
- 2. EVESON, J. W. et al. Tumours of the salivary glands. In: LEON BARNES, L. et al. (Ed.) Pathology and genetics. Head and neck tumours World Health Organization Classification of Tumours. Lyon: IARCPress, 2008. p. 244.
- 3. FANG, X. et al. Osteoclast-like giant cell tumor of the salivary gland. Ann Diagn Pathol, v. 13, n. 2, p. 114-8, 2009.
- 4. GALLI, J. et al. Carcinosarcoma of the submandibular salivary gland: clinical case and review of the literature. J Otolaryngol, v. 34, n. 1, p. 66-9, 2005.
- 5. GRENKO, R. T.; TYTOR, M.; BOERYD, B. Giant-cell tumour of the salivary gland with associated carcinosarcoma. Histopathology, v. 23, n. 6, p. 594-5, 1993.
- 6. KARAMAN, E. et al. Follicular dendritic cell sarcoma of the parotid gland recurring 6 times within 12 years. J Craniofac Surg, v. 20, n. 6, p. 2171-2, 2009.
- 7. KWON, M. Y.; GU, M. True malignant mixed tumor (carcinosarcoma) of parotid gland with unusual mesenchymal component: a case report and review of the literature. Arch Pathol Lab Med, v. 125, n. 6, p. 812-5, 2001.
- 8. LIESS, B. D. et al. Carcinosarcoma of the parotid gland: report of a case with immunohistochemical findings. Ann Otol Rhinol Laryngol, v. 116, n. 9, p. 702-4, 2007.
- 9. MARDI, K.; SHARMA, J. True malignant mixed tumor (carcinosarcoma) of parotid gland: a case report. Indian J Pathol Microbiol, v. 47, n. 1, p. 64-6, 2004.
- 10. MENCZER, J. et al. Expression of c-kit in uterine carcinosarcoma. Gynecol Oncol, v. 96, n. 1, p. 210-5, 2005.
- 11. QURESHI, A. True malignant mixed tumor of parotid. J Coll Physicians Surg Pak, v. 17, n. 11, p. 697-8, 2007.
- 12. RASPOLLINI, M. R. et al. COX-2, c-KIT and HER-2/neu expression in uterine carcinosarcomas: prognostic factors or potential markers for targeted therapies? Gynecol Oncol, v. 96, n. 1, p. 159-67, 2005.
- 13. STAFFIERI, C. et al. Carcinosarcoma de novo of the parotid gland. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, v. 104, n. 2, p. e35-40, 2007.
- 14. VEKONY, H. et al. Salivary gland carcinosarcoma: oligonucleotide array CGH reveals similar genomic profiles in epithelial and mesenchymal components. Oral Oncol, v. 45, n. 3, p. 259-65, 2009.
Publication Dates
-
Publication in this collection
14 May 2012 -
Date of issue
Apr 2012
History
-
Received
12 July 2011 -
Accepted
29 Dec 2011 -
Reviewed
19 Nov 2011