Abstracts
OBJECTIVE: Eighty-three soccer players aged between 14 and 19 years, in the basic category of a professional soccer club in the city of Belo Horizonte, were followed up during the 2009 season. METHODS: A prospective observational cohort study was conducted, in which these soccer players were divided randomly into two groups. The first consisted of individuals with joint hypermobility syndrome (JHS), totaling 22 players, and the second was a control group with 61 players without this syndrome, determined through a physical examinati. RESULTS: Both groups were studied with regard to incidence of ankle sprains. At the end of this period, the data were compiled and statistical analysis was performed. A total of 43 cases of ankle injury due to sprains were recorded, of which nine episodes were in players with JHS, thus making p = 0.106. The significance level was 5%. CONCLUSION: We were able to conclude that in our study there was insufficient evidence to assert that there is an association with increased incidence of ankle sprains among patients with JHS .
Ankle; Soccer; Joint Instability
OBJETIVO: Foram acompanhados 83 atletas, com idade entre 14 e 19 anos, das categorias de base de um clube de futebol da cidade de Belo Horizonte, durante a temporada de 2009. MÉTODOS: Foi realizado estudo prospectivo observacional tipo coorte, no qual esses atletas foram separados aleatoriamente, em dois grupos, sendo o primeiro composto por portadores de síndrome da hipermobilidade articular (SHA) totalizando 22 jogadores, e o segundo como grupo controle com 61 atletas não portadores, após a realização de exame físico. RESULTADOS: Ambos os grupos foram estudados quanto à incidência de entorses de tornozelo. Ao final desse período, foi feita a compilação dos dados e sua análise estatística. Foi registrado um total de 43 lesões no tornozelo por entorse, sendo nove episódios em portadores da SHA, perfazendo um p = 0,106. O nível de significância utilizado foi de 5%. CONCLUSÃO: Podemos concluir que em nosso estudo não houve evidências suficientes para afirmarmos que exista associação entre o aumento na incidência de entorse em tornozelo em pacientes com a SHA.
Tornozelo; Futebol; Instabilidade Articular
ORIGINAL ARTICLE
IPreceptor of the Medical Residency Service of the Minas Gerais School of Medical Sciences - Hospital Universitário São José - Belo Horizonte, MG, Brazil
IIFormer Resident of the Medical Residency Service of the Minas Gerais School of Medical Sciences - Hospital Universitário São José - Belo Horizonte, MG, Brazil
IIIFormer Student of the Minas Gerais School of Medical Sciences - Hospital Universitário São José - Belo Horizonte, MG, Brazil
IV Master's degree in Orthopedics from USP; Associate Professor of the Orthopedics and Traumatology Clinic of the Minas Gerais School of Medical Sciences - Belo Horizonte, MG, Brazil
Correspondence
ABSTRACT
OBJECTIVE: Eighty-three soccer players aged between 14 and 19 years, in the basic category of a professional soccer club in the city of Belo Horizonte, were followed up during the 2009 season.
METHODS: A prospective observational cohort study was conducted, in which these soccer players were divided randomly into two groups. The first consisted of individuals with joint hypermobility syndrome (JHS), totaling 22 players, and the second was a control group with 61 players without this syndrome, determined through a physical examinati.
RESULTS: Both groups were studied with regard to incidence of ankle sprains. At the end of this period, the data were compiled and statistical analysis was performed. A total of 43 cases of ankle injury due to sprains were recorded, of which nine episodes were in players with JHS, thus making p = 0.106. The significance level was 5%.
CONCLUSION: We were able to conclude that in our study there was insufficient evidence to assert that there is an association with increased incidence of ankle sprains among patients with JHS.
Keywords: Ankle; Soccer; Joint Instability
INTRODUCTION
According to the FIFA Big Count 2006 study, around 265 million people play soccer worldwide, of which 22 million are under 20 years of age(1), making this the most widely played sport in the world. In the USA, between 1990 and 2003, around 1.6 million injuries were registered in soccer players aged under 18 years, mainly affecting the lower limbs, with ankle sprains being the most common type of injury(2).
Joint hypermobility syndrome (JHS) is a pathology caused by variation or mutation of the genes that encode collagen, elastin, fibrin and tenascin, affecting the musculoskeletal system(3-6). This disorder affects 0.6 to 31% of the population, and is five times more prevalent in women(7). The diagnosis of JHS is essentially clinical, since there are no laboratory or radiological parameters available for this purpose. A work originally carried out by Carter and Wilkinson(8), and later modified by Carr et al(9), analyzes criteria of the physical exam that can be used to diagnose people with JHS.
Hall et al(10) report that individuals with JHS display poorer proprioceptive responses, leading to reduced sensory feedback and causing a higher incidence of joint injuries, particularly sprains. Lompa et al(11) confirm, in their work, that JHS predisposes individuals with this disease to musculoskeletal injuries.
The purpose of this study is to evaluate the relationship between soccer players aged under 20 years with joint hypermobility syndrome, and incidence of ankle sprains, compared with players who do not have the disease.
MATERIAL AND METHOD
A transversal, observational, prospective study was carried out. During a routine physical examination in the pre-season period of 2009, 89 male athletes aged between 14 and 19 years were randomly selected from the youth divisions of a soccer club in the Brazilian Championship first division. These players underwent the characteristic clinical exam for joint hypermobility syndrome (JHS), as described by Carter and Wilkinson(8). The players were then divided into two groups: those with JHS, and those without JHS. These athletes were monitored during the 2009 season, which ran from February 2009 to January 2010.
Each time these players entered the medical department of the club for consultation and treatment due to episodes of ankle sprains, a questionnaire was filled out, with the athlete's data, his position in the team, the affected side of the body, and the moment of the trauma (during a game, during training, other)(8-11).
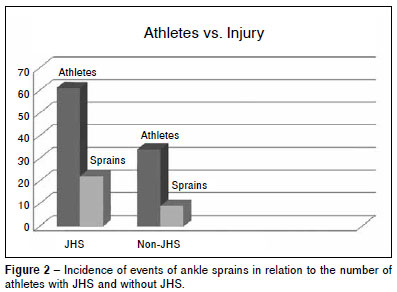
During the season, six athletes were lost due to departure from the club; as a result, the sample of this study included a total of 83 players. Of these, 22 (26.5%) had JHS and 61 (73.5%) did not (Figure 1).
Fisher's test was used to verify the association between the variables. The level of significance adopted was 5%. The software R was used for the calculations. It was not possible to use the chi-square test, as the premises for this were not satisfactory.
RESULT
The total of episodes of ankle sprains during the 2009 season was 43. Of these, 34 (79%) sprains occurred in players without JHS, while nine (21%) occurred in patients with JHS, making a p = 0.1060 (Figure 2).
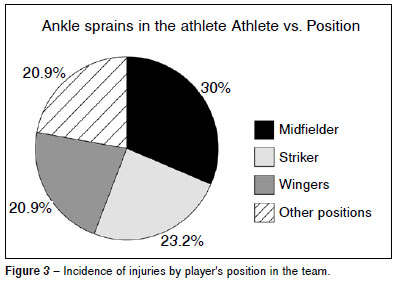
According to the player's position on the team, the most common injuries were among midfielders, with 13 (30%) episodes, followed by strikers, with 10 (23.2%), wingers, with nine (20.9%) and the other positions with nine (20.9%) sprains (Figure 3).
The trauma occurred during training in 29 (67.44%) of the cases, and eight (18.6%) during actual games.
DISCUSSION
Joint hypermobility syndrome (JHS) is a common source of joint or muscle complaints, often giving rise to concern among parents, and in the case of athletes, the medical team. The clinical symptom is ligamentous laxity, which may be associated with pain during the day, waking at night, or discomfort during physical activities. Another characteristic is muscle weakness, accompanied by joint instability, loss of proprioception, and a tendency to incur traumatic injuries(12). Based on this, the hypothesis was proposed that injuries in athletes may be linked to JHS; such a finding would enable athletes with this syndrome to receive training to improve joint stability. According to Everman and Robin(5), and Russek(6), the training methods for this syndrome should be focused on the joint insufficiency and limitation; although they do not decrease the elasticity, strengthening and proprioceptive exercises improve muscle tone and the structures around the joint. Analysis of the prevalence and risk factors of sports-related injuries and the development of preventative programs may be extremely important in reducing the incidence of these injuries.
Sahin et al(3), in a study to evaluate proprioception in knees of individuals with JHS, showed that it is decreased, but that proprioception exercises can lower pain and improve the stability of the knee. Hall and Brody(13) affirm that decreased proprioception results in a greater predisposition to develop osteoarthritis. Diaz et al(14) correlated JHS in soldiers of the same age (17 years) with the incidence of musculoligamentous lesions and compared this with individuals without this characteristic, observing a higher incidence in the first group. Carter and Sweetnam(15) correlated JHS with dislocation of the patella and shoulder. There have been few articles related to the practice of sports. Lichtor(16), for example, suggest carrying out a prior assessment, so that athletes with JHS can be recommended a regimen of physical activity that does not include contact sports. On the other hand, JHS can be an initial advantage in some sports, although in the long term, it can be a disadvantage. This occurs, for example, in ballet students, for whom JHS gives an advantage in the selection test in schools, due to the greater agility; however, with intense activity, they can suffer from a higher incidence of lesions(17).
To characterize the presence of JHS, the scoring system of Carter and Wilkinson(8) was used, with the following criteria:
1. Touching the thumb to the forearm with flexion of the wrist;
2. Index finger and forearm parallel with the wrist extended;
3. Hyperextension of the elbow;
4. Recurvatum of the knee;
5. Hyperextension of the femoral neck.
To be classified as having JHS, the athlete must present three of the five characteristics described above.
Note that in the medical literature, there are also the criteria of Brighton's apud Grahame(18,19) for diagnosing JHS, and that to date, there are no laboratory criteria for diagnosing JHS.
The injuries were defined in the same way as any other injury that occurs during games, club training, or extra-club activities, with reduction or complete withdrawal of the athlete's participation in the sports activities, or requiring special training in order to continue playing. In this work, we found that 18.6% of the injuries occurred during games, while 67.44% occurred during training, contradicting the study by Woods et al(20), who found an incidence of around 66% of lesions occurring during games, and 33% during training. During our study, no player presented severe trauma, such as dislocation or fracture. In previous studies, the prevalence of JHS in the population studied reached levels of between 7.6% and 64.6%(11,21,22), corroborating with the data found in this study, which was 26.5% of the soccer players included in the sample.
Cohen et al(23) investigated orthopedic injuries in soccer, and concluded that joint sprain lesions represent 17 (9%) of injuries, that the majority of injuries occurred in midfielders and strikers, and that non-contact injuries were the most frequent. In our work, the injuries evaluated were only those of the lower limbs, ankle injuries being the most prevalent in the striker and midfielder positions, which corroborates the study in question.
A study by Lompa et al(11) showed a prevalence of 7.62% of athletes with this syndrome, in a sample that included both males and females; in that study, the athletes that were in older age groups had less tissue elasticity, compared with those in younger age groups. The athletes with JHS showed a significantly higher incidence of lesions than those without JHS. Contrary to the researcher's expectations, our study, which included only males, did not show any association between JHS and ankle injuries. Attention should be drawn to some data of the study. The prevalence of JHS in a male population is lower than among females(8-11); as children become adolescents, there is a tendency for the joint mobility to decrease(10).
CONCLUSION
The authors conclude that patients with joint hypermobility syndrome (JHS) had the same incidence of ankle sprain injuries as the population without JHS.
REFERENCES
- 1. FIFA Big Count 2006=270 million people active in football. FIFA Communications Division, Information Services, 31.05.2007.
- 2. Leininger RE, Knox CL, Comstock RD. Epidemiology of 1.6 million pediatric soccer-related injuries presenting to US emergency departments from 1990 to 2003. Am J Sports Med. 2007;35(2):288-93.
- 3. Sahin N,Baskent A, Camak A, Salli A, Ugurlu H, Berker E. Evaluation of knee proprioception and eVects of proprioception exercise in patients with benign joint hypermobility syndrome. Rheumatol Int. 2008;28(10):995-1000.
- 4. Grahame R. Hypermobility--not a circus act.. Int J Clin Pract. 2000;54(5):314-5.
- 5. Everman DB, Robin NH. Hypermobility Syndrome. Pediatr Rev. 1998;19(4):111-7.
- 6. Russek LN. Hypermobility syndrome. Phys Ther. 1999;79(6):591-5.
- 7. Silverman S, Constine L, Harvey W. Survey of joint mobility and in vivo skin elasticity in London schoolchildren. Ann Rheum Dis. 1975;34(2):177-80.
- 8. Carter C, Wilkinson J. Persistent joint laxity and congenital dislocation of the hip. J Bone Joint Surg Br. 1964;46:41-5.
- 9. Carr AJ, Jefferson RJ, Benson MK. Joint laxity and hip rotation in normal children and in those with congenital dislocation of the hip. J Bone Joint Surg Br. 1993;75(1):76-8.
- 10. Hall MG, Ferrell WR, Sturrock RD, Hamblen DL, Baxendale RH. The effect of the hypermobility syndrome on knee joint proprioception. Br J Rheumatol. 1995;34(2):121-5.
- 11. Lompa PA, Schio CL, Müller LM, Mallamann LF. Incidência de lesões esportivas em atletas com e sem síndrome de hipermobilidade articular familiar. Rev Bras Ortop. 1998;33(11/12):933-8.
- 12. Maillard S, Murray KJ. Hypermobility syndrome in children. In: Keer R, Grahame R, editors. Hypermobility syndrome. London: Elsevier; 2003.p. 41-3.
- 13. Hall C, Brody LT. Impairment of muscle performance. In: Hall CM, Brody LT, editors. Therapeutic exercise moving toward function. Philadelphia: Williams and Wilkins; 1999. p. 59-60.
- 14. Acasuso Díaz M, Collantes Estévez E, Sánchez Guijo P. Joint hyperlaxity and musculoligamentous lesions: study of a population of homogenous age, sex and physical exertion. Br J Rheumatol. 1993;32(2):120-2.
- 15. Carter C, Sweetnam R. Recurrent dislocation of the patella and of the shoulder, their association with familial joint laxity. J Bone Joint Surg Am. 1960;42:721-7.
- 16. Lichtor J. The loose-jointed young athlete: recognition and treatment with special emphasis on knee injuries. J Sports Med. 1972;1(1):22-23.
- 17. Grahame R. Joint hypermobility and the performing musician. N Engl J Med. 1993;329(15):1120-1.
- 18. Grahame R. Hypermobility and hypermobility syndrome. In: Keer R, Grahame R, editors. Hypermobility syndrome. London: Elsevier; 2003. p. 1-12.
- 19. Grahame R, Brid H, Child A. The revised (Brighton 1998) criteria for the diagnosis of benign joint hypermobility syndrome. J Rheumatol. 2000;27(7):1777-9.
- 20. Woods C, Hawkins R, Hulse M, Hodson A. The Football Association Medical Research Programme: an audit injuries in professional football: an analysis of ankle sprains. Br J Sports Med. 2003;37(3):233-8.
- 21. Lamari NM, Chueire AG, Cordeiro JA. Analysis of joint mobility patterns among preschool children. Sao Paulo Med J. 2005;123(3):119-23.
- 22. Seckin U, Tur BS, Yilmaz O, Yagci I, Bodur H, Arasil T. The prevalence of joint hypermobility among high school students. Rheumatol Int. 2005;25(4):260-3.
- 23. Cohen M, Abdalla RJ, Ejnisman B, Amaro JT. Lesões ortopédicas no futebol. Rev Bras Ortop. 1997;32(12):940-4.
Iincidence of ankle sprains in soccer players with joint hypermobility syndrome
Publication Dates
-
Publication in this collection
18 Feb 2013 -
Date of issue
2012
History
-
Received
02 June 2011 -
Accepted
03 May 2012