Abstracts
Psoriasis is a cutaneous-articular disease, whose incidence ranges from 1% to 3%. Stress tends to be a triggering or aggravating factor in psoriasis. In addition, the disease itself can generate emotional stress because of its lesions. Several psychological disorders can be associated with psoriasis, and feelings such as rage, depression, shame, and anxiety have been commonly reported, which can culminate in social isolation and sexual dysfunction. Despite being a common complaint among patients with psoriasis, sexual dysfunction has been rarely reported in the literature. This study aimed at performing a systematic review of the prevalence of sexual dysfunction in psoriasis and psoriatic arthritis, assessing the role played by factors such as depression and severity of disease in this relation. This systematic review showed that data on the sexual difficulties of patients with psoriasis are scarce. The hypotheses to explain sexual dysfunction in that group of patients include the severity of skin findings, the psychological effects of the condition on the patient, concerns of the sexual partner, and side effects of the medical treatments for psoriasis. Those data emphasize that this type of symptomatology is frequently neglected in medical practice, and stress the importance of assessing the impact of psoriasis regarding not only cutaneous and joint involvements, but also psychosocial and sexual impairments. Considering the sociocultural diversities of each population, a specific study of the Brazilian population to provide more information about our patients is required.
psoriasis; psoriatic arthritis; gender; sexuality
A psoríase é uma doença cutaneoarticular, cuja incidência varia entre 1%-3%. O estresse tende a ser um fator desencadeante ou de agravamento na psoríase. Além disso, a própria doença pode gerar estresse emocional, pelo constrangimento das lesões. Uma série de alterações psicológicas pode estar associada à psoríase, e são comuns os relatos de sentimentos de raiva, depressão, vergonha e ansiedade, culminando no isolamento social e, possivelmente, na disfunção sexual. Apesar de a disfunção sexual ser uma queixa comum, são poucos os dados encontrados a respeito na literatura. O objetivo deste estudo foi realizar uma revisão sistemática da prevalência da disfunção sexual na psoríase e na artrite psoriásica, avaliando a participação de fatores como depressão e extensão da doença nessa relação. O resultado da revisão sistemática sobre o assunto aponta que os dados a respeito das dificuldades sexuais nos pacientes com psoríase são limitados. As hipóteses aventadas para explicar a ocorrência de disfunção sexual nesse grupo de pacientes incluem a extensão do quadro cutâneo, os efeitos psicológicos da condição no paciente, a preocupação do parceiro e os efeitos colaterais relacionados aos tratamentos médicos para a psoríase. Os dados apresentados enfatizam a negligência frequente dada a este tipo de sintomatologia na prática médica e ressaltam a importância da avaliação do impacto da psoríase não apenas em relação ao acometimento cutâneo e articular, mas também psicossocial e sexual. Face às diversidades socioculturais de cada população, sugere-se a necessidade de um estudo específico na população brasileira a fim de fornecer maiores informações sobre nossos pacientes.
psoríase; artrite psoriásica; gênero; sexualidade
REVIEW ARTICLE
IDermatologist; Student of the Post-Graduation Program on Medical Sciences, Medical School, Universidade de Brasília - FMUnB
IIPhD in Medical Sciences, FMUnB; Advisor in the Post-Graduation Program of Medical Sciences, FMUnB
Correspondence to
ABSTRACT
Psoriasis is a cutaneous-articular disease, whose incidence ranges from 1% to 3%. Stress tends to be a triggering or aggravating factor in psoriasis. In addition, the disease itself can generate emotional stress because of its lesions. Several psychological disorders can be associated with psoriasis, and feelings such as rage, depression, shame, and anxiety have been commonly reported, which can culminate in social isolation and sexual dysfunction. Despite being a common complaint among patients with psoriasis, sexual dysfunction has been rarely reported in the literature. This study aimed at performing a systematic review of the prevalence of sexual dysfunction in psoriasis and psoriatic arthritis, assessing the role played by factors such as depression and severity of disease in this relation. This systematic review showed that data on the sexual difficulties of patients with psoriasis are scarce. The hypotheses to explain sexual dysfunction in that group of patients include the severity of skin findings, the psychological effects of the condition on the patient, concerns of the sexual partner, and side effects of the medical treatments for psoriasis. Those data emphasize that this type of symptomatology is frequently neglected in medical practice, and stress the importance of assessing the impact of psoriasis regarding not only cutaneous and joint involvements, but also psychosocial and sexual impairments. Considering the sociocultural diversities of each population, a specific study of the Brazilian population to provide more information about our patients is required.
Keywords: psoriasis, psoriatic arthritis, gender, sexuality.
INTRODUCTION
Psoriasis is a recurring, cutaneous-articular, chronic inflammatory disease, resulting from immune and proliferative changes that affect the skin and, sometimes, the mucosae. Its world incidence is estimated to be 1%-3%.1-3 In 5%-42% of the patients, the skin findings are associated with inflammatory arthritis, usually negative for rheumatoid factor, a condition denominated psoriatic arthritis.4,5
Stress tends to be a triggering or aggravating factor in psoriasis. In addition, the disease itself can generate emotional stress because of its lesions.6 Several psychological disorders can be associated with psoriasis, and feelings such as rage, depression, shame and anxiety have been commonly reported, which can culminate in social isolation and higher consumption of alcohol and tobacco.7-11
According to the World Health Organization, sexuality is a basic need and an aspect of human beings that cannot be separated from others,12 extremely important in maintaining good mental health. The impact of psoriasis on sexual functioning is significant, because the condition causes intense interpersonal strain, hindering quality of life.
Sexual impotence and erectile dysfunction due to the medicamentous therapy for the disease, such as etretinate and methotrexate, have been reported.13-15 However, few studies have directly related sexual dysfunction to psoriasis.16,17
Systematic reviews of prevalence studies are important because they provide useful information regarding both medical practice and research projects. A deep view of the study's design and methodology applied to data collection is fundamental to planning future studies.
This study aimed at performing a systematic review of the studies on sexual dysfunction of patients with psoriasis and psoriatic arthritis, assessing aspects commonly identified as associated, such as psychological problems and disease severity.
METHODS
FromAugust to October 2011, searches were performed within the following databases in Portuguese, English, French and Spanish: Medline (1966-2011); Cochrane Library; LILACS; PubMed (1991-2011); and Scopus. The following keywords were used: "psoriasis"; "sexual dysfunction"; and "psoriatic arthritis".
Cross-sectional observational studies, prospective cohorts, randomized controlled studies, and case-control studies about the sexual function of patients with psoriasis and/or psoriatic arthritis were included.
The title and abstract of the articles obtained in the initial search were reviewed by two independent observers to identify the relevant articles. The full text of all articles meeting the inclusion criteria was reviewed, and their bibliographic references were assessed in the search for additional sources. The articles upon which the two observers had agreed were considered for the analysis.
From the studies selected, the following data were assessed: type of study; sample size; instruments used; statistical analysis; and results.
RESULTS
Of the articles identified in the databases cited, only 14 related directly to the topic investigated. Of those 14, seven were excluded because they were either case reports or review articles. In addition to the remaining seven articles, one more was identified in the assessment of the bibliographic references, adding up to a total of eight articles selected.
Of the eight articles selected, three were of the case-control type, and five were observational cross-sectional studies. Neither randomized controlled studies, nor prospective cohort studies, were found. Regarding the three case-control studies, two have compared men and women with psoriasis to healthy individuals,18,19 and one has compared men with psoriasis with men with other dermatological diseases.20 All observational studies have included patients of both sexes. Table 1 shows the types of studies and the samples assessed.
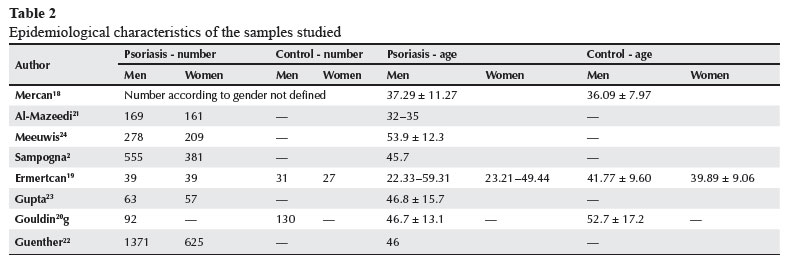
A total of 4,039 patients with psoriasis was assessed, of whom 2,567 were men (63.55%) and 1,472, women (36.45%). Those patients' ages ranged from 23-62 years. Table 2 shows the epidemiological characteristics of the samples of each study.
The severity of psoriasis has been assessed by dermatologists based on the Psoriasis Area and Severity Index (PASI) in three studies19,21,22 and on the Total Body Surface Area (BSA) in one study,23 and by patients by use of the Self-Administered Psoriasis Area and Severity Index (SAPASI) in two studies.2,24 Two studies have not assessed the extent of psoriasis.18,20 The presence of genital lesions2,20,23,24 and the involvement of joints2,22-24 have been reported in four studies.
All studies have assessed the sexual function by means of self-administered questionnaires, and some studies have also assessed psychological aspects and quality of life. The most often used questionnaires to assess sexual function were as follows: the Dermatology Life Quality Index (DLQI), Question #9 (Over the last week, how much has your skin caused any sexual difficulties - not at all, a little, a lot, very much);2,19,22,24 the International Index of Erectile Function (IIEF);19,20,24 and the Female Sexual Function Index (FSFI).19,24 Gupta et al.23 have elaborated and used their own questionnaire, and Ermertcan et al.19 have elaborated a questionnaire based on questions about sexual health extracted from several quality of life questionnaires, such as Skindex-29, DLQI, Psoriasis Disability Index (PDI), and Impact of Psoriasis on Quality of Life (IPSO) questionnaire. Table 3 shows the instruments used by each author.
Quality of life, depression and sexual function
In the study by Mercan et al.,18 sexual dysfunction was more common in the group of patients with psoriasis than in the control group, and statistically significant difference (P < 0.05) was observed between the orgasmic experience total score and subscore of the Arizona Sexual Experience Scale (ASEX). Ten patients of the psoriasis group had BDI score > 17, being considered clinically depressed. After their exclusion, ANOVA and Tuckey test in the two groups showed similar results of ASEX score.
Al-Mazeedi et al.21 have reported a greater prevalence of psychological disorders in the severe psoriasis group. The sexual activity was affected in 31.6% of the patients. Dysfunction was identified in 38.9% of the patients with severe psoriasis, in 29.7% of those with moderate psoriasis, and in 30.8% of those with mild psoriasis. The difference between the groups, however, was not statistically significant.
The study by Meeuwis et al.24 has focused mainly on the presence of genital psoriasis. The mean total score of DLQI was 6.6 ± 5.5. Patients with genital lesions scored worse than those without genital lesions, especially in the question referring to sexual life.
Using the Sexual Quality of Life Questionnaire for Men (SQoL-M), men with psoriasis scored 77.2 ± 24.1 (the index ranges from 0 to 100, and the higher the score, the better the quality of sexual life); when using the IIEF, their score was 55.7 ± 17.2 (the index ranges from 5-75, and the higher the score, the better the sexual function), with no statistically significant difference between the groups with and without genital lesion. Regarding women, 37.7% had a Female Sexual Distress Scale (FSDS) score > 15, evidencing an alteration in sexual life. The mean score of women with genital lesions was significantly higher than that of those without genital lesions. Regarding FSFI, 48.7% of the women scored < 26, indicating sexual dysfunction. That alteration was equally distributed among women with and without genital lesions.
Sampogna et al.2 have reported that 48.2% of their patients could be characterized as having minor psychological disorders (depression and anxiety). The prevalence of sexual dysfunction varied according to the question analyzed, from 35.5% with the PDI question to 71.3% with the IPSO question. The prevalence was higher among patients with psoriatic arthritis, psychological disorders and SAPASI scores > 20 in all questions. Regarding the IPSO question, the prevalence of sexual dysfunction was higher among women.
In the study by Ermertcan et al.,19 the patients were divided into six groups as follows: female and male healthy controls; female and male psoriasis groups without depression; and female and male psoriasis groups with depression. The mean PASI among women without depression was 6.53 ± 4.25, and among those with depression, 6.54 ± 6.96. The DLQI showed a more significant worsening of quality of life in the group with depression as compared with that without depression. The FSfitotal score showed significant sexual dysfunction in the groups with psoriasis with and without depression as compared with the control group. However, no statistically significant difference was observed between the two groups with psoriasis. When the domains were assessed separately, the scores of all domains, except for lubrication and pain, were significantly worse in the groups with psoriasis. A negative correlation was observed between the FSfiand DLQI scores, but PASI showed no correlation.
Regarding the male groups, the mean PASI was 9.27 ± 6.03 in those with psoriasis alone, and 7.31 ± 4.51 in those with psoriasis and depression. The DLQI total score was significantly higher in patients with psoriasis and depression when compared with those without depression, characterizing worse quality of life. The IIEF total score showed significant dysfunction in the groups with psoriasis as compared with the control group, and no difference was observed between the two groups with psoriasis. When the domains were assessed separately, the satisfaction with sexual relationship was significantly low in patients with psoriasis; the other domains were also lower, but with no statistically significant difference. The IIEF total score showed correlation with neither PASI nor DLQI.
Gupta et al.23 have found that, of 120 patients studied, 49 (40.8%) reported a decline in sexual activity after the onset of psoriasis. In the group with sexual dysfunction, 77% of the patients had joint pain as compared with 54% of those in the group without sexual dysfunction. The group with sexual dysfunction also had significantly more depression and higher tendency towards alcohol consumption. The decline in sexual activity was associated with the effect of psoriasis on physical appearance by 60% of the patients, while 14.9% attributed it to decreased sex drive of their spouse/partner.
The study by Goulding et al.20 has focused mainly on the presence of erectile dysfunction. The mean DLQI score was significantly higher in the group with psoriasis. Of 92 individuals, 53 (58%) had an IIEF score < 21, which indicates erectile dysfunction, which occurred in 64 of 120 controls (49%), showing no statistically significant difference.
Guenther et al.22 have assessed the treatment with ustekinumab in 1,996 patients. Prior to treatment, 22.6% of the patients had sexual dysfunction, assessed based on DLQI Question #9. Sexual dysfunction was most frequent in women (27.1%) than in men (20.8%). The proportion of patients with sexual dysfunction was directly correlated with the PASI.
DISCUSSION
Data on the sexual difficulties of patients with psoriasis are scarce. The hypotheses to explain sexual dysfunction in that group of patients include the severity of skin findings, the psychological effects of the condition on patients, concerns of the sexual partner, and side effects of the medical treatments for psoriasis.22
Multiple studies have associated psoriasis with psychological morbidity, especially depression and anxiety.10,25,26 Some authors have suggested that high levels of pro-inflammatory cytokines, specifically tumor necrosis factor alpha and interleukine 1, involved in the pathogenesis of psoriasis, are related to depression.27 Those psychological conditions were more prevalent in patients with psoriasis in four of the studies analyzed.
A positive correlation between sexual dysfunction and depression has been reported in the studies by Mercan et al.,18 Sampogna et al.,2 and Gupta et al.23 However, Mercan et al.18 have observed that patients with psoriasis had more sexual disorders related to orgasm than to sexual drive. Because the sexual disorders of depression affect typically the sexual drive rather than orgasm itself, those authors have suggested that the sexual dysfunction in psoriasis might be related to other reasons than depression. Ermertcan et al.,19 comparing healthy individuals and individuals with psoriasis with and without depression, have found no correlation between psychological problems and presence of sexual dysfunction.
Regarding the clinical findings, the severe/moderate form was more associated with sexual dysfunction in two studies,2,22 but two other showed no statistically significant difference.19,21 The presence of psoriatic arthritis has been also related in two studies.2,23 The presence of genital lesion had an impact on quality of life, but showed no correlation with sexual function,2,19,20 except in the study by Meeuwis et al.24 In that study, women with genital psoriasis had impaired sexual function, but that did not happen to the male group. The authors have suggested that the presence of the genital lesion itself might not be the cause of sexual function decline, but the patient's subjective experience.
Except for the study by Goulding et al.,20 all others have shown a decline in the sexual function of patients with psoriasis. An explanation for that could be the fact that those authors have used in the control group individuals with other dermatological diseases, but including some conditions that can be extensive, with esthetic and physical limitations similar to those of psoriasis, such as atopic eczema and lupus erythematosus. The authors have reported high prevalence of erectile dysfunction in the total sample studied (50%), corresponding to the population with dermatological diseases. In addition, sexual dysfunction has already been correlated with other skin conditions, such as sexually transmissible diseases,28,29 vitiligo,30,31 chronic urticaria,31 and neurodermatitis.18,28
Finally, it is worth noting the result reported by Meeuwis et al.,24 according to which only 9% of their patients were satisfied with the attention given by healthcare professionals to their sexual problems, while 43% perceived it as insufficient. Those data emphasize that this type of symptomatology is frequently neglected in medical practice,32 and stress the importance of assessing the impact of psoriasis regarding not only cutaneous and joint involvements, but also psychosocial and sexual impairments.
During this study review, the association of the term "Brazil" in the database search identified no article. Considering the sociocultural diversities of each population, a specific study of the Brazilian population to provide more information about our patients is required.
REFERENCES
-
1Myers WA, Gottlieb AB, Mease P. Psoriasis and psoriatic arthritis: clinical features and disease mechanisms. Clin Dermatol 2006;24(5):438-47.
-
2Sampogna F, Gisondi P, Tabolli S, Abeni D; IDI Multipurpose Psoriasis Research on Vital Experiences investigators. Impairment of sexual life in patients with psoriasis. Dermatology 2007;214(2):144-50.
-
3Langham S, Langham J, Goertz HP, Ratcliffe M. Large-scale, prospective, observational studies in patients with psoriasis and psoriatic arthritis: a systematic and critical view. BMC Med Res Methodol 2011;11:32.
-
4Chandran V, Chentag CT, Gladman DD. Sensitivity of the classification of psoriatic arthritis criteria in early psoriatic arthritis. Arthritis Rheum 2007;57(8):1560-3.
-
5Kleinert S, Feuchtenberger M, Kneitz C, Tony HP. Psoriatic arthritis: clinical spectrum and diagnostic procedures. Clin Dermatol 2007;25(6):519-23.
-
6Silva KS, Silva EAT. Psoríase e sua relação com aspectos psicológicos, stress e eventos da vida. Est Psicol 2007;24:257-66.
-
7Finlay AY, Cole EC. The effect of severe psoriasis on the quality of life of 369 patients. Br J Dermatol 1995;132(2):236-44.
-
8Lee YW, Park EJ, Kwon IH, Kim KH, Kim KJ. Impact of Psoriasis on Quality of Life: Relationship between Clinical Response to Therapy and Change in Health-related Quality of Life. Ann Dermatol 2010;22(4):389-96.
-
9Rapp SR, Feldman SR, Exum ML, Fleischer AB Jr, Reboussin DM. Psoriasis causes as much disability as other major medical diseases. J Am Acad Dermatol 1999;41(3 Pt1):401-7.
-
10Russo PAJ, Ilchef R, Cooper AJ. Psychiatric morbidity in psoriasis: a review. Austral J Dermatol 2004;45(3):155-9.
-
11Martins GA, Arruda L, Mugnaini AS. Validação de questionários de avaliação da qualidade de vida em pacientes de psoríase. An Bras Dermatol 2004;79(5):521-35.
-
12Organização Mundial de Saúde (OMS) -Classificação de transtornos mentais e de comportamento da CID 10. Descrições clínicas e diretrizes diagnósticas. Trad D Caetano. Porto Alegre, Artes Médicas, 1993.
-
13Wylie G, Evans CD, Gupta G. Reduced libido and erectile dysfunction: rarely reported side-effects of methotrexate. Clin Exp Dermatol 2009;34(7):e234.
-
14Reynolds OD. Erectile dysfunction in etretinate treatment. Arch Dermatol 1991;127(3):425-6.
-
15Aguirre MA, Vélez A, Romero M, Collantes E. Gynecomastia and sexual impotence associated with methotrexate treatment. J Rheumatol 2002;29(8):1793-4.
-
16Niemeier V, Winckelsesser T, Gieler U. Skin disease and sexuality. An empirical study of sex behavior on patients with psoriasis vulgaris and neurodermatitis in comparison with skin-healthy probands. Hautarzt 1997;48(9):629-33.
-
17Ramsay B, O'Reagan M. A survey of the social and psychological effects of psoriasis. Br J Dermatol 1988;118(2):195-201.
-
18Mercan S, Altunay IK, Demir B, Akpinar A, Kayaoglu S. Sexual dysfunctions in patients with neurodermatitis and psoriasis. J Sex Marital Ther 2008;34(2):160-8.
-
19Türel Ermertcan A, Temeltaş G, Deveci A, Dinç G, Güler HB, Oztürkcan S. Sexual dysfunction in patients with psoriasis. J Dermatol 2006;33(11):772-8.
-
20Goulding JMR, Price CL, Defty CL, Hulangamuwa CS, Bader E, Ahmed I. Erectile dysfunction in patients with psoriasis: increased prevalence, an unmet need, and a chance to intervene. Br J Dermatol 2011;164(1):103-9.
-
21Al-Mazeedi K, El-Shazly M, Al-Ajmi HS. Impact of psoriasis on quality of life in Kuwait. Int J Dermatol 2006;45(4):418-24.
-
22Guenther L, Han C, Szapary P, Schenkel B, Poulin Y, Bourcier M et al Impact of ustekinumab on health-related quality of life and sexual difficulties associated with psoriasis: results from phase III clinical trials. J Eur Acad Dermatol Venereol 2011;25(7):851-7.
-
23Gupta MA, Gupta AK. Psoriasis and sex: a study of moderately to severely affected patients. Int J Dermatol 1997;36(4):259-62.
-
24Meeuwis KA, de Hullu JA, van de Nieuwenhof HP, Evers AW, Massuger LF, van de Kerkhof PC et al Quality of life and sexual health in patients with genital psoriasis. Br J Dermatol 2011;164(6):1247-55.
-
25Krueger G, Koo J, Lebwohl M, Menter A, Stern RS, Rolstad T.The impact of psoriasis on quality of life: results of a 1998 National Psoriasis Foundation patient-membership survey. Arch Dermatol 2001;137(3):280-4.
-
26Ginsburg IH, Link BG. Psychossocial consequences of rejection and stigma feelings in psoriasis patients. Int J Dermatol 1993;32(8):578-91.
-
27Schiepers OJ, Wichers MC, Maes M. Cytokines and major depression. Prog Neuropsychopharmacol Biol Psychiatry 2005;29(2):201-17.
-
28Ermertcan AT. Sexual dysfunction in dermatological diseases. J Eur Acad Dermatol Venereol 2009;23(9):999-1007.
-
29Mandal MC, Mullick SI, Nahar JS, Khanum M, Lahiry S, Islam MA. Prevalence of psychiatric ailments among patients with sexually transmitted disease. Mymensingh Med J 2007;16(2 suppl):S23-7.
-
30Ahmed I, Ahmed S, Nasreen S. Frequency and pattern of psychiatric disorders in patients with vitiligo. J Ayub Med Coll Abbottabad 2007;19(3):19-21.
-
31Sukan M, Maner F. The problems in sexual functions of vitiligo and chronic urticaria patients. J Sex Marital Ther 2007;33(1):55-64.
-
32Ostensen M. Função sexual comprometida em pacientes com doença reumática independente da atividade da doença, tratamento e função gonadal. Rev Bras Reumatol 2009;49(6):639-42.
Sexual dysfunction in patients with psoriasis and psoriatic arthritis - a systematic review
Publication Dates
-
Publication in this collection
04 Dec 2012 -
Date of issue
Dec 2012
History
-
Received
03 Nov 2011 -
Accepted
05 Sept 2012