ABSTRACT
OBJECTIVE
To evaluate the prevalence of leisure-time physical inactivity in Brazilian adolescents and their association with geographical and sociodemographic variables.
METHODS
The sample was composed by 74,589 adolescents participating in the Study of Cardiovascular Risks in Adolescents (ERICA). This cross-sectional study of school basis with national scope involved adolescents aged from 12 to 17 years in Brazilian cities with more than 100 thousand inhabitants. The prevalence of leisure-time physical inactivity was categorized according to the volume of weekly practice (< 300; 0 min). The prevalences were estimated for the total sample and by sex. Poisson regression models were used to assess associated factors.
RESULTS
The prevalence of leisure-time physical inactivity was 54.3% (95%CI 53.4-55.2), and higher for the female sex (70.7%, 95%CI 69.5-71.9) compared to the male (38.0%, 95%CI 36.7-39.4). More than a quarter of adolescents (26.5%, 95%CI 25.8-27.3) reported not practicing physical activity in the leisure time, a condition more prevalent for girls (39.8%, 95%CI 38.8-40.9) than boys (13.4%, 95%CI 12.4-14.4). For girls, the variables that were associated with physical inactivity were: reside in the Northeast (RP = 1.13, 95%CI 1.08-1.19), Southeast (RP = 1.16, 95%CI 1.11-1.22) and South (RP = 1.12, 95%CI 1.06-1.18); have 16-17 years (RP = 1.06, 95%CI 1.12-1.15); and belong to the lower economic class (RP = 1.33, 95%CI 1.20-1.48). The same factors, except reside in the Southeast and South, were also associated with not practicing physical activity in the leisure time for the same group. In males, as well as the region, being older (p < 0.001) and declaring to be indigenous (RP = 0.37, 95%CI 0.19-0.73) were also associated with not practicing physical activities in the leisure time.
CONCLUSIONS
The prevalence of leisure-time physical inactivity in Brazilian adolescents is high. It presents regional variations and is associated with age and low socioeconomic status. Special attention should be given to girls and to those who do not engage in any physical activity during the leisure time, so that they can adopt a more active lifestyle.
Adolescent; Motor Activity; Sedentary Lifestyle; Prevalence; Cross-Sectional Studies
RESUMO
OBJETIVO
Avaliar a prevalência de inatividade física no lazer em adolescentes brasileiros e sua associação com variáveis geográficas e sociodemográficas.
MÉTODOS
A amostra foi composta por 74.589 adolescentes participantes do Estudo de Riscos Cardiovasculares em Adolescentes (ERICA). Esse estudo transversal de base escolar com abrangência nacional envolveu adolescentes brasileiros de 12 a 17 anos de municípios com mais de 100 mil habitantes. A prevalência de inatividade física no lazer foi categorizada de acordo com o volume de prática semanal (< 300; zero min). As prevalências foram estimadas para o total da amostra analisada e por sexo. Modelos de regressão de Poisson foram utilizados para avaliar fatores associados.
RESULTADOS
A prevalência de inatividade física no lazer foi de 54,3% (IC95% 53,4-55,2), superior no sexo feminino (70,7%, IC95% 69,5-71,9) comparado ao masculino (38,0%, IC95% 36,7-39,4). Mais de um quarto dos adolescentes (26,5%, IC95% 25,8-27,3) referiram não praticar atividade física no lazer, condição mais prevalente no sexo feminino (39,8%, IC95% 38,8-40,9) que no masculino (13,4%, IC95% 12,4-14,4). Para o sexo feminino, as variáveis que se associaram à inatividade física foram: residir nas regiões Nordeste (RP = 1,13, IC95% 1,08-1,19), Sudeste (RP = 1,16, IC95% 1,11-1,22) e Sul (RP = 1,12, IC95% 1,06-1,18); ter 16-17 anos (RP = 1,12, IC95% 1,06-1,15); e pertencer à classe econômica mais baixa (RP = 1,33, IC95% 1,20-1,48). Os mesmos fatores, exceto residir no Sudeste e Sul, também associaram-se com não praticar atividade física no lazer no mesmo grupo. No sexo masculino, além da região, ser mais velho (p < 0,001) e declarar-se indígena (RP = 0,37, IC95% 0,19-0,73) associaram-se à prevalência de não praticar atividade física no lazer.
CONCLUSÕES
A prevalência de inatividade física no lazer em adolescentes brasileiros é elevada, apresenta variações regionais e está associada à idade e ao baixo nível socioeconômico. Especial atenção deve ser dada às meninas e aos que não praticam nenhuma atividade física no lazer, a fim de que estes possam adotar estilo de vida mais ativo.
Adolescente; Atividade Motora; Estilo de Vida Sedentário; Prevalência; Estudo Transversal
INTRODUCTION
Physical inactivity is one of the main risk factors for the development of chronic diseases2525. World Health Organization. Global status report on noncommunicable diseases 2010. Geneva; 2011.. According to the study by Lee et al.1717. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219-29. DOI:10.1016/S0140-6736(12)61031-9, it is possible to assign to physical inactivity the occurrence of 5.3 million deaths in the world only in the year of 2008. In Brazil, 13.0% of deaths in 2008 were attributed to physical inactivity1717. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219-29. DOI:10.1016/S0140-6736(12)61031-9. This information relate directly to the adult population, but also to the population of adolescents, since active adolescents have a higher chance to remain active in adulthood11. Azevedo MR, Araujo CL, Silva MC, Hallal PC. Tracking of physical activity from adolescence to adulthood: a population-based study. Rev Saude Publica. 2007;41(1):69-75. DOI:10.1590/S0034-89102007000100010,2222. Telama R, Yang X, Viikari J, Valimaki I, Wanne O, Raitakari O. Physical activity from childhood to adulthood: a 21-year tracking study. Am J Prev Med. 2005;28(3):267-73. DOI:10.1016/j.amepre.2004.12.003. Practicing physical activities in this age group is associated with immediate benefits, such as prevention of cardiovascular and metabolic risk factors1111. Ekelund U, Luan J, Sherar LB, Esliger DW, Griew P, Cooper A. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA. 2012;307(7):704-12. DOI:10.1001/jama.2012.156,1818. Moliner-Urdiales D, Ruiz JR, Ortega FB, Rey-Lopez JP, Vicente-Rodriguez G, España-Romero V et al. Association of objectively assessed physical activity with total and central body fat in Spanish adolescents; the HELENA Study. Int J Obes (Lond). 2009;33(10):1126-35. DOI:10.1038/ijo.2009.139, and also predicts better health in adulthood1515. Hasselstrom H, Hansen SE, Froberg K, Andersen LB. Physical fitness and physical activity during adolescence as predictors of cardiovascular disease risk in young adulthood. Danish Youth and Sports Study: an eight-year follow-up study. Int J Sports Med. 2002;23 Suppl 1:S27-31. DOI:10.1055/s-2002-28458.
Nevertheless, the world prevalence of physical inactivity in adolescents (13-15 years) is of 80.0%, considering the recommendation of at least 60 min/day of moderate or vigorous physical activity1414. Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380(9838):247-57. DOI:10.1016/S0140-6736(12)60646-1. In Brazil, a systematic review with meta-analysis showed great variation in the prevalence of physical inactivity, both in male adolescents (2.0%-80.0%) and females (14.0%-91.0%). The study also noted the data shortage in the North (one study) and Midwest (no studies) regions, and the great variability in the definition of physical inactivity22. Barufaldi LA, Abreu GA, Coutinho ESF, Bloch KV. Meta-analysis of the prevalence of physical inactivity among Brazilian adolescents. Cad Saude Publica. 2012;28(6):1019-32. DOI:10.1590/S0102-311X2012000600002.
The Pesquisa Nacional de Saúde do Escolar (PeNSE – National Survey of Students’ Health), which involved Brazilian adolescents of the ninth year of basic education to all regions of the Country and used the cutting point of less than 300 min/week to define physical inactivity, found prevalence of 57.0% in 20091313. Hallal PC, Knuth AG, Cruz DKA, Mendes MI, Malta DC. Prática de atividade física em adolescentes brasileiros. Cienc Saude Coletiva. 2010;15 Supl 2:3035-42. DOI:10.1590/S1413-81232010000800008. The same survey conducted in 2012, with some changes in the methodology and in the research tool, found prevalence of physical inactivity of 71.0%, being greater in the Northeast (76.0%) and lower in the South region (65.0%)1919. Rezende LF, Azeredo CM, Canella DS, Claro RM, Castro IR, Levy RB et al. Sociodemographic and behavioral factors associated with physical activity in Brazilian adolescents. BMC Public Health. 2014;14:485. DOI:10.1186/1471-2458-14-485.
These data reinforce the need for continuous monitoring of the population levels of physical activity in adolescence, to provide more effective intervention strategies. Thus, the objective of this study was to evaluate the prevalence of leisure-time physical inactivity in Brazilian adolescents and their association with geographical and sociodemographic variables.
METHODS
The sample was composed of adolescents participating in the Study of Cardiovascular Risks in Adolescents (ERICA). This is a cross-sectional study of school basis with national scope, including public and private schools located in urban and rural areas. The data collection took place between February 2013 and November 2014. We assessed 85,615 students, residents of Brazilian municipalities with more than 100 thousand inhabitants (medium and large municipalities). In this study, we used data from 74,589 adolescents aged between 12 and 17 years, who have fully completed the block on practice of physical activity in ERICA.
For sampling, the target population of ERICA was divided into 32 geographical strata: 26 state capitals and the Federal District, and five more sets representing other municipalities with more than 100 thousand inhabitants in each macro-region of the country. The sample size was calculated for each stratum, to ensure representative estimates of each one. The schools were selected with probability proportional to a size directly proportional to the number of students at the school in the school years considered, and inversely proportional to the distance between the municipality and the capital of the state in question. In total, 1,247 schools participated in this study, of 124 municipalities with more than 100 thousand inhabitants.
In the second stage, we selected three combinations of shift (morning and afternoon) and eligible years (seventh, eighth and ninth years of Elementary School and first, second and third years of High School). In the third stage, a class of each combination of shift and year was selected by means of equiprobability. All students of the selected classes were invited to participate of ERICA. More details about the design of the sample of ERICA can be obtained in a previous publication2323. Vasconcellos MTL, Silva PLN, Szklo M, Kuschnir MCC, Klein CH, Abreu GA et al. Desenho da amostra do Estudo do Risco Cardiovascular em Adolescentes (ERICA). Cad Saude Publica. 2015;31(5):921-30. DOI:10.1590/0102-311X00043214.
The research protocol of ERICA was described by Bloch et al.44. Bloch KV, Szklo M, Kuschnir MC, Abreu GA, Barufaldi LA, Klein CH et al. The Study of Cardiovascular Risk in Adolescents - ERICA: rationale, design and sample characteristics of a national survey examining cardiovascular risk factor profile in Brazilian adolescents. BMC Public Health. 2015;15:94. DOI:10.1186/s12889-015-1442-x In summary, after being selected, the schools were contacted and invited to participate in the study. ERICA data collection involved the application of a structured questionnaire, anthropometric assessment, measurement of blood pressure and blood collection. The variables used in this study were obtained by structured questionnaire, filled by the adolescents on their own, inserted into an electronic data collector (personal digital assistant – PDA).
To determine the level of physical activity of adolescents, we used an adaptation of the Self-Administered Physical Activity Checklist2020. Sallis JF, Strikmiller PK, Harsha DW, Feldman HA, Ehlinger S, Stone EJ et al. Validation of interviewer- and self-administered physical activity checklists for fifth grade students. Med Sci Sports Exerc. 1996;28(7):840-51. DOI:10.1097/00005768-199607000-00011, which consists of a list of 24 modes and allows the adolescents to report frequency (days) and the time (hours and minutes) that they performed, in the last week, some of the activities listed. This questionnaire has already been used in other research on Brazil33. Bastos JP, Araujo CLP, Hallal PC. Prevalence of insufficient physical activity and associated factors in Brazilian adolescents. J Phys Act Health. 2008;5(6):777-94.,77. Cureau FV, Duarte P, Santos DL, Reichert FF. Clustering of risk factors for noncommunicable diseases in Brazilian adolescents: prevalence and correlates. J Phys Act Health. 2014;11(5):942-9. DOI:10.1123/jpah.2012-0247 and the version used in ERICA was validated in Brazilian adolescents1212. Farias Júnior JC, Lopes AS, Mota J, Santos MP, Ribeiro JC, Hallal PC. Validade e reprodutibilidade de um questionário para medida de atividade física em adolescentes: uma adaptação do Self-Administered Physical Activity Checklist. Rev Bras Epidemiol. 2012;15(1):198-210. DOI:10.1590/S1415-790X2012000100018. For estimates of the prevalence of leisure-time physical inactivity, were used only questions relating to this domain (21 questions).
To determine the level of physical activity, we calculated the product between time and frequency in each activity and the sum of the times obtained. The adolescents who not accumulated at least 300 min/week of physical activity in the leisure time were considered inactive2424. World Health Organization. Global recommendations on physical activity for health. Geneva; 2010.. The prevalence of adolescents who did not report any practice of physical activity during the leisure time in the week preceding the survey (0 min/week) was also evaluated.
Among the independent variables, we analyzed the geographic location according to the region of residence of adolescents (North, Northeast, Midwest, Southeast and South) and the following sociodemographic characteristics: sex; age in full years, later recategorized (12-13, 14-15, 16-17 years); and self-declared skin color (white, black, brown (mixed), yellow (Asian) or indigenous). Socioeconomic status was defined using the Critério Brasil55. Associação Brasileira de Empresas de Pesquisa. Critério Brasil de avaliação econômica 2013. São Paulo: ABEP; 2013. Disponível em: http://www.abep.org/criterio-brasil
http://www.abep.org/criterio-brasil...
, which considers possession of goods, presence of housekeeper and education of the chief of the household. The score obtained can range from 0 to 46 points. This score was categorized into levels according to recommendation of the instrument: A (35-46 points), B (23-34 points), C (14-22 points), D (8-13 points) and E (0-7 points). Classes D and E were regrouped in the same category, due to low frequency.
The analysis of data involved the estimation of prevalence of leisure-time physical inactivity (< 300 min/week) and of those who did not perform any physical activity during the leisure time at all (0 min/week), with their respective 95% confidence intervals (95%CI). The prevalences were estimated for the entire sample, stratified by sex and described according to the independent variables studied.
The associations of the two categories of physical inactivity with exposure variables were investigated using Poisson regression. The adjusted model was built with only one level of the input variables, which were taken from those with less influence to obtain the final model. We analyzed the presence of multicollinearity. The adjustment of the model was evaluated by goodness-of-fit test. The presence of interactions was tested by multiplicative approach through heterogeneity test. Poisson regression models showed good overall adjustment and we did not observe multicollinearity problems or significant interactions.
The results of the sample were expanded to represent the Brazilian population of schoolchildren in Brazilian cities with more than 100 thousand inhabitants. The sample weights calculated for the study were considered to obtain the estimates2323. Vasconcellos MTL, Silva PLN, Szklo M, Kuschnir MCC, Klein CH, Abreu GA et al. Desenho da amostra do Estudo do Risco Cardiovascular em Adolescentes (ERICA). Cad Saude Publica. 2015;31(5):921-30. DOI:10.1590/0102-311X00043214. Analyses were conducted in Stata 14 with a significance level of 5%.
All adolescents agreed in writing to participate in the study; five states also requested signing of an informed consent signed by the parent or legal guardian, according to the determination of the Research Ethics Committees (REC) or State Secretariat of Education. ERICA was approved by the REC of each of the 27 Federation units in Brazil.
RESULTS
Half of the sample was composed of adolescents who studied in strata of the Southeast and Northeast regions, 75.0% in capitals, and 79.0% in public schools. The vast majority of the schools were located in urban areas (98.0%). The girls are the majority in the sample (55.0%), as well as those in the age group of 14-15 years (37.0%), brown skin color (52.0%) and intermediate (B and C) economic classes (86.0%).
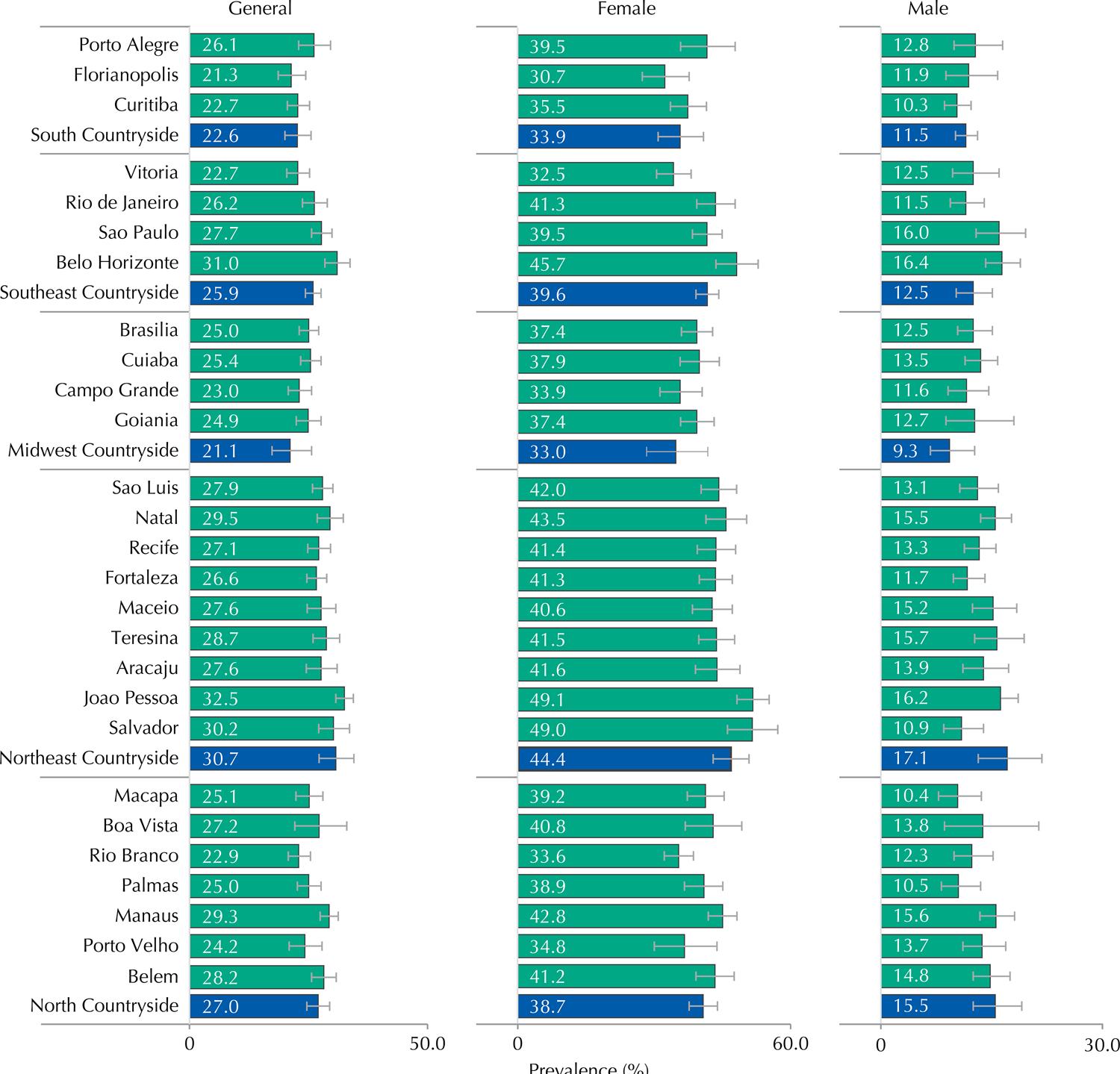
The prevalence of leisure-time physical inactivity was 54.3% (95%CI 53.4-55.2), higher for the female sex (70.7%, 95%CI 69.5-71.9) compared to the male (38.0%, 95%CI 36.7-39.4) (Table 1). Figure 1 shows the prevalence of adolescents who not accumulated at least 300 min/week of physical activity in the leisure time. The results point to Belo Horizonte (58.0%, 95%CI 55.1-60.9) as the capital with the highest prevalence of general leisure-time physical inactivity, while Macapa (44.8%, 95%CI 42.1-47.6) was the capital with the lowest prevalence. The highest prevalence of physical inactivity by sex were observed in Salvador (75.7%, 95%CI 71.4-79.5) and Florianopolis (44.4%, 95%CI 38.5-50.4) for female and male sexes, respectively (Figure 1).
Prevalence of leisure-time physical inactivity (< 300 min/week) in adolescents from the 27 Brazilian capitals (green bars) and set of municipalities with more than 100 thousand inhabitants, not capitals of regions, according to sex. ERICA, 2013-2014.
Among Brazilian adolescents, 26.5% (95%CI 25.8-27.3) reported not to perform physical activity during the leisure time (0 min/week), with higher prevalence in females (39.8%, 95%CI 38.8-40.9%) than males (13.4%, 95%CI 12.4-14.4) (Table 1). In Joao Pessoa, the capital with higher prevalence of no physical activity, one every three adolescents does not practice any physical activity during the leisure time, a ratio that changes to one for every two when considering the female sex (Figure 2).
Prevalence (%) of no physical activity during the leisure time (0 min/week) in adolescents of the 27 Brazilian capitals (green bars) and set of municipalities with more than 100,000 inhabitants, not capitals of regions, according to sex. ERICA, 2013-2014.
Table 1 presents the prevalence and adjusted prevalence ratios in the total sample, to physical inactivity and no physical activity according to the independent variables. The highest prevalence of leisure-time physical inactivity were observed in the Northeast for any physical activity; and in the Northeast and South when the cutoff point was at least 300 min/week. In the adjusted model, the prevalence of physical inactivity in both categories is associated directly with age and inversely with economic level (p-value for linear trend < 0.05).
After stratification by sex, the highest prevalence of physical inactivity were in the Northeast and Southeast in the female sex, and in the South region between male adolescents. Among girls, the higher age (p < 0.001) and the lowest socioeconomic class (p < 0.001) were associated with higher prevalence of physical inactivity. In male adolescents, the prevalence of physical inactivity tended to increase as the socioeconomic condition decreased (p = 0.003); to declare oneself as indigenous, black or brown were protection factors regarding physical inactivity in the adjusted model (p < 0.05) (Table 2).
Concerning the non-practice of physical activity (Table 3), we also observed an increasing gradient of the prevalence of no physical activity at leisure with increasing age in both sexes (p < 0.001). Worst socioeconomic condition was associated with higher prevalence of no leisure-time physical activity only among female adolescents (p = 0.001).
DISCUSSION
ERICA data showed that more than half of Brazilian adolescents, residents of cities of medium and large size, do not reach the recommendation of at least 300 min/week of physical activity for health promotion. This percentage is even higher among girls, surpassing 70.0%. Equally disturbing is the fact that one in four adolescents do not practice any physical activity in the leisure time, a prevalence that approaches 50.0% among girls in some capitals.
The measurement of population levels of physical activity, especially in childhood and adolescence, is quite complex and to compare studies is difficult. The use of questionnaires does not always produce accurate estimates, which can lead to misclassification, and its agreement with direct measures is only partial2121. Steene-Johannessen J, Anderssen SA, Ploeg HP, Hendriksen IJ, Donnelly AE, Brage S et al. Are self-report measures able to define individuals as physically active or inactive? Med Sci Sports Exerc. 2015 Oct 1. DOI:10.1249/MSS.0000000000000760. However, using direct measurement methods, such as accelerometer, would be infeasible in a study as ERICA due to high costs and the complex logistics involved. The use of an already validated instrument1212. Farias Júnior JC, Lopes AS, Mota J, Santos MP, Ribeiro JC, Hallal PC. Validade e reprodutibilidade de um questionário para medida de atividade física em adolescentes: uma adaptação do Self-Administered Physical Activity Checklist. Rev Bras Epidemiol. 2012;15(1):198-210. DOI:10.1590/S1415-790X2012000100018 increases the reliability of the data, however it does not reduce the difficulty of comparisons due to the different instruments used and the different domains of physical activity assessed in each study. In this study we decided to investigate only physical activity during the leisure time, because it is the most explored domain on the ERICA questionnaire, when compared to the other issues, and because it is the most important area for the implementation of the recommendations of physical activity among Brazilian adolescents1919. Rezende LF, Azeredo CM, Canella DS, Claro RM, Castro IR, Levy RB et al. Sociodemographic and behavioral factors associated with physical activity in Brazilian adolescents. BMC Public Health. 2014;14:485. DOI:10.1186/1471-2458-14-485.
The scientific literature shows that the practice of physical activity in adolescence is associated with numerous health benefits during adolescence and with equally important reflections on adulthood1111. Ekelund U, Luan J, Sherar LB, Esliger DW, Griew P, Cooper A. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA. 2012;307(7):704-12. DOI:10.1001/jama.2012.156,1515. Hasselstrom H, Hansen SE, Froberg K, Andersen LB. Physical fitness and physical activity during adolescence as predictors of cardiovascular disease risk in young adulthood. Danish Youth and Sports Study: an eight-year follow-up study. Int J Sports Med. 2002;23 Suppl 1:S27-31. DOI:10.1055/s-2002-28458,1818. Moliner-Urdiales D, Ruiz JR, Ortega FB, Rey-Lopez JP, Vicente-Rodriguez G, España-Romero V et al. Association of objectively assessed physical activity with total and central body fat in Spanish adolescents; the HELENA Study. Int J Obes (Lond). 2009;33(10):1126-35. DOI:10.1038/ijo.2009.139. Although many studies use the recommendation of at least 300 min/week of moderate to vigorous physical activity for health promotion in adolescents, evidence support that smaller volumes can also bring benefits. These variations are supported by multicausal origins of each morbidity, especially chronic ones, as well as by different physiological mechanisms that can relate physical activity to a certain morbidity. A systematic review showed that 30 min/day of physical activity are sufficient to obtain cardiovascular benefits in health among adolescents1616. Janssen I, Leblanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010;7:40. DOI:10.1186/1479-5868-7-40. However, a randomized clinical trial involving overweight and inactive young people pointed out that 20 min of aerobic physical activity, practiced five times a week, for 13 weeks, already reduces the risk of developing diabetes, general percentage of fat and visceral fat, and also improves physical fitness when compared to the control group that kept usual routine88. Davis CL, Pollock NK, Waller JL, Allison JD, Dennis BA, Bassali R et al. Exercise dose and diabetes risk in overweight and obese children: a randomized controlled trial. JAMA. 2012;308(11):1103-12. DOI:10.1001/2012.jama.10762.
Interventions that encourage the transition from total physical inactivity to a state of action, regardless of the frequency of physical activity initially practiced, can promote immediate impacts. This strategy can work complementary to programs aimed at the maintenance and gradual increase of the practice of physical activity among adolescents. The leisure domain is favorable to the development of interventions.
In this context, school seems to be the ideal space to conduct these interventions, due to the large concentration of adolescents, safety, physical space and professionals able to stimulate and supervise these activities. To increase the effective time of physical practice during physical education classes and to make them more attractive should be a goal, as well as reducing the number of layoffs. Other actions such as sedentary time interruptions during class, active intervals proposition and extracurricular activities are strategies that have been studied and could increase the practice of physical activities in schools and have important consequences outside them66. Centers for Disease Control and Prevention. School health guidelines to promote healthy eating and physical activity. MMWR Recomm Rep. 2011;60(RR-5):1-76.. However, these actions must be connected to an increased social support for practice and improving access, making it socially egalitarian, especially in countries of socioeconomic conditions so heterogeneous as Brazil.
The interest in the study of physical (in)activity epidemiology in Brazil is growing, with the majority of publications focused on South-Southeast axis and recent growth of publications in the Northeast region. However, studies conducted in the North and Midwest regions of the Country are still rare in this thematic22. Barufaldi LA, Abreu GA, Coutinho ESF, Bloch KV. Meta-analysis of the prevalence of physical inactivity among Brazilian adolescents. Cad Saude Publica. 2012;28(6):1019-32. DOI:10.1590/S0102-311X2012000600002. In ERICA, these regions showed the lowest prevalence of leisure-time physical inactivity, regardless of sex. The latest edition of PeNSE also noted greater performance of leisure time activities in the North region, and related this result to cultural issues and favorable urban features not always found in more urbanized regions such as the Southeast, Northeast and South of the Country1919. Rezende LF, Azeredo CM, Canella DS, Claro RM, Castro IR, Levy RB et al. Sociodemographic and behavioral factors associated with physical activity in Brazilian adolescents. BMC Public Health. 2014;14:485. DOI:10.1186/1471-2458-14-485. However, further studies are needed in those regions for a better understanding of the associated and promoters factors of the practice of physical activity.
Higher prevalence of physical inactivity in the female sex is often seen, especially during the leisure time33. Bastos JP, Araujo CLP, Hallal PC. Prevalence of insufficient physical activity and associated factors in Brazilian adolescents. J Phys Act Health. 2008;5(6):777-94.,1414. Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380(9838):247-57. DOI:10.1016/S0140-6736(12)60646-1,1919. Rezende LF, Azeredo CM, Canella DS, Claro RM, Castro IR, Levy RB et al. Sociodemographic and behavioral factors associated with physical activity in Brazilian adolescents. BMC Public Health. 2014;14:485. DOI:10.1186/1471-2458-14-485. The same occurs with increasing age1010. Dumith SC, Gigante DP, Domingues MR, Kohl HW 3rd. Physical activity change during adolescence: a systematic review and a pooled analysis. Int J Epidemiol. 2011;40(3):685-98. DOI:10.1093/ije/dyq272, being even more pronounced in the transition from adolescence to adulthood11. Azevedo MR, Araujo CL, Silva MC, Hallal PC. Tracking of physical activity from adolescence to adulthood: a population-based study. Rev Saude Publica. 2007;41(1):69-75. DOI:10.1590/S0034-89102007000100010, a phase that the adolescents studied have yet to experience. Socioeconomic status was associated with physical inactivity among girls, especially in relation to not reaching the recommendation of at least 300 min/week, reinforcing the interpretations that related this variable to the opportunity to practice structured physical activity (purchase of equipment, transportation, payment of fees, among others) and emotional and social support of family (as permission, stimulus, company to practice and easier access to information)99. Dollman J, Lewis NR. The impact of socioeconomic position on sport participation among South Australian youth. J Sci Med Sport. 2010;13(3):318-22. DOI:10.1016/j.jsams.2009.04.007.
The first data about physical inactivity of ERICA help size how challenging is this problem in Brazil. These results are useful for directing actions that seek to reduce physical inactivity in Brazilian adolescents. Future analyses of ERICA can expand this knowledge by assessing, for example, the importance of the school structure, seasonality and climatic variations, and the relation of physical inactivity with several cardiovascular risk factors surveyed.
Investment in stimulus policies to physical activity in adolescents should be treated as priority by Government agendas relating to sport, health and education, as well as research funding institutions. Governmental actions as the Segundo Tempo, Mais Educação and Atleta na Escola programs are important steps that should be expanded. The construction of the Bill of Guidelines and Bases of the National Sport System, which aims to make the investment in sport in a government policy to mainstream the practice of sports in the country, may also be favorable.
These resources should assist in changing the current scenario in a comprehensive manner, making school an important partner for the promotion of activities that involve the whole school community. The development of actions aimed at the transition of those who engage in no physical activity to adopt some practice must be a priority, even if these people do not achieve, at first, the recommendations of physical activity for health.
REFERENCES
-
1Azevedo MR, Araujo CL, Silva MC, Hallal PC. Tracking of physical activity from adolescence to adulthood: a population-based study. Rev Saude Publica 2007;41(1):69-75. DOI:10.1590/S0034-89102007000100010
-
2Barufaldi LA, Abreu GA, Coutinho ESF, Bloch KV. Meta-analysis of the prevalence of physical inactivity among Brazilian adolescents. Cad Saude Publica 2012;28(6):1019-32. DOI:10.1590/S0102-311X2012000600002
-
3Bastos JP, Araujo CLP, Hallal PC. Prevalence of insufficient physical activity and associated factors in Brazilian adolescents. J Phys Act Health 2008;5(6):777-94.
-
4Bloch KV, Szklo M, Kuschnir MC, Abreu GA, Barufaldi LA, Klein CH et al. The Study of Cardiovascular Risk in Adolescents - ERICA: rationale, design and sample characteristics of a national survey examining cardiovascular risk factor profile in Brazilian adolescents. BMC Public Health 2015;15:94. DOI:10.1186/s12889-015-1442-x
-
5Associação Brasileira de Empresas de Pesquisa. Critério Brasil de avaliação econômica 2013. São Paulo: ABEP; 2013. Disponível em: http://www.abep.org/criterio-brasil
» http://www.abep.org/criterio-brasil -
6Centers for Disease Control and Prevention. School health guidelines to promote healthy eating and physical activity. MMWR Recomm Rep 2011;60(RR-5):1-76.
-
7Cureau FV, Duarte P, Santos DL, Reichert FF. Clustering of risk factors for noncommunicable diseases in Brazilian adolescents: prevalence and correlates. J Phys Act Health 2014;11(5):942-9. DOI:10.1123/jpah.2012-0247
-
8Davis CL, Pollock NK, Waller JL, Allison JD, Dennis BA, Bassali R et al. Exercise dose and diabetes risk in overweight and obese children: a randomized controlled trial. JAMA 2012;308(11):1103-12. DOI:10.1001/2012.jama.10762
-
9Dollman J, Lewis NR. The impact of socioeconomic position on sport participation among South Australian youth. J Sci Med Sport 2010;13(3):318-22. DOI:10.1016/j.jsams.2009.04.007
-
10Dumith SC, Gigante DP, Domingues MR, Kohl HW 3rd. Physical activity change during adolescence: a systematic review and a pooled analysis. Int J Epidemiol 2011;40(3):685-98. DOI:10.1093/ije/dyq272
-
11Ekelund U, Luan J, Sherar LB, Esliger DW, Griew P, Cooper A. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA 2012;307(7):704-12. DOI:10.1001/jama.2012.156
-
12Farias Júnior JC, Lopes AS, Mota J, Santos MP, Ribeiro JC, Hallal PC. Validade e reprodutibilidade de um questionário para medida de atividade física em adolescentes: uma adaptação do Self-Administered Physical Activity Checklist. Rev Bras Epidemiol 2012;15(1):198-210. DOI:10.1590/S1415-790X2012000100018
-
13Hallal PC, Knuth AG, Cruz DKA, Mendes MI, Malta DC. Prática de atividade física em adolescentes brasileiros. Cienc Saude Coletiva 2010;15 Supl 2:3035-42. DOI:10.1590/S1413-81232010000800008
-
14Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet 2012;380(9838):247-57. DOI:10.1016/S0140-6736(12)60646-1
-
15Hasselstrom H, Hansen SE, Froberg K, Andersen LB. Physical fitness and physical activity during adolescence as predictors of cardiovascular disease risk in young adulthood. Danish Youth and Sports Study: an eight-year follow-up study. Int J Sports Med 2002;23 Suppl 1:S27-31. DOI:10.1055/s-2002-28458
-
16Janssen I, Leblanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010;7:40. DOI:10.1186/1479-5868-7-40
-
17Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 2012;380(9838):219-29. DOI:10.1016/S0140-6736(12)61031-9
-
18Moliner-Urdiales D, Ruiz JR, Ortega FB, Rey-Lopez JP, Vicente-Rodriguez G, España-Romero V et al. Association of objectively assessed physical activity with total and central body fat in Spanish adolescents; the HELENA Study. Int J Obes (Lond) 2009;33(10):1126-35. DOI:10.1038/ijo.2009.139
-
19Rezende LF, Azeredo CM, Canella DS, Claro RM, Castro IR, Levy RB et al. Sociodemographic and behavioral factors associated with physical activity in Brazilian adolescents. BMC Public Health 2014;14:485. DOI:10.1186/1471-2458-14-485
-
20Sallis JF, Strikmiller PK, Harsha DW, Feldman HA, Ehlinger S, Stone EJ et al. Validation of interviewer- and self-administered physical activity checklists for fifth grade students. Med Sci Sports Exerc 1996;28(7):840-51. DOI:10.1097/00005768-199607000-00011
-
21Steene-Johannessen J, Anderssen SA, Ploeg HP, Hendriksen IJ, Donnelly AE, Brage S et al. Are self-report measures able to define individuals as physically active or inactive? Med Sci Sports Exerc 2015 Oct 1. DOI:10.1249/MSS.0000000000000760
-
22Telama R, Yang X, Viikari J, Valimaki I, Wanne O, Raitakari O. Physical activity from childhood to adulthood: a 21-year tracking study. Am J Prev Med 2005;28(3):267-73. DOI:10.1016/j.amepre.2004.12.003
-
23Vasconcellos MTL, Silva PLN, Szklo M, Kuschnir MCC, Klein CH, Abreu GA et al. Desenho da amostra do Estudo do Risco Cardiovascular em Adolescentes (ERICA). Cad Saude Publica 2015;31(5):921-30. DOI:10.1590/0102-311X00043214
-
24World Health Organization. Global recommendations on physical activity for health. Geneva; 2010.
-
25World Health Organization. Global status report on noncommunicable diseases 2010. Geneva; 2011.
-
Funding: Departamento de Ciência e Tecnologia da Secretaria de Ciência, Tecnologia e Insumos Estratégicos do Ministério da Saúde (Decit/SCTIE/MS), Fundo Setorial de Saúde (CT-Saúde) do Ministério da Ciência, Tecnologia e Inovação (MCTI – Process FINEP: 01090421), the Conselho Nacional de Pesquisa (CNPq – Processes: 565037/2010-2, 405009/2012-7 e 457050/2013-6) and Fundo de Incentivo à Pesquisa do Hospital de Clinicas de Porto Alegre (FIPE-HCPA – Process: 09-098). The authors: Cureau FV has a CAPES sandwich PhD scholarship (Process BEX 9556/14-1) and Bloch KV (Process 304595/2012-8) and Schaan BD (Process 305116/2012-6) have research productivity scholarships from CNPq.
Publication Dates
-
Publication in this collection
2016
History
-
Received
14 Sept 2015 -
Accepted
28 Oct 2015