|
A. GPR versus no treatment
|
Durmus et al.2121 Durmuş D, Alayli G, Uzun O, Tander B, Canturk F, Bek Y, et al. Effects of two exercise interventions on pulmonary functions in the patients with ankylosing spondylitis. Joint Bone Spine. 2009;76(2):150-5. http://dx.doi.org/10.1016/j.jbspin.2008.06.013. PMid:19084457.
http://dx.doi.org/10.1016/j.jbspin.2008....
(ankylosing Spondylitis) |
12 weeks |
Pain (0-10): MD –2.90 (95% CI –3.99 to –1.80) favoring GPR
|
GPR significantly reduced pain and disease activity and improved functional capacity compared to no intervention. |
Functional capacity (0-100)11 Ferrari S, Vanti C, O’Reilly C. Clinical presentation and physiotherapy treatment of 4 patients with low back pain and isthmic spondylolisthesis. J Chiropr Med. 2012;11(2):94-103. http://dx.doi.org/10.1016/j.jcm.2011.11.001. PMid:23204952.
http://dx.doi.org/10.1016/j.jcm.2011.11....
: MD 1.02 (95% CI –2.15 to 0.11) favoring GPR |
| Disease activity22 Ribeiro F, Leite M, Silva F, Sousa O. Physical exercise in the treatment of Ankylosing Spondylitis: a systematic review. Acta Reumatol Port. 2007;32(2):129-37. PMid:17572651. (0-10): MD –0.98 (95% CI -1.57 to –0.38) favoring GPR
|
Gil et al.2222 Gil VFB, Osis MJD, Faúndes A. Lumbar pain during pregnancy: efficacy of Global Postural Reeducation (GPR) treatment. Fisioter Pesqui. 2011;18(2):164-70.
(pregnancy-related back pain) |
8 weeks |
Pain (0-10): MD –5.5 (95% CI –6.08 to –4.91) favoring GPR
|
GPR significantly reduced pain and disability compared to no intervention. |
Disability33 Gyurcsik ZN, Andras A, Bodnar N, Szekanecz Z, Szanto S. Improvement in pain intensity, spine stiffness, and mobility during a controlled individualized physiotherapy program in ankylosing spondylitis. Rheumatol Int. 2012;32(12):3931-6. http://dx.doi.org/10.1007/s00296-011-2325-9. PMid:22198694.
http://dx.doi.org/10.1007/s00296-011-232...
: MD -9.10 (95% CI –11.09 to –7.10) favoring GPR
|
Lawand et al.3535 Lawand P, Lombardi Júnior I, Jones A, Sardim C, Ribeiro LH, Natour J. Effect of a muscle stretching program using the global postural reeducation method for patients with chronic low back pain: a randomized controlled trial. Joint Bone Spine. 2015;82(4):272-7. http://dx.doi.org/10.1016/j.jbspin.2015.01.015. PMid:25881758.
http://dx.doi.org/10.1016/j.jbspin.2015....
(chronic low back pain) |
12 weeks |
Pain (0-10): MD –3.1 (95% CI –3.79 to –2.40) favoring GPR* |
GPR significantly reduced pain and disability and improved some domains of SF-36 (vitality, emotional aspects and mental health) compared to no intervention. |
| Disability (0-24): MD –4.4 (95% CI –6.05 to –2.74) favoring GPR
|
| 6 months |
Pain (0-10): MD –1.5 (95% CI –2.16 to –0.83) favoring GPR
|
| Disability (0-24): MD –4 (95% CI –5.8 to –2.18) favoring GPR
|
|
B. GPR versus segmental stretching
|
Amorim et al.3232 Amorim CS, Gracitelli ME, Marques AP, Alves VL. Effectiveness of global postural reeducation compared to segmental exercises on function, pain, and quality of life of patients with scapular dyskinesis associated with neck pain: a preliminary clinical trial. J Manipulative Physiol Ther. 2014;37(6):441-7. http://dx.doi.org/10.1016/j.jmpt.2013.08.011. PMid:25092553.
http://dx.doi.org/10.1016/j.jmpt.2013.08...
(neck pain) |
10 weeks |
Pain (0-10): MD –2.06 (95% CI –3.05 to –1.06) favoring GPR
|
GPR reduced pain and disability compared to segmental stretching alone. |
Disability (0-50)11 Ferrari S, Vanti C, O’Reilly C. Clinical presentation and physiotherapy treatment of 4 patients with low back pain and isthmic spondylolisthesis. J Chiropr Med. 2012;11(2):94-103. http://dx.doi.org/10.1016/j.jcm.2011.11.001. PMid:23204952.
http://dx.doi.org/10.1016/j.jcm.2011.11....
: MD –7.3 (95% CI –12.16 to –2.61) favoring GPR
|
Cunha et al.44 Cunha AC, Burke TN, Franca FJ, Marques AP. Effect of global posture reeducation and of static stretching on pain, range of motion, and quality of life in women with chronic neck pain: a randomized clinical trial. Clinics (Sao Paulo). 2008;63(6):763-70. http://dx.doi.org/10.1590/S1807-59322008000600010. PMid:19060998.
http://dx.doi.org/10.1590/S1807-59322008...
(neck pain) |
6 weeks |
Pain (0-10): MD 1.0 (95% CI 0.04 to 1.96) favoring SS
|
Segmental stretching alone was significantly better than GPR for pain reduction immediately and after six weeks. |
| 12 weeks |
Pain (0-10): MD 1.1 (95% CI 0.05 to 2.14) favoring SS
|
Cabral et al.2020 Cabral CM, Yumi C, Sacco ICN, Casarotto RA, Marques AP. Efficacy of two muscle stretching modalities in treating the patellofemoral syndrome: a comparative study. Fisioter Pesqui. 2007;14(2):48-56.
(patellofemoral pain) |
8 weeks |
Pain (0-10): MD 0.7 (95% CI –2.64 to 0.12) favoring GPR; |
GPR did not significantly reduce pain or disability compared to segmental stretching. |
|
Disability (0-100)22 Ribeiro F, Leite M, Silva F, Sousa O. Physical exercise in the treatment of Ankylosing Spondylitis: a systematic review. Acta Reumatol Port. 2007;32(2):129-37. PMid:17572651.: MD –5.5 (95% CI –14.63 to 3.63) favoring the control condition |
Maluf et al.55 Maluf SA, Moreno BG, Crivello O, Cabral CM, Bortolotti G, Marques AP. Global postural reeducation and static stretching exercises in the treatment of myogenic temporomandibular disorders: a randomized study. J Manipulative Physiol Ther. 2010;33(7):500-7. http://dx.doi.org/10.1016/j.jmpt.2010.08.005. PMid:20937428.
http://dx.doi.org/10.1016/j.jmpt.2010.08...
(temporomandibular disorder) |
8 weeks |
Pain (0-10)
|
GPR did not reduce TMJ pain compared to segmental stretching. Conversely, segmental stretching was more effective than GPR in reducing headache intensity at 8 weeks. |
| TMJ: MD –0.5 (95% CI –1.68 to 0.62) favoring GPR |
| Neck pain: MD –0.4 (95% CI –1.79 to 0.85) favoring GPR |
| Headache: MD 1.50 (95% CI 0.24 to 2.75) favoring SS
|
| 16 weeks |
Pain (0-10)
|
| TMJ: MD –0.98 (95% CI –2.11 to 0.15) favoring GPR |
| Neck pain: –1.25 (95% CI –2.52 to 0.02) favoring GPR |
| Headache: MD –0.23 (95% CI –1.43 to 0.97) favoring GPR |
|
C. GPR versus other treatments
|
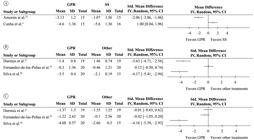
Adorno
et al.3131 Adorno MLGR, Brasil-Neto JP. Avaliação da qualidade de vida com o instrumento SF-36 em lombalgia crônica. Acta Ortop Bras. 2013;21(4):202-7. http://dx.doi.org/10.1590/S1413-78522013000400004. PMid:24453669.
http://dx.doi.org/10.1590/S1413-78522013...
(back pain) |
12 weeks |
Pain (0-10): MD 0.7 (95% CI –2.44 to 1.04) favoring Isostretching; |
GPR did not significantly reduce pain immediately and at three months follow-up compared to Isostreching. |
| 20 weeks |
Pain (0-10): MD –1.2 (95% CI –2.8 to 0.43) favoring GPR; |
Durmus et al.2121 Durmuş D, Alayli G, Uzun O, Tander B, Canturk F, Bek Y, et al. Effects of two exercise interventions on pulmonary functions in the patients with ankylosing spondylitis. Joint Bone Spine. 2009;76(2):150-5. http://dx.doi.org/10.1016/j.jbspin.2008.06.013. PMid:19084457.
http://dx.doi.org/10.1016/j.jbspin.2008....
(Ankylosing Spondylitis) |
12 weeks |
Pain (0-10):MD –0.46 (95% CI –1.48 to 0.56) favoring GPR; |
GPR did not significantly reduce pain and functional capacity compared to conventional exercise regimen, but significantly reduced disease activity. |
Functional capacity11 Ferrari S, Vanti C, O’Reilly C. Clinical presentation and physiotherapy treatment of 4 patients with low back pain and isthmic spondylolisthesis. J Chiropr Med. 2012;11(2):94-103. http://dx.doi.org/10.1016/j.jcm.2011.11.001. PMid:23204952.
http://dx.doi.org/10.1016/j.jcm.2011.11....
(0-10): MD –0.01 (95% CI –0.65 to 0.62) favoring GPR |
| Disease activity22 Ribeiro F, Leite M, Silva F, Sousa O. Physical exercise in the treatment of Ankylosing Spondylitis: a systematic review. Acta Reumatol Port. 2007;32(2):129-37. PMid:17572651. (0-10): MD –3.63 (95% CI –4.71 to –2.56) favoring GPR
|
Fernandez-de-las-Peñas et al.3333 Fernandez-de-Las-Penas C, Alonso-Blanco C, Morales-Cabezas M, Miangolarra-Page JC. Two exercise interventions for the management of patients with ankylosing spondylitis: a randomized controlled trial. Am J Phys Med Rehabil. 2005;84(6):407-19. http://dx.doi.org/10.1097/01.phm.0000163862.89217.fe. PMid:15905654.
http://dx.doi.org/10.1097/01.phm.0000163...
(Ankylosing Spondylitis) |
16 weeks |
Functional capacity33 Gyurcsik ZN, Andras A, Bodnar N, Szekanecz Z, Szanto S. Improvement in pain intensity, spine stiffness, and mobility during a controlled individualized physiotherapy program in ankylosing spondylitis. Rheumatol Int. 2012;32(12):3931-6. http://dx.doi.org/10.1007/s00296-011-2325-9. PMid:22198694.
http://dx.doi.org/10.1007/s00296-011-232...
(0-10): MD –0.42 (–1.05 to 0.20) favoring GPR
Disease activity22 Ribeiro F, Leite M, Silva F, Sousa O. Physical exercise in the treatment of Ankylosing Spondylitis: a systematic review. Acta Reumatol Port. 2007;32(2):129-37. PMid:17572651. (0-10): MD 0.12 (95% CI –0.50, 0.74) favoring conventional physical therapy |
GPR did not significantly reduce disease activity nor improve pain compared to conventional exercise regimen, immediately and at one year follow-up. |
|
|
|
Fernandez-de-las-Peñas et al.3434 Fernandez-de-Las-Penas C, Alonso-Blanco C, Alguacil-Diego IM, Miangolarra-Page JC. One-year follow-up of two exercise interventions for the management of patients with ankylosing spondylitis: a randomized controlled trial. Am J Phys Med Rehabil. 2006;85(7):559-67. http://dx.doi.org/10.1097/01.phm.0000223358.25983.df. PMid:16788386.
http://dx.doi.org/10.1097/01.phm.0000223...
(b)
(Ankylosing Spondylitis) |
One year |
Functional capacity33 Gyurcsik ZN, Andras A, Bodnar N, Szekanecz Z, Szanto S. Improvement in pain intensity, spine stiffness, and mobility during a controlled individualized physiotherapy program in ankylosing spondylitis. Rheumatol Int. 2012;32(12):3931-6. http://dx.doi.org/10.1007/s00296-011-2325-9. PMid:22198694.
http://dx.doi.org/10.1007/s00296-011-232...
(0-10): MD –0.61 (95% CI –1.38 to 0.16) favoring GPR
Disease activity22 Ribeiro F, Leite M, Silva F, Sousa O. Physical exercise in the treatment of Ankylosing Spondylitis: a systematic review. Acta Reumatol Port. 2007;32(2):129-37. PMid:17572651. (0-10): MD –0.06 (95% CI –0.83 to 0.71) favoring GPR |
Silva et al.3030 Silva EM, Andrade SC, Vilar MJ. Evaluation of the effects of Global Postural Reeducation in patients with ankylosing spondylitis. Rheumatol Int. 2012;32(7):2155-63. http://dx.doi.org/10.1007/s00296-011-1938-3. PMid:21544639.
http://dx.doi.org/10.1007/s00296-011-193...
(Ankylosing Spondylitis) |
16 weeks |
Pain (0-10)
Cervical pain: MD 1.3 (95% CI 1.02 to 1.57) favoring the control condition
Dorsal pain: MD 0.1 (95% CI –0.15 to 0.35) favoring the control condition
Lumbar pain: MD –0.5 (95% CI –0.77 to –0.22) favoring GPR
Functional capacity: MD –0.60 (95% CI –0.68 to –0.51) favoring GPR
Disease activity: MD –1.4 (95% CI –1.59 to –1.20) favoring GPR
|
GPR did not reduce cervical and dorsal pain compared to the control intervention. Lumbar pain significantly reduced for the GPR group. Functional capacity and disease activity significantly improved in the GPR group compared to the control intervention. |

 Thumbnail
Thumbnail
 Thumbnail
Thumbnail

