| Huang et al., 2020 14
|
Wuhan, China |
Series a comprised of 41 cases hospitalized as at January 2 nd 2020 |
RT-PCR + for COVID-19 |
Leukopenia (25%) and lymphopenia (63%) |
Fever (98%) + coughing (76%) + myalgia/fatigue (44%), dyspnea (55%), sputum production (28%), headache (8%), (5%) and diarrhea (3%) |
Symptoms such as diarrhea, nausea, vomiting and headache were present; 32% of total cases and 38% of cases admitted to ITU had comorbidities, of which diabetes was the most common (20%). All cases had pneumonia, 98% bilateral. |
| Guan WJ et al., 2020 12
|
China |
Cohort a of 1,099 cases from 552 hospitals in 30 provinces |
RT-PCR + for COVID-19 |
Lymphopenia (83.2%) |
Coughing (67.8%) + fever (43.8% at admission and 88.7% during hospitalization) |
15% had the severe form of the disease; 23.7% had at least one comorbidity (38% of severe cases). |
| Chen T et al., 2020 30
|
China |
Retrospective case series, that (i) died (n=113) and (ii) that recovered (n=161) |
RT-PCR + for COVID-19 |
Lymphopenia in 39% of deaths and 5% of recovered and leukocytosis in 50% of deaths and 4% of recovered |
Fever (~90%) + coughing (~66-70%) + milder symptoms; dyspnea and tight chest more common among deaths, as well as loss of consciousness |
63% of cases that died and 39% of those that recovered had at least one chronic disease: hypertension (48%), cardiovascular diseases (14%) and cerebrovascular diseases (4%). Deaths presented tachycardia (50%) and tachypnea (27%), and saturation ≤ 93% (64%); 8% of cases that died and 10% of those that recovered did not have fever, but did have fatigue (~50%), coughing (68%), dyspnea (44%), myalgia (22%) or diarrhea (28%) as initial symptoms. |
| Bhatraju PK et al., 2020 13
|
Seattle, United States |
Series with 24 cases ≥18 years old hospitalized in ITU |
RT-PCR + for COVID-19 |
75% lymphopenia and search for other pathogens |
Dyspnea and coughing (88%) + fever (50%); sputum production (42%), rhinorrhea (17%), sore throat (8%) and headache (8%) |
58% had diabetes and 14% had asthma and the disease was exacerbated with use of glucocorticoids; 22% were smokers; 33% had more than one chronic condition. |
| Wang Z et al., 2020 15
|
China |
Retrospective series with 69 cases hospitalized at the Union Hospital, in Wuhan, between January 16 and 29, 2020 |
RT-PCR + for COVID-19 |
Reduction in neutrophils (39%), eosinophils (72%) and lymphocytes; lymphopenia (42%), higher among deaths (79% vs 32%) |
Fever (87%), coughing (55%), fatigue (42%), myalgia (33%) |
All 14 deaths (20%) had saturation ≤90%, were older (70.5 years vs 37 years), had more comorbidities (hypertension 36% vs 7%), cardiovascular disease (36% vs 5%) and diabetes (43% vs 2%), and increased inflammatory cytokines. |
| Mao L et al., 2020 29
|
Wuhan, China |
Retrospective series of 214 hospitalized cases; data retrieved from medical records |
RT-PCR + for COVID-19 |
Inflammatory response pattern, principally in severe cases: more leukocytes and neutrophils, fewer lymphocytes and higher CRP levels |
Fever (132 [61.7%]), dry cough (107 [50.0%]) and anorexia (68 [31.8%]). CNS: dizziness (16.8%) and headache (13.1%). PNS: anosmia (5.1%) and ageusia (5.6%) |
Severe cases were older (58.7 ± 15.0 years vs 48.9 ± 14.7 years), had more comorbidities (42 [47.7%] vs 41 [32.5%]), hypertension (32 [36.4%] vs 19 [15.1%]), and had fewer symptoms considered typical such as fever (40 [45.5%] vs 92 [73%]) and coughing (30 [34.1%] vs 77 [61.1%]). Severe cases presented damage to liver, kidneys and muscles. NS symptoms were more common in severe cases, but with no laboratory differences between those who did or did not have PNS symptoms. |
| Giacomelli A et al., 2020 19
|
Milan, Italy |
( Letter to the editor ) Cross-sectional study with 88 hospitalized cases; 59 interviewed |
Not reported |
Not reported |
Fever (72.8%), coughing (37.3%), dyspnea (25.4%), arthralgia (5.1%), at least one smell or taste sense disorder (33.9%) or both (18.6%) |
Symptoms appeared more in women (52.6% vs 25%) and younger people (median 56 years, IQR 47-60 years vs 66 years, IQR 52-77). 72.8% had pneumonia at hospital admission. |
| Vaira LA et al., 2020 20
|
Italia |
Brief communication: 320 cases |
Not reported |
Not reported |
Anosmia and ageusia associated with fever. Some kind of dysfunction: 19.4% (not accompanied by nasal obstruction or rhinitis symptoms) |
|
| Pan L et al., 2020 21
|
Hubei, China |
Cross-sectional study: 204 hospitalized cases |
RT-PCR + for COVID-19 |
Increased AST and ALT in the group of patients with ALT (20.4%) and AST (16.5%) digestive symptoms, compared to the group with no ALT (5.9%) and AST (5.0%) digestive symptoms |
50.5% of hospitalized patients had digestive symptoms: loss of appetite (78.64%), diarrhea (34%) and vomiting (3.9%). Concomitantly, 94% had respiratory symptoms: fever (92.23%) and weakness (52.42%) |
Descriptive, cross-section and multicenter study. Cases with digestive symptoms had longer hospitalization time in relation to patients without digestive symptoms (9 days vs 7.3 days). However, there was no significant difference in the time of hospital discharge, days in ITU or mortality between the groups . |
| Jin X et al., 2020 22
|
Zhejiang, China |
Retrospective study with 651 hospitalized cases and clinical/ epidemiological analysis of 74 cases with digestive symptoms |
RT-PCR + for COVID-19 |
Increase in AST isolated in patients with GI symptoms greater than in those with no GI symptoms (29.35 vs 24.4). No significant different in makers related to CRP infection and procalcitonin |
Digestive symptoms (diarrhea, vomiting, nausea) in 11.4% of total cases. Fever (85.54%), coughing (71.62%), sputum (39.19%), fatigue (31.08%) and headache (21.62%) |
Retrospective study. Chronic liver disease rate was higher in cases with GI symptoms in relation to those with no GI symptoms (10.81% vs 2.95%). Severe/critical type rate was greater in cases with GI symptoms than in those without symptoms (22.97% vs 8.14%). |

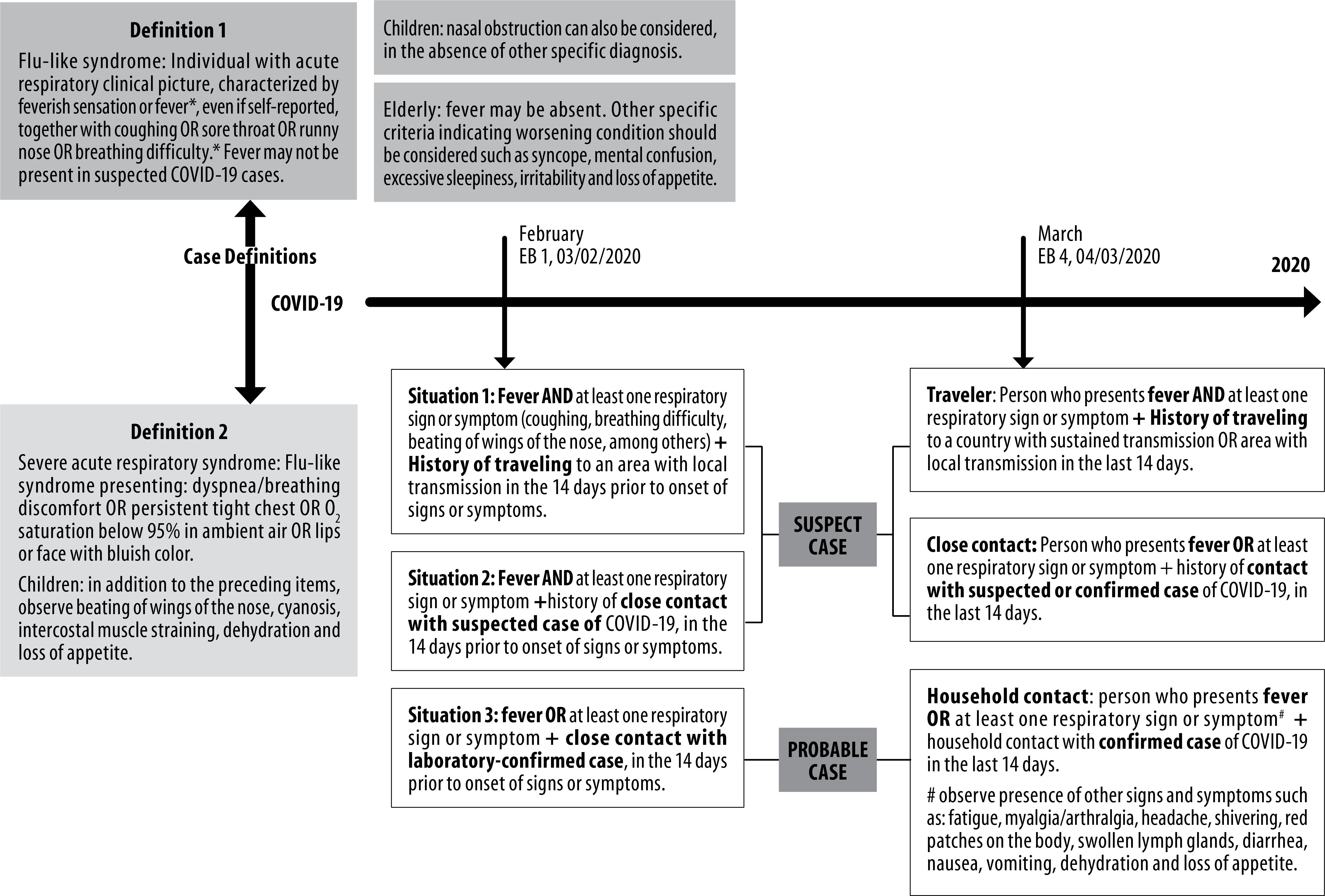 Legend: COVID-19, diseases caused by Sars-CoV-2; EB, Brazilian Health Ministry Epidemiological Bulletin.
Legend: COVID-19, diseases caused by Sars-CoV-2; EB, Brazilian Health Ministry Epidemiological Bulletin.