Abstract
INTRODUCTION: Echocardiographic, electrocardiographic and other cardiorespiratory variables can change during weaning from mechanical ventilation. OBJECTIVES: To analyze changes in cardiac function, using Doppler echocardiogram, in critical patients during weaning from mechanical ventilation, using two different weaning methods: pressure support ventilation and T-tube; and comparing patient subgroups: success vs. failure in weaning. METHODS: Randomized crossover clinical trial including patients under mechanical ventilation for more than 48 h and considered ready for weaning. Cardiorespiratory variables, oxygenation, electrocardiogram and Doppler echocardiogram findings were analyzed at baseline and after 30 min in pressure support ventilation and T-tube. Pressure support ventilation vs. T-tube and weaning success vs. failure were compared using ANOVA and Student's t-test. The level of significance was p<0.05. RESULTS: Twenty-four adult patients were evaluated. Seven patients failed at the first weaning attempt. No echocardiographic or electrocardiographic differences were observed between pressure support ventilation and T-tube. Weaning failure patients presented increases in left atrium, intraventricular septum thickness, posterior wall thickness and diameter of left ventricle and shorter isovolumetric relaxation time. Successfully weaned patients had higher levels of oxygenation. CONCLUSION: No differences were observed between Doppler echocardiographic variables and electrocardiographic and other cardiorespiratory variables during pressure support ventilation and T-tube. However cardiac structures were smaller, isovolumetric relaxation time was larger, and oxygenation level was greater in successfully weaned patients
Echocardiography; Doppler echocardiogram; Cardiorespiratory variables; Ventilator weaning; Artificial ventilation
CLINICAL SCIENCE
Echocardiographic evaluation during weaning from mechanical ventilation
Luciele Medianeira SchifelbainI; Silvia Regina Rios VieiraII; Janete Salles BraunerIII; Deise Mota PachecoIV; Alexandre Antonio NaujorksIV
IIntensive Care Unit, Hospital de Caridade Dr. Astrogildo de Azevedo, Santa Maria, RS, Brazil. E-mail: luciele@terra.com.br Tel.: 55 55 3222-2448
IIIntensive Care Unit, Hospital de Clínicas de Porto Alegre (HCPA), Porto Alegre, RS, Brazil
IIIIntensive Care Unit, HCPA, Porto Alegre, RS, Brazil; Hospital Nossa Senhora da Conceição, Porto Alegre, RS, Brazil
IVDepartment of Cardiology, Hospital de Caridade Dr. Astrogildo de Azevedo, Santa Maria, RS, Brazil
ABSTRACT
INTRODUCTION: Echocardiographic, electrocardiographic and other cardiorespiratory variables can change during weaning from mechanical ventilation.
OBJECTIVES: To analyze changes in cardiac function, using Doppler echocardiogram, in critical patients during weaning from mechanical ventilation, using two different weaning methods: pressure support ventilation and T-tube; and comparing patient subgroups: success vs. failure in weaning.
METHODS: Randomized crossover clinical trial including patients under mechanical ventilation for more than 48 h and considered ready for weaning. Cardiorespiratory variables, oxygenation, electrocardiogram and Doppler echocardiogram findings were analyzed at baseline and after 30 min in pressure support ventilation and T-tube. Pressure support ventilation vs. T-tube and weaning success vs. failure were compared using ANOVA and Student's t-test. The level of significance was p<0.05.
RESULTS: Twenty-four adult patients were evaluated. Seven patients failed at the first weaning attempt. No echocardiographic or electrocardiographic differences were observed between pressure support ventilation and T-tube. Weaning failure patients presented increases in left atrium, intraventricular septum thickness, posterior wall thickness and diameter of left ventricle and shorter isovolumetric relaxation time. Successfully weaned patients had higher levels of oxygenation.
CONCLUSION: No differences were observed between Doppler echocardiographic variables and electrocardiographic and other cardiorespiratory variables during pressure support ventilation and T-tube. However cardiac structures were smaller, isovolumetric relaxation time was larger, and oxygenation level was greater in successfully weaned patients.
Keywords: Echocardiography; Doppler echocardiogram; Cardiorespiratory variables; Ventilator weaning; Artificial ventilation.
INTRODUCTION
Weaning from mechanical ventilation (MV) involves changes in the interaction between patient and ventilator. During weaning, the support provided by the ventilator is reduced, while the patient progressively takes over the work of breathing.1 Changes associated with transition from MV to spontaneous ventilation overload the cardiorespiratory system with increases in: venous return, left ventricle (LV) afterload, O2 consumption and catecholamine secretion.
The return of spontaneous breathing can increase myocardial O2 demand and the product of heart rate × arterial blood pressure by as much as 35%, which can lead to myocardial ischemia. However, this increase was not associated with weaning failure.2-4 A study of 15 patients with chronic obstructive pulmonary disease who failed during weaning from MV demonstrated that, during the first 10 min of spontaneous breathing, there was an increase in cardiac index (CI), heart rate (HR), central venous pressure (CVP) and arterial blood pressure (BP).5 An increase in pulmonary capillary wedge pressure (PCWP) from 8 to 25 mmHg was associated with evidence of acute respiratory failure due to increased preload.5 After 1 week of treatment with diuretics, these patients were weaned successfully.5 There is evidence that 6-10% of patients exhibit electrocardiographic findings of cardiac ischemia while being weaned, mainly those with coronary artery disease.5
Echocardiography is being used routinely in some intensive care units (ICUs). It permits direct observation of all cardiac structures and the patient's hemodynamic status, allowing immediate intervention related to volume replacement and the use of inotropic agents.6,7 In patients on MV, its use can explain some cardiac morphological and functional analyses that may influence weaning from MV, particularly when weaning is difficult or there is refractory hypoxemia that cannot be explained by lung disease alone.8 Nevertheless, there are few descriptions in the literature of bedside studies of these cardiorespiratory changes during weaning from MV using echocardiography.9,10
The objective of this study was to analyze changes in cardiac function using Doppler echocardiogram in critical patients in a general ICU during weaning from MV using pressure support ventilation (PSV) and T-tube, and to compare a subgroup of patients: success vs. failure during the weaning trial.
MATERIALS AND METHODS
This study included adult patients (18 years or more) admitted to the adult general ICU of a hospital requiring invasive MV for at least 48 h and considered ready for weaning by the medical team. It was a randomized crossover clinical trial aiming to study changes in echocardiographic cardiac function variables (both systolic and diastolic) and other cardiorespiratory and electrocardiographic variables related to weaning from MV during two methods of weaning (PSV and T-tube). The research protocol was approved by the appropriate research ethics committee.
All patients were hemodynamically stable with normal central blood pressure values, conscious (Glasgow scale >13), with adequate gaseous exchange (O2 saturation >95%, fraction of inspired oxygen (FiO2) <40% and positive end-expiratory pressure (PEEP) = 5, with pulmonary radiological characteristics as in baseline conditions, no acidosis or alkalosis), normal electrolyte levels and the presence of respiratory drive. Informed consent was signed by the patients and/or family members. Exclusion criteria included hemodynamic instability, severe intracranial disease and barotrauma.
The sequence in which the methods were implemented was determined by randomly selecting sealed envelopes. This randomization was carried out by the duty physician before the patient was enrolled in the protocol. Patients were submitted to a baseline assessment and then placed on the first method of weaning for 30 min. After a rest period of 30 min, patients were submitted to the other method for 30 min.
One weaning method was T-tube, in which patients made the inspiratory and expiratory effort unaided, receiving oxygen at 5 L/min. The other method was PSV in which patients breathing was aided by equipment with graduated inspiratory pressure at an inspiratory level of 10 cmH2O. This PSV level is routinely used in the ICU during weaning trials. The humidification system used was heat-and moisture-exchanging (HME) filters.
The weaning protocol was interrupted if the patient exhibited: oxygen arterial saturation (SaO2) ,88%, oxygen arterial pressure (PaO2) ,60-55 mmHg; respiratory rate (ƒ) >35-38 rpm or increased by 50%; HR >140 bpm or increased by 20%; systolic blood pressure >180 mmHg or <90 mmHg or increased/reduced by 20%; and agitation, diaphoresis or a reduced level of consciousness. This was considered failure of the weaning trial.
Clinical status, respiratory mechanics and arterial blood gas analyses, electrocardiograms (ECG) and echocardiograms were performed during the trial period (at baseline and at the 30th minute of each ventilation mode). If the patient showed signs of decompensation before the predetermined time, the assessment was performed immediately and the patient placed back on MV with the same parameters used at the beginning of the weaning protocol.
Clinical assessment included data on identification, diagnosis, Acute Physiologic and Chronic Health Evaluation (APACHE) II score for the first 24 h after admission, level of consciousness, preexisting heart disease, use of sedative drugs and opioids, type of mechanical ventilator used, ventilation mode, MV parameters and arterial blood gas analysis. Patients were also monitored non-invasively: BP, HR, f and SaO2 using a multiparameter monitor (Philips; USA). Ventilation mechanics were monitored using a VENTRAK 1500 (Novametrix Medical Systems, Walling-ford, CT, USA) connected to a PC Pentium 100 using software provided by Novametrix for data storage and later analysis. The following parameters were analyzed: ƒ (rpm), tidal volume (VT = mL), minute volume (Ve = L/min), rapid-shallow breathing index (RSBI or ƒ/VT) and airway occlusion pressure (P0.1).
Cardiac performance was assessed using 12-lead ECG and echocardiogram using a Caris ultrasound machine (Esaote Spa, Genova, Italy) with pulse, continuous and color Doppler, and a 2.5-3.5 MHz transducer, coupled to a 17-inch Sony Cpd-e200 monitor. The following data were analyzed: Mode M; bidimensional mode; spectral and tissue Doppler and myocardial performance index (Tei index). Ejection fraction was determined using the Teicholz method as it offers greater accuracy than the Cubo method, has less interobserver variation and is less dependent on an optimal echocardiographic window to obtain measurements than the Simpson method.11 Doppler echocardiography was used to assess LV systolic and diastolic function and structural abnormalities. Echocardiogram was always performed by the same cardiologist. Echocardiogram and ECG were done at baseline and in the 30th minute of each method after resting for 30 min between methods.
Statistical analysis
Measurements obtained during PSV and T-tube were compared. Patients were classified into two groups based on weaning success or failure.
Analyses were performed with the aid of Statistical Package for the Social Sciences (SPSS) 12.0, and results were presented as mean±standard deviation or median (interquartile 25-75). Comparisons were made using Student's t-test for paired and unpaired samples and analysis of variance (ANOVA) for repeated measures. The level of significance was set at p<0.05.
RESULTS
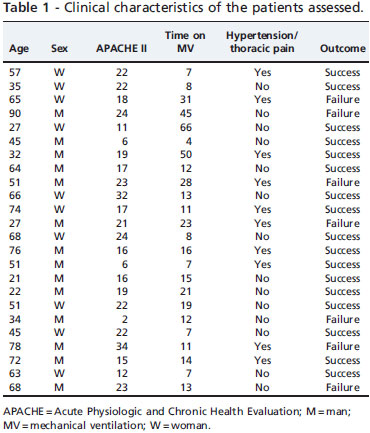
During the period between December 2005 and August 2007, 24 patients were assessed. Thirteen (58%) patients were male, and the mean age was 53±20 years. Mean APACHE score was 18±14. Median time on MV was 13 (8-21) days and length of stay in the ICU was 22 (13-35) days. Eight patients (33%) had neurological diseases, and the remaining patients had been admitted for sepsis, general postoperative care, neoplasms and respiratory infections. Ten patients (41.7%) had a history of hypertension and/or thoracic pain, with no history of myocardial infarction or previous left ventricular failure. Eleven patients were tracheostomized. Seven patients failed during the weaning trial. Two of them died and five were weaned later. Of the successfully weaned patients, only one was reintubated after 5 days, and one died because of a lymphoma. The individual characteristics of the patients assessed are described in Table 1.
At baseline, all patients were on MV settings, with PSV at 15-20 cmH2O, PEEP at 5 cmH2O and a FiO2 of 0.4. With respect to the variables analyzed at baseline and at the end of 30 min using Doppler echocardiogram, the size of the left atrium (LA), the interventricular septum, the posterior wall and LV diastolic diameter (LVD) were all significantly smaller among patients who were successfully weaned from MV at the first attempt. Isovolumetric relaxation time (IVRT) was significantly shorter among patients whose weaning failed. The Tei index values were slightly higher among patients who failed, but without statistical significance (Table 2).
The mean Doppler echocardiography results during the two weaning modes (PSV, T-tube) were very similar, and no differences were observed when comparing the outcome (success vs. failure in Table 3). Results observed during PSV and T-tube were similar to values observed at baseline.
Twelve-lead electrocardiograms did not detect any differences between baseline assessment and weaning modes assessed. No changes in ST segment were detected during continuous cardiac monitoring.
There were no statistical differences for cardiorespiratory assessment during baseline and weaning trials. However, patients whose weaning was successful showed higher PaO2 and SaO2 (133±30 vs. 103±33, p=0.04; and 98±1.1 vs. 96±1.9, p=0.01). We also observed a tendency to a lower ƒ/VT (75±39 vs. 91±19, p=0.13) and to a lower P0.1 (0.46±0.17 vs. 0.62±0.09, p=0.4) during T-tube in this group of patients.
DISCUSSION
There were no differences between the Doppler echocardiography variables during the two weaning methods. The analysis of the Doppler echocardiograms demonstrated that the sizes of cardiac structures were significantly smaller in patients who were successfully weaned from MV at the first attempt, whereas IVRT was significantly shorter among patients whose weaning failed. Considering cardiorespiratory variables, PaO2 and SaO2 were significantly higher among successfully weaned patients with no other significant differences.
Several research teams have investigated prognostic indices for weaning success, including ƒ/VT ratio12-14 and P0.1.15 The lower the ƒ/VT , the greater the chance of successfully withdrawing MV.12,14,16 In our study, f/VT was higher and P0.1 was lower among patients who could not be weaned, although without statistical difference. However, in agreement with the literature, successfully weaned patients showed better oxygenation levels.15
Physiological changes associated with the transition from MV to spontaneous breathing involve an overload of the cardiorespiratory system: increased venous return (pre-load), increased LV afterload, increase in O2 consumption from 15% to 25% and increased secretion of catecholamines.
In patients with preexisting heart disease (coronary artery disease and LV insufficiency), these physiological changes associated with spontaneous breathing can trigger LV failure, which in turn may lead to respiratory failure and unsuccessful weaning.2,3,17 In our study, there were no differences in cardiorespiratory variables analyzed by echocardiography between the two weaning methods, suggesting equivalency between both methods of weaning in the population studied. Our results are in disagreement with recent data published in the literature.10,18Caille et al.10 analyzed weaning patients and observed that echocardiogram can detect T-tube-induced changes in the central hemodynamic status, helping to identify patients at high risk of cardiac-related weaning failure. Cabello et al.,18 monitoring weaning patients with a Swan-Ganz catheter, also observed differences in cardiovascular responses comparing T-tube with PSV. It is important to consider that, in these studies, there was a large number of patients with cardiac diseases and/or signs of cardiac failure. In our sample, patients were under MV for a long period of time, but there was no evidence of preexisting defined heart disease or LV failure.
The baseline LA diameter, intraventricular septum thickness, posterior wall thickness and LV diastolic diameter were significantly larger among patients whose weaning failed. It has been demonstrated that increased LA size could cause an increased filling pressure due to reduced LV compliance or diastolic dysfunction. There is evidence in the literature suggesting that this increase in the size of the LA measured by echocardiography could be predictive of cardiovascular outcomes even in individuals without atrial pathologies or valve disease.19,20
We also observed in our study that the value of IVRT was significantly lower among failing weaning patients. Also, the pressure gradient represented by the deceleration time, which normally changes in line with IVRT, was lower, although not statistically significant among patients who failed. The deceleration time is characteristically prolonged when relaxation is abnormal and becomes shorter when relaxation is rapid or high ventricular filling pressures occur.21 The IVRT can be influenced by factors including ischemia, hypoxemia and right ventricle overload (which prolong the time) and blood volume status (indirect variation). Its absolute value is inversely related to PCWP,22 i.e. the lower the value of IVRT, the higher the PCWP.23 Our patients did not exhibit hypervolemia, which could have influenced the behavior of echocardiographic measurements. The preload, assessed in terms of the E/E' ratio measured by tissue Doppler, demonstrated variation within normal limits (below 15),24 without any significant difference between the two groups of patients.
Our research did not demonstrate electrocardiographic abnormalities at all assessment situations, suggesting less or no heart disease among these patients who were admitted predominantly as a result of neurological and infectious diseases, with only prior history of hypertension recorded. Research evaluation of weaning from MV has demonstrated cardiac ischemia mainly in patients with known coronary artery disease, and sometimes also in normal patients.4,25-29 In an earlier study carried out by our team, ST segment abnormalities suggestive of myocardial ischemia were also observed on ECG during both methods of weaning, but in this previous study, a greater number of severe cardiac patients was included.30
As limitations of this study, we have to consider that the number of patients evaluated was small. In addition, no severe ischemic heart or heart failure patients were included, which may explain the absence of ischemia and cardiac dysfunction during weaning. Another limitation is that, although no patient had clinical signs of cardiac failure, fluid balance or the use of diuretic drugs before the weaning trial were not recorded.
CONCLUSION
In the present study, there were no differences in echocardiographic evaluation or in electrocardiographic and other cardiorespiratory variables comparing PSV and T-tube in this population of cardiac patients receiving MV for a long period of time. Weaning failure patients presented LA diameter, intraventricular septum thickness, posterior wall thickness and LV diameter significantly larger than weaning success patients. Further studies with a greater number of patients and including subjects with heart disease are necessary in order to clarify echocardiographic changes during weaning from MV and differences between cardiac and non-cardiac patients. It seems that echocardiogram tests could be useful in identifying failure weaning patients in a subgroup of cardiac ones.
ACKNOWLEDGMENTS
We thank the Cardiovascular Institute in Santa Maria/RS (ICARDIO) for assistance with Doppler echocardiography and ECG tests.
REFERENCES
1. Hess D. Ventilator modes used in weaning. Chest. 2001;120(6 Suppl):S474-6, doi: 10.1378/chest.120.6_suppl.474S.
2. Chatila W, Ani S, Guaglianone D, Jacob B, Amoateng-Adjepong Y, Manthous CA. Cardiac ischemia during weaning from mechanical ventilation. Chest. 1996;109:1577-83, doi: 10.1378/chest.109.6.1577.
3. Lessard MR, Brochard LJ. Weaning from ventilatory support. Clin Chest Med. 1996;17:475-89, doi: 10.1016/S0272-5231(05)70328-2.
4. Srivastava S, Chatila W, Amoateng-Adjepong Y, Kanagasegar S, Jacob B, Zarich S, et al. Myocardial ischemia and weaning failure in patients with coronary artery disease: an update. Crit Care Med. 1999;27:2109-12, doi: 10.1097/00003246-199910000-00005.
5. Lemaire F, Teboul JL, Cinotti L, Giotto G, Abrouk F, Steg G, et al. Acute left ventricular dysfunction during unsuccessful weaning from mechanical ventilation. Anesthesiology. 1988;69:171-9, doi: 10.1097/00000542198808000-00004.
6. Loubieres Y, Vieillard-Baron A, Beauchet A, Fourme T, Page B, Jardin F. Echocardiographic evaluation of left ventricular function in critically ill patients: dynamic loading challenge using medical antishock trousers. Chest. 2000;118:1718-23, doi: 10.1378/chest.118.6.1718.
7. Dittoe N, Stultz D, Schwartz BP, Hahn HS. Quantitative left ventricular systolic function: from chamber to myocardium. Crit Care Med. 2007;35(8 Suppl):S330-9, doi: 10.1097/01.CCM.0000270245.70103.7E.
8. Ribeiro J, Marcelino P, Marum S, Fernandes A. Echocardiography: a fundamental part of the intensive care curriculum. Crit Care. 2002;6:175, doi: 10.1186/cc1478.
9. Vieillard-Baron A, Slama M, Cholley B, Janvier G, Vignon P. Echocardiography in the intensive care unit: from evolution to revolution? Intens Care Med. 2008;34:243-9, doi: 10.1007/s00134-007 0923-5.
10. Caille V, Arniel JB, Charron C, Belliard G, Vieillard-Baron A, Vignon P. Echocardiography: a help in the weaning process. Crit Care. 2010;14:R120, doi: 10.1186/cc9076.
11. Aurigemma GP, Gaash WN. Quantitative evaluation of left ventricular structure, wall stress and systolic function. In: Otto CM, editor. The Practice of Clinical Echocardiography. Philadelphia: WB Saunders; 2002.
12. Tobin MJ. Advances in mechanical ventilation. N Engl J Med. 2001;344:1986-96, doi: 10.1056/NEJM200106283442606.
14. MacIntyre NR, Cook DJ, Ely EW Jr, Epstein SK, Fink JB, Heffner JE, et al. American College of Chest Physicians; American Association for Respiratory Care; American College of Critical Care Medicine: Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest. 2001;120(6 Suppl):S375-95, doi: 10.1378/chest.120.6_suppl.375S.
15. Meade M, Guyatt G, Cook D, Griffith L, Sinuff T, Kergl C, et al. Predicting success in weaning from mechanical ventilation. Chest. 2001;120(6 Suppl):S400-24, doi: 10.1378/chest.120.6_suppl.400S.
16. Vallverdú I, Calaf N, Subirana M, Net A, Benito S, Mancebo J. Clinical characteristics, respiratory functional parameters, and outcome of a two-hour T-piece trial in patients weaning from mechanical ventilation. Am J Respir Crit Care Med. 1998;158:1855-62.
17. Pinsky MR. Breathing as exercise: the cardiovascular response to weaning from mechanical ventilation. Intens Care Med. 2000;26:1164-6, doi: 10.1007/s001340000619.
18. Cabello B, Thille AW, Roche-Campo F, Brochard L, Gómez FJ, Mancebo J. Physiological comparison of three spontaneous breathing trials in difficult-to-wean patients. Intens Care Med. 2010;36:1171-9, doi: 10.1007/s00134-010-1870-0.
19. Moller JE, Hillis GS, Oh JK, Seward JB, Reeder GS, Wright RS, et al. Left atrial volume: a powerful predictor of survival after acute myocardial infarction. Circulation. 2003;107:2207-12, doi: 10.1161/01.CIR.0000066318.21784.43.
20. Abhayaratna WP, Seward JB, Appleton CP, Douglas PS, Oh JK, Tajik AJ, et al. Left atrial size: physiologic determinants and clinical applications. J Am Coll Cardiol. 2006;47:2357-63, doi: 10.1016/j.jacc.2006.02.048.
21. Oh JK, Appleton CP, Hatle LK, Nishimura RA, Seward JB, Tajik AJ. The noninvasive assessment of left ventricular diastolic function with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 1997;10:246-70, doi: 10.1016/S0894-7317(97)70062-2.
22. Marcelino P, Fernandes AP, Marum S, Ribeiro JP. The influence of cardiac diastole on weaning from mechanical ventilation. Rev Port Cardiol. 2002;21:849-57.
23. Gonzalez-Vilchez F, Ares M, Ayuela J, Alonso L. Combined use of pulsed and color M-mode Doppler echocardiography for the estimation of pulmonary capillary wedge pressure: an empirical approach based on an analytical relation. J Am Coll Cardiol. 1999;34:515-23, doi: 10.1016/ S0735-1097(99)00230-2.
24. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quiñones MA. Doppler tissue imaging: a noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol. 1997;30:1527-33, doi: 10.1016/S0735-1097(97)00344-6.
25. Frazier SK, Brom H, Widener J, Pender L, Stone KS, Moser DK. Prevalence of myocardial ischemia during mechanical ventilation and weaning and its effects on weaning success. Heart Lung. 2006;35:363-73, doi: 10.1016/j.hrtlng.2005.12.006.
26. Demoule A, Lefort Y, Lopes ME, Lemaire F. Successful weaning from mechanical ventilation after coronary angioplasty. Br J Anaesth. 2004;93:295-7, doi: 10.1093/bja/aeh185.
27. Pinsky MR. Cardiovascular issues in respiratory care. Chest. 2005;128(5 Suppl 2):S592-7, doi: 10.1378/chest.128.5_suppl_2.592S.
28. Richard C, Teboul JL. Weaning failure from cardiovascular origin. Intens Care Med. 2005;31:1605-7, doi: 10.1007/s00134-005-2698-x.
29. Monnet X, Teboul JL, Richard C. Cardiopulmonary interactions in patients with heart failure. Curr Opin Crit Care. 2007;13:6-11, doi: 10.1097/MCC.0b013e328013c865.
30. Costa AD, Rieder Mde M, Vieira SR. Weaning from mechanical ventilation by using pressure support or T-tube ventilation. Comparison between patients with and without heart disease. Arq Bras Cardiol. 2005;85:32-8, doi: 10.1590/S0066-782X2005001400007.
Received for publication on October 14, 2010; First review completed on October 14, 2010; Accepted for publication on October 19, 2010
- 1. Hess D. Ventilator modes used in weaning. Chest. 2001;120(6 Suppl):S474-6, doi: 10.1378/chest.120.6_suppl.474S.
- 2. Chatila W, Ani S, Guaglianone D, Jacob B, Amoateng-Adjepong Y, Manthous CA. Cardiac ischemia during weaning from mechanical ventilation. Chest. 1996;109:1577-83, doi: 10.1378/chest.109.6.1577.
- 3. Lessard MR, Brochard LJ. Weaning from ventilatory support. Clin Chest Med. 1996;17:475-89, doi: 10.1016/S0272-5231(05)70328-2.
- 4. Srivastava S, Chatila W, Amoateng-Adjepong Y, Kanagasegar S, Jacob B, Zarich S, et al. Myocardial ischemia and weaning failure in patients with coronary artery disease: an update. Crit Care Med. 1999;27:2109-12, doi: 10.1097/00003246-199910000-00005.
- 5. Lemaire F, Teboul JL, Cinotti L, Giotto G, Abrouk F, Steg G, et al. Acute left ventricular dysfunction during unsuccessful weaning from mechanical ventilation. Anesthesiology. 1988;69:171-9, doi: 10.1097/00000542198808000-00004.
- 6. Loubieres Y, Vieillard-Baron A, Beauchet A, Fourme T, Page B, Jardin F. Echocardiographic evaluation of left ventricular function in critically ill patients: dynamic loading challenge using medical antishock trousers. Chest. 2000;118:1718-23, doi: 10.1378/chest.118.6.1718.
- 7. Dittoe N, Stultz D, Schwartz BP, Hahn HS. Quantitative left ventricular systolic function: from chamber to myocardium. Crit Care Med. 2007;35(8 Suppl):S330-9, doi: 10.1097/01.CCM.0000270245.70103.7E.
- 8. Ribeiro J, Marcelino P, Marum S, Fernandes A. Echocardiography: a fundamental part of the intensive care curriculum. Crit Care. 2002;6:175, doi: 10.1186/cc1478.
- 9. Vieillard-Baron A, Slama M, Cholley B, Janvier G, Vignon P. Echocardiography in the intensive care unit: from evolution to revolution? Intens Care Med. 2008;34:243-9, doi: 10.1007/s00134-007 0923-5.
- 10. Caille V, Arniel JB, Charron C, Belliard G, Vieillard-Baron A, Vignon P. Echocardiography: a help in the weaning process. Crit Care. 2010;14:R120, doi: 10.1186/cc9076.
- 11. Aurigemma GP, Gaash WN. Quantitative evaluation of left ventricular structure, wall stress and systolic function. In: Otto CM, editor. The Practice of Clinical Echocardiography. Philadelphia: WB Saunders; 2002.
- 12. Tobin MJ. Advances in mechanical ventilation. N Engl J Med. 2001;344:1986-96, doi: 10.1056/NEJM200106283442606.
- 13. Yang KL, Tobin MJ. A prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilation. N Engl J Med. 1991;324:1445-50, doi: 10.1056/NEJM199105233242101.
- 14. MacIntyre NR, Cook DJ, Ely EW Jr, Epstein SK, Fink JB, Heffner JE, et al. American College of Chest Physicians; American Association for Respiratory Care; American College of Critical Care Medicine: Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest. 2001;120(6 Suppl):S375-95, doi: 10.1378/chest.120.6_suppl.375S.
- 15. Meade M, Guyatt G, Cook D, Griffith L, Sinuff T, Kergl C, et al. Predicting success in weaning from mechanical ventilation. Chest. 2001;120(6 Suppl):S400-24, doi: 10.1378/chest.120.6_suppl.400S.
- 16. Vallverdú I, Calaf N, Subirana M, Net A, Benito S, Mancebo J. Clinical characteristics, respiratory functional parameters, and outcome of a two-hour T-piece trial in patients weaning from mechanical ventilation. Am J Respir Crit Care Med. 1998;158:1855-62.
- 17. Pinsky MR. Breathing as exercise: the cardiovascular response to weaning from mechanical ventilation. Intens Care Med. 2000;26:1164-6, doi: 10.1007/s001340000619.
- 18. Cabello B, Thille AW, Roche-Campo F, Brochard L, Gómez FJ, Mancebo J. Physiological comparison of three spontaneous breathing trials in difficult-to-wean patients. Intens Care Med. 2010;36:1171-9, doi: 10.1007/s00134-010-1870-0.
- 19. Moller JE, Hillis GS, Oh JK, Seward JB, Reeder GS, Wright RS, et al. Left atrial volume: a powerful predictor of survival after acute myocardial infarction. Circulation. 2003;107:2207-12, doi: 10.1161/01.CIR.0000066318.21784.43.
- 20. Abhayaratna WP, Seward JB, Appleton CP, Douglas PS, Oh JK, Tajik AJ, et al. Left atrial size: physiologic determinants and clinical applications. J Am Coll Cardiol. 2006;47:2357-63, doi: 10.1016/j.jacc.2006.02.048.
- 21. Oh JK, Appleton CP, Hatle LK, Nishimura RA, Seward JB, Tajik AJ. The noninvasive assessment of left ventricular diastolic function with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 1997;10:246-70, doi: 10.1016/S0894-7317(97)70062-2.
- 22. Marcelino P, Fernandes AP, Marum S, Ribeiro JP. The influence of cardiac diastole on weaning from mechanical ventilation. Rev Port Cardiol. 2002;21:849-57.
- 23. Gonzalez-Vilchez F, Ares M, Ayuela J, Alonso L. Combined use of pulsed and color M-mode Doppler echocardiography for the estimation of pulmonary capillary wedge pressure: an empirical approach based on an analytical relation. J Am Coll Cardiol. 1999;34:515-23, doi: 10.1016/ S0735-1097(99)00230-2.
- 24. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quiñones MA. Doppler tissue imaging: a noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol. 1997;30:1527-33, doi: 10.1016/S0735-1097(97)00344-6.
- 25. Frazier SK, Brom H, Widener J, Pender L, Stone KS, Moser DK. Prevalence of myocardial ischemia during mechanical ventilation and weaning and its effects on weaning success. Heart Lung. 2006;35:363-73, doi: 10.1016/j.hrtlng.2005.12.006.
- 26. Demoule A, Lefort Y, Lopes ME, Lemaire F. Successful weaning from mechanical ventilation after coronary angioplasty. Br J Anaesth. 2004;93:295-7, doi: 10.1093/bja/aeh185.
- 27. Pinsky MR. Cardiovascular issues in respiratory care. Chest. 2005;128(5 Suppl 2):S592-7, doi: 10.1378/chest.128.5_suppl_2.592S.
- 28. Richard C, Teboul JL. Weaning failure from cardiovascular origin. Intens Care Med. 2005;31:1605-7, doi: 10.1007/s00134-005-2698-x.
- 29. Monnet X, Teboul JL, Richard C. Cardiopulmonary interactions in patients with heart failure. Curr Opin Crit Care. 2007;13:6-11, doi: 10.1097/MCC.0b013e328013c865.
- 30. Costa AD, Rieder Mde M, Vieira SR. Weaning from mechanical ventilation by using pressure support or T-tube ventilation. Comparison between patients with and without heart disease. Arq Bras Cardiol. 2005;85:32-8, doi: 10.1590/S0066-782X2005001400007.
Publication Dates
-
Publication in this collection
14 Mar 2011 -
Date of issue
2011
History
-
Received
14 Oct 2010 -
Reviewed
14 Oct 2010 -
Accepted
19 Oct 2010