
Abstracts
Natalizumab is currently one of the best options for treatment of patients with Multiple Sclerosis who have failed traditional prior therapies. However, prolonged use, prior immunosuppressive therapy and anti-JCV antibody status have been associated with increased risk of developing progressive multifocal leukoencephalopathy (PML). The evaluation of these conditions has been used to estimate risks of PML in these patients, and distinct (sometimes extreme) approaches are used to avoid the PML onset. At this time, the biggest issue facing the use of Natalizumab is how to get a balance between the risks and the benefits of the treatment. Hence, strategies for monitor JCV-positive patients undergoing Natalizumab treatment are deeply necessary. To illustrate it, we monitored JCV/DNA in blood and urine of a patient receiving Natalizumab for 12 months. We also bring to discussion the effectiveness of the current methods used for risk evaluation, and the real implications of viral reactivation.
multiple sclerosis; Natalizumab; JCV; risk factors; progressive multifocal leucoencephalopaty; viruria
Natalizumabe é atualmente uma das melhores opções para o tratamento de pacientes com Esclerose Múltipla que não respondem aos tratamentos tradicionais. No entanto, o seu uso prolongado, o uso de terapia imunossupressora prévia e o status sorológico antivírus JC têm sido associados com o risco aumentado de desenvolvimento de Leucoencefalopatia Multifocal Progressiva (LEMP). A avaliação destas condições tem sido utilizada para estimar os riscos do desenvolvimento de LEMP nestes pacientes, e abordagens distintas (por vezes extremas) são empregadas para evitar o aparecimento dessa patologia. Atualmente, o grande desafio está em obter um equilíbrio entre os riscos e os benefícios do tratamento com Natalizumabe. Assim, é crucial desenvolver estratégias para monitorar pacientes portadores do vírus JC sob tratamento com Natalizumabe. A título de ilustração, pesquisamos o vírus no sangue e na urina de um paciente sob tratamento durante 12 meses. Também discutimos a eficácia dos métodos atualmente utilizados para avaliação de riscos e as implicações reais de reativação viral.
esclerose múltipla; Natalizumabe; vírus JC; leucoencefalopatia multifocal progressiva; viruria
Natalizumab (Tysabri), used for treatment of relapsing-remitting multiple sclerosis (MS),
is a monoclonal antibody directed to the a4β1 integrin, a subunit of an adhesion
molecule expressed on the surface of T lymphocytes. The antibodies act by blocking the
migration of T Lymphocytes from blood to the CNS through the blood brain barrier (BBB)
and attenuate the inflammatory effects11 Yednock TA, Cannon C, Fritz LC, Sanchez-Madrid F, Strinman L, Karin
N. Prevention of experimental autoimmune encephalomyelitis by antibodies against
alpha 4 beta 1 integrin. Nature. 1992;356(6364):63-6.
http://dx.doi.org/10.1038/356063a0
https://doi.org/10.1038/356063a0...
. The AFFIRM study showed that monotherapy with Natalizumab (NTZ)
for 2 years decreased the relapse rate by 68% and the disability progression rate by 42%
compared with placebo22 Polman CH, O'Connor PW, Havrodova E, Hutschinson M, Kappos L,
Miller DH et al. A randomized, placebo-controlled trial of natalizumab for
relapsing multiple sclerosis. N Engl J Med. 2006;354(9):899-910.
http://dx.doi.org/10.1056/NEJMoa044397
https://doi.org/10.1056/NEJMoa044397...
. NTZ is well
tolerated and the overall incidence of serious adverse events is low. Although the
efficacy of NTZ is up to 3 times higher over disease-modifying drugs (DMDs), in 2005 it
was announced the withdrawal of NTZ from the market since 2 patients with MS and 1
patient with Crohn disease were diagnosed with Progressive Multifocal
Leukoencephalopathy (PML). In 2006, NTZ was reintroduced into the market and approved as
monotherapy for the treatment of relapsing forms of MS. However, even with a careful
administration protocol, PML cases in MS patients have been growing, with more than 400
cases reported so far
(http://multiple-sclerosis-research.blogspot.com.br/2013/10/natalizumab-pml-update-september-2013.html).
A SHORT BACKGROUND OF PML
Progressive multifocal leukoencephalopathy is a demyelinating disease of the central
nervous system that usually leads to death or severe disability. PML is
characterized by destruction of myelin-producing oligodendrocytes and astrocytes and
has almost exclusively been reported in immunocompromised patients. Particularly, it
manifests in individuals with reduced cellular immunity, including patients with
HIV, hematological diseases, or receiving immunosuppressive therapies. Since the
late 1980s until 2008 PML was responsible to be the cause of death of 4-5% of
HIV-infected patients33 Greenlee JE. Progressive multifocal encephalopathy. Handb Clin
Neurol. 1998;123:399-430.
http://dx.doi.org/10.1016/b978-0-444-53488-0.00017-1
https://doi.org/10.1016/b978-0-444-53488...
,44 Vidal JE, Oliveira ACP, Fink MC, Pannuti CS, Trujillo JR.
Aids-related progressive multifocal leukoencephalopathy: a retrospective study
in a referral center in Sao Paulo, Brazil. Rev Inst Med Trop São Paulo.
2008;50(4):209-12.
http://dx.doi.org/10.1590/s0036-46652008000400004
https://doi.org/10.1590/s0036-4665200800...
.
JC virus is the PML etiological agent. It is a non-enveloped double-stranded circular DNA virus of 5,130 base pairs. The viral genome codes for six genes: Large and small T antigen, capsid genes VP1, VP2 and VP3, agnoprotein and the regulatory region (RR), which can be classified as the archetype or rearranged according to their structural features55 Imperiale MJ. Polyomaviruses. In: Knipe DV, Howley PM, editors. Field's virology. New York: Lippincott Williams & Wilkins; 2007. p. 2263-98..
The genetic structure of RR directly affects viral transcription and replication by
change the level of DNA/protein and cofactors binding sites, thus leading to
distinct cellular tropism66 Ravichandran V, Major EO. Viral proteomics: a promising approach for
understanding JC virus tropism. Proteomics. 2006;6(20):5628-36.
http://dx.doi.org/10.1002/pmic.200600261
https://doi.org/10.1002/pmic.200600261...
. The
urinary shedding of JCV with archetype structure is frequent among healthy and
immunocompromised individuals77 Behzad-Behbahani A, Klapper PE, Vallely PJ, Cleator CM, Khoo SH.
Detection of BK virus and JC virus DNA in urine samples from immunocompromised
(HIV-infected) and immunocompetent (HIV-non-infected) patients using polymerase
chain reaction and microplate hybridisation. J Clin Virol. 2004;29(4):224-9.
10.1016/S1386-6532(03)00155-0
https://doi.org/10.1016/S1386-6532(03)00...
,88 Rossi A, Delbue S, Mazziotti R, Vlli M, Borghi E, Mancuso R et al.
Presence, quantitation and characterization of JC virus in the urine of Italian
immunocompetent subjects. J Med Virol. 2007;79(4):408-12.
http://dx.doi.org/10.1002/jmv.20829
https://doi.org/10.1002/jmv.20829...
,99 Nali LHS, Centrone CC, Urbano PRP, Penalva-de-Oliveira AC, Vidal JE,
Miranda EP et al. High prevalence of the simultaneous excretion of
polyomaviruses JC and BK in the urine of HIV-infected patients without
neurological symptoms in Sao Paulo, Brazil. Rev Inst Med Trop São Paulo.
2012;54(4):201-5.
http://dx.doi.org/10.1590/S0036-46652012000400004
https://doi.org/10.1590/S0036-4665201200...
,1010 Yogo Y, Kitamura T, Sujimoto C, Ueki T, Aso Y, Hara K et al.
Isolation of a possible archetypal JC virus DNA sequence from
nonimmunocompromised individuals. J Virol. 1990;64(6):3139-43., but rearranged forms with deletions, insertions and
duplications are usually found in viruses from blood and brain of patients with
PML1111 Pfister LA, Letvin NL, Koralnik IJ. JC virus regulatory region
tandem repeats in plasma and central nervous system isolates correlate with poor
clinical outcome in patients with progressive multifocal leukoencephalopathy. J
Virol. 2001;75(12):5672-6.
http://dx.doi.org/10.1128/jvi.75.12.5672-5676.2001
https://doi.org/10.1128/jvi.75.12.5672-5...
,1212 Yogo Y, Matsushina-Ohno T, Hayashi T, Sujimoto S, Sakurai M,
Kanazawa I. JC virus regulatory region rearrangements in the brain of a long
surviving patient with progressive multifocal leukoencephalopathy. J Neurol
Neurosurg Psychiatry. 2001;71(3):397-400.
http://dx.doi.org/10.1136/jnnp.71.3.397
https://doi.org/10.1136/jnnp.71.3.397...
. Much less frequently, the
rearranged form of JCV can be found in the urine of patients experiencing
asymptomatic reactivation1313 Chen Y, Bord E, Tompkins T, Miller J, Tan CS, Kinkel RP et al.
Asymptomatic reactivation of JC virus in patients treated with natalizumab. N
Engl J Med. 2009;361(11):1067-74.
http://dx.doi.org/10.1056/NEJMoa0904267
https://doi.org/10.1056/NEJMoa0904267...
. In
addition to RR, variability in VP1 sequences found in CSF and brain of PML patients,
but not in urine, also reinforces the relationship between the variants or genetic
changes and viral tropism1414 Marshall LJ, Major EO. Molecular regulation of JC virus tropism:
insights into potential therapeutic targets for progressive multifocal
leukoencephalopathy. J Neuroimmune Pharmacol. 2010;5(3):404-17.
http://dx.doi.org/10.1007/s11481-010-9203-1
https://doi.org/10.1007/s11481-010-9203-...
,1515 Reid CE, Li H, Sur G, Carmillo P, Bushnell S, Tizard R al.
Sequencing and analysis of JC virus DNA from natalizumab-treated PML patients. J
Infect Dis. 2011;204(2):237-44.
http://dx.doi.org/10.1093/infdis/jir256
https://doi.org/10.1093/infdis/jir256...
.
Currently, the most accepted idea is that PML arises as a consequence of reactivation
of latent JCV in the kidneys, leading to viremia and as a consequence, viruses
present in blood and/or B-lymphocytes enter the brain and cause disease. However,
viral reactivation in kidneys or blood preceding its migration to the brain is
controversial since different groups have found viruses in brain of healthy
individuals1616 White III FA, Ishaq M, Stoner GL, Frisque RJ. JC virus DNA is
present in many human brain samples from patients without progressive multifocal
leukoencephalopathy. J Virol. 1992;66(10):5726-34.,1717 Elsner C, Dörries K. Evidence of human polyomavirus BK and JC
infection in normal brain tissue. Virology. 1992;191(1):72-80.
http://dx.doi.org/10.1016/0042-6822(92)90167-n
https://doi.org/10.1016/0042-6822(92)901...
as well as no viremia at all in
some affected patients. It was also found latent JCV in lymph, spleen, bone marrow
and tonsil demonstrating that the virus may establishes latency in many tissues1818 Monaco MC, Jensen PN, Hou J, Durham LC, Major EO. Detection of JC
virus DNA in human tonsil tissue: evidence for site of initial viral infection.
J Virol. 1998;72(12):9918-23.,1919 Tan CS, Ellis LC, Wüthrich C, Ngo L, Broge TA, Saint-Aubyn J et
al. JC virus latency in the brain and extraneural organs of patients with and
without progressive multifocal leukoencephalopathy. J Virol. 2010;84(18):9200-9.
http://dx.doi.org/10.1128/jvi.00609-10
https://doi.org/10.1128/jvi.00609-10...
.
NATALIZUMAB AND PML
PML in patients receiving Natalizumab was first reported in 2005 in three individuals
during clinical studies. By the middle of 2011, all reported cases of PML in people
receiving NTZ arose in patients who were under treatment for more than 1 year. In
the same year, based on post-marketing reports, the overall risk of PML was
estimated around 1.51 per 1,000 patients (95%CI 1.27-1.79). More detailed historic
investigation of these patients revealed that particular conditions could work as
risk factors for PML development. For example, patients who developed PML were more
likely to have been treated with immunosuppressant before receiving Natalizumab and
the incidence of PML over time tended to be lower in the first 12 months of
treatment but increased through time. Therefore, risk management strategies have
been developed based on increased risk in patients with (i) anti-JCV antibodies,
(ii) longer duration of Natalizumab treatment and (iii) prior immunosuppressive
therapy2020 Sorensen PS, Bertolotto A, Edan G, Giovannnoni G, Gold R, Havrdova E
et al. Risk stratification for progressive multifocal leukoencephalopathy in
patients treated with natalizumab. Mult Scler. 2012;18(2):143-52.
http://dx.doi.org/10.1177/1352458511435105
https://doi.org/10.1177/1352458511435105...
(Figure 1). The risk of PML among patients with
none of these conditions is very low and almost unchangeable through the treatment
since the annual seroconversion rate is low.
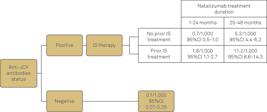
Risk for PML in MS patients under NTZ therapy. The risk is based on the time of treatment with NTZ, anti-JCV antibodies status and previous Immunosuppressive therapy. IS=Immunosuppressive (adapted from http://multiple-sclerosis-research.blogspot.com.br/)
Although the outcomes of natalizumab-treated patients with PML are generally better than those reported in HIV infected individuals, the clinical vigilance, early PML diagnosis, and cessation of Natalizumab treatment on suspicion of PML has been used to avoid the onset of the disease.
JCV is ubiquitous in human population and can be as prevalent as 80% according to
some studies2121 Antonsson A, Green AC, Mallitt KA, O'Rourke PK, Pawlita M,
Waterboer T et al. Prevalence and stability of antibodies to the BK and JC
polyomaviruses: a long-term longitudinal study of Australians. J Gen Virol.
2010;91(7):1849-53. http://dx.doi.org/10.1099/vir.0.020115-0
https://doi.org/10.1099/vir.0.020115-0...
,2222 Egli A, Infanti L, Dumoulin A, Buser A, Samaridis J, Stebler C et
al. Prevalence of polyomavirus BK and JC infection and replication in 400
healthy blood donors. J Infect Dis. 2009;199(6):837-46.
http://dx.doi.org/10.1086/597126
https://doi.org/10.1086/597126...
,2323 Bozic C, Richman S, Plavina T, Natarajan A, Scanlon JV, Subramanyam
M et al. Anti-John Cunnigham virus antibody prevalence in multiple sclerosis
patients: baseline results of STRATIFY-1. Ann Neurol. 2011;70(5):742-50.
http://dx.doi.org/10.1002/ana.22606
https://doi.org/10.1002/ana.22606...
,2424 Kean JM, Rao S, Wang M, Garcea RL. Seroepidemiology of human
polyomaviruses. PLoS Pathog. 2009;5(3):e1000363.
http://dx.doi.org/10.1371/journal.ppat.1000363
https://doi.org/10.1371/journal.ppat.100...
,2525 Trampe AK, Hemmelmann C, Stroet A, Haghikia A, Hellwig K, Wiendl H
et al. Anti-JC virus antibodies in a large German natalizumab-treated multiple
sclerosis cohort. Neurology. 2012;78(22):1736-42.
http://dx.doi.org/10.1212/WNL.0b013e3182583022
https://doi.org/10.1212/WNL.0b013e318258...
. It is important to remind that JCV establishes
latency in urinary tract and may be excreted during life without any consequence. In
other words, JCV antibody detection does not provide all the necessary information
regarding viral replication in MS patients undergoing NTZ treatment.
Given the risk to PML development increases according to the treatment extent2626 Fernandez O. Best practice in the use of natalizumab in multiple
sclerosis. Ther Adv Neurol Disord. 2013;6(2):69-79.
http://dx.doi.org/10.1177/1756285612470401
https://doi.org/10.1177/1756285612470401...
, some MS centers employ few
months suspension of Natalizumab after one year of treatment (drug holiday) in order
to restore the immune surveillance in JCV-positive patients. However, this approach
remarkably increases the risk of rebound of MS activity2727 Killestein J, Vennegoor A, Strijbis EM. Natalizumab drug holiday in
multiple sclerosis: poorly tolerated. Ann Neurol. 2010;68(3):392-5.
http://dx.doi.org/10.1002/ana.22074
https://doi.org/10.1002/ana.22074...
and is not sufficient to extinguish the risk of
developing the disease2828 Gheuens S, Smith DR, Wang X, Alsop DC, Lenkinski RE, Koralnik IJ.
Simultaneous PML-IRIS after discontinuation of natalizumab in a patient with MS.
Neurology. 2012;78(18):1390-3.
http://dx.doi.org/10.1212/WNL.0b013e318253d61e
https://doi.org/10.1212/WNL.0b013e318253...
. It is
now evident that PML is a complex and not fully understood disease, in which viral
and host factors might play a role in disease onset.
For this reason, the development of clinical and laboratory markers that assure the treatment safety for extended time in JC serologically positive individuals are pivotal.
To illustrate it, we describe the JCV replication dynamics in the urine and blood of a JCV positive MS patient receiving NTZ over 12 months and the detailed molecular investigation of the complete VP1 gene and RR.
THE FOLLOW UP
Urine and blood samples from a 38 year-old female patient, with MS first diagnosed as
relapsing-remitting form in 1990 and receiving NTZ were monthly monitored through
Real Time PCR for one year for the presence and viral load of JCV2929 Pal A, Sirota L, Maudru T, Peden K, Lewis AM. Real-time,
quantitative PCR assays for the detection of virus-specific DNA in samples with
mixed populations of polyomaviruses. J Virol Methods. 2006;135(1):32-42.
http://dx.doi.org/10.1016/j.jviromet.2006.01.018
https://doi.org/10.1016/j.jviromet.2006....
. From all positive samples, we
sequenced the VP1 and RR (see Table for primers used in both reactions).
The patient was previously treated with Glatiramer acetate and interferon β-1A. She responded well to the NTZ and no relapses were reported during the follow-up. The average expanded disability status scale (EDSS) score was evaluated before NTZ introduction (EDSS=6) and remained stable throughout the treatment.
JCV DNA was not detected in blood samples in any time-point evaluated. However, all
the urine samples were positive, including the one collected before NTZ
introduction. The viral load, which was about 770,000 copies/ml at the first
sampling, experienced a slightly decrease in the first three months of treatment but
significantly increased after the fourth month, reaching to 1.1099 Nali LHS, Centrone CC, Urbano PRP, Penalva-de-Oliveira AC, Vidal JE,
Miranda EP et al. High prevalence of the simultaneous excretion of
polyomaviruses JC and BK in the urine of HIV-infected patients without
neurological symptoms in Sao Paulo, Brazil. Rev Inst Med Trop São Paulo.
2012;54(4):201-5.
http://dx.doi.org/10.1590/S0036-46652012000400004
https://doi.org/10.1590/S0036-4665201200...
copies/ml during the
8th, 9th and 10th months of treatment (Figure 2). This observation is in keeping with
the Laroni et al., that found that viruria could occur before the Natalizumab
introduction, but gradually increase during the treatment3030 Laroni A, Giacomazzi CG, Grimaldi L, Gallo P, Sormani MP, Bertolotto
A et al. Urinary JCV-DNA testing during natalizumab treatment may increase
accuracy of PML risk stratification. J Neuroimmune Pharmacol. 2012;7(3):665-72.
http://dx.doi.org/10.1007/s11481-012-9366-z
https://doi.org/10.1007/s11481-012-9366-...
.

Viral load/ml in urine samples. The graph shows the number of JC viruses/ml detected through Real Time PCR in urine at each time-point. Time 0 corresponds to the sample collected immediately before the first Natalizumab infusion.
The JCV/VP1 gene and RR were successfully sequenced from viruses sampled at all time-points (the RR from the last three months was also cloned to deep investigate putative mutants present as minor population) and no nucleotide change was detected in the consensus sequences during the follow-up. Nevertheless, a careful inspection of the electropherograms revealed the emergence of a non-synonymous change at nucleotide 86 of the VP1 gene, at the very end of the N’ terminal region (aminoacid site 29) in viruses from the sixth, seventh, eighth and ninth months of treatment (Figure 3). This change (Adenine to Guanine) would lead to the substitution of a glutamate to glycine (E29G). However, these mutants never reached to the majority population, and were no longer observed in the following months. This mutation was not related to any change already described as associated to PML.

Electropherograms of VP1 sequences. Selected regions evidence the mixture detected in VP1 sequences. Adenine is present in the original and predominant population and Guanine emerged as variants. Variants were detected at the 6th to 9th months of the treatment.
Intra-host JCV variability, especially in the RR region is almost a consensus for PML
patients, but the origin of the mutants has been subject of investigation. Some
argue that the high rate of viral replication in urine or blood of an infected
patient allows the emergence of mutant viruses with different tropism3131 Gosert R, Kardas P, Major EO, Hirsch HH. Rearranged JC virus
noncoding control regions found in progressive multifocal leukoencephalopathy
patient samples increase virus early gene expression and replication rate. J
Virol. 2010;84(20):1048-56.
http://dx.doi.org/10.1128/jvi.00614-10
https://doi.org/10.1128/jvi.00614-10...
,3232 Raj GV, Khalili K. Transcriptional regulation: lessons from the
human neurotropic polyomavirus, JCV. Virology. 1995;213(2):283-91.
http://dx.doi.org/10.1006/viro.1995.0001
https://doi.org/10.1006/viro.1995.0001...
. In contrast, it has also been suggested that
variants with different tropism circulates among the population, and the infection
by a more or less pathogenic strain happens by chance2929 Pal A, Sirota L, Maudru T, Peden K, Lewis AM. Real-time,
quantitative PCR assays for the detection of virus-specific DNA in samples with
mixed populations of polyomaviruses. J Virol Methods. 2006;135(1):32-42.
http://dx.doi.org/10.1016/j.jviromet.2006.01.018
https://doi.org/10.1016/j.jviromet.2006....
. There is also the possibility that JCV establish
latency in other tissues besides the urinary tract, as indicated by findings of JCV
in brain of healthy individuals1616 White III FA, Ishaq M, Stoner GL, Frisque RJ. JC virus DNA is
present in many human brain samples from patients without progressive multifocal
leukoencephalopathy. J Virol. 1992;66(10):5726-34.,1717 Elsner C, Dörries K. Evidence of human polyomavirus BK and JC
infection in normal brain tissue. Virology. 1992;191(1):72-80.
http://dx.doi.org/10.1016/0042-6822(92)90167-n
https://doi.org/10.1016/0042-6822(92)901...
,1818 Monaco MC, Jensen PN, Hou J, Durham LC, Major EO. Detection of JC
virus DNA in human tonsil tissue: evidence for site of initial viral infection.
J Virol. 1998;72(12):9918-23.. It is in accordance to the usual presence of archetype
virus in urine but rearranged forms in blood and brain of PML individuals.
Here we showed that despite no JCV rearranged forms came out in the urine and no
viremia occurred after 12 months of treatment, VP1 mutant viruses emerged in the
urine concomitant to the increase of the viral load (see Figures 2 and 3). The
emergence of variants during extensive viral replication is not surprising for
viruses that experience high evolutionary rates3333 Shankarappa R, Margolick JB, Gange SJ, Rodrigo AG, Upchurch D,
Farzadegan H et al. Consistent viral evolutionary changes associated with the
progression of human immunodeficiency virus type 1 infection. J Virol.
1999;73:10489-1502.,3434 Rambaut A, Posada D, Crandall KA, Holmes EC. The causes and
consequences of HIV evolution. Nat Rev Genet. 2004;5(1):52-61.
http://dx.doi.org/10.1038/nrg1246
https://doi.org/10.1038/nrg1246...
,3535 Ueda E, Enomoto N, Sakamoto N, Hamano K, Sato C, Izumi N et al.
Changes of HCV quasispecies during combination therapy with interferon and
ribavirin. Hepatol Res. 2004;29(2):89-96.
http://dx.doi.org/10.1016/j.hepres.2004.02.014
https://doi.org/10.1016/j.hepres.2004.02...
. Nevertheless, JCV, similarly to other DNA viruses, is
genetically stable through time since its substitution rate ranges between
10-7 to 10-8 s/s/y3636 Hatwell JN, Sharp PM. Evolution of human polyomavirus JC. J Gen
Virol. 2000;81(5):1191-200.. Thus, it is less likely (although not impossible)
that JCV variant, observed in this study, results from a within-patient mutation
emergence.
We then envisage a scenario where the patient analyzed was infected during its lifetime by distinct variants, and the virus predominantly detected during the whole study was probably the one with the best fitness (variant A). Through the follow-up, the variant that emerged at the sixth month (variant B) was reactivated, possibly as a consequence of the Natalizumab treatment or any other unknown cause.
In situations where high-load persistent viral infection is already established and
viral replication is constant, functional impairments or low frequencies of
virus-specific T cells is not uncommon3737 Fuse S, Molloy MJ, Usherwood EJ. Immune responses against persistent
viral infections: possible avenues for immunotherapeutic interventions. Crit Rev
Immunol. 2008;28(2):159-83.
http://dx.doi.org/10.1615/critrevimmunol.v28.i2.40
https://doi.org/10.1615/critrevimmunol.v...
. Therefore, it is possible that the emergence of the
variant B concomitant to the already established variant A caused both, increased
viral load, and stimulated the cellular immune response. As a consequence, the
variant B was controlled, the viral load decreased and only the original (and
possibly less immunogenic) viruses remained detectable.
Furthermore, it is also possible that the inefficient viral control is consequence of
the effects of NTZ in the immune system. NTZ was showed to disturb the balance
between cytokines, up regulating some pro inflammatory cytokines3838 Benkert TF, Dietz L, Hartmann EM, Leich E, Rosenwald A, Serfling E
et al. Natalizumab exerts direct signaling capacity and supports a
pro-inflammatory phenotype in some patients with multiple sclerosis. PLoS ONE.
2012;7(12):e52208.
http://dx.doi.org/10.1371/journal.pone.0052208
https://doi.org/10.1371/journal.pone.005...
and decreasing the expression of
the co-stimulatory molecule CD134 on CD4(+)CD26(HIGH) T-cells3939 Bornsen L, Christensen JR, Ratzer R, Oturai AB, Sørensen PS,
Søndergaard HB et al. Effect of natalizumab on circulating CD4+ T-cells in
multiple sclerosis. PLoS ONE 2012;7(11):e47578.
http://dx.doi.org/10.1371/journal.pone.0047578
https://doi.org/10.1371/journal.pone.004...
. Also, Perkins and coworkers reported that
patients receiving Natalizumab who developed PML do not present JCV-specific T cell
response or had JCV-specific CD4 T cell responses uniquely dominated by IL-10
production4040 Perkins MR, Ryschkewitsch C, Liebner JC, Monaco MCG, Himelfarb D,
Ireland S et al. Changes in JC virus-specific T cell responses during
natalizumab treatment and in natalizumab-associated progressive multifocal
leukoencephalopathy. PLoS Pathog. 2012;8(11):e1003014.
http://dx.doi.org/10.1371/journal.ppat.1003014
https://doi.org/10.1371/journal.ppat.100...
. Unfortunately,
no immunological test was performed in the present study to confirm if this would be
the case here. Altogether, the above-discussed data reinforce that PML in NTZ
patients is a combination of altered cellular and cytokine expression and viral
factors.
In summary, the availability of NTZ represents a real gain in terms of better quality
of life for MS patients, but it also resulted in a new group of risk for PML. While
the minimal risk of PML among these patients is as low as 0.00006% the maximal risk
can reach to 1.17% in a JCV carrier with previous exposure to other chemotherapies
and receiving NTZ for more than 24 months2020 Sorensen PS, Bertolotto A, Edan G, Giovannnoni G, Gold R, Havrdova E
et al. Risk stratification for progressive multifocal leukoencephalopathy in
patients treated with natalizumab. Mult Scler. 2012;18(2):143-52.
http://dx.doi.org/10.1177/1352458511435105
https://doi.org/10.1177/1352458511435105...
.
The putative JCV reactivation, associated to an inefficient viral control caused by Natalizumab support that both viral replication and immunological status of the patients should be monitored through the treatment in order to identify patients at imminent risk of PML without the need to suspend arbitrarily the therapy.
Acknowledgments
We thank the Neuroscience Group of Instituto de Infectologia Emílio Ribas for helpful discussions. We are also in debt with Rosa M. Marcusso for the administrative support.
References
-
1Yednock TA, Cannon C, Fritz LC, Sanchez-Madrid F, Strinman L, Karin N. Prevention of experimental autoimmune encephalomyelitis by antibodies against alpha 4 beta 1 integrin. Nature. 1992;356(6364):63-6. http://dx.doi.org/10.1038/356063a0
» https://doi.org/10.1038/356063a0 -
2Polman CH, O'Connor PW, Havrodova E, Hutschinson M, Kappos L, Miller DH et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med. 2006;354(9):899-910. http://dx.doi.org/10.1056/NEJMoa044397
» https://doi.org/10.1056/NEJMoa044397 -
3Greenlee JE. Progressive multifocal encephalopathy. Handb Clin Neurol. 1998;123:399-430. http://dx.doi.org/10.1016/b978-0-444-53488-0.00017-1
» https://doi.org/10.1016/b978-0-444-53488-0.00017-1 -
4Vidal JE, Oliveira ACP, Fink MC, Pannuti CS, Trujillo JR. Aids-related progressive multifocal leukoencephalopathy: a retrospective study in a referral center in Sao Paulo, Brazil. Rev Inst Med Trop São Paulo. 2008;50(4):209-12. http://dx.doi.org/10.1590/s0036-46652008000400004
» https://doi.org/10.1590/s0036-46652008000400004 -
5Imperiale MJ. Polyomaviruses. In: Knipe DV, Howley PM, editors. Field's virology. New York: Lippincott Williams & Wilkins; 2007. p. 2263-98.
-
6Ravichandran V, Major EO. Viral proteomics: a promising approach for understanding JC virus tropism. Proteomics. 2006;6(20):5628-36. http://dx.doi.org/10.1002/pmic.200600261
» https://doi.org/10.1002/pmic.200600261 -
7Behzad-Behbahani A, Klapper PE, Vallely PJ, Cleator CM, Khoo SH. Detection of BK virus and JC virus DNA in urine samples from immunocompromised (HIV-infected) and immunocompetent (HIV-non-infected) patients using polymerase chain reaction and microplate hybridisation. J Clin Virol. 2004;29(4):224-9. 10.1016/S1386-6532(03)00155-0
» https://doi.org/10.1016/S1386-6532(03)00155-0 -
8Rossi A, Delbue S, Mazziotti R, Vlli M, Borghi E, Mancuso R et al. Presence, quantitation and characterization of JC virus in the urine of Italian immunocompetent subjects. J Med Virol. 2007;79(4):408-12. http://dx.doi.org/10.1002/jmv.20829
» https://doi.org/10.1002/jmv.20829 -
9Nali LHS, Centrone CC, Urbano PRP, Penalva-de-Oliveira AC, Vidal JE, Miranda EP et al. High prevalence of the simultaneous excretion of polyomaviruses JC and BK in the urine of HIV-infected patients without neurological symptoms in Sao Paulo, Brazil. Rev Inst Med Trop São Paulo. 2012;54(4):201-5. http://dx.doi.org/10.1590/S0036-46652012000400004
» https://doi.org/10.1590/S0036-46652012000400004 -
10Yogo Y, Kitamura T, Sujimoto C, Ueki T, Aso Y, Hara K et al. Isolation of a possible archetypal JC virus DNA sequence from nonimmunocompromised individuals. J Virol. 1990;64(6):3139-43.
-
11Pfister LA, Letvin NL, Koralnik IJ. JC virus regulatory region tandem repeats in plasma and central nervous system isolates correlate with poor clinical outcome in patients with progressive multifocal leukoencephalopathy. J Virol. 2001;75(12):5672-6. http://dx.doi.org/10.1128/jvi.75.12.5672-5676.2001
» https://doi.org/10.1128/jvi.75.12.5672-5676.2001 -
12Yogo Y, Matsushina-Ohno T, Hayashi T, Sujimoto S, Sakurai M, Kanazawa I. JC virus regulatory region rearrangements in the brain of a long surviving patient with progressive multifocal leukoencephalopathy. J Neurol Neurosurg Psychiatry. 2001;71(3):397-400. http://dx.doi.org/10.1136/jnnp.71.3.397
» https://doi.org/10.1136/jnnp.71.3.397 -
13Chen Y, Bord E, Tompkins T, Miller J, Tan CS, Kinkel RP et al. Asymptomatic reactivation of JC virus in patients treated with natalizumab. N Engl J Med. 2009;361(11):1067-74. http://dx.doi.org/10.1056/NEJMoa0904267
» https://doi.org/10.1056/NEJMoa0904267 -
14Marshall LJ, Major EO. Molecular regulation of JC virus tropism: insights into potential therapeutic targets for progressive multifocal leukoencephalopathy. J Neuroimmune Pharmacol. 2010;5(3):404-17. http://dx.doi.org/10.1007/s11481-010-9203-1
» https://doi.org/10.1007/s11481-010-9203-1 -
15Reid CE, Li H, Sur G, Carmillo P, Bushnell S, Tizard R al. Sequencing and analysis of JC virus DNA from natalizumab-treated PML patients. J Infect Dis. 2011;204(2):237-44. http://dx.doi.org/10.1093/infdis/jir256
» https://doi.org/10.1093/infdis/jir256 -
16White III FA, Ishaq M, Stoner GL, Frisque RJ. JC virus DNA is present in many human brain samples from patients without progressive multifocal leukoencephalopathy. J Virol. 1992;66(10):5726-34.
-
17Elsner C, Dörries K. Evidence of human polyomavirus BK and JC infection in normal brain tissue. Virology. 1992;191(1):72-80. http://dx.doi.org/10.1016/0042-6822(92)90167-n
» https://doi.org/10.1016/0042-6822(92)90167-n -
18Monaco MC, Jensen PN, Hou J, Durham LC, Major EO. Detection of JC virus DNA in human tonsil tissue: evidence for site of initial viral infection. J Virol. 1998;72(12):9918-23.
-
19Tan CS, Ellis LC, Wüthrich C, Ngo L, Broge TA, Saint-Aubyn J et al. JC virus latency in the brain and extraneural organs of patients with and without progressive multifocal leukoencephalopathy. J Virol. 2010;84(18):9200-9. http://dx.doi.org/10.1128/jvi.00609-10
» https://doi.org/10.1128/jvi.00609-10 -
20Sorensen PS, Bertolotto A, Edan G, Giovannnoni G, Gold R, Havrdova E et al. Risk stratification for progressive multifocal leukoencephalopathy in patients treated with natalizumab. Mult Scler. 2012;18(2):143-52. http://dx.doi.org/10.1177/1352458511435105
» https://doi.org/10.1177/1352458511435105 -
21Antonsson A, Green AC, Mallitt KA, O'Rourke PK, Pawlita M, Waterboer T et al. Prevalence and stability of antibodies to the BK and JC polyomaviruses: a long-term longitudinal study of Australians. J Gen Virol. 2010;91(7):1849-53. http://dx.doi.org/10.1099/vir.0.020115-0
» https://doi.org/10.1099/vir.0.020115-0 -
22Egli A, Infanti L, Dumoulin A, Buser A, Samaridis J, Stebler C et al. Prevalence of polyomavirus BK and JC infection and replication in 400 healthy blood donors. J Infect Dis. 2009;199(6):837-46. http://dx.doi.org/10.1086/597126
» https://doi.org/10.1086/597126 -
23Bozic C, Richman S, Plavina T, Natarajan A, Scanlon JV, Subramanyam M et al. Anti-John Cunnigham virus antibody prevalence in multiple sclerosis patients: baseline results of STRATIFY-1. Ann Neurol. 2011;70(5):742-50. http://dx.doi.org/10.1002/ana.22606
» https://doi.org/10.1002/ana.22606 -
24Kean JM, Rao S, Wang M, Garcea RL. Seroepidemiology of human polyomaviruses. PLoS Pathog. 2009;5(3):e1000363. http://dx.doi.org/10.1371/journal.ppat.1000363
» https://doi.org/10.1371/journal.ppat.1000363 -
25Trampe AK, Hemmelmann C, Stroet A, Haghikia A, Hellwig K, Wiendl H et al. Anti-JC virus antibodies in a large German natalizumab-treated multiple sclerosis cohort. Neurology. 2012;78(22):1736-42. http://dx.doi.org/10.1212/WNL.0b013e3182583022
» https://doi.org/10.1212/WNL.0b013e3182583022 -
26Fernandez O. Best practice in the use of natalizumab in multiple sclerosis. Ther Adv Neurol Disord. 2013;6(2):69-79. http://dx.doi.org/10.1177/1756285612470401
» https://doi.org/10.1177/1756285612470401 -
27Killestein J, Vennegoor A, Strijbis EM. Natalizumab drug holiday in multiple sclerosis: poorly tolerated. Ann Neurol. 2010;68(3):392-5. http://dx.doi.org/10.1002/ana.22074
» https://doi.org/10.1002/ana.22074 -
28Gheuens S, Smith DR, Wang X, Alsop DC, Lenkinski RE, Koralnik IJ. Simultaneous PML-IRIS after discontinuation of natalizumab in a patient with MS. Neurology. 2012;78(18):1390-3. http://dx.doi.org/10.1212/WNL.0b013e318253d61e
» https://doi.org/10.1212/WNL.0b013e318253d61e -
29Pal A, Sirota L, Maudru T, Peden K, Lewis AM. Real-time, quantitative PCR assays for the detection of virus-specific DNA in samples with mixed populations of polyomaviruses. J Virol Methods. 2006;135(1):32-42. http://dx.doi.org/10.1016/j.jviromet.2006.01.018
» https://doi.org/10.1016/j.jviromet.2006.01.018 -
30Laroni A, Giacomazzi CG, Grimaldi L, Gallo P, Sormani MP, Bertolotto A et al. Urinary JCV-DNA testing during natalizumab treatment may increase accuracy of PML risk stratification. J Neuroimmune Pharmacol. 2012;7(3):665-72. http://dx.doi.org/10.1007/s11481-012-9366-z
» https://doi.org/10.1007/s11481-012-9366-z -
31Gosert R, Kardas P, Major EO, Hirsch HH. Rearranged JC virus noncoding control regions found in progressive multifocal leukoencephalopathy patient samples increase virus early gene expression and replication rate. J Virol. 2010;84(20):1048-56. http://dx.doi.org/10.1128/jvi.00614-10
» https://doi.org/10.1128/jvi.00614-10 -
32Raj GV, Khalili K. Transcriptional regulation: lessons from the human neurotropic polyomavirus, JCV. Virology. 1995;213(2):283-91. http://dx.doi.org/10.1006/viro.1995.0001
» https://doi.org/10.1006/viro.1995.0001 -
33Shankarappa R, Margolick JB, Gange SJ, Rodrigo AG, Upchurch D, Farzadegan H et al. Consistent viral evolutionary changes associated with the progression of human immunodeficiency virus type 1 infection. J Virol. 1999;73:10489-1502.
-
34Rambaut A, Posada D, Crandall KA, Holmes EC. The causes and consequences of HIV evolution. Nat Rev Genet. 2004;5(1):52-61. http://dx.doi.org/10.1038/nrg1246
» https://doi.org/10.1038/nrg1246 -
35Ueda E, Enomoto N, Sakamoto N, Hamano K, Sato C, Izumi N et al. Changes of HCV quasispecies during combination therapy with interferon and ribavirin. Hepatol Res. 2004;29(2):89-96. http://dx.doi.org/10.1016/j.hepres.2004.02.014
» https://doi.org/10.1016/j.hepres.2004.02.014 -
36Hatwell JN, Sharp PM. Evolution of human polyomavirus JC. J Gen Virol. 2000;81(5):1191-200.
-
37Fuse S, Molloy MJ, Usherwood EJ. Immune responses against persistent viral infections: possible avenues for immunotherapeutic interventions. Crit Rev Immunol. 2008;28(2):159-83. http://dx.doi.org/10.1615/critrevimmunol.v28.i2.40
» https://doi.org/10.1615/critrevimmunol.v28.i2.40 -
38Benkert TF, Dietz L, Hartmann EM, Leich E, Rosenwald A, Serfling E et al. Natalizumab exerts direct signaling capacity and supports a pro-inflammatory phenotype in some patients with multiple sclerosis. PLoS ONE. 2012;7(12):e52208. http://dx.doi.org/10.1371/journal.pone.0052208
» https://doi.org/10.1371/journal.pone.0052208 -
39Bornsen L, Christensen JR, Ratzer R, Oturai AB, Sørensen PS, Søndergaard HB et al. Effect of natalizumab on circulating CD4+ T-cells in multiple sclerosis. PLoS ONE 2012;7(11):e47578. http://dx.doi.org/10.1371/journal.pone.0047578
» https://doi.org/10.1371/journal.pone.0047578 -
40Perkins MR, Ryschkewitsch C, Liebner JC, Monaco MCG, Himelfarb D, Ireland S et al. Changes in JC virus-specific T cell responses during natalizumab treatment and in natalizumab-associated progressive multifocal leukoencephalopathy. PLoS Pathog. 2012;8(11):e1003014. http://dx.doi.org/10.1371/journal.ppat.1003014
» https://doi.org/10.1371/journal.ppat.1003014
-
Support: This research was made possible by FAPESP, project number 2010/10619-0. LHSN had a CAPES scholarship. The authors declare that they have no conflict of interest.
Publication Dates
-
Publication in this collection
02 Dec 2014 -
Date of issue
Dec 2014
History
-
Received
21 Jan 2014 -
Reviewed
16 July 2014 -
Accepted
04 Aug 2014



