Abstract
INTRODUCTION
American tegumentary leishmaniasis (ATL) is an endemic disease in many regions of Brazil; however, only few reports on the actual epidemiological conditions are available. Here, we aimed to assess the clinical, epidemiological, and laboratory characteristics of ATL patients and their treatment in the 15th Regional Health Division of Paraná State, Maringá, Brazil.
METHODS
This epidemiological study included patients diagnosed with ATL from January 2010 to September 2014, from the 15th Regional Health Division database.
RESULTS
A total of 220 cases aged 3-84 years (85% male and 60.9% with up to 8 years of schooling) were included. The cases were classified as having the cutaneous form (n=183; 83.2%), mucosal form (n=26; 11.8%), mucocutaneous form (n=11; 5%), and relapses (n=21; 9.6%). Diagnosis was made via laboratory test results in 197 (89.5%) patients, and 172 (78.2%) completed the treatment within the study period. With regard to patients with the cutaneous form, 134 (95%) were cured, 131 (97.8%) were treated with Glucantime(r), and 47 (36.7%) received dosage of >15 and <20mg Sb5+/kg/day. Among the cases with mucosal involvement, 87.1% were cured and most were treated with <20mg Sb5+/kg/day. Thus, the cure rate was 93.6%.
CONCLUSIONS
During the study period in the 15th Regional Health Division of Paraná State, ATL cases had a good response to treatment with a low rate of relapse or treatment failure, although a high percentage of mucosal or mucocutaneous form cases was also noted.
Keywords:
Cutaneous leishmaniasis; Mucocutaneous leishmaniasis; Leishmaniasis; Therapeutics. Epidemiology
INTRODUCTION
Leishmaniases are zoonoses caused by more than 20 Leishmania species; more than 90 species of sand flies can transmit the parasite, and approximately 70 animal species have been found to be natural hosts of the parasite. It is estimated that 0.7-1.3 million new cases of tegumentary leishmaniasis (TL) occur annually worldwide11. World Health Organization (WHO). Leishmaniasis fact sheet from WHO. Updated September 2016. http://www.who.int/mediacentre/factsheets/fs375/en/. Accessed 14 Jun 2016.
http://www.who.int/mediacentre/factsheet...
. In particular, 95% of TL cases occur in the Americas, the Mediterranean basin, Central Asia, and the Middle East. Furthermore, more than two-thirds of the new TL cases occur in Afghanistan, Algeria, Brazil, Colombia, Iran, and Syria11. World Health Organization (WHO). Leishmaniasis fact sheet from WHO. Updated September 2016. http://www.who.int/mediacentre/factsheets/fs375/en/. Accessed 14 Jun 2016.
http://www.who.int/mediacentre/factsheet...
.
In Brazil, a total of 635,399 cases of American tegumentary leishmaniasis (ATL) were reported from 1990 to 2013, with an average detection rate of 15.7 cases per 100,000 inhabitants22. Ministério da Saúde. Secretaria de Vigilância Sanitária. Casos de Leishmaniose Tegumentar Americana. Brasil, Grandes Regiões e Unidades Federadas. 1990 a 2013. Available from: http://portalsaude.saude.gov.br/images/pdf/2014/setembro/09/LT-Casos.pdf. Accessed 04 Mar 2015.
http://portalsaude.saude.gov.br/images/p...
. Of 13,889 reported cases in the South region, 95% were reported in the Paraná State, with an average detection rate of 5.8 cases per 100,000 inhabitants33. Ministério da Saúde. Secretaria de Vigilância Sanitária. Coeficiente de detecção de casos de Leishmaniose Tegumentar Americana por 100.000 habitantes. Brasil, Grandes Regiões e Unidades Federadas. 1990 a 2013. Available from: http://portalsaude.saude.gov.br/images/pdf/2014/setembro/09/LT-Coef-Detec----o.pdf. Accessed 04 March 2015.
http://portalsaude.saude.gov.br/images/p...
.
In Paraná State, ATL has persisted even after the original forest vegetation was replaced by coffee, soybean, corn, cotton, and pastures, and has affected individuals of all age groups and both sexes44. Lima AP, Minelli L, Comunello E, Teodoro U. Distribuição da leishmaniose tegumentar por imagens de sensoriamento remoto orbital, no Estado do Paraná, Sul do Brasil. An Bras Dermatol 2002; 77:681-692.) (55. Monteiro WM, Neitzke HC, Lonardoni MVC, Silveira TGV, Ferreira MEMC, Teodoro U. Distribuição geográfica e características epidemiológicas da leishmaniose tegumentar americana em áreas de colonização antiga do Estado do Paraná, Sul do Brasil. Cad Saude Publica 2008; 24:1291-1303.. In urban areas, the disease usually occurs in small areas with preserved forest cover66. Monteiro WM, Neitzke HC, Silveira TGV, Lonardoni MVC, Teodoro U, Ferreira MEMC. Pólos de produção de leishmaniose tegumentar americana no norte do Estado do Paraná, Brasil. Cad Saude Publica 2009; 25:1083-1092.. Two circuits for ATL were identified in Paraná State: the Paraná-Paranapanema circuit, which highlights the Ivaí-Pirapó pole where the municipalities of the 15th Regional Health Division are located, and the Ribeira circuit66. Monteiro WM, Neitzke HC, Silveira TGV, Lonardoni MVC, Teodoro U, Ferreira MEMC. Pólos de produção de leishmaniose tegumentar americana no norte do Estado do Paraná, Brasil. Cad Saude Publica 2009; 25:1083-1092.. In the North and Northwest regions of Paraná State, Leishmania (Viannia) braziliensis is the prevalent species responsible for ATL77. Silveira TGV, Arraes SMAA, Bertolini DA, Teodoro U, Lonardoni MVC, Roberto ACBS, et al. Observações sobre o diagnóstico laboratorial e a epidemiologia da leishmaniose tegumentar no Estado do Paraná, sul do Brasil. Rev Soc Bras Med Trop 1999; 32:413-423.) (88. Castro EA, Soccol VT, Membrive N, Luz E. Estudo das características epidemiológicas e clínicas de 332 casos de leishmaniose tegumentar notificados na região norte do Estado do Paraná de 1993 a 1998. Rev Soc Bras Med Trop 2002; 35:445-452.. The clinical forms of L. (V.) braziliensis infection include cutaneous, mucosal, and disseminated leishmaniasis99. Jirmanus L, Glesby MJ, Guimarães LH, Lago E, Rosa ME, Machado PR, et al. Epidemiological and clinical changes in American tegumentary leishmaniasis in an area of Leishmania (Viannia) braziliensis transmission over a 20-year period. Am J Trop Med Hyg 2012; 86:426-433..
American tegumentary leishmaniasis can be diagnosed based on clinical-epidemiological and laboratorial criteria. In addition, parasitological and immunological diagnostic tests can enhance the efficacy of disease diagnosis77. Silveira TGV, Arraes SMAA, Bertolini DA, Teodoro U, Lonardoni MVC, Roberto ACBS, et al. Observações sobre o diagnóstico laboratorial e a epidemiologia da leishmaniose tegumentar no Estado do Paraná, sul do Brasil. Rev Soc Bras Med Trop 1999; 32:413-423.. Although ATL does not cause death in the absence of complications, it can cause debilitating and stigmatizing lesions1010. Lewnard JA, Jirmanus L, Neri Junior N, Machado PR, Glesby MJ, Ko AI, et al. Forecasting temporal dynamics of cutaneous leishmaniasis in Northeast Brazil. PLoS Negl Trop Dis 2014; 8:e3283. doi: 10.1371/journal.pntd.0003283.
https://doi.org/10.1371/journal.pntd.000...
. Moreover, the drugs recommended for ATL treatment (pentavalent antimony, Amphotericin B, and pentamidine) may cause serious side-effects that can lead to the discontinuation of treatment in some cases1111. Gontijo B, Carvalho MLR. Leishmaniose tegumentar americana. Rev Soc Bras Med Trop 2003; 36:71-80. and even to death1212. Oliveira MC, Amorim RFB, Freitas RA, Costa ALL. Óbito em caso de leishmaniose cutaneomucosa após o uso de antimonial pentavalente. Rev Soc Bras Med Trop 2005; 38:258-260..
Although ATL is an endemic disease in many regions of Brazil, these studies are essential for designing health surveillance actions for prevention, treatment, and disease control. In the present study, we aimed to assess the clinical, epidemiological, and laboratory profile, as well as the treatment of ATL in recent years in the 15th Regional Health Division of Paraná, Maringá, Brazil.
METHODS
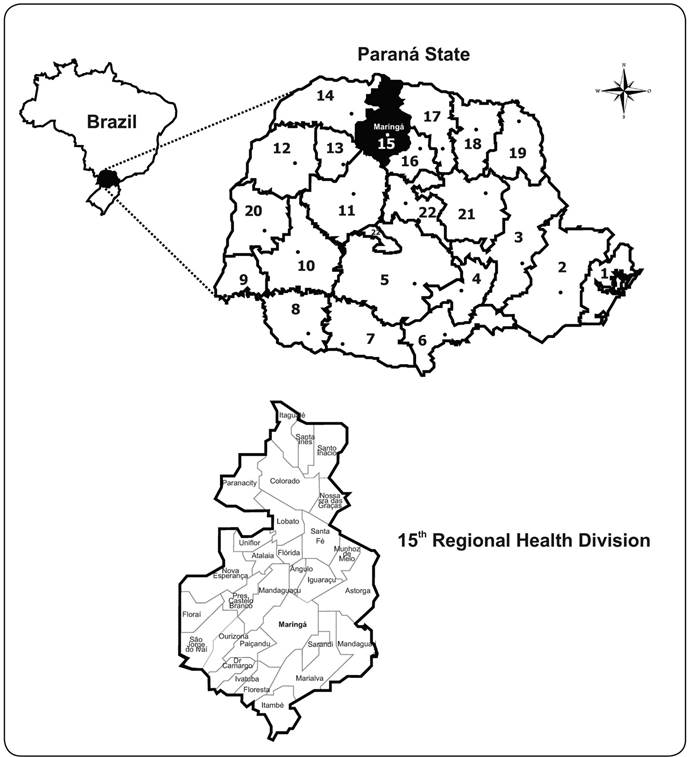
We conducted an epidemiology study using the database of the 15th Regional Health Division (15th RH) of Paraná, Maringá, Paraná State, Brazil, which included patients diagnosed with ATL from January 2010 to September 2014. The 15th RH covers 30 municipalities and is bordered by the latitudes 22.54°S and 23.82°S, and the longitudes 51.66°W and 52.42°W (Figure 1). To complement the information in the structured form, an active search for cases reported to the Sistema de Informação de Agravos de Notificação (SINAN) was performed in the database of the Consórcio Público Intermunicipal de Saúde do Setentrião Paranaense (CISAMUSEP), Maringá, Paraná, which offers specialized medical service to cases referred by the regional municipalities. In the 15th RH, ATL treatment is administered based on the recommendations of the Ministry of Health1313. Ministério da Saúde. Secretaria de Vigilância Sanitária. Manual de vigilância da leishmaniose tegumentar americana. Brasília: 2013. 2ª edição atualizada. 3ª reimpressão. Available from: Available from: http://bvsms.saude.gov.br/bvs/publicacoes/manual_vigilancia_leishmaniose_tegumentar_americana_2edicao.pdf
. Accessed 04 Mar 2015.
http://bvsms.saude.gov.br/bvs/publicacoe...
.

A map of the 15th Regional Health Division of Paraná, Maringá, Paraná State, Brazil, comprising 30 municipalities.
Data from 2 databases were analyzed separately, tabulated in an Excel spreadsheet, and analyzed using Mid-P exact, G, Student's t, and Z tests with the BioEstat(r) 5.3 and OpenEpi(r) 3.03 software, and a 5% significance level.
Ethical considerations
This study was approved by the Committee on Ethics in Research Involving Human Subjects (COPEP) of the State University of Maringá (Report No. 781257 on August 11, 2014).
RESULTS
A total of 220 ATL cases [187 (85%) male; age range, 3-84 years)] were reported from the 15th RH database during the study period; of these patients, 139 (63.2%) were recruited from the complementary search on the CISAMUSEP database.
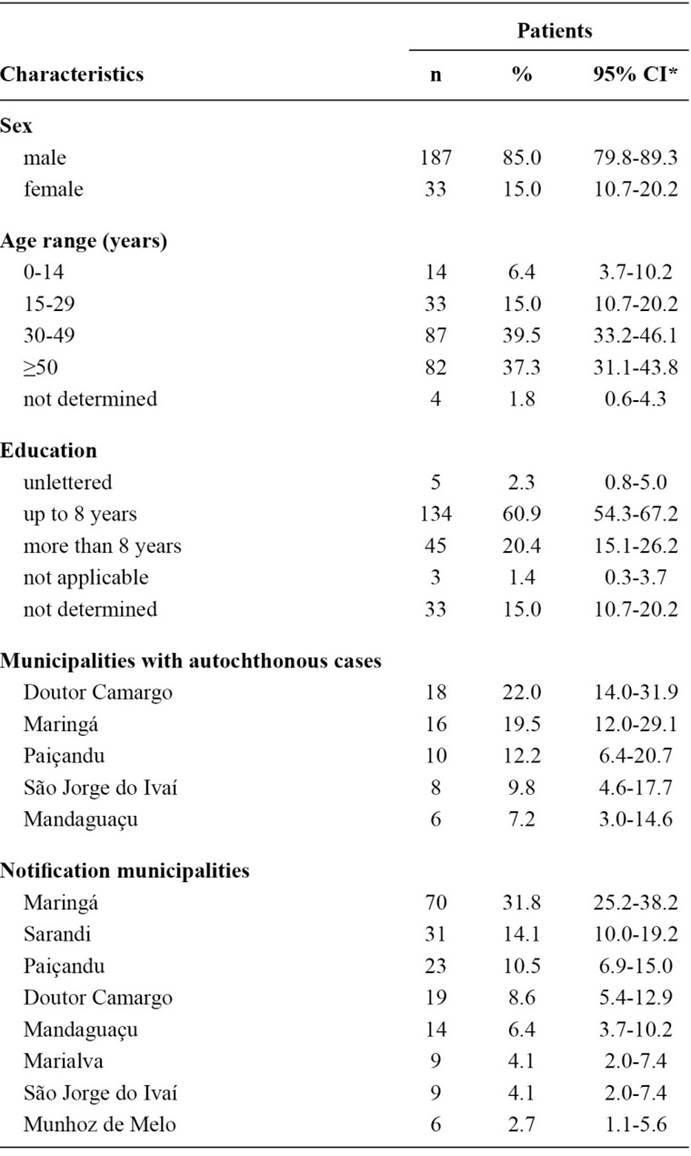
The median age among the female patients was 37 years, whereas that among the male patients was 43 years. The disease was more common in patients aged 30-49 years (87; 39.5%) and ≥50 years (82; 37.3%). Fourteen (6.4%) patients were aged ≤14 years (Table 1). Most of the patients (134; 60.9%) had up to 8 years of schooling. With regard to the epidemiological characteristics, 102 (46.4%) cases were autochthonous, 82 (80.4%) of which were autochthonous for the notification municipality, including Doutor Camargo (18 cases; 22%), Maringá (16 cases; 19.5%), Paiçandu (10 cases; 12.2%), and São Jorge do Ivaí (8 cases; 9.8%). In 12 (5.5%) cases, ATL was acquired from work-related activities. The municipalities with the highest number of cases were Maringá (70; 31.8%), Sarandi (31; 14.1%), Paiçandu (23; 10.5%), Doutor Camargo (19; 8.6%), and Mandaguaçu (14; 6.4%).
With regard to the clinical characteristics (Table 2), 183 (83.2%) cases were classified as cutaneous, 26 (11.8%) were classified as mucosal, and 11 (5%) were classified as mucocutaneous. Twenty-one (9.5%) cases involved disease recurrence. Of the 139 cases from the CISAMUSEP database, 117 completed treatment within the study period (89 with the cutaneous form and 28 with the mucosal form). Cutaneous lesions were most commonly found on the lower limbs (35; 39.3%), followed by the upper limbs (21; 23.6%) and head (9; 10%). The average number of ampoules per patient did not differ when the cutaneous lesions were located on the head, lower limbs, or upper limbs (p>0.05).
In 197 (89.5%) patients, ATL was diagnosed based on the results of laboratory tests. Among 128 patients with cutaneous form ATL, parasitological examination indicated positive results in 115 (89.8%), Montenegro skin test (MST) positivity in 103/109 (94.5%) patients, detection of parasite on histology examination in 46/65 (70.7%) patients, and compatibility with TL in 7/65 (10.8%) patients (Table 3). Among patients with mucosal form ATL, parasitological examination indicated positive results in 8/10 (80%) patients, MST positivity in 12/13 (92.3%) patients, detection of parasite on histology examination in 5/16 (31.2%) patients, and compatibility with TL in 10/16 (62.5%) patients. For patients with mucocutaneous form ATL, parasitological examination indicated positive results in 6/7 (85.7%) patients, MST positivity in 6/7 (85.7%) patients, detection of parasite on histology examination in 2/4 (50%) patients, and compatibility with TL in 1/4 (25%) patient. There was a significant difference in the distribution of the histology results (p=0.016), wherein the presence of the parasite was detected more frequently in cutaneous form ATL and compatibility with TL was more frequent in mucosal form ATL. With regard to the results of parasitological examination and/or histology, the parasite was detected in 84.8% (134/158) of patients with cutaneous form ATL, in 52.4% (11/21) of those with mucosal form ATL, and in 80% (8/10) of those with mucocutaneous form ATL.
Glucantime(r) was used for the treatment of 91.8% patients (202/220). Amphotericin B was used in 35.7% (5/14) of the patients who failed to respond to glucantime therapy. Of the 220 patients, 161 (73.2%) were considered to be cured. Of the 172 patients who completed treatment within the study period, 141 (82%) had cutaneous form ATL, 21 (12.2%) had mucosal form ATL, and 10 (5.8%) had mucocutaneous form ATL (Table 4). Of 141 patients with cutaneous form ATL, 134 (95%) were cured, 131 (97.8%) were treated with Glucantime(r), and 47 (36.7%) received a daily dose of >15 and <20 mg Sb5+/kg; the average number of ampoules per patient was 64.7±32.4. Of the 21 patients with mucosal form ATL, 18 (85.7%) were cured, all were treated with Glucantime(r), and 9 (50%) received a daily dose of ≥20mg Sb5+/kg; the average number of ampoules per patient was 87.5±43.4. Of the 10 patients with mucocutaneous form ATL, 9 (90%) were cured and 4 (44.5%) received a daily dose of ≥20mg Sb5+/kg; the average number of ampoules per patient was 98.9±43.7. The number of ampoules used by patients with cutaneous form ATL was significantly inferior to that used by patients with mucosal form ATL (p=0.044) and mucocutaneous form ATL (p=0.046).
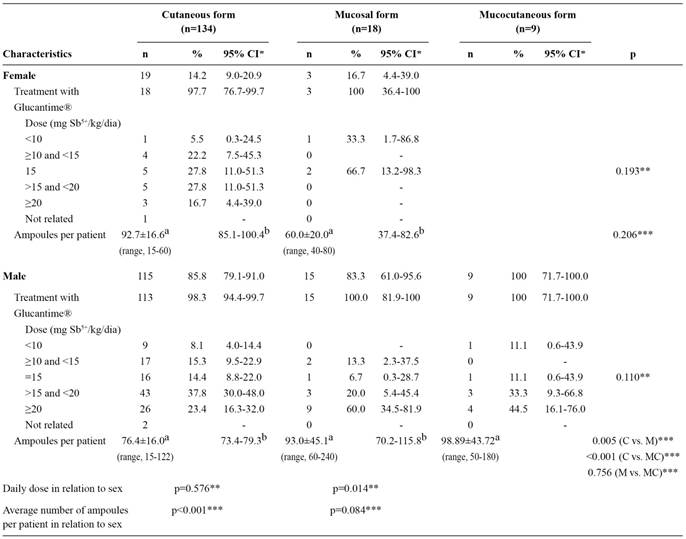
The characteristics of treatment are described in Table 5. The average number of ampoules received by men was higher in the mucosal (p<0.01) and mucocutaneous (p<0.001) form ATL groups as compared to that in the cutaneous form ATL group. The dose prescribed in the mucosal form ATL was greater for men (p=0.014) and the dose prescribed in the cutaneous form ATL was greater for women (p<0.001).
The mean treatment durations of cutaneous and mucosal form ATL were 5.6±4.8 and 5.2±5.4 months, respectively. The average number of visits was 4.3±3.2 for patients with cutaneous form ATL and 4.1±3.3 for those with mucosal involvement. There was no difference in the treatment duration or the average number of visits between the cutaneous and mucosal forms. Moreover, there was no difference in the treatment duration or the average number of visits according to sex for patients with cutaneous form ATL.
DISCUSSION
The endemic nature of ATL in Paraná State has been confirmed by several authors44. Lima AP, Minelli L, Comunello E, Teodoro U. Distribuição da leishmaniose tegumentar por imagens de sensoriamento remoto orbital, no Estado do Paraná, Sul do Brasil. An Bras Dermatol 2002; 77:681-692.) (55. Monteiro WM, Neitzke HC, Lonardoni MVC, Silveira TGV, Ferreira MEMC, Teodoro U. Distribuição geográfica e características epidemiológicas da leishmaniose tegumentar americana em áreas de colonização antiga do Estado do Paraná, Sul do Brasil. Cad Saude Publica 2008; 24:1291-1303.) (66. Monteiro WM, Neitzke HC, Silveira TGV, Lonardoni MVC, Teodoro U, Ferreira MEMC. Pólos de produção de leishmaniose tegumentar americana no norte do Estado do Paraná, Brasil. Cad Saude Publica 2009; 25:1083-1092.) (77. Silveira TGV, Arraes SMAA, Bertolini DA, Teodoro U, Lonardoni MVC, Roberto ACBS, et al. Observações sobre o diagnóstico laboratorial e a epidemiologia da leishmaniose tegumentar no Estado do Paraná, sul do Brasil. Rev Soc Bras Med Trop 1999; 32:413-423.) (88. Castro EA, Soccol VT, Membrive N, Luz E. Estudo das características epidemiológicas e clínicas de 332 casos de leishmaniose tegumentar notificados na região norte do Estado do Paraná de 1993 a 1998. Rev Soc Bras Med Trop 2002; 35:445-452.) (1414. Curti MCM, Silveira TGV, Arraes SMAA, Bertolini DA, Zanzarini PD, Venazzi EAS, et al. Epidemiological and clinical characteristics of cutaneous leishmaniasis and their relationship with laboratory data, South Brazil. Braz J Infect Dis 2011; 15:12-16.) (1515. Curti MCM, Silveira TGV, Arraes SMAA, Bertolini DA, Zanzarini PD, Venazzi EAS, et al. Aspectos epidemiológicos da leishmaniose tegumentar americana na região Noroeste do Estado do Paraná. Rev Cienc Farm Basica Apl 2009; 30:63-68.) (1616. Roberto ACBS, Lima AP, Peixoto PRF, Misuta NM, Fucushigue Y, Ferreira MEMC, et al. Avaliação da terapia com antimoniato de N-metil glucamina e de notificação da leishmaniose tegumentar. An Bras Dermatol 1997; 72:129-136.. In Paraná State, the geographical distribution of ATL is wide and irregular, with a greater concentration of cases in the Northern and Western municipalities, including areas that suffer intense anthropy44. Lima AP, Minelli L, Comunello E, Teodoro U. Distribuição da leishmaniose tegumentar por imagens de sensoriamento remoto orbital, no Estado do Paraná, Sul do Brasil. An Bras Dermatol 2002; 77:681-692.) (55. Monteiro WM, Neitzke HC, Lonardoni MVC, Silveira TGV, Ferreira MEMC, Teodoro U. Distribuição geográfica e características epidemiológicas da leishmaniose tegumentar americana em áreas de colonização antiga do Estado do Paraná, Sul do Brasil. Cad Saude Publica 2008; 24:1291-1303..
In Brazil, ATL is prevalent in both sexes and across all age groups; however, ATL is predominant in individuals aged >10 years (90%), including male patients (74%)1313. Ministério da Saúde. Secretaria de Vigilância Sanitária. Manual de vigilância da leishmaniose tegumentar americana. Brasília: 2013. 2ª edição atualizada. 3ª reimpressão. Available from: Available from: http://bvsms.saude.gov.br/bvs/publicacoes/manual_vigilancia_leishmaniose_tegumentar_americana_2edicao.pdf
. Accessed 04 Mar 2015.
http://bvsms.saude.gov.br/bvs/publicacoe...
. In the present study, ATL was predominant in males (85%) and in those aged ≥30 years (76.8%). In previous studies in Paraná State, Silveira et al.77. Silveira TGV, Arraes SMAA, Bertolini DA, Teodoro U, Lonardoni MVC, Roberto ACBS, et al. Observações sobre o diagnóstico laboratorial e a epidemiologia da leishmaniose tegumentar no Estado do Paraná, sul do Brasil. Rev Soc Bras Med Trop 1999; 32:413-423., Castro et al.88. Castro EA, Soccol VT, Membrive N, Luz E. Estudo das características epidemiológicas e clínicas de 332 casos de leishmaniose tegumentar notificados na região norte do Estado do Paraná de 1993 a 1998. Rev Soc Bras Med Trop 2002; 35:445-452., and Curti et al.1414. Curti MCM, Silveira TGV, Arraes SMAA, Bertolini DA, Zanzarini PD, Venazzi EAS, et al. Epidemiological and clinical characteristics of cutaneous leishmaniasis and their relationship with laboratory data, South Brazil. Braz J Infect Dis 2011; 15:12-16.) reported a higher prevalence of ATL in patients aged 15-49 years, whereas Pontello et al.1717. Pontello Junior R, Gon AS, Ogama A. American cutaneous leishmaniasis: epidemiological profile of patients treated in Londrina from 1998 to 2009. An Bras Dermatol 2013; 88:748-753. reported an associated age of 21-40 years. According to Silva et al. (1818. Silva JSF, Galvão TF, Pereira MG, Silva MT. Treatment of American tegumentary leishmaniasis in special populations: a summary of evidence. Rev Soc Bras Med Trop 2013; 46:669-477., the ATL incidence in individuals aged >65 years has increased significantly in Brazil. In fact, in the present study, 19.5% of the patients were aged >60 years and 6 deaths occurred in individuals aged ≥59 years, including 1 registered in the SINAN as due to ATL. Among these individuals there is a higher risk of co-morbidities complicated by ATL treatment1313. Ministério da Saúde. Secretaria de Vigilância Sanitária. Manual de vigilância da leishmaniose tegumentar americana. Brasília: 2013. 2ª edição atualizada. 3ª reimpressão. Available from: Available from: http://bvsms.saude.gov.br/bvs/publicacoes/manual_vigilancia_leishmaniose_tegumentar_americana_2edicao.pdf
. Accessed 04 Mar 2015.
http://bvsms.saude.gov.br/bvs/publicacoe...
. Death due to ATL was reported in 2.3% cases in Alagoas State1919. Nunes WS, Araújo SR, Calheiros CML. Epidemiological profile of leishmaniasis at reference service in the state of Alagoas, Brazil, from January 2000 to September 2008. Braz J Infec Dis 2010; 14:342-345., which emphasizes the importance of rigorous clinical evaluation prior to and during treatment.
An education level of up to 8 years was common among the ATL patients included in this study, consistent with the findings of Fonseca et al.2020. Fonseca ES, D'Andrea LAZ, Taniguchi HH, Hiramoto RM, Tolezano JE, Guimarães RB. Spatial epidemiology of American cutaneous leishmaniasis in a municipality of west São Paulo State, Brazil. J Vector Borne Dis 2014; 51:271-275.) in the Western State of São Paulo.
ATL was considered an occupational disease since most of the affected individuals were men exposed to forest areas2121. Martins ALGP, Barreto JA, Lauris JRP, Martins ACGP. American tegumentary leishmaniasis: correlations among immunological, histopathological and clinical parameters. An Bras Dermatol 2014; 89:52-58.. However, in recent decades, the vector has adapted to the peri-domiciliary areas of rural regions and urbanized areas, and has hence begun infecting women and children as well2121. Martins ALGP, Barreto JA, Lauris JRP, Martins ACGP. American tegumentary leishmaniasis: correlations among immunological, histopathological and clinical parameters. An Bras Dermatol 2014; 89:52-58.. A small portion (5.5%) of the cases reported in the 15th RH Division were considered to have disease related to work activities, in contrast with the value of 33% previously reported by Silveira et al.77. Silveira TGV, Arraes SMAA, Bertolini DA, Teodoro U, Lonardoni MVC, Roberto ACBS, et al. Observações sobre o diagnóstico laboratorial e a epidemiologia da leishmaniose tegumentar no Estado do Paraná, sul do Brasil. Rev Soc Bras Med Trop 1999; 32:413-423. in a study performed in the same area. Martins et al.2121. Martins ALGP, Barreto JA, Lauris JRP, Martins ACGP. American tegumentary leishmaniasis: correlations among immunological, histopathological and clinical parameters. An Bras Dermatol 2014; 89:52-58.) indicated that, in São Paulo State, ATL was prevalent among adult male patients and rural workers (40.4%), whereas Marlow et al.2222. Marlow MA, Mattos MS, Makowiecky ME, Eger I, Rossetto AL, Grisard EC, et al. Divergent profile of emerging cutaneous leishmaniasis in subtropical Brazil: new endemic areas in the Southern frontier. PlosOne 2013; 8:e56177. doi: 10.1371/journal.pone.0056177.
https://doi.org/10.1371/journal.pone.005...
) reported that, in the State of Santa Catarina, 67.3% of patients were male and 77.8% lived in urban zones. The presence of children (6.4%) and women (15%) among the patients indicates the possibility of peri-domiciliary transmission, and represents significant changes in vector behavior2323. Teodoro U, Silveira TGV, Santos DR, Santos ES, Santos AR, Oliveira O, et al. Freqüência da fauna de flebotomíneos no domicílio e em abrigos de animais domésticos no peridomicílio, nos municípios de Cianorte e Doutor Camargo, Estado do Paraná, Brasil. Rev Patol Trop 2001; 30:209-224.. In this region, the transmission of ATL has also occurred in leisure activities in the vicinity of residual forests2424. Silveira TG, Roberto ACBS, Zanzarini PD, Venazzi EAS, Mangabeira HN, Teodoro U, et al. Leishmaniose tegumentar americana: surto na região urbana, no município de Maringá, Norte do Paraná. Rev Soc Bras Med Trop 2004; 37 (supl III):49., and peridomicile in old rural areas converted into housing complexes or condominiums in small towns.
In the present study, infections occurred mainly in the municipalities of Doutor Camargo, Maringá, Paiçandu, São Jorge do Ivaí, and Mandaguaçu, consistent with the findings of Curti, et al.1515. Curti MCM, Silveira TGV, Arraes SMAA, Bertolini DA, Zanzarini PD, Venazzi EAS, et al. Aspectos epidemiológicos da leishmaniose tegumentar americana na região Noroeste do Estado do Paraná. Rev Cienc Farm Basica Apl 2009; 30:63-68., who reported Maringá, Doutor Camargo, São Jorge do Ivaí, and Sarandi as municipalities where cases were predominant, as well as with those of Roberto et al.1616. Roberto ACBS, Lima AP, Peixoto PRF, Misuta NM, Fucushigue Y, Ferreira MEMC, et al. Avaliação da terapia com antimoniato de N-metil glucamina e de notificação da leishmaniose tegumentar. An Bras Dermatol 1997; 72:129-136., who stated that the largest number of cases occurred in Doutor Camargo, Maringá, and São Jorge do Ivaí. Furthermore, these data are consistent with the findings of Monteiro et al.66. Monteiro WM, Neitzke HC, Silveira TGV, Lonardoni MVC, Teodoro U, Ferreira MEMC. Pólos de produção de leishmaniose tegumentar americana no norte do Estado do Paraná, Brasil. Cad Saude Publica 2009; 25:1083-1092. who described that the Ivaí-Pirapó pole was an important component of the Paraná-Paranapanema circuit for ATL production.
The mucosal or mucocutaneous form of ATL is related to the prevalence of the L. (V.) braziliensis species in the North and Northwest regions of Paraná State77. Silveira TGV, Arraes SMAA, Bertolini DA, Teodoro U, Lonardoni MVC, Roberto ACBS, et al. Observações sobre o diagnóstico laboratorial e a epidemiologia da leishmaniose tegumentar no Estado do Paraná, sul do Brasil. Rev Soc Bras Med Trop 1999; 32:413-423.) (88. Castro EA, Soccol VT, Membrive N, Luz E. Estudo das características epidemiológicas e clínicas de 332 casos de leishmaniose tegumentar notificados na região norte do Estado do Paraná de 1993 a 1998. Rev Soc Bras Med Trop 2002; 35:445-452.. Of the cases reported in the 15th RH Division, 16.8% were classified as mucosal or mucocutaneous form ATL. This percentage is higher than that previously reported in the 15th RH Division by Silveira et al.77. Silveira TGV, Arraes SMAA, Bertolini DA, Teodoro U, Lonardoni MVC, Roberto ACBS, et al. Observações sobre o diagnóstico laboratorial e a epidemiologia da leishmaniose tegumentar no Estado do Paraná, sul do Brasil. Rev Soc Bras Med Trop 1999; 32:413-423., who found 7.7% of cases with mucosal involvement from 1986 to 1997, by Curti et al1515. Curti MCM, Silveira TGV, Arraes SMAA, Bertolini DA, Zanzarini PD, Venazzi EAS, et al. Aspectos epidemiológicos da leishmaniose tegumentar americana na região Noroeste do Estado do Paraná. Rev Cienc Farm Basica Apl 2009; 30:63-68., who found 11.1% of cases with mucosal involvement from 1986 to 2005, and Roberto et al.1616. Roberto ACBS, Lima AP, Peixoto PRF, Misuta NM, Fucushigue Y, Ferreira MEMC, et al. Avaliação da terapia com antimoniato de N-metil glucamina e de notificação da leishmaniose tegumentar. An Bras Dermatol 1997; 72:129-136., who found 9.7% of cases with mucosal or mucocutaneous involvement from 1991 to 1994. Castro et al.88. Castro EA, Soccol VT, Membrive N, Luz E. Estudo das características epidemiológicas e clínicas de 332 casos de leishmaniose tegumentar notificados na região norte do Estado do Paraná de 1993 a 1998. Rev Soc Bras Med Trop 2002; 35:445-452. identified 2% of mucocutaneous lesions among patients in the Arapongas Regional Division of FUNASA (in Northern Paraná State) from 1993 to 1998, whereas Pontello et al.1717. Pontello Junior R, Gon AS, Ogama A. American cutaneous leishmaniasis: epidemiological profile of patients treated in Londrina from 1998 to 2009. An Bras Dermatol 2013; 88:748-753.) identified 15.1% of cases with mucosal involvement among patients in the 17th RH Division (in Northern Paraná State) from 1998 to 2009. In Brazil, the Ministry of Health estimates that 3-5% of cutaneous cases develop into mucosal forms1313. Ministério da Saúde. Secretaria de Vigilância Sanitária. Manual de vigilância da leishmaniose tegumentar americana. Brasília: 2013. 2ª edição atualizada. 3ª reimpressão. Available from: Available from: http://bvsms.saude.gov.br/bvs/publicacoes/manual_vigilancia_leishmaniose_tegumentar_americana_2edicao.pdf
. Accessed 04 Mar 2015.
http://bvsms.saude.gov.br/bvs/publicacoe...
. In Western São Paulo State, 4.9% of cases with mucosal involvement2020. Fonseca ES, D'Andrea LAZ, Taniguchi HH, Hiramoto RM, Tolezano JE, Guimarães RB. Spatial epidemiology of American cutaneous leishmaniasis in a municipality of west São Paulo State, Brazil. J Vector Borne Dis 2014; 51:271-275. were reported from 1998 to 2011, and on the Northern coastline, 1.6% of cases with mucocutaneous involvement were reported from 1993 to 20052525. Condino MLF, Galati EAB, Holcman MM, Salum MRB, Silva DC, Novaes Junior RA. Leishmaniose tegumentar americana no Litoral Norte Paulista, período 1993 a 2005. Rev Soc Bras Med Trop 2008; 41:635-641.. In fact, from 1988 to 2008, of 1209 patients with ATL in Bahia State, 4.3% were found to have mucosal involvement99. Jirmanus L, Glesby MJ, Guimarães LH, Lago E, Rosa ME, Machado PR, et al. Epidemiological and clinical changes in American tegumentary leishmaniasis in an area of Leishmania (Viannia) braziliensis transmission over a 20-year period. Am J Trop Med Hyg 2012; 86:426-433.. Mucocutaneous leishmaniasis can develop several months to ≥20 years after a cutaneous lesion. In particular, malnourished young adult male migrants are at a higher risk. The other risk factors include the location of the primary lesion above the waist, multiple or large primary lesions, or delayed healing of the primary cutaneous leishmaniasis2626. World Health Organization. WHO Technical Report Series 949. Report of a Meeting of the WHO Expert Committee on the Control of Leishmaniases. Geneva: 22-26 March 2010. p. 202. http://apps.who.int/iris/bitstream/10665/44412/1/WHO_TRS_949_eng.pdf. Accessed 14 June 2016.
http://apps.who.int/iris/bitstream/10665...
. The increase in the rates of mucosal or mucocutaneous forms in the 15th RH Division may be related to several factors, such as an increase in the diagnostic rates, late demand for treatment of cutaneous leishmaniasis, failure in the health care network, and changing epidemiological profile of the disease. It should be noted that, during the study period, there was a discontinuity of care provided by the regionalized assistance network, which can have an influence on the high proportion of cases with mucosal involvement.
In the present study, there was a predominance of lesions in the lower limbs (39.3%), followed by the upper limbs (23.6%), consistent with that reported in the literature. Similarly, Pontello et al.1717. Pontello Junior R, Gon AS, Ogama A. American cutaneous leishmaniasis: epidemiological profile of patients treated in Londrina from 1998 to 2009. An Bras Dermatol 2013; 88:748-753. reported a predominance of lesions in the upper limbs (41.4%), followed by lower limbs (30.3%). Moreover, Martins et al.2121. Martins ALGP, Barreto JA, Lauris JRP, Martins ACGP. American tegumentary leishmaniasis: correlations among immunological, histopathological and clinical parameters. An Bras Dermatol 2014; 89:52-58. reported that the regions of the body most frequently affected were the limbs (59.6%), followed by the face (34%). In addition, Murback et al.2727. Murback NDN, Hans Filho G, Nascimento RAF, Nakazato KRO, Dorval MEMC. Leishmaniose tegumentar americana: estudo clínico, epidemiológico e laboratorial realizado no Hospital Universitário de Campo Grande, Mato Grosso do Sul, Brasil. An Bras Dermatol 2011; 86:55-63. found that lesions were located in the lower limbs in 34%, in the face in 25.5%, and in the upper limbs in 19.1%, whereas Name et al.2828. Name RQ, Borges KT, Nogueira LSC, Sampaio JHD, Tauil PL, Sampaio RNR. Estudo clínico, epidemiológico e terapêutico de 402 pacientes com leishmaniose tegumentar americana atendidos no Hospital Universitário de Brasília, DF, Brasil. An Bras Dermatol 2005; 80:249-254.) found that lesions were located in the lower limbs in 56.5%, in the upper limbs in 28.4%, and in the head in 13.6%. The amount of Glucantime(r) ampoules used did not differ according to the location of lesions at different sites.
During the study period, ATL was diagnosed based on clinical and epidemiological criteria in 10.5% of cases, despite the availability of laboratory tests for ATL diagnosis in municipalities of the 15th RH Division. Nevertheless, the diagnosis can be definitively made only when the parasite is detected on direct examination, culture in particular media, histopathology examination, and polymerase chain reaction (PCR)2626. World Health Organization. WHO Technical Report Series 949. Report of a Meeting of the WHO Expert Committee on the Control of Leishmaniases. Geneva: 22-26 March 2010. p. 202. http://apps.who.int/iris/bitstream/10665/44412/1/WHO_TRS_949_eng.pdf. Accessed 14 June 2016.
http://apps.who.int/iris/bitstream/10665...
. Immunological methods such as the MST and serology tests can also help confirm the diagnosis, but do not distinguish between past and present infections2626. World Health Organization. WHO Technical Report Series 949. Report of a Meeting of the WHO Expert Committee on the Control of Leishmaniases. Geneva: 22-26 March 2010. p. 202. http://apps.who.int/iris/bitstream/10665/44412/1/WHO_TRS_949_eng.pdf. Accessed 14 June 2016.
http://apps.who.int/iris/bitstream/10665...
.
The parasitological examination indicated positive results in 89.8% of patients with cutaneous form ATL, 80% with mucosal form ATL, and 85.7% with mucocutaneous form ATL. These rates are higher than those obtained by Silveira et al.77. Silveira TGV, Arraes SMAA, Bertolini DA, Teodoro U, Lonardoni MVC, Roberto ACBS, et al. Observações sobre o diagnóstico laboratorial e a epidemiologia da leishmaniose tegumentar no Estado do Paraná, sul do Brasil. Rev Soc Bras Med Trop 1999; 32:413-423.) for cutaneous form ATL (59.4%) and by Curti et al.1414. Curti MCM, Silveira TGV, Arraes SMAA, Bertolini DA, Zanzarini PD, Venazzi EAS, et al. Epidemiological and clinical characteristics of cutaneous leishmaniasis and their relationship with laboratory data, South Brazil. Braz J Infect Dis 2011; 15:12-16. for cutaneous form ATL (65.1%) in the same area. Murback et al.2727. Murback NDN, Hans Filho G, Nascimento RAF, Nakazato KRO, Dorval MEMC. Leishmaniose tegumentar americana: estudo clínico, epidemiológico e laboratorial realizado no Hospital Universitário de Campo Grande, Mato Grosso do Sul, Brasil. An Bras Dermatol 2011; 86:55-63. observed a rate of 58.8% for positive direct examination in Mato Grosso do Sul State, whereas Reis et al. (2929. Reis LC, Brito MEF, Almeida EL, Félix SM, Medeiros ACR, Silva CJ, et al. Clinical, epidemiological and laboratory aspects of patients with American cutaneous leishmaniasis in the State of Pernambuco. Rev Soc Bras Med Trop 2008: 41:439-443.) observed a rate of 58% for positive direct examination in Pernambuco State. These variations may be due to several factors such as Leishmania species, parasite load, quality of the material collected, site of the lesion where the parasite is investigated, the number of microscopic fields and slides examined, and experience of the technician3030. Mello CX, Schubach AO, Oliveira RVC, Conceição-Silva F, Pimentel MIF, Lyra MR,Vasconcellos ÉCF, Madeira MF. Comparison of the sensitivity of imprint and scraping techniques in the diagnosis of American tegumentary leishmaniasis in a referral centre in Rio de Janeiro, Brazil. Parasitol Res 2011; 109:927-933..
The MST indicated positive results in 94.5%, 92.3%, and 85.7% of patients with cutaneous, mucosal, and mucocutaneous form ATL. In the same area, Silveira et al.77. Silveira TGV, Arraes SMAA, Bertolini DA, Teodoro U, Lonardoni MVC, Roberto ACBS, et al. Observações sobre o diagnóstico laboratorial e a epidemiologia da leishmaniose tegumentar no Estado do Paraná, sul do Brasil. Rev Soc Bras Med Trop 1999; 32:413-423.) described MST positivity in 95.1%, whereas Curti et al.1414. Curti MCM, Silveira TGV, Arraes SMAA, Bertolini DA, Zanzarini PD, Venazzi EAS, et al. Epidemiological and clinical characteristics of cutaneous leishmaniasis and their relationship with laboratory data, South Brazil. Braz J Infect Dis 2011; 15:12-16.) described MST positivity in 92.3% with cutaneous form ATL. Pontello et al.1717. Pontello Junior R, Gon AS, Ogama A. American cutaneous leishmaniasis: epidemiological profile of patients treated in Londrina from 1998 to 2009. An Bras Dermatol 2013; 88:748-753. exhibited 84.4% positivity, Nunes et al.1919. Nunes WS, Araújo SR, Calheiros CML. Epidemiological profile of leishmaniasis at reference service in the state of Alagoas, Brazil, from January 2000 to September 2008. Braz J Infec Dis 2010; 14:342-345. exhibited 56.1% positivity, and Murback et al.2727. Murback NDN, Hans Filho G, Nascimento RAF, Nakazato KRO, Dorval MEMC. Leishmaniose tegumentar americana: estudo clínico, epidemiológico e laboratorial realizado no Hospital Universitário de Campo Grande, Mato Grosso do Sul, Brasil. An Bras Dermatol 2011; 86:55-63.) exhibited 91.4% positivity for MST among the ATL cases.
In the histology examinations, the parasite was detected in 70.7% of patients with cutaneous form ATL, and compatible histology results were more (62.5%) frequently detected for mucosal form ATL. Pontello et al.1717. Pontello Junior R, Gon AS, Ogama A. American cutaneous leishmaniasis: epidemiological profile of patients treated in Londrina from 1998 to 2009. An Bras Dermatol 2013; 88:748-753. reported that the diagnosis was confirmed by biopsy in 26.5% cases. In the present study, the parasite was detected (parasitological examination and/or histology) in 84.8% of cases with the cutaneous form and in 61.3% of cases with mucosal involvement. In the review by Strazzulla et al.3131. Strazzulla A, Cocuzza S, Pinzone MR, Postorino MC, Cosentino S, Serra A, et al. Mucosal leishmaniasis: an underestimated presentation of a neglected disease. BioMed Res Int 2013; 2013: doi: 10.1155/2013/805108. on mucosal form ATL, the presence of Leishmania amastigotes had 35-70% sensitivity and >95% specificity for the mucosal form of L. braziliensis.
Pentavalent antimony (PA) has been used for >70 years, and remains the first-line treatment for leishmaniasis1313. Ministério da Saúde. Secretaria de Vigilância Sanitária. Manual de vigilância da leishmaniose tegumentar americana. Brasília: 2013. 2ª edição atualizada. 3ª reimpressão. Available from: Available from: http://bvsms.saude.gov.br/bvs/publicacoes/manual_vigilancia_leishmaniose_tegumentar_americana_2edicao.pdf
. Accessed 04 Mar 2015.
http://bvsms.saude.gov.br/bvs/publicacoe...
. However, meglumine antimoniate (Glucantime(r)) is used for the treatment of patients in the 15th RH Division of Maringá, based on the recommendation by the Brazilian Ministry of Health1313. Ministério da Saúde. Secretaria de Vigilância Sanitária. Manual de vigilância da leishmaniose tegumentar americana. Brasília: 2013. 2ª edição atualizada. 3ª reimpressão. Available from: Available from: http://bvsms.saude.gov.br/bvs/publicacoes/manual_vigilancia_leishmaniose_tegumentar_americana_2edicao.pdf
. Accessed 04 Mar 2015.
http://bvsms.saude.gov.br/bvs/publicacoe...
. According to WHO, in cases with cutaneous lesions, the overall cure rate at 3 months after treatment is approximately 77-90% when PA is administered at a dose of 20 mg Sb5+/kg per day for 20 days. In cases with mucocutaneous lesions, the cure rates after treatment with PA range from 30% to 100%, with a regimen of 20 mg Sb5+/kg per day for 30 days, depending on the lesion location and geographical area2626. World Health Organization. WHO Technical Report Series 949. Report of a Meeting of the WHO Expert Committee on the Control of Leishmaniases. Geneva: 22-26 March 2010. p. 202. http://apps.who.int/iris/bitstream/10665/44412/1/WHO_TRS_949_eng.pdf. Accessed 14 June 2016.
http://apps.who.int/iris/bitstream/10665...
.
In the present study, 95.0% of patients with the cutaneous form and 85.7% of those with the mucosal form were considered to be cured, which were higher than those (59.1%) described in Northern Paraná State1717. Pontello Junior R, Gon AS, Ogama A. American cutaneous leishmaniasis: epidemiological profile of patients treated in Londrina from 1998 to 2009. An Bras Dermatol 2013; 88:748-753., in Alagoas State (44.5%)1919. Nunes WS, Araújo SR, Calheiros CML. Epidemiological profile of leishmaniasis at reference service in the state of Alagoas, Brazil, from January 2000 to September 2008. Braz J Infec Dis 2010; 14:342-345., and in Rio de Janeiro State (74%)3232. Azeredo-Coutinho RBG, Mendonça SCF. An intermittent schedule is better than continuous regimen of antimonial therapy for cutaneous leishmaniasis in the municipality of Rio de Janeiro, Brazil. Rev Soc Bras Med Trop 2002; 35:477-481.. Similar results were reported by Name et al.2828. Name RQ, Borges KT, Nogueira LSC, Sampaio JHD, Tauil PL, Sampaio RNR. Estudo clínico, epidemiológico e terapêutico de 402 pacientes com leishmaniose tegumentar americana atendidos no Hospital Universitário de Brasília, DF, Brasil. An Bras Dermatol 2005; 80:249-254.) who found a clinical cure rate of 81.6% in patients with the cutaneous form and 69.6% in patients with the mucocutaneous form in Brasília.
Although the suggested dose is 15mg Sb5+/kg/day for the cutaneous form and the recommended dose is 20mg Sb5+/kg/day for the mucosal form1313. Ministério da Saúde. Secretaria de Vigilância Sanitária. Manual de vigilância da leishmaniose tegumentar americana. Brasília: 2013. 2ª edição atualizada. 3ª reimpressão. Available from: Available from: http://bvsms.saude.gov.br/bvs/publicacoes/manual_vigilancia_leishmaniose_tegumentar_americana_2edicao.pdf
. Accessed 04 Mar 2015.
http://bvsms.saude.gov.br/bvs/publicacoe...
, 59.4% of cases with the cutaneous form received a daily dose >15mg Sb5+/kg and 51.9% of cases with mucosal involvement received a daily dose <20mg Sb5+/kg.
The average number of ampoules used by patients with mucosal and mucocutaneous involvement was greater than that used by patients with cutaneous involvement. Overall, the average number of Glucantime(r) ampoules prescribed per patient was 69.3, which is lower than that reported by Roberto et al.1616. Roberto ACBS, Lima AP, Peixoto PRF, Misuta NM, Fucushigue Y, Ferreira MEMC, et al. Avaliação da terapia com antimoniato de N-metil glucamina e de notificação da leishmaniose tegumentar. An Bras Dermatol 1997; 72:129-136. in the same area, wherein the average number of Glucantime(r) ampoules prescribed per patient, from 1991 to 1994, was 75.6. Moreover, we found that the doses prescribed for men were higher than for those prescribed for women with the mucosal form, whereas the number of ampoules administered to women was higher than that for men with the cutaneous form. This is inconsistent with the findings of Name et al.2828. Name RQ, Borges KT, Nogueira LSC, Sampaio JHD, Tauil PL, Sampaio RNR. Estudo clínico, epidemiológico e terapêutico de 402 pacientes com leishmaniose tegumentar americana atendidos no Hospital Universitário de Brasília, DF, Brasil. An Bras Dermatol 2005; 80:249-254., who reported that PA was more effective in females with the cutaneous form. However, no difference in treatment time or the average number of visits for patients with the cutaneous or mucosal forms was noted.
Resistance to PA is often encountered in South America and is a frequent cause of recurrence or treatment failure3131. Strazzulla A, Cocuzza S, Pinzone MR, Postorino MC, Cosentino S, Serra A, et al. Mucosal leishmaniasis: an underestimated presentation of a neglected disease. BioMed Res Int 2013; 2013: doi: 10.1155/2013/805108.. Failure of treatment with PA occurred in 6.4% of patients. This failure rate was lower than that described by the World Health Organization (WHO)2626. World Health Organization. WHO Technical Report Series 949. Report of a Meeting of the WHO Expert Committee on the Control of Leishmaniases. Geneva: 22-26 March 2010. p. 202. http://apps.who.int/iris/bitstream/10665/44412/1/WHO_TRS_949_eng.pdf. Accessed 14 June 2016.
http://apps.who.int/iris/bitstream/10665...
and that reported in Rio de Janeiro State (12.5%)3232. Azeredo-Coutinho RBG, Mendonça SCF. An intermittent schedule is better than continuous regimen of antimonial therapy for cutaneous leishmaniasis in the municipality of Rio de Janeiro, Brazil. Rev Soc Bras Med Trop 2002; 35:477-481.. In these cases, amphotericin B (2.3%) and pentamidine (0.9%) were used instead. In Northern Paraná1717. Pontello Junior R, Gon AS, Ogama A. American cutaneous leishmaniasis: epidemiological profile of patients treated in Londrina from 1998 to 2009. An Bras Dermatol 2013; 88:748-753., 5.6% of patients were treated with pentamidine due to the side-effects of amphotericin B.
The limitations of this study include the small sample size and the inability to recruit all the patients from the SINAN registry; nevertheless, this study enables the comprehensive assessment of ATL behavior in the region, and the data can be used to design novel health surveillance measures.
In the 15th RH Division of Paraná State, ATL was more frequent among men, particularly in the cutaneous form, although 16.8% of the cases had the mucosal or mucocutaneous form. This rate is higher than that estimated by the Brazilian Health Ministry, and an increase in the number of cases with mucosal involvement is evident in comparison with the findings of previous studies in the same area. ATL was primarily diagnosed based on laboratory test results. The drug used in most of the cases was Glucantime(r), which showed a good response to treatment and low rate of relapse or treatment failure. Most of the patients with the mucosal form received doses lower than that recommended by the Ministry of Health. Furthermore, the rate of mucosal leishmaniasis was greater than that reported in the literature.
Acknowledgments
We offer our deepest thanks to the institutions that provided technical support for the development and implementation of this study. The authors would like to thank Dr. Izabel Galhardo Demarchi, Departamento de Análises Clínicas e Biomedicina, Universidade Estadual de Maringá, Brazil, for drawing the map.
References
-
1World Health Organization (WHO). Leishmaniasis fact sheet from WHO. Updated September 2016. http://www.who.int/mediacentre/factsheets/fs375/en/ Accessed 14 Jun 2016.
» http://www.who.int/mediacentre/factsheets/fs375/en/ -
2Ministério da Saúde. Secretaria de Vigilância Sanitária. Casos de Leishmaniose Tegumentar Americana. Brasil, Grandes Regiões e Unidades Federadas. 1990 a 2013. Available from: http://portalsaude.saude.gov.br/images/pdf/2014/setembro/09/LT-Casos.pdf. Accessed 04 Mar 2015.
» http://portalsaude.saude.gov.br/images/pdf/2014/setembro/09/LT-Casos.pdf. -
3Ministério da Saúde. Secretaria de Vigilância Sanitária. Coeficiente de detecção de casos de Leishmaniose Tegumentar Americana por 100.000 habitantes. Brasil, Grandes Regiões e Unidades Federadas. 1990 a 2013. Available from: http://portalsaude.saude.gov.br/images/pdf/2014/setembro/09/LT-Coef-Detec----o.pdf. Accessed 04 March 2015.
» http://portalsaude.saude.gov.br/images/pdf/2014/setembro/09/LT-Coef-Detec----o.pdf. -
4Lima AP, Minelli L, Comunello E, Teodoro U. Distribuição da leishmaniose tegumentar por imagens de sensoriamento remoto orbital, no Estado do Paraná, Sul do Brasil. An Bras Dermatol 2002; 77:681-692.
-
5Monteiro WM, Neitzke HC, Lonardoni MVC, Silveira TGV, Ferreira MEMC, Teodoro U. Distribuição geográfica e características epidemiológicas da leishmaniose tegumentar americana em áreas de colonização antiga do Estado do Paraná, Sul do Brasil. Cad Saude Publica 2008; 24:1291-1303.
-
6Monteiro WM, Neitzke HC, Silveira TGV, Lonardoni MVC, Teodoro U, Ferreira MEMC. Pólos de produção de leishmaniose tegumentar americana no norte do Estado do Paraná, Brasil. Cad Saude Publica 2009; 25:1083-1092.
-
7Silveira TGV, Arraes SMAA, Bertolini DA, Teodoro U, Lonardoni MVC, Roberto ACBS, et al. Observações sobre o diagnóstico laboratorial e a epidemiologia da leishmaniose tegumentar no Estado do Paraná, sul do Brasil. Rev Soc Bras Med Trop 1999; 32:413-423.
-
8Castro EA, Soccol VT, Membrive N, Luz E. Estudo das características epidemiológicas e clínicas de 332 casos de leishmaniose tegumentar notificados na região norte do Estado do Paraná de 1993 a 1998. Rev Soc Bras Med Trop 2002; 35:445-452.
-
9Jirmanus L, Glesby MJ, Guimarães LH, Lago E, Rosa ME, Machado PR, et al. Epidemiological and clinical changes in American tegumentary leishmaniasis in an area of Leishmania (Viannia) braziliensis transmission over a 20-year period. Am J Trop Med Hyg 2012; 86:426-433.
-
10Lewnard JA, Jirmanus L, Neri Junior N, Machado PR, Glesby MJ, Ko AI, et al. Forecasting temporal dynamics of cutaneous leishmaniasis in Northeast Brazil. PLoS Negl Trop Dis 2014; 8:e3283. doi: 10.1371/journal.pntd.0003283.
» https://doi.org/10.1371/journal.pntd.0003283 -
11Gontijo B, Carvalho MLR. Leishmaniose tegumentar americana. Rev Soc Bras Med Trop 2003; 36:71-80.
-
12Oliveira MC, Amorim RFB, Freitas RA, Costa ALL. Óbito em caso de leishmaniose cutaneomucosa após o uso de antimonial pentavalente. Rev Soc Bras Med Trop 2005; 38:258-260.
-
13Ministério da Saúde. Secretaria de Vigilância Sanitária. Manual de vigilância da leishmaniose tegumentar americana. Brasília: 2013. 2ª edição atualizada. 3ª reimpressão. Available from: Available from: http://bvsms.saude.gov.br/bvs/publicacoes/manual_vigilancia_leishmaniose_tegumentar_americana_2edicao.pdf Accessed 04 Mar 2015.
» http://bvsms.saude.gov.br/bvs/publicacoes/manual_vigilancia_leishmaniose_tegumentar_americana_2edicao.pdf -
14Curti MCM, Silveira TGV, Arraes SMAA, Bertolini DA, Zanzarini PD, Venazzi EAS, et al. Epidemiological and clinical characteristics of cutaneous leishmaniasis and their relationship with laboratory data, South Brazil. Braz J Infect Dis 2011; 15:12-16.
-
15Curti MCM, Silveira TGV, Arraes SMAA, Bertolini DA, Zanzarini PD, Venazzi EAS, et al. Aspectos epidemiológicos da leishmaniose tegumentar americana na região Noroeste do Estado do Paraná. Rev Cienc Farm Basica Apl 2009; 30:63-68.
-
16Roberto ACBS, Lima AP, Peixoto PRF, Misuta NM, Fucushigue Y, Ferreira MEMC, et al. Avaliação da terapia com antimoniato de N-metil glucamina e de notificação da leishmaniose tegumentar. An Bras Dermatol 1997; 72:129-136.
-
17Pontello Junior R, Gon AS, Ogama A. American cutaneous leishmaniasis: epidemiological profile of patients treated in Londrina from 1998 to 2009. An Bras Dermatol 2013; 88:748-753.
-
18Silva JSF, Galvão TF, Pereira MG, Silva MT. Treatment of American tegumentary leishmaniasis in special populations: a summary of evidence. Rev Soc Bras Med Trop 2013; 46:669-477.
-
19Nunes WS, Araújo SR, Calheiros CML. Epidemiological profile of leishmaniasis at reference service in the state of Alagoas, Brazil, from January 2000 to September 2008. Braz J Infec Dis 2010; 14:342-345.
-
20Fonseca ES, D'Andrea LAZ, Taniguchi HH, Hiramoto RM, Tolezano JE, Guimarães RB. Spatial epidemiology of American cutaneous leishmaniasis in a municipality of west São Paulo State, Brazil. J Vector Borne Dis 2014; 51:271-275.
-
21Martins ALGP, Barreto JA, Lauris JRP, Martins ACGP. American tegumentary leishmaniasis: correlations among immunological, histopathological and clinical parameters. An Bras Dermatol 2014; 89:52-58.
-
22Marlow MA, Mattos MS, Makowiecky ME, Eger I, Rossetto AL, Grisard EC, et al. Divergent profile of emerging cutaneous leishmaniasis in subtropical Brazil: new endemic areas in the Southern frontier. PlosOne 2013; 8:e56177. doi: 10.1371/journal.pone.0056177.
» https://doi.org/10.1371/journal.pone.0056177 -
23Teodoro U, Silveira TGV, Santos DR, Santos ES, Santos AR, Oliveira O, et al. Freqüência da fauna de flebotomíneos no domicílio e em abrigos de animais domésticos no peridomicílio, nos municípios de Cianorte e Doutor Camargo, Estado do Paraná, Brasil. Rev Patol Trop 2001; 30:209-224.
-
24Silveira TG, Roberto ACBS, Zanzarini PD, Venazzi EAS, Mangabeira HN, Teodoro U, et al. Leishmaniose tegumentar americana: surto na região urbana, no município de Maringá, Norte do Paraná. Rev Soc Bras Med Trop 2004; 37 (supl III):49.
-
25Condino MLF, Galati EAB, Holcman MM, Salum MRB, Silva DC, Novaes Junior RA. Leishmaniose tegumentar americana no Litoral Norte Paulista, período 1993 a 2005. Rev Soc Bras Med Trop 2008; 41:635-641.
-
26World Health Organization. WHO Technical Report Series 949. Report of a Meeting of the WHO Expert Committee on the Control of Leishmaniases. Geneva: 22-26 March 2010. p. 202. http://apps.who.int/iris/bitstream/10665/44412/1/WHO_TRS_949_eng.pdf Accessed 14 June 2016.
» http://apps.who.int/iris/bitstream/10665/44412/1/WHO_TRS_949_eng.pdf -
27Murback NDN, Hans Filho G, Nascimento RAF, Nakazato KRO, Dorval MEMC. Leishmaniose tegumentar americana: estudo clínico, epidemiológico e laboratorial realizado no Hospital Universitário de Campo Grande, Mato Grosso do Sul, Brasil. An Bras Dermatol 2011; 86:55-63.
-
28Name RQ, Borges KT, Nogueira LSC, Sampaio JHD, Tauil PL, Sampaio RNR. Estudo clínico, epidemiológico e terapêutico de 402 pacientes com leishmaniose tegumentar americana atendidos no Hospital Universitário de Brasília, DF, Brasil. An Bras Dermatol 2005; 80:249-254.
-
29Reis LC, Brito MEF, Almeida EL, Félix SM, Medeiros ACR, Silva CJ, et al. Clinical, epidemiological and laboratory aspects of patients with American cutaneous leishmaniasis in the State of Pernambuco. Rev Soc Bras Med Trop 2008: 41:439-443.
-
30Mello CX, Schubach AO, Oliveira RVC, Conceição-Silva F, Pimentel MIF, Lyra MR,Vasconcellos ÉCF, Madeira MF. Comparison of the sensitivity of imprint and scraping techniques in the diagnosis of American tegumentary leishmaniasis in a referral centre in Rio de Janeiro, Brazil. Parasitol Res 2011; 109:927-933.
-
31Strazzulla A, Cocuzza S, Pinzone MR, Postorino MC, Cosentino S, Serra A, et al. Mucosal leishmaniasis: an underestimated presentation of a neglected disease. BioMed Res Int 2013; 2013: doi: 10.1155/2013/805108.
-
32Azeredo-Coutinho RBG, Mendonça SCF. An intermittent schedule is better than continuous regimen of antimonial therapy for cutaneous leishmaniasis in the municipality of Rio de Janeiro, Brazil. Rev Soc Bras Med Trop 2002; 35:477-481.
-
Programa de Apoio à Pós-Graduação/Coordenação de Aperfeiçoamento de Pessoal de Nível Superior and Laboratório de Ensino e Pesquisa em Análises Clínicas/Universidade Estadual de Maringá
Publication Dates
-
Publication in this collection
Sep-Oct 2016
History
-
Received
25 May 2016 -
Accepted
23 Sept 2016