Abstract
OBJECTIVE:
To examine the association of atherogenic and thrombogenic markers and lymphotoxin-alfa gene mutations with the risk of premature coronary disease.
METHODS:
This cross-sectional, case-control, age-adjusted study was conducted in 336 patients with premature coronary disease (<50 years old) and 189 healthy controls. The control subjects had normal clinical, resting, and exercise stress electrocardiographic assessments. The coronary disease group patients had either angiographically documented disease (>50% luminal reduction) or a previous myocardial infarction. The laboratory data evaluated included thrombogenic factors (fibrinogen, protein C, protein S, and antithrombin III), atherogenic factors (glucose and lipid profiles, lipoprotein(a), and apolipoproteins AI and B), and lymphotoxin-alfa mutations. Genetic variability of lymphotoxin-alfa was determined by polymerase chain reaction analysis.
RESULTS:
Coronary disease patients exhibited lower concentrations of HDL-cholesterol and higher levels of glucose, lipoprotein(a), and protein S. The frequencies of AA, AG, and GG lymphotoxin-alfa mutation genotypes were 55.0%, 37.6%, and 7.4% for controls and 42.7%, 46.0%, and 11.3% for coronary disease patients (p = 0.02), respectively. Smoking, dyslipidemia, family history, and lipoprotein(a) and lymphotoxin-alfa mutations in men were independent variables associated with coronary disease. The area under the curve (C-statistic) increased from 0.779 to 0.802 (p<0.05) with the inclusion of lipoprotein(a) and lymphotoxin-alfa mutations in the set of conventional risk factors.
CONCLUSIONS:
The inclusion of lipoprotein(a) and lymphotoxin-alfa mutations in the set of conventional risk factors showed an additive but small increase in the risk prediction of premature coronary disease.
Coronary Artery Disease; Risk Factors; Thrombosis; Inflammation; Lipids; Lipoprotein(a); Risk Prediction; Lymphotoxin-Alfa
INTRODUCTION
Coronary atherosclerosis and its complications constitute a complex and polygenic disorder
resulting from the combined effects of multiple environmental and genetic factors (11. Wang Q. Molecular genetics of coronary artery disease. Curr Opin Cardiol.
2005;20(3):182-8, http://dx.doi.org/10.1097/01.hco.0000160373.77190.f1.
http://dx.doi.org/10.1097/01.hco.0000160...
). Several traditional risk factors increase the risk of coronary
heart disease (CHD) and heart attack (22. Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010
ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: executive summary:
a report of the American College of Cardiology Foundation/American Heart Association Task Force on
Practice Guidelines. Circulation. 2010;122(25):2748-64.
3. Peden JF, Farrall M. Thirty-five common variants for coronary artery disease: the
fruits of much collaborative labour. Hum Mol Genet. 2011;20(R2):R198-R205,
http://dx.doi.org/10.1093/hmg/ddr384.
http://dx.doi.org/10.1093/hmg/ddr384...
-44. Ross R. Atherosclerosis an inflammatory disease. N Engl J Med.
1999;340(2):115-26.). Coronary artery disease (CAD) results from the progression of atherosclerotic
plaque. Studies show that almost half of an individual's susceptibility to CAD is heritable
(33. Peden JF, Farrall M. Thirty-five common variants for coronary artery disease: the
fruits of much collaborative labour. Hum Mol Genet. 2011;20(R2):R198-R205,
http://dx.doi.org/10.1093/hmg/ddr384.
http://dx.doi.org/10.1093/hmg/ddr384...
). Lipid metabolism and inflammation have been identified
as main biological pathways in the pathogenesis of CAD. Arterial inflammation is a key component of
plaque progression and plaque rupture, with atherosclerotic lesions established as active sites of
inflammation (44. Ross R. Atherosclerosis an inflammatory disease. N Engl J Med.
1999;340(2):115-26.). Biomarkers, coagulation factors, and
proteins appear to coordinate the development of atherosclerosis and lead to the formation of
complex atherosclerotic plaques and thrombus formation (55. Weber C, Noels H. Atherosclerosis: current pathogenesis and therapeutic options.
Nat Med. 2011;17(11):1410-22, http://dx.doi.org/10.1038/nm.2538.
http://dx.doi.org/10.1038/nm.2538...
6. Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Rumberger J, et al. From
vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies:
Part I. Circulation. 2003;108(14):1664-72,
http://dx.doi.org/10.1161/01.CIR.0000087480.94275.97.
http://dx.doi.org/10.1161/01.CIR.0000087...
-77. Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Rumberger J, et al. From
vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies:
Part II. Circulation. 2003;108(15):1772-8,
http://dx.doi.org/10.1161/01.CIR.0000087481.55887.C9.
http://dx.doi.org/10.1161/01.CIR.0000087...
). Several biomarkers and cytokines likely play a
role in determining the degree of inflammation and contribute to the promotion or retardation of
atherothrombosis development. Despite the improved understanding of atherothrombosis
pathophysiology, the conventional CAD risk factors do not fully account for the overall CAD risk
(88. Sposito AC, Alvarenga BF, Alexandre AS, Araújo AL, Santos SN, Andrade JM, et
al. Most of the patients presenting myocardial infarction would not be eligible for intensive
lipid-lowering based on clinical algorithms or plasma C reactive protein. Atherosclerosis.
2011;214(1):148-50, http://dx.doi.org/10.1016/j.atherosclerosis.2010.10.034.
http://dx.doi.org/10.1016/j.atherosclero...
,99. Lloyd-Jones DM, Wilson PW, Larson MG, Beiser A, Leip EP, D'Agostino RB, et
al. Framingham risk score and prediction of lifetime risk for coronary heart disease.
Am J Cardiol. 2004;94(1):20-4,
http://dx.doi.org/10.1016/j.amjcard.2004.03.023.
http://dx.doi.org/10.1016/j.amjcard.2004...
). Moreover, risk
factors associated with premature CAD are poorly recognized. Studies also show conflicting results
with respect to some atherogenic and thrombogenic biomarkers of CAD (1010. Kistorp C, Raymond I, Pedersen F, Gustafsson F, Faber J, Hildebrandt P, et al.
N-terminal pro-brain natriuretic peptide, C-reactive protein, and urinary albumin levels as
predictors of mortality and cardiovascular events in older adults. JAMA. 2005;293(13):1609-16,
http://dx.doi.org/10.1001/jama.293.13.1609.
http://dx.doi.org/10.1001/jama.293.13.16...
11. Zethelius B, Berglund L, Sundström J, Ingelsson E, Basu S, Larsson A, et
al. Use of multiple biomarkers to improve the prediction of death from cardiovascular causes.
N Engl J Med. 2008;358(20):2107-16.-1212. Brown TM, Bittner V. Biomarkers of atherosclerosis: clinical applications. Curr
Cardiol Rep. 2008;10(6):497-504, http://dx.doi.org/10.1007/s11886-008-0078-1.
http://dx.doi.org/10.1007/s11886-008-007...
). Genetic influence is often suggested as an
important factor associated with the risk of premature CAD (1313. Roberts R, Stewart AF. The genetics of coronary artery disease. Curr Opin
Cardiol. 2012;27(3):221-7, http://dx.doi.org/10.1097/HCO.0b013e3283515b4b.
http://dx.doi.org/10.1097/HCO.0b013e3283...
). The proinflammatory cytokine lymphotoxin-alfa (LTA) is a key mediator of the initiation
of local vascular inflammatory responses. The actions of LTA are characterized by the stimulation of
adhesion molecule production, thrombogenesis, smooth muscle proliferation, platelet activation,
release of vasoactive agents (1414. Pober JS, Lapierre LA, Stolpen AH, Brock TA, Springer TA, Fiers W, et al.
Activation of cultured human endothelial cells by recombinant lymphotoxin: comparison with tumor
necrosis factor and interleukin 1 species. J Immunol. 1987;138(10):3319-24.
15. Cavender DE, Edelbaum D, Ziff M. Endothelial cell activation induced by tumor
necrosis factor and lymphotoxin. Am J Pathol. 1989;134(3):551-60.
16. Kratz A, Campos-Neto A, Hanson MS, Ruddle NH. Chronic inflammation caused by
lymphotoxin is lymphoid neogenesis. J Exp Med 1996;183(4):1461-72,
http://dx.doi.org/10.1084/jem.183.4.1461.
http://dx.doi.org/10.1084/jem.183.4.1461...
-1717. Ozaki K, Inoue K, Sato H, Iida A, Ohnishi Y, Sekine A, et al. Functional
variation in LGALS2 confers risk of myocardial infarction and regulates lymphotoxin-alpha secretion
in vitro. Nature. 2004;429(6987):72-5, http://dx.doi.org/10.1038/nature02502.
http://dx.doi.org/10.1038/nature02502...
), and control of nitric oxide production (88. Sposito AC, Alvarenga BF, Alexandre AS, Araújo AL, Santos SN, Andrade JM, et
al. Most of the patients presenting myocardial infarction would not be eligible for intensive
lipid-lowering based on clinical algorithms or plasma C reactive protein. Atherosclerosis.
2011;214(1):148-50, http://dx.doi.org/10.1016/j.atherosclerosis.2010.10.034.
http://dx.doi.org/10.1016/j.atherosclero...
). Functional single nucleotide polymorphisms (SNPs) in the LTA gene have been found to be
associated with MI in the Japanese population (1717. Ozaki K, Inoue K, Sato H, Iida A, Ohnishi Y, Sekine A, et al. Functional
variation in LGALS2 confers risk of myocardial infarction and regulates lymphotoxin-alpha secretion
in vitro. Nature. 2004;429(6987):72-5, http://dx.doi.org/10.1038/nature02502.
http://dx.doi.org/10.1038/nature02502...
,1818. Ozaki K, Ohnishi Y, Iida A, Sekine A, Yamada R, Tsunoda T, et al. Functional
SNPs in the lymphotoxin-alpha gene that are associated with susceptibility to myocardial infarction.
Nat Genet. 2002;32(4):650-4, http://dx.doi.org/10.1038/ng1047.
http://dx.doi.org/10.1038/ng1047...
). However, other researchers failed to provide evidence of the
relationship between LTA and CAD (1919. Ozaki K, Tanaka T. Genome-wide association study to identify SNPs conferring
risk of myocardial infarction and their functional analyses. Cell Mol Life Sci. 2005;62(16):1804-13,
http://dx.doi.org/10.1007/s00018-005-5098-z.
http://dx.doi.org/10.1007/s00018-005-509...
20. Li W, Xu J, Wang X, Chen J, Zhang C, Sun K, et al. Lack of association between
lymphotoxin-alpha, galectin-2 polymorphisms and coronary artery disease: a meta-analysis.
Atherosclerosis. 2010;208(2):433-6,
http://dx.doi.org/10.1016/j.atherosclerosis.2009.08.014.
http://dx.doi.org/10.1016/j.atherosclero...
-2121. Ryan AW, O'Brien E, Shields D, McManus R. Lack of association between
NFKBIL1/LTA polymorphisms and hypertension, myocardial infarct, unstable angina and stable angina in
a large Irish population sample. Atherosclerosis. 2008;197(1):465-466,
http://dx.doi.org/10.1016/j.atherosclerosis.2007.03.032.
http://dx.doi.org/10.1016/j.atherosclero...
). The mutant allele results in significantly increased production of LTA in
mononuclear cells stimulated in vitro, which is related to increased gene
transcription (1717. Ozaki K, Inoue K, Sato H, Iida A, Ohnishi Y, Sekine A, et al. Functional
variation in LGALS2 confers risk of myocardial infarction and regulates lymphotoxin-alpha secretion
in vitro. Nature. 2004;429(6987):72-5, http://dx.doi.org/10.1038/nature02502.
http://dx.doi.org/10.1038/nature02502...
). The aim of this study was to investigate
whether traditional risk factors, thrombogenic and atherogenic biomarkers, and the mutation A252G in
the LTA gene may be related to an increased predisposition to premature CAD and its interaction with
traditional risk factor modulation.
MATERIALS AND METHODS
Study population
A cross-sectional, case-control, age-matched study was conducted in 525 consecutive subjects <50 years of age. Clinical characteristics and laboratory data were analyzed in 189 healthy control individuals and in 336 patients with documented premature stable CAD (<50 years of age) selected from the outpatient clinic of the Heart Institute (InCor), Faculdade de Medicina da Universidade de São Paulo, Brazil. We hypothesized that young adult patients exhibit a larger proportion of CAD driven by genetic risk factors compared with older patients with CAD. The control group with no CAD included healthy subjects with normal clinical histories, physical examinations, and resting and exercise stress electrocardiographic assessments. The CAD group included outpatients from the Heart Institute (InCor) with angiographically documented disease (>50% luminal reduction) and patients with a previous myocardial infarct episode. The local institutional review boards approved the study protocol, and written informed consent was obtained from each study participant.
Data collection
The clinical data obtained included age, gender, body mass index (weight [kg]/height [m2]), smoking history, arterial hypertension, diabetes, dyslipidemia, previous myocardial infarction, and family history of premature CAD. Smokers who had quit more than 1 year prior to the study were considered ex-smokers. Current and former smokers were considered as one group and were compared with the patients who had never smoked. Hypertension was defined as a systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg, or both measured at study entry or following antihypertensive treatment. A family history of CAD was defined as obstructive CAD occurring in parents (before age 55 for men and 65 for women) and siblings. Dyslipidemia was considered as the presence of hypercholesterolemia (total cholesterol >6.2 mmol/L) or hypertriglyceridemia (triglycerides >2.87 mmol/L) with medication use (e.g., fibrates and statins). Diabetes was diagnosed when a patient was taking hypoglycemic drugs or exhibited fasting glucose blood levels >7.0 mmol/L. No patients used contraceptives or hormone replacement therapy. Thrombogenic factors (fibrinogen, assessed by the Clauss method; protein C, protein S, and antithrombin III, assessed by chromogenic methods); and atherogenic factors (fasting glucose and lipid profiles, assessed by standard protocols; and lipoprotein (a) and apolipoprotein AI and B fractions, assessed using the immunoturbidimetric method) were determined.
Genotyping
Genomic DNA was extracted from peripheral blood leukocytes by the standard salting-out procedure
(1010. Kistorp C, Raymond I, Pedersen F, Gustafsson F, Faber J, Hildebrandt P, et al.
N-terminal pro-brain natriuretic peptide, C-reactive protein, and urinary albumin levels as
predictors of mortality and cardiovascular events in older adults. JAMA. 2005;293(13):1609-16,
http://dx.doi.org/10.1001/jama.293.13.1609.
http://dx.doi.org/10.1001/jama.293.13.16...
). We studied SNP 252A>G (rs909253) in the LTA gene,
which encodes LTA on Chromosome 6p21 in intron 1 (1111. Zethelius B, Berglund L, Sundström J, Ingelsson E, Basu S, Larsson A, et
al. Use of multiple biomarkers to improve the prediction of death from cardiovascular causes.
N Engl J Med. 2008;358(20):2107-16.). The
genetic variability of LTA was determined by amplification of the genomic DNA using polymerase chain
reaction (PCR) followed by the restriction fragment length polymorphism (RFLP) technique. A 30-cycle
PCR was performed in a PTC-DNA Engine Tetrad2 (MJ Research, Waltham, Massachusetts, USA) using a
10-μL reactive solution containing 10 mM Tris-HCl (pH 9.0), 50 mM KCl, 2.5 mM
MgCl2, 100 μM of each dNTP, 0.3 U of Easy Taq DNA Polymerase, 5 pmol of each
primer, and 1 μL of genomic DNA template. PCR products were digested with 1 U of NcoI
restriction enzyme and visualized using 2.5% agarose gel electrophoresis. The presence of the 782-pb
fragments indicated homozygosis of the wild allele (AA), while the presence of the 586- and 196-pb
products indicated homozygosis of the mutant allele (GG) and the presence of 782-, 586-, and 196-pb
products indicated heterozygosis (AG genotype). Genotype distribution was in Hardy-Weinberg
equilibrium in all study samples (p>0.001).
Statistical methods
The Hardy Weinberg equilibrium for the distribution of genotypes was estimated by the chi-square test in the groups studied (no-CAD and CAD). Chi-square tests, t tests, and analysis of variance with Tukey's correction for multiple comparisons were used for baseline comparisons. The odds ratios for different association models were calculated with a 95% confidence interval (CI) by multiple logistic regressions with confounders determined by a backward conditional elimination method for a significance level below 0.05. Logistic regression was used to estimate the cross-sectional association of the traditional risk factors for CAD with the following independent variables: gender, smoking status, family history of premature CAD, diabetes, dyslipidemia, history of arterial hypertension, Lp(a), and LTA polymorphisms. Lp(a) was dichotomized into normal (<30 mg/dL) and high (≥30 mg/dL) values. CAD was the dependent variable. To evaluate the model's performance, a receiver operating characteristic (ROC) curve was developed, and the area under the ROC curve (AUC or C-statistic) was used to measure the discriminative power. The C-statistic for the clinical model and the biomarker information added to the clinical model were compared. The significance level adopted for the statistical tests was 5% (p<0.05). Statistical analyses were performed using the SAS for Windows (Statistical Analysis System) program, version 9.2 (SAS Institute Inc., 1989-1996, Cary, NC, USA).
RESULTS
Baseline characteristics
The demographic and laboratory characteristics of the study population are shown in Table 1.
Females, smokers, and individuals with hypertension, diabetes, dyslipidemia, and a family history of CAD were significantly more prevalent in the CAD group. Compared with the controls, the CAD patients exhibited significantly lower plasma concentrations of HDL-cholesterol (p<0.001) and higher levels of fasting glucose (p = 0.005), lipoprotein (a) (p<0.001), and protein S (p = 0.038). The genotypic frequency distributions of the LTA A252G polymorphism for A/A homozygotes, A/G heterozygotes, and G/G homozygotes were 47.1%, 42.9, and 10% for all subjects; 55.0%, 37.6%, and 7.4% for the control group; and 42.7%, 46.0%, and 11.3% for the patient group, respectively (p = 0.021). The frequencies of the A and G alleles of the LTA gene were 68.6% and 31.4% among the 524 individuals in the entire population; 73.8% and 26.2% in the controls; and 65.7% and 34.3% in the CAD group, respectively. Genotyping distributions in both the control and CAD groups were consistent with Hardy-Weinberg equilibrium.
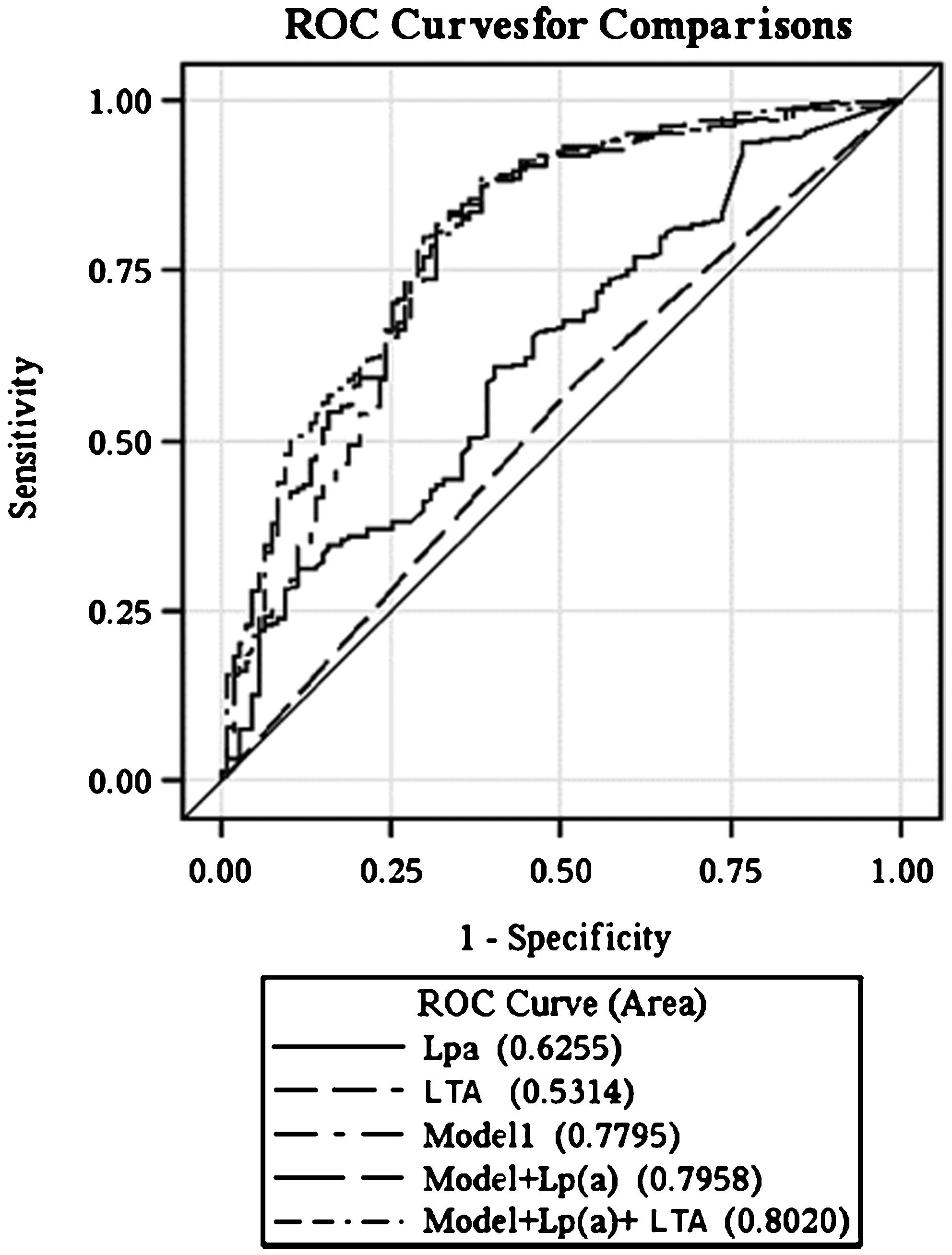
No association was observed between LTA A252G and traditional risk factors. HDL-cholesterol and C-reactive protein plasma levels were higher in the AA (p = 0.038) and GG genotype subjects (p = 0.030), respectively. A multivariate logistic regression analysis showed that smoking (OR 4.81; 95% CI 1.98 - 11.7, p = 0.001), dyslipidemia (OR 2.35; 95% CI 1.10 - 5.05, p = 0.028), family history of CAD (OR 8.20; 95% CI 4.692 - 12.103, p<0.001), and Lp(a) (OR 1.29; 95% CI 1.01 - 1.65, p = 0.042) and LTA (OR 3.38; 95% CI 1.03 - 11.10, p = 0.007) mutations in men, but not in women (OR 1.34; 95% CI 0.49 - 3.63, p = 0.567), were independent factors associated with CAD (Figure 1). The performances of the predictive risk models are shown in the ROC curves (Figure 2). Model1 included the clinical variables gender, hypertension, smoking, diabetes, family history of CAD, dyslipidemia, and body mass index. The AUC (C-statistic) of this model for the prediction of CAD in patients <50 years old was 0.779. There was a progressive increase in the AUC with the inclusion of the Lp(a) and Lp(a) + LTA mutation variables of 0.796 (p = 0.047, for comparisons between model1 and model1+Lp(a)) and 0.802 (p = 0.024, for comparisons between model1 and model1+Lp(a)+LTA mutation).
Predicted probabilities of coronary artery disease based on a multivariate-adjusted model. LTA+ means LTA genotype GG.
Receiver operating characteristic (ROC) curves. Model1 included the following variables: gender, hypertension, smoking, diabetes, family history of CAD, dyslipidemia, and body mass index. Model1 vs. Model1+Lp(a) (p = 0.047); Model1 vs. Model1+Lp(a)+LTA (p = 0.024).
DISCUSSION
Our study shows that Lp(a) and LTA mutations in men are associated with premature CAD. Lp(a) and
LTA mutations exhibit an additive effect on the C-statistic AUC for the traditional risk factors.
Several studies have shown conflicting results regarding the association between specific biomarkers
and the prediction of CAD (2222. Ingelsson E, Schaefer EJ, Contois JH, McNamara JR, Sullivan L, Keyes MJ, et al.
Clinical utility of different lipid measures for prediction of coronary heart disease in men and
women. JAMA. 2007;298(7):776-85, http://dx.doi.org/10.1001/jama.298.7.776.
http://dx.doi.org/10.1001/jama.298.7.776...
23. Ray KK, Cannon CP, Cairns R, Morrow DA, Ridker PM, Braunwald E. Prognostic
utility of apoB/AI, total cholesterol/HDL, non-HDL cholesterol, or hs-CRP as predictors of clinical
risk in patients receiving statin therapy after acute coronary syndromes: results from PROVE IT-TIMI
22. Arterioscler Thromb Vasc Biol. 2009;29(3):424-430,
http://dx.doi.org/10.1161/ATVBAHA.108.181735.
http://dx.doi.org/10.1161/ATVBAHA.108.18...
24. Sierra-Johnson J, Fisher RM, Romero-Corral A, Somers VK, Lopez-Jimenez F, Ohrvik
J, et al. Concentration of apolipoprotein B is comparable with the apolipoprotein B/apolipoprotein
A-I ratio and better than routine clinical lipid measurements in predicting coronary heart disease
mortality: findings from a multi-ethnic US population. Eur Heart J.
2009;3096:710-7.
25. Wang TJ, Gona P, Larson MG, Tofler GH, Levy D, Newton-Cheh C, et al. Multiple
biomarkers for the prediction of first major cardiovascular events and death.
N Engl J Med. 2006;355(25):2631-9.
26. Zethelius B, Berglund L, Sundström J, Ingelsson E, Basu S, Larsson A, et
al. Use of multiple biomarkers to improve the prediction of death from cardiovascular causes.
N Engl J Med. 2008;358(20):2107-16.-2727. Shlipak MG, Ix JH, Bibbins-Domingo K, Lin F, Whooley MA. Biomarkers to predict
recurrent cardiovascular disease: the Heart and Soul Study. Am J Med.
2008;121(1):50-7.).
Lipoprotein (a) and risk prediction for CAD
In a nested case-control study, Kim et al. (2828. Kim HC, Greenland P, Rossouw JE, Manson JE, Cochrane BB, Lasser NL, et al.
Multimarker prediction of coronary heart disease risk: the Women's Health Initiative. J Am
Coll Cardiol. 2010;55(19):2080-91, http://dx.doi.org/10.1016/j.jacc.2009.12.047.
http://dx.doi.org/10.1016/j.jacc.2009.12...
) analyzed
18 biomarkers previously associated with CAD in 321 patients with CAD and 743 control postmenopausal
women. Five (vWF, factor VIII, homocysteine, IL-6, and D-dimer) of the 18 biomarkers tested were
associated with CAD, but only D-dimer improved the C-statistic compared with traditional risk
factors. Contrary to our results, Lp(a) was not associated with CAD, but the previous study included
only women who were older (aged between 50 and 79 years) than our patients. Blakenberg et al. (2929. Blankenberg S, Zeller T, Saarela O, Havulinna AS, Kee F, Tunstall-Pedoe H, et
al. Contribution of 30 biomarkers to 10-year cardiovascular risk estimation in 2 population cohorts:
the MONICA, risk, genetics, archiving, and monograph (MORGAM) biomarker project. Circulation.
2010;121(22):2388-97, http://dx.doi.org/10.1161/CIRCULATIONAHA.109.901413.
http://dx.doi.org/10.1161/CIRCULATIONAHA...
) analyzed the risk prediction of CAD associated with 30
biomarkers in 2 middle-aged European populations. The study analyzed Lp(a) and other biomarkers and
showed that no biomarker improved risk estimation in either population. The structure of lipoprotein
(a) is similar to the structure of LDL cholesterol, which includes one additional plasminogen-like
glycoprotein, namely apolipoprotein (a). Due to these characteristics, this particle may contribute
to the processes of atherogenesis and thrombogenesis. Lp(a) studies showed conflicting results
regarding the risk prediction of CAD (3030. Erqou S, Kaptoge S, Perry PL, Di Angelantonio E, Thompson A, White IR, et al.
Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular
mortality. JAMA. 2009;302(4):412-23.
31. Bennet A, Di Angelantonio E, Erqou S, Eiriksdottir G, Sigurdsson G, Woodward M,
et al. Lipoprotein(a) levels and risk of future coronary heart disease: large-scale prospective
data. Arch Intern Med. 2008;168(6):598-608,
http://dx.doi.org/10.1001/archinte.168.6.598.
http://dx.doi.org/10.1001/archinte.168.6...
32. Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, Ray KK, Thompson A, et al.
Major lipids, apolipoproteins, and risk of vascular disease. JAMA.
2009;302(18):1993-2000.
33. Virani SS, Brautbar A, Davis BC, Nambi V, Hoogeveen RC, Sharrett AR, et al.
Associations between lipoprotein(a) levels and cardiovascular outcomes in black and white subjects:
the Atherosclerosis Risk in Communities (ARIC) Study. Circulation. 2012;125(2):241-9,
http://dx.doi.org/10.1161/CIRCULATIONAHA.111.045120.
http://dx.doi.org/10.1161/CIRCULATIONAHA...
-3434. Sawabe M, Tanaka N, Mieno MN, Ishikawa S, Kayaba K, Nakahara K, et al. Low
lipoprotein(a) concentration is associated with cancer and all-cause deaths: a population-based
cohort study (the JMS cohort study). PLoS One. 2012;7(4):e31954,
http://dx.doi.org/10.1371/journal.pone.0031954.
http://dx.doi.org/10.1371/journal.pone.0...
). Bennet et al. (3131. Bennet A, Di Angelantonio E, Erqou S, Eiriksdottir G, Sigurdsson G, Woodward M,
et al. Lipoprotein(a) levels and risk of future coronary heart disease: large-scale prospective
data. Arch Intern Med. 2008;168(6):598-608,
http://dx.doi.org/10.1001/archinte.168.6.598.
http://dx.doi.org/10.1001/archinte.168.6...
)
showed that the odds ratios for CAD were progressively higher with increasing Lp(a) levels in a
large, prospective, population-based cohort that was adjusted for several established risk factors.
Virani et al. (3333. Virani SS, Brautbar A, Davis BC, Nambi V, Hoogeveen RC, Sharrett AR, et al.
Associations between lipoprotein(a) levels and cardiovascular outcomes in black and white subjects:
the Atherosclerosis Risk in Communities (ARIC) Study. Circulation. 2012;125(2):241-9,
http://dx.doi.org/10.1161/CIRCULATIONAHA.111.045120.
http://dx.doi.org/10.1161/CIRCULATIONAHA...
) also showed that Lp(a) levels are
associated with an increased risk of cardiovascular diseases in both African American and Caucasian
male and female subjects. Sawage et al. (3434. Sawabe M, Tanaka N, Mieno MN, Ishikawa S, Kayaba K, Nakahara K, et al. Low
lipoprotein(a) concentration is associated with cancer and all-cause deaths: a population-based
cohort study (the JMS cohort study). PLoS One. 2012;7(4):e31954,
http://dx.doi.org/10.1371/journal.pone.0031954.
http://dx.doi.org/10.1371/journal.pone.0...
) demonstrated an
association between low Lp(a) levels and all-cause or cancer deaths and similar outcomes for low and
high Lp(a) levels for cardiovascular deaths.
Use of genetic markers in risk prediction for CAD
Few studies have utilized genetic markers of CAD in risk prediction. Rossouw et al. (3535. Rossouw JE, Cushman M, Greenland P, Lloyd-Jones DM, Bray P, Kooperberg C, et al.
Inflammatory, lipid, thrombotic, and genetic markers of coronary heart disease risk in the
women's health initiative trials of hormone therapy. Arch Intern Med. 2008;168(20):2245-53,
http://dx.doi.org/10.1001/archinte.168.20.2245.
http://dx.doi.org/10.1001/archinte.168.2...
) analyzed 23 inflammatory, lipid, and thrombotic biomarkers and
8 genetic polymorphisms in postmenopausal women (aged 50-79 years) receiving hormone replacement
therapy in a nested case-control study. Of the 23 biomarkers, the following 13 were associated with
CHD events: interleukin 6, matrix metalloproteinase 9, HDL-C, LDL-C, total cholesterol,
triglycerides, D-dimer, factor VIII, von Willebrand factor, leukocyte count, homocysteine, fasting
insulin, and 1 genetic polymorphism (the glycoprotein IIIa leu33pro mutation). Additive risk
prediction of the biomarkers over the conventional risk factors was not performed. Ripatti et al.
(3636. Ripatti S, Tikkanen E, Orho-Melander M, Havulinna AS, Silander K, Sharma A, et
al. A multilocus genetic risk score for coronary heart disease: case-control and prospective cohort
analyses. Lancet. 2010;376(9750):1393-400,
http://dx.doi.org/10.1016/S0140-6736(10)61267-6.
http://dx.doi.org/10.1016/S0140-6736(10)...
) calculated a genetic risk score based on 13 SNPs and
observed an association with a first coronary heart disease event, but the genetic risk score did
not improve risk prediction compared with risk prediction based on traditional risk factors and
family history. Paynter et al. (3737. Paynter NP, Chasman DI, Paré G, Buring JE, Cook NR, Miletich JP, et al.
Association between a literature-based genetic risk score and cardiovascular events in women. JAMA.
2010;303(7):631-7, http://dx.doi.org/10.1001/jama.2010.119.
http://dx.doi.org/10.1001/jama.2010.119...
) calculated a genetic risk
score based on 101 SNPs in 19,313 healthy Caucasian women who were followed up over a median of 12.3
years in a prospective study. After adjustment for traditional cardiovascular risk factors, the
genetic risk score was not associated with cardiovascular disease risk. The LTA gene mutation was
not included in the genetic risk score of the two previous studies. Thanassoulis et al. (3838. Thanassoulis G, Peloso GM, Pencina MJ, Hoffmann U, Fox CS, Cupples LA, et al. A
genetic risk score is associated with incident cardiovascular disease and coronary artery calcium:
the Framingham Heart Study. Circ Cardiovasc Genet. 2012;5(1):113-21,
http://dx.doi.org/10.1161/CIRCGENETICS.111.961342.
http://dx.doi.org/10.1161/CIRCGENETICS.1...
) showed a marginal increase in the risk prediction of
cardiovascular events with the genetic risk score in addition to standard cardiovascular risk
factors and a high risk of coronary artery calcium. However, future studies evaluating the utility
of coronary artery calcium and genetic risk scores in predicting lifetime risk are needed.
Genome-wide single nucleotide polymorphism association studies have identified several SNPs that are
significantly associated with CAD and with traditional risk factors for CAD (3939. Samani NJ, Erdmann J, Hall AS, Hengstenberg C, Mangino M, Mayer B, et al. WTCCC
and the Cardiogenics Consortium. Genomewide association analysis of coronary artery disease.
N Engl J Med. 2007;357(5):443-53.
40. Sandhu MS, Waterworth DM, Debenham SL, Wheeler E, Papadakis K, Zhao JH, et al.
LDL-cholesterol concentrations: a genome-wide association study. Lancet. 2008;371(9611):483-91,
http://dx.doi.org/10.1016/S0140-6736(08)60208-1.
http://dx.doi.org/10.1016/S0140-6736(08)...
41. Wang AZ, Li L, Zhang B, Shen GQ, Wang QK. Association of SNP rs17465637 on
chromosome 1q41 and rs599839 on 1p13.3 with myocardial infarction in an American caucasian
population. Ann Hum Genet. 2011;75(4):475-82,
http://dx.doi.org/10.1111/j.1469-1809.2011.00646.x.
http://dx.doi.org/10.1111/j.1469-1809.20...
-4242. Angelakopoulou A, Shah T, Sofat R, Shah S, Berry DJ, Cooper J, et al.
Comparative analysis of genome-wide association studies signals for lipids, diabetes, and coronary
heart disease: Cardiovascular Biomarker Genetics Collaboration. Eur Heart J.
2012;33(3):393-407, http://dx.doi.org/10.1093/eurheartj/ehr225.
http://dx.doi.org/10.1093/eurheartj/ehr2...
). However, the results of all these
studies still showed inconsistencies with regard to the presence of a causal relationship between
biomarkers, with or without the inclusion of genetic markers, and CAD and traditional risk factors.
A mechanistic basis for the association between SNPs and coronary heart disease was observed,
although the atherosclerotic process was unknown (4343. McPherson R, Pertsemlidis A, Kavaslar N, Stewart A, Roberts R, Cox DR, et al. A
common allele on chromosome 9 associated with coronary heart disease. Science.
2007;316(5830):1488-91, http://dx.doi.org/10.1126/science.1142447.
http://dx.doi.org/10.1126/science.114244...
).
However, none of the previously mentioned studies analyzed multiple biomarkers for the prediction of
CAD in young adults aged <50 years.
In this study, we analyzed several biomarkers related to thrombogenic and atherogenic processes,
and we included the LTA mutation as a candidate gene approach to risk assessment. The LTA mutation
was frequently associated with CAD. In our study, the presence of the LTA gene mutant allele
provided incremental information about CAD risk prediction. Previous case-control and
cross-sectional studies examined the association between LTA gene polymorphisms and cardiovascular
disease, but the results were inconsistent. The study by Ozaki et al. (1717. Ozaki K, Inoue K, Sato H, Iida A, Ohnishi Y, Sekine A, et al. Functional
variation in LGALS2 confers risk of myocardial infarction and regulates lymphotoxin-alpha secretion
in vitro. Nature. 2004;429(6987):72-5, http://dx.doi.org/10.1038/nature02502.
http://dx.doi.org/10.1038/nature02502...
) described significant associations between LTA gene polymorphisms and
myocardial infarction; however, the authors did not adjust for relevant covariates, including gender
and age, and the genotype distributions among the control subjects were not in Hardy-Weinberg
equilibrium. The association between LTA gene polymorphisms and CHD was confirmed in another
Japanese population and in the family-based European PROCARDIS (precocious coronary artery disease)
study (4444. PROCARDIS Consortium. A trio family study showing association of the
lymphotoxin-alpha N26 (804A) allele with coronary artery disease. Eur J Hum Genet.
2004;12(9):770-4.). A significant association was observed between
the LTA C804A genotype and the extent of coronary atherosclerosis in Caucasian patients with
angiographically confirmed coronary atherosclerosis (4545. Laxton R, Pearce E, Kyriakou T, Ye S. Association of the lymphotoxinalpha gene
Thr26Asn polymorphism with severity of coronary atherosclerosis. Genes Immunol. 2005;6(6):539-41,
http://dx.doi.org/10.1038/sj.gene.6364236.
http://dx.doi.org/10.1038/sj.gene.636423...
).
However, several other studies did not detect an association between LTA gene polymorphisms and
myocardial infarction (1010. Kistorp C, Raymond I, Pedersen F, Gustafsson F, Faber J, Hildebrandt P, et al.
N-terminal pro-brain natriuretic peptide, C-reactive protein, and urinary albumin levels as
predictors of mortality and cardiovascular events in older adults. JAMA. 2005;293(13):1609-16,
http://dx.doi.org/10.1001/jama.293.13.1609.
http://dx.doi.org/10.1001/jama.293.13.16...
,1414. Pober JS, Lapierre LA, Stolpen AH, Brock TA, Springer TA, Fiers W, et al.
Activation of cultured human endothelial cells by recombinant lymphotoxin: comparison with tumor
necrosis factor and interleukin 1 species. J Immunol. 1987;138(10):3319-24.,1515. Cavender DE, Edelbaum D, Ziff M. Endothelial cell activation induced by tumor
necrosis factor and lymphotoxin. Am J Pathol. 1989;134(3):551-60.). A meta-analysis performed by Clarke et al.
(4646. Clarke R, Xu P, Bennett D, Lewington S, Zondervan K, Parish S, et al.
International Study of Infarct Survival (ISIS) Collaborators. Lymphotoxin-alpha gene and risk of
myocardial infarction in 6,928 cases and 2,712 controls in the ISIS case-control study. PLoS Genet.
2006;2(7):e107, http://dx.doi.org/10.1371/journal.pgen.0020107.) also showed no relationship between LTA gene
polymorphisms and CHD. However, they did not study the LTA gene polymorphism (rs909253) evaluated in
the Japanese study and our study. The most straightforward explanation for the findings of our study
may be associated with the genetic differences of studied populations. Among populations with
similar genetic backgrounds, the differences in allele frequency make it difficult to extrapolate
genetic findings from one population to another. In our population, we demonstrated an association
between LTA gene polymorphisms and increased risk of well-documented stable CAD in younger patients
aged <50 years. Genetic diversity in different populations may be especially relevant to the
LTA genomic region, which lies within the HLA region and has an erratic pattern of LD structure,
with both short LD islands and long-range haplotypes (4747. Palikhe A, Sinisalo J, Seppnen M, Valtonen V, Nieminen MS, Lokki ML. Human MHC
region harbors both susceptibility and protective haplotypes for coronary artery disease. Tissue
Antigens. 2007;69(1):47-55, http://dx.doi.org/10.1111/j.1399-0039.2006.00735.x.
http://dx.doi.org/10.1111/j.1399-0039.20...
). In
our study, Lp(a) and LTA mutations alone were associated with lower risk prediction for CAD compared
with conventional risk factors, but the inclusion of each mutation with conventional risk factors
resulted in a progressive and statistically significant increase in risk prediction for CAD (Figure 2). The impact of the increased risk prediction based on
AUC/C-statistics from 0.779 to 0.802 in clinical practice is uncertain and needs to be confirmed in
future studies.
Study limitations
Our study has several limitations. This was a case-control study, and in such studies, casual associations are frequent when the sample size is relatively small for the association analysis of complex diseases with genetic mutations of multifactorial traits. Additionally, this case-control study was age-matched but not gender-matched. Therefore, the clinical and laboratory features observed more often in women may have influenced the final results. The analysis of one mutation can lead to results not identified in prospective studies with a larger number of individuals. The analysis of a significantly higher number of mutations, use of better laboratory techniques, and application of more sophisticated statistical models improved the genetic risk prediction for CAD. This study examined a significant number of atherogenic and thrombogenic markers in patients with premature CAD, but the markers represent a small portion of those involved in the atherosclerosis process. The complex interaction between genetic factors and the environment, including the impact of current medications on the treatment of CAD, may have further influenced the data interpretation.
Traditional risk factors played a strong role in risk prediction for the onset of premature coronary atherosclerosis in our population. The inclusion of Lp(a) and LTA mutations in the set of conventional risk factors showed an additive but small increase in the risk prediction for premature CAD.
Financial support was provided by “Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP)” number 01/06632-1.
REFERENCES
-
1Wang Q. Molecular genetics of coronary artery disease. Curr Opin Cardiol. 2005;20(3):182-8, http://dx.doi.org/10.1097/01.hco.0000160373.77190.f1.
» http://dx.doi.org/10.1097/01.hco.0000160373.77190.f1 -
2Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2010;122(25):2748-64.
-
3Peden JF, Farrall M. Thirty-five common variants for coronary artery disease: the fruits of much collaborative labour. Hum Mol Genet. 2011;20(R2):R198-R205, http://dx.doi.org/10.1093/hmg/ddr384.
» http://dx.doi.org/10.1093/hmg/ddr384 -
4Ross R. Atherosclerosis an inflammatory disease. N Engl J Med. 1999;340(2):115-26.
-
5Weber C, Noels H. Atherosclerosis: current pathogenesis and therapeutic options. Nat Med. 2011;17(11):1410-22, http://dx.doi.org/10.1038/nm.2538.
» http://dx.doi.org/10.1038/nm.2538 -
6Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Rumberger J, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation. 2003;108(14):1664-72, http://dx.doi.org/10.1161/01.CIR.0000087480.94275.97.
» http://dx.doi.org/10.1161/01.CIR.0000087480.94275.97 -
7Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Rumberger J, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part II. Circulation. 2003;108(15):1772-8, http://dx.doi.org/10.1161/01.CIR.0000087481.55887.C9.
» http://dx.doi.org/10.1161/01.CIR.0000087481.55887.C9 -
8Sposito AC, Alvarenga BF, Alexandre AS, Araújo AL, Santos SN, Andrade JM, et al. Most of the patients presenting myocardial infarction would not be eligible for intensive lipid-lowering based on clinical algorithms or plasma C reactive protein. Atherosclerosis. 2011;214(1):148-50, http://dx.doi.org/10.1016/j.atherosclerosis.2010.10.034.
» http://dx.doi.org/10.1016/j.atherosclerosis.2010.10.034 -
9Lloyd-Jones DM, Wilson PW, Larson MG, Beiser A, Leip EP, D'Agostino RB, et al. Framingham risk score and prediction of lifetime risk for coronary heart disease. Am J Cardiol. 2004;94(1):20-4, http://dx.doi.org/10.1016/j.amjcard.2004.03.023.
» http://dx.doi.org/10.1016/j.amjcard.2004.03.023 -
10Kistorp C, Raymond I, Pedersen F, Gustafsson F, Faber J, Hildebrandt P, et al. N-terminal pro-brain natriuretic peptide, C-reactive protein, and urinary albumin levels as predictors of mortality and cardiovascular events in older adults. JAMA. 2005;293(13):1609-16, http://dx.doi.org/10.1001/jama.293.13.1609.
» http://dx.doi.org/10.1001/jama.293.13.1609 -
11Zethelius B, Berglund L, Sundström J, Ingelsson E, Basu S, Larsson A, et al. Use of multiple biomarkers to improve the prediction of death from cardiovascular causes. N Engl J Med. 2008;358(20):2107-16.
-
12Brown TM, Bittner V. Biomarkers of atherosclerosis: clinical applications. Curr Cardiol Rep. 2008;10(6):497-504, http://dx.doi.org/10.1007/s11886-008-0078-1.
» http://dx.doi.org/10.1007/s11886-008-0078-1 -
13Roberts R, Stewart AF. The genetics of coronary artery disease. Curr Opin Cardiol. 2012;27(3):221-7, http://dx.doi.org/10.1097/HCO.0b013e3283515b4b.
» http://dx.doi.org/10.1097/HCO.0b013e3283515b4b -
14Pober JS, Lapierre LA, Stolpen AH, Brock TA, Springer TA, Fiers W, et al. Activation of cultured human endothelial cells by recombinant lymphotoxin: comparison with tumor necrosis factor and interleukin 1 species. J Immunol. 1987;138(10):3319-24.
-
15Cavender DE, Edelbaum D, Ziff M. Endothelial cell activation induced by tumor necrosis factor and lymphotoxin. Am J Pathol. 1989;134(3):551-60.
-
16Kratz A, Campos-Neto A, Hanson MS, Ruddle NH. Chronic inflammation caused by lymphotoxin is lymphoid neogenesis. J Exp Med 1996;183(4):1461-72, http://dx.doi.org/10.1084/jem.183.4.1461.
» http://dx.doi.org/10.1084/jem.183.4.1461 -
17Ozaki K, Inoue K, Sato H, Iida A, Ohnishi Y, Sekine A, et al. Functional variation in LGALS2 confers risk of myocardial infarction and regulates lymphotoxin-alpha secretion in vitro. Nature. 2004;429(6987):72-5, http://dx.doi.org/10.1038/nature02502.
» http://dx.doi.org/10.1038/nature02502 -
18Ozaki K, Ohnishi Y, Iida A, Sekine A, Yamada R, Tsunoda T, et al. Functional SNPs in the lymphotoxin-alpha gene that are associated with susceptibility to myocardial infarction. Nat Genet. 2002;32(4):650-4, http://dx.doi.org/10.1038/ng1047.
» http://dx.doi.org/10.1038/ng1047 -
19Ozaki K, Tanaka T. Genome-wide association study to identify SNPs conferring risk of myocardial infarction and their functional analyses. Cell Mol Life Sci. 2005;62(16):1804-13, http://dx.doi.org/10.1007/s00018-005-5098-z.
» http://dx.doi.org/10.1007/s00018-005-5098-z -
20Li W, Xu J, Wang X, Chen J, Zhang C, Sun K, et al. Lack of association between lymphotoxin-alpha, galectin-2 polymorphisms and coronary artery disease: a meta-analysis. Atherosclerosis. 2010;208(2):433-6, http://dx.doi.org/10.1016/j.atherosclerosis.2009.08.014.
» http://dx.doi.org/10.1016/j.atherosclerosis.2009.08.014 -
21Ryan AW, O'Brien E, Shields D, McManus R. Lack of association between NFKBIL1/LTA polymorphisms and hypertension, myocardial infarct, unstable angina and stable angina in a large Irish population sample. Atherosclerosis. 2008;197(1):465-466, http://dx.doi.org/10.1016/j.atherosclerosis.2007.03.032.
» http://dx.doi.org/10.1016/j.atherosclerosis.2007.03.032 -
22Ingelsson E, Schaefer EJ, Contois JH, McNamara JR, Sullivan L, Keyes MJ, et al. Clinical utility of different lipid measures for prediction of coronary heart disease in men and women. JAMA. 2007;298(7):776-85, http://dx.doi.org/10.1001/jama.298.7.776.
» http://dx.doi.org/10.1001/jama.298.7.776 -
23Ray KK, Cannon CP, Cairns R, Morrow DA, Ridker PM, Braunwald E. Prognostic utility of apoB/AI, total cholesterol/HDL, non-HDL cholesterol, or hs-CRP as predictors of clinical risk in patients receiving statin therapy after acute coronary syndromes: results from PROVE IT-TIMI 22. Arterioscler Thromb Vasc Biol. 2009;29(3):424-430, http://dx.doi.org/10.1161/ATVBAHA.108.181735.
» http://dx.doi.org/10.1161/ATVBAHA.108.181735 -
24Sierra-Johnson J, Fisher RM, Romero-Corral A, Somers VK, Lopez-Jimenez F, Ohrvik J, et al. Concentration of apolipoprotein B is comparable with the apolipoprotein B/apolipoprotein A-I ratio and better than routine clinical lipid measurements in predicting coronary heart disease mortality: findings from a multi-ethnic US population. Eur Heart J. 2009;3096:710-7.
-
25Wang TJ, Gona P, Larson MG, Tofler GH, Levy D, Newton-Cheh C, et al. Multiple biomarkers for the prediction of first major cardiovascular events and death. N Engl J Med. 2006;355(25):2631-9.
-
26Zethelius B, Berglund L, Sundström J, Ingelsson E, Basu S, Larsson A, et al. Use of multiple biomarkers to improve the prediction of death from cardiovascular causes. N Engl J Med. 2008;358(20):2107-16.
-
27Shlipak MG, Ix JH, Bibbins-Domingo K, Lin F, Whooley MA. Biomarkers to predict recurrent cardiovascular disease: the Heart and Soul Study. Am J Med. 2008;121(1):50-7.
-
28Kim HC, Greenland P, Rossouw JE, Manson JE, Cochrane BB, Lasser NL, et al. Multimarker prediction of coronary heart disease risk: the Women's Health Initiative. J Am Coll Cardiol. 2010;55(19):2080-91, http://dx.doi.org/10.1016/j.jacc.2009.12.047.
» http://dx.doi.org/10.1016/j.jacc.2009.12.047 -
29Blankenberg S, Zeller T, Saarela O, Havulinna AS, Kee F, Tunstall-Pedoe H, et al. Contribution of 30 biomarkers to 10-year cardiovascular risk estimation in 2 population cohorts: the MONICA, risk, genetics, archiving, and monograph (MORGAM) biomarker project. Circulation. 2010;121(22):2388-97, http://dx.doi.org/10.1161/CIRCULATIONAHA.109.901413.
» http://dx.doi.org/10.1161/CIRCULATIONAHA.109.901413 -
30Erqou S, Kaptoge S, Perry PL, Di Angelantonio E, Thompson A, White IR, et al. Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular mortality. JAMA. 2009;302(4):412-23.
-
31Bennet A, Di Angelantonio E, Erqou S, Eiriksdottir G, Sigurdsson G, Woodward M, et al. Lipoprotein(a) levels and risk of future coronary heart disease: large-scale prospective data. Arch Intern Med. 2008;168(6):598-608, http://dx.doi.org/10.1001/archinte.168.6.598.
» http://dx.doi.org/10.1001/archinte.168.6.598 -
32Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, Ray KK, Thompson A, et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009;302(18):1993-2000.
-
33Virani SS, Brautbar A, Davis BC, Nambi V, Hoogeveen RC, Sharrett AR, et al. Associations between lipoprotein(a) levels and cardiovascular outcomes in black and white subjects: the Atherosclerosis Risk in Communities (ARIC) Study. Circulation. 2012;125(2):241-9, http://dx.doi.org/10.1161/CIRCULATIONAHA.111.045120.
» http://dx.doi.org/10.1161/CIRCULATIONAHA.111.045120 -
34Sawabe M, Tanaka N, Mieno MN, Ishikawa S, Kayaba K, Nakahara K, et al. Low lipoprotein(a) concentration is associated with cancer and all-cause deaths: a population-based cohort study (the JMS cohort study). PLoS One. 2012;7(4):e31954, http://dx.doi.org/10.1371/journal.pone.0031954.
» http://dx.doi.org/10.1371/journal.pone.0031954 -
35Rossouw JE, Cushman M, Greenland P, Lloyd-Jones DM, Bray P, Kooperberg C, et al. Inflammatory, lipid, thrombotic, and genetic markers of coronary heart disease risk in the women's health initiative trials of hormone therapy. Arch Intern Med. 2008;168(20):2245-53, http://dx.doi.org/10.1001/archinte.168.20.2245.
» http://dx.doi.org/10.1001/archinte.168.20.2245 -
36Ripatti S, Tikkanen E, Orho-Melander M, Havulinna AS, Silander K, Sharma A, et al. A multilocus genetic risk score for coronary heart disease: case-control and prospective cohort analyses. Lancet. 2010;376(9750):1393-400, http://dx.doi.org/10.1016/S0140-6736(10)61267-6.
» http://dx.doi.org/10.1016/S0140-6736(10)61267-6 -
37Paynter NP, Chasman DI, Paré G, Buring JE, Cook NR, Miletich JP, et al. Association between a literature-based genetic risk score and cardiovascular events in women. JAMA. 2010;303(7):631-7, http://dx.doi.org/10.1001/jama.2010.119.
» http://dx.doi.org/10.1001/jama.2010.119 -
38Thanassoulis G, Peloso GM, Pencina MJ, Hoffmann U, Fox CS, Cupples LA, et al. A genetic risk score is associated with incident cardiovascular disease and coronary artery calcium: the Framingham Heart Study. Circ Cardiovasc Genet. 2012;5(1):113-21, http://dx.doi.org/10.1161/CIRCGENETICS.111.961342.
» http://dx.doi.org/10.1161/CIRCGENETICS.111.961342 -
39Samani NJ, Erdmann J, Hall AS, Hengstenberg C, Mangino M, Mayer B, et al. WTCCC and the Cardiogenics Consortium. Genomewide association analysis of coronary artery disease. N Engl J Med. 2007;357(5):443-53.
-
40Sandhu MS, Waterworth DM, Debenham SL, Wheeler E, Papadakis K, Zhao JH, et al. LDL-cholesterol concentrations: a genome-wide association study. Lancet. 2008;371(9611):483-91, http://dx.doi.org/10.1016/S0140-6736(08)60208-1.
» http://dx.doi.org/10.1016/S0140-6736(08)60208-1 -
41Wang AZ, Li L, Zhang B, Shen GQ, Wang QK. Association of SNP rs17465637 on chromosome 1q41 and rs599839 on 1p13.3 with myocardial infarction in an American caucasian population. Ann Hum Genet. 2011;75(4):475-82, http://dx.doi.org/10.1111/j.1469-1809.2011.00646.x.
» http://dx.doi.org/10.1111/j.1469-1809.2011.00646.x -
42Angelakopoulou A, Shah T, Sofat R, Shah S, Berry DJ, Cooper J, et al. Comparative analysis of genome-wide association studies signals for lipids, diabetes, and coronary heart disease: Cardiovascular Biomarker Genetics Collaboration. Eur Heart J. 2012;33(3):393-407, http://dx.doi.org/10.1093/eurheartj/ehr225.
» http://dx.doi.org/10.1093/eurheartj/ehr225 -
43McPherson R, Pertsemlidis A, Kavaslar N, Stewart A, Roberts R, Cox DR, et al. A common allele on chromosome 9 associated with coronary heart disease. Science. 2007;316(5830):1488-91, http://dx.doi.org/10.1126/science.1142447.
» http://dx.doi.org/10.1126/science.1142447 -
44PROCARDIS Consortium. A trio family study showing association of the lymphotoxin-alpha N26 (804A) allele with coronary artery disease. Eur J Hum Genet. 2004;12(9):770-4.
-
45Laxton R, Pearce E, Kyriakou T, Ye S. Association of the lymphotoxinalpha gene Thr26Asn polymorphism with severity of coronary atherosclerosis. Genes Immunol. 2005;6(6):539-41, http://dx.doi.org/10.1038/sj.gene.6364236.
» http://dx.doi.org/10.1038/sj.gene.6364236 -
46Clarke R, Xu P, Bennett D, Lewington S, Zondervan K, Parish S, et al. International Study of Infarct Survival (ISIS) Collaborators. Lymphotoxin-alpha gene and risk of myocardial infarction in 6,928 cases and 2,712 controls in the ISIS case-control study. PLoS Genet. 2006;2(7):e107, http://dx.doi.org/10.1371/journal.pgen.0020107.
-
47Palikhe A, Sinisalo J, Seppnen M, Valtonen V, Nieminen MS, Lokki ML. Human MHC region harbors both susceptibility and protective haplotypes for coronary artery disease. Tissue Antigens. 2007;69(1):47-55, http://dx.doi.org/10.1111/j.1399-0039.2006.00735.x.
» http://dx.doi.org/10.1111/j.1399-0039.2006.00735.x
-
No potential conflict of interest was reported.
Publication Dates
-
Publication in this collection
Dec 2013
History
-
Received
15 May 2013 -
Reviewed
4 June 2013 -
Accepted
15 June 2013