Abstracts
Cerebral hemiatrophy or Dyke-Davidoff-Masson syndrome is a condition characterized by seizures, facial asymmetry, contralateral hemiplegia or hemiparesis, and mental retardation. These findings are due to cerebral injury that may occur early in life or in utero. The radiological features are unilateral loss of cerebral volume and associated compensatory bone alterations in the calvarium, like thickening, hyperpneumatization of the paranasal sinuses and mastoid cells and elevation of the petrous ridge. The authors describe three cases. Classical findings of the syndrome are present in variable degrees according to the extent of the brain injury. Pathogenesis is commented.
Dyke-Davidoff-Masson syndrome; brain atrophy; computerized tomography; magnetic resonance image
Hemiatrofia cerebral ou síndrome de Dyke-Davidoff-Masson é entidade clínica caracterizada por convulsões, assimetria facial , hemiparesia ou hemiplegia contralateral e déficit cognitivo. Estes achados estão relacionados a lesão cerebral ocorrida na infância ou in utero. As características radiológicas são hemiatrofia cerebral e alteracões ósseas no crânio, como espessamento, hiperpneumatização dos seios paranasais e células da mastóide e elevação do ápice da pirâmide petrosa. Descrevemos três casos com achados clássicos da síndrome discutindo aspectos fisiopatológicos.
síndrome de Dyke-Davidoff-Masson; atrofia cerebral; tomografia computadorizada; ressonância magnética
MR AND CT IMAGING IN THE DYKE-DAVIDOFF-MASSON SYNDROME
REPORT OF THREE CASES AND CONTRIBUTION TO PATHOGENESIS AND DIFFERENTIAL DIAGNOSIS
PAULO HENRIQUE AGUIAR * * Division of Neurosurgery, Department of Neurology of Hospital das Clínicas, University of São Paulo Medical School, São Paulo, Brazil; ** Department of Radiology, Rebouças Tomography Unit, São Paulo, Brazil. Aceite: 11-setembro-1998. , CHING WEI LIU ** * Division of Neurosurgery, Department of Neurology of Hospital das Clínicas, University of São Paulo Medical School, São Paulo, Brazil; ** Department of Radiology, Rebouças Tomography Unit, São Paulo, Brazil. Aceite: 11-setembro-1998. , HELIO LEITÃO ** * Division of Neurosurgery, Department of Neurology of Hospital das Clínicas, University of São Paulo Medical School, São Paulo, Brazil; ** Department of Radiology, Rebouças Tomography Unit, São Paulo, Brazil. Aceite: 11-setembro-1998. , F. ISSA * * Division of Neurosurgery, Department of Neurology of Hospital das Clínicas, University of São Paulo Medical School, São Paulo, Brazil; ** Department of Radiology, Rebouças Tomography Unit, São Paulo, Brazil. Aceite: 11-setembro-1998. , GUILHERME LEPSKI * * Division of Neurosurgery, Department of Neurology of Hospital das Clínicas, University of São Paulo Medical School, São Paulo, Brazil; ** Department of Radiology, Rebouças Tomography Unit, São Paulo, Brazil. Aceite: 11-setembro-1998. , EBERVAL GADELHA FIGUEIREDO* * Division of Neurosurgery, Department of Neurology of Hospital das Clínicas, University of São Paulo Medical School, São Paulo, Brazil; ** Department of Radiology, Rebouças Tomography Unit, São Paulo, Brazil. Aceite: 11-setembro-1998. , FERNANDO GOMES - PINTO * * Division of Neurosurgery, Department of Neurology of Hospital das Clínicas, University of São Paulo Medical School, São Paulo, Brazil; ** Department of Radiology, Rebouças Tomography Unit, São Paulo, Brazil. Aceite: 11-setembro-1998. , RAUL MARINO JR * * Division of Neurosurgery, Department of Neurology of Hospital das Clínicas, University of São Paulo Medical School, São Paulo, Brazil; ** Department of Radiology, Rebouças Tomography Unit, São Paulo, Brazil. Aceite: 11-setembro-1998.
ABSTRACT - Cerebral hemiatrophy or Dyke-Davidoff-Masson syndrome is a condition characterized by seizures, facial asymmetry, contralateral hemiplegia or hemiparesis, and mental retardation. These findings are due to cerebral injury that may occur early in life or in utero. The radiological features are unilateral loss of cerebral volume and associated compensatory bone alterations in the calvarium, like thickening, hyperpneumatization of the paranasal sinuses and mastoid cells and elevation of the petrous ridge. The authors describe three cases. Classical findings of the syndrome are present in variable degrees according to the extent of the brain injury. Pathogenesis is commented.
KEY WORDS: Dyke-Davidoff-Masson syndrome, brain atrophy, computerized tomography, magnetic resonance image.
Achados radiológicos na síndrome de Dyke-Davidoff¾Masson: relato de três casos e contribuição para patogênese e diagnóstico diferencial
RESUMO ¾ Hemiatrofia cerebral ou síndrome de Dyke-Davidoff-Masson é entidade clínica caracterizada por convulsões, assimetria facial , hemiparesia ou hemiplegia contralateral e déficit cognitivo. Estes achados estão relacionados a lesão cerebral ocorrida na infância ou in utero. As características radiológicas são hemiatrofia cerebral e alteracões ósseas no crânio, como espessamento, hiperpneumatização dos seios paranasais e células da mastóide e elevação do ápice da pirâmide petrosa. Descrevemos três casos com achados clássicos da síndrome discutindo aspectos fisiopatológicos.
PALAVRAS-CHAVE: síndrome de Dyke-Davidoff-Masson, atrofia cerebral, tomografia computadorizada, ressonância magnética.
Cerebral hemiatrophy or Dyke-Davidoff-Masson syndrome is a congenital, neonatal or early infantile condition characterized clinically by variable degrees of facial asymmetry, seizures, contralateral hemiplegia or hemiparesis, and mental retardation. Mental retardation is not always present1-3 and seizures may appear months or years after the onset of hemiparesis3. Patients may also have speech or language disorders1. Radiologically, magnetic resonance (MR) and computed tomography (CT) demonstrate the parenchymal abnormalities of unilateral loss of cerebral volume and compensatory bone alterations in the calvarium, such as thickening, hyperpneumatization of the paranasal sinuses and mastoid cells as well as elevation of the petrous ridge and greater wing of the sphenoid bone2,3.
CASE REPORTS
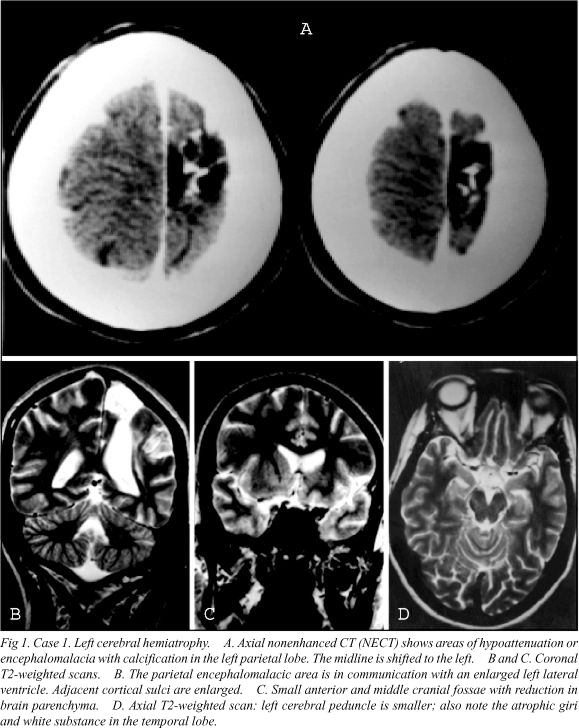
Case 1. A 39-year-old female with a history of traumatic delivery presented for routine medical evaluation for a diagnosed cerebral palsy. Physical examination revealed facial asymmetry and right hemiatrophy. She had right hemiparesis since birth, seizures at age 18 months, and mild mental retardation. CT an MR showed dilated sulci in the affected minor hemisphere (left), ipsilateral ventricular enlargement, gliosis and encephalomalacia, midline shift to the left, small left cerebral peduncle, small left anterior and middle cranial fossae, and calvarial thickening (Fig 1).
Case 2. A 19-year-old male had a normal development until age 3 months when he had meningitis. Since then, he evolved with mental retardation, spastic left hemiparesis and seizures. CT demonstrated a small right hemicranium with a small middle fossa and a porencephalic cyst in communication with a dilated lateral ventricle, ipsilateral widened sulci, hyperpneumatization of the frontal and sphenoid sinuses and mastoid air cells, and calvarial thickening (Fig 2).
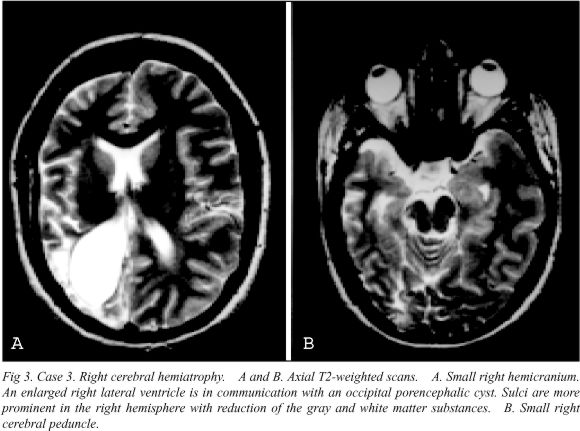
Case 3. A 28-year-old female was evaluated for recurrent seizures. She was born at 36 weeks by cesarean delivery after unsuccessful forceps vaginal delivery. Facial asymmetry was noted at age 3 years, and seizures started at age 7 years. No detectable mental retardation. MRI revealed a small right hemicranium, with a hypoplasic temporal lobe, occipital porencephalic cyst in communication with a dilated lateral ventricle and adjacent prominent sulci, small cerebral peduncle, and hyperpneumatized right frontal sinus (Fig 3).
DISCUSSION
The etiology of cerebral hemiatrophy may be classified into two groups: congenital or primary and acquired or secondary. In the congenital type, cerebral damage which usually has a vascular origin, occurs during intrauterine life and symptoms appear at birth or shortly thereafter. In the acquired or secondary type, cerebral insults occur during the perinatal period or later. The main etiologic factors involved are trauma, infection, vascular abnormalities of the cerebral circulation, ischaemic and haemorrhagic states, and in premature infants, subependymal germinal matrix and intraventricular haemorrhage2,3. Coarctation of the midaortic arch has also been involved 4.
The hemiatrophic cerebral parenchyma will have prominent sulci if the vascular insult occurs after birth or after sulcation is complete. On the other hand, if the vascular ischaemia occurs during embryogenesis, when the formation of gyri and sulci is incomplete, no prominent sulci will be present. Encephalomalacia, gliosis, porencephaly, loss of white and gray matter substance, hypoplastic cerebral peduncle, thalamus and internal capsule, ventricular enlargement and midline shift toward the atrophic side may also be present in the hemiatrophic brain2,3.
The compensatory skull changes reflect adaptations to the unilateral decrease of brain substance and consist of ipsilateral calvarial thickening (diploic space and inner table) with loss of convolutional markings of the inner table of the skull, overdevelopment of the paranasal sinuses (mainly frontal) and mastoid air cells, elevation of the petrous ridge, sphenoid wing and orbital roof, diminished size of the middle/anterior cranial fossae and displacement of falx attachment1-5.
In the present study, the classical features of the acquired type of cerebral hemiatrophy were found in all patients. The findings of dilated sulci and encephalomalacia in the minor hemisphere reflect a late onset of brain insults which were the consequence of traumatic delivery (Cases 1 and 3) or intracranial infection (Case 2).
Vermian-cerebellar hypoplasia may be present in Dyke-Davidoff-Masson syndrome6. It occurs during early embryologic time and may be an occasional finding or associated with other supratentorial abnormalities and syndromes, familial or not. The causes of this condition and of Dandy-Walker malformation and variants are unknown, but there are similar predisposing factors such as gestational exposure to infection, alchool and to some drugs. In the Dandy-Walker malformation, anomalies of the posterior inferior cerebellar arteries, especially absence of the inferior vermian branches and absence of the inferior vermian vein are present7. These features support an early onset of insults during the intrauterine life of our patient, probably of vascular origin. Less common than ipislateral cerebellar atrophy6, contralateral or crossed cerebellar atrophy has also been described in the cerebral hemiatrophy syndrome and it is associated with long-standing, extensive and unilateral cerebral lesions with onset during infancy or early childhood8.
In the differential diagnosis are other conditions that are associated with cerebral hemiatrophy such as Sturge-Weber syndrome, some brain tumors2, Silver's syndrome1, as well as conditions that are associated with unilateral megalencephaly as in the linear nevus sebaceous syndrome. A proper clinical history will provide the correct diagnosis.
Acknowledgements - The authors are thankful to Miss Fiona Reeves from Dublin, Ireland, for revision of the English.
Dr. P. H. Aguiar - Rua Maestro Torquato Amore 332/102 - 05622-050 São Paulo SP - Brasil.
- 1. Parker CE, Harris N, Mavalwala J. Dyke-Davidoff-Masson syndrome: five case studies and deductions from dermatoglyphics. Clin Pediatr 1972;11:288-292.
- 2. Sener RN, Jinkins JR. MR of craniocerebral hemiatrophy. Clin Imaging 1992;16:93-97.
- 3. Zilkha A . CT of cerebral hemiatrophy. AJR 1980;135:259-262.
- 4. Stred SE, Byrum CF, Bove EB, Oliphant M. Coarctation of the midaortic arch presenting with monoparesis. Ann Thorac Surg 1986;42:210-212.
- 5. Lerner MA, Gadoth N, Streifler J, Gordon CR, Young LW. Radiological case of the month. Dyke-Davidoff-Masson syndrome. Am J Dis Child 1988;142:303-304.
- 6. Latchaw RE, Hogg JP, Painter MJ. Congenital anomalies of the brain. In: Latchaw RE (ed). MR and CT imaging of the head, neck and spine. 2.Ed. New York: Mosby Year Book, 1991;1:789-792.
- 7. Kollias SS, Ball WS, Prenger EC. Cystic malformations of the posterior fossa: differential diagnosis clarified through embryologic analysis. Radiographics 1993;13:1211-1231.
- 8. Carrazana EJ, Liu GT, Holmes GL. Crossed cerebellar atrophy in the Dyke-Davidoff-Masson syndrome. Neuroradiology 1992;34:326-327.
Publication Dates
-
Publication in this collection
06 Nov 2000 -
Date of issue
Dec 1998
History
-
Accepted
11 Sept 1998