Abstracts
Postpolio syndrome (PPS) is characterized by progressive muscle weakness due to former infection with poliomyelitis and can be associated with other symptoms such as cold intolerance (CI). Dăoyĭn Qìgōng (DQ) is a technique in Traditional Chinese Medicine that impacts the circulation of energy and blood. OBJECTIVE: It was to verify the effects of DQ in PPS patients complaining of cold intolerance. METHODS: Ten PPS patients were assessed using the visual analogue scale (VAS) adapted for CI before and after intervention with DQ; patients practiced it in a sitting position for 40 minutes, 3 times per week over 3 consecutive months. Patients were reassessed three months after ceasing DQ. RESULTS: There was a statistically significant difference in local and systemic VAS-Cold both at the end of DQ training and three months past the end of this. CONCLUSION: The DQ technique ameliorated CI complaints in patients with PPS.
Postpoliomyelitis syndrome; Qìgōng; breathing exercises; public health
A síndrome pós-poliomielite (SPP) é caracterizada por instalação de nova fraqueza muscular às manifestações residuais da poliomielite, associada a outros sintomas, como intolerância ao frio (IF). O Dăoyĭn Qìgōng (DQ) é uma técnica da medicina tradicional chinesa que interfere na circulação da energia e do sangue. OBJETIVO: Foi verificar os efeitos do DQ em pacientes com SPP com queixa de intolerância ao frio. MÉTODO: Dez pacientes com SPP foram avaliados com a escala visual analógica (EVA) adaptada para IF antes e após intervenção com DQ, adaptados para a posição sentada, com duração de 40 minutos, 3 vezes por semana, durante 3 meses. RESULTADOS: Verificou-se diferença estatisticamente significante, na EVA-frio local e sistêmica, após o término do treinamento. CONCLUSÃO: O DQ é uma técnica que interferiu positivamente na queixa de IF em pacientes com SPP.
síndrome pós-poliomielite; Qìgōng; exercícios respiratórios; saúde pública
ARTICLE
Effects of Dăoyĭn Qìgōng in postpolio syndrome patients with cold intolerance
Efeitos do Dăoyĭn Qìgōng em pacientes com síndrome pós-pólio com queixa de intolerância ao frio
Paulo Eduardo RamosI; Gislaine Cristina AbeI; Márcia Pradella-HallinanI,II; Abrahão Augusto Juviniano QuadrosI; Beny SchmidtI; Acary Souza Bulle OliveiraI
IDepartment of Neurology and Neurosurgery, Department of Clinical Neurology, Division of Neuromuscular Disease Research, Clinic of Traditional Chinese Medicine, Universidade Ferderal de São Paulo (UNIFESP), São Paulo SP, Brazil
IIDepartment of Psychobiology, Sleep Institute, UNIFESP, São Paulo SP, Brazil
Correspondence Correspondence: Gislaine Cristina Abe Universidade Federal de São Paulo Rua Estado de Israel 899 04022-002 São Paulo SP - Brasil E-mail: gislaineabe@hotmail.com
ABSTRACT
Postpolio syndrome (PPS) is characterized by progressive muscle weakness due to former infection with poliomyelitis and can be associated with other symptoms such as cold intolerance (CI). Dăoyĭn Qìgōng (DQ) is a technique in Traditional Chinese Medicine that impacts the circulation of energy and blood.
OBJECTIVE: It was to verify the effects of DQ in PPS patients complaining of cold intolerance.
METHODS: Ten PPS patients were assessed using the visual analogue scale (VAS) adapted for CI before and after intervention with DQ; patients practiced it in a sitting position for 40 minutes, 3 times per week over 3 consecutive months. Patients were reassessed three months after ceasing DQ.
RESULTS: There was a statistically significant difference in local and systemic VAS-Cold both at the end of DQ training and three months past the end of this.
CONCLUSION: The DQ technique ameliorated CI complaints in patients with PPS.
Key words: Postpoliomyelitis syndrome, Qìgōng, breathing exercises, public health.
RESUMO
A síndrome pós-poliomielite (SPP) é caracterizada por instalação de nova fraqueza muscular às manifestações residuais da poliomielite, associada a outros sintomas, como intolerância ao frio (IF). O Dăoyĭn Qìgōng (DQ) é uma técnica da medicina tradicional chinesa que interfere na circulação da energia e do sangue.
OBJETIVO: Foi verificar os efeitos do DQ em pacientes com SPP com queixa de intolerância ao frio.
MÉTODO: Dez pacientes com SPP foram avaliados com a escala visual analógica (EVA) adaptada para IF antes e após intervenção com DQ, adaptados para a posição sentada, com duração de 40 minutos, 3 vezes por semana, durante 3 meses.
RESULTADOS: Verificou-se diferença estatisticamente significante, na EVA-frio local e sistêmica, após o término do treinamento.
CONCLUSÃO: O DQ é uma técnica que interferiu positivamente na queixa de IF em pacientes com SPP.
Palavras-Chave: síndrome pós-poliomielite, Qìgōng, exercícios respiratórios, saúde pública.
Post-polio syndrome (PPS) is characterized by progressive muscle weakness due to former infection with poliomyelitis and is often associated with other symptoms such as muscle fatigue, muscle and or joint pain, cold intolerance (CI) and sleep disorders1-3. A Brazilian study of 167 patients who had previously been diagnosed with paralytic poliomyelitis and subsequently with PPS highlighted a CI frequency of 69.8%4,5. The affected extremities are often unseasonably cold due to involvement of the sympathetic nerve cells, leading to vasoconstriction5. Until now, CI in patients with PPS had no defined etiology or specific rehabilitative or pharmacological treatment; muscle-strengthening exercises and static magnetic fields seem to be beneficial, but these therapies warrant further research6. Guidelines for the treatment of symptoms include adequate clothing, distal/proximal massage and local heat for a short period of time5,7.
From a clinical and histological perspective, the pathophysiology of PPS is associated with lower motor neuron dysfunction. One of the main mechanisms which may lead to this syndrome is overtraining. This activity favors the dysfunction of motor neurons which survive axon terminals which are completely destroyed. Compensatory mechanisms are triggered to reinerve muscle tissue, thereby increasing the drive motor through stimulation of intact motor axons. This mechanism occurs for the axons that are partially jeopardized. However, any exposure to stress will contribute to electrophysiological changes, which, in turn, challenge the nerve conduction velocity. This favors early degeneration of any remaining motor neurons8.
In the language of Traditional Chinese Medicine (TCM), CI is the main symptom of patients with a yáng (陽) deficiency; in TCM, the dynamic balance between yīn(陰) and yáng (陽) is one of the basic principles underlying homeostasis. In general, certain diseases are more likely to lead to imbalances that may cause susceptibility to cold9.
Dăoyĭn Qìgōng (DQ) (導引氣功), one of the various treatment techniques used in TCM, is a form of exercise that aligns gentle movements with controlled breathing. DQ has been practiced in China since ancient times to promote health, longevity and achieve spiritual immortality10-12.
The objective of this study was to evaluate the effects of DQ in patients with PPS and CI complaints.
METHODS
Patients
The study included ten patients (three males, seven females) aged between 30 and 60 years with clinical diagnoses of PPS, according to criteria developed by Mulder13. Our study was conducted by the Division of Neuromuscular Disease Research with the approval of the Ethics Committee of UNIFESP, nº; 529/09.
Allocation
Patients were randomly selected according to their record numbers. Patients signed a consent form after being informed about the study.
Inclusion criteria
We included patients diagnosed with PPS who complained of CI.
Exclusion criteria
Patients with medical histories featuring diseases that could mimic PPS, patients with diagnoses of stable polio sequela, individuals with diagnoses of peripheral vascular disorders and individuals with well-established diagnoses of PPS that were likely to experience difficulties in the execution of the exercises.
DQ exercises used
We selected eight types of DQ exercises that had been adapted to the sitting position. The exercises were applied in sessions of 40 minutes, 3 times per week for 3 consecutive months. We used the visual analogue scale (VAS)-Cold as an assessment instrument before and after intervention; the test was administered by an appraiser who did not attend the DQ training and was unaware of patient diagnosis.
Description of the exercises
Mángzhòng WŬ Yuè Jié Zuò Gōng Tú (芒种五月節坐功圖)
1. Turn your palms outward and lift them above your head, drawing a circle in the air with both hands.
2. With your torso erect, shrink it as much as possible.
3. Lift the torso, stand erect, feeling the spine straight and your hands above your head holding up the sky.
4. Stretch your arms up as if to push up the sky.
5. Release your body, turn your palms down and repeat.
DàshŬ Liù Yuè Zhōng Zuò Gōng Tú (大暑六月中坐功圖)
1. Keep your torso erect and your hands loose by your sides.
2. Rotate your torso and look over your left shoulder. Rotate your torso and look over your right shoulder.
Qīngmíng Sān Yuè jié Zuò Gōng Tú (清明三月節坐功圖)
1. Get in a sitting position with back straightened.
2. The right hand flexes with the index and middle fingers stretched out as if arrowheads were about to be released.
3. Tilt your body to the left, stretching your right arm and pulling the elbow of your left arm back.
4. Release your right arm by bending it in front of your chest with fingers curled.
5. Shrink your left arm stretching the index and middle fingers.
6. Tilt your body to the right, stretching your left arm and pulling the elbow of right arm back.
Lìdōng Shíyuè Jié Zuò Gōng Tú (立冬十月節坐功圖)
1. Sit with your back straight and arms hanging down the sides.
2. Lift your right arm with the palm facing down.
3. At the same time, the left arm bends into the body with the palm facing down.
4. Stretch your right arm above your head and push down with your left palm.
5. Rotate your torso to the left, lowering your right arm while lifting your left arm.
6. Stretch your left arm above your head and push down with your right palm.
7. Rotate your torso to the right, lowering your left arm, then move back to the second movement.
Báilù Bā Yuè Jié Zuò Gōng Tú (白露八月節坐功圖)
1. In a sitting position, keep your back straight and hands on thighs.
2. Relax your back and try to lay your head three times on your right knee. Resume the initial position.
3. Relax your back and try to lay your head three times on your left knee. Resume the initial position.
4. Turn your torso clockwise and counterclockwise.
Jīngzhé èr Yuè Jié Zuò Gōng Tú (惊 蛰 二月節坐功圖)
1. Bend your body forward, shrinking the stomach, arms simulating a pendulum.
2. Raise your body and lift your arms up the level of your waist. Open them at the level of your head and bend your arms in front of your chest to enable both elbows to touch (breathe out slowly).
3. Release the remaining air and arms, bending your body forward, shrinking your stomach.
4. Return to the initial movement and repeat.
Qiūfēn Bā Yuè Zhōng Zuò Gōng Tú (秋分八月中坐功圖)
1. Keep in a sitting position, with back straight and arms on the side of the body.
2. Tilt and rotate your back slowly placing your neck against your shoulder.
3. Stretch your spine, pulling your shoulders back and craning your neck forward.
Lìqiū Qī Yuè Jié Zuò Gōng Tú (立秋七月節坐功圖)
1. Slowly bend your body forward, looking straight ahead with arms relaxed.
2. Bring your chin onto your chest.
3. Lift your body and lean back.
4. Turn your arms out with your palms facing back and then return to the initial movement.
Statistics
We used the test for equality of two proportions, the Anderson-Darling nonparametric test, Student's t -test and the Friedman test. The confidence interval was set at 95%, and p-values were set to p<0.05. The statistical software used in this analysis was SPSS V16, Minitab 15 and Excel Office 2007.
RESULTS
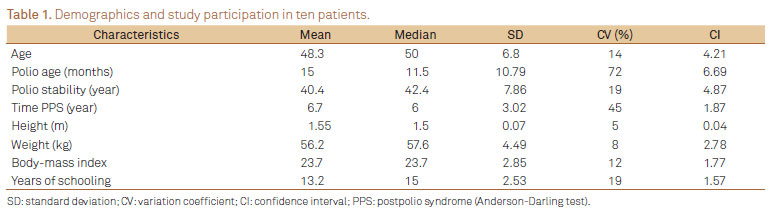
The mean age of participants was 48.3 ± 4.21 years, with a mean schooling level of 13.2 ± 1.57 years. Body mass index (BMI) averaged 23.67 ± 1.77 (Table 1). No differences were found between male and female participants on the basis of BMI (t(8)=0.68, p=0.051), education (t(8)=1.94, p=0.08) and duration of PPS symptoms (t(8)=-0.20, p=0.84). Most participants (70%) were female. All patients (100%) presented with residual motor sequelae in the left leg, and 80% of patients showed motor paralysis in the right leg. There were significant differences between pre- and post-intervention assessments in local and systemic VAS-Cold values (p<0.019). Significant differences persisted until the three-month post-intervention follow-up (Table 2 and Figure).
DISCUSSION
There is no defined etiology for CI complaints in patients with PPS. Studies show that the hypothalamus (the temperature regulation center) and the anterior horn of the spinal cord are also affected by poliovirus, which is one possible explanation for CI7, 14-16.
We found that all patients achieved statistically significant improvement in CI symptoms as a result of DQ practice compared to their previous complaints and were able to maintain these improvements. A study conducted in Brazil reported that CI, among other symptoms, is more prevalent among women (75%)8. In this study, our patients were predominantly female, which is consistent with other PPS studies conducted in Brazil4,5 as well as internationally17-19. In Brazil, the predominance of female patients is attributed to the fact that women seek health services more often than men (excluding one case in which gender predominance was reversed)20. The average age of patients in this study was 48.3 years, that is similar to Brazilian and international studies in which an average age of 50 to 63 years was reported17,21,22.
The level of patient schooling averaged 13.20 ± 1.57 years. Data from the Brazilian Institute of Geography and Statistics census (2000), regarding the general population of 25 years and older, show an average of 6.1 years of schooling. In the subset of individuals with some kind of disability, 10% experienced eight years of education23. The body mass index of subjects averaged 23.67 ± 1.77 and did not appear to impact the assessment; this is an important fact because subcutaneous tissue and fat compose the thermal insulation of the body and promote retention of body heat.
All processes that occur in an organism to maintain its proper functioning have certain environmental requirements, especially those relating to water and temperature. This is because the activity of proteins, enzymes, chemicals and physical reactions occur at speeds according to the temperature of the medium in which they are located. Human beings can be exposed to temperatures ranging from 13º; to 65º;C for several hours without any change in their internal temperature24. Heat is a byproduct of all metabolic processes, including the metabolism of carbohydrates, fats and proteins. The body can increase heat production in response to low external temperatures or dissipate heat when temperatures are high. These external influences impact the body through radiation, conduction and convection. During physical activity, the metabolic rate increases and the biochemical transformations of nutrients promote muscle work (approximately 80% of body heat is produced in skeletal muscle), which together generate heat and raise body temperature24.
The body loses heat through radiation, conduction, evaporation of water from the airways and skin along with excretion of feces and urine. Circulatory adjustments promote cutaneous vasodilation, which raises the temperature of the skin and favors the exchange of heat with the environment. The sympathetic vasoconstrictor nerves are the primary mediators of this response. Peripheral vasodilation is, therefore, a result of the inhibition of sympathetic tone. Heat can reduce this tone via an increase in the temperature of the central nervous system (CNS) or reflexively through the mediation of thermoreceptors in the skin25.
The blood flow of an organ plays an important role in capturing and redistributing heat to cooler parts of the body. However, the ability to sense temperature and the efficiency of thermoregulation to trigger a physiological response and resist exposure to cold declines with age, which is usually a factor in individuals with dementia or those who are sedentary26-28. Vasoconstriction and shivering, which are the primary means of maintaining body temperature during exposure to cold, are less efficient with this decline in vitality29,30. In normal aging, such changes are part of the overall framework of physiological changes. However, individuals with PPS undergo these typically age-related changes precociously, experiencing such things as a substitution of lean mass for fat and hypersensitivity to cold26. Several studies have demonstrated that Chinese exercises (Qìgōng 氣功) have, as one function, a modulation of the autonomic nervous system (sympathetic)31-35. Our study suggests that DQ provides an increase in internal temperature through the voluntary contraction of muscles in the pelvic cavity (during expiration) that are associated with diaphragmatic excursion (during inspiration). The literature has shown that physical activity may promote increased blood flow to skeletal muscle under conditions in which the activity significantly increases sympathetic vasoconstrictor muscle capacity. This process requires the involvement of vasodilators and sympatholytic signals capable of replacing the increased vasoconstriction with neural reflexes in the muscle36-38. The temperature generated by the triggered muscle activity may activate the release of adenosine triphosphate (ATP) within the vascular lumen of the arterial tree, providing oxygenation to the limb tissue (including skeletal muscle and skin) and an increase in intravascular ATP38-43. This phenomenon suggests that overheating the thermostatic preoptic area (POA) of the anterior hypothalamus increases the rate of heat loss from the body through two mechanisms: (1) evaporative heat loss by stimulating the sweat glands and (2) inhibition of the sympathetic centers in the posterior hypothalamus, which normally cause constriction of cutaneous vessels; this inhibition triggers vasodilatation and a consequent increase in heat loss. Because automatic physiological adjustments involve the autonomic nervous system (ANS), there is a contribution from the connections between the hypothalamus, the parasympathetic nuclei of the brain stem and the intermediolateral sympathetic column of the spinal cord44,45. Exercises that combine movement with breathing, such as yoga, cause significant increases in brain levels of gamma-aminobutyric acid (GABA) post-workout46. One study demonstrated that the action of GABA in the mid-dorsal region of the POA causes an increase in the core temperature through stimulation of thermogenesis in brown adipose tissue47.
Finally, the literature suggests that CNS plasticity may be induced by functional or motor tasks48,49. Motor activities and neuroplasticity have been researched in humans in recent decades. Four weeks of daily training sessions for functional tasks allow activation of the primary sensorimotor cortex, ipsilateral and contralateral premotor cortices and ipsilateral cerebellum48,50. This plasticity occurs not only in the cortex, but it can also be seen in subcortical regions such as the thalamus and brain stem51. These cortical neural connections can be remodeled by our experiences and by learning49,52-55.
Our hypothesis is that DQ positively influences the modulation and coordinated recovery of the balance of sympathetic and parasympathetic responses, thereby enhancing the neuroplasticity of these structures.
In conclusion, DQ exercises positively influenced CI symptoms in patients with PPS. The results remained constant three months after cessation of DQ training. Additional studies will be required to understand the mechanism of action of DQ, as well as the duration of its benefits.
ACKNOWLEDGMENTS
We thank Ms. Wu Pi Chun, Eneida de Souza Bulle Oliveira, Celso Antonio de Souza Mello and Bruna Terumi Sato Yonamine for their invaluable help. This project was undertaken by voluntary researchers without funding.
References
1. Codd MPM, Mulder DW, Kurland LT, Beard CM, O'Fallon WM. Poliomyelitis in Rochester, Minnesota 1935-55: Epidemiology and long-term sequelae - a preliminary report. In: Halstead LS, Weicher DO (eds). Late effects of poliomyelits. Miami: Miami Symposia Foundation Inc.; 1985:121-133.
2. Dalakas M, Illa I. Post-polio syndrome: concepts in clinical diagnosis, pathogenesis, and etiology. Adv Neurol 1991;56:495-511.
3. Dalakas MC. Post-polio syndrome 12 years later. How it all started. Ann N Y Acad Sci 1995;753:11-18.
4. Quadros AAJ, Oliveira ASB. Síndrome pós-poliomielite (SPP): avaliação de 167 pacientes. XXII Congresso Brasileiro de Neurologia - V Encontro Luso-Brasileiro. Recife. Arq Neuropsiquiatr 2006;64:75.
5. Maggi F, Marques B, Fávero FM, et al. Intolerância ao frio: uma manifestação clínica da síndrome pós-poliomielite (SPP). XXII Congresso Brasileiro de Neurologia - V Encontro Luso-Brasileiro. Recife. Arq Neuropsiquiatr 2006;64:73.
6. Koopman FS, Uegaki K, Gilhus NE, Beelen A, de Visser M, Nollet F. Treatment for postpolio syndrome. Cochrane Database Syst Rev 2011; CD007818.
7. Bodian D. The generalized vertebrate neuron. Science 1962;137:323-326.
8. Oliveira ASB, Maynard FM. Síndrome pós-poliomielite: aspectos neurológicos. Rev Neurociências 2002;10:31-34.
9. Wang Q, Yao S. Molecular basis for cold-intolerant yang-deficient constitution of traditional Chinese medicine. Am J Chin Med 2008;36:827-834.
10. Abe GC, Ramos PE, Fontes SV, et al. Poliomielite e síndrome pós-poliomielite pela Medicina Tradicional Chinesa: do diagnóstico aos mecanismos fisiopatológicos. Rev Neurociências 2011;19:365-381.
11. 吉,布. 導引術. 西安: 陝西師范大學出版社; 2007;193-199.
12. 魏 成. 天下氣功. 四川: 四川人民出版社; 1995;79-86.
13. Mulder DW. Clinical observations on acute poliomyelitis. Ann N Y Acad Sci 1995;753:1-10.
14. Bodian D. Histopathologic basis of clinical findings in poliomyelitis. Am J Med 1949;6:563-578.
15. Bodian D. Letter to the Editor. Science 1962;135:245-248.
16. Bodian D, Bergman RA. Muscle receptor organs of crayfish:functional-anatomical correlations. Bull Johns Hopkins Hosp 1962;110:78-106.
17. Farbu E, Gilhus NE, Barnes MP, et al. EFNS guideline on diagnosis and management of post-polio syndrome. Report of an EFNS task force. Eur J Neurol 2006;13:795-801.
18. Vasconcelos OM, Poehm EH, McCarter RJ, Quezado ZM. Potential outcome factors in subacute combined degeneration: review of observational studies. J Gen Intern Med 2006;21:1063-1068.
19. Fordyce CB, Gagne D, Jalili F, et al. Elevated serum inflammatory markers in post-poliomyelitis syndrome. J Neurol Sci 2008;271:80-86.
20. Pinheiro R, Viacava F, Travassos C, Brito A. Genero, morbidade, acesso e utilização de serviços de saúde no Brasila. Ciênc Saúde Coletiva 2002;7:687-707.
21. Vasconcelos OM, Prokhorenko OA, Kelley KF, et al. A comparison of fatigue scales in postpoliomyelitis syndrome. Arch Phys Med Rehabil 2006;87:1213-1217.
22. Davidson AC, Auyeung V, Luff R, Holland M, Hodgkiss A, Weinman J. Prolonged benefit in post-polio syndrome from comprehensive rehabilitation: a pilot study. Disabil Rehabil 2009;31:309-317.
23. IBGE. Tabulação avançada do censo demográfico 2000: resultados preliminares da amostra. Available at: http://www.ibge.gov.br/home/presidencia/noticias/08052002tabulacao.shtm [cited 2002 May 8 ] .
24. Vogelaere P, Pereira C. Termorregulação e envelhecimento. Rev Port Cardiol 2005;24:747-761.
25. Guyton AC, Hall JE. Fisiologia humana e mecanismos das doenças. 6 ed. Rio de Janeiro: Guanabara Koogan; 1998:516-518.
26. Horvath SM, Radcliffe CE, Hutt BK, Spurr GB. Metabolic responses of old people to a cold environment. J Appl Physiol 1955;8:145-148.
27. Watts AJ. Hypothermia in the aged: a study of the role of cold-sensitivity. Environ Res 1972;5:119-126.
28. Sugarek NJ. Temperature lowering after iced water. Enhanced effects in the elderly. J Am Geriatr Soc 1986;34:526-529.
29. Wagner JA, Horvath SM, Kitagawa K, Bolduan NW. Comparisons of blood and urinary responses to cold exposures in young and older men and women. J Gerontol 1987;42:173-179.
30. Khan F, Spence VA, Belch JJ. Cutaneous vascular responses and thermoregulation in relation to age. Clin Sci (Lond) 1992;82:521-528.
31. Cheung BM, Lo JL, Fong DY, et al. Randomised controlled trial of qigong in the treatment of mild essential hypertension. J Hum Hypertens 2005;19:697-704.
32. Lee MS, Rim YH, Jeong DM, Kim MK, Joo MC, Shin SH. Nonlinear analysis of heart rate variability during Qi therapy (external Qigong). Am J Chin Med 2005;33:579-588.
33. Griffith JM, Hasley JP, Liu H, Severn DG, Conner LH, Adler LE. Qigong stress reduction in hospital staff. J Altern Complement Med 2008;14:939-945.
34. Johansson M, Hassmén P. Acute psychological responses to Qigong exercise of varying durations. Am J Chin Med 2008;36:449-458.
35. Stenlund T, Birgander LS, Lindahl B, Nilsson L, Ahlgren C. Effects of Qigong in patients with burnout: a randomized controlled trial. J Rehabil Med 2009;41:761-767.
36. Niimi Y, Matsukawa T, Sugiyama Y, et al. Effect of heat stress on muscle sympathetic nerve activity in humans. J Auton Nerv Syst 1997;63:61-67.
37. Padilla J, Garcia-Villalón AL, Fernandez N, Monge L, Gómez B, Diéguez G. Effects of hyperthermia on contraction and dilatation of rabbit femoral arteries. J Appl Physiol 1998;85:2205-2212.
38. Pearson J, Low DA, Stöhr E, et al. Hemodynamic responses to heat stress in the resting and exercising human leg: insight into the effect of temperature on skeletal muscle blood flow. Am J Physiol Regul Integr Comp Physiol 2011;300:R663-R673.
39. González-Alonso J, Mortensen SP, Jeppesen TD, et al. Haemodynamic responses to exercise, ATP infusion and thigh compression in humans: insight into the role of muscle mechanisms on cardiovascular function. J Physiol 2008;586:2405-2417.
40. González-Alonso J, Olsen DB, Saltin B. Erythrocyte and the regulation of human skeletal muscle blood flow and oxygen delivery: role of circulating ATP. Circ Res 2002;91:1046-1055.
41. Kirby BS, Voyles WF, Carlson RE, Dinenno FA. Graded sympatholytic effect of exogenous ATP on postjunctional alpha-adrenergic vasoconstriction in the human forearm: implications for vascular control in contracting muscle. J Physiol 2008;586:4305-4316.
42. Rosenmeier JB, Hansen J, Gonzalez-Alonso J. Circulating ATP-induced vasodilatation overrides sympathetic vasoconstrictor activity in human skeletal muscle. J Physiol 2004;558:351-365.
43. Rosenmeier JB, Yegutkin GG, González-Alonso J. Activation of ATP/UTP-selective receptors increases blood flow and blunts sympathetic vasoconstriction in human skeletal muscle. J Physiol 2008;586:4993-5002.
44. Simon E, Pierau FK, Taylor DC. Central and peripheral thermal control of effectors in homeothermic temperature regulation. Physiol Rev 1986;66:235-300.
45. Morrison SF. Central pathways controlling brown adipose tissue thermogenesis. News Physiol Sci 2004;19:67-74.
46. Streeter CC, Whitfield TH, Owen L, et al. Effects of yoga versus walking on mood, anxiety, and brain GABA levels: a randomized controlled MRS study. J Altern Complement Med 2010;16:1145-1152.
47. Osaka T. Cold-induced thermogenesis mediated by GABA in the preoptic area of anesthetized rats. Am J Physiol Regul Integr Comp Physiol 2004;287:R306-R313.
48. Borella MdP, Sacchelli T. Os efeitos da prática de atividades motoras sobre a neuroplasticidade. Rev Neurocienc 2009;17:161-169.
49. Fisher BE, Sullivan KJ. Activity-dependent factors affecting poststroke functional outcomes. Top Stroke Rehabil 2001;8:31-44.
50. Lindberg P, Schmitz C, Forssberg H, Engardt M, Borg J. Effects of passive-active movement training on upper limb motor function and cortical activation in chronic patients with stroke: a pilot study. J Rehab Med 2004;36:117-123.
51. Jones EG, Pons TP. Thalamic and brainstem contributions to large-scale plasticity of primate somatosensory cortex. Science 1998;282:1121-1125.
52. Nudo RJ. Adaptive plasticity in motor cortex: implications for rehabilitation after brain injury. J Rehabil Med 2003:41:S7-S10.
53. Adkins DL, Boychuk J, Remple MS, Kleim JA. Motor training induces experience-specific patterns of plasticity across motor cortex and spinal cord. J Appl Physiol 2006;101:1776-1782.
54. Kelly C, Foxe JJ, Garavan H. Patterns of normal human brain plasticity after practice and their implications for neurorehabilitation. Arch Phys Med Rehabil 2006;87:S20-S29.
55. Johansson BB. Brain plasticity and stroke rehabilitation. The Willis lecture. Stroke 2000;31:223-230.
Received 28 March 2012
Received in final form 18 April 2012
Accepted 25 April 2012
Conflict of interest: There is no conflict of interest to declare.
- 1. Codd MPM, Mulder DW, Kurland LT, Beard CM, O'Fallon WM. Poliomyelitis in Rochester, Minnesota 1935-55: Epidemiology and long-term sequelae - a preliminary report. In: Halstead LS, Weicher DO (eds). Late effects of poliomyelits. Miami: Miami Symposia Foundation Inc.; 1985:121-133.
- 2. Dalakas M, Illa I. Post-polio syndrome: concepts in clinical diagnosis, pathogenesis, and etiology. Adv Neurol 1991;56:495-511.
- 3. Dalakas MC. Post-polio syndrome 12 years later. How it all started. Ann N Y Acad Sci 1995;753:11-18.
- 4. Quadros AAJ, Oliveira ASB. Síndrome pós-poliomielite (SPP): avaliação de 167 pacientes. XXII Congresso Brasileiro de Neurologia - V Encontro Luso-Brasileiro. Recife. Arq Neuropsiquiatr 2006;64:75.
- 5. Maggi F, Marques B, Fávero FM, et al. Intolerância ao frio: uma manifestação clínica da síndrome pós-poliomielite (SPP). XXII Congresso Brasileiro de Neurologia - V Encontro Luso-Brasileiro. Recife. Arq Neuropsiquiatr 2006;64:73.
- 6. Koopman FS, Uegaki K, Gilhus NE, Beelen A, de Visser M, Nollet F. Treatment for postpolio syndrome. Cochrane Database Syst Rev 2011; CD007818.
- 7. Bodian D. The generalized vertebrate neuron. Science 1962;137:323-326.
- 8. Oliveira ASB, Maynard FM. Síndrome pós-poliomielite: aspectos neurológicos. Rev Neurociências 2002;10:31-34.
- 9. Wang Q, Yao S. Molecular basis for cold-intolerant yang-deficient constitution of traditional Chinese medicine. Am J Chin Med 2008;36:827-834.
- 13. Mulder DW. Clinical observations on acute poliomyelitis. Ann N Y Acad Sci 1995;753:1-10.
- 14. Bodian D. Histopathologic basis of clinical findings in poliomyelitis. Am J Med 1949;6:563-578.
- 15. Bodian D. Letter to the Editor. Science 1962;135:245-248.
- 16. Bodian D, Bergman RA. Muscle receptor organs of crayfish:functional-anatomical correlations. Bull Johns Hopkins Hosp 1962;110:78-106.
- 17. Farbu E, Gilhus NE, Barnes MP, et al. EFNS guideline on diagnosis and management of post-polio syndrome. Report of an EFNS task force. Eur J Neurol 2006;13:795-801.
- 18. Vasconcelos OM, Poehm EH, McCarter RJ, Quezado ZM. Potential outcome factors in subacute combined degeneration: review of observational studies. J Gen Intern Med 2006;21:1063-1068.
- 19. Fordyce CB, Gagne D, Jalili F, et al. Elevated serum inflammatory markers in post-poliomyelitis syndrome. J Neurol Sci 2008;271:80-86.
- 20. Pinheiro R, Viacava F, Travassos C, Brito A. Genero, morbidade, acesso e utilização de serviços de saúde no Brasila. Ciênc Saúde Coletiva 2002;7:687-707.
- 21. Vasconcelos OM, Prokhorenko OA, Kelley KF, et al. A comparison of fatigue scales in postpoliomyelitis syndrome. Arch Phys Med Rehabil 2006;87:1213-1217.
- 22. Davidson AC, Auyeung V, Luff R, Holland M, Hodgkiss A, Weinman J. Prolonged benefit in post-polio syndrome from comprehensive rehabilitation: a pilot study. Disabil Rehabil 2009;31:309-317.
- 23. IBGE. Tabulação avançada do censo demográfico 2000: resultados preliminares da amostra. Available at: http://www.ibge.gov.br/home/presidencia/noticias/08052002tabulacao.shtm [cited 2002 May 8 ]
- 24. Vogelaere P, Pereira C. Termorregulação e envelhecimento. Rev Port Cardiol 2005;24:747-761.
- 25. Guyton AC, Hall JE. Fisiologia humana e mecanismos das doenças. 6 ed. Rio de Janeiro: Guanabara Koogan; 1998:516-518.
- 26. Horvath SM, Radcliffe CE, Hutt BK, Spurr GB. Metabolic responses of old people to a cold environment. J Appl Physiol 1955;8:145-148.
- 27. Watts AJ. Hypothermia in the aged: a study of the role of cold-sensitivity. Environ Res 1972;5:119-126.
- 28. Sugarek NJ. Temperature lowering after iced water. Enhanced effects in the elderly. J Am Geriatr Soc 1986;34:526-529.
- 29. Wagner JA, Horvath SM, Kitagawa K, Bolduan NW. Comparisons of blood and urinary responses to cold exposures in young and older men and women. J Gerontol 1987;42:173-179.
- 30. Khan F, Spence VA, Belch JJ. Cutaneous vascular responses and thermoregulation in relation to age. Clin Sci (Lond) 1992;82:521-528.
- 31. Cheung BM, Lo JL, Fong DY, et al. Randomised controlled trial of qigong in the treatment of mild essential hypertension. J Hum Hypertens 2005;19:697-704.
- 32. Lee MS, Rim YH, Jeong DM, Kim MK, Joo MC, Shin SH. Nonlinear analysis of heart rate variability during Qi therapy (external Qigong). Am J Chin Med 2005;33:579-588.
- 33. Griffith JM, Hasley JP, Liu H, Severn DG, Conner LH, Adler LE. Qigong stress reduction in hospital staff. J Altern Complement Med 2008;14:939-945.
- 34. Johansson M, Hassmén P. Acute psychological responses to Qigong exercise of varying durations. Am J Chin Med 2008;36:449-458.
- 35. Stenlund T, Birgander LS, Lindahl B, Nilsson L, Ahlgren C. Effects of Qigong in patients with burnout: a randomized controlled trial. J Rehabil Med 2009;41:761-767.
- 36. Niimi Y, Matsukawa T, Sugiyama Y, et al. Effect of heat stress on muscle sympathetic nerve activity in humans. J Auton Nerv Syst 1997;63:61-67.
- 37. Padilla J, Garcia-Villalón AL, Fernandez N, Monge L, Gómez B, Diéguez G. Effects of hyperthermia on contraction and dilatation of rabbit femoral arteries. J Appl Physiol 1998;85:2205-2212.
- 38. Pearson J, Low DA, Stöhr E, et al. Hemodynamic responses to heat stress in the resting and exercising human leg: insight into the effect of temperature on skeletal muscle blood flow. Am J Physiol Regul Integr Comp Physiol 2011;300:R663-R673.
- 39. González-Alonso J, Mortensen SP, Jeppesen TD, et al. Haemodynamic responses to exercise, ATP infusion and thigh compression in humans: insight into the role of muscle mechanisms on cardiovascular function. J Physiol 2008;586:2405-2417.
- 40. González-Alonso J, Olsen DB, Saltin B. Erythrocyte and the regulation of human skeletal muscle blood flow and oxygen delivery: role of circulating ATP. Circ Res 2002;91:1046-1055.
- 41. Kirby BS, Voyles WF, Carlson RE, Dinenno FA. Graded sympatholytic effect of exogenous ATP on postjunctional alpha-adrenergic vasoconstriction in the human forearm: implications for vascular control in contracting muscle. J Physiol 2008;586:4305-4316.
- 42. Rosenmeier JB, Hansen J, Gonzalez-Alonso J. Circulating ATP-induced vasodilatation overrides sympathetic vasoconstrictor activity in human skeletal muscle. J Physiol 2004;558:351-365.
- 43. Rosenmeier JB, Yegutkin GG, González-Alonso J. Activation of ATP/UTP-selective receptors increases blood flow and blunts sympathetic vasoconstriction in human skeletal muscle. J Physiol 2008;586:4993-5002.
- 44. Simon E, Pierau FK, Taylor DC. Central and peripheral thermal control of effectors in homeothermic temperature regulation. Physiol Rev 1986;66:235-300.
- 45. Morrison SF. Central pathways controlling brown adipose tissue thermogenesis. News Physiol Sci 2004;19:67-74.
- 46. Streeter CC, Whitfield TH, Owen L, et al. Effects of yoga versus walking on mood, anxiety, and brain GABA levels: a randomized controlled MRS study. J Altern Complement Med 2010;16:1145-1152.
- 47. Osaka T. Cold-induced thermogenesis mediated by GABA in the preoptic area of anesthetized rats. Am J Physiol Regul Integr Comp Physiol 2004;287:R306-R313.
- 48. Borella MdP, Sacchelli T. Os efeitos da prática de atividades motoras sobre a neuroplasticidade. Rev Neurocienc 2009;17:161-169.
- 49. Fisher BE, Sullivan KJ. Activity-dependent factors affecting poststroke functional outcomes. Top Stroke Rehabil 2001;8:31-44.
- 50. Lindberg P, Schmitz C, Forssberg H, Engardt M, Borg J. Effects of passive-active movement training on upper limb motor function and cortical activation in chronic patients with stroke: a pilot study. J Rehab Med 2004;36:117-123.
- 51. Jones EG, Pons TP. Thalamic and brainstem contributions to large-scale plasticity of primate somatosensory cortex. Science 1998;282:1121-1125.
- 52. Nudo RJ. Adaptive plasticity in motor cortex: implications for rehabilitation after brain injury. J Rehabil Med 2003:41:S7-S10.
- 53. Adkins DL, Boychuk J, Remple MS, Kleim JA. Motor training induces experience-specific patterns of plasticity across motor cortex and spinal cord. J Appl Physiol 2006;101:1776-1782.
- 54. Kelly C, Foxe JJ, Garavan H. Patterns of normal human brain plasticity after practice and their implications for neurorehabilitation. Arch Phys Med Rehabil 2006;87:S20-S29.
- 55. Johansson BB. Brain plasticity and stroke rehabilitation. The Willis lecture. Stroke 2000;31:223-230.
Correspondence:
Publication Dates
-
Publication in this collection
13 Sept 2012 -
Date of issue
Sept 2012
History
-
Received
28 Mar 2012 -
Accepted
25 Apr 2012 -
Reviewed
18 Apr 2012