Abstracts
OBJECTIVE:
To evaluate the growth pattern of low birth weight preterm infants born to hypertensive mothers, the occurrence of growth disorders, and risk factors for inadequate growth at 24 months of corrected age (CA).
METHODS:
Cohort study of preterm low birth weight infants followed until 24 months CA, in a university hospital between January 2009 and December 2010. Inclusion criteria: gestational age < 37 weeks and birth weight of 1,500-2,499 g. Exclusion criteria: multiple pregnancies, major congenital anomalies, and loss to follow up in the 2nd year of life. The following were evaluated: weight, length, and BMI. Outcomes: growth failure and risk of overweight at 0, 12, and 24 months CA. Student's t-test, Repeated measures ANOVA (RM-ANOVA), and multiple logistic regression were used.
RESULTS:
A total of 80 preterm low birth weight infants born to hypertensive mothers and 101 born to normotensive mothers were studied. There was a higher risk of overweight in children of hypertensive mothers at 24 months; however, maternal hypertension was not a risk factor for inadequate growth. Logistic regression showed that being born small for gestational age and inadequate growth in the first 12 months of life were associated with poorer growth at 24 months.
CONCLUSION:
Preterm low birth weight born infants to hypertensive mothers have an increased risk of overweight at 24 months CA. Being born small for gestational age and inadequate growth in the 1st year of life are risk factors for growth disorders at 24 months CA.
Child; Low birth weight; Premature; Maternal hypertension; Growth
OBJETIVO:
Avaliar o padrão de crescimento de prematuros de baixo peso nascidos de mães hipertensas, a ocorrência de distúrbios de crescimento e os fatores de risco para inadequado crescimento aos 24 meses de idade corrigida (IC).
MÉTODOS:
Estudo de coorte de prematuros de baixo peso acompanhados até 24 meses IC, em um hospital universitário, entre janeiro de 2009 e dezembro de 2010. Critérios de inclusão: idade gestacional < 37 semanas e peso de nascimento de 1500-2499 g. Excluídas: gestações múltiplas, anomalias congênitas maiores e perda de seguimento no segundo ano de vida. Foram avaliados: peso, comprimento e IMC. Desfechos: falha de crescimento e risco de sobrepeso com 0, 12 e 24 meses de IC. Teste t de Student, X2, Anova-RM e regressão logística múltipla foram usados.
RESULTADOS:
Foram estudados 80 prematuros de baixo peso nascidos de mães hipertensas e 101 de mães normotensas. Houve maior risco de sobrepeso em crianças de mães hipertensas aos 24 meses, entretanto a hipertensão materna não foi fator de risco para inadequado crescimento. A regressão logística mostrou que nascer pequeno para idade gestacional e ter inadequado crescimento nos primeiros 12 meses de vida associaram-se com pior crescimento aos 24 meses.
CONCLUSÃO:
Prematuros de baixo peso nascidos de mães hipertensas têm risco aumentado de sobrepeso aos 24 meses de IC. Ser pequeno para idade gestacional e ter inadequado crescimento no primeiro ano são fatores de risco para distúrbios no crescimento aos 24 meses de IC.
Criança; Baixo peso ao nascer; Prematuro; Hipertensão materna; Crescimento
Introduction
Among the causes of prematurity, hypertensive disorder of pregnancy is one of the most important, affecting 5% to 10% of pregnancies and demonstrating an increasing incidence in developing countries.11 Roberts CL, Algert CS, Morris JM, Ford JB, Henderson-Smart DJ. Hypertensive disorders in pregnancy: a population-based study. Med J Aust. 2005;182:332-5. and 22 Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol. 2009;33:130-7. This disease is an important cause of maternal and fetal mortality and morbidity, as well as one of the main medical indications of preterm birth, often associated with fetal growth restriction.11 Roberts CL, Algert CS, Morris JM, Ford JB, Henderson-Smart DJ. Hypertensive disorders in pregnancy: a population-based study. Med J Aust. 2005;182:332-5. and 33 Rugolo LM, Bentlin MR, Trindade CE. Preeclampsia: effect on the fetus and newborn. Neoreviews. 2011;12:e198-206.
Preterm infants born small for gestational age (SGA) due to intrauterine growth restriction are at higher risk of neonatal morbimortality and growth and development disorders, when compared with those born with adequate weight for gestational age (AGA).44 Bocca-Tjeertes IF, Kerstjens JM, Reijneveld SA, de Winter AF, Bos AF. Growth and predictors of growth restraint in moderately preterm children aged 0 to 4 years. Pediatrics. 2011;128:e1187-94. and 55 Grisaru-Granovsky S, Reichman B, Lerner-Geva L, Boyko V, Hammerman C, Samueloff A, et al. Mortality and morbidity in preterm small-for-gestational-age infants: a population-based study. Am J Obstet Gynecol. 2012;206(150):e1-7. Another point of concern regarding the consequences of prematurity or low birth weight in the long-term is that inadequate growth during the fetal period and in the early years of life increases the risk of chronic diseases such as hypertension, myocardial infarction, and diabetes in adulthood.66 Victora CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, et al. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371:340-57.
There are scarce and contradictory studies on the prognosis of infants born to hypertensive mothers. There is evidence that exposure to oxidative stress in utero, triggered by maternal hypertensive disease, has implications in the pathogenesis of several diseases of preterm infants,33 Rugolo LM, Bentlin MR, Trindade CE. Preeclampsia: effect on the fetus and newborn. Neoreviews. 2011;12:e198-206. and is associated with higher neonatal morbimortality, although it has not been established whether the worse prognosis of these preterm infants is due to maternal disease or degree of prematurity.33 Rugolo LM, Bentlin MR, Trindade CE. Preeclampsia: effect on the fetus and newborn. Neoreviews. 2011;12:e198-206. and 77 Habli M, Levine RJ, Qian C, Sibai B. Neonatal outcomes in preg- nancies with preeclampsia or gestational hypertension and in normotensive pregnancies that delivered at 35, 36, or 37 weeks of gestation. Am J Obstet Gynecol. 2007;197(406):e1-7. However, some studies found no differences in the prognosis of preterm infants born to hypertensive mothers88 Friedman SA, Schiff E, Kao L, Sibai BM. Neonatal outcome after preterm delivery for preeclampsia. Am J Obstet Gynecol. 1995;172:1785-92. and 99 Boomsma JM, van Lingen RA, van Eyck J, Tamminga P, Kollen BJ, van Elburg RM. Short- and long-term outcome of infants born after maternal (pre)-eclampsia, HELLP syndrome and throm- bophilia: a retrospective, cohort study. Eur J Obstet Gynecol Reprod Biol. 2010;153:47-51. and others have suggested that stress in utero triggered by hypertension can accelerate the maturation of organs and improve the prognosis of these preterm infants.1010 Withagen MI, Wallenburg HC, Steegers EA, Hop WC, Visser W. Morbidity and development in childhood of infants born after temporising treatment of early onset pre-eclampsia. BJOG. 2005;112:910-4. A recent study showed that most preterm infants born to mothers with severe hypertension syndrome have intrauterine growth restriction and achieve complete "catch up" in the first 4 years, but at that age, these children are smaller and thinner compared to the population mean.1111 Beukers F, Cranendonk A, de Vries JI, Wolf H, Lafeber HN, Vriesendorp HC, et al. Catch-up growth in children born growth restricted to mothers with hypertensive disorders of pregnancy. Arch Dis Child. 2013;98:30-5.
The scarcity and the lack of consensus of studies on the prognosis of premature infants born to mothers with gestational hypertension syndrome justify the need for surveillance of neonatal complications, and follow-up of these infants, for better understanding the impact of maternal disease on growth and development.
This study aimed to analyze the growth pattern of low birth-weight preterm infants born to hypertensive mothers, as well as evaluate the occurrence of growth disorders and risk factors for inadequate growth at 24 months corrected age (CA).
Methods
This was a prospective cohort study of low birth weight preterm infants admitted to the Neonatal Care Unit and followed during the first 2 years of life at the Low Birth Weight Infant Outpatient Clinic of Faculdade de Medicina de Botucatu-UNESP, from January of 2009 to December of 2010.
The study was approved by the Research Ethics Committee of the institution. Maternal and neonatal data of interest were obtained from medical records at the first outpatient routine consultation, after obtaining the signed informed consent.
A convenience sample was studied, corresponding to the total number of patients who met the inclusion criteria during a two-year enrollment period, accepting a maximum loss of 20% of the cohort.
In the Low Birth Weight Infant Outpatient Clinic, starting in January of 2009, all preterm infants younger than 1 year were selected on the day of consultation and included in the study, when they met the following criteria: born in the Clinic's maternity ward, single gestation, gestational age < 37 weeks, birth weight between 1,500 and 2,499 g, without multiple congenital anomalies and no congenital infection, and who had at least three consultations in the 1st year of life. Lack of follow-up in the 2nd year of life was considered as a loss.
The study variables included: maternal data (age, level of schooling, height, and smoking status); pregnancy data (hypertensive disorder of pregnancy, regardless of the type and severity of the disease, diabetes mellitus; intrauterine growth restriction, preterm premature rupture of membranes, fetal distress, and type of delivery); neonatal data (gestational age according to the best obstetric estimate, birth weight and AGA according to Alexander et al.,1212 Alexander GR, Himes JH, Kaufman RB, Mor J, Kogan M. A United States national reference for fetal growth. Obstet Gynecol. 1996;87:163-8. gender, Apgar score at 1 and 5 minutes after birth, neonatal morbidity, and length of hospital stay). After hospital discharge, the following variables were considered: breastfeeding in the 1st year of life; hospitalization in the first 2 years, anthropometric measurements (weight and length), and body mass index.
Anthropometric measurements were obtained at each visit by the previously trained medical and nursing staff of the service. Patients were weighed on a digital scale (Filizzola(r), SP, Brazil) for children, with an accuracy of 5 g. Length was measured in the supine position, using a wooden stadiometer or in the standing position, using a ruler in millimeters.
CA was used for all preterm infants in the first 2 years of life, and anthropometric measurements were evaluated by calculating the Z-score to follow growth, as classically done in the literature. Growth assessment was performed by quarters in the 1st year and every six months in the 2nd year of life, considering the consultation that was closer to the expected date of assessment, namely: 40 weeks, 3 months, 6 months, 9 months, 12 months, 18 months, and 24 months CA.
Based on whether or not the cohort was exposed to gestational hypertension syndrome, the study groups were formed: preterm infants of hypertensive mothers and preterm infants of normotensive mothers. The outcomes of interest were: growth failure or risk of overweight at 12 and 24 months of age, according to the growth curve of the World Health Organization (WHO; 2006).1313 World Health Organization (WHO). The WHO Child Growth Stan- dards. 2006. [cited 30 Nov 2011]. Available from: http://www.who.int/childgrowth/em/
http://www.who.int/childgrowth/em/...
Definitions used in the study:
- Gestational hypertensive syndrome: blood pressure 140/90 mmHg or higher, on two occasions, with an interval ≥ 4 hours, according to the criteria of the Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy.1414 Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol. 2000;183:S1-22. Hypertension diagnosed after the 20th week of gestation associated with proteinuria (> 300 mg in 24-hour urine) characterized pre-eclampsia. - SGA: birth weight < 10th percentile, according to Alexander et al.1212 Alexander GR, Himes JH, Kaufman RB, Mor J, Kogan M. A United States national reference for fetal growth. Obstet Gynecol. 1996;87:163-8. - Growth failure: weight or length below the 3rd percentile on the WHO curve (2006).1313 World Health Organization (WHO). The WHO Child Growth Stan- dards. 2006. [cited 30 Nov 2011]. Available from: http://www.who.int/childgrowth/em/
http://www.who.int/childgrowth/em/...
- Thinness: BMI ≥ 0.1 percentile and < 3rd percentile on the WHO curve (2006).1313 World Health Organization (WHO). The WHO Child Growth Stan- dards. 2006. [cited 30 Nov 2011]. Available from: http://www.who.int/childgrowth/em/
http://www.who.int/childgrowth/em/...
- Risk of overweight: BMI > 85th percentile and ≤ 97th percentile according to the WHO curve (2006).1313 World Health Organization (WHO). The WHO Child Growth Stan- dards. 2006. [cited 30 Nov 2011]. Available from: http://www.who.int/childgrowth/em/
http://www.who.int/childgrowth/em/...
Statistical analysis
Data were described by calculating the distribution of frequencies, means and standard deviations, medians, and percentiles. Associations between numerical variables were assessed by Student's t-test or the Mann-Whitney test when indicated, and the chi-squared test was used for categorical variables.
RM-ANOVA followed by Tukey's test was used for multiple comparisons between groups, and the chi-squared test for trend was used to assess change of proportions over time, with the sample stratified according to maternal hypertension and adequacy of birth weight for gestational age.
The outcomes of interest were analyzed by logistic regression for repeated measures. SAS software for Windows, release 9.2 (SAS Institute Inc, NC, USA), was used in the statistical analyses and the significance level was set at 5%.
Results
From January 2009 to December 2010, 241 premature infants eligible for the study were born in the Maternity Ward of Hospital das Clínicas da Faculdade de Medicina de Botucatu-UNESP. Among these, there were three in-hospital deaths and 238 were referred for follow-up at the Low Birth Weight Infant Outpatient Clinic, but in four cases the consultation was not scheduled (2%). Thus, 234 eligible preterm infants were enrolled in the study, but 40 of these preterm infants were twins, and 13 had malformations and were excluded. Therefore, the cohort consisted of 181 preterm infants, 101 born to normotensive mothers and 80 to hypertensive mothers, of whom 63 (80%) had pre-eclampsia.
At the end of the first year of life, 69 preterm infants of hypertensive mothers (86%) and 84 preterm infants of normotensive mothers (83%) were evaluated. At 24 months, 149 preterm infants were evaluated, with a loss of cohort of 15% in the hypertensive group and 20% in the normotensive group. There were no differences in the neonatal characteristics of preterm infants followed up to 24 months compared to those who were lost to follow-up, except for gestational age, which was lower in the lost cohort of the normotensive group (32 ± 2 weeks vs. 33 ± 2 weeks in the other groups, p = 0.035).
Mean maternal age was 25-26 years, mean height was 1.59 m, and 40% of the mothers had only elementary education, with no difference between groups. Premature rupture of membranes was more frequent in the normotensive group (41% vs. 2.5%, p < 0.001), whereas cesarean delivery predominated in the hypertensive group (82% vs. 40%, p < 0.001).
Table 1 shows the main neonatal characteristics. This table highlights the high percentage of infants born SGA in the two groups of preterm infants, and also the high frequency of breastfeeding at discharge, with exclusive breastfeeding more frequent in the normotensive group (p = 0.033).
At the outpatient follow-up during the first 2 years of life, few preterm infants required hospitalization (2%) and the incidence of complications was low in both groups; the most common problem was anemia, diagnosed in 8% of patients, with no difference between groups. The feeding pattern of the preterm infants, monitored by the medical team with support from a nutritionist, was satisfactory in the 1st year of life, with high rates of exclusive or predominant breastfeeding (two-thirds of the sample in the two groups) in the first 6 months of life. The median duration of breastfeeding was 6.5 (3-12) months for preterm infants born to hypertensive mothers and 6 (3 to 11.5) months in the normotensive group.
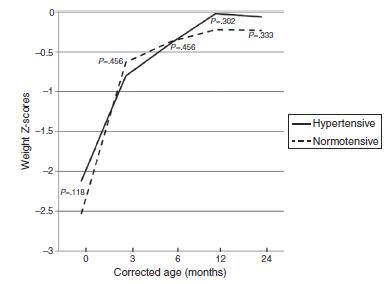
In both groups of preterm infants, the curves of Z-scores for weight and length were superimposed in the first 2 years of life (Figure 1 and Figure 2).
Evolution of the weight Z-scores in preterm infants of normotensive and hypertensive mothers up to 24 months corrected age.
Evolution of length Z-scores in preterm infants of normotensive and hypertensive mothers up to 24 months corrected age.
Table 2 shows the mean values of Z scores for weight, height, and BMI, and the frequency of growth disorders at term, with 12 and 24 months CA. This table highlights the higher percentage of preterm infants born to hypertensive mothers with BMI > 85th percentile at 24 months CA (Table 2).
To determine whether gestational hypertension syndrome is a risk factor for growth disorders in low birth weight preterm infants, logistic regression models were constructed, controlled for gestational age and gender, including maternal hypertension, adequacy of birth weight for gestational age, and effect of time on anthropometric measurements.
Logistic regression showed that maternal hypertension was not a risk factor for inadequate growth in weight (OR = 0.47, 95% CI: -0.10-1.05) and length (OR = 0.20, 95% CI: -0.29-0.69) at 24 months CA. Two risk factors for growth disorders were identified at 24 months CA: SGA and inadequate growth in the 1st year of life.
SGA increased the risk of inadequate weight by approximately two-fold (OR = 2.36, 95% CI: 1:34-4.14) and length (OR = 2.13, 95% CI: 1.30-3.50). Inadequate weight gain at 3 months (OR = 5.89, 95% CI: 3.07-11.30), at 6 months (OR = 2.95, 95% CI: 1.61-5.45), and at 12 months (OR = 2.45, 95% CI: 1.45-4.18) showed influence on weight at 24 months CA, whereas inadequate growth in length at 3 months (OR = 7.12, 95% CI: 3.80-13.35) and at 6 months (OR = 2.78, 95% CI; 1:45-5.35) was a risk factor for inadequate stature at 24 months CA.
Discussion
The main results of this study indicate a higher frequency of growth disorders in low birth weight preterm infants born to hypertensive mothers, but the effect of maternal disease was indirect, with inadequate fetal growth and growth failure in the first year of life representing the risk factors for the occurrence of growth disorders at 24 months CA.
In the present study, the growth profiles of preterm infants of normotensive and hypertensive mothers were similar in the first 2 years of life and found to be satisfactory according to the WHO standards. It must be considered that these preterm infants' birth weight was between 1,500 and 2,499 g, constituting a scarcely studied group whose prognosis for growth is not well established. An important fact that may have positively influenced the results was the high rate of breastfeeding at hospital discharge, with a mean duration of breastfeeding of 6 months in both groups. The literature highlights the importance of breastfeeding for preterm low birth weight infants, which results in a better pattern of growth and development for these children.1515 Han Y, Chang EY, Kim J, Ahn K, Kim HY, Hwang EM, et al. Asso- ciation of infant feeding practices in the general population with infant growth and stool characteristics. Nutr Res Pract. 2011;5:308-12.
The study sample was homogeneous regarding gestational age and birth weight, and may be considered of low neonatal risk, except for the high percentage of SGA preterm infants in both groups (51% and 40% in the hypertensive and normotensive groups, respectively). These figures are found in tertiary care services, with incidence reported in the literature of approximately 15-50% SGA newborns in pregnancies complicated by hypertension.11 Roberts CL, Algert CS, Morris JM, Ford JB, Henderson-Smart DJ. Hypertensive disorders in pregnancy: a population-based study. Med J Aust. 2005;182:332-5. and 1616 Ray JG, Burrows RF, Burrows EA, Vermeulen MJ. MOS HIP: McMaster outcome study of hypertension in pregnancy. Early Hum Dev. 2001;64:129-43. Impaired fetal growth is expected especially in pre-eclampsia due to the physiopathology of the disease, which involves alterations in placental blood flow.22 Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol. 2009;33:130-7. A study of pregnancies under 34 weeks complicated by hypertensive syndrome demonstrated that alteration in the umbilical artery Doppler velocimentry increases the incidence of SGA infants by 2.5-fold.1717 Moura MD, Margotto PR, Rugolo LM. Changes of blood flow in the umbilical artery in hypertensive pregnancy and the impli- cations in the neonatal outcomes. Rev Bras Ginecol Obstet. 2013;35:71-7.
The growth prognosis for preterm infants born to hypertensive mothers has been poorly studied and the results are controversial. Silveira et al.1818 Silveira RC, Procianoy RS, Koch MS, Benjamin AC, Schlindwein CF. Growth and neurodevelopment outcome of very low birth weight infants delivered by preeclamptic mothers. Acta Paedi- atr. 2007;96:1738-42. evaluated 40 very low birth weight preterm infants born to mothers with pre-eclampsia and 46 born to normotensive mothers, and showed that at 12 and 18 months CA, the preterm infants of mothers with pre-eclampsia showed no catch-up weight, whereas growth in height and head circumference did not differ between groups. The authors attributed the failure to thrive to the high percentage of SGA preterm infants in the pre-eclampsia group (62% vs. 39% in the normotensive group). A recent study assessed the growth of preterm infants born to mothers with hypertensive syndrome who had fetal growth restriction and showed good prognosis for growth in stature, with catch-up in 94% of children, although the children became thinner during the first 5 years of life. 1111 Beukers F, Cranendonk A, de Vries JI, Wolf H, Lafeber HN, Vriesendorp HC, et al. Catch-up growth in children born growth restricted to mothers with hypertensive disorders of pregnancy. Arch Dis Child. 2013;98:30-5.
Postnatal growth restriction is a very frequent event in very low birth weight preterm infants and those admitted at the neonatal ICU, who mostly demonstrate retarded growth, with decreased Z-scores for weight and length between birth and 40 weeks CA.1919 Modi M, Saluja S, Kler N, Batra A, Kaur A, Garg P, et al. Growth and neurodevelopmental outcome of VLBW infants at 1 year corrected age. Indian Pediatr. 2013;50:573-7. and 2020 Rugolo LM, Bentlin MR, Rugolo AJ, Dalben I, Trindade CE. Growth of extremely low birth weight infants during the first two years of life. Rev Paul Pediatr. 2007;25:142-9. Consistent with this expectation, in this study more than one-quarter of the sample had weight below the 5th percentile when they reached term, but at the end of the 1st year of life, weight was higher than the 5th percentile in more than 90% of preterm infants in the two groups. Similar developments occurred in height growth. These results are in agreement with literature data showing that most preterm infants experience catch-up growth, reaching their percentis between the limits of normality on reference curves by 2-3 years of age.2121 Rugolo LM. Crescimento e desenvolvimento a longo prazo do prematuro extremo. J Pediatr (Rio J). 2005;81: S101-10.
By analyzing the evolution of BMI, an important aspect was demonstrated at 24 months; there was an increased risk of overweight in preterm infants of hypertensive mothers. There is no data in the literature to justify this result; therefore, the authors' hypothesis is that this finding could reflect excessive catch-up, which may be associated with future complications, including obesity in childhood, adolescence, and adulthood, as well as increased risk of metabolic syndrome.2222 Ibáñez L, Ong K, Dunger DB, de Zegher F. Early development of adiposity and insulin resistance after catch-up weight gain in small-for-gestational-age children. J Clin Endocrinol Metab. 2006;91:2153-8. and 2323 Gaskins RB, LaGasse LL, Liu J, Shankaran S, Lester BM, Bada HS, et al. Small for gestational age and higher birth weight predict childhood obesity in preterm infants. Am J Perinatol. 2010;27:721-30. It is suggested that maternal hypertension may have an impact on growth in premature infants, which occurs in the medium or long term, and warns of the need for prolonged follow-up of these children. More studies are needed to confirm these findings.
As there was a higher risk of overweight in the hypertensive group, maternal hypertension was investigated as a risk factor for growth disorders at 24 months of CA by logistic regression. However, in this analysis, maternal hypertension was not an independent risk factor for growth disorders in both weight and height. The identified risk factors were SGA and inadequate growth in the first year, especially in the first semester of life.
This study has some limitations, as the severity of maternal hypertensive disease was not assessed and the follow-up time was limited to the first 2 years of life. However, the study sample was homogeneous, the loss of the cohort was acceptable (≤ 20%), and the results brought new knowledge on the growth of preterm infants with birth weight between 1,500-2,499 g.
The lack of effect of maternal hypertension on the preterm infant growth can be partly attributed to the fact that maternal disease severity was not evaluated. Nonetheless, this study reinforces two issues that have been highlighted in the literature: the direct influence of fetal growth on postnatal growth and the importance of the early years of life, a critical period for the occurrence of catch-up growth in preterm infants.2121 Rugolo LM. Crescimento e desenvolvimento a longo prazo do prematuro extremo. J Pediatr (Rio J). 2005;81: S101-10.
Kelleher et al.2424 Kelleher KJ, Casey PH, Bradley RH, Pope SK, Whiteside L, Barrett KW, et al. Risk factors and outcomes for failure to thrive in low birth weight preterm infants. Pediatrics. 1993;91:941-8. documented an incidence of 20% of growth failure in low birth weight preterm infants followed until age 3 years and identified SGA as an independent risk factor for growth failure.
The most important results of this study are related to the lack of differences in the growth of preterm infants of normotensive and hypertensive mothers in the first 2 years of life; however, at 24 months, the preterm infants of hypertensive mothers showed higher frequency of overweight, which can translate as a late-manifestation effect of maternal disease. These data indicate the importance of follow-up of preterm infants of hypertensive mothers in the long term, as excess adiposity in early life can later develop into metabolic syndrome, with negative effects on adult health.2222 Ibáñez L, Ong K, Dunger DB, de Zegher F. Early development of adiposity and insulin resistance after catch-up weight gain in small-for-gestational-age children. J Clin Endocrinol Metab. 2006;91:2153-8. and 2525 Victora CG, Barros FC, Horta BL, Martorell R. Short-term ben- efits of catch-up growth for small-for-gestational-age infants. Int J Epidemiol. 2001;30:1325-30.
In conclusion, preterm low birth weight infants born to hypertensive mothers have an increased risk of overweight at 24 months of CA. SGA and inadequate growth in the first year are risk factors for growth disorders at 24 months of CA.
Acknowledgments
The authors would like to thank all the medical and nursing staff who participated in the follow-up of the preterm infants.
References
-
1Roberts CL, Algert CS, Morris JM, Ford JB, Henderson-Smart DJ. Hypertensive disorders in pregnancy: a population-based study. Med J Aust. 2005;182:332-5.
-
2Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol. 2009;33:130-7.
-
3Rugolo LM, Bentlin MR, Trindade CE. Preeclampsia: effect on the fetus and newborn. Neoreviews. 2011;12:e198-206.
-
4Bocca-Tjeertes IF, Kerstjens JM, Reijneveld SA, de Winter AF, Bos AF. Growth and predictors of growth restraint in moderately preterm children aged 0 to 4 years. Pediatrics. 2011;128:e1187-94.
-
5Grisaru-Granovsky S, Reichman B, Lerner-Geva L, Boyko V, Hammerman C, Samueloff A, et al. Mortality and morbidity in preterm small-for-gestational-age infants: a population-based study. Am J Obstet Gynecol. 2012;206(150):e1-7.
-
6Victora CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, et al. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371:340-57.
-
7Habli M, Levine RJ, Qian C, Sibai B. Neonatal outcomes in preg- nancies with preeclampsia or gestational hypertension and in normotensive pregnancies that delivered at 35, 36, or 37 weeks of gestation. Am J Obstet Gynecol. 2007;197(406):e1-7.
-
8Friedman SA, Schiff E, Kao L, Sibai BM. Neonatal outcome after preterm delivery for preeclampsia. Am J Obstet Gynecol. 1995;172:1785-92.
-
9Boomsma JM, van Lingen RA, van Eyck J, Tamminga P, Kollen BJ, van Elburg RM. Short- and long-term outcome of infants born after maternal (pre)-eclampsia, HELLP syndrome and throm- bophilia: a retrospective, cohort study. Eur J Obstet Gynecol Reprod Biol. 2010;153:47-51.
-
10Withagen MI, Wallenburg HC, Steegers EA, Hop WC, Visser W. Morbidity and development in childhood of infants born after temporising treatment of early onset pre-eclampsia. BJOG. 2005;112:910-4.
-
11Beukers F, Cranendonk A, de Vries JI, Wolf H, Lafeber HN, Vriesendorp HC, et al. Catch-up growth in children born growth restricted to mothers with hypertensive disorders of pregnancy. Arch Dis Child. 2013;98:30-5.
-
12Alexander GR, Himes JH, Kaufman RB, Mor J, Kogan M. A United States national reference for fetal growth. Obstet Gynecol. 1996;87:163-8.
-
13World Health Organization (WHO). The WHO Child Growth Stan- dards. 2006. [cited 30 Nov 2011]. Available from: http://www.who.int/childgrowth/em/
» http://www.who.int/childgrowth/em/ -
14Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol. 2000;183:S1-22.
-
15Han Y, Chang EY, Kim J, Ahn K, Kim HY, Hwang EM, et al. Asso- ciation of infant feeding practices in the general population with infant growth and stool characteristics. Nutr Res Pract. 2011;5:308-12.
-
16Ray JG, Burrows RF, Burrows EA, Vermeulen MJ. MOS HIP: McMaster outcome study of hypertension in pregnancy. Early Hum Dev. 2001;64:129-43.
-
17Moura MD, Margotto PR, Rugolo LM. Changes of blood flow in the umbilical artery in hypertensive pregnancy and the impli- cations in the neonatal outcomes. Rev Bras Ginecol Obstet. 2013;35:71-7.
-
18Silveira RC, Procianoy RS, Koch MS, Benjamin AC, Schlindwein CF. Growth and neurodevelopment outcome of very low birth weight infants delivered by preeclamptic mothers. Acta Paedi- atr. 2007;96:1738-42.
-
19Modi M, Saluja S, Kler N, Batra A, Kaur A, Garg P, et al. Growth and neurodevelopmental outcome of VLBW infants at 1 year corrected age. Indian Pediatr. 2013;50:573-7.
-
20Rugolo LM, Bentlin MR, Rugolo AJ, Dalben I, Trindade CE. Growth of extremely low birth weight infants during the first two years of life. Rev Paul Pediatr. 2007;25:142-9.
-
21Rugolo LM. Crescimento e desenvolvimento a longo prazo do prematuro extremo. J Pediatr (Rio J). 2005;81: S101-10.
-
22Ibáñez L, Ong K, Dunger DB, de Zegher F. Early development of adiposity and insulin resistance after catch-up weight gain in small-for-gestational-age children. J Clin Endocrinol Metab. 2006;91:2153-8.
-
23Gaskins RB, LaGasse LL, Liu J, Shankaran S, Lester BM, Bada HS, et al. Small for gestational age and higher birth weight predict childhood obesity in preterm infants. Am J Perinatol. 2010;27:721-30.
-
24Kelleher KJ, Casey PH, Bradley RH, Pope SK, Whiteside L, Barrett KW, et al. Risk factors and outcomes for failure to thrive in low birth weight preterm infants. Pediatrics. 1993;91:941-8.
-
25Victora CG, Barros FC, Horta BL, Martorell R. Short-term ben- efits of catch-up growth for small-for-gestational-age infants. Int J Epidemiol. 2001;30:1325-30.
-
☆
Please cite this article as: Kiy AM, Rugolo LM, Luca AK, Corrente JE. Growth of preterm low birth weight infants until 24 months corrected age: effect of maternal hypertension. J Pediatr (Rio J). 2015;91:256-62.
Publication Dates
-
Publication in this collection
May-Jun 2015
History
-
Received
26 June 2014 -
Accepted
25 July 2014