Abstracts
Background and objectives:
We investigated the effect of dexmedetomidine on ischemic renal failure in rats.
Methods:
In the present study, 26 male adult Wistar albino rats weighting 230-300 g were randomly separated into four groups: sham-operated (n = 5), ischemia reperfusion (IR) (IR group, n = 7), IR/reperfusion treatment with dexmedetomidine (Dex. R group, n = 7) and IR/pre-ischemic treatment with dexmedetomidine (Dex. I group, n = 7). In the first group, sham operation was achieved and renal clamps were not applied. For the IR group, renal ischemia was induced by occlusion of the bilateral renal arteries and veins for 60 min followed by reperfusion for 24 h. For the Dex. R and Dex. I groups, the same surgical procedure as in the IR group was performed, and dexmedetomidine (100 mcg/kg intraperitoneal) was administrated at the 5th min after reperfusion and before ischemia. At the end of reperfusion, blood samples were drawn, the rats were sacrificed, and the left kidney was processed for histopathology.
Results:
The blood urea nitrogen (BUN) levels in groups Dex. R and Dex. I were significantly lower than in the IR group (p = 0.015, p = 0.043), although urine flow was significantly higher in group Dex. R (p = 0.003). The renal histopathological score in the IR group was significantly higher than in the other groups. There was no significant difference between the Dex. R and Dex. I groups.
Conclusions:
The results were shown that administration of dexmedetomidine reduced the renal IR injury histomorphologically. Administration of dexmedetomidine in the reperfusion period was considered as more effective due to increase in urinary output and decrease in BUN levels.
Kidney; Ischemia/reperfusion; Dexmedetomidine; Acute renal failure
Justificativa e objetivos:
Investigar os efeitos de dexmedetomidina sobre a insuficiência renal isquêmica em ratos.
Métodos:
No presente estudo, 26 ratos machos adultos, albinos Wistar, com peso 230-300 g, foram randomicamente divididos em quatro grupos: pseudo-operado (n = 5), isquemia-reperfusão (grupo IR, n = 7), IR/tratamento de reperfusão com dexmedetomidina (grupo Dex-R, n = 7) e IR/tratamento pré-isquemia com dexmedetomidina (grupo Dex-I, n = 7). No primeiro grupo, uma pseudo-operação foi feita e clampeamentos renais não foram aplicados. No grupo IR, isquemia renal foi induzida por oclusão das artérias e veias renais bilaterais durante 60minutos seguida por reperfusão durante 24horas. Nos grupos Dex-R e Dex-I, o mesmo procedimento cirúrgico destinado ao grupo IR foi feito e dexmedetomidina (100mcg/kg intraperitoneal) foi administrada cinco minutos após a reperfusão e antes da isquemia. No fim da reperfusão, amostras de sangue foram coletadas, os ratos foram sacrificados e os rins esquerdos processado para histologia.
Resultados:
Os níveis de nitrogênio ureico no sangue (BUN) dos grupos Dex-R e Dex-I estavam significativamente mais baixos do que os do grupo IR (p = 0,015, p = 0,043), embora o fluxo urinário tenha sido significativamente maior no grupo Dex-R (p = 0,003). O escore histopatológico renal do grupo IR foi significativamente maior do que os dos outros grupos. Não houve diferença significativa entre os grupos Dex-R e Dex-I.
Conclusões:
Os resultados demonstraram que a administração de dexmedetomidina reduziu histomorfologicamente a lesão de IR renal. A administração de dexmedetomidina durante o período de reperfusão foi considerada como mais eficaz por causa do aumento do débito urinário e da diminuição dos níveis de BUN.
Renal; Isquemia/reperfusão; Dexmedetomidina; Insuficiência renal aguda
Justificación y objetivos:
investigar los efectos de la dexmedetomidina sobre la insuficiencia renal isquémica en ratones.
Métodos:
en el presente estudio, 26 ratones machos adultos, albinos Wistar, con un peso de 230-300 g fueron divididos aleatoriamente en 4 grupos: seudooperado (n = 5), isquemia-reperfusión (grupo IR, n = 7), IR/tratamiento de reperfusión con dexmedetomidina (grupo Dex-R, n = 7) e IR/tratamiento preisquemia con dexmedetomidina (grupo Dex-I, n = 7). En el primer grupo, se realizó una seudooperación y no se aplicaron pinzamientos renales. En el grupo IR, la isquemia renal fue inducida por oclusión de las arterias y venas renales bilaterales durante 60 min seguida por reperfusión durante 24 h. En los grupos Dex-R y Dex-I, se llevó a cabo el mismo procedimiento quirúrgico destinado al grupo IR, y la dexmedetomidina (100 µg /kg intraperitoneal) fue administrada 5 min después de la reperfusión y antes de la isquemia. Al final de la reperfusión, fueron recogidas muestras de sangre, los ratones fueron sacrificados y el riñón izquierdo procesado para histología.
Resultados:
los niveles de nitrógeno ureico en la sangre (BUN) de los grupos Dex-R y Dex-I eran significativamente más bajos que los del grupo IR (p = 0,015; p = 0,043), aunque el flujo urinario era significativamente mayor en el grupo Dex-R (p = 0,003). La puntuación histopatológica renal del grupo IR fue significativamente mayor que la de los otros grupos. No hubo diferencia significativa entre los grupos Dex-R y Dex-I.
Conclusiones:
los resultados demostraron que la administración de dexmedetomidina redujo histomorfológicamente la lesión de IR renal. La administración de dexmedetomidina durante el período de reperfusión fue considerada más eficaz debido al aumento de producción de orina y a la disminución de los niveles de nitrógeno ureico en la sangre.
Renal; Isquemia-reperfusión; Dexmedetomidina; Insuficiencia renal aguda
Introduction
Acut renal failure is an acute ischemic response of the kidneys occurring due to hypoperfusion secondary to hypotension, hypovolemia and dehydration as well as ischemia/reperfusion (IR) injury presenting with high mortality and morbidity in clinical practice.11. Thadhani R, Pascual M, Bonventre JV. Acute renal failure. N Engl J Med. 1996;334:1448-60. , 22. Brezis M, Rosen S, Silva P, et al. Renal ischemia: a new perspective. Kidney Int. 1984;26:375-83. and 33. Caron A, Desrosiers RR, Béliveau R. Kidney ischemia reperfusion regulates expression and distribution of tubulin subunits, beta-actin and rho GTPases in proximal tubules. Arch Biochem Biophys. 2004;431:31-46.
Increased microvascular permeability, interstitial edema, impaired vasoregulation, inflammatory cell infiltration, parenchymal cell dysfunction, and acute tubular necrosis (ATN) have been shown in the histopathological studies related to renal IR injury.44. Granger DN, Korthuis RJ. Physiologic mechanisms of postischemic tissue injury. Annu Rev Physiol. 1995;57:311-32. , 55. Brezis M, Rosen S. Hypoxia of the renal medulla-its implications for disease. N Engl J Med. 1995;332:647-55. and 66. Chiao H, Kohda Y, McLeroy P, et al. Alpha-melanocytestimulating hormone protects against renal injury after ischemia in mice and rats. J Clin Invest. 1997;99:1165-72. These changes peaked at the 24th hours after reperfusion and they correlated with increased levels of blood urea nitrogen (BUN) and serum creatinine (Cr) which they are used as an indicator for renal function in clinical settings.77. Williams P, Lopez H, Britt D, et al. Characterization of renal ischemia-reperfusion injury in rats. J Pharmacol Toxicol Methods. 1997;37:1-7. and 88. Billings FT, Chen SW, Kim M, et al. Alpha-2 adrenergic agonists protect against radiocontrast-induced nephropathy in mice. Am J Physiol Renal Physiol. 2008;295:741-8.
Dexmedetomidine is an active dextro-stereoisomer of medetomidine and selective a2-adrenoceptor agonist.99. Wikberg JE, Uhlén S, Chhajlani V. Medetomidine stereoisomers delineate two closely related subtypes of idazoxan (imidazoline) I-receptors in the guinea pig. Eur J Pharmacol. 1991;193:335-400. Dexmedetomidine reduces the plasma levels of catecholamines,1010. Scheinin M, Kallio A, Koulu M, et al. Sedative and cardiovascular effects of medetomidine, a novel seletive alpha2-adrenoceptor agonist, in healthy volunteers. Br J Clin Pharmacol. 1987;24:443-51. and 1111. Kallio A, Scheinin M, Koulu M, et al. Effects of deksmedetomidine, a seletive alpha 2-adrenoceptor agonist, on hemodynamic control mechanisms. Clin Pharmacol Ther. 1989;46:33-42. provides hemodynamic stability during surgery1212. Aho M, Scheinin M, Lehtinen AM, et al. Intramusculary administered deksmedetomidine attenuates hemodynamic and stress hormone responses to gynecologic laparoscopy. Anesth Analg. 1992;75:932-9. and 1313. Talke P, Chen R, Thomas B, et al. The hemodynamic and adrenergic effects of perioperative deksmedetomidine infusion after vascular surgery. Anesth Analg. 2000;90:834-9. and increases the urinary flow rate.1414. Jalonen J, Hynynen M, Kuitunen A, et al. Deksmedetomidine as an anesthetic adjunct in coronary artery bypass grafting. Anesthesiology. 1997;86:331-45. Villela et al.1515. Villela NR, do Nascimento Júnior P, de Carvalho LR, et al. Effects of dexmedetomidine on renal system and on vasopressin plasma levels. Experimental study in dogs. Rev Bras Anestesiol. 2005;55:429-40. , and Frumento et al.1616. Frumento RJ, Logginidou HG, Wahlander S, et al. Deksmedetomidine infusion is associated with enhanced renal function after thoracic surgery. J Clin Anesth. 2006;18:422-6. showed that dexmedetomidine caused aqueous diuresis by reducing central vasopressin secretion and significantly improved renal functions postoperatively in their both clinical and experimental studies. Kocoglu et al.1717. Kocoglu H, Ozturk H, Ozturk H, et al. Effect of deksmedetomidine on ischemia-reperfusion injury in rat kidney a histopathologic study. Renal Failure. 2009;31:70-4. have been studied the effects of dexmedetomidine on renal IR injury. They found improved histological scores at the end of the 45 min of reperfusion following 1 h of complete renal ischemia.
The aim of this study was to examine the histopathologic and biochemical effects of dexmedetomidine administrated two different times (before ischemia and at the beginning of reperfusion) on renal IR injury at 24th hour of reperfusion.
Materials and methods
Twenty-six adult Wistar albino rats weighing 230-300 g were used in this study. The animals were housed in a light controlled room with a 12-h light/dark cycle and allowed access to food and water. Experimental protocols and animal care methods in the experiment were approved by the Experimental Animal Research Committee of our institution.
Rats were divided into four groups: sham operated group (n = 5), IR/untreated group (IR group, n = 7), reperfusion treatment with dexmedetomidine (100 µg/kg at 5 min after the reperfusion, ip) (Dex. R group, n = 7), preischemic treatment with dexmedetomidine (100 µg/kg at 5 min before the ischemia, ip) (Dex. I group, n = 7). The rats were anesthetized with ketamine (50 mg/kg ip) and xylazine hydrochloride (10 mg/kg ip) and bilateral renal pedicles were exposed after laparotomy. After anesthesia, the rats were heated with a heating lamp to maintain a rectal body temperature of 37 °C. Isotonic saline solution accounted of 25% of rat body weight was given intraperitoneally before closure of abdomen. For ischemia and reperfusion injury induced, bilateral renal pedicle occlusion was performed with hemostasis clip for 60 min. At the end ischemic period, the clips were removed for blood reperfusion. In sham operated group, bilateral renal pedicles were exposed without any intervention after laparotomy. The animals exposed to 60 min ischemia were housed in metabolic cages 24 h after reperfusion; 24 h urine samples were collected. At the beginning of study, 1 ml of blood sample was drawn from the lateral tail vein for the measurement of basal renal function parameters before abdominal incision. At the end of reperfusion, the animals were anesthetized, the blood samples were drawn from the right atrium for the measurement of renal function parameters and left kidneys were excised. The kidneys were fixed in 10% buffered formalin and embedded in paraffin wax, cut at 4-5 µm and stained with hematoxylin and eosin for histological studies using light microscope.
Histopathologic changes were analyzed for mononuclear cell infiltration, erythrocyte extravasation, capillary dilatation, renal corpuscle morphology, vacuolization of proximal tubules, apoptosis, loss of tubular brush border, tubular dilatation and cast formation. Tubulointersititial injury was scored as follows: 0 = none, 1 = 0-10%, 2 = 11-25%, 3 = 26-45%, 4 = 46-75%, and 5 = 76-100%.1818. Feng L, Xiong Y, Cheng F, et al. Effect of ligustrazine on ischemia-reperfusion injury in murine kidney. Transplant Proc. 2004;36:1949-51. The scoring of the histological data was performed by blind investigator.
Blood urea nitrogen and plasma Cr levels were measured. Fractional sodium excretion (FANa) and Cr clearance (CCr) were calculated from the following formula: FANa = UNaV/(PNa × creatinine clearance) × 100 (UNaV: urinary sodium, PNa: plasma sodium);1919. Fujii T, Takaoka M, Muraoka T, et al. Preventive effect of lcarnosine on ischemia/reperfusion-induced acute renal failure in rats. Eur J Pharmacol. 2003;474:261-7. CCr = (Urine Cr × urine volume)/(Plasma Cr × time).2020. Hull ME. A new doctor for a men diabetes and hypertension;. In: Scott MG, Gronowski AM, Eby CS, editors. Tietz's applied laboratory medicine. 2nd ed. Hoboken: John Wiley & Sons Inc; 2007. p. 65-74.
For statistical analysis, SPSS 15.0 (Statistical Package for the Social Sciences ver. 15,Chicago, IL, USA) was used. All data were expressed as mean ± standard deviation (mean ± SD). Univariate analysis was conducted via Mann-Whitney U test to compare two independent groups. The level of statistical significance was accepted as p < 0.05.
Results
A total of 26 rats were included in the study. One rat in the IR group died during the ischemia period and was excluded from the study; thus, 25 subjects completed the study. The histopathological scores of the rats in all groups are presented in Table 1.
The histomorphologic injury scores of the sham operated group were statistically significant lower than IR, Dex. I and Dex. R groups (respectively, p = 0.003, p = 0.002, p = 0.002). The scores were significantly higher in the IR group than Dex. I and Dex. R groups (respectively, p = 0.018, p = 0.026). The difference between the scores of the Dex. R and Dex. I groups was not statistically significant (p = 0.59).
Mononuclear cell infiltration
The histomorphologic injury scores of the sham-control group were significantly lower than of the IR, Dex. I and Dex. R groups (respectively, p = 0.01, p = 0.029, p = 0.03). The differences between the scores of the IR, Dex. I and Dex. R groups were not statistically significant (respectively, p = 0.08, p = 0.29). The difference between the scores of the Dex. R and Dex. I groups was not statistically significant (p = 0.59).
Erythrocyte extravasation
The histomorphologic injury scores of the sham-control group were statistically significant lower than IR, Dex. I and Dex. R groups (respectively, p = 0.004, p = 0.002, p = 0.002). The scores of the IR group were significantly higher than Dex. R group (p = 0.03), but there was no statistically significant difference between the scores of the IR and Dex. I groups (p = 0.29).
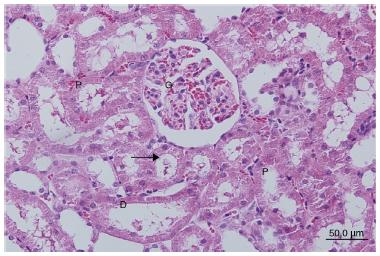
The sham operated group showed normal morphological features. No cell infiltration or loss of tubular brush border was observed (Fig. 1).
The sections of sham operated group. G: glomerulus, P: proximal tubule, D: distal tubule, (→) tubular brush border.
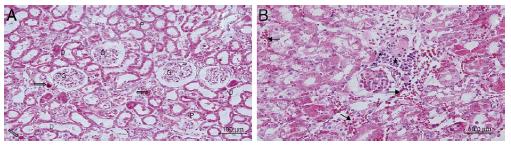
For the IR group, infiltration of mononuclear cells in the peritubular area, especially the cortical area, brush border loss in the proximal tubule cells, tubular atrophy, tubular dilatation, and vacuolization were observed. In some tubules, proteinaceous material deposition with cast formation and cell debris in the lumen of the tubule were observed. In some areas in the cortex, vasodilatation and erythrocyte extravasation were prominent (Fig. 2A-C).
(A) The sections of ischemia reperfusion group. G: glomerulus, P: proximal tubule, D: distal tubule, (→) the accumulation of proteinaceous material at tubules, (→): proximal tubule epithelia cells poured into the lumen. (B) The sections of ischemia reperfusion group. G: glomerulus, P: proximal tubule, D: distal tubule, (→) mononucleer cell infiltration, (→): proximal tubule epithelia cells poured into the lumen. (C) The sections of ischemia reperfusion group. (→) erythrocyte extravasation, (→): tubules and the accumulation of proteinaceous material at tubules.
In the Dex. R group, mononuclear cell infiltration in the peritubular area and erythrocyte extravasation was observed less than in the IR group.
Tubular atrophy, tubular dilation and vacuolization, proteinaceous material deposition in the tubules, and loss of cell debris and brush border to tubule lumen, which were observed in the IR group, were observed less in the Dex. R group (Fig. 3A, Fig. 3B).
(A-B) The sections of reperfusion treatment with dexmedetomidine group. G:glomerulus, P:proximal tubule, D: distal tubule, (→) the apperence that the accumulation of proteinaceus material at tubules reduced compared to other groups.
In the Dex. I group, reductions in mononuclear cell infiltration in the cortical region, especially in the peritubular area and in degeneration tubule cells and erythrocyte extravasation were observed compared to the IR group. (Fig. 4A, Fig. 4B).
(A-B) The sections of preischemic treatment with dexmedetomidine group. G:glomerulus, P:proximal tubule, D: distal tubule, (→) proximal tubule epithelial cells poured into the lumen.
In the histomorphologic comparison of the Dex. R and Dex. I groups, the brush border loss observed in proximal tubule cells, tubular atrophy, tubular dilatation, vacuolization, proteinaceous material deposition in some tubules, cast formation, and cell debris in the lumen of tubules seen in the Dex. I group were observed less in Dex. R group. In the statistical analysis of the semiquantitative light microscopy scoring for these two groups, no statistically significant differences were determined in the scores of erythrocyte extravasation, proximal tubule and mononuclear cell infiltration.
Biochemical parameters
For the IR group, urine volume and CCr were significantly lower (respectively, p = 0.006, p = 0.025) and BUN, blood Cr and FANa excretion levels were significantly higher than in the sham-control group (respectively, p = 0.006, p = 0.006, p = 0.025).
Urine volume was significantly higher in the Dex. R group than in the IR and Dex. I groups (respectively, p = 0.003, p = 0.030) and BUN value was significantly lower in the Dex. R and Dex. I groups than in the IR group (respectively, p = 0.015, p = 0.043). Biochemical data of the groups were presented in Table 2.
Discussion
In this experimental study, a 60-min rat renal IR model was used to create a life-threatening renal injury, which was induced by bilateral clamping of renal vascular structures. Renal injury was examined according to the changes in histomorphology and renal function at the 24th hour of reperfusion. At current study compared to the sham operated group, as signs of this impairment in renal function, a significant decrease in UV and CCr and significant increase in the levels of FANa, BUN and Cr were found in IR group.
In addition, the presence of renal tubular injury was supported by significantly increased histopathologic injury scores compared with the sham operated group. These histological and biochemical findings in accordance with prior studies have shown that IR injury caused both glomerular and tubular dysfunction in the kidney.1717. Kocoglu H, Ozturk H, Ozturk H, et al. Effect of deksmedetomidine on ischemia-reperfusion injury in rat kidney a histopathologic study. Renal Failure. 2009;31:70-4. , 1919. Fujii T, Takaoka M, Muraoka T, et al. Preventive effect of lcarnosine on ischemia/reperfusion-induced acute renal failure in rats. Eur J Pharmacol. 2003;474:261-7. and 2121. Hussein Ael-A, Shokeir AA, Sarhan ME, et al. Effects of combined erythropoietin and epidermal growth factor on renal ischaemia/reperfusion injury: a randomized experimental controlled study. BJU Int. 2011;107:323-8.
In the previous studies in which renal IR injury models were created, different ischemia and reperfusion durations were applied.77. Williams P, Lopez H, Britt D, et al. Characterization of renal ischemia-reperfusion injury in rats. J Pharmacol Toxicol Methods. 1997;37:1-7. , 1717. Kocoglu H, Ozturk H, Ozturk H, et al. Effect of deksmedetomidine on ischemia-reperfusion injury in rat kidney a histopathologic study. Renal Failure. 2009;31:70-4. , 1919. Fujii T, Takaoka M, Muraoka T, et al. Preventive effect of lcarnosine on ischemia/reperfusion-induced acute renal failure in rats. Eur J Pharmacol. 2003;474:261-7. , 2020. Hull ME. A new doctor for a men diabetes and hypertension;. In: Scott MG, Gronowski AM, Eby CS, editors. Tietz's applied laboratory medicine. 2nd ed. Hoboken: John Wiley & Sons Inc; 2007. p. 65-74. and 2222. Gu J, Sun P, Zhao H, et al. Dexmedetomidine provides renoprotection against ischemia-reperfusion injury in mice. Crit Care. 2011;15:153. Williams et al.77. Williams P, Lopez H, Britt D, et al. Characterization of renal ischemia-reperfusion injury in rats. J Pharmacol Toxicol Methods. 1997;37:1-7. created ischemia for 45 min with application of clips at the bilateral renal arteries and veins and investigated the effects of IR injury on blood BUN and Cr levels and renal histology, at reperfusion for 0, 0.5, 1, 2, 4, 6, 9, and 24 h and after 1 week. These investigators reported that the earliest renal injury started at the 4th h following ischemia for 45 min and peaked at the 24th hour. Similarly, Yamamoto et al.2323. Yamamoto K, Wilson DR, Baumal R. Outer medullary circulatory defect in ischemic acute renal failure. Am J Pathol. 1984;116:253-61. and Arendshorst et al.2424. Arendshorst WJ, Finn WF, Gottschalk CW. Pathogenesis of acute renal failure following temporary renal ischemia in the rat. Circ Res. 1975;37:558-68. showed that ATN and medullary perfusion defect became more manifest after 22-48 h of reperfusion. Gu et al.2222. Gu J, Sun P, Zhao H, et al. Dexmedetomidine provides renoprotection against ischemia-reperfusion injury in mice. Crit Care. 2011;15:153. created a moderate renal damage with application of clips on bilateral renal pedicles for 25 min. For a life-threatening renal injury in rats, they performed that clip application on the right renal pedicle for 40 min, harvesting the left kidney. These researchers showed that plasma mean Cr and urea levels increased more than 7 times at the 24th hour of reperfusion following ischemia for 40 min. Kocoglu et al.1717. Kocoglu H, Ozturk H, Ozturk H, et al. Effect of deksmedetomidine on ischemia-reperfusion injury in rat kidney a histopathologic study. Renal Failure. 2009;31:70-4. documented histological data of reperfusion injury for 45 min following 60-min ischemia on the left kidney of rats subjected to right kidney nephrectomy. In our study, a 60-min ischemia model was created with application of clips on bilateral renal pedicles, and the effects of IR and dexmedetomidine treatments were studied 24 hours after reperfusion. Acute renal failure due to ischemia is a complex syndrome involving renal vasoconstriction, tubular damage, tubular cell necrosis, glomerular filtration failure, and glomerular damage.2525. Bird JE, Milhoan K, Wilson CB, et al. Ischemic acute renal failure and antioxidant therapy in the rat: the relation between glomerular and tubular dysfunction. J Clin Invest. 1988;81:1630-8. and 2626. Weinberg JM. The cell biology of ischemic renal injury. Kidney Int. 1991;39:476-500. The medications that may be effective on the various factors that contribute to this damage have been used in prophylaxis and treatment. Sympathetic activation due to presynaptic release of noradrenaline and increase in noradrenaline levels in the circulation induced by stress in the kidney, and accordingly, reduction in renal blood flow and glomerular filtration, has been suggested as one of the possible mechanisms of acute renal failure produced by IR injury.
Dexmedetomidine is a selective and potent a2-adrenoceptor agonist. Dexmedetomidine has been reported to have effective protective efficacy on focal ischemia in rabbits, and cardiac ischemia, reperfusion injury, and incomplete forebrain ischemia in rats.2727. Hoffman WE, Kochs E, Werner C, et al. Deksmedetomidine improves neurologic outcome from incomplete ischemia in the rat. Reversal by the alpha 2-adrenergic antagonist atipamezole. Anesthesiology. 1991;75:328-32. , 2828. Maier CM, Sun GH, Kunis DM, et al. Neuroprotection by the N- methyl- d- aspartate receptor antagonist CGP 40116: In vivo and in vitro studies. J Neurochem. 1995;65:652-9. and 2929. Koçŏglu H, Karaaslan K, Gonca E, et al. Preconditioning effects of dexmedetomidine on myocardial ischemia/reperfusion injury in rats. Curr Ther Res. 2008;69:150-8. The precise mechanism of the protective effect of a2-adrenergic agonists in the brain is unclear. Catecholaminergic neurotransmission is considered to possibly be related to this effect. Dexmedetomidine reduces excessive secretion of noradrenaline due to ischemia by activating presynaptic a2-adrenoceptor. This prevents excessive noradrenaline metabolism, which causes the formation of free radicals. It is suggested that protection in brain injury provided with H2O2 production decreases in reperfusion due to prevention of oxidative deamination of catecholamines.3030. Simonson SG, Zhang J, Canada Jr AT, et al. Hydrogen peroxide production by monoamine oxidase during ischemia-reperfusion in the rat brain. J Cereb Blood Flow Metab. 1993;13:125-34. and 3131. Suzuki T, Akaike N, Ueno K, et al. MAO inhibitors, clorgyline and lazabemide, prevent hydroxyl radical generation caused by brain ischemiarreperfusion in mice. Pharmacology. 1995;50:357-62. In addition, dexmedetomidine is considered to cause reduction in necrotic cell death by decreased sympathetic tone, as well as inhibition of ion flow mediated by N-methyl-D-aspartate receptor.3232. Engelhard K, Werner C, Eberspächer E, et al. The effect of the alpha 2-agonist deksmedetomidine and the N-methyl- d- aspartate antagonist S(+)-ketamine on the expression of apoptosis regulating proteins after incomplete cerebral ischemia and reperfusion in rats. Anesth Analg. 2003;96:524-31. In addition to these possible mechanisms, Engelhard et al.3232. Engelhard K, Werner C, Eberspächer E, et al. The effect of the alpha 2-agonist deksmedetomidine and the N-methyl- d- aspartate antagonist S(+)-ketamine on the expression of apoptosis regulating proteins after incomplete cerebral ischemia and reperfusion in rats. Anesth Analg. 2003;96:524-31. reported that dexmedetomidine caused an increase in the concentration of antiapoptotic proteins. In another study, Wijeysundera et al.3333. Wijeysundera DN, Naik JS, Beattie WS. Alpha-2 adrenergic agonists to prevent perioperative cardiovascular complications: a meta-analysis. Am J Med. 2003;114:742-52. suggested that a2-adrenergic agonists reduced mortality and myocardial infarction in vascular surgery. In the earlier studies, the anti-ischemic effect of dexmedetomidine was demonstrated to occur in high-dose administration, as 100 µg/kg; therefore, in our study, 100 µg/kg dose of dexmedetomidine was used for renal IR injury.1717. Kocoglu H, Ozturk H, Ozturk H, et al. Effect of deksmedetomidine on ischemia-reperfusion injury in rat kidney a histopathologic study. Renal Failure. 2009;31:70-4. , 2727. Hoffman WE, Kochs E, Werner C, et al. Deksmedetomidine improves neurologic outcome from incomplete ischemia in the rat. Reversal by the alpha 2-adrenergic antagonist atipamezole. Anesthesiology. 1991;75:328-32. and 3434. Hoffman WE, Baughman VL, Albrecht RF. Interaction of catecholamines and nitrous oxide ventilation during incomplete brain ischemia in rats. Anesth Analg. 1993;77: 908-12.
Kocoglu et al.1717. Kocoglu H, Ozturk H, Ozturk H, et al. Effect of deksmedetomidine on ischemia-reperfusion injury in rat kidney a histopathologic study. Renal Failure. 2009;31:70-4. reported that dexmedetomidine dose of 100 µg/kg i.p. administered at the start of reperfusion prevents the injury produced by 60-min ischemia and followed by reperfusion of 45 min, which caused acute renal failure, and they showed normal glomeruli and a slight edema of tubular cells. In our study, different from that of Kocoglu et al.1717. Kocoglu H, Ozturk H, Ozturk H, et al. Effect of deksmedetomidine on ischemia-reperfusion injury in rat kidney a histopathologic study. Renal Failure. 2009;31:70-4. , dexmedetomidine was used at two different times: at the beginning of reperfusion and before ischemia. Additionally, whether the renoprotective effect continued until the 24th hour when IR injury peaked, was evaluated by using histopathological examination and renal function tests. Our study has shown that mononuclear cell infiltration, brush border loss of proximal tubule cells, tubular atrophy, tubular dilatation, vacuolization, protein and cell debris accumulation in some tubules, and erythrocyte extravasation were seen in the IR group. We also showed that proximal tubule changes, which were seen in the IR group, decreased significantly in both groups treated with dexmedetomidine, and further, erythrocyte extravasation changes decreased significantly in the group administered dexmedetomidine in the reperfusion period. These histologic findings have shown that, dexmedetomidine had a partial renoprotective effect in both groups in the 24th hour of reperfusion.
Gu et al.2222. Gu J, Sun P, Zhao H, et al. Dexmedetomidine provides renoprotection against ischemia-reperfusion injury in mice. Crit Care. 2011;15:153. investigated the effects of dexmedetomidine in both human cell cultures as in vitro and with rats as in vivo studies. Their in vitro studies demonstrated that dexmedetomidine provided protection of tubular structure and prevention of cell death with activation of the Akt pathway and weakening of the HMGB1/TLR4 pathway mediated by a2- adrenergic receptor. They demonstrated in their in vivo studies with rats that the administration of dexmedetomidine at a dose of 25 µg/kg i.p. before ischemia caused a significant reduction in the levels of urea, and Cr increased at the 24th hour, due to the effect of ischemia produced by a 25-min application of clips to bilateral renal pedicles. The investigators also showed a reduction in histological damage scores, at 53% and 38%, respectively, with pre- and post-ischemic dexmedetomidine. Again, in that same study, it was reported that renal function deterioration produced by ischemia for 40 min, which was more serious (seven fold at 24th hour after IR injury), significantly decreased with both pre- and post-ischemic treatment and this effect was dependent on a2 adrenoreceptor. In our study, similarly with the results of Gu et al.2222. Gu J, Sun P, Zhao H, et al. Dexmedetomidine provides renoprotection against ischemia-reperfusion injury in mice. Crit Care. 2011;15:153. , we found that renal histology and function (for only BUN levels) improved significantly with dexmedetomidine used pre- and post-ischemia in more severe IR injury. Furthermore, Curtis et al.3535. Curtis FG, Vianna PT, Viero RM, et al. Dexmedetomidine and S(+)-ketamine in ischemia and reperfusion injury in the rat kidney. Acta Cir Bras. 2011;26:202-6. studied the effects of dexmedetomidine on renal histological changes and blood Cr level after IR injury in rats anesthetized with ketamin. These investigators, different from us, administered an a2-adrenoceptor agonist dose of 1 µg/kg intravenous (i.v.) for 10 min and continued with a dose of 1 µg/kg/h. In that study, ischemia time was 45 min, and nephrectomy and blood sampling were performed 48 h after reperfusion.
In accordance with our and Gu et al.2222. Gu J, Sun P, Zhao H, et al. Dexmedetomidine provides renoprotection against ischemia-reperfusion injury in mice. Crit Care. 2011;15:153. studies, they also demonstrated that dexmedetomidine protected the kidneys partially against IR injury at late period of reperfusion.
In their experimental study, Villela et al.1515. Villela NR, do Nascimento Júnior P, de Carvalho LR, et al. Effects of dexmedetomidine on renal system and on vasopressin plasma levels. Experimental study in dogs. Rev Bras Anestesiol. 2005;55:429-40. reported that, followed by administration of low dose dexmedetomidine (1 and 2 µg/kg bolus dose application followed by 1 and 2 µg/kg, 1-h i.v. infusion) to the dogs under anesthesia caused free water diuresis with decrease in urine osmolality and plasma vasopressin levels. Frumento et al.1616. Frumento RJ, Logginidou HG, Wahlander S, et al. Deksmedetomidine infusion is associated with enhanced renal function after thoracic surgery. J Clin Anesth. 2006;18:422-6. demonstrated improvement in postoperative renal function with infusion of dexmedetomidine in patients without renal disease who underwent thoracic surgery, by using glomerular filtration indicators involving urine flow, serum Cr and fractional changes of serum Cr level. In that study, decrease in serum Cr levels peaked in the first postoperative week. The decrease of Cr levels identified in the period of without drug administration was accepted as proof of the beneficial effect of the drug on glomerular filtration. According to Frumento et al.1616. Frumento RJ, Logginidou HG, Wahlander S, et al. Deksmedetomidine infusion is associated with enhanced renal function after thoracic surgery. J Clin Anesth. 2006;18:422-6. , the improvement in renal function was related with decreased renal vasoconstriction by dexmedetomidine. In our study, different from these investigators, we determined limited recovery in biochemical renal parameters in IR injury. In this study, in both groups administered dexmedetomidine, BUN values were determined to be significantly lower than in the IR group. In addition, administration of dexmedetomidine at the 5th min of reperfusion provided a significant increase in uriner output. However, this improvement determined in diuresis and BUN levels could not be shown in blood Cr levels and CCr, which are more specific, tests for the kidney. The results of our study suggest that, a partial histomorphological and a functional protection were obtained with dexmedetomidine in renal IR injury.
In the present study, Ketamine-Xylazine (KX) was used as the anesthetic regimen which was appropriate for ischemia-reperfusion studies. As ketamine is compatible with the other medications and has a wide confidence interval, it is one of the anesthetic drugs with the widest usage range in experimental studies. Previous studies in the medical literature had conflicting results on the effect of ketamine in renal IR injury.3535. Curtis FG, Vianna PT, Viero RM, et al. Dexmedetomidine and S(+)-ketamine in ischemia and reperfusion injury in the rat kidney. Acta Cir Bras. 2011;26:202-6. , 3636. Yuzer H, Yuzbasioglu MF, Ciralik H, et al. Effects of intravenous anesthetics on renal ischemia/reperfusion injury. Renal Failure. 2009;31:290-6. , 3737. Rusafa Neto E, Vianna PT, Viero RM, et al. Influence of S(+)-ketamine analgesia in renal intraoperative ischemia. Histological study in rats. Acta Cir Bras. 2006;21:242-6. and 3838. Lee HT, Ota-Setlik A, Fu Y, et al. Differential protective effects of volatile anesthetics against renal ischemia-reperfusion injury in vivo. Anesthesiology. 2004;101:1313-24. These studies in the literature that compare different anesthetics lack a true control group. Similarly, one limitation to our study is lack of a true control (no anesthetic drug) group, as all animals received KX as the anesthetic regimen in accordance with our institutional ethics committee. Therefore we could not determine the extent of protection induced by the KX anesthesia compared with a 'no-drug' group. In order to standardize the effect of anesthetic regimen in our study, the anesthesia was provided by KX in all the groups. In addition; there were sham and control (IR) groups in our study and when we evaluated the results of these groups, in which no active material was used apart from the KX anesthesia, renal I/R injury was not observed in the sham group but occurred in the control group. Therefore, we are convinced that the results we obtained were independent from the effect of KX anesthesia.
In conclusion, dexmedetomidine used both before ischemia and after reperfusion reduced the effects of renal IR injury at the 24th hour histomorphologically. Although no histomorphologic significant difference was determined between the two methods, administration of dexmedetomidine in the reperfusion period was considered more effective due to the decrease in BUN levels and increase in urinary output.
References
-
1Thadhani R, Pascual M, Bonventre JV. Acute renal failure. N Engl J Med. 1996;334:1448-60.
-
2Brezis M, Rosen S, Silva P, et al. Renal ischemia: a new perspective. Kidney Int. 1984;26:375-83.
-
3Caron A, Desrosiers RR, Béliveau R. Kidney ischemia reperfusion regulates expression and distribution of tubulin subunits, beta-actin and rho GTPases in proximal tubules. Arch Biochem Biophys. 2004;431:31-46.
-
4Granger DN, Korthuis RJ. Physiologic mechanisms of postischemic tissue injury. Annu Rev Physiol. 1995;57:311-32.
-
5Brezis M, Rosen S. Hypoxia of the renal medulla-its implications for disease. N Engl J Med. 1995;332:647-55.
-
6Chiao H, Kohda Y, McLeroy P, et al. Alpha-melanocytestimulating hormone protects against renal injury after ischemia in mice and rats. J Clin Invest. 1997;99:1165-72.
-
7Williams P, Lopez H, Britt D, et al. Characterization of renal ischemia-reperfusion injury in rats. J Pharmacol Toxicol Methods. 1997;37:1-7.
-
8Billings FT, Chen SW, Kim M, et al. Alpha-2 adrenergic agonists protect against radiocontrast-induced nephropathy in mice. Am J Physiol Renal Physiol. 2008;295:741-8.
-
9Wikberg JE, Uhlén S, Chhajlani V. Medetomidine stereoisomers delineate two closely related subtypes of idazoxan (imidazoline) I-receptors in the guinea pig. Eur J Pharmacol. 1991;193:335-400.
-
10Scheinin M, Kallio A, Koulu M, et al. Sedative and cardiovascular effects of medetomidine, a novel seletive alpha2-adrenoceptor agonist, in healthy volunteers. Br J Clin Pharmacol. 1987;24:443-51.
-
11Kallio A, Scheinin M, Koulu M, et al. Effects of deksmedetomidine, a seletive alpha 2-adrenoceptor agonist, on hemodynamic control mechanisms. Clin Pharmacol Ther. 1989;46:33-42.
-
12Aho M, Scheinin M, Lehtinen AM, et al. Intramusculary administered deksmedetomidine attenuates hemodynamic and stress hormone responses to gynecologic laparoscopy. Anesth Analg. 1992;75:932-9.
-
13Talke P, Chen R, Thomas B, et al. The hemodynamic and adrenergic effects of perioperative deksmedetomidine infusion after vascular surgery. Anesth Analg. 2000;90:834-9.
-
14Jalonen J, Hynynen M, Kuitunen A, et al. Deksmedetomidine as an anesthetic adjunct in coronary artery bypass grafting. Anesthesiology. 1997;86:331-45.
-
15Villela NR, do Nascimento Júnior P, de Carvalho LR, et al. Effects of dexmedetomidine on renal system and on vasopressin plasma levels. Experimental study in dogs. Rev Bras Anestesiol. 2005;55:429-40.
-
16Frumento RJ, Logginidou HG, Wahlander S, et al. Deksmedetomidine infusion is associated with enhanced renal function after thoracic surgery. J Clin Anesth. 2006;18:422-6.
-
17Kocoglu H, Ozturk H, Ozturk H, et al. Effect of deksmedetomidine on ischemia-reperfusion injury in rat kidney a histopathologic study. Renal Failure. 2009;31:70-4.
-
18Feng L, Xiong Y, Cheng F, et al. Effect of ligustrazine on ischemia-reperfusion injury in murine kidney. Transplant Proc. 2004;36:1949-51.
-
19Fujii T, Takaoka M, Muraoka T, et al. Preventive effect of lcarnosine on ischemia/reperfusion-induced acute renal failure in rats. Eur J Pharmacol. 2003;474:261-7.
-
20Hull ME. A new doctor for a men diabetes and hypertension;. In: Scott MG, Gronowski AM, Eby CS, editors. Tietz's applied laboratory medicine. 2nd ed. Hoboken: John Wiley & Sons Inc; 2007. p. 65-74.
-
21Hussein Ael-A, Shokeir AA, Sarhan ME, et al. Effects of combined erythropoietin and epidermal growth factor on renal ischaemia/reperfusion injury: a randomized experimental controlled study. BJU Int. 2011;107:323-8.
-
22Gu J, Sun P, Zhao H, et al. Dexmedetomidine provides renoprotection against ischemia-reperfusion injury in mice. Crit Care. 2011;15:153.
-
23Yamamoto K, Wilson DR, Baumal R. Outer medullary circulatory defect in ischemic acute renal failure. Am J Pathol. 1984;116:253-61.
-
24Arendshorst WJ, Finn WF, Gottschalk CW. Pathogenesis of acute renal failure following temporary renal ischemia in the rat. Circ Res. 1975;37:558-68.
-
25Bird JE, Milhoan K, Wilson CB, et al. Ischemic acute renal failure and antioxidant therapy in the rat: the relation between glomerular and tubular dysfunction. J Clin Invest. 1988;81:1630-8.
-
26Weinberg JM. The cell biology of ischemic renal injury. Kidney Int. 1991;39:476-500.
-
27Hoffman WE, Kochs E, Werner C, et al. Deksmedetomidine improves neurologic outcome from incomplete ischemia in the rat. Reversal by the alpha 2-adrenergic antagonist atipamezole. Anesthesiology. 1991;75:328-32.
-
28Maier CM, Sun GH, Kunis DM, et al. Neuroprotection by the N- methyl- d- aspartate receptor antagonist CGP 40116: In vivo and in vitro studies. J Neurochem. 1995;65:652-9.
-
29Koçŏglu H, Karaaslan K, Gonca E, et al. Preconditioning effects of dexmedetomidine on myocardial ischemia/reperfusion injury in rats. Curr Ther Res. 2008;69:150-8.
-
30Simonson SG, Zhang J, Canada Jr AT, et al. Hydrogen peroxide production by monoamine oxidase during ischemia-reperfusion in the rat brain. J Cereb Blood Flow Metab. 1993;13:125-34.
-
31Suzuki T, Akaike N, Ueno K, et al. MAO inhibitors, clorgyline and lazabemide, prevent hydroxyl radical generation caused by brain ischemiarreperfusion in mice. Pharmacology. 1995;50:357-62.
-
32Engelhard K, Werner C, Eberspächer E, et al. The effect of the alpha 2-agonist deksmedetomidine and the N-methyl- d- aspartate antagonist S(+)-ketamine on the expression of apoptosis regulating proteins after incomplete cerebral ischemia and reperfusion in rats. Anesth Analg. 2003;96:524-31.
-
33Wijeysundera DN, Naik JS, Beattie WS. Alpha-2 adrenergic agonists to prevent perioperative cardiovascular complications: a meta-analysis. Am J Med. 2003;114:742-52.
-
34Hoffman WE, Baughman VL, Albrecht RF. Interaction of catecholamines and nitrous oxide ventilation during incomplete brain ischemia in rats. Anesth Analg. 1993;77: 908-12.
-
35Curtis FG, Vianna PT, Viero RM, et al. Dexmedetomidine and S(+)-ketamine in ischemia and reperfusion injury in the rat kidney. Acta Cir Bras. 2011;26:202-6.
-
36Yuzer H, Yuzbasioglu MF, Ciralik H, et al. Effects of intravenous anesthetics on renal ischemia/reperfusion injury. Renal Failure. 2009;31:290-6.
-
37Rusafa Neto E, Vianna PT, Viero RM, et al. Influence of S(+)-ketamine analgesia in renal intraoperative ischemia. Histological study in rats. Acta Cir Bras. 2006;21:242-6.
-
38Lee HT, Ota-Setlik A, Fu Y, et al. Differential protective effects of volatile anesthetics against renal ischemia-reperfusion injury in vivo. Anesthesiology. 2004;101:1313-24.
Publication Dates
-
Publication in this collection
May-Jun 2014
History
-
Received
10 Jan 2013 -
Accepted
10 June 2013