Abstracts
Fanconi anemia is a rare autosomal recessive inherited bone marrow failure syndrome with congenital and hematological abnormalities. Literature regarding the anesthetic management in these patients is limited. A management of a developmental dislocation of the hip was described in a patient with fanconi anemia. Because of the heterogeneous nature, a patient with fanconi anemia should be established thorough preoperative evaluation in order to diagnose on clinical features. In conclusion, we preferred caudal anesthesia in this patient with fanconi anemia without thrombocytopenia, because of avoiding from N2O, reducing amount of anesthetic, existing microcephaly, hypothyroidism and elevated liver enzymes, providing postoperative analgesia, and reducing amount of analgesic used postoperatively.
Fanconi anemia; Caudal anesthesia; Developmental dislocation of the hip
A anemia de Fanconi é uma síndrome hereditária autossômica recessiva rara, caracterizada por deficiência da medula óssea e anomalias congênitas e hematológicas. A literatura sobre o manejo anestésico dos pacientes é limitada. O manejo de uma displasia do desenvolvimento do quadril foi descrito em um paciente com anemia de Fanconi. Por causa da natureza heterogênea, um paciente com anemia de Fanconi deve ser submetido à avaliação pré-operatória para diagnosticar as características clínicas. Em conclusão, o bloqueio caudal foi a nossa escolha para esse paciente com anemia de Fanconi, sem trombocitopenia, para evitar o N2O, reduzir a quantidade de anestésico, a microcefalia existente, o hipotireoidismo e o aumento das enzimas hepáticas, proporcionar analgesia pós-operatória e reduzir a quantidade de analgésico usada no pós-operatório.
Anemia de Fanconi; Bloqueio caudal; Displasia do desenvolvimento do quadril
La anemia de Fanconi es un síndrome hereditario autosómico recesivo raro, caracterizado por deficiencia de la médula ósea y por anomalías congénitas y hematológicas. La literatura sobre el manejo anestésico de esos pacientes es limitada. El manejo de una displasia del desarrollo de la cadera fue descrito en un paciente con anemia de Fanconi. Debido a la naturaleza heterogénea, un paciente con anemia de Fanconi debe ser sometido a la evaluación preoperatoria para diagnosticar las características clínicas. En conclusión, el bloqueo caudal fue nuestra elección para ese paciente con anemia de Fanconi sin trombocitopenia para evitar el N2O, reducir la cantidad de anestésico, microcefalia existente, hipotiroidismo y aumento de las enzimas hepáticas, proporcionar analgesia postoperatoria y reducir la cantidad de analgésico usado en el postoperatorio.
Anemia de Fanconi; Bloqueo caudal; Displasia del desarrollo de la cadera
Introduction
Fanconi anemia (FA) is a rare autosomal recessive inherited bone marrow failure syndrome, characterized by increased chromosomal fragility, and generally associated with multiple congenital anomalies.11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12.
Literature regarding the anesthetic management in these patients is limited. A management of a developmental dislocation of the hip was described in a patient with FA.
Case report
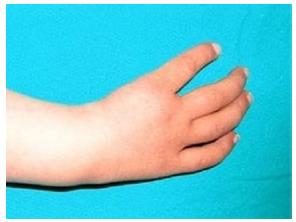
A 2.5-year-old girl, born to first degree consanguineous parents presented with a failure to walking. She was delivered by spontaneous vaginal in time and small for gestational age, weighing 2.2 kg at birth. Physical examination revealed retarded growth (5.7 kg weight and 68 cm height) with absence of bilateral thumb (Fig. 1), café au lait spots at back, hypopigmentation at abdomen, generalized hyperpigmentation, and microcephaly.
Laboratory investigations did not reveal pancytopenia; hemoglobin, WBC and platelets were 11.4 g dl-1, 7.4 × 103 dl-1 and 162 × 103 dl-1 respectively. ALP, GGT and LDH levels were elevated and 564, 420 and 289 respectively. Ultrasound revealed hypoplastic horseshoe kidney.
The patient's medication included only levothyroxine because of hypothyroidism. No medication exist related FA.
Other investigations including electrolytes, BUN, creatinine, bilirubins, AST, ALT, prothrombin time, partial thromboplastin time, ECG, and echocardiogram were normal. The patient was euthyroidic.
Evaluation of the airway revealed no abnormalities, except microcephaly, and vital signs were normal. Adequate blood and blood products ordered depending on the procedure.
No medication was administered prior to the procedure apart from antibiotics. Anesthesia was induced with 8% sevoflurane in 100% oxygen. After peripheral i.v. access was secured, she was turned to the left lateral position. Caudal block was performed by using a 22-gauge short-bevel needle under aseptic conditions with bupivacaine 0.25% at 1 ml kg-1. After caudal blockade inhalation anesthesia was lowered to 0.5-1% in 100% oxygen in order to obtain 4 or 5 point of Ramsay sedation scale. Peripheral oxygen saturation (SpO2), heart rate, noninvasive blood pressure and end-tidal CO2 (ETCO2) were monitored throughout surgery. Ventilation was maintained via an oxygen mask with 2 L dk-1 fresh flow spontaneously (Fig. 2).
Whole procedure including open reduction and putting the limb in a plaster cast from induction to recovery lasted 140 min and was uneventful. Recovery was fast and uneventful. Postoperative analgesia was not required for ten hours.
Discussion
Fanconi anemia is an autosomal recessive disorder in over 99% of cases with 25% risk to siblings.11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. The incidence of FA is approximately three per million and the heterozygote frequency is estimated at one in 300 in Europe and the USA,22. Tischkowitz MD, Hodgson SV. Fanconi anaemia. J Med Genet. 2003;40:1-10. 1/100 in Ashkenazi Jews and South African Afrikaners due to "founder effect".11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. and 33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365. Consanguinity has been implicated in its incidence.33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365.
Clinical features of FA can be broadly divided into two categories: congenital abnormalities and hematological abnormalities, which may include altered skin pigmentation and/or café au lait spots, short stature (impaired growth hormone secretion), thumb or thumb and radial anomalies, hip anomalies, vertebral scoliois, rib anomalies, male hypogenitalism, mental retardation, anorectal atresia, duodenal atresia, microcephaly, eye anomalies (microphthalmia, strabismus, ptosis, nystagmus), structural renal defects, low-birth weight, developmental delay, abnormal ears or hearing, and cardiopulmonary defects.11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. , 22. Tischkowitz MD, Hodgson SV. Fanconi anaemia. J Med Genet. 2003;40:1-10. and 33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365. The most important clinical features of FA are hematological. Pancytopenia is the usual finding and typically presents between the ages of 5 and 10 years, the median age of onset being 7 years.11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. Clinically, the affected FA patient may present with bleeding, pallor and/or recurring infections.22. Tischkowitz MD, Hodgson SV. Fanconi anaemia. J Med Genet. 2003;40:1-10. The major cause of death in FA is bone marrow failure, followed in frequency by leukemia and solid tumors. The projected median survival from all causes for more than 1000 cases reported in the literature is age 20 years.33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365. Of patients thirty or forty percent lack obvious physical abnormalities.11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. , 22. Tischkowitz MD, Hodgson SV. Fanconi anaemia. J Med Genet. 2003;40:1-10. and 33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365. There is great clinical heterogeneity even within a genotype (sibling may be phenotypically different).11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. The gold-standard screening test for FA is based on the characteristic hypersensitivity of FA cells to the crosslinking agents, such as mitomycin C (MMC) or diepoxybutane (DEB).55. Auerbach AD. Fanconi anemia diagnosis and the diepoxybutane (DEB) test. Exp Hematol. 1993;21:731-3. FANCA is the most common complementation group, representing about 70% of cases.11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. Androgen therapy (oxymetholone), cytokines (G-CSF and GM-CSF), and supportive therapies such as blood and platelet transfusions form the mainstay of treatment prior to allogeneic hematopoietic stem cell transplantation. Gene therapy is experimental. E-amino caproic acid may be used for symptomatic bleeding. Steroids are occasionally used.11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. , 22. Tischkowitz MD, Hodgson SV. Fanconi anaemia. J Med Genet. 2003;40:1-10. and 33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365. FA frequently terminates in myelodysplastic syndrome and/or leukemia.11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. Hematopoietic stem cell transplantation (bone marrow, cord blood, or peripheral blood stem cells) may cure aplastic anemia and prevent myelodysplastic syndrome or leukemia.22. Tischkowitz MD, Hodgson SV. Fanconi anaemia. J Med Genet. 2003;40:1-10. and 33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365.
Patients with FA may present for procedures such as Hickman catheter insertion for bone marrow transplantation, limb reconstructive surgeries, splenectomy, gastrointestinal anomalies, congenital heart defects, trauma or other related and/or non-related indications. The insufficiency of literature regarding anesthetic management of this condition makes it difficult to estimate the real impact of individual anomalies on the perioperative management.66. Jacop R, Venkatesan T. Anesthesia and Fanconi anemia. Paediatr Anaesth. 2006;16:981-5. It is important to emphasize that of patients thirty or forty percent have no abnormalities.11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. , 22. Tischkowitz MD, Hodgson SV. Fanconi anaemia. J Med Genet. 2003;40:1-10. and 33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365.
Because of the heterogeneous nature of the condition, FA is difficult to diagnose on clinical features.22. Tischkowitz MD, Hodgson SV. Fanconi anaemia. J Med Genet. 2003;40:1-10. A thorough preoperative evaluation includes airway examination, and hematological, cardiopulmonary, hepatorenal and endocrine evaluation for any component of the disease or any complication of the treatment of the disease. For example hyperbilirubinemia and hepatomegaly with fatty infiltrates could be attributed to therapy with androgen. All transfusions and any transfusion reactions must be documented.66. Jacop R, Venkatesan T. Anesthesia and Fanconi anemia. Paediatr Anaesth. 2006;16:981-5. Adequate blood and blood products should be ordered depending on the procedure. No family member should be used as a blood product donor until it has been determined that a transplant will not be performed.33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365. Leukocyte-filtered blood products should be used to reduce reactions and HLA sensitization in case of future stem cell transplant. Similarly, single-donor platelets are preferred to reduce the frequency of antibody formation.33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365.
Because thrombocytopenia usually develops initially,44. Dror Y. Inhereted bone marrow failure syndromes. In: Arceci ˙ JR, Hann MI, Smith PO, editors. Pediatric hematology. 3rd edn. Massachusetts: Blacwell Publishing; 2006. p. 32-7. particularly, thrombocyte count should be evaluated. Repeated respiratory tract infections and neutropenic sepsis may be present because of pancytopenia. Children with neutropenic sepsis may have subclinical coagulopathy that should be corrected preoperatively.77. Culshaw V, Yule M, Lawson R. Considerations for anaesthesia in children with haematological malignancy undergoing short procedures. Paediatr Anaesth. 2003;13:375-83. In case of neutropenia, it is mandatory to maintain strict aseptic precautions while handling these patients. Bacterial and viral filters should be used in the breathing circuits.66. Jacop R, Venkatesan T. Anesthesia and Fanconi anemia. Paediatr Anaesth. 2006;16:981-5.
Endocrinopathies are a common feature of FA. In a prospective study of 54 FA patients, it was found that hypothyroidism, impaired glucose tolerance, hyperinsulinemia, and subnormal response to growth hormone stimulation.77. Culshaw V, Yule M, Lawson R. Considerations for anaesthesia in children with haematological malignancy undergoing short procedures. Paediatr Anaesth. 2003;13:375-83. A complete endocrine assessment should be made to detect these aspects. Patients, who are on steroid therapy, must be documented regarding replacement therapy, glucose monitoring, edema, hypokalemia, myopathy, infection, and gastric prophylaxia.
Drug therapy for FA may also have anesthetic implications. Some of the serious adverse effects of androgen include hepatomegaly, cholestatic hepatitis, and elevated liver enzyme levels.33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365. Androgens may increase the anticoagulant effect of oral anticoagulants (warfarin)88. Meeks ML, Mahaffey KW, Katz MD. Danazol increases the anticoagulant effect of warfarin. Ann Pharmacother. 1992;26:641-2. and may also increase insulin effects.99. Bruce R, Godsland I, Stevenson J, et al. Danazol induces resistance to both insulin and glucagon in young women. Clin Sci (Lond). 1992;82:211-7. Adverse effects of G-CSF treatment relevant to anesthetic management include pericardial and pleural effusions and generalized capillary leak syndromes, which may result in interstitial pulmonary edema and arterial hypoxemia.1010. Tobias JD, Fueman WL. Anesthetic considerations in patients receiving colony-stimulating factors (G-CSF and GM-CSF). Anesthesiology. 1991;75:536-8.
Other drugs and chemicals causing acquired aplastic anemia should be avoided during the perioperative period. Medications interfere with platelet function should not be given to thrombocytopenic patients.33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365. These include aspirin, antihistamines, and nonsteroidal anti-inflammatory drugs.66. Jacop R, Venkatesan T. Anesthesia and Fanconi anemia. Paediatr Anaesth. 2006;16:981-5.
Normal fasting regimes and minimal monitoring standards, if any indication exist, more monitorizations, should be applied throughout the perioperative period. Significant thrombocytopenia, if present, may preclude regional anesthesia. Infective endocarditis prophylaxis has to be considered for patients with cardiac involvement.66. Jacop R, Venkatesan T. Anesthesia and Fanconi anemia. Paediatr Anaesth. 2006;16:981-5.
A possible anesthetic consideration may include the avoidance of high inspired oxygen concentrations (FiO2). There is sensitivity to oxygen-free radicals and to ionizing radiation.11. Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12. Clarke et al. suggest that the sensitivity of FA group C cells to apoptosis induced by MMC is because of reactive oxygen species generation in the presence of high oxygen concentrations and not DNA cross-linking.1111. Clarke AA, Philpott NJ, Gordon-Smith EC, et al. The sensitivity of Fanconi anemia group C cells to apoptosis induced by mitomycin C is due to oxygen radical generation, not DNA crosslinking. Br J Haematol. 1997;96:240-7. Low oxygen tension or antioxidants may be used to improve growth and decrease spontaneous or induced chromosome breaks in FA cells.33. Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365.
In this case caudal anesthesia was preferred to avoid from N2O, to reduce amount of anesthetic agent, to provide postoperative analgesia, and to reduce amount of nonsteroidal anti-inflammatory drugs and morphine.
Caudal epidural blockade is widely used to provide perioperative analgesia in pediatric practice. As a single injection, it offers a reliable and effective block for patients undergoing subumbilical surgery.1212. Tsui BCH, Berde CB. Caudal analgesia and anesthesia techniques in children. Curr Opin Anaesthesiol. 2005;18:283-8.
Nitrous oxide-induced bone marrow depression is an additional concern. Some studies suggest that the use of nitrous oxide (N2O) is harmful producing bone marrow suppression as it impairs methionine synthetase activity, disturbing folate metabolism and thus vitamin B12 metabolism.1313. Carmel R, Rabinowitz AP, Mazumder A. Metabolic evidence of cobalamine deficiency in bone marrow cells harvested for transplantation from donors given nitrous oxide. Eur J Haematol. 1993;50:228-33. On the other hand, we do not have any data in patient with FA.
In view of the hepatorenal derangement which can occur any time during the course of the disease, it is imperative to avoid anesthetic agents with potential hepatorenal toxicity. In this respect, it may be advisable to avoid halothane, long-acting muscle relaxants, nonsteroidal anti-inflammatory agents, and long-acting opioids such as morphine and pethidine.66. Jacop R, Venkatesan T. Anesthesia and Fanconi anemia. Paediatr Anaesth. 2006;16:981-5. Postoperative analgesia could be provided by caudal injection perfectly. Thus, amount of analgesic drug, such as nonsteroidal anti-inflammatory agents, morphine and pethidine, could be reduced. In this manner potential hepatorenal toxicity owing to analgesic agent could be avoided.
In conclusion, we preferred in the patient with FA without thrombocytopenia, because of avoiding from N2O, reducing amount of anesthetic, existing microcephaly, hypothyroidism and elevated liver enzymes, providing postoperative analgesia, and reducing amount of analgesic used postoperatively.
References
-
1Lanzkowsky P. Congenital aplastic anemias. In: Lanzkowsky P, editor. Manual of pediatric hematology and oncology. 4th edn. California: Elsevier Inc.; 2005. p. 105-12.
-
2Tischkowitz MD, Hodgson SV. Fanconi anaemia. J Med Genet. 2003;40:1-10.
-
3Alter BP. Inherited bone marrow failure syndromes. In: Nathan DG, Orkin SH, Ginsburg D, Look AT, editors. Nathan and Oski's hematology of infancy and childhood. 6th edn. Philadelphia: W.B. Saunders Company; 2003. p. 280-365.
-
4Dror Y. Inhereted bone marrow failure syndromes. In: Arceci ˙ JR, Hann MI, Smith PO, editors. Pediatric hematology. 3rd edn. Massachusetts: Blacwell Publishing; 2006. p. 32-7.
-
5Auerbach AD. Fanconi anemia diagnosis and the diepoxybutane (DEB) test. Exp Hematol. 1993;21:731-3.
-
6Jacop R, Venkatesan T. Anesthesia and Fanconi anemia. Paediatr Anaesth. 2006;16:981-5.
-
7Culshaw V, Yule M, Lawson R. Considerations for anaesthesia in children with haematological malignancy undergoing short procedures. Paediatr Anaesth. 2003;13:375-83.
-
8Meeks ML, Mahaffey KW, Katz MD. Danazol increases the anticoagulant effect of warfarin. Ann Pharmacother. 1992;26:641-2.
-
9Bruce R, Godsland I, Stevenson J, et al. Danazol induces resistance to both insulin and glucagon in young women. Clin Sci (Lond). 1992;82:211-7.
-
10Tobias JD, Fueman WL. Anesthetic considerations in patients receiving colony-stimulating factors (G-CSF and GM-CSF). Anesthesiology. 1991;75:536-8.
-
11Clarke AA, Philpott NJ, Gordon-Smith EC, et al. The sensitivity of Fanconi anemia group C cells to apoptosis induced by mitomycin C is due to oxygen radical generation, not DNA crosslinking. Br J Haematol. 1997;96:240-7.
-
12Tsui BCH, Berde CB. Caudal analgesia and anesthesia techniques in children. Curr Opin Anaesthesiol. 2005;18:283-8.
-
13Carmel R, Rabinowitz AP, Mazumder A. Metabolic evidence of cobalamine deficiency in bone marrow cells harvested for transplantation from donors given nitrous oxide. Eur J Haematol. 1993;50:228-33.
Publication Dates
-
Publication in this collection
May-Jun 2014
History
-
Received
12 Nov 2012 -
Accepted
19 Dec 2012