ABSTRACT
Objective:
To identify and analyze risk factors associated with strabismus, the eye data and personal and family history.
Methods:
A prospective, descriptive and analytical study, with 240 patients who consulted for the first time in strabismus clinics. We evaluated the frequency and association between strabismus and data eye examination and personal and family history to identify risk factors.
Results:
There was a higher prevalence of strabismus in women (56.96%) compared to men (43.02%). The age group most satisfied in strabismus clinic are children up to 15 years of age (83.54%). Met more esotropia (55.27%) than exotropia (42.20%) and lower portion of isolated vertical strabismus (2.53%). Preterm birth was associated with convergent strabismus (p = 0.023) but not the diverging (p = 0.086). Maternal diabetes mellitus was associated with esotropia (p = 0.024) and exotropia (p = 0.036) on the child, but the mother’s high blood pressure, medications for hypertension and diabetes during pregnancy and illicit drugs was not statistically significant. Patients with cerebral palsy association with exotropes had more (p = 0.008) which esotropia (p = 0.019). Congenital malformations, consanguinity between parents and ocular trauma showed no statistically significant association for strabismus. Most patients with strabismus showed good visual acuity, normal fundus. In the analysis of proportions farsightedness was more common in esotropia (68.7%).
Conclusions:
Internal and external risk factors can interfere in the formation and development of the eye in eye plasticity phase with impaired visual binocularity and may result in strabismus. There are differences with respect to risk factors associated truly and more studies are needed to identify.
Keywords:
Strabismus; Esotropia; Exotropia; Riskfactors; Vision, binocular; Eyes movements
RESUMO
Objetivo:
Identificar e analisar fatores de risco associados ao estrabismo, dados oftalmológicos e antecedentes pessoais e familiares.
Métodos:
Estudo prospectivo, descritivo e analítico realizado com 240 pacientes que consultaram pela primeira vez nos ambulatórios de estrabismo. Foram avaliadas a frequência e associação entre estrabismo, dados de exames oftalmológicos e antecedentes pessoais e familiares para identificação dos fatores de risco.
Resultados:
Observou-se maior prevalência de estrabismo em mulheres (56,96%) em relação aos homens (43,02%). A faixa etária mais atendida no ambulatório de estrabismo foi composta de crianças até 15 anos de idade (83,54%). Encontrou-se mais esotropia (55,27%) que exotropia (42,20%) e parcela menor de estrabismo vertical isolado (2,53%). A prematuridade foi associada ao estrabismo convergente (p=0,023) e não ao divergente (p=0,086). O diabetes mellitus materno foi associado à esotropia (p=0,024) e exotropia (p=0,036) no filho, mas a hipertensão arterial materna, uso de medicamentos para hipertensão e diabetes durante a gravidez e drogas ilícitas não foram estatisticamente significativos. Pacientes com paralisia cerebral tiveram mais associação com exotropia (p=0,008) que esotropia (p=0,019). Malformações congênitas, consanguinidade entre os pais e traumas oculares não apresentaram associação estatisticamente significativa para o estrabismo. A maioria dos pacientes com estrabismo apresentou boa acuidade visual corrigida e fundoscopia normal. Na análise de proporções a hipermetropia foi mais frequente na esotropia (68,7%).
Conclusão:
Os fatores de riscos internos e externos podem interferir na formação e desenvolvimento do olho na fase de plasticidade ocular, com prejuízo da binocularidade visual, podendo resultar em estrabismo. Há divergências com relação aos fatores de risco realmente associados e mais estudos são necessários para a identificação.
Descritores:
Estrabismo; Esotropia; Exotropia; Fatores de risco; Visão binocular; Movimentos oculares
INTRODUCTION
At birth there is a structuring of the macular area, which was previously similar to the peripheral retina, and the development of the afferent and efferent visual pathways takes place, with neural connections through the dendrites. The cones are retinal cells concentrated in foveola responsible for sharp vision. At this point the visual acuity (VA) is very low, around 0.03 due to macular immaturity and lack of visual stimuli. At the end of the first year the VA can be normal, and generally the development of the visual functions is completed until 5 years old.Visual fixation occurs earlier because premature infants of 33 weeks are already able to fix. The newborn fixes objects and follows them with slow movements in the horizontal plane.The vertical movements appear in the second month, and the full and mature tracking occurs upon completing one year of life. The image fusion begins in the first month of life and should be complete by the end of the sixth month. It is the binocular vision setting in.This visual development happens more rapidly in the first year of life, but there is an improvement of visual functions until five years of age. If there is an obstacle to the formation of the image in one or both retinas in this critical phase, this development is impaired in inverse proportion to the age at which the change happened. The coordinated eye movements and the parallelism between the eyes are crucial conditions for the binocular vision, and are maintained by the balance of the muscular strength from the extraocular muscles. Until 6 months of age the sporadic eye deviations are common due to the immaturity of the reflection of the fusion. However, if these deviations are frequent or constant at this stage they are considered abnormal. After the sixth month any deviation is normal because the fusion is already developed11 Graziano RM, PolatiM, Crestana AB.Oftalmologia. São Paulo: Ed. Manole; 2013. cap.9, p. 242. [Coleção Pediatria do Instituto da Criança].
Strabismus is a congenital or acquired dysfunction of the extraocular muscles with high prevalence in the population, around 2-4%, with varied clinical forms and medical or surgical corrective treatment22 Rocha MN. Análise das condições de saúde ocular em população atendida no Centro de Referencia em Oftalmologia do Hospital das Clínicas/UFG[dissertação]. Goiânia: Universidade Federal de Goiás; 2011.,33 Rocha MM. Tratamento cirúrgico do estrabismo: avaliação técnicoeconômica. ArqBras Oftalmol. 2005;68(1):61-9. There is a deviation from the binocular alignment due to lack of fixing symmetry of the object by the foveae. The direction of the deviation in the relation visual axis focused object may be convergent or esodeviation (ET), divergent or exodeviation (XT) and vertically or hyperdeviation (HT; DVD). It can happen at any age, but when it happens in adults it can be secondary to neurological or vascular (diabetes mellitus, hypertension) disorders, thyroid disease, brain tumors and cranial trauma, after loss of stimulus from the fusion due to the reduction of the visual acuity in cataract, ametropies and lesions44 Shimauti AT, Pesci LT, Sousa RL, PadovaniCR, SchelliniSA. Estrabismo: detecção em uma amostra populacional e fatoresdemográficos associados. Strabismus: detection in a population-based sample and associated demographic factors. ArqBrasOftalmol. 2012;75(2):92-6.
The etiology of strabismus is not well known, but an increased prevalence in pre-term suggests a common etiology. The age of onset of strabismus in children of low weight is variable, and may be from the earliest months until several years later. The increased risk of strabismus in children was well set when in the presence of Retinopathy of Prematurity (ROP) mainly the scar form, refractive errors and neurological changes. There are also risk factors to be considered, such as birth weight, anisometropy, maternal age, smoking, ethnic origin, preterm development pattern. These factors are important and complex to identify children with serious risk to develop strabismus55 O'Connor AR, Wilson CM, Fielder AR. Ophthalmological problems associated with preterm birth. Eye (Lond). 2007;21(10):1254-60. Review..
Determining the risk factors for strabismus is important for the early diagnosis of amblyopia and guidance for the treatment with the results66 Holmes JM, Lazar EL, Melia BM, Astle WF, Dagi LR, Donahue SP, Frazier MG,Hertle RW, Repka MX, Quinn GE, Weise KK; Pediatric Eye Disease InvestigatorGroup. Effect of age on response to amblyopia treatment in children. Arch Ophthalmol. 2011;129(11):1451-7.. A study of systematic review of the literature found significant risk factors for strabismus, as low birth weight, cicatricial retinopathy of prematurity, smoking during pregnancy, anisometropy and hyperopia. Certain population groups are at increased risk of developing concomitant strabismus, and can be identified earlier. Genetics helps in understanding the causes and development of strabismus. The intermittent and accommodative strabismus with strong heritage require more genetic studies to identify possible links of subtypes. The inheritance was studied in twins and has proved complex, with the presence of the gene STBMS1, being other types registered as well. Concomitant strabismus is a variety of eye misalignment which risk factors are complex and associated to genetic and environmental factors77 Maconachie GD, Gottlob I, McLean RJ. Risk factors and genetics in common comitant strabismus: a systematic review of the literature. JAMA Ophthalmol. 2013;131(9):1179-86..
The general objective of the present study was to investigate the risk factors in patients with strabismus in appointments in two ophthalmology hospitals of the public health system, the Reference Center in Ophthalmology of the Clinical Hospital of the Federal University of Goiás (CEROF/ HC/UFG) and the Hospital of the Eye Bank Foundation of Goiás (FUBOG). The specific objectives were to study the associations between the data of eye examination and different forms of strabismus and to identify the relations between personal and family antecedents and risk of strabismus in its many kinds.
METHODS
Study transverse lineament, observational, analytical and prospective study involving patients seen in SUS (Brazilian Single Health System). This study met the standards of the Declaration of Helsinki (2008) and follows the terms recommended by the Guidelines and Norms Regulating Research Involving Human Beings - Resolution 196/96 of the National Health Council, submitted for approval by the Medical Research Ethics Committee in Humans and Animals (CEPMHA) of the Clinical Hospital of the Federal University of Goiás and the Eye Bank Foundation of Goiás (FUBOG) in Goiânia, Goiás. We collected the eye examination data necessary for assessment as visual acuity with and without correction, inspection of the extrinsic and eyelid ocular motility, biomicroscopy, refraction, tonometry and ophthalmoscopy, in addition to personal and family information related to risk factors for strabismus in a questionnaire prepared for the research. An Informed Consent (IC) was signed by each patient involved in the research.
The determination of the minimum sample size was based on calculation of the proportion of a population that had as strabismus as prevalence parameters found in a previous work22 Rocha MN. Análise das condições de saúde ocular em população atendida no Centro de Referencia em Oftalmologia do Hospital das Clínicas/UFG[dissertação]. Goiânia: Universidade Federal de Goiás; 2011.with 7955 patients, equal to 2.64%, considering a margin of error of 2% and a confidence level of 95% and significance of p <0.05. The sample calculated of 247 patients was corrected to 240 of strabismus patients according to the finite and known size of the population. They sample included patients with strabismus regardless of age, type of strabismus and etiological factor.Those refusing to participate were excluded from the research. Data were organized in Excel spreadsheets (Microsoft 2010) and analyzed in the software Stata 12.0. First a descriptive analysis was performed, and the variables were expressed by absolute and relative frequencies. Later the prevalence of strabismus according to the exposure variables (antecedent) and the eye examination were analyzed. The difference in proportion was analyzed using the chi-square test or the Fisher’s exact, considering a significance level of 5% (p <0.05).
RESULTS
A sample of 240 patients had exclusion of three patients, one patient with nystagmus and no carrier of strabismus, and two patients with pseudostrabismus, leaving 237 for analysis. Of these, 135 (56.96%) were females and 102 (43.02%) were male. It was observed that 23 (9.70%) patients who consulted with strabismus were children up to 1 year of age, 56 (23.63%) were between 2 and 4 years, 63 (26.58%) between 5 and 8 years, 56 (23.63%) between 9 and 15 years, 5 (2.11%) between 16 and 20 years, 23 (9.70%) between 21 and 40 years, and 10 (4.22%) with age equal or above 41 years; 1 patient had no age recorded. The data are shown in Figure 1.
There was a predominance of patients aged from 2 to 15 years, followed by children under 1 year of age and between 21 to 40 years, as shown in Figure 2.
Distribution of patients with strabismus in the sample studied according to the age in the appointment
In the population studied, 131 ET (55.27%) and 100 XT (42.20%), and 6 (2.53%) cases of isolated vertical strabismus (Table 1) were found.
Estropies were the most frequent, isolated (119 cases; 50.21%) or associated with alphabetical concomitances or vertical deviation (12 cases, 5.06%); whereas exotropies were less recorded, isolated (92 cases, 38.82%) or associated with vertical incomitâncias or vertical deviations (9 cases, 3.38%). The vertical deviations were less observed (5 cases, 0.42%), and there was 1 case (0.42%) of incomitance in V, with increased convergence to look down by symmetrical hyperfunction of the upper oblique muscles. The distribution is listed in Table 2.
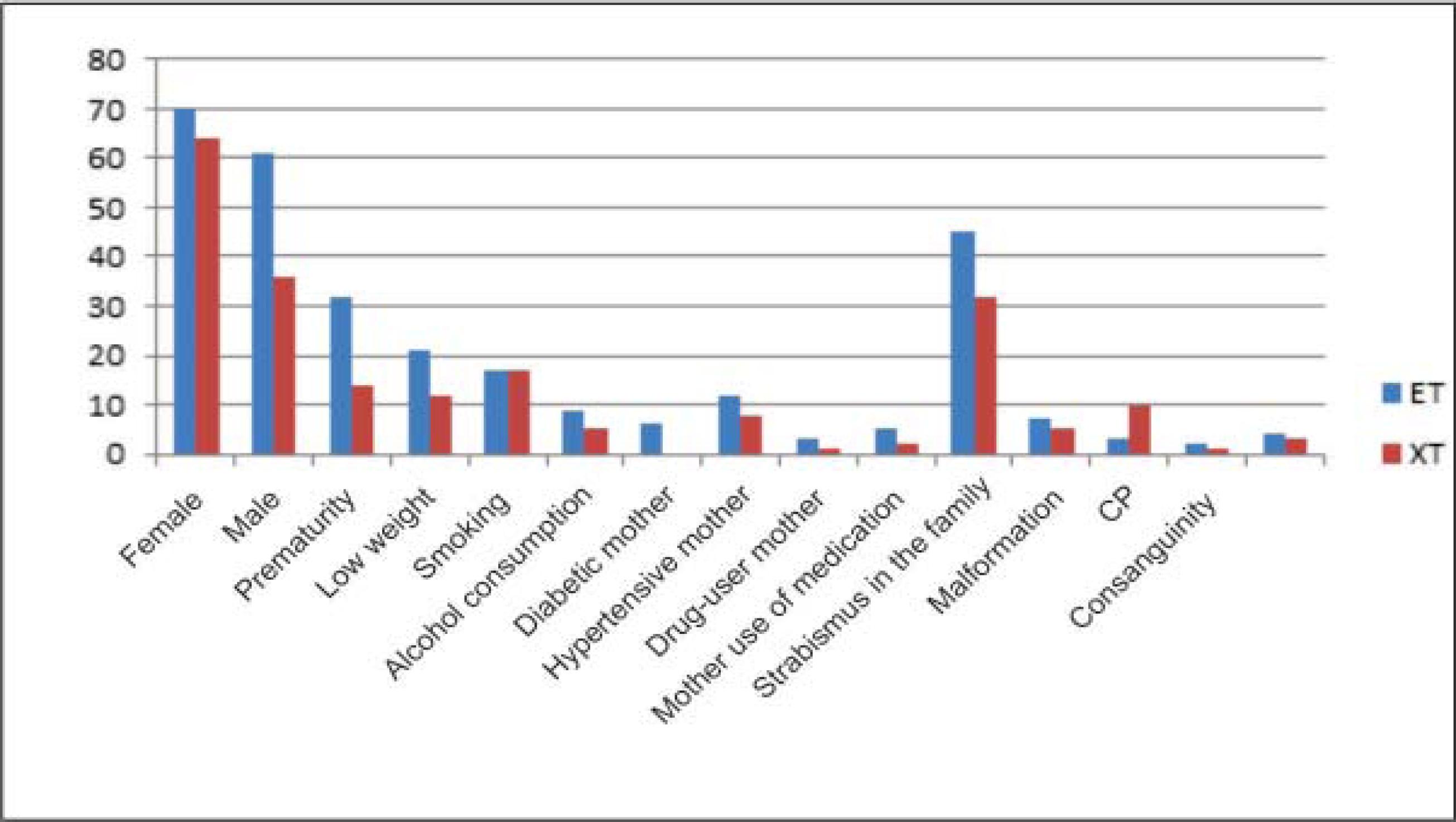
In the antecedents surveyed, 279 cases were found among 237 patients, with some patients (64; 27.00%) not showing antecedents and others with more than one antecedent (Table 3 and Figure 3).
The distribution of strabismus by sex and risk factors surveyed, separated into convergent and divergent strabismus, is shown in Table 4.
Distribution of the prevalence of ET and XT according to sex and antecedents in the sample studied
With respect to visual acuity (VA) with the best possible correction, there were records in 193 patients, and most of the eyes showed visual acuity above 0.7, followed by VA between 0.6 to 0.3. The right eye (RE) presented better VA in relation to the left eye (LE). Blindness by eye (VA<0.05) was greater than the low vision (VA<0.3 to 0.05), being most prevalent in the RE.
Most patients with strabismus showed good acuity corrected in both eyes, especially in the XT (p = 0.11) compared to ET (p = 0.67), followed by a lower portion of cases of subnormal vision and blindness. In isolated vertical strabismus, although in a low number (6 cases), a VA between 1.0 and 07 was registered in 100% of cases. The XT and ET data are shown in table 5.
The refraction of the 237 patients surveyed showed 154 patients with hyperopia (Hm) with or without astigmatism (Ast), and 54 patients with myopia (Mp) with or without astigmatism (Ast). The anisometropy was recorded in 19 patients, and flat refraction in both eyes in 14 patients. Of the total, 15 patients had no record of the refraction. The association between ametropies and strabismus is shown in table 6.
The eye fundus exam of 237 patients recorded 218 (91.98%) normal cases, 10 (4.22%) cases with unilateral or bilateral chorioretinitis scar and 9 (3.80%) cases of unilateral or bilateral optic atrophy. Of the total cases of ET (131), most presented normal fundoscopy (93.20%), and in the XT there was 91% normal. The association between fundoscopy and strabismus results is displayed in table 7.
DISCUSSION
The sample of 237 patients with strabismus showed the number of esotropies greater (n=131; 55.27%) than exotropies (n=100; 48,82%), and the vertical isolated strabismus were found: vertical incomitance in V, dissociated vertical divergence (DVD) and hypertrophy (HT) in small number (n = 6, 2.11%). Among the 131 cases of convergent strabismus (55.27%) 119 (50.21%) cases of only horizontal strabismus were registered, and 12 (5.06%) cases associated to vertical strabismus. The divergent strabismus, with 100 cases (42.20%) showed 92 (38.82%) patients with only XT, 8 (3.38%) patients with horizontal strabismus associated to vertical strabismus, and 6 (2.53%) cases with vertical strabismus isolated. The horizontal and vertical strabismus data were similar to those found by Shimauti et al. , and there was a difference in the form of aggregation of categories. In this study, the vertical strabismus associated to horizontal was analyzed as horizontal, and the pure verticals were analyzed separately44 Shimauti AT, Pesci LT, Sousa RL, PadovaniCR, SchelliniSA. Estrabismo: detecção em uma amostra populacional e fatoresdemográficos associados. Strabismus: detection in a population-based sample and associated demographic factors. ArqBrasOftalmol. 2012;75(2):92-6.
The horizontal strabismus was found in 135 women (56.96%) and 102 men (43.04%). The prevalence of ET was higher among men, 61 (58.6%) in relation to women, 70 (51.4%), although not statistically significant (p= 0.268). With respect to the XT, the reverse happened, which was more prevalent in women with n = 64 (47.1% of women) than in men with 36 (34.6%) p = 0.05. These data for ET are found in the literature.77 Maconachie GD, Gottlob I, McLean RJ. Risk factors and genetics in common comitant strabismus: a systematic review of the literature. JAMA Ophthalmol. 2013;131(9):1179-86. 99 Souza-Dias C, Goldchmit M. Os Estrabismos:teorias e casos comentados. Rio de Janeiro:Cultura Médica: Guanabara Koogan;2011.There is a need for more studies to relate sex to strabismus, mainly horizontal strabismus, more common in practice.
With age, the sample had a predominance of children up to 15 years of age (n=198, 83.44%), followed by adults aged 16 years or more (n=38, 16.14%). In 1 (0.42%) case the age was not recorded.This proportion is expected in strabismus ambulatories, where one observes a larger number of children appointments due to the dual purpose of the treatment: functional and aesthetic. There was still a considerable number of adults attended in the strabismus ambulatory for the first time in search of improved aesthetics but already with amblyopia and irreversible losses of binocularity dut to lack of access to free care, which is still bad.
Prematurity was statistically associated to the ET (p=0.03), but not to the XT (p=0.07). In relation to the patients born with low birth weight (below 2500 g) there was no significant association for ET (p=0.30) and XT (p=0.46). There is no doubt about the greatest prevalence of strabismus in premature children compared to those born at term, although the etiological process is not very clear. There are several studies that show the association between prematurity and born of low weight (<2500 g) and strabismus, probably due to lack of maturity of the cortical areas related to vision and eye movements, despite the mechanisms1010 Holmström G, el Azazi M, Kugelberg U. Ophthalmological follow up of preterm infants: a population based, prospective study of visual acuity and strabismus. Br J Ophthalmol. 1999;83(2):143-50.
11 Holmström G, Rydberg A, Larsson E. Prevalence and development of strabismus in 10-year-old premature children: a population-based study. J PediatrOphthalmol Strabismus. 2006;43(6):346-52.
12 O'Connor AR, Stephenson TJ, Johnson A, Tobin MJ, Ratib S, Fielder AR. Strabismus in children of birth weight less than 1701 g. Arch Ophthalmol. 2002;120(6):767-73.
13 Pennefather PM, Clarke MP, Strong NP, Cottrell DG, Dutton J, Tin W. Risk factors for strabismus in children born before 32 weeks' gestation. Br J Ophthalmol. 1999;83(5):514-8.-1414 Chew E, Remaley NA, Tamboli A, Zhao J, Podgor MJ, Klebanoff M. Risk factors for esotropia and exotropia. Arch Ophthalmol. 1994;112(10):1349-55..
In active or passive maternal smoking, there was also no significant association to ET (p=0.50) or XT (p=0.32). The use of alcohol during pregnancy was not associated to the risk of ET (p=0.48) and XT (p=0.61)1212 O'Connor AR, Stephenson TJ, Johnson A, Tobin MJ, Ratib S, Fielder AR. Strabismus in children of birth weight less than 1701 g. Arch Ophthalmol. 2002;120(6):767-73.
13 Pennefather PM, Clarke MP, Strong NP, Cottrell DG, Dutton J, Tin W. Risk factors for strabismus in children born before 32 weeks' gestation. Br J Ophthalmol. 1999;83(5):514-8.-1414 Chew E, Remaley NA, Tamboli A, Zhao J, Podgor MJ, Klebanoff M. Risk factors for esotropia and exotropia. Arch Ophthalmol. 1994;112(10):1349-55..
The maternal diseases surveyed during pregnancy were Diabetes mellitus (DM) and systemic arterial hypertension (SAH), that are the most common ones.There was a statistically significant association between maternal ET with ET (p = 0.02) and XT (p = 0.03), but not between ET (p = 0.66) and XT (p = 0.84) and SAH.
Drug use by the mother during pregnancy was not statistically associated to ET (p=0.42) and XT (P=0.48). The same has been found in relation to the use of medication for DM and SAH and ET (p= 0.38) and XT (p= 0.46).
The presence of strabismus in the family showed no aswith ET (p= 0.83) and XT (p= 0.62), although studies show the heredity as a factor associated to strabismus77 Maconachie GD, Gottlob I, McLean RJ. Risk factors and genetics in common comitant strabismus: a systematic review of the literature. JAMA Ophthalmol. 2013;131(9):1179-86.,88 Major A, Maples WC, Toomey S, DeRosier W, Gahn D. Variables associated withthe incidence of infantile esotropia. Optometry. 2007;78(10):534-41.,1414 Chew E, Remaley NA, Tamboli A, Zhao J, Podgor MJ, Klebanoff M. Risk factors for esotropia and exotropia. Arch Ophthalmol. 1994;112(10):1349-55.. There is a need for more research in this area to check this association, since it is common the presence of several cases of strabismus in the same family, mainly ET.
The presence of systemic malformation was not statistically significant for ET (p=0.83) and XT (p= 0.97), although Torp-Pedersen et al. have registered the relation between congenital abnormalities and strabismus.There is a great diversity of isolated or multiple malformations, composing syndromes, and the strabismus was analyzed separately.
Congenital cerebral palsy was associated to the risk of ET (p = 0.02), and especially for XT (p = 0.01). Studies show that patients with cerebral palsy have a prevalence of about 25.5% strabismus, probably by early lesion affecting brain areas of motor fusion between the occipital cortex and the premotor area1515 Torp-Pedersen T, Boyd HA, Poulsen G, Haargaard B, Wohlfahrt J, Holmes JM, Melbye M. Perinatal risk factors for strabismus. Int J Epidemiol. 2010;39(5):1229-39.,1616 Celino AC, Trigueiro S, Ventura LO, Toscano J, Barroca R. Alterações oculares em crianças portadoras de paralisia cerebral. RevBras Oftalmol. 2003;62(4):248-51. 2003..
Inbreeding among parents (cousins) was not associated to ET (p = 0.69) and XT (p = 0.75).
The eye trauma showed no significant association to ET (p= 0.92) and XT (p= 0.97). Studies have shown the association between trauma and paralytic strabismus, especially ET (VI cranial nerve palsy)1717 Behera S, DuttaBK , Chowdhury RK, Sar M. A Clinico-anatomical studyofstrabismus in a tertiarycare hospital.J DentMedSci. 2014; 13(1):32-5..
Strabismus patients generally have good VA in both eyes, and the cases of blindness are probably related to deep strabismus amblyopia due to the lack of treatment or response to a penalty, or dut to being the cause of strabismus in monocular lesions.A national study showed similar result44 Shimauti AT, Pesci LT, Sousa RL, PadovaniCR, SchelliniSA. Estrabismo: detecção em uma amostra populacional e fatoresdemográficos associados. Strabismus: detection in a population-based sample and associated demographic factors. ArqBrasOftalmol. 2012;75(2):92-6. In exodeviations, the corrected VA levels were better, although the proportion difference was not statistically significant. The isolated vertical strabismus did not record low VA, with no significant statistical proportion (p=0.06), which shall be searched in a study with a higher number of cases.
Patients with ET showed a higher frequency of hyperopia, whereas myopia was more frequent in XT. The anisometropy in strabismus was found in 18 (5.56%) cases with recorded refraction (222 records). The analysis of proportion showed no statistically significant difference, although there are studies showing the association44 Shimauti AT, Pesci LT, Sousa RL, PadovaniCR, SchelliniSA. Estrabismo: detecção em uma amostra populacional e fatoresdemográficos associados. Strabismus: detection in a population-based sample and associated demographic factors. ArqBrasOftalmol. 2012;75(2):92-6,1010 Holmström G, el Azazi M, Kugelberg U. Ophthalmological follow up of preterm infants: a population based, prospective study of visual acuity and strabismus. Br J Ophthalmol. 1999;83(2):143-50..
CONCLUSION
Strabismus presents a complexity involving integration between the cortical areas, the neurological connections and the structures of the eye resulting in binocularity. Internal factors interfering in these areas since the embryogenesis until the development of the eye during the ocular plasticity or external factors that cause eye loss with damage of vision can cause strabismus. Preventing irreversible sensory damage such as visual loss and binocularity with early treatment is possible in many cases.Access to the ophthalmologist, the understanding of the family, especially in low income populations, could reduce the prevalence of strabismus and visual injury resulting from the lack of treatment. There are also differences with respect to the risk factors in fact associated, and further studies are needed to reach the goals intended with the identification.
-
Institutions where the study was carried out: Hospital da Fundação Banco de Olhos de Goiás; Centro de Referência em Oftalmologia Hospital das Clínicas da Universidade Federal de Goiás Goiânia, GO, Brazil.
REFERÊNCIAS
-
1Graziano RM, PolatiM, Crestana AB.Oftalmologia. São Paulo: Ed. Manole; 2013. cap.9, p. 242. [Coleção Pediatria do Instituto da Criança]
-
2Rocha MN. Análise das condições de saúde ocular em população atendida no Centro de Referencia em Oftalmologia do Hospital das Clínicas/UFG[dissertação]. Goiânia: Universidade Federal de Goiás; 2011.
-
3Rocha MM. Tratamento cirúrgico do estrabismo: avaliação técnicoeconômica. ArqBras Oftalmol. 2005;68(1):61-9
-
4Shimauti AT, Pesci LT, Sousa RL, PadovaniCR, SchelliniSA. Estrabismo: detecção em uma amostra populacional e fatoresdemográficos associados. Strabismus: detection in a population-based sample and associated demographic factors. ArqBrasOftalmol. 2012;75(2):92-6
-
5O'Connor AR, Wilson CM, Fielder AR. Ophthalmological problems associated with preterm birth. Eye (Lond). 2007;21(10):1254-60. Review.
-
6Holmes JM, Lazar EL, Melia BM, Astle WF, Dagi LR, Donahue SP, Frazier MG,Hertle RW, Repka MX, Quinn GE, Weise KK; Pediatric Eye Disease InvestigatorGroup. Effect of age on response to amblyopia treatment in children. Arch Ophthalmol. 2011;129(11):1451-7.
-
7Maconachie GD, Gottlob I, McLean RJ. Risk factors and genetics in common comitant strabismus: a systematic review of the literature. JAMA Ophthalmol. 2013;131(9):1179-86.
-
8Major A, Maples WC, Toomey S, DeRosier W, Gahn D. Variables associated withthe incidence of infantile esotropia. Optometry. 2007;78(10):534-41.
-
9Souza-Dias C, Goldchmit M. Os Estrabismos:teorias e casos comentados. Rio de Janeiro:Cultura Médica: Guanabara Koogan;2011.
-
10Holmström G, el Azazi M, Kugelberg U. Ophthalmological follow up of preterm infants: a population based, prospective study of visual acuity and strabismus. Br J Ophthalmol. 1999;83(2):143-50.
-
11Holmström G, Rydberg A, Larsson E. Prevalence and development of strabismus in 10-year-old premature children: a population-based study. J PediatrOphthalmol Strabismus. 2006;43(6):346-52.
-
12O'Connor AR, Stephenson TJ, Johnson A, Tobin MJ, Ratib S, Fielder AR. Strabismus in children of birth weight less than 1701 g. Arch Ophthalmol. 2002;120(6):767-73.
-
13Pennefather PM, Clarke MP, Strong NP, Cottrell DG, Dutton J, Tin W. Risk factors for strabismus in children born before 32 weeks' gestation. Br J Ophthalmol. 1999;83(5):514-8.
-
14Chew E, Remaley NA, Tamboli A, Zhao J, Podgor MJ, Klebanoff M. Risk factors for esotropia and exotropia. Arch Ophthalmol. 1994;112(10):1349-55.
-
15Torp-Pedersen T, Boyd HA, Poulsen G, Haargaard B, Wohlfahrt J, Holmes JM, Melbye M. Perinatal risk factors for strabismus. Int J Epidemiol. 2010;39(5):1229-39.
-
16Celino AC, Trigueiro S, Ventura LO, Toscano J, Barroca R. Alterações oculares em crianças portadoras de paralisia cerebral. RevBras Oftalmol. 2003;62(4):248-51. 2003.
-
17Behera S, DuttaBK , Chowdhury RK, Sar M. A Clinico-anatomical studyofstrabismus in a tertiarycare hospital.J DentMedSci. 2014; 13(1):32-5.
Publication Dates
-
Publication in this collection
Jan-Feb 2016
History
-
Received
13 Sept 2015 -
Accepted
27 Oct 2015