Abstracts
OBJECTIVE: To describe the prevalence of stunting in children under five and identify factors associated. METHODS: Population-based cross-sectional study conducted in 1991, 1997 and 2006 in the state of Pernambuco, northeastern Brazil. The following variables associated with the prevalence of stunting (height-for-age < -2 z-score) were studied: socioeconomic condition, maternal and child characteristics, and health care provided. A hierarchical model was used in the multiple logistic regression to assess the impact of explanatory variables on children's stunting. RESULTS: The prevalence of child malnutrition (height-for-age) was reduced by 65% from 1991 to 2006. Socioeconomic variables (per capita family income, maternal education, number of people living in the household and access to consumer goods), maternal height and birth weight were associated with stunting in children under five. CONCLUSIONS: All the determinants studied improved over the study period though not consistently. Despite significant reduction of child malnutrition in Pernambuco there remain differences regarding stunting, and children with better socioeconomic conditions have more favorable outcomes.
Infant; Child; Stature by Age; Malnutrition; Risk Factors; Socioeconomic Factors; Cross-Sectional Studies
OBJETIVO: Descrever o déficit estatural de menores de cinco anos e identificar fatores associados. MÉTODOS: Estudo transversal de base populacional realizado em 1991, 1997 e 2006 no Estado de Pernambuco. A análise da prevalência e fatores associados ao déficit estatural (altura para idade < -2 escore Z) incluiu: condições socioeconômicas, características maternas e da criança e de assistência à saúde. A regressão logística múltipla utilizou o modelo hierarquizado, para avaliar o impacto das variáveis explanatórias sobre o déficit de estatura das crianças. RESULTADOS: A prevalência da desnutrição em crianças pelo índice altura para idade diminuiu 65% entre 1991 e 2006. As variáveis socioeconômicas (renda familiar per capita, escolaridade materna, número de pessoas na residência e acesso a bens de consumo), a altura materna e o peso ao nascer permaneceram entre os fatores associados ao déficit estatural das crianças. CONCLUSÕES: Todos os determinantes analisados melhoraram no período analisado, nem sempre de forma igualitária. Apesar da redução expressiva da desnutrição nas crianças pernambucanas, ainda existem diferenciais em relação ao déficit de estatura, sendo mais favoráveis para as crianças em melhores condições socioeconômicas.
Lactente; Criança; Estatura-Idade; Desnutrição; Fatores de Risco; Fatores Socioeconômicos; Estudos Transversais
OBJETIVO: Describir el déficit de estatura de menores de cinco años e identificar factores asociados. MÉTODOS: Estudio transversal de base poblacional realizado en 1991, 1997 y 2006 en el Estado de Pernambuco, Noreste de Brasil. El análisis de prevalencia y factores asociados al déficit de estatura (altura-para-edad < -2 escore Z) incluyó: condiciones socioeconómicas, características maternas y del niño y de asistencia a la salud. La regresión logística múltiple utilizó el modelo jerarquizado, para evaluar el impacto de las variables explicativas sobre el déficit de estatura de los niños. RESULTADOS: La prevalencia de la desnutrición en niños por el índice altura-para-edad disminuyó 65% entre 1991 y 2006. Las variables socioeconómicas (renta familiar per capita, escolaridad materna, número de personas en la residencia y acceso a bienes de consumo), la altura materna y el peso al nacer permanecieron entre los factores asociados al déficit de estatura de los niños. CONCLUSIONES: Todos los determinantes analizados mejoraron en el período analizado, no siempre de forma similar. A pesar de la reducción expresiva de la desnutrición en los niños pernambucanos, aún existen diferenciales con relación al déficit de estatura, siendo más favorables para los niños en mejores condiciones socioeconómicas.
Lactante; Niño; Estatura por Edad; Desnutrición; Factores de Riesgo; Factores Socioeconómicos; Estudios Transversales
ORIGINAL ARTICLES
Risia Cristina Egito de MenezesI; Pedro Israel Cabral de LiraII; Vanessa Sá LealI; Juliana Souza OliveiraIII; Sandra Cristina da Silva SantanaIV; Leopoldina Augusta de Souza SequeiraII; Anete RissinV; Malaquias Batista FilhoV
IFaculdade de Nutrição. Universidade Federal de Alagoas. Maceió, AL, Brasil
IIDepartamento de Nutrição. Universidade Federal de Pernambuco (UFPE). Recife, PE, Brasil
IIICentro Acadêmico de Vitória. UFPE. Recife, PE, Brasil
IVFaculdade Maurício de Nassau. Recife, PE, Brasil
VInstituto de Medicina Integral Prof. Fernando Figueira. Recife, PE, Brasil
Correspondence
ABSTRACT
OBJECTIVE: To describe the prevalence of stunting in children under five and identify factors associated.
METHODS: Population-based cross-sectional study conducted in 1991, 1997 and 2006 in the state of Pernambuco, northeastern Brazil. The following variables associated with the prevalence of stunting (height-for-age < -2 z-score) were studied: socioeconomic condition, maternal and child characteristics, and health care provided. A hierarchical model was used in the multiple logistic regression to assess the impact of explanatory variables on children's stunting.
RESULTS: The prevalence of child malnutrition (height-for-age) was reduced by 65% from 1991 to 2006. Socioeconomic variables (per capita family income, maternal education, number of people living in the household and access to consumer goods), maternal height and birth weight were associated with stunting in children under five.
CONCLUSIONS: All the determinants studied improved over the study period though not consistently. Despite significant reduction of child malnutrition in Pernambuco there remain differences regarding stunting, and children with better socioeconomic conditions have more favorable outcomes.
Descriptors: Infant. Child. Stature by Age. Malnutrition. Risk Factors. Socioeconomic Factors. Cross-Sectional Studies.
RESUMEN
OBJETIVO: Describir el déficit de estatura de menores de cinco años e identificar factores asociados.
MÉTODOS: Estudio transversal de base poblacional realizado en 1991, 1997 y 2006 en el Estado de Pernambuco, Noreste de Brasil. El análisis de prevalencia y factores asociados al déficit de estatura (altura-para-edad < -2 escore Z) incluyó: condiciones socioeconómicas, características maternas y del niño y de asistencia a la salud. La regresión logística múltiple utilizó el modelo jerarquizado, para evaluar el impacto de las variables explicativas sobre el déficit de estatura de los niños.
RESULTADOS: La prevalencia de la desnutrición en niños por el índice altura-para-edad disminuyó 65% entre 1991 y 2006. Las variables socioeconómicas (renta familiar per capita, escolaridad materna, número de personas en la residencia y acceso a bienes de consumo), la altura materna y el peso al nacer permanecieron entre los factores asociados al déficit de estatura de los niños.
CONCLUSIONES: Todos los determinantes analizados mejoraron en el período analizado, no siempre de forma similar. A pesar de la reducción expresiva de la desnutrición en los niños pernambucanos, aún existen diferenciales con relación al déficit de estatura, siendo más favorables para los niños en mejores condiciones socioeconómicas.
Descriptores: Lactante. Niño. Estatura por Edad. Desnutrición. Factores de Riesgo. Factores Socioeconómicos. Estudios Transversales.
INTRODUCTION
Child malnutrition is one of the main nutritional status alterations in developing countries, and it is also considered a public health problem.15 Studies have shown the degree and distribution of this multifactorial problem in populations, as well as its association with factors related to maternal level of schooling, healthcare provided, sanitization of the environment, housing conditions, family's purchasing power,
Economic, social and demographic transformations have considerably modified the nutritional profile of the child population in the last decades, and the World Health Organization (WHO) estimates that 7% of the children younger than five years are stunted.17 In Brazil, the frequencies of weight-for-height and weight-for-age deficits (1.4% and 1.9%, respectively) point to the virtual control of the risk of child malnutrition, as they are in the expected level for healthy and well-nourished populations.17,ª
The decline in child malnutrition in Brazil has been recently attributed to the significant rise in families' purchasing power, to the increase in maternal schooling, to greater access to maternal and child healthcare and to the amplification of essential public services, such as water supply networks and garbage collection.13,ª
In view of this and of the negative repercussions of malnutrition among children, this study aimed to describe stunting in children under five and identify associated factors.
METHODS
This population-based cross-sectional study used data from Pesquisa Estadual de Saúde e Nutrição (PESN - State Health and Nutrition Survey), carried out in the State of Pernambuco (Northeastern Brazil) in 1997 and 2006. The objective of the inquiries was the diagnosis of health, nutrition and eating habits of children under five, including demographic, socioeconomic and environmental data, as well as data related to health services utilization and childcare.
The random and stratified probability sample was constituted by children aged zero-59 months and totaled 935 children in the first phase of the research, (1991), 2,040 in the second (1997) and 1,609 in the third (2006). The fieldwork was performed by teams of interviewers and anthropometrists. Anthropometric evaluation was carried out after the researchers were trained according to the technical procedures recommended by the WHO17 and the norms of the Manual de Acompanhamento do Crescimento e Desenvolvimento do Ministério da Saúde (Growth and Development Follow-up Manual of the Ministry of Health).
The software Anthro version 2
The independent variables were child's age, household situation, per capita family income, maternal schooling, number of people residing in the household, ownership of goods, access to essential services, maternal height and body mass index (BMI), child's birth weight and healthcare provided (adequate: with six prenatal consultations and hospital delivery; inadequate: access to only one or none of these services).
The data were processed and analyzed by means of a database with available variables in the two phases of the study. The software EpiInfo version 6.04 was used for the double data input.
Stunting for the years of 1991, 1997 and 2006 was analyzed according to household situation. The evolution of the influence of stunting determinants was obtained by comparing the percentages and their confidence intervals (95%CI) for the periods of 1997 and 2006. The data from the 1991 survey were not analyzed in view of the limitation of the information of some variables, which hampered comparability with the other studied years. To compare the categorical variables, the chi-square test was used, or the chi-square test with Yates' correction for the dichotomous variables, considering p < 0.05 as statistical significance. The programs EpiInfo version 6.04 and SPSS version 8.0 were utilized.
The determinant factors of malnutrition were analyzed with data from the 2006 PESN. Odds ratio (OR) of stunting were calculated to each exposure variable through logistic regression. The variables with p < 0.20 in the bivariate analysis were selected for initial inclusion in the regression analysis. Multiple logistic regression was performed with the adoption of a process of hierarchical modeling per blocks18 using the method enter, so that the first block contained the socioeconomic variables: maternal schooling and per capita family income. In the second block, the following variables were introduced: household situation, consumer goods, access to essential services and number of people residing in the household; in the third block, maternal height; and, finally, in the fourth block, the variable related to healthcare (prenatal assistance and delivery) and birth weight. To adjust the odds ratio, the variables of the first hierarchical block were included in the regression model. The variables of this level that showed association with stunting (p < 0.05) were maintained in the model in the lower hierarchical levels. The same procedure was adopted to the other hierarchical levels.
The PESN editions were approved by the Ethics Committee of Research in Human Beings of the Health Sciences Center of Universidade Federal de Pernambuco and of Instituto Materno-Infantil de Pernambuco (II PESN: Directive no. 044/96-CCS, of December 17, 1996).
RESULTS
The prevalence of stunting among children in the State as a whole decreased from 24.6%, in 1991 to 8.7% in 2006, which represents a 64.6% reduction (Figure). The Metropolitan Region of Recife showed prevalences inferior to those of inland municipalities in the analyzed period, when these regions registered reductions of 73% e 65%, respectively.
In 1997 and 2006, the lowest prevalences of stunting were found among children from families with higher per capita income (> 0.50 minimum salary); of mothers with at least four years of schooling; from less numerous families; with access to the listed consumer goods and to better sanitation conditions, with statistical significance for both years (Table 1).
Stunting exhibited a significant reduction trend for all the strata of the variables studied in the two periods, with percentages that varied from 31% to 64%.
In 2006, the occurrence of stunting among low birth weight children of mothers with short stature was three times higher when compared to those born with more than 2,500 g of mothers whose height was above 1.50 m (Table 2). Children whose mothers had received better prenatal and delivery assistance presented lower prevalence of stunting.
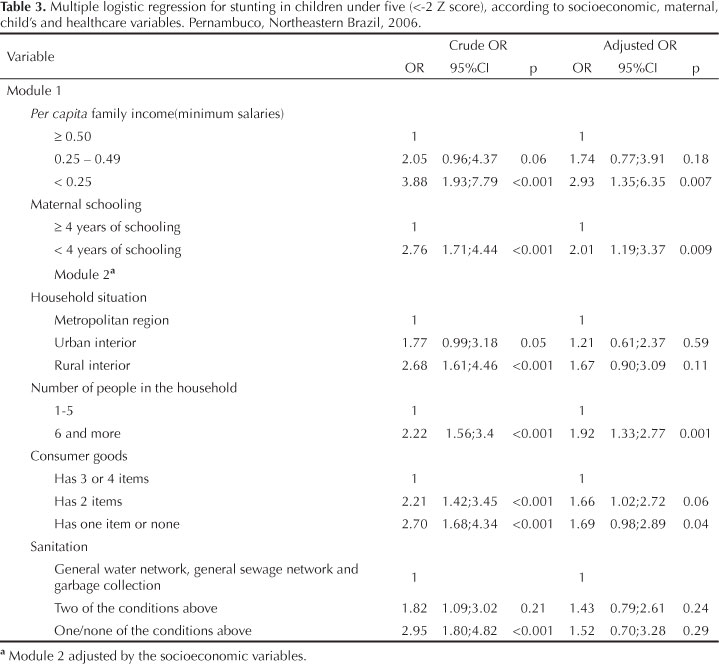
The results of the multiple logistic regression analysis and the adjusted effects of the explanatory variables in relation to the height-for-age index can be found in Tables 3 and 4. The adjusted OR shows that the socioeconomic variables (per capita family income, maternal schooling, number of people in the household and access to consumer goods), maternal height and birth weight remained among the factors associated with stunting in children.
DISCUSSION
The prevalence of child malnutrition according to the height-for-age index decreased by 65% in the State of Pernambuco between 1991 and 2006. This result is similar to the one found by Monteiro et al12 (2009), who studied the prevalence of malnutrition in the Brazilian population of children under five between 1996 and 2006 and indicated a 50% decline.
Despite the similarity in relation to the temporal variation trend, the prevalence estimated to the State as a whole (8.7%) in 2006 was higher than the ones verified to the Northeast (5.7%) and to Brazil (7.0%) by Pesquisa Nacional de Demografia e Saúde da Criança e da Mulher (PNDS - National Survey of Children's and Women's Demography and Health) in this same year.ª The interior of the State (10.1%) and more specifically the rural zone (11.4%) presented even higher prevalences.
The higher prevalence of malnutrition in the interior of the State delimits spatial differences that agree with the trends found in the 2006 PNDS for the North Region of Brazil (14.8%). These results express socioeconomic inequalities and difficulty to access primary healthcare services and basic social work services, and make these regions be priority areas for efforts to control child malnutrition in Brazil.ª
According to the results of the present study, stunting is statistically associated with socioeconomic conditions. Children of mothers with less than four years of schooling have odds two times higher of being stunted, which was also observed in the 2006 PNDS.ª In the evaluated period, the socioeconomic conditions improved, mainly regarding maternal schooling: mothers with less than four years of education decreased from 24.2% (1997) to 10.7% (2006) in the State as a whole. However, lower maternal schooling continues to be associated with higher malnutrition indexes, with two times higher odds of occurrence in comparison to those with higher level of schooling, a fact that was also observed in the 2006 PNDS.ª
Maternal schooling has been pointed out as a factor associated with child growthª in the scientific literature.7,10,12 The way in which the mother dedicates attention to her children, both directly and through caregivers, as well as her access to healthcare services are influenced by the level of schooling.11
Studies also show the influence of family income on children's nutritional status.4,10,12,ª In relation to the per capita family income, the difference in stunting prevalence between the extremes of the purchasing power classes is of approximately three times, with concentration of infant growth retardation in the less favored strata. Despite the economic development and the advances in the Brazilian population's quality of life that were observed in the last decades, there was no adequate or better income distribution.g,h,i
Traditionally, populations that live in the interior of the State, especially in rural areas, have been more susceptible to nutritional deficits, mainly children. In the last decades, with the fast reduction in malnutrition, although still with disadvantages to the rural areas, the differences in prevalences have not presented statistical significance when they interact with other determinants.i In the present study, although the highest OR for stunting correspond to the rural area, the same was not confirmed in the multiple analysis after adjustment by the other factors. In the 2006 PNDS, the difference in the prevalences of stunting-for-age was of 0.7 percentage point (urban = 6.9%; rural = 7.6%).ª
In relation to family composition, important demographic changes have occurred in the last years, mainly in the number of people in the households.1 The continuous decline in fertility, even after it reached low levels, is, to a large extent, responsible for the reduction in the number of components in the Brazilian households, in such a way that family density decreased from the mean of 4.1 to 3.1 people.g This scenario of demographic changes, with less numerous families, will result in children's improved health condition, accompanying the improvement in the Brazilian population's quality of life that has been observed in the last decades.1,g
In the present study, stunting in the group of children belonging to the most numerous families was approximately two times higher when compared to that of households with fewer dwellers, a result that was also observed in the 1997 PESN.14 These results are corroborated by other studies.1,5
The results of the present study reflect an advance in the ownership of durable consumer goods, a fact that has also been observed in the Brazilian population.7,h In spite of this progress, it is still possible to visualize an inverse relationship between ownership of goods and child malnutrition: the frequency of malnourished children increases as the number of goods that the family owns decreases, with odds of malnutrition higher than 1.5 times among economically vulnerable children.
The basic infrastructure that is available to the households is an important indicator of socioeconomic conditions, and it behaves as a marker of the sanitary and health conditions of the population.1,3,14 The percentage of households with access to the services of water supply, sewage and garbage collection has increased significantly; however, it is still restricted to a small part of the population. This indicator has not improved in the same rhythm of that of durable consumer goods.
These data indicate that the policies in the scope of public health will not be effective in disease prevention if there are no intersectoral actions with this purpose. Access, total or partial, to basic infrastructure is one of the factors that has been traditionally associated with improvements in the malnutrition indexes.15 Sociocultural factors, such as poverty and social deprivation, as well as mothers' biological and nutritional factors, can also be important determinants of malnutrition.6,8,9 This is what data in relation to mothers' height suggest: in the present study, maternal stunting was associated with three times higher odds of stunting in their children.
The pregnant woman's poor nutritional condition at birth constitutes a significant risk factor for subsequent infant growth retardation, mainly in the first years of life.5 In fact, in the present study, low birth weight represented three times higher odds of malnutrition in children under five.
It is known that low birth weight can express a population's standard of life, and its most severe consequences happen during fetal development and in the first years of life, with serious implications for the future nutritional status. It may even become one of the main components of child mortality.5 Thus, the findings point to the need of establishing strategies that enable to prevent low birth weight, which is operationally translated as adequate prenatal care, appropriate assistance to childbirth and child's health.
Healthcare showed a significant statistical relationship in the bivariate analysis, but it was not maintained in the multiple logistic regression analysis. Therefore, healthcare is not an independent associated factor in this population, unlike birth weight, which was maintained in the succession of explanatory models of stunting. Thus, results grounded in inductive indicators should be analyzed with caution.
The present study was founded on population-based state inquiries, which grants it internal validity and enables a better healthcare planning in the State. Besides, the results presented here may serve as reference to studies in areas whose socioeconomic and cultural characteristics are similar to those of Pernambuco, like other states of the Northeastern region of Brazil. Despite the reduced prevalence of malnutrition, the sample size was sufficient to the performance of the multiple logistic statistical analysis, with the utilization of a hierarchical determination model.
Sample losses inferior to 3% during data collection can be considered a limitation. In addition, it is not possible to generalize the results, because it is fundamental to consider the differences and specificities of the studied population to make a more specific criticism, understanding, in each context, the behavior of the variables, how they articulate with each other and how they result in varied outcomes, in view of the fact that there is no single and universal model destined to the explanation of the diverse circumstances of reality.2
In conclusion, there is a clear difference in stunting that is reflected on practically all the analyzed indicators, always in favor of children in better socioeconomic condition.
Temporal trend studies like the present one have a strategic importance to guide universal policies of employment and income (social inclusion), as well as primary healthcare.
REFERENCES
- 1. Alves JED, Cavenaghi S. Questões conceituais e metodológicas relativas a domicílio, família e condições habitacionais. Pap Poblac. 2005;(43):105-31.
- 2. Batista Filho M, Rissin A. A transição nutricional no Brasil: tendências regionais e temporais. Cad Saude Publica. 2003;19(1):181-91. DOI:10.1590/S0102-311X2003000700019
- 3. Barcellos C, Coutinho K, Pina MF, Magalhães MMAF, Paola JCMD, Santos SM. Inter-relacionamento de dados ambientais e de saúde: análise de risco à saúde aplicada ao abastecimento de água no Rio de Janeiro utilizando Sistemas de Informações Geográficas. Cad Saude Publica. 1998;14(3):597-605. DOI:10.1590/S0102-311X1998000300016
- 4. Barros FC, Victora CG, Scherpbier R, Gwatkin D. Iniquidades sociais na saúde e nutrição de crianças em países de renda baixa e média. Rev Saude Publica. 2010; 44(1):1-16. DOI:10.1590/S0034-89102010000100001
- 5. Barroso GS, Sichieri R, Salles-Costa R. Fatores associados ao déficit nutricional em crianças residentes em uma área de prevalência elevada de insegurança alimentar. Rev Bras Epidemiol. 2008;11(3):484-94. DOI:10.1590/S1415-790X2008000300015
- 6. Black RE, Allen LH, Bhutta ZA, Caulfield LE, Onis M, Ezzati M, et al. Maternal and child under nutrition: global and regional exposures and health consequences. Lancet 2008;371(9608):243-60. DOI:10.1016/S0140-6736(07)61690-0
- 7. Bobak M, Bohumir K, Leon DA, Danová J, Marmot M. Socioeconomic factors on height of preschool children in the Czech Republic. Am J Publ Health. 1994;84(7):1167-70. DOI:10.2105/AJPH.84.7.1167
- 8. Drachler ML, Andersson MCS, Leite JCC, Marshall T, Aerts DRGC, Freitas PF, et al. Desigualdade social e outros determinantes da altura em crianças: uma análise multinível. Cad Saude Publica. 2003;19(6):1815-25. DOI:10.1590/S0102-311X2003000600025
- 9. James WPT, Ferro-Luzzi A, Waterlow JC. Definition of chronic energy deficiency in adults. Report of a working party of the International Dietary Energy Consultative Group. Eur J Clin Nutr. 1988;42(12):969-81.
- 10. Lima ALL, Silva ACF, Konno SC, Conde WL, Benicio MHD'A, Monteiro CA. Causas do declínio acelerado da desnutrição infantil no Nordeste do Brasil (1986-1996-2006). Rev Saude Publica. 2010;44(1):17-27. DOI:10.1590/S0034-89102010000100002
- 11. Monteiro CA, Freitas ICM. Evolução de condicionantes socioeconômicos da saúde na infância na cidade de São Paulo (1984-1996). Rev Saude Publica. 2000;34(6 Supl):S8-12. DOI:10.1590/S0034-89102000000700004
- 12. Monteiro CA, Benicio MHD, Konno SC, Silva ACF, Lima ALL, Conde WL. Causas do declínio da desnutrição infantil no Brasil, 1996-2007. Rev Saude Publica. 2009;43(1):35-43. DOI:10.1590/S0034-89102009000100005
- 13. Onis M, Blössner M, Borghi E, Frongillo EA, Morris R. Estimates of global of childhood underweight in 1990 and 2015. JAMA 2009;291(21) 2600-6. DOI:10.1001/jama.291.21.2600
- 14. Rissin A, Batista Filho M, Benício MHD'A, Figueiroa. Condições de moradia como preditores de riscos nutricionais em crianças de Pernambuco, Brasil. Rev Bras Saude Matern Inf. 2006;6(1):59-67. DOI:10.1590/S1519-38292006000100007
- 15. Valente FLS. Fome e desnutrição: determinantes sociais. São Paulo: Editora Cortez; 1988.
- 16. Victora CG, Huttly SR, Fuchs SC, Olinto MTA. The role conceptual frameworks in epidemiological analysis: a hierarquical approach. Int J Epdemiol. 1997;26(1):224-7. DOI:10.1093/ije/26.1.224.
- 17. World Health Organization. Physical Status; The use and interpretation of anthropometry. Geneva; 1995. (Technical Report Series, 854).
- 18. World Health Organization. Multicentre Growth Reference Study Group. Who child growth standards based on length/height, weight and age. Acta Paediatr Suppl. 2006; (450):76-85.
Determinants of stunting in children under five in Pernambuco, Northeastern Brazil
Publication Dates
-
Publication in this collection
22 Nov 2011 -
Date of issue
Dec 2011
History
-
Received
27 Oct 2010 -
Accepted
13 May 2011