Abstracts
The use of yoga as an effective cardiac rehabilitation in patients with chronic heart failure (CHF) remains controversial.
We performed a meta-analysis to examine the effects of yoga on exercise capacity and health-related quality of life (HRQOL) in patients with CHF. Methods: We searched MEDLINE, Cochrane Central Register of Controlled Trials, Excerpta Medica database, LILACS, Physiotherapy Evidence Database, The Scientific Electronic Library Online, and Cumulative Index to Nursing and Allied Health (from the earliest date available to December 2013) for randomized controlled trials (RCTs) examining the effects of yoga versus exercise and/or of yoga versus control on exercise capacity (peakVO2) and quality-of-life (HRQOL) in CHF. Two reviewers selected studies independently. Weighted mean differences (WMDs) and 95% confidence intervals (CIs) were calculated, and heterogeneity was assessed using the I2 test.
Two studies met the selection criteria (total: 30 yoga and 29 control patients). The results suggested that yoga compared with control had a positive impact on peak VO2 and HRQOL. Peak VO2, WMD (3.87 95% CI: 1.95 to 5.80), and global HRQOL standardized mean differences (-12.46 95% CI: -22.49 to -2.43) improved in the yoga group compared to the control group.
Yoga enhances peak VO2 and HRQOL in patients with CHF and could be considered for inclusion in cardiac rehabilitation programs. Larger RCTs are required to further investigate the effects of yoga in patients with CHF.
Yoga; Heart Failure; Complementary Therapies/utilization; Exercise Therapy; Meta-Analysis
A eficácia da prática de yoga na reabilitação cardíaca em pacientes com insuficiência cardíaca crônica (ICC) permanece controversa.
Uma meta-análise foi realizada para verificar os efeitos do Yoga sobre a capacidade de exercício e qualidade de vida relacionada à saúde (QVRS) em pacientes com ICC. Material e métodos: As bases MEDLINE, Cochrane Controlled Trials Register, EMBASE, SPORT Scielo, CINAHL (da data mais antiga disponível a dezembro de 2013) foram pesquisadas para a identificação de ensaios clínicos randomizados (ECRs) que investigaram os efeitos do Yoga (em relação ao grupo praticante de exercícios físicos e/ou grupo controle) sobre a capacidade de exercício (VO2 pico) e qualidade de vida relacionada à saúde (QVRS) em pacientes com ICC. Dois avaliadores selecionaram os ensaios clínicos de forma independente. Diferenças médias ponderadas (DMPs) e intervalos de confiança de 95% (IC 95%) foram calculados, e a heterogeneidade foi avaliada através do teste I2.
Dois ensaios clínicos atenderam os critérios de elegibilidade, perfazendo um grupo amostral com 30 pacientes praticantes de Yoga e 29 pacientes controle. Os resultados sugerem que o Yoga teve um impacto positivo sobre o VO2 pico e QVRS em comparação com o grupo controle. O grupo praticante de Yoga apresentou um aumento no VO2 pico e na diferença média ponderada (IC 95% 3,87: 1,95-5,80) e aumento na diferença média padronizada na QVRS (IC 95% -12,46: -22,49 a -2,43) em comparação ao grupo controle.
A prática de Yoga aumenta o VO2 pico e QVRS em pacientes com ICC e poderá ser incluída em programas de reabilitação cardíaca. ECRs mais abrangentes são necessários para elucidar os efeitos do Yoga em pacientes com ICC.
Ioga; Insuficiência Cardíaca; Terapias Complementares/utilização; Terapia por Execício; Metanálise
Introduction
Chronic heart failure (CHF) can be considered the end stage of heart disease. This syndrome is clinically characterized by poor exercise capacity and quality of life. In context, exercise training is widely recognized as non-pharmacological intervention to improve patient's exercise tolerance and quality of life11 Piepoli MF, Conraads V, Corrà U, Dickstein K, Francis DP, Jaarsma T, et al. Exercise training in heart failure: from theory to practice: a consensus document of the Heart Failure Association and the European Association for Cardiovascular Prevention and Rehabilitation. Eur J Heart Fail. 2001;13(4):347-57..
Despite the well-known benefits of exercise training in patients with CHF, such as improvements in peak oxygen consumption (peak VO2) and health-related quality of life (HRQOL) and reduced heart failure-related hospitalizations22 Davies EJ, Moxham T, Rees K, Singh S, Coats AJ, Ebrahim S, et al. Exercise training for systolic heart failure: Cochrane systematic review and meta-analysis. Eur J Heart Fail. 2010;12(7):706-15., there is no consensus regarding which method of exercise is the most efficient. On the other hand, cardiac rehabilitation teams employ non-conventional methods of exercise training according to patient preference and availability, such as hydrotherapy33 Cider A, Schaufelberger M, Sunnerhagen KS, Andersson B. Hydrotherapy--a new approach to improve function in the older patient with chronic heart failure. Eur J Heart Fail. 2003;5(4):527-35., dance44 Belardinelli R, Lacalaprice F, Ventrella C, Volpe L, Faccenda E. Waltz dancing in patients with chronic heart failure: new form of exercise training. Circ Heart Fail. 2008;1(2):107-14., and yoga55 Howie-Esquivel J, Lee J, Collier G, Mehling W, Fleischmann K.Yoga in heart failure patients: a pilot study. J Cardiac Fail. 2010;16(9):742-9..
Yoga is a relaxation and meditation technique based on postures, exercises, and breathing techniques that have various medical benefits in the treatment of anxiety66 Kirkwood G, Rampes H, Tuffrey V, Richardson J, Pilkington K. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39(12):884-91., depression77 Cramer H, Lauche R, Langhorst J, Dobos G. Yoga for depression: a systematic review and meta-analysis. Depress Anxiety. 2013;30(11):1068-83., breast cancer88 Zhang J, Yang KH, Tian JH, Wang CM. Effects of yoga on psychologic function and quality of life in women with breast cancer: a meta-analysis of randomized controlled trials. J Altern Complement Med. 2012;18(11):994-1002., chronic low back pain99 Holtzman S, Beggs RT. Yoga for chronic low back pain: a meta-analysis of randomized controlled trials. Pain Res Manag. 2013;18(5):267-72., and hypertension1010 Hagins M, States R, Selfe T, Innes K. Effectiveness of yoga for hypertension: systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:649836.. A systematic review on yoga in patients with heart diseases was recently published1111 Cramer H, Lauche R, Haller H, Gustav Dobos G, Michalsen A. A systematic review of yoga for heart disease . Eur J Prev Cardiol. 2014;3:1-12 .. It clarified many clinical aspects of yoga; however, the main outcome measures were mortality, non-fatal cardiac events, exercise capacity, HRQOL, and modifiable cardiac risk factors.
Meta-analyses have never been performed to investigate the outcomes of yoga in patients with CHF. It is known that meta-analysis technique minimizes subjectivity by standardizing treatment implications of relevant studies into effect sizes, pooling the data, and then analyzing it to draw conclusions. The aim of this systematic review was to meta-analyze published randomized controlled trials (RCTs) that investigated the effects of yoga in peakVO2 and HRQOL in patients with CHF.
Methods
Eligibility Criteria
Types of studies
This meta-analysis included RCTs that examined the impact of any type of yoga in patients with CHF. Studies were considered for inclusion regardless of their publication status, language, or size.
Types of participants
Trials enrolling patients with systolic or diastolic CHF were included in this meta-analysis. To be eligible, a trial required patients with CHF randomized to at least one group of any type of yoga. The studies that enrolled patients with any kind of respiratory diseases were excluded from this systematic review.
Types of outcome measures
The main outcomes of interest were peak oxygen consumption (mL/kg/min) measured by gas analysis and HRQOL (measured by any questionnaire).
Search methods for identification of studies
Electronic searches
We searched for references on MEDLINE via PubMed, LILACS, Excerpta Medica database (EMBASE), The Scientific Electronic Library Online, Cumulative Index to Nursing and Allied Health, Physiotherapy Evidence Database (PEDro), and Cochrane Central Register of Controlled Trials up to December 2013, without language restrictions. A standard protocol for this search was developed and whenever possible, controlled vocabulary (medical subject heading term for MEDLINE and Cochrane, and Emtree (a life science thesaurus) for EMBASE) were used. Keywords and their synonyms were used to sensitize the search. Table 1 presents the search strategy for MEDLINE via PubMed.
For the identification of RCTs in PubMed/MEDLINE, the optimal sensitive strategy developed by the Cochrane Collaboration was used1010 Hagins M, States R, Selfe T, Innes K. Effectiveness of yoga for hypertension: systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:649836.. To identify the RCTs in EMBASE, a search strategy using similar terms was adopted. In the search strategy, there were four groups of keywords: study design, participants, interventions, and outcome measures. All eligible articles for this meta-analysis had their references analyzed in order to detect other potentially eligible studies. For ongoing studies or when the confirmation of any data or additional information was needed, the authors were contacted by e-mail.
Data collection and analysis
Assessment of study eligibility
The previously described search strategy was used to obtain titles and abstracts of studies that might be relevant for this review. Each abstract identified in the research was independently evaluated by two authors. If at least one of the authors considered one reference eligible, the full text was obtained for complete assessment.
In a similar fashion, two authors independently evaluated full-text articles for eligibility and filled inclusion and exclusion criteria in a standard form. A standardized data extraction form was used for the inclusion and exclusion criteria. In case of any disagreement, the authors discussed the reasons for their decisions and a final decision was made by consensus.
Data extraction
Two authors independently extracted data from the published reports using standard data extraction forms adapted from the Cochrane Collaboration's1212 Higgins JPT, Green S (eds.) The Cochrane Handbook for Systematic Reviews of Interventions 4.2.6 [updated Sept.2006] . In: The Cochrane Library, Issue 4, 2006. Chichester (UK): John Wiley & Sons, Ltd.; 2006. model for data extraction, considering 1) aspects of the study population, such as the average age and sex; 2) aspects of the intervention performed (sample size, type of yoga performed, presence of supervision, frequency, and duration of each session); 3) follow-up; 4) loss to follow-up; 5) outcome measures; and 6) presented results. Disagreements were resolved by one of the authors. Any further information required from the original author was requested by e-mail.
Risk of bias of included studies
The risk of bias of included studies was assessed independently by two authors using the Cochrane Collaboration's Risk of Bias tool1212 Higgins JPT, Green S (eds.) The Cochrane Handbook for Systematic Reviews of Interventions 4.2.6 [updated Sept.2006] . In: The Cochrane Library, Issue 4, 2006. Chichester (UK): John Wiley & Sons, Ltd.; 2006.. The following criteria were assessed: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, intention-to-treat analysis, and completeness of follow-up.
Quality of meta-analysis evidence
The quality of evidence generated by this meta-analysis was classified using the PEDro scale. There are several scales for assessing the quality of RCTs. The PEDro scale assesses the methodological quality of a study based on important criteria, such as concealed allocation, intention-to-treat analysis, and the adequacy of follow-up. These characteristics make the PEDro scale a useful tool for assessing the quality of physical therapy and rehabilitation trials1313 Olivo SA, Macedo LG, Gadotti IN, Fuentes J, Stanton T, Magee DJ. Scales to assess the quality of randomized controlled trials: a systematic review. PhysTher. 2008;88(2):156-75..
Methodological quality was independently assessed by two researchers. Studies were scored on the PEDro scale based on the Delphi list , which consisted of 11 items. One item on the PEDro scale (eligibility criteria) is related to external validity and is generally not used to calculate the method score, leaving a score range of 0 to 10. Any disagreements were resolved by a third rater1414 Verhagen AP, de Vet HCW, de Bie RA, Kessels AGH, Boers M, Bouter LM, et al. The Delphi List: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi Consensus. J Clin Epidemiol. 1998;51(12):1235-41.,1515 Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating of quality randomized controlled trials. Phys Ther. 2003;83(8):713-21..
Statistical assessment
Pooled effect estimates were obtained by comparing the least square mean percentage
change from baseline to study end for each group, and were expressed as the weighted
mean difference (WMD) between groups. Calculations were performed using a fixed
effects model. One comparison was made: yoga versus control group. An α value of 0.05
was considered statistically significant. Statistical heterogeneity of the treatment
effect among studies was assessed using Cochran's Q test and the inconsistency
I2 test, in which values above 25% and 50% were
considered indicative of moderate and high heterogeneity, respectively1616 Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in
meta-analyses. BMJ. 2003; 327(7414):557-60.. All analyses were conducted using Review
Manager version 5.0 (Cochrane Collaboration)1717 The Cochrane Collaboration. [Internet]. [Cited in 2013 Feb 12].
Available from: http://www.cochrane.org/handbook
http://www.cochrane.org/handbook...
.
Results
Description of selected studies
The initial search led to the identification of 10 abstracts, from which 4 studies were considered as potentially relevant and were retrieved for detailed analysis. After a complete reading of four articles, two were excluded because although yoga was used as a treatment, the sample had patients with other cardiac diseases. Only two papers1818 Pullen PR, Nagamia SH, Mehta PK, Thompson WR, Benardon D, Hammoud R, et al. Effects of yoga on inflammation and exercise capacity in patients with chronic heart failure. J Cardiac Fail. 2008;14(5):407-13.,1919 Pullen PP, Thompson WR, Benardon D, Brandon J, Mehta PK, Rifai L, et al. Benefits of yoga for African American Heart Failure Patients. Med Sci Sports Exerc. 2010; 42(4):651-7.met the eligibility criteria. Figure 1 shows the PRISMA2020 Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA GROUP. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339: b2535. flow diagram of studies in this review.
The remaining two articles were fully analyzed and approved by both reviewers and data were extracted from each RCT. Table 2 individually displays the results of the assessment of the PEDro scale. The studies failed to provide sufficient detail for us to assess the potential risk of bias. Information regarding the generation and concealment of the random allocation sequence was not reported. The two studies presented objective evidence of balance in baseline characteristics and stated that they took measures to blind those involved in assessments.
Study characteristics
The final sample size ranged from 1918 to 4019, and the mean age of participants
ranged from 51 to 54 years. The two studies included patients of both genders, but
there was a predominance of males. All studies analyzed in this review included
out-patients with documented heart failure New York Heart Association class I-III.
One study included patients with systolic and diastolic CHF1717 The Cochrane Collaboration. [Internet]. [Cited in 2013 Feb 12].
Available from: http://www.cochrane.org/handbook
http://www.cochrane.org/handbook...
, and the other just systolic CHF1818 Pullen PR, Nagamia SH, Mehta PK, Thompson WR, Benardon D, Hammoud R, et
al. Effects of yoga on inflammation and exercise capacity in patients with chronic
heart failure. J Cardiac Fail. 2008;14(5):407-13.. Furthermore, one study reported the race of the patients (95%
were African American)1919 Pullen PP, Thompson WR, Benardon D, Brandon J, Mehta PK, Rifai L, et al.
Benefits of yoga for African American Heart Failure Patients. Med Sci Sports Exerc.
2010; 42(4):651-7..
Outcomes of included studies
Peak VO2
In both studies, peak VO2 was assessed by a cardiopulmonary exercise test and a treadmill was used for the graded exercise test1818 Pullen PR, Nagamia SH, Mehta PK, Thompson WR, Benardon D, Hammoud R, et al. Effects of yoga on inflammation and exercise capacity in patients with chronic heart failure. J Cardiac Fail. 2008;14(5):407-13.,1919 Pullen PP, Thompson WR, Benardon D, Brandon J, Mehta PK, Rifai L, et al. Benefits of yoga for African American Heart Failure Patients. Med Sci Sports Exerc. 2010; 42(4):651-7..
HRQOL
The Minnesota Living with Heart Failure Questionnaire was used in both studies1818 Pullen PR, Nagamia SH, Mehta PK, Thompson WR, Benardon D, Hammoud R, et al. Effects of yoga on inflammation and exercise capacity in patients with chronic heart failure. J Cardiac Fail. 2008;14(5):407-13.,1919 Pullen PP, Thompson WR, Benardon D, Brandon J, Mehta PK, Rifai L, et al. Benefits of yoga for African American Heart Failure Patients. Med Sci Sports Exerc. 2010; 42(4):651-7.. Table 3 presents summary data from the two RCTs eligible for this systematic review.
Characteristics of the outcomes, measures, and results of yoga therapy in the trials included in the review
Characteristics of intervention programs
The characteristics of the intervention (yoga) were reported in the studies. The duration of the yoga program ranged from 819 to 1018 weeks. Regarding the time of the session, there was a variation from 6018 to 7019 min. In the study by Pullen et al1818 Pullen PR, Nagamia SH, Mehta PK, Thompson WR, Benardon D, Hammoud R, et al. Effects of yoga on inflammation and exercise capacity in patients with chronic heart failure. J Cardiac Fail. 2008;14(5):407-13., during each session, subjects completed the following: a 10-min warm-up phase, a 40-min period of standing or seated yoga postures (asana), and finally a 20-min relaxation phase including breathing exercises (pranayama), and meditation. A 5-min warm-up phase including breathing exercises (pranayama), a 40-min period of standing and/or seated yoga postures (asana), and finally, a 15-min relaxation phase were used in the other study1919 Pullen PP, Thompson WR, Benardon D, Brandon J, Mehta PK, Rifai L, et al. Benefits of yoga for African American Heart Failure Patients. Med Sci Sports Exerc. 2010; 42(4):651-7.. Both studies used hatha yoga intervention.
The frequency of sessions was two times a week in both studies1818 Pullen PR, Nagamia SH, Mehta PK, Thompson WR, Benardon D, Hammoud R, et al. Effects of yoga on inflammation and exercise capacity in patients with chronic heart failure. J Cardiac Fail. 2008;14(5):407-13.,1919 Pullen PP, Thompson WR, Benardon D, Brandon J, Mehta PK, Rifai L, et al. Benefits of yoga for African American Heart Failure Patients. Med Sci Sports Exerc. 2010; 42(4):651-7.. Yoga sessions were conducted by a registered yoga teacher (Yoga Alliance) certified by the American College of Sports Medicine.
The analyzed studies reported that both treatment groups (yoga and control) received an educational program and a brochure with instructions for following a home walk program (standard medical treatment). Both groups were followed by blinded researchers from the beginning to the end of the study.
Peak VO2
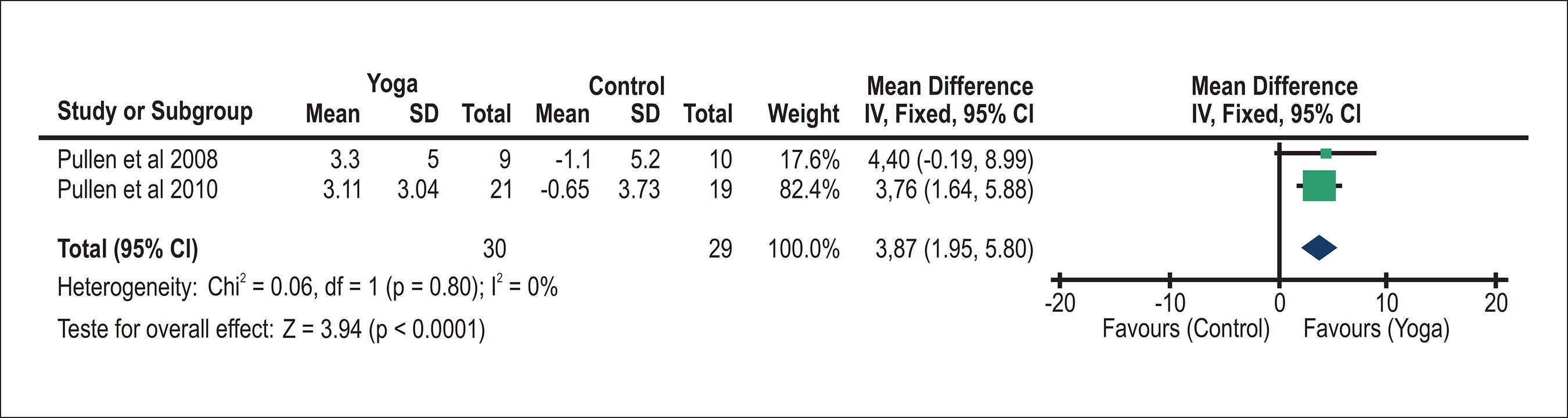
Both studies assessed peak VO2 as an outcome1818 Pullen PR, Nagamia SH, Mehta PK, Thompson WR, Benardon D, Hammoud R, et al. Effects of yoga on inflammation and exercise capacity in patients with chronic heart failure. J Cardiac Fail. 2008;14(5):407-13.,1919 Pullen PP, Thompson WR, Benardon D, Brandon J, Mehta PK, Rifai L, et al. Benefits of yoga for African American Heart Failure Patients. Med Sci Sports Exerc. 2010; 42(4):651-7.. The meta-analyses showed (Figure 2) a significant improvement in peak VO2 of 3.87 mL·kg-1·min-1 (95% confidence interval (CI): 1.95, 5.80, N = 59) for participants in the yoga group compared with controls.
Yoga versus controls: VO2 Peak. Review Manager (version 5.2; the Cochrane Collaboration, 2013). SD: standard deviation; CI = Confidence intervals
Quality of life
Both studies assessed HRQOL1818 Pullen PR, Nagamia SH, Mehta PK, Thompson WR, Benardon D, Hammoud R, et al. Effects of yoga on inflammation and exercise capacity in patients with chronic heart failure. J Cardiac Fail. 2008;14(5):407-13.,1919 Pullen PP, Thompson WR, Benardon D, Brandon J, Mehta PK, Rifai L, et al. Benefits of yoga for African American Heart Failure Patients. Med Sci Sports Exerc. 2010; 42(4):651-7.. Significant enhancements were found among patients in the yoga group compared to the control group. Due to the difference between the instruments used in the measurement of quality of life, we performed a meta-analysis with a standardized mean difference. The meta-analyses showed (Figure 3) significant improvement in HRQOL of -12.46 (95% CI: -22.49, -2.43, n = 59) for participants in the yoga group in comparison to controls.
Yoga versus controls: Quality of Life. Review Manager (version 5.2; the Cochrane Collaboration, 2013). SD: standard deviation; CI: Confidence intervals.
Discussion
In the present systematic review, a meta-analysis of two studies demonstrated augmentations in peak VO2 and HRQOL in patients with CHF after yoga sessions when compared to controls.
Yoga is an emerging therapy for the rehabilitation of chronic diseases. However, to date, no meta-analysis examined the impact of yoga in patients with CHF. This review is important because it analyzes yoga as a potential modality in cardiovascular rehabilitation.
Our meta-analysis showed 22.0% improvement in peak VO2 in the yoga group. The mean peak VO2 in the two studies analyzed was 15.85 mL·kg-1·min-1 at baseline and 19.05 mL·kg-1 ·min-1 at the end of the intervention. Specifically, the WMD in peak VO2 peak was 3.97 mL·kg-1 ·min-1 from baseline to post-intervention. The magnitude of change is similar to a previous meta-analysis that evaluated the effect of different modalities of exercise in patients with CHF2121 Haykowsky MJ, Liang Y, Pechter D, Jones LW, McAlister FA, Clark AM. A meta-analysis of the effect of exercise training on left ventricular remodeling in heart failure patients: the benefit depends on the type of training performed. J Am Coll Cardiol. 2007;49(24):2329-36.,2222 Haykowsky MJ, Timmons MP, Kruger C, McNeely M, Taylor DA, Clark AM. Meta-analysis of aerobic interval training on exercise capacity and systolic function in patients with heart failure and reduced ejection fractions. Am J Cardiol. 2013;111(10):1466-9..
Another important factor to be described is the extent of the improvement and the peak VO2 of 19.05 mL·kg-1 ·min-1 achieved after the intervention. A minimum peak VO2 of 15 mL·kg-1 ·min-1 in women and 18 mL·kg-1 ·min-1 in men aged 85 years has been demonstrated to be necessary for full and independent living (e.g., garden activities, walking up stairs, etc.)2323 Paterson DH, Cunningham DA, Koval JJ, St Croix CM. Aerobic fitness in a population of independently living men and women aged 55-86 years. Med Sci Sports Exerc.1999;31(12):1813-20.. Thus, yoga patients with CHF improve their medical condition, so they can productively carry out everyday activities.
In this study, yoga is shown to be effective in the rehabilitation of patients with CHF. Considering peak VO2, it is well known that improvements above 10% after a cardiovascular rehabilitation program are satisfactory and represents a good prognosis in patients with CHF2424 Frankenstein L, Nelles M, Hallerbach M, Dukic D, Fluegel A, Schellberg D, et al. Prognostic impact of peakVO2-changes in stable CHF on chronic beta-blocker treatment. Int J Cardiol. 2007;122(2):125-30..
The assessment of the HRQOL is an essential outcome in the rehabilitation process. It is recognized that HRQOL is also associated with mental and physical status. Yoga is reported to improve important mental endpoints, such as anxiety and depression. In addition, yoga has been found to be critical for the enhancement of patients' exercise capacity.
In regards to HRQOL, our meta-analysis showed a 24.1% increase in the yoga group. The mean of MLFHQ of both studies analyzed was 37.5 at baseline and 28.45 at the end of the intervention, demonstrating an improvement of nine points on the scale. The study by Arnold et al2525 Arnold M, Rajda M, Ignaszewski A, Howlett J, Leblanc M-H. Changes in the Minnesota living with heart failure questionnaire score and clinical outcomes in a large contemporary population of ambulatory heart failure patients in the Canadian Heart Failure Network. J Card Fail. 2012;18(8 Supplement):S79. showed that the minimal clinically important difference for the MLFHQ is five points. The WMD in the MLFHQ was -12.46 from baseline to post-intervention. The magnitude of change is similar to that reported in a previous meta-analysis study that included six RCTs about exercise in CHF2525 Arnold M, Rajda M, Ignaszewski A, Howlett J, Leblanc M-H. Changes in the Minnesota living with heart failure questionnaire score and clinical outcomes in a large contemporary population of ambulatory heart failure patients in the Canadian Heart Failure Network. J Card Fail. 2012;18(8 Supplement):S79..
Our results are similar to the ones found in previous studies concerning exercise training2121 Haykowsky MJ, Liang Y, Pechter D, Jones LW, McAlister FA, Clark AM. A meta-analysis of the effect of exercise training on left ventricular remodeling in heart failure patients: the benefit depends on the type of training performed. J Am Coll Cardiol. 2007;49(24):2329-36.,2222 Haykowsky MJ, Timmons MP, Kruger C, McNeely M, Taylor DA, Clark AM. Meta-analysis of aerobic interval training on exercise capacity and systolic function in patients with heart failure and reduced ejection fractions. Am J Cardiol. 2013;111(10):1466-9.,2626 Davies EJ, Moxham T, Rees K, Singh S, Coats AJS, Ebrahim S. Exercise training for systolic heart failure: Cochrane systematic review and meta-analysis. Eur J Heart Fail. 2010;12 (7):706-15.. The adherence of patients with CHF to exercise training is low; therefore, the investigation of new strategies is important in the context of rehabilitation. Despite the best method to improve exercise capacity and/or HRQOL, the first point that should be considered is patient preference. Taking this into account, the number of subjects that drop out of cardiovascular rehabilitation programs could possibly be decreased.
This review is limited because we did not consider the strict description of the criteria used by the authors to diagnose CHF, which can compromise the reliability of the results. It is not possible to consistently recommend yoga in patients with CHF. Our search strategy only found two RCTs with small samples and low duration of intervention. Furthermore, different variables may influence the effects of yoga as a therapy, such as personal approach and culture. Despite this, yoga appears to be an interesting means of cardiac rehabilitation and deserves further investigation with better-controlled RCTs.
Conclusion
Considering the available data, our meta-analysis showed that yoga improved peak VO2 and HRQOL in patients with CHF. Yoga should be considered as an alternative method of exercise training in patients with CHF.
References
-
1Piepoli MF, Conraads V, Corrà U, Dickstein K, Francis DP, Jaarsma T, et al. Exercise training in heart failure: from theory to practice: a consensus document of the Heart Failure Association and the European Association for Cardiovascular Prevention and Rehabilitation. Eur J Heart Fail. 2001;13(4):347-57.
-
2Davies EJ, Moxham T, Rees K, Singh S, Coats AJ, Ebrahim S, et al. Exercise training for systolic heart failure: Cochrane systematic review and meta-analysis. Eur J Heart Fail. 2010;12(7):706-15.
-
3Cider A, Schaufelberger M, Sunnerhagen KS, Andersson B. Hydrotherapy--a new approach to improve function in the older patient with chronic heart failure. Eur J Heart Fail. 2003;5(4):527-35.
-
4Belardinelli R, Lacalaprice F, Ventrella C, Volpe L, Faccenda E. Waltz dancing in patients with chronic heart failure: new form of exercise training. Circ Heart Fail. 2008;1(2):107-14.
-
5Howie-Esquivel J, Lee J, Collier G, Mehling W, Fleischmann K.Yoga in heart failure patients: a pilot study. J Cardiac Fail. 2010;16(9):742-9.
-
6Kirkwood G, Rampes H, Tuffrey V, Richardson J, Pilkington K. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39(12):884-91.
-
7Cramer H, Lauche R, Langhorst J, Dobos G. Yoga for depression: a systematic review and meta-analysis. Depress Anxiety. 2013;30(11):1068-83.
-
8Zhang J, Yang KH, Tian JH, Wang CM. Effects of yoga on psychologic function and quality of life in women with breast cancer: a meta-analysis of randomized controlled trials. J Altern Complement Med. 2012;18(11):994-1002.
-
9Holtzman S, Beggs RT. Yoga for chronic low back pain: a meta-analysis of randomized controlled trials. Pain Res Manag. 2013;18(5):267-72.
-
10Hagins M, States R, Selfe T, Innes K. Effectiveness of yoga for hypertension: systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:649836.
-
11Cramer H, Lauche R, Haller H, Gustav Dobos G, Michalsen A. A systematic review of yoga for heart disease . Eur J Prev Cardiol. 2014;3:1-12 .
-
12Higgins JPT, Green S (eds.) The Cochrane Handbook for Systematic Reviews of Interventions 4.2.6 [updated Sept.2006] . In: The Cochrane Library, Issue 4, 2006. Chichester (UK): John Wiley & Sons, Ltd.; 2006.
-
13Olivo SA, Macedo LG, Gadotti IN, Fuentes J, Stanton T, Magee DJ. Scales to assess the quality of randomized controlled trials: a systematic review. PhysTher. 2008;88(2):156-75.
-
14Verhagen AP, de Vet HCW, de Bie RA, Kessels AGH, Boers M, Bouter LM, et al. The Delphi List: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi Consensus. J Clin Epidemiol. 1998;51(12):1235-41.
-
15Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating of quality randomized controlled trials. Phys Ther. 2003;83(8):713-21.
-
16Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327(7414):557-60.
-
17The Cochrane Collaboration. [Internet]. [Cited in 2013 Feb 12]. Available from: http://www.cochrane.org/handbook
» http://www.cochrane.org/handbook -
18Pullen PR, Nagamia SH, Mehta PK, Thompson WR, Benardon D, Hammoud R, et al. Effects of yoga on inflammation and exercise capacity in patients with chronic heart failure. J Cardiac Fail. 2008;14(5):407-13.
-
19Pullen PP, Thompson WR, Benardon D, Brandon J, Mehta PK, Rifai L, et al. Benefits of yoga for African American Heart Failure Patients. Med Sci Sports Exerc. 2010; 42(4):651-7.
-
20Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA GROUP. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339: b2535.
-
21Haykowsky MJ, Liang Y, Pechter D, Jones LW, McAlister FA, Clark AM. A meta-analysis of the effect of exercise training on left ventricular remodeling in heart failure patients: the benefit depends on the type of training performed. J Am Coll Cardiol. 2007;49(24):2329-36.
-
22Haykowsky MJ, Timmons MP, Kruger C, McNeely M, Taylor DA, Clark AM. Meta-analysis of aerobic interval training on exercise capacity and systolic function in patients with heart failure and reduced ejection fractions. Am J Cardiol. 2013;111(10):1466-9.
-
23Paterson DH, Cunningham DA, Koval JJ, St Croix CM. Aerobic fitness in a population of independently living men and women aged 55-86 years. Med Sci Sports Exerc.1999;31(12):1813-20.
-
24Frankenstein L, Nelles M, Hallerbach M, Dukic D, Fluegel A, Schellberg D, et al. Prognostic impact of peakVO2-changes in stable CHF on chronic beta-blocker treatment. Int J Cardiol. 2007;122(2):125-30.
-
25Arnold M, Rajda M, Ignaszewski A, Howlett J, Leblanc M-H. Changes in the Minnesota living with heart failure questionnaire score and clinical outcomes in a large contemporary population of ambulatory heart failure patients in the Canadian Heart Failure Network. J Card Fail. 2012;18(8 Supplement):S79.
-
26Davies EJ, Moxham T, Rees K, Singh S, Coats AJS, Ebrahim S. Exercise training for systolic heart failure: Cochrane systematic review and meta-analysis. Eur J Heart Fail. 2010;12 (7):706-15.
-
Author contributionsConception and design of the research and Writing of the manuscript: Gomes-Neto M, Rodrigeus-Jr ES, Carvalho VO; Acquisition of data: Rodrigeus-Jr ES, Carvalho VO; Analysis and interpretation of the data and Statistical analysis: Gomes-Neto M, Silva-Jr WM; Critical revision of the manuscript for intellectual content: Gomes-Neto M, Silva-Jr WM, Carvalho VO.
-
Sources of FundingThere were no external funding sources for this study.
-
Study AssociationThis study is not associated with any thesis or dissertation work.
Publication Dates
-
Publication in this collection
10 Oct 2014 -
Date of issue
Nov 2014
History
-
Received
20 Feb 2014 -
Reviewed
30 June 2014 -
Accepted
28 July 2014