1. Definition of the Problem
A) Purpose of the Guideline
The main aim of the guidelines is to update the concepts promulgated by its two predecessors, namely, the I and II Guidelines for Perioperative Evaluation of the Brazilian Society of Cardiology published in 2007 and 2011, respectively.11 Gualandro DM, Yu PC, Calderaro D, Marques AC, Pinho C, Caramelli B, et al. II Guidelines for perioperative evaluation of the Brazilian Society of Cardiology. Arq Bras Cardiol. 2011;96(3 Suppl 1):1-68. When the systematic review of the collected evidence was conducted after five years since the last publication, we noticed a remarkable evolution of the knowledge on the subject, particularly in cardiology. In the perioperative environment, the physician needs to simultaneously gather concepts from different specialties to understand different aspects of the same problem and to optimize the language among clinicians, surgeons, anesthesiologists, and intensivists. Although problems related to other disciplines are addressed in this III Guidelines, we decided that the text should adopt the point of view of a cardiologist. In line with this decision, the III Guidelines incorporated the term cardiovascular and was thus termed Guidelines for Perioperative Cardiovascular Evaluation. Based on new findings, some novelties were included, such as new oral anticoagulants and surgical interventions in patients with dual antiplatelet therapy (DAPT), in patients with last generation stents. Anticoagulants and antiplatelet agents were discussed in more detail for specific surgical procedures, such as dental, dermatological, endoscopic, and ophthalmologic.
B) Methodology and Evidence
The systematic review performed to elaborate the III Guidelines considered aspects related to the serious allegations of fraud involving the work of the group led by Don Poldermans of the Erasmus Medical Center in the Netherlands. The group published studies, known as DECREASE trials, which investigated important aspects in the perioperative environment, such as the use of β-blockers and biomarkers and invasive stratification, in significant groups of patients. The report released by the Erasmus Medical Center describes several problems in these studies, including neglect and scientific inaccuracies, especially in DECREASE IV.22 Dunkelgrun M, Boersma E, Schouten O, Koopman-van Gemert AW, van Poorten F, Bax JJ, et al; Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Bisoprolol and fluvastatin for the reduction of perioperative cardiac mortality and myocardial infarction in intermediate-risk patients undergoing noncardiovascular surgery: a randomized controlled trial (DECREASE-IV). Ann Surg. 2009;249(6):921-6. Other studies from the same group, such as DECREASE V and VI, also presented similar problems, although to a lesser extent.33 Poldermans D, Schouten O, Vidakovic R, Bax JJ, Thomson IR, Hoeks SE, et al; DECREASE Study Group. A clinical randomized trial to evaluate the safety of a noninvasive approach in high-risk patients undergoing major vascular surgery: the DECREASE-V Pilot Study. J Am Coll Cardiol. 2007;49(17):1763-9.,44 Goei D, van Kuijk JP, Flu WJ, Hoeks SE, Chonchol M, Verhagen HJ, et al. Usefulness of repeated N-terminal pro-B-type natriuretic peptide measurements as incremental predictor for long-term cardiovascular outcome after vascular surgery. Am J Cardiol. 2011;107(4):609-14. The conclusions of the report led to the dismissal of Don Poldermans from the Erasmus Medical Center and to the notification of the journals where these papers were published. However, as of the date of the publication of the III Guidelines, the published studies are still available on the sites of the journals and have not been withdrawn. The members of the writing committee of the III Guidelines discussed the matter and unanimously decided that the recommendations should NOT consider the findings of DECREASE IV, V, and VI and that the readers would be informed of this decision.
The methodology and levels of evidence considered for III Guidelines are as follows:
2. Preoperative Evaluation
A) History
Collection of clinical history is the first approach in perioperative evaluation. Anamnesis performed with the patient or family members may provide information on the clinical conditions that determine the estimated surgical risk. The algorithms for perioperative risk assessment use the data obtained by clinical history and physical examination. The study of medical records in medical charts and anesthetic records is useful for retrieving previous information.55 Dakik HA, Kobrossi S, Tamim H. The yield of routine pre-operative cardiovascular evaluation in stable patients scheduled for elective non-cardiac surgery. Int J Cardiol. 2015;186:325-7.,66 Heinisch RH, Barbieri CF, Nunes Filho JR, Oliveira GL, Heinisch LM. Prospective assessment of different indices of cardiac risk for patients undergoing noncardiac surgeries. Arq Bras Cardiol. 2002;79(4):327-38.
To guide the evaluation of surgical risk, the following data are obtained in clinical history: Information of the underlying disease, which indicates the surgical procedure, including information from the surgeon on the risk and location of the procedure, the availability of technical support regarding personnel and equipment, the type of anesthesia, the estimated surgical time, and the need for transfusion; clinical, sociodemographic, and cultural data, such as age, gender, blood type, positive serology for hepatitis C virus, and acceptance of transfusion; data to assess the patient’s psychological/psychiatric condition; thorough investigation of surgical or anesthetic history that may reveal potentially preventable complications or allergies; determination of functional capacity, investigating daily activities (Chart 1).
Investigation of the clinical condition and the need to compensate for coexisting diseases, with a focus on identifying the presence of serious cardiovascular conditions in the perioperative stage (Chart 2).
In patients more than 65 years old, verification of the degree of fragility;88 Melin AA, Schmid KK, Lynch TG, Pipinos II, Kappes S, Longo GM, et al. Preoperative frailty Risk Analysis Index to stratify patients undergoing carotid endarterectomy. J Vasc Surg. 2015;61(3):683-9.
9 Rinkinen J, Agarwal S, Beauregard J, Aliu O, Benedict M, Buchman SR, et al. Morphomic analysis as an aid for preoperative risk stratification in patients undergoing major head and neck cancer surgery. J Surg Res. 2015;194(1):177-84.
10 Scandrett KG, Zuckerbraun BS, Peitzman AB. Operative risk stratification in the older adult. Surg Clin North Am. 2015;95(1):149-72.
11 Amrock LG, Deiner S. The implication of frailty on preoperative risk assessment. Curr Opin Anaesthesiol. 2014;27(3):330-5.
12 Amrock LG, Neuman MD, Lin HM, Deiner S. Can routine preoperative data predict adverse outcomes in the elderly? Development and validation of a simple risk model incorporating a chart-derived frailty score. J Am Coll Surg. 2014;219(4):684-94.
13 Dunne MJ, Abah U, Scarci M. Frailty assessment in thoracic surgery. Interact Cardiovasc Thorac Surg. 2014;18(5):667-70.
14 Hasselager R, Gögenur I. Core muscle size assessed by perioperative abdominal CT scan is related to mortality, postoperative complications, and hospitalization after major abdominal surgery: a systematic review. Langenbecks Arch Surg. 2014;399(3):287-95.
15 Revenig LM, Canter DJ, Taylor MD, Tai C, Sweeney JF, Sarmiento JM, et al. Too frail for surgery? Initial results of a large multidisciplinary prospective study examining preoperative variables predictive of poor surgical outcomes. J Am Coll Surg. 2013;217(4):665-70.e1.
16 Robinson TN, Wu DS, Pointer L, Dunn CL, Cleveland JC, Moss M. Simple frailty score predicts postoperative complications across surgical specialties. Am J Surg. 2013;206(4):544-50.
17 Lee JS, He K, Harbaugh CM, Schaubel DE, Sonnenday CJ, Wang SC, et al; Michigan Analytic Morphomics Group (MAMG). Frailty, core muscle size, and mortality in patients undergoing open abdominal aortic aneurysm repair. J Vasc Surg. 2011;53(4):912-7.-1818 Makary MA, Segev DL, Pronovost PJ, Syin D, Bandeen-Roche K, Patel P, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210(6):901-8. identification of the presence of valvular heart disease (item 4.D), valvular prostheses, and the need for prophylaxis for bacterial endocarditis (item 7.E); investigation of risk factors for cardiopathies; record of the presence of pacemaker or cardioverter/implantable defibrillator and adequate management (item 4.G); diagnosis of peripheral vascular disease, renal insufficiency, cerebral vascular disease, diabetes mellitus (DM), liver disease, hemorrhagic disorders, thyroid disorders, obstructive sleep apnea, and chronic lung disease; use of drugs, phytotherapics, alcohol, illicit drugs, and evaluation of potential interference with the operative procedure.
Doubts of the patient and their relatives regarding the procedure and its risks. Awareness and agreement on the risks and benefits of the procedures. Awareness that surgical risk is not limited to the intraoperative period and, eventually, a prolonged follow-up will be needed. Awareness that complications are not limited to the cardiovascular system;
The data obtained in the clinical evaluation should be dated and recorded in appropriate documents. The day and time of receiving the request and writing the evaluation response should be recorded. Establish a system that expedites preoperative consultation requests in the institution. The information must be available in a legible and explicit format, and the most relevant should be underlined. The preoperative consultation may not be finalized in the first evaluation; ensure that the preoperative consultation has been forwarded and, if necessary, contact the surgeon or anesthesiologist in person or by other means of communication;
Consider the patient’s expectations regarding return to appointments, performance of tests, scheduled date for surgery, waiting list for the surgical procedure, precocity of the procedure, availability of appointments, and operating room.
B) Physical Examination
Physical examination is useful during the perioperative risk assessment process and should not be limited to the cardiovascular system. This examination aims to identify pre-existing or potential cardiopathy (risk factors), define the severity and stability of the heart disease, and identify possible comorbidities.
Patients with heart disease whose general condition is compromised by other conditions, such as neurological diseases, renal failure, infections, liver abnormalities, malnutrition, and pulmonary dysfunction, are at a higher risk of cardiac complications because such conditions exacerbate surgical stress. Patients with peripheral vascular disease have a high incidence of ischemic heart disease, which is a prognostic factor of perioperative complication.
Evidence of, for example, changes in arterial pulses or carotid bruit should be investigated in physical examination. On the other hand, turgid jugulars in preoperative consultation, indicating high central venous pressure (CVP), suggest that the patient may develop postoperative pulmonary edema.1919 Goldman L, Caldera DL, Nussbaum SR, Southwick FS, Krogstad D, Murray B, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med. 1977;297(16):845-50. The evidence of a third heart sound (S3) in the preoperative evaluation is indicative of poor prognosis with an increased risk of pulmonary edema, myocardial infarction, or cardiac death. The evidence of lower limb edema (bilateral) should be analyzed in combination with the presence or absence of jugular venous distention. If CVP is increased, visualized by the height of the oscillation of the pulse of the internal jugular vein, then cardiopathy and pulmonary hypertension (PH) are responsible, at least partially, for the patient’s edema. If CVP is not increased, other causes, such as liver disease, nephrotic syndrome, chronic peripheral venous insufficiency, or use of some medication, are responsible for the edema. Evidence of edema alone and without knowledge of the patient’s CVP is not a definite sign of heart disease.2020 Butman SM, Ewy GA, Standen JR, Kern KB, Hahn E. Bedside cardiovascular examination in patients with severe chronic heart failure: importance of rest or inducible jugular venous distension. J Am Coll Cardiol. 1993;22(4):968-74. In the presence of heart murmurs, the physician should be able to distinguish between organic and functional murmurs, determine if they are significant or not, and identify their origin. The origin will indicate whether endocarditis prophylaxis or evaluation of valvular lesion severity is necessary (items 4.D and 7.E).
In elderly patients, a brief assessment of fragility can be performed using the timed up and go test. In this test, time is measured in seconds with a timer starting from the point when the patient is given the command to get up from a chair and walk three meters forward and return, and ending when the patient sits back in the chair. A test time equal to or greater than 20 seconds is considered poor/low. A test time equal to or greater than 15 seconds is associated with postoperative complications and increased mortality in a period of one year.1515 Revenig LM, Canter DJ, Taylor MD, Tai C, Sweeney JF, Sarmiento JM, et al. Too frail for surgery? Initial results of a large multidisciplinary prospective study examining preoperative variables predictive of poor surgical outcomes. J Am Coll Surg. 2013;217(4):665-70.e1.
Recommendations for Performing a Physical Exam in a Patient Being Evaluated for Perioperative Risk of a Non-cardiac Surgery
C) Additional Tests
In the perioperative evaluation of patients scheduled for surgical procedures, requesting of preoperative tests [electrocardiogram (ECG), chest X-ray, and laboratory tests] is a common and routine clinical practice. However, this is not related to the reduction or prediction of perioperative complications and has a high economic cost for the health system. Therefore, revisions elaborated by several societies have recommended the rational use of tests.2121 Munro J, Booth A, Nicholl J. Routine preoperative testing: a systematic review of the evidence. Health Technol Assess. 1997;1(12):i-iv; 1-62.
22 American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice advisory for preanesthesia evaluation: a report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2002;96(2):485-96.-2323 Health NIf, Care E. NICE Guideline: Routine preoperative tests for elective surgery. United Kingdom; 2016. [Access in 2016 Nov 12]. Available from: https://www.nice.org.uk/guidance/ng45/resources/routine-preoperative-tests-for-elective-surgery-1837454508997
https://www.nice.org.uk/guidance/ng45/re...
In the literature, few studies have evaluated the benefit and impact of preoperative routine tests. Cataract surgery is the surgical procedure that presents the best evidence. Three randomized studies compared performing and not performing routine preoperative examinations and the occurrence of postoperative events in patients undergoing cataract surgery.2424 Schein OD, Katz J, Bass EB, Tielsch JM, Lubomski LH, Feldman MA, et al. The value of routine preoperative medical testing before cataract surgery. Study of Medical Testing for Cataract Surgery. N Engl J Med. 2000;342(3):168-75.
25 Lira RP, Nascimento MA, Moreira-Filho DC, Kara-José N, Arieta CE. Are routine preoperative medical tests needed with cataract surgery? Rev Panam Salud Publica. 2001;10(1):13-7.-2626 Cavallini GM, Saccarola P, D'Amico R, Gasparin A, Campi L. Impact of preoperative testing on ophthalmologic and systemic outcomes in cataract surgery. Eur J Ophthalmol. 2004;14(5):369-74. The systematic review of these three studies, involving 21,531 patients, showed a similar frequency of complications between the two groups. The authors concluded that performing preoperative tests does not increase the safety of cataract surgery and is associated with a 2.5-fold higher cost when compared to the group that did not perform preoperative tests.2727 Keay L, Lindsley K, Tielsch J, Katz J, Schein O. Routine preoperative medical testing for cataract surgery. Cochrane Database Syst Rev. 2012 Mar 14;(3):CD007293. Despite the evidence in the literature, routinely requesting preoperative tests is still common in clinical practice. In a cohort study with 440,857 patients, the authors observed that more than half of the patients undergoing cataract surgery had a preoperative test, especially when the evaluation is performed by ophthalmologists.2828 Chen CL, Lin GA, Bardach NS, Clay TH, Boscardin WJ, Gelb AW, et al. Preoperative medical testing in Medicare patients undergoing cataract surgery. N Engl J Med. 2015;372(16):1530-8.
For other surgeries, only one randomized study investigated the effect of routine preoperative tests on the occurrence of postoperative events and complications.2929 Chung F, Yuan H, Yin L, Vairavanathan S, Wong DT. Elimination of preoperative testing in ambulatory surgery. Anesth Analg. 2009;108(2):467-75. The population of this study mainly consisted of patients with low clinical risk, without serious diseases or decompensated clinical conditions, who underwent small and outpatient surgeries. In this study, the patients were randomized to perform the proposed surgery with or without preoperative tests (ECG, chest X-ray, blood count, urea, creatinine, electrolytes, and glucose). No difference in perioperative morbidity and mortality was found between patients who performed preoperative evaluation with complementary tests and those who did not perform additional tests. The American National Institute of Health conducted an observational study on 73,596 patients undergoing low-risk and selected outpatient procedures (hernia surgeries). The authors reported that 54% of those without comorbidities underwent preoperative tests. The frequency of perioperative complications was extremely low (0.3%). The performance of preoperative tests or the presence of abnormalities in these tests did not predict complications.3030 Benarroch-Gampel J, Sheffield KM, Duncan CB, Brown KM, Han Y, Townsend CM, et al. Preoperative laboratory testing in patients undergoing elective, low-risk ambulatory surgery. Ann Surg. 2012;256(3):518-28.
An extensive review of the literature has shown very limited evidence of clinical effectiveness to recommend routine preoperative tests. No study has demonstrated the cost-effectiveness of preoperative tests in healthy individuals undergoing low-risk or intermediate non-cardiac surgeries.3131 Czoski-Murray C, Lloyd Jones M, McCabe C, Claxton K, Oluboyede Y, Roberts J, et al. What is the value of routinely testing full blood count, electrolytes and urea, and pulmonary function tests before elective surgery in patients with no apparent clinical indication and in subgroups of patients with common comorbidities: a systematic review of the clinical and cost-effective literature. Health Technol Assess. 2012;16(50):i-xvi, 1-159. Abnormal findings in routine tests are relatively frequent, but these results rarely lead to changes in surgical procedure or surgery suspension. In addition, changes in preoperative tests do not predict complications.
In conclusion, there is no indication to perform routine laboratory tests in the preoperative evaluation in asymptomatic patients submitted to low-risk procedures. The indication of preoperative tests should be customized in accordance to the history and physical examination, the diseases and comorbidities presented by the patients, as well as the type and extent of the proposed surgery.
I. Electrocardiogram
The ECG analysis may complement cardiologic evaluation and allow the identification of patients at high cardiac risk. The ECG can detect arrhythmias, conduction disorders, previous myocardial ischemia or acute myocardial infarction (MI), ventricular overloads, and changes due to electrolyte disorders or drug effects. In addition, a baseline electrocardiographic tracing is important for perioperative comparative evaluation in patients at high risk for cardiovascular events.
However, routine application of a test with limited specificity may lead to false-positive results in asymptomatic patients, since electrocardiographic abnormalities often concern the surgical and anesthetic staff and may prompt the unnecessary cancelation of the surgery.3232 Goldberger AL, O'Konski M. Utility of the routine electrocardiogram before surgery and on general hospital admission. Critical review and new guidelines. Ann Intern Med. 1986;105(4):552-7. Abnormalities found on the ECG tend to increase with age and the presence of comorbidities, and these electrocardiographic changes usually have a low prognostic value regarding complications.3333 Liu LL, Dzankic S, Leung JM. Preoperative electrocardiogram abnormalities do not predict postoperative cardiac complications in geriatric surgical patients. J Am Geriatr Soc. 2002;50(7):1186-91.,3434 van Klei WA, Bryson GL, Yang H, Kalkman CJ, Wells GA, Beattie WS. The value of routine preoperative electrocardiography in predicting myocardial infarction after noncardiac surgery. Ann Surg. 2007;246(2):165-70. In a retrospective study involving more than 23,000 patients, the presence of preoperative electrocardiographic changes was associated with higher incidence of cardiac deaths within 30 days.3535 Noordzij PG, Boersma E, Bax JJ, Feringa HH, Schreiner F, Schouten O, et al. Prognostic value of routine preoperative electrocardiography in patients undergoing noncardiac surgery. Am J Cardiol. 2006;97(7):1103-6. This result was corroborated by two prospective studies that found similar results, where preoperative ECG abnormalities predicted perioperative cardiovascular events.3636 Payne CJ, Payne AR, Gibson SC, Jardine AG, Berry C, Kingsmore DB. Is there still a role for preoperative 12-lead electrocardiography? World J Surg. 2011;35(12):2611-6.,3737 Biteker M, Duman D, Tekkesin AI. Predictive value of preoperative electrocardiography for perioperative cardiovascular outcomes in patients undergoing noncardiac, nonvascular surgery. Clin Cardiol. 2012;35(8):494-9. However, in the group of patients submitted to low to moderate risk surgery, preoperative ECG presented limited prognostic information.
Therefore, the indication for preoperative ECG depends on clinical history, surgery type, and diseases presented by the patient.
II. Chest X-ray
Studies evaluating the routine use of chest radiography (X-ray) in the preoperative evaluation have shown that the result of the test rarely interferes with the management of the anesthetic technique and does not predict perioperative complications. Abnormalities found in the X-ray are usually related to chronic diseases, such as COPD and/or cardiomegaly, and are more frequent in male patients older than 60 years, with a higher cardiac risk and with more comorbidities.4040 Silvestri L, Gullo A. Pre-operative chest radiograph. The challenge continues. Minerva Anestesiol. 2004;70(6):437-42.,4141 Joo HS, Wong J, Naik VN, Savoldelli GL. The value of screening preoperative chest x-rays: a systematic review. Can J Anaesth. 2005;52(6):568-74. The indication for preoperative chest X-ray should be based on an initial careful evaluation by using the clinical history and physical exams of the patients. There is no indication for routine chest X-rays in asymptomatic patients as part of the preoperative evaluation.
Recommendations for Requesting an Electrocardiogram2121 Munro J, Booth A, Nicholl J. Routine preoperative testing: a systematic review of the evidence. Health Technol Assess. 1997;1(12):i-iv; 1-62.
22 American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice advisory for preanesthesia evaluation: a report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2002;96(2):485-96.-2323 Health NIf, Care E. NICE Guideline: Routine preoperative tests for elective surgery. United Kingdom; 2016. [Access in 2016 Nov 12]. Available from: https://www.nice.org.uk/guidance/ng45/resources/routine-preoperative-tests-for-elective-surgery-1837454508997
https://www.nice.org.uk/guidance/ng45/re... ,3838 Feely MA, Collins CS, Daniels PR, Kebede EB, Jatoi A, Mauck KF. Preoperative testing before noncardiac surgery: guidelines and recommendations. Am Fam Physician. 2013;87(6):414-8.,3939 García-Miguel FJ, Serrano-Aguilar PG, López-Bastida J. Preoperative assessment. Lancet. 2003;362(9397):1749-57.
Recommendations for Requesting a Chest X-ray2121 Munro J, Booth A, Nicholl J. Routine preoperative testing: a systematic review of the evidence. Health Technol Assess. 1997;1(12):i-iv; 1-62.
22 American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice advisory for preanesthesia evaluation: a report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2002;96(2):485-96.-2323 Health NIf, Care E. NICE Guideline: Routine preoperative tests for elective surgery. United Kingdom; 2016. [Access in 2016 Nov 12]. Available from: https://www.nice.org.uk/guidance/ng45/resources/routine-preoperative-tests-for-elective-surgery-1837454508997
https://www.nice.org.uk/guidance/ng45/re... ,3838 Feely MA, Collins CS, Daniels PR, Kebede EB, Jatoi A, Mauck KF. Preoperative testing before noncardiac surgery: guidelines and recommendations. Am Fam Physician. 2013;87(6):414-8.,3939 García-Miguel FJ, Serrano-Aguilar PG, López-Bastida J. Preoperative assessment. Lancet. 2003;362(9397):1749-57.
III. Recommendations for Requesting Laboratory Tests2121 Munro J, Booth A, Nicholl J. Routine preoperative testing: a systematic review of the evidence. Health Technol Assess. 1997;1(12):i-iv; 1-62.
22 American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice advisory for preanesthesia evaluation: a report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2002;96(2):485-96.-2323 Health NIf, Care E. NICE Guideline: Routine preoperative tests for elective surgery. United Kingdom; 2016. [Access in 2016 Nov 12]. Available from: https://www.nice.org.uk/guidance/ng45/resources/routine-preoperative-tests-for-elective-surgery-1837454508997
https://www.nice.org.uk/guidance/ng45/re... ,3838 Feely MA, Collins CS, Daniels PR, Kebede EB, Jatoi A, Mauck KF. Preoperative testing before noncardiac surgery: guidelines and recommendations. Am Fam Physician. 2013;87(6):414-8.,3939 García-Miguel FJ, Serrano-Aguilar PG, López-Bastida J. Preoperative assessment. Lancet. 2003;362(9397):1749-57.
III.A. Complete Blood Count
D) Perioperative Evaluation Algorithms
Over the years, several indices have been developed to estimate the risk of perioperative events in noncardiac surgeries. Based on these risk indexes, algorithms/flowcharts are suggested to facilitate the perioperative evaluation process and propose strategies to reduce the risk of the events.
I. Risk Indices
Several papers in the literature have compared the accuracy of existing indices for different populations of surgical patients.4242 Gilbert K, Larocque BJ, Patrick LT. Prospective evaluation of cardiac risk indices for patients undergoing noncardiac surgery. Ann Intern Med. 2000;133(5):356-9.
43 Press MJ, Chassin MR, Wang J, Tuhrim S, Halm EA. Predicting medical and surgical complications of carotid endarterectomy: comparing the risk indexes. Arch Intern Med. 2006;166(8):914-20.-4444 Smeili LA, Lotufo PA. Incidence and predictors of cardiovascular complications and death after vascular surgery. Arq Bras Cardiol. 2015;105(5):510-8. Most of these studies show that the various existing indices, although not very accurate, can predict events and should be used in perioperative assessment.
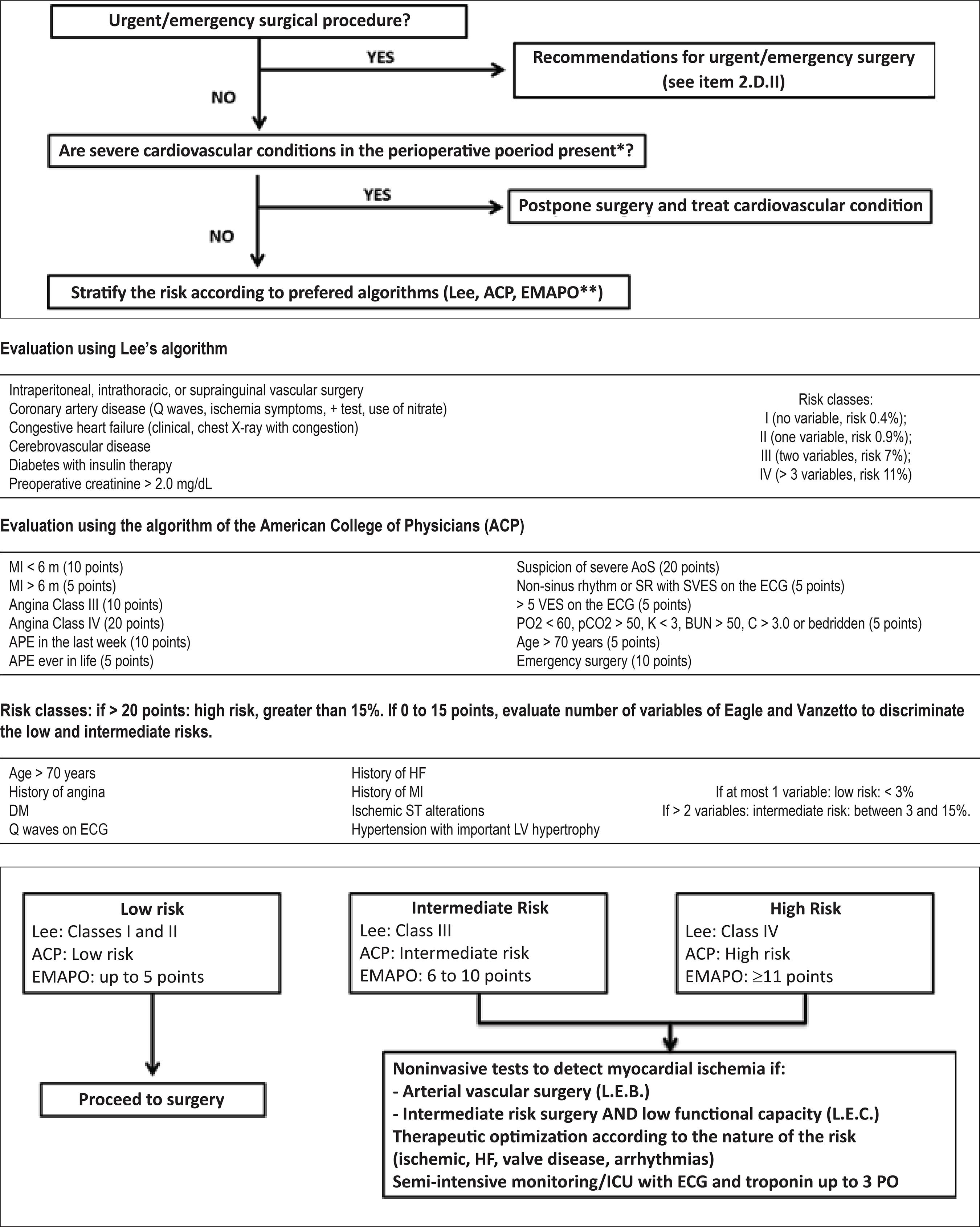
Among the risk indices with cardiovascular outcomes, we highlight the Lee’s Revised Cardiac Risk Index (RCRI),4545 Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043-9. the index developed by the American College of Physicians (ACP),4646 Guidelines for assessing and managing the perioperative risk from coronary artery disease associated with major noncardiac surgery. American College of Physicians. Ann Intern Med. 1997;127(4):309-12.,4747 Palda VA, Detsky AS. Perioperative assessment and management of risk from coronary artery disease. Ann Intern Med. 1997;127(4):313-28. and the Multicenter Perioperative Evaluation Study (EMAPO-www.consultoriodigital.com.br4848 Pinho C, Grandini PC, Gualandro DM, Calderaro D, Monachini M, Caramelli B. Multicenter study of perioperative evaluation for noncardiac surgeries in Brazil (EMAPO). Clinics (Sao Paulo). 2007;62(1):17-22. - the Multicenter Perioperative Evaluation Study was developed and validated in the Brazilian population. All indices have advantages and disadvantages that must be considered during their use. When estimating risk, we should consider which outcome we are predicting: the ACP algorithm predicts the occurrence of AMI and cardiovascular death. The RCRI estimates the risk of AMI, acute pulmonary edema, total atrioventricular block, and cardiorespiratory arrest. The RCRI is widely validated in the literature and shows moderate level of accuracy in predicting events in noncardiac surgeries; this index is less accurate in patients undergoing arterial aortic vascular surgeries and peripheral revascularizations.4949 Ford MK, Beattie WS, Wijeysundera DN. Systematic review: prediction of perioperative cardiac complications and mortality by the revised cardiac risk index. Ann Intern Med. 2010;152(1):26-35. Thus, in a specific evaluation guideline on risk assessment in patients undergoing vascular surgeries,5050 Marques AC, Bellen BV, Caramelli B, Presti C, Pinho C, Calderaro D, et al; Sociedade Brasileira de Cardiologia. [Update and focus on arterial vascular surgeries from the II Guidelines for Perioperative Evaluation of the Brazilian Society of Cardiology]. Arq Bras Cardiol 2013;101(4 Suppl 2):2-32. the VSG-CRI (Vascular Study Group of New England Cardiac Risk Index) is proposed as an alternative to the RCRI; it is adapted from RCRI with additional variables.5151 Bertges DJ, Goodney PP, Zhao Y, Schanzer A, Nolan BW, Likosky DS, et al; Vascular Study Group of New England. The Vascular Study Group of New England Cardiac Risk Index (VSG-CRI) predicts cardiac complications more accurately than the Revised Cardiac Risk Index in vascular surgery patients. J Vasc Surg. 2010;52(3):674-83, 83.e1-83.e3.
When the aim is to estimate global risk, not only related to cardiovascular morbidity and mortality, the ACS NSQIP Surgical Risk Calculator (www.riskcalculator.facs.org), which has been recently developed by the American College of Surgeons, can be used. This tool was developed using data from more than 1 million surgeries in 393 hospitals in the United States. It had good prediction accuracy in that population. This index includes, in addition to the specific type of surgical procedure, 21 clinical variables, providing a risk assessment of 8 different outcomes.5252 Bilimoria KY, Liu Y, Paruch JL, Zhou L, Kmiecik TE, Ko CY, et al. Development and evaluation of the universal ACS NSQIP surgical risk calculator: a decision aid and informed consent tool for patients and surgeons. J Am Coll Surg. 2013;217(5):833-42.e1-3. On the other hand, this tool presents some limitations related to subjective variables and still needs validation in other populations.
As already discussed, risk indices have advantages and limitations, and none of them is perfect. It should be kept in mind that the risk index selected should be used as a complement, but never a replacement, to the evaluator’s opinion. Data or evidence is not always available in the literature for all situations. Thus, assessment should be customized. In those cases where the evaluating physician considers that the index is underestimating the actual risk, this observation should be mentioned in the evaluation.
In addition to the risk indices already mentioned, other features related to surgical procedure and patient should be considered in the evaluation of the risk of perioperative events. We recommend using a flowchart proposed in this guideline (Figure 1).
II. Emergency and Urgent Surgeries vs. Elective Surgeries
In situations when the prognosis of the underlying disease that led to surgical indication demands an emergency intervention, the role of the cardiologist should be restricted to monitoring measures and interventions to reduce the risk in the intra and postoperative periods, with no indication of complementary tests that delay the proposed surgery. For urgent surgeries, there is time to optimize the cardiovascular therapy or to perform complementary tests, such as transthoracic echocardiography, when indicated (item 3.A). On the other hand, the request of functional tests to evaluate myocardial ischemia should not be performed, because the result will not change the plan and the proposed surgery cannot be postponed for 6 weeks (time required for preoperative myocardial revascularization or antiplatelet therapy, if indicated - see items 7.A.V and 7.B).
III. Severe Cardiovascular Conditions in the Perioperative
The first step in elective surgeries is the verification of the patient’s baseline clinical conditions. There are clinical circumstances in which the spontaneous risk of complications is very high, regardless of the surgical procedure. Identification of such conditions is fundamental, because their treatment should take priority over elective surgery, which should be, whenever possible, postponed and reconsidered only after clinical compensation (Chart 2).
IV. Intrinsic Risk of the Procedure
The intrinsic risk of the surgical procedure corresponds to the probability of occurrence of perioperative cardiovascular events, independently of the clinical variables of the patients. It is related to the duration of the procedure, hemodynamic stress, and loss of blood and fluids that occurs during the intervention. Patients with stable clinical conditions who do not present high-risk cardiac conditions may be referred for low intrinsic risk procedures without the need for further evaluation. Despite the difficulty in determining a specific risk for surgical procedures, since they occur in different circumstances, a risk classification of cardiovascular events (death or non-fatal AMI) was proposed for noncardiac surgeries (Chart 3).5353 Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleischmann KE, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery); American Society of Echocardiography.; American Society of Nuclear Cardiology; Heart Rhythm Society; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society for Vascular Medicine and Biology; Society for Vascular Surgery. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery): developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. Circulation. 2007;116(17):e418-99. Erratum in: Circulation. 2008;117(5):e154. Circulation. 2008;118(9): e143-4.
V. Functional Capacity
Patients with low functional capacity are more prone to perioperative complications.1818 Makary MA, Segev DL, Pronovost PJ, Syin D, Bandeen-Roche K, Patel P, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210(6):901-8.,5454 Reilly DF, McNeely MJ, Doerner D, Greenberg DL, Staiger TO, Geist MJ, et al. Self-reported exercise tolerance and the risk of serious perioperative complications. Arch Intern Med. 1999;159(18):2185-92. Functional capacity can be measured objectively using the exercise stress test (which is not always possible or desirable) or clinical history. Limitations in performing activities of daily living, such as walking quickly, climbing stairs, doing household activities or exercising regularly, are evaluated (Chart 1). In addition to the greater probability of poor perioperative evolution, patients with low functional capacity may have their symptoms underestimated due to their restrictions. Therefore, this can be considered when deciding to request complementary tests, such as, for example, non-invasive testing of ischaemic heart disease.
VI. Perioperative Evaluation Flowchart
Based on the above, the III Guideline for Perioperative Cardiovascular Evaluation of the Brazilian Society of Cardiology proposes a flowchart for perioperative evaluation by using the existing risk indices and relevant risk variables for this period (Figure 1). The algorithm contains the conditions that must be analyzed sequentially according to their relevance for the determination of the risk.
Depending on the estimated risk and the nature of the risk, interventions for clinical treatment or additional risk stratification with complementary tests are proposed. This applies to increased risk of ischemic events, decompensation of HF/valvular heart disease, and arrhythmias, considering the current specific guidelines for each case. As an example, if the nature of the risk is ischemic, non-invasive testing of ischaemic heart disease should be considered.
In addition, for patients classified as intermediate or high risk by the algorithms, surveillance for postoperative cardiac events must be performed, including, monitoring in a semi-intensive or intensive care unit (ICU), ECG and troponin being performed once daily up to the third postoperative day.
Perioperative evaluation is a unique opportunity to identify and advice patients about cardiovascular risk factors. During this period, diagnosis of previously unknown diseases, which can be optimized for a better perioperative evolution and, more importantly, for a better long-term prognosis, is often possible.5555 Marques AC, Calderaro D, Yu PC, Gualandro DM, Carmo GA, Azevedo FR, et al. Impact of cardiology referral: clinical outcomes and factors associated with physicians' adherence to recommendations. Clinics (Sao Paulo). 2014;69(10):666-71.
3. Additional Preoperative Evaluation
A) Evaluation of Ventricular Function at Rest
Resting echocardiography in the preoperative period of noncardiac surgery is not a routine test. However, in specific situations, it may offer additional risk information that may be useful for future therapeutic decisions. The use of this procedure in preoperative patients is to evaluate right and left ventricular dysfunction and signs of myocardial ischemia or valvular abnormalities, which are not detected previously in the clinical examination, chest X-ray, or even the ECG. Although controversial, it may be indicated in patients with a surgical risk that justifies this investigation.5656 Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.,5757 Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130(24):e278-333.
Transthoracic echocardiography is the main diagnostic method in patients with suspected or known HF. By using this method, including refined methods of analysis, such as myocardial strain imaging and three-dimensional echocardiography, we can accurately assess ventricular volume, ejection fraction, cardiac output, longitudinal strain, and degree of hemodynamic impairment. Assessment can be performed by determining the diastolic function and pressures in the pulmonary artery and left atrium using the E/e’ ratio and the presence and location of cardiac dys-synchrony in patients with a left ventricular ejection fraction < 35% or with a QRS > 120 ms.5858 Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al; American Society of Echocardiography's Nomenclature and Standards Committee.; Task Force on Chamber Quantification.; American College of Cardiology Echocardiography Committee.; American Heart Association.; European Association of Echocardiography, European Society of Cardiology. Recommendations for chamber quantification. Eur J Echocardiogr. 2006;7(2):79-108.
59 Mor-Avi V, Lang RM, Badano LP, Belohlavek M, Cardim NM, Derumeaux G, et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. J Am Soc Echocardiogr. 2011;24(3):277-313.-6060 Cowie B. Focused transthoracic echocardiography predicts perioperative cardiovascular morbidity. J Cardiothorac Vasc Anesth. 2012;26(6):989-93. However, routine echocardiography is not indicated in all patients because no evidence exists to support that its use is associated with increased survival or shorter hospital stays. Several studies suggest that echocardiography increases hospitalization time, without leading to clinical benefit.6161 Wijeysundera DN, Beattie WS, Karkouti K, Neuman MD, Austin PC, Laupacis A. Association of echocardiography before major elective non-cardiac surgery with postoperative survival and length of hospital stay: population based cohort study. BMJ. 2011;342:d3695. Additionally, in patients with acute HF, clinical compensation should be performed, whenever possible, prior to the intervention.6262 McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al; ESC Committee for Practice Guidelines. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2012;14(8):803-69. Erratum in: Eur J Heart Fail. 2013;15(3):361-2.
In patients with known or suspected valve disease, particularly those with moderate or severe aortic stenosis, severe mitral stenosis, severe mitral or aortic regurgitation, and those with intracardiac prostheses, transthoracic or transesophageal echocardiography should be used to determine the severity of the valve disease, help preoperative clinical treatment and guide prophylaxis or therapy for infective endocarditis (item 7.E).6363 Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Barón-Esquivias G, Baumgartner H, et al; ESC Committee for Practice Guidelines (CPG).; Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC).; European Association for Cardio-Thoracic Surgery (EACTS). Guidelines on the management of valvular heart disease (version 2012): the Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur J Cardiothorac Surg. 2012;42(4):S1-44.
64 Calleja AM, Dommaraju S, Gaddam R, Cha S, Khandheria BK, Chaliki HP. Cardiac risk in patients aged >75 years with asymptomatic, severe aortic stenosis undergoing noncardiac surgery. Am J Cardiol. 2010;105(8):1159-63.
65 Kristensen SD, Knuuti J, Saraste A, Anker S, Bøtker HE, Hert SD, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J. 2014;35(35):2383-431.
66 Habib G, Hoen B, Tornos P, Thuny F, Prendergast B, Vilacosta I, et al; ESC Committee for Practice Guidelines. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J. 2009;30(19):2369-413.-6767 Samarendra P, Mangione MP. Aortic stenosis and perioperative risk with noncardiac surgery. J Am Coll Cardiol. 2015;65(3):295-302.
B) Noninvasive Tests to Detect Myocardial Ischemia
I. Electrocardiogram Exercise Testing
The pathophysiology of perioperative MI differs from that of spontaneous MI. Perioperative MI can be caused by plaque rupture in approximately half of the cases or by imbalance between myocardial oxygen supply (anemia, low flow, etc.) and demand (tachycardia and hypertension).6868 Gualandro DM, Campos CA, Calderaro D, Yu PC, Marques AC, Pastana AF, et al. Coronary plaque rupture in patients with myocardial infarction after noncardiac surgery: frequent and dangerous. Atherosclerosis. 2012;222(1):191-5.
69 Gualandro DM, Calderaro D, Yu PC, Caramelli B. Acute myocardial infarction after noncardiac surgery. Arq Bras Cardiol. 2012;99(5):1060-7.-7070 Padma S, Sundaram PS. Current practice and recommendation for presurgical cardiac evaluation in patients undergoing noncardiac surgeries. World J Nucl Med. 2014;13(1):6-15.
Exercise ECG testing is a safe, useful, and effective tool to detect myocardial ischemia, which is produced by an imbalance between supply and demand. Therefore, it is reasonable to assume that detection of abnormalities while performing this test may be reproducible during the perioperative period and its varying levels of stress. However, whether this strategy leads to reduction of perioperative cardiovascular events in all cases is unknown. It should also be considered that lower prevalence of coronary disease in a population results in lower positive predictive value of the exercise ECG testing.
Considering that risk stratification aims to reduce perioperative risk, performing the test in a population already stratified as low risk by the recommended algorithms is not logical. Therefore, in cases of low prevalence of coronary artery disease (CAD), the exercise ECG testing would not add value to the perioperative clinical stratification. It could also delay the surgery and require more specific tests to differentiate the true results from the false-positive.7171 Wijeysundera DN, Beattie WS, Austin PC, Hux JE, Laupacis A. Non-invasive cardiac stress testing before elective major non-cardiac surgery: population based cohort study. BMJ. 2010;340:b5526.,7272 Grayburn PA, Hillis LD. Cardiac events in patients undergoing noncardiac surgery: shifting the paradigm from noninvasive risk stratification to therapy. Ann Intern Med. 2003;138(6):506-11.
Even in high-risk individuals, such as those undergoing preoperative vascular surgery, the predictive value, sensitivity, and specificity of the exercise ECG testing (10%, 74%, and 69%, respectively) are low, but with a high negative predictive value (98%).7373 Kertai MD, Boersma E, Bax JJ, Heijenbrok-Kal MH, Hunink MG, L'talien GJ, et al. A meta-analysis comparing the prognostic accuracy of six diagnostic tests for predicting perioperative cardiac risk in patients undergoing major vascular surgery. Heart. 2003;89(11):1327-34. On the other hand, in a cohort study, performance of provocative ischemic preoperative tests in high-risk patients, with three or more clinical risk factors, is associated with shorter hospital stays and lower mortality.7171 Wijeysundera DN, Beattie WS, Austin PC, Hux JE, Laupacis A. Non-invasive cardiac stress testing before elective major non-cardiac surgery: population based cohort study. BMJ. 2010;340:b5526. Thus, among asymptomatic individuals with a higher prevalence of the disease, the exercise ECG testing could be requested only if the result would influence the prognosis and, consequently, preoperative decisions, or to provide a more intensive clinical therapy or even a myocardial revascularization procedure.5757 Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130(24):e278-333. In this case, the onset of ischemic response at low load is associated with a higher number of perioperative cardiac events. On the other hand, patients with exercise tolerance up to 4-5 METS have a good perioperative prognosis.6565 Kristensen SD, Knuuti J, Saraste A, Anker S, Bøtker HE, Hert SD, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J. 2014;35(35):2383-431.,7474 Morris CK, Ueshima K, Kawaguchi T, Hideg A, Froelicher VF. The prognostic value of exercise capacity: a review of the literature. Am Heart J. 1991;122(5):1423-31.
II. Stress Myocardial Perfusion Scintigraphy
The exercise ECG testing is safe, useful, and effective to detect myocardial ischemia and has a good cost-risk-benefit ratio,7575 Vacanti LJ, Sposito AC, Séspedes L, Sarpi M, Ramires JA, Bortnick AE. In comparison to the myocardial perfusion scintigraphy, a treadmill stress test is a viable, efficient and cost effective option to predict cardiovascular events in elderly patients. Arq Bras Cardiol. 2007;88(5):531-6. but has limitations, such as patients with physical limitations, patients who present abnormal ST-segment changes or left bundle bock in the baseline ECG. The alternative for such patients is an imaging method with pharmacological stress (adenosine, dobutamine, or dipyridamole).
In this context, myocardial perfusion scintigraphy (MPS), when possible associated with exercise and, within the physical limitations, pharmacological stress, has a good accuracy and prognostic value.7070 Padma S, Sundaram PS. Current practice and recommendation for presurgical cardiac evaluation in patients undergoing noncardiac surgeries. World J Nucl Med. 2014;13(1):6-15. In a meta-analysis of 1,179 patients submitted to vascular surgery, MPS with dipyridamole demonstrated a greater number of perioperative cardiovascular events, proportional to the presence and extent of perfusion defects. Those with reversible ischemia in up to 20% of the left ventricular extension had the same events with those without ischemia. However, when the area affected was 20-29%, 30-49%, and above 50%, the probability of cardiac events was 1.6, 2.9, and 11 times higher, respectively.7676 Etchells E, Meade M, Tomlinson G, Cook D. Semiquantitative dipyridamole myocardial stress perfusion imaging for cardiac risk assessment before noncardiac vascular surgery: a meta-analysis. J Vasc Surg. 2002;36(3):534-40.
Another meta-analysis with the same method and similar profile of patients showed that patients without perfusion defect, with fixed defect, and with reversible defect presented mortality and nonfatal MI rates of 1%, 7%, and 9%, respectively. Patients with two or more perfusion defects have a high incidence of cardiac events.7777 Shaw LJ, Eagle KA, Gersh BJ, Miller DD. Meta-analysis of intravenous dipyridamole-thallium-201 imaging (1985 to 1994) and dobutamine echocardiography (1991 to 1994) for risk stratification before vascular surgery. J Am Coll Cardiol. 1996;27(4):787-98.
Gated-associated MPS, which allows assessment of both myocardial perfusion and cardiac function, has been recently shown to be a useful tool for risk stratification in vascular surgeries. In one study, abnormal final systolic volume (more than twice the standard deviation) was the only independent variable to predict cardiac events. Patients with normal perfusion but with changes in contractility had significantly more cardiac events than those with normal contractility and perfusion (16% x 2%; p < 0.0001).7878 Kayano D, Nakajima K, Ohtake H, Kinuya S. Gated myocardial perfusion SPECT for preoperative risk stratification in patients with noncardiac vascular disease. Ann Nucl Med. 2009;23(2):173-81.
In conclusion, in the perioperative evaluation, the indications for Gated-associated MPS are similar to those of the exercise ECG testing. It is the best option for patients with physical limitations. It is also the best alternative when the ECG is impossible to interpret due to baseline changes of the ST-segment and when the result of the exercise ECG testing is a possible false positive
III. Stress Echocardiography with Dobutamine
Stress echocardiography is an accurate and reliable tool to identify patients with CAD and has an important role in the prognosis of cardiac events7979 Mathias W Jr, Arruda A, Santos FC, Arruda AL, Mattos E, Osório A, et al. Safety of dobutamine-atropine stress echocardiography: A prospective experience of 4,033 consecutive studies. J Am Soc Echocardiogr. 1999;12(10):785-91.,8080 Chuah SC, Pellikka PA, Roger VL, McCully RB, Seward JB. Role of dobutamine stress echocardiography in predicting outcome in 860 patients with known or suspected coronary artery disease. Circulation. 1998;97(15):1474-80.
Dobutamine and exercise stress echocardiography have similar diagnostic accuracies, which are higher than that of dipyridamole stress.8181 Dagianti A, Penco M, Agati L, Sciomer S, Rosanio S, Fedele F. Stress echocardiography: comparison of exercise, dipyridamole and dobutamine in detecting and predicting the extent of coronary artery disease. J Am Coll Cardiol. 1995;26(1):18-25. If a dobutamine stress echocardiography does not demonstrate the presence of residual ischemia in a patient with a history of infarction, the prognosis is good and the probability of reinfarction, death, and acute pulmonary edema is low in the perioperative period of a noncardiac surgery.7373 Kertai MD, Boersma E, Bax JJ, Heijenbrok-Kal MH, Hunink MG, L'talien GJ, et al. A meta-analysis comparing the prognostic accuracy of six diagnostic tests for predicting perioperative cardiac risk in patients undergoing major vascular surgery. Heart. 2003;89(11):1327-34.
The use of dobutamine stress echocardiography in perioperative risk assessment is already well documented in the literature, with a positive predictive value ranging from 25-55% and a negative predictive value of 93-100% for cardiac events in patients undergoing noncardiac surgery,7373 Kertai MD, Boersma E, Bax JJ, Heijenbrok-Kal MH, Hunink MG, L'talien GJ, et al. A meta-analysis comparing the prognostic accuracy of six diagnostic tests for predicting perioperative cardiac risk in patients undergoing major vascular surgery. Heart. 2003;89(11):1327-34.,8282 Das MK, Pellikka PA, Mahoney DW, Roger VL, Oh JK, McCully RB, et al. Assessment of cardiac risk before nonvascular surgery: dobutamine stress echocardiography in 530 patients. J Am Coll Cardiol. 2000;35(6):1647-53. The results were generally used to determine preoperative clinical decisions, particularly the decision to perform coronary angiography or myocardial revascularization before or after the elective surgery.
A meta-analysis of 15 studies was performed to compare dipyridamole thallium-201 and dobutamine stress echocardiography in vascular risk stratification before surgery. It demonstrated that the prognostic value of the abnormalities is similar in both imaging methods for perioperative ischemic events.7777 Shaw LJ, Eagle KA, Gersh BJ, Miller DD. Meta-analysis of intravenous dipyridamole-thallium-201 imaging (1985 to 1994) and dobutamine echocardiography (1991 to 1994) for risk stratification before vascular surgery. J Am Coll Cardiol. 1996;27(4):787-98.
C) Invasive Coronary Angiography
Coronary angiography is a well-established invasive procedure, but it is rarely indicated for risk assessment in noncardiac surgeries. The available data are insufficient to recommend the use of coronary angiography in all patients (i.e., routine tests), including those undergoing high-risk surgeries. In general, the indications for coronary angiography in the preoperative period are similar to those for angiography in other situations. In addition, invasive coronary angiography assessment may cause unnecessary and unpredictable delay to an already scheduled surgical intervention, as well as add the risk of the procedure.8383 Illuminati G, Ricco JB, Greco C, Mangieri E, Calio F, Ceccanei G, et al. Systematic preoperative coronary angiography and stenting improves postoperative results of carotid endarterectomy in patients with asymptomatic coronary artery disease: a randomised controlled trial. Eur J Vasc Endovasc Surg. 2010;39(2):139-45. Notably, in services where non-invasive tests are unavailable for the detection of myocardial ischemia, coronary angiography should not be requested as an alternative to these tests.
D) Additional Tests
I. Coronary Computed Tomography Angiography
Coronary Angio-CT has been increasingly used to evaluate patients with suspected CAD. It presents high sensitivity for the detection of coronary stenosis, including multiarterial disease and lesion in the left coronary trunk.8484 Leschka S, Alkadhi H, Plass A, Desbiolles L, Grünenfelder J, Marincek B, et al. Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J. 2005;26(15):1482-7.
85 Mollet NR, Cademartiri F, Krestin GP, McFadden EP, Arampatzis CA, Serruys PW, et al. Improved diagnostic accuracy with 16-row multi-slice computed tomography coronary angiography. J Am Coll Cardiol. 2005;45(1):128-32.
86 Sheth T, Amlani S, Ellins ML, Mehta S, Velianou J, Cappelli G, et al. Computed tomographic coronary angiographic assessment of high-risk coronary anatomy in patients with suspected coronary artery disease and intermediate pretest probability. Am Heart J. 2008;155(5):918-23.-8787 Raff GL, Gallagher MJ, O'Neill WW, Goldstein JA. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005;46(3):552-7. However, it has not been extensively investigated in the perioperative period of noncardiac surgeries.
Ahn et al.8888 Ahn JH, Park JR, Min JH, Sohn JT, Hwang SJ, Park Y, et al. Risk stratification using computed tomography coronary angiography in patients undergoing intermediate-risk noncardiac surgery. J Am Coll Cardiol. 2013;61(6):661-8. analyzed retrospective data and concluded that angiotomography may be advantageous in reclassifying the risk of patients assessed by Lee’s revised score (RCRI), when submitted to intermediate risk procedures.4545 Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043-9.,8888 Ahn JH, Park JR, Min JH, Sohn JT, Hwang SJ, Park Y, et al. Risk stratification using computed tomography coronary angiography in patients undergoing intermediate-risk noncardiac surgery. J Am Coll Cardiol. 2013;61(6):661-8. On the other hand, a cohort showed a fivefold higher probability of overestimating the risk of angiotomography in patients who present an event.8989 Sheth T, Chan M, Butler C, Chow B, Tandon V, Nagele P, et al; Coronary Computed Tomographic Angiography and Vascular Events in Noncardiac Surgery Patients Cohort Evaluation Study Investigators. Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study. BMJ. 2015;350:h1907.
A few studies have shown an association between elevated coronary calcium score and cardiovascular events. Angiotomography could still be applied as an instrument for risk reclassification.8888 Ahn JH, Park JR, Min JH, Sohn JT, Hwang SJ, Park Y, et al. Risk stratification using computed tomography coronary angiography in patients undergoing intermediate-risk noncardiac surgery. J Am Coll Cardiol. 2013;61(6):661-8.,9090 Ghadri JR, Fiechter M, Veraguth K, Gebhard C, Pazhenkottil AP, Fuchs TA, et al. Coronary calcium score as an adjunct to nuclear myocardial perfusion imaging for risk stratification before noncardiac surgery. J Nucl Med. 2012;53(7):1081-6.
Nevertheless, the information obtained through such tests was still not correlated with new interventions (revascularization, pharmacoprotection, or monitoring) to reduce perioperative coronary events. Therefore, angiotomography or coronary calcium score is not recommended in the preoperative period.9191 Lange RA. Pre-operative risk assessment with cardiac computed tomography: all dressed up and nowhere to go. J Am Coll Cardiol. 2013;61(6):669-71.
II. Ankle-brachial Index
The ankle-brachial index (ABI) is one of the preferred methods for the diagnosis of peripheral occlusive arterial disease (PAOD). Values ≤ 0.9 show good accuracy for the diagnosis. ABI is associated with poor cardiovascular prognosis, significantly increasing the risk of amputation, CAD, and cerebrovascular disease.9292 Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1-75.,9393 Aboyans V, Criqui MH, Abraham P, Allison MA, Creager MA, Diehm C, et al; American Heart Association Council on Peripheral Vascular Disease; Council on Epidemiology and Prevention; Council on Clinical Cardiology; Council on Cardiovascular Nursing; Council on Cardiovascular Radiology and Intervention, and Council on Cardiovascular Surgery and Anesthesia. Measurement and interpretation of the ankle-brachial index: a scientific statement from the American Heart Association. Circulation. 2012;126(24):2890-909. Erratum in: Circulation. 2013;127(1):e264. It can be used as a risk reclassification tool in conjunction with the Framingham risk score, increasing the mortality risk due to all causes in all risk categories.9494 Fowkes FG, Murray GD, Butcher I, Heald CL, Lee RJ, Chambless LE, et al; Ankle Brachial Index Collaboration. Ankle brachial index combined with Framingham Risk Score to predict cardiovascular events and mortality: a meta-analysis. JAMA. 2008;300(2):197-208. Although ABI is a promising method because of its low cost, rapid standardization, good acceptance by patients, and low intra- and inter-observer variability, it is poorly investigated in the perioperative context.9595 Carmo GA, Calderaro D, Yu PC, Gualandro DM, Marques AC, Bittar CS, et al. Perioperative cardiovascular evaluation: heads or tails? Rev Assoc Med Bras (1992). 2012;58(4):505-12. Flu et al.9696 Flu WJ, van Kuijk JP, Voûte MT, Kuiper R, Verhagen HJ, Bax JJ, et al. Asymptomatic low ankle-brachial index in vascular surgery patients: a predictor of perioperative myocardial damage. Eur J Vasc Endovasc Surg. 2010;39(1):62-9. showed that patients with ABI ≤0.9 submitted to vascular surgery had an odds ratio (OR) of 2.4 for the occurrence of myocardial injury. Two other studies evaluated ABI in patients undergoing noncardiac and nonvascular surgeries and obtained ORs of 10.2 and 7.0 for the occurrence of major cardiovascular events, including isolated increase of troponin.9797 Fisher BW, Ramsay G, Majumdar SR, Hrazdil CT, Finegan BA, Padwal RS, et al. The ankle-to-arm blood pressure index predicts risk of cardiac complications after noncardiac surgery. Anesth Analg. 2008;107(1):149-54.,9898 Carmo GA, Calderaro D, Gualandro DM, Pastana AF, Yu PC, Marques AC, et al. The ankle-brachial index is associated with cardiovascular complications after noncardiac surgery. Angiology. 2016;67(2):187-92.
Association of this test with perioperative risk scores has not yet been studied, and the risk reclassification capacity is unknown. Therefore, routine use of ABI is not recommended as a risk estimation tool. For patients with previously known vasculopathies, focusing on the pharmacological prevention of cardiovascular events and monitoring, as discussed in other topics of this guideline, is recommended.
III. Holter
Holter is a continuous electrocardiographic monitoring tool that identifies the presence of atrial and ventricular arrhythmias and their complexity. It also identifies dynamic changes of the ST-segment that are indicative of myocardial ischemia. This method is not routinely used in the evaluation of preoperative ischemia, because other diagnostic methods are more sensitive and specific for this purpose. Its possible application during the perioperative period is monitoring ischemic events that occur in the intra- and postoperative periods, which can have a particularly high incidence in some specific groups of patients.
Electrocardiographic monitoring in the postoperative period using Holter was not very sensitive (50%), although very specific (92%), for the diagnosis of reinfarction in patients undergoing noncardiac surgeries and who had a previous history of myocardial infarction.9999 Heim C, Geel A, Münzer T, Angehrn W, Roelli H, Niederhauser H. [Perioperative myocardial infarction and cardiac complications after noncardiac surgery in patients with prior myocardial infarction. II: Perioperative long-term ECG--clinical relevance practicability]. Anaesthesist. 1996;45(3):220-4. Therefore, routine use of this test is not recommended. Requesting a Holter in the preoperative period follows the same indications of other contexts.
E) Biomarkers
I. Cardiac Troponins
The increased sensitivity of the available troponin kits provided a greater accuracy and rapidity in the diagnosis of MI in patients with chest pain in the emergency room.100100 Lipinski MJ, Baker NC, Escárcega RO, Torguson R, Chen F, Aldous SJ, et al. Comparison of conventional and high-sensitivity troponin in patients with chest pain: a collaborative meta-analysis. Am Heart J. 2015;169(1):6-16.e6. On the other hand, in the perioperative period of noncardiac operations, the available scientific evidence does not include all troponins (I and T) or all assays used, which have different detection limits and reference values. For this reason and due to the importance of this diagnostic tool, we decided to include a detailed explanation of the available methods before the recommendations in this guideline.
The detection limit represents the minimum value that is detected by the method. The reference value of normality is determined using the 99th percentile, which is obtained by performing the test in a normal population, and indicates that 99% of normal individuals have values below this cut-off.
Troponin assays can be classified as low sensitivity (conventional), medium sensitivity (contemporary or sensitive), or high sensitivity. This classification is based on the percentage of healthy individuals in whom troponin can be detected. Contemporary troponin assays (medium sensitivity) can detect values above the 99% percentile (altered values); however, troponin is only detected in a few normal individuals. High sensitivity assays can determine values of this marker (limit of detection) in 50-95% of normal individuals.101101 Jarolim P. High sensitivity cardiac troponin assays in the clinical laboratories. Clin Chem Lab Med. 2015;53(5):635-52.
Table 1 presents some troponin assays and their classification and respective reference values of normality.101101 Jarolim P. High sensitivity cardiac troponin assays in the clinical laboratories. Clin Chem Lab Med. 2015;53(5):635-52.,102102 Twerenbold R, Wildi K, Jaeger C, Gimenez MR, Reiter M, Reichlin T, et al. Optimal cutoff levels of more sensitive cardiac troponin assays for the early diagnosis of myocardial infarction in patients with renal dysfunction. Circulation. 2015;131(23):2041-50. To properly interpret and request troponin as a biomarker in the perioperative period, the physician must be familiar with the troponin assay used in their hospital. Notably, in the preoperative period, only the Roche high-sensitivity troponin T (hs-TnT) assay has been tested in the available studies and may have clinical applicability. In the postoperative period, most studied troponins are conventional and some are sensitive (as specified in item 7.F).
Some published papers demonstrate the efficacy of high sensitivity preoperative troponin as a marker of perioperative cardiovascular complications and general mortality in noncardiac surgeries. Nagele et al.103103 Nagele P, Brown F, Gage BF, Gibson DW, Miller JP, Jaffe AS, et al. High-sensitivity cardiac troponin T in prediction and diagnosis of myocardial infarction and long-term mortality after noncardiac surgery. Am Heart J. 2013;166(2):325-32.e1. studied 608 patients who underwent noncardiac surgery. They showed that 41% had increased values of hs-TnT above the 99th percentile (> 14 ng/L) in the preoperative period. The increase in preoperative hs-TnT was associated with a higher total mortality during a 3-year follow-up.103103 Nagele P, Brown F, Gage BF, Gibson DW, Miller JP, Jaffe AS, et al. High-sensitivity cardiac troponin T in prediction and diagnosis of myocardial infarction and long-term mortality after noncardiac surgery. Am Heart J. 2013;166(2):325-32.e1. These findings were confirmed in a study involving 455 patients undergoing vascular surgeries. In this study, patients with increased hs-TnT in the preoperative period presented a greater number of cardiovascular events in the postoperative period.104104 Gillmann HJ, Meinders A, Grosshennig A, Larmann J, Bünte C, Calmer S, et al. Perioperative levels and changes of high-sensitivity troponin T are associated with cardiovascular events in vascular surgery patients. Crit Care Med. 2014;42(6):1498-506. In a comparison to Lee’s RCRI algorithm in 979 patients aged more than 55 years with at least one cardiovascular risk factor submitted to noncardiac surgeries, preoperative hs-TnT presented an area under the ROC curve (0.78) similar to the RCRI (0.68; p = 0.07) in predicting combined cardiovascular events (mortality, MI, recovered cardiac arrest, and acute HF). In addition, in a multivariate analysis, increased hs-TnT in the preoperative period was an independent predictor of these combined events (HR 2.6; p = 0.008). As for general mortality, hs-TnT was superior to RCRI (area under the curve 0.81 × 0.66, p = 0.006).105105 Weber M, Luchner A, Manfred S, Mueller C, Liebetrau C, Schlitt A, et al. Incremental value of high-sensitive troponin T in addition to the revised cardiac index for peri-operative risk stratification in non-cardiac surgery. Eur Heart J. 2013;34(11):853-62. Erratum in: Eur Heart J. 2013;34(24):1853. The prevalence of preoperative hs-TnT increases varies between 21% and 41%, depending on the age and risk factors, such as diabetes, CAD, systemic arterial hypertension, and renal failure.103103 Nagele P, Brown F, Gage BF, Gibson DW, Miller JP, Jaffe AS, et al. High-sensitivity cardiac troponin T in prediction and diagnosis of myocardial infarction and long-term mortality after noncardiac surgery. Am Heart J. 2013;166(2):325-32.e1.
104 Gillmann HJ, Meinders A, Grosshennig A, Larmann J, Bünte C, Calmer S, et al. Perioperative levels and changes of high-sensitivity troponin T are associated with cardiovascular events in vascular surgery patients. Crit Care Med. 2014;42(6):1498-506.
105 Weber M, Luchner A, Manfred S, Mueller C, Liebetrau C, Schlitt A, et al. Incremental value of high-sensitive troponin T in addition to the revised cardiac index for peri-operative risk stratification in non-cardiac surgery. Eur Heart J. 2013;34(11):853-62. Erratum in: Eur Heart J. 2013;34(24):1853.
106 Kavsak PA, Walsh M, Srinathan S, Thorlacius L, Buse GL, Botto F, et al. High sensitivity troponin T concentrations in patients undergoing noncardiac surgery: a prospective cohort study. Clin Biochem. 2011;44(12):1021-4.-107107 Alcock RF, Kouzios D, Naoum C, Hillis GS, Brieger DB. Perioperative myocardial necrosis in patients at high cardiovascular risk undergoing elective non-cardiac surgery. Heart. 2012;98(10):792-8.
No study has evaluated the role of high-sensitivity troponin I (hs-TnI) in predicting cardiovascular events in the preoperative period. Contemporary/sensitive TnI was evaluated in 560 patients undergoing noncardiac surgeries, with only 5% presenting preoperative values above the 99th percentile. Its use did not improve the prediction of risk of perioperative cardiovascular events.108108 Biccard BM, Naidoo P, de Vasconcellos K. What is the best pre-operative risk stratification tool for major adverse cardiac events following elective vascular surgery? A prospective observational cohort study evaluating pre-operative myocardial ischaemia monitoring and biomarker analysis. Anaesthesia. 2012;67(4):389-95.
In conclusion, measurement of troponins with conventional or contemporary/sensitive assays is not useful in the preoperative period and should not be performed. On the other hand, the hs-TnT measurement in the preoperative period can be used as a tool for risk stratification associated with the use of the algorithms. In addition, these data help to establish a baseline value in patients with indication for postoperative monitoring, facilitating the interpretation of postoperative values of hs-TnT and the diagnosis of postoperative MI (items 7.F and 8.A).
II. Natriuretic Peptides
OThe risk scores usually used in the perioperative evaluation enable to estimate the risk of cardiovascular events in the perioperative period with moderate accuracy. Tests to evaluate ischemia, as well as biomarkers (troponins and natriuretic peptides), allow to refine the risk assessment before surgery.109109 Sankar A, Beattie WS, Wijeysundera DN. How can we identify the high-risk patient? Curr Opin Crit Care. 2015;21(4):328-35.
Natriuretic peptides are released into the bloodstream by the heart in response to multiple physiological stimuli, such as myocardial stress and ischemia. Several studies demonstrated that high preoperative levels of BNP are potent predictors of perioperative cardiovascular complications.110110 Karthikeyan G, Moncur RA, Levine O, Heels-Ansdell D, Chan MT, Alonso-Coello P, et al. Is a pre-operative brain natriuretic peptide or N-terminal pro-B-type natriuretic peptide measurement an independent predictor of adverse cardiovascular outcomes within 30 days of noncardiac surgery? A systematic review and meta-analysis of observational studies. J Am Coll Cardiol. 2009;54(17):1599-606.
The two studies by Biccard et al.111111 Biccard BM, Naidoo P. The role of brain natriuretic peptide in prognostication and reclassification of risk in patients undergoing vascular surgery. Anaesthesia. 2011;66(5):379-85. conducted investigations on patients submitted to arterial vascular surgery. In 2011, they reported that preoperative BNP was an independent predictor of increased postoperative troponin levels in a cohort of 267 patients undergoing vascular surgery. They also reported that the use of this biomarker improved the risk prediction of Lee’s RCRI in 38-70% in patients classified as intermediate risk.111111 Biccard BM, Naidoo P. The role of brain natriuretic peptide in prognostication and reclassification of risk in patients undergoing vascular surgery. Anaesthesia. 2011;66(5):379-85. In 2012, the authors evaluated 788 patients undergoing vascular surgery and showed that increased preoperative BNP levels was an independent predictor of cardiac events in a period of 30 days (OR = 5.0; p < 0.001).108108 Biccard BM, Naidoo P, de Vasconcellos K. What is the best pre-operative risk stratification tool for major adverse cardiac events following elective vascular surgery? A prospective observational cohort study evaluating pre-operative myocardial ischaemia monitoring and biomarker analysis. Anaesthesia. 2012;67(4):389-95.
A meta-analysis involving individual data from six different studies evaluated natriuretic peptides as predictors of events in patients undergoing vascular surgeries. The study confirmed that increased preoperative natriuretic peptide level is an independent predictor of events (cardiac death or nonfatal MI) in up to 30 days after surgery. It was also observed that it improves the predictive value of the RCRI.112112 Rodseth RN, Lurati Buse GA, Bolliger D, Burkhart CS, Cuthbertson BH, Gibson SC, et al. The predictive ability of pre-operative B-type natriuretic peptide in vascular patients for major adverse cardiac events: an individual patient data meta-analysis. J Am Coll Cardiol. 2011;58(5):522-9.
With regard to patients undergoing nonvascular surgeries, there are no studies that exclusively evaluate this population. The vast majority of the studies involve both vascular and nonvascular surgeries.
In a meta-analysis published in 2009, including 15 prospective observational studies and 4,856 patients submitted to vascular or nonvascular surgeries, the authors found that increased preoperative BNP or NT-proBNP levels was associated with a high (nearly 20-fold higher) risk of major cardiovascular events, cardiac mortality, and mortality due to all causes (almost 10-fold) in the perioperative period (< 43 days after surgery).113113 Ryding AD, Kumar S, Worthington AM, Burgess D. Prognostic value of brain natriuretic peptide in noncardiac surgery: a meta-analysis. Anesthesiology. 2009;111(2):311-9. However, whether prognostic information was improved in these studies, considering the existing risk indices, were not determined.114114 Beattie WS, Wijeysundera DN. Perioperative cardiac biomarkers: the utility and timing. Curr Opin Crit Care. 2013;19(4):334-41.
More recently, a prospective multicenter observational study analyzed 979 patients aged more than 55 years with at least one cardiovascular risk factor (hypertension, diabetes, dyslipidemia, smoking, family history) in the preoperative period of noncardiac surgery. The study aimed to assess increases in hs-Tn as a risk predictor compared to the Lee’s RCRI, with 93% of the patients with RCRI < 2. In this study, the authors also evaluated the role of natriuretic peptides as risk predictors in noncardiac surgery. They observed that both hs-Tn levels and NTproBNP levels were higher in individuals with cardiovascular events and seemed to provide additional information to the RCRI.105105 Weber M, Luchner A, Manfred S, Mueller C, Liebetrau C, Schlitt A, et al. Incremental value of high-sensitive troponin T in addition to the revised cardiac index for peri-operative risk stratification in non-cardiac surgery. Eur Heart J. 2013;34(11):853-62. Erratum in: Eur Heart J. 2013;34(24):1853.
Finally, a meta-analysis conducted in 2014 included 18 prospective observational studies. The authors assessed individual data from 2,179 patients undergoing noncardiac (vascular and nonvascular) surgery. They demonstrated that postoperative levels of BNP and NTproBNP provide additional risk prediction of death or nonfatal infarction in a period of 30 and 180 days to a risk prediction model that includes preoperative BNP. They also showed that high values of BNP/NTproBNP both in the postoperative (OR = 3.7; p < 0.001) and preoperative (OR = 1.9; p < 0.001) periods were independent predictors of death or nonfatal MI in a period of 30 days.115115 Rodseth RN, Biccard BM, Le Manach Y, Sessler DI, Lurati Buse GA, Thabane L, et al. The prognostic value of pre-operative and post-operative B-type natriuretic peptides in patients undergoing noncardiac surgery: B-type natriuretic peptide and N-terminal fragment of pro-B-type natriuretic peptide: a systematic review and individual patient data meta-analysis. J Am Coll Cardiol. 2014;63(2):170-80.
Therefore, we consider that BNP/NTproBNP measurement can provide additional prognostic information on the risk stratification of patients undergoing vascular and nonvascular arterial surgeries.
4. Diseases and Conditions with Specific Features in the Perioperative Period
A) Coronary Artery Disease
Objectively discriminating the surgical risk for each specific coronary artery disease (CAD) condition is critical for preventing and reducing morbidity of perioperative events. About four decades ago, perioperative risk analysis of CAD patients consisted of measuring the temporal relationship between a given cardiac ischemic event and the proposed surgery. At present, in addition to the mentioned interval,116116 Livhits M, Ko CY, Leonardi MJ, Zingmond DS, Gibbons MM, de Virgilio C. Risk of surgery following recent myocardial infarction. Ann Surg. 2011;253(5):857-64. we consider all the relevant factors for the prognosis of patients with CAD, independently of the perioperative context. These factors include presence of angina, HF, electrocardiographic signs, extent, and threshold of ischemia, and coronary anatomy, if relevant. The routine and indiscriminate performance of additional tests, such as functional tests and invasive coronary angiography, has no proven benefit, even in the population already diagnosed with CAD. A careful anamnesis associated with propaedeutics of the circulatory system and basic additional tests, such as rest ECG and chest X-ray, is often sufficient to determine the surgical risk of CAD patients. The request for functional tests must comply with the indications mentioned in item 3.B.IV.
B) Systemic Arterial Hypertension
Systemic arterial hypertension is a very common clinical condition, not only in the general population but also in patients who undergo surgical procedures. This condition, especially if uncontrolled, is one of the most common reasons for cancelling surgery.117117 Dix P, Howell S. Survey of cancellation rate of hypertensive patients undergoing anaesthesia and elective surgery. Br J Anaesth. 2001;86(6):789-93. This is because systemic hypertension is associated with increased perioperative mortality.118118 Browner WS, Li J, Mangano DT. In-hospital and long-term mortality in male veterans following noncardiac surgery. The Study of Perioperative Ischemia Research Group. JAMA. 1992;268(2):228-32. On the other hand, a study of carotid endarterectomy suggested that a patient with hypertension under control may not have an increased risk of perioperative morbidity and mortality, which suggests the importance of adequate control.119119 Kang JL, Chung TK, Lancaster RT, Lamuraglia GM, Conrad MF, Cambria RP. Outcomes after carotid endarterectomy: is there a high-risk population? A National Surgical Quality Improvement Program report. J Vasc Surg. 2009;49(2):331-8, 9.e1.
Recommendations for Preoperative BNP/NTproBNP Measurement to Predict Risk of Perioperative Cardiovascular Events
Major hemodynamic changes can occur during a surgical procedure, being more pronounced in patients with hypertension. These hemodynamic changes, which are associated with pain and anxiety, are aggravated by withdrawal of antihypertensive drugs on the day before the procedure.120120 Dodson GM, Bentley WE 4th, Awad A, Muntazar M, Goldberg ME. Isolated perioperative hypertension: clinical implications & contemporary treatment strategies. Curr Hypertens Rev. 2014;10(1):31-6. Increasing knowledge on the pathophysiology of hypertension and antihypertensive therapy, as well as the development of new anesthetics and muscle relaxants with minimal hemodynamic effects, in addition to postoperative pain control protocols, have contributed to minimize the occurrence of complications during the perioperative period of hypertensive patients.
One of the mechanisms involved is the sympathetic activation observed during anesthetic induction and in the postoperative period. Increases in sympathetic activity may cause significant increases in blood pressure, particularly in patients with uncontrolled arterial hypertension. Supporting the importance of sympathetic hyperactivity, evidence suggests that clonidine, when used in the perioperative period of hypertensive patients, significantly reduces blood pressure and heart rate variation, as well as reduces the need for anesthetic (isoflurane) and narcotic administration in these patients.121121 Ghignone M, Calvillo O, Quintin L. Anesthesia and hypertension: the effect of clonidine on perioperative hemodynamics and isoflurane requirements. Anesthesiology. 1987;67(1):3-10. Despite this, no evidence is available on the choice of antihypertensive agents in the perioperative period.120120 Dodson GM, Bentley WE 4th, Awad A, Muntazar M, Goldberg ME. Isolated perioperative hypertension: clinical implications & contemporary treatment strategies. Curr Hypertens Rev. 2014;10(1):31-6.
In general, stage 2 hypertension with SBP > 180 mmHg and DBP > 110 mmHg must be controlled before surgery. However, in mild or moderate hypertension, in which metabolic or cardiovascular changes do not occur, no evidence has been established on the benefits of postponing surgery.5757 Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130(24):e278-333.,120120 Dodson GM, Bentley WE 4th, Awad A, Muntazar M, Goldberg ME. Isolated perioperative hypertension: clinical implications & contemporary treatment strategies. Curr Hypertens Rev. 2014;10(1):31-6. The perioperative strategy should generally be to maintain blood pressure within 20% of the preoperative values (provided this value is not too uncontrolled), which implies flexibility in the control, not necessarily to normal levels. This may reduce the occurrence of hypertensive emergencies in the perioperative period.
Patients with some degree of autonomic dysfunction (such as that in hypertensive patients) are more susceptible to intraoperative hypotension than normotensive patients. This phenomenon appears to be more frequent in patients who use angiotensin-converting enzyme (ACE) inhibitors in the preoperative period. In most cases, this may be related to reduced intravascular volume; thus, avoiding perioperative hypovolemia is fundamental. However, abrupt withdrawal of these drugs should not be performed, because both uncontrolled blood pressure and decompensated HF may increase the risk of cardiovascular complications.
Patients with suspected secondary hypertension should be investigated prior to surgery, except in urgent/emergency cases. There is no conclusive evidence on the increase in perioperative risk in patients with secondary hypertension; however, patients with undiagnosed pheochromocytoma have a mortality rate of approximately 80% during surgery.122122 Sellevold OF, Raeder J, Stenseth R. Undiagnosed phaeochromocytoma in the perioperative period. Case reports. Acta Anaesthesiol Scand. 1985;29(5):474-9.
Cardiac and blood pressure monitoring in hypertensive patients is essential during the surgical procedure to detect variations of blood pressure and signs of ischemia as early as possible. In addition to being a risk factor for CAD, hypertension is associated with ventricular hypertrophy, systolic dysfunction, renal failure, and cerebrovascular events during the perioperative period. This aspect should be considered in the perioperative volume management of hypertensive patients with altered ventricular geometry and arterial elasticity, particularly the elderly.123123 Deague JA, Wilson CM, Grigg LE, Harrap SB. Physiological relationships between central vascular haemodynamics and left ventricular structure. Clin Sci (Lond). 2001;101(1):79-85. In the intraoperative period, the ideal antihypertensive agent should be easily titrated, rapid acting, have minimal side effects, and inexpensive. Several antihypertensive classes are available, including β-blockers (esmolol, labetalol), calcium channel blockers (nicardipine), and nitrates (sodium nitroprusside and nitroglycerin).
C) Heart Failure
HF affects about 1-2% of the general population in developed countries and more than 10% of the population aged more than 70 years,6565 Kristensen SD, Knuuti J, Saraste A, Anker S, Bøtker HE, Hert SD, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J. 2014;35(35):2383-431.,124124 Mosterd A, Hoes AW. Clinical epidemiology of heart failure. Heart. 2007;93(9):1137-46. CVDs are the main cause of death in Brazil, representing approximately 29% of the deaths in the country. Ischemic heart disease and HF are responsible for approximately 39% of these CVD deaths.125125 Gaui EN, Oliveira GM, Klein CH. Mortality by heart failure and ischemic heart disease in Brazil from 1996 to 2011. Arq Bras Cardiol. 2014;102(6):557-65.
HF is a well-known risk factor for perioperative cardiac events. Data from a large registry of noncardiac surgeries, which included more than 150,000 procedures, revealed that the presence of HF was associated with a 63% increase in the risk of perioperative mortality and a 51% increase in the risk of rehospitalization in a period of 30 days, when compared to the group with CAD without HF.126126 Hammill BG, Curtis LH, Bennett-Guerrero E, O'Connor CM, Jollis JG, Schulman KA, et al. Impact of heart failure on patients undergoing major noncardiac surgery. Anesthesiology. 2008;108(4):559-67.
Reduced ejection fraction is considered a strong predictor of events in patients undergoing vascular surgery. However, most of studies analyzed ejection fraction as a categorical variable (higher or lower than 40%). A recent study involving 174 patients with HF revealed that only severely reduced ejection fraction (< 30%) is an independent predictor of mortality. Moderate (30-40%) or mild (40-50%) ejection fraction reduction and preserved ejection fraction HF (> 50%) were not independent predictor of death in a period of 30 days.127127 Healy KO, Waksmonski CA, Altman RK, Stetson PD, Reyentovich A, Maurer MS. Perioperative outcome and long-term mortality for heart failure patients undergoing intermediate- and high-risk noncardiac surgery: impact of left ventricular ejection fraction. Congest Heart Fail. 2010;16(2):45-9. Despite the predictive value of ejection fraction, performing routine echocardiography for all patients undergoing noncardiac surgery is not indicated. A Canadian cohort study involving more than 250,000 patients (15% with preoperative echocardiography) revealed that preoperative echocardiography is not associated with improvement in survival or reduction of hospitalization time after major noncardiac surgery.6161 Wijeysundera DN, Beattie WS, Karkouti K, Neuman MD, Austin PC, Laupacis A. Association of echocardiography before major elective non-cardiac surgery with postoperative survival and length of hospital stay: population based cohort study. BMJ. 2011;342:d3695.
Increased level of natriuretic peptides in the preoperative period is related to worse prognosis in the perioperative period, because it is related to worsening of ventricular function and higher rate of cardiovascular events.128128 Biccard BM, Lurati Buse GA, Burkhart C, Cuthbertson BH, Filipovic M, Gibson SC, et al. The influence of clinical risk factors on pre-operative B-type natriuretic peptide risk stratification of vascular surgical patients. Anaesthesia. 2012;67(1):55-9.,129129 Rajagopalan S, Croal BL, Reeve J, Bachoo P, Brittenden J. N-terminal pro-B-type natriuretic peptide is an independent predictor of all-cause mortality and MACE after major vascular surgery in medium-term follow-up. Eur J Vasc Endovasc Surg. 2011;41(5):657-62. Measurement of these biomarkers may aid in the risk stratification of patients with HF. However, clinical evaluation and functional condition are even more relevant in the perioperative assessment of patients with HF.
Clinical management in the perioperative period requires special care regarding the blood volume of the patient. Both hypovolemia, which may intensify hypotension, and hypervolemia, which may lead to pulmonary and systemic congestion, should be avoided.
Patients with preserved fraction HF due to increased left ventricular stiffness are also susceptible to pulmonary edema, secondary to volume overload. Therefore, the use of diuretics and vasodilators may be necessary to avoid hypervolemia and afterload increases.
D) Valvular Heart Disease
Patients with valvular heart disease have a higher risk of presenting cardiovascular complications in the perioperative period of noncardiac surgeries.63 The risk varies depending on the valvular heart disease and its anatomic severity, as well as the type of noncardiac surgery to be performed.4545 Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043-9. The main cardiovascular complications in the perioperative period of noncardiac surgeries in patients with valvular heart disease are as follows: pulmonary congestion/acute pulmonary edema, cardiogenic shock, MI, tachyarrhythmias, embolic events, bleeding, and infective endocarditis.130130 Polanczyk CA, Goldman L, Marcantonio ER, Orav EJ, Lee TH. Supraventricular arrhythmia in patients having noncardiac surgery: clinical correlates and effect on length of stay. Ann Intern Med. 1998;129(4):279-85.,131131 Sprung J, Abdelmalak B, Gottlieb A, Mayhew C, Hammel J, Levy PJ, et al. Analysis of risk factors for myocardial infarction and cardiac mortality after major vascular surgery. Anesthesiology. 2000;93(1):129-40. In patients with valvular heart disease, particularly if anatomically relevant, clinical evaluation performed by a cardiologist should be considered in the preoperative period of noncardiac surgeries.
When valvular heart disease is suspected after detailed medical history and physical examination, transthoracic echocardiography should be performed with the following objectives: quantify the anatomic severity of valvular disease, assess ventricular function and remodeling of cardiac chambers, and estimate right chamber pressure. If doubt persists, other diagnostic methods may be performed, such as transesophageal echocardiography, magnetic resonance imaging, computed tomography, and cardiac catheterization.
Stenotic valvular heart disease have a higher perioperative risk than regurgitant valvular heart disease . Therefore, additional care should be given to patients with aortic (AoS) or mitral (MS) stenosis undergoing noncardiac surgery.
Symptomatic patients with anatomically relevant valvular heart disease already present high morbidity and mortality in the history of valvular heart disease and are indicated for interventional valve treatment.132132 Tarasoutchi F, Montera MW, Grinberg M, Piñeiro DJ, Sánchez CR, Bacelar AC, et al. [Brazilian Guidelines for Valve Disease - SBC 2011 / I Guideline Inter-American Valve Disease - 2011 SIAC]. Arq Bras Cardiol. 2011;97(5 Suppl 1):1-67.,133133 Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Guyton RA, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(22):e57-185. Erratum in: J Am Coll Cardiol. 2014;63(22):2489. This patient group presents a high risk of perioperative cardiac complications if submitted to noncardiac surgery. Therefore, they should initially treat valvular heart disease and subsequently undergo noncardiac surgery. However, if the noncardiac surgery is an emergency, it should be performed without prior correction of valvular heart disease, even if it is anatomically relevant.
The use of statins in the perioperative period of patients with valvular heart disease has not been evaluated in prospective studies. Therefore, statins should not be prescribed without another indication. Similarly, the use of nitroglycerin or even the use of intraoperative cardiac output monitoring has not been evaluated in these patients.
On the other hand, although there is no formal indication for the use of β-blockers in valvular heart disease patients in the perioperative period of noncardiac surgeries, these drugs can be used in patients with MS.
I. Aortic Stenosis
AoS is the most common valvular heart disease in elderly patients, affecting 2-4% of adults aged more than 65 years. The prevalence of AoS is expected to double in the next 20 years, with the progressive aging of the population.134134 Freeman RV, Otto CM. Spectrum of calcific aortic valve disease: pathogenesis, disease progression, and treatment strategies. Circulation. 2005;111(24):3316-26.,135135 Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368(9540):1005-11.
Several studies have shown that patients with moderate to severe AoS may have a high risk of cardiac complications during noncardiac surgery.1919 Goldman L, Caldera DL, Nussbaum SR, Southwick FS, Krogstad D, Murray B, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med. 1977;297(16):845-50.,136136 Skinner JF, Pearce ML. Surgical risk in the cardiac patient. J Chronic Dis. 1964;17:57-72.
137 Detsky AS, Abrams HB, McLaughlin JR, Drucker DJ, Sasson Z, Johnston N, et al. Predicting cardiac complications in patients undergoing non-cardiac surgery. J Gen Intern Med. 1986;1(4):211-9.
138 Rohde LE, Polanczyk CA, Goldman L, Cook EF, Lee RT, Lee TH. Usefulness of transthoracic echocardiography as a tool for risk stratification of patients undergoing major noncardiac surgery. Am J Cardiol. 2001;87(5):505-9.-139139 Zahid M, Sonel AF, Saba S, Good CB. Perioperative risk of noncardiac surgery associated with aortic stenosis. Am J Cardiol. 2005;96(3):436-8. However, in many of these studies, the definition and degree of AoS were ambiguous or based on few details. Since most studies included symptomatic or ventricular dysfunction patients, it is unclear whether aortic valve replacement surgery should precede the noncardiac procedure. The study by Calleja et al., which included 30 patients with anatomically relevant AoS and 60 controls (mild to moderate AoS), was the only one to exclude symptomatic patients. They showed similar MI or death rates during noncardiac surgery, mostly with low or intermediate risk.6464 Calleja AM, Dommaraju S, Gaddam R, Cha S, Khandheria BK, Chaliki HP. Cardiac risk in patients aged >75 years with asymptomatic, severe aortic stenosis undergoing noncardiac surgery. Am J Cardiol. 2010;105(8):1159-63.
For these reasons, Samarendra et al. recommended a new flowchart to assess the perioperative risk of noncardiac surgeries in patients with AoS. Patients with a high risk of cardiac complications are those with an average gradient > 45-50 mmHg and/or valvular area < 0.8 cm22 Dunkelgrun M, Boersma E, Schouten O, Koopman-van Gemert AW, van Poorten F, Bax JJ, et al; Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Bisoprolol and fluvastatin for the reduction of perioperative cardiac mortality and myocardial infarction in intermediate-risk patients undergoing noncardiovascular surgery: a randomized controlled trial (DECREASE-IV). Ann Surg. 2009;249(6):921-6.; left ventricular systolic dysfunction; symptomatic AoS; significant mitral regurgitation or other associated valvular diseases; increase in ≥ 18 mmHg in the average gradient during exercise; and associated CAD.6767 Samarendra P, Mangione MP. Aortic stenosis and perioperative risk with noncardiac surgery. J Am Coll Cardiol. 2015;65(3):295-302.
Furthermore, in a recent study with 218 patients, Mizuno et al.140140 Mizuno R, Yamagami ST, Higashi T, Nakada Y, Takeda Y, Okayama S, et al. Major non-cardiac surgery is a risk factor for rapid hemodynamic progression of non-rheumatic aortic stenosis. Circ J. 2015;79(4):867-72. demonstrated that patients with AoS who underwent a major noncardiac surgery present a faster progression of aortic valve disease compared to controls with AoS who did not undergo surgical intervention.
For the above reasons, it is recommended to first correct the anatomically relevant AoS, even if asymptomatic, in patients who will undergo intermediate- or high-risk noncardiac surgeries.
On the other hand, some patients with relevant AoS scheduled for noncardiac surgery have clinical indication for correction of valvular heart disease , but present a high risk for cardiac surgery or are ineligible for the conventional cardiac procedure. For these cases, a transcatheter aortic valve implantation (TAVI) is an option preceding noncardiac surgery.141141 Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al; PARTNER Trial Investigators. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-607.
142 Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, et al; PARTNER Trial Investigators. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-98.-143143 Torsher LC, Shub C, Rettke SR, Brown DL. Risk of patients with severe aortic stenosis undergoing noncardiac surgery. Am J Cardiol. 1998;81(4):448-52.
When patients with relevant AoS are submitted to urgent/emergency noncardiac surgery, preoperative clinical compensation is recommended with the use of diuretics, as well as postoperative period in an ICU, with hemodynamic and electrocardiographic monitoring and serial measurement of myocardial necrosis markers.
II. Mitral Stenosis
Patients with MS and formal indication for surgical or percutaneous correction of valvular heart disease should be submitted to the valve procedure before elective noncardiac surgery.144144 Reyes VP, Raju BS, Wynne J, Stephenson LW, Raju R, Fromm BS, et al. Percutaneous balloon valvuloplasty compared with open surgical commissurotomy for mitral stenosis. N Engl J Med. 1994;331(15):961-7. If noncardiac surgery is an emergency, it can be performed with invasive hemodynamics monitoring, optimization of blood volume, and prevention of tachycardia and hypotension. Increased heart rate, particularly if there is development of atrial fibrillation (AF), can lead to congestion and pulmonary edema. Therefore, β-blockers and/or diuretics may be used during the perioperative period.
III. Aortic Insufficiency and Mitral Insufficiency
Regurgitant valvular heart disease are associated with increased cardiac risk during noncardiac surgery, but are better tolerated than stenotic valve lesions.145145 Lai HC, Lee WL, Wang KY, Ting CT, Hung CJ, Liu TJ. Impact of chronic advanced aortic regurgitation on the perioperative outcome of noncardiac surgery. Acta Anaesthesiol Scand. 2010;54(5):580-8.,146146 Bajaj NS, Agarwal S, Rajamanickam A, Parashar A, Poddar KL, Griffin BP, et al. Impact of severe mitral regurgitation on postoperative outcomes after noncardiac surgery. Am J Med. 2013;126(6):529-35. However, aortic insufficiency (AoI) and mild or moderate mitral insufficiency (MI) do not increase the risk of cardiovascular complications during noncardiac surgery.
On the other hand, patients with symptomatic AoI or MI associated with ventricular dysfunction have a high risk of cardiovascular complications, and valvular heart disease should be performed before elective noncardiac surgery. Urgent or emergency noncardiac procedure should be performed after optimization of pharmacological treatment and optimal hemodynamic stability through the preferential use of vasodilators and diuretics, in addition to the postoperative period in an ICU.
IV. Valve Prosthesis
Patients with valve prostheses with normal function, without left ventricular dysfunction, may undergo noncardiac surgery without additional risk. For mechanical prosthesis, oral anticoagulation and bridge with heparin should be performed as described in section 7.D.132132 Tarasoutchi F, Montera MW, Grinberg M, Piñeiro DJ, Sánchez CR, Bacelar AC, et al. [Brazilian Guidelines for Valve Disease - SBC 2011 / I Guideline Inter-American Valve Disease - 2011 SIAC]. Arq Bras Cardiol. 2011;97(5 Suppl 1):1-67.
E) Cardiac Arrhythmias
Cardiac arrhythmias are common in patients with or without structural cardiopathy. The impact on morbidity and mortality in the perioperative period is mainly related to the underlying diseases, because arrhythmias that occur in patients without structural cardiopathy generally do not increase the risk of cardiac complications.4545 Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043-9. This distinction must be made by the cardiologist before the elective procedures.
There is limited data in the literature on the real impact of arrhythmias in this period, impairing the selection of a specific approach. Therefore, the recommendations are usually extrapolated from routine evaluation and outpatient or emergency decisions.147147 Scanavacca MI, de Brito FS, Maia I, Hachul D, Gizzi J, Lorga A, et al; Sociedade Brasileira de Cardiologia. [Guidelines for the evaluation and treatment of patients with cardiac arrhythmias]. Arq Bras Cardiol. 2002;79 Suppl 5:1-50.
The factors that can trigger supraventricular and ventricular arrhythmias and should be investigated include electrolyte imbalances (hypokalemia, hypomagnesemia, hypocalcemia), hypoxemia, proarrhythmic drugs (antidepressants, stimulants, positive inotropes, anesthetics), and metabolic disorders (hyperthyroidism or hypothyroidism). The priority is the correction of reversible factors in the preoperative or intraoperative period in cases of urgent or emergency surgery.
I. Paroxysmal Supraventricular Tachycardia
Supraventricular paroxysmal tachycardias are more prevalent in structurally normal youngsters and rarely present hemodynamic intolerance. They can occur by atrial tachycardia, ortho-ventricular atrioventricular tachycardia (in patients with accessory pathway), and nodal reentrant tachycardia. Asymptomatic patients who present ECGs with ventricular pre-excitation also have a low risk of perioperative complication. Attention should be only given to the occurrence of supraventricular tachycardia and pre-excited AF, and treatment follows the ACLS standard care.148148 Blomström-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, et al; European Society of Cardiology Committee, NASPE-Heart Rhythm Society. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias--executive summary. a report of the American college of cardiology/American heart association task force on practice guidelines and the European society of cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J Am Coll Cardiol. 2003;42(8):1493-531.
In this period, occurrence of pain, nausea, gagging, hypothermia, sympathetic blockade in anesthesia, laparoscopic insufflation, laryngoscopy, hyperventilation, anesthetics, and cholinergic drugs may precipitate arrhythmia due to autonomic imbalance. Such stimuli may trigger supraventricular tachycardias but do not increase surgical morbidity and mortality.
Controlling triggering factors mentioned above can minimize the occurrence of arrhythmias. In patients taking antiarrhythmic drugs, these drugs should be continued because preoperative interruption may promote arrhythmia.
II. Ventricular Extrasystoles and Tachycardias
Detection of extrasystolic arrhythmias in the preoperative period is common in high-risk patients. On the other hand, about 20% of the population can present these arrhythmias in the 24-hour Holter exam performed routinely.
Evaluation of extrasystolic arrhythmias includes collecting personal and family history. The occurrence of symptoms of hemodynamic intolerance (syncope or pre-syncope, precordial pain) may indicate complex or sustained arrhythmias. The presence of family history of sudden cardiac death may indicate the need for specific evaluation. In asymptomatic young patients with no personal or family history of heart disease, isolated monomorphic ventricular extrasystoles may generally be benign and with no implications in the perioperative period. In low-risk surgeries, evaluation of the ECG and cardiac area by chest X-ray may be sufficient and suspension of noncardiac surgery is unnecessary.149149 Pedersen CT, Kay GN, Kalman J, Borggrefe M, Della-Bella P, Dickfeld T, et al; EP-Europace,UK. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm. 2014;11(10):e166-96.
Suspicion of adjacent structural disease can be detected in ECG. ECG can identify ventricular overload, inactive area, conduction system diseases, and other rarer arrhythmic syndromes. Thoracic radiography is an important screening procedure for pulmonary diseases and detection of increased cardiothoracic index. Echocardiogram is a sensitive method that should be used for additional morphological analysis. An exercise ECG testing may be useful to demonstrate the presence of ischemia as a triggering factor for ventricular arrhythmias or to demonstrate benignity when dealing with idiopathic arrhythmias, which are suppressed by sinus tachycardia at the peak of the exercise.149149 Pedersen CT, Kay GN, Kalman J, Borggrefe M, Della-Bella P, Dickfeld T, et al; EP-Europace,UK. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm. 2014;11(10):e166-96.
Monomorphic ventricular tachycardia (VT) is often due to myocardial scarring. Polymorphic tachycardia may indicate ischemia, which reinforces the need for further investigation according to the specific guidelines.149149 Pedersen CT, Kay GN, Kalman J, Borggrefe M, Della-Bella P, Dickfeld T, et al; EP-Europace,UK. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm. 2014;11(10):e166-96.
The first preoperative treatment of ventricular arrhythmias is correction of reversible causes. There is no evidence that unsusceptible extrasystoles or VTs worsen the perioperative prognosis, nor is there is a proven benefit of suppression with antiarrhythmics.150150 Mahla E, Rotman B, Rehak P, Atlee JL, Gombotz H, Berger J, et al. Perioperative ventricular dysrhythmias in patients with structural heart disease undergoing noncardiac surgery. Anesth Analg. 1998;86(1):16-21.
III. Atrial Fibrillation and Flutter
AF is the most common sustained tachyarrhythmia and its prevalence increases with age. Patients who present a previous diagnosis of AF with adequate clinical control, considering symptoms and basal heart rate, do not need special considerations, except recommendations on anticoagulation (see item 7.D).151151 Chatterjee A, Hage FG. Guidelines in review: 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Nucl Cardiol. 2015;22(1):158-61.
In the preoperative period of elective surgeries, β-blockers or non-dihydropyridine calcium channel blockers (verapamil and diltiazem) are essential to control heart rate when patients have persistent AF/Flutter with high ventricular response. Administration of these drugs should preferably be performed slowly to avoid hypotension, which is known to be deleterious postoperatively. Calcium channel blockers may cause depression of myocardial function, particularly in patients with structural cardiopathy.152152 January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, et al; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267. Digoxin may be attenuated by surgical hyperadrenergic condition.6565 Kristensen SD, Knuuti J, Saraste A, Anker S, Bøtker HE, Hert SD, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J. 2014;35(35):2383-431. There are specific situations, such as pre-excited AF, in which ablation can be considered before surgery.153153 Bengali R, Wellens HJ, Jiang Y. Perioperative management of the Wolff-Parkinson-White syndrome. J Cardiothorac Vasc Anesth. 2014;28(5):1375-86. It should be noted that patients with AF with ventricular response above 120 bpm have a severe cardiovascular condition. In these cases, surgery should be postponed until the heart rate is controlled.
Control of rhythm, i.e., reversal of AF, could be an option before the procedure, depending on the symptoms and specific evaluation by cardiologists based on the current guidelines. However, interruption of anticoagulation for the procedure could only be performed after 4 weeks, and perioperative adrenergic stress facilitates recurrence.152152 January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, et al; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267.,154154 Martinelli Filho M, Moreira DA, Lorga AM, Sosa E, Atié J, Pimenta J, et al. [Guideline of atrial fibrillation]. Arq Bras Cardiol. 2003;81 Suppl 6:3-24.
Regardless of the control strategy selected (rhythm or heart rate), patients should be assessed for risk of cardioembolism and risk of bleeding using the CHA2DS2Vasc and HAS-BLED scores, respectively.152152 January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, et al; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267.
Prevention of Postoperative Atrial Fibrillation in Patients with Sinus Rhythm
The occurrence of postoperative AF (POAF) is associated with increased time in ICU, increased morbidity (including stroke, with incidence of 1.3-1.7%) and mortality, and consequently increased hospital costs. The AF preventive measures are adequate hydroelectrolytic control in the pre- and postoperative periods (normovolemia, magnesium and potassium monitoring, and replacement), in addition to maintenance of drugs previously used if hemodynamically tolerated.155155 Bessissow A, Khan J, Devereaux PJ, Alvarez-Garcia J, Alonso-Coello P. Postoperative atrial fibrillation in non-cardiac and cardiac surgery: an overview. J Thromb Haemost. 2015;13 Suppl 1:S304-12.
Some drugs have been investigated to reduce the incidence of POAF and its deleterious consequences. Preventive antiarrhythmic therapy with amiodarone or venous magnesium should be discussed individually. Retrospective studies showed that the use of amiodarone for anesthetic induction in patients submitted to esophagectomy may reduce the rate of POAF, but did not reduce the mortality and hospitalization rates. Moreover, its use in patients submitted to pulmonary resection is associated with reduced POAF and decreased time in ICU.156156 Tisdale JE, Wroblewski HA, Kesler KA. Prophylaxis of atrial fibrillation after noncardiac thoracic surgery. Semin Thorac Cardiovasc Surg. 2010;22(4):310-20.
157 Tisdale JE, Wroblewski HA, Wall DS, Rieger KM, Hammoud ZT, Young JV, et al. A randomized, controlled study of amiodarone for prevention of atrial fibrillation after transthoracic esophagectomy. J Thorac Cardiovasc Surg. 2010;140(1):45-51.-158158 Tisdale JE, Wroblewski HA, Wall DS, Rieger KM, Hammoud ZT, Young JV, et al. A randomized trial evaluating amiodarone for prevention of atrial fibrillation after pulmonary resection. Ann Thorac Surg. 2009;88(3):886-93. Riber et al.159159 Riber LP, Christensen TD, Jensen HK, Hoejsgaard A, Pilegaard HK. Amiodarone significantly decreases atrial fibrillation in patients undergoing surgery for lung cancer. Ann Thorac Surg. 2012;94(2):339-44. conducted a randomized, double-blind, placebo-controlled study. They demonstrated that administration of 300 mg of intravenous amiodarone in the early postoperative period, followed by 1200 mg of oral drug per day for 5 days, in hemodynamically stable patients reduced the POAF rate (9% versus 32% in the control group). On the other hand, Khalil et al.160160 Khalil MA, Al-Agaty AE, Ali WG, Abdel Azeem MS. A comparative study between amiodarone and magnesium sulfate as antiarrhythmic agents for prophylaxis against atrial fibrillation following lobectomy. J Anesth. 2013;27(1):56-61. compared the use of amiodarone in the immediate postoperative period for 48 hours (attack of 5 mg/kg, followed by 15 mg/kg) with venous magnesium sulfate (attack of 80 mg/kg, followed by 8 mg/kg/h) and with a control group from a retrospective analysis in patients submitted to pulmonary resection. Their results showed POAF rates of 10, 12.5, and 20.5%.
Other medications were studied to reduce the incidence of POAF. A meta-analysis with statins showed a potential role in the prevention of AF, although, of the 16 trials included, only 4 were conducted in noncardiac surgeries.161161 Chopra V, Wesorick DH, Sussman JB, Greene T, Rogers M, Froehlich JB, et al. Effect of perioperative statins on death, myocardial infarction, atrial fibrillation, and length of stay: a systematic review and meta-analysis. Arch Surg. 2012;147(2):181-9. Thus, its benefit to this population remains inconclusive.
Colchicine, an anti-inflammatory drug, is being studied for prevention in high-risk patients submitted to thoracic surgery.155155 Bessissow A, Khan J, Devereaux PJ, Alvarez-Garcia J, Alonso-Coello P. Postoperative atrial fibrillation in non-cardiac and cardiac surgery: an overview. J Thromb Haemost. 2015;13 Suppl 1:S304-12.
IV. Hereditary Arrhythmias
Genetically determined arrhythmias are a heterogeneous group of diseases and may occur due to defects in ion channels (channelopathies). Protein defects lead to atrial or ventricular arrhythmias, which may be manifested by tachycardic palpitations, arrhythmic characteristic syncope, or sudden death. The most prevalent channelopathies are Brugada Syndrome (1:5,000) and Long QT Syndrome (1:5,000). Other rarer diseases are catecholaminergic polymorphic ventricular tachycardia and short QT syndrome.
The estimated cardiovascular risk in this population is very variable and there is no complementary test that adequately stratifies it. The surgical and perioperative risk of these patients is poorly known, but some recommendations are well established by specialists.162162 Staikou C, Chondrogiannis K, Mani A. Perioperative management of hereditary arrhythmogenic syndromes. Br J Anaesth. 2012;108(5):730-44. In a retrospective analysis of 1,700 cases of early sudden death, 50 occurred postoperatively in young patients with no history of cardiopathy and a part may represent primary arrhythmias.163163 Tabib A, Loire R, Miras A, Thivolet-Bejui F, Timour Q, Bui-Xuan B, et al. Unsuspected cardiac lesions associated with sudden unexpected perioperative death. Eur J Anaesthesiol. 2000;17(4):230-5.
Symptomatic patients (syncope or palpitation) have a higher risk and sometimes need drugs (quinidine, β-blockers) or pacemaker defibrillators.164164 Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al; Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Europace. 2015;17(11):1601-87. Except for urgent surgeries, these patients should be evaluated by cardiologists before surgical release.
Channelopathies present specific anesthetic indications and immediate therapeutic interventions, which make perioperative management of these patients a challenge for the anesthesiologist.162162 Staikou C, Chondrogiannis K, Mani A. Perioperative management of hereditary arrhythmogenic syndromes. Br J Anaesth. 2012;108(5):730-44. In addition to cardiac monitoring and adequate electrolyte balance, all the drugs used in the perioperative period should be checked on specific sites, such as www.brugadadrugs.org, for Brugada Syndrome, and www.crediblemed.org, mainly for Long QT Syndrome, and also for all other channelopathies.164164 Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al; Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Europace. 2015;17(11):1601-87.
F) Conduction Disorders and Provisional Pacemaker Indications
Atrioventricular and intraventricular conduction disorders are uncommon in the perioperative period. When they occur, identification of the cause and drug therapy are usually sufficient for treatment. Even in individuals with bifascicular block or left bundle branch block and first-degree AV block, progression of the block or severe bradycardia in the perioperative period is rare.165165 Gauss A, Hübner C, Radermacher P, Georgieff M, Schütz W. Perioperative risk of bradyarrhythmias in patients with asymptomatic chronic bifascicular block or left bundle branch block: does an additional first-degree atrioventricular block make any difference? Anesthesiology. 1998;88(3):679-87. Erratum in: Anesthesiology 1998;88(6):1697.,166166 Gauss A, Hübner C, Meierhenrich R, Röhm HJ, Georgieff M, Schütz W. Perioperative transcutaneous pacemaker in patients with chronic bifascicular block or left bundle branch block and additional first-degree atrioventricular block. Acta Anaesthesiol Scand. 1999;43(7):731-6.
First-degree AV block, second-degree type Mobitz I, and uni- or bifascicular blocks, particularly in asymptomatic individuals, during the preoperative evaluation represent benign conditions that do not pose a greater risk. On the other hand, individuals presenting syncope, dyspnea or dizziness and type II second degree AV block, advanced AV block, and complete AV block constitute a higher risk group. A more rigorous evaluation is necessary in the preoperative period, and implantation of a pacemaker should be considered. If the surgery is urgent or an emergency, when it is not possible to comply with the ideal time between implantation of the definitive pacemaker and noncardiac surgery, the provisional pacemaker should be implanted in the preoperative period. Indications for implantation of the device under these conditions have already been considered in the Brazilian Guidelines for Implantable Electronic Cardiac Devices.167167 Martinelli Filho M, Zimerman LI, Lorga AM, Vasconcelos JT, Rassi A Jr. Guidelines for implantable electronic cardiac devices of the Brazilian Society of Cardiology. Arq Bras Cardiol. 2007;89(6):e210-e38.
Indications for a temporary transvenous pacemaker include syncope at rest or hemodynamic impairment due to bradyarrhythmia or occurrence of ventricular tachycardia in response to bradycardia. These recommendations may be based on clinical experience rather than on scientific studies.168168 Gammage MD. Temporary cardiac pacing. Heart. 2000;83(6):715-20. In rare occasions, these devices may be electively indicated to assist in procedures that may promote bradycardia or for general anesthesia in patients with second- or third-degree AV block, intermittent AV block, bifascicular block with first-degree AVB, and first-degree AV block with left bundle branch block.168168 Gammage MD. Temporary cardiac pacing. Heart. 2000;83(6):715-20.
G) Cardiac Implantable Electronic Devices
Technological progress of artificial cardiac pacing has greatly developed in the last years with the emergence of a wide variety of implantable devices able to provide new interactions with the cardiac rhythm. In addition, an increasing number of patients receive treatment with these new technologies each year. In the USA, approximately 500,000 individuals have these prostheses, and approximately 115,000 new devices are implanted annually. In Brazil, around 25,320 devices are implanted per year (average of the last 5 years) according to the Brazilian Pacemaker Registry.
A concern in the perioperative period of patients with these implantable devices is the possibility of electromagnetic interference when using an electric scalpel and other equipment during surgical procedures.169 Prostheses currently implanted may be functionally simple or have great complexity. We will address conventional pacing (uni or bicameral) (CP), cardiac resynchronizers (CR), implantable cardioverter defibrillator (ICD), and combined prostheses. These prostheses are generally referred to as cardiac implantable electronic devices (CIED).
I. Cardiac Implantable Electronic Devices Implanted Less than 60 Days
Most current pacemakers have active fixation electrodes, which enable them to be actively fixed to the endocardium and cardiac veins. Displacement of these electrodes is rare, but it is a possible complication at this stage. The area where the generator is implanted is in the process of surgical recovery. Inflammatory responses, bruises, edema, rejections, and even infections, which could still be subclinical at that stage, can occur with various intensities. The CIED and electrodes are susceptible to infections by organisms originating from other areas and even from surgical manipulations. If possible, it is recommended to wait until the end of the second post-implant month to perform elective noncardiac surgery to minimize the risk of complications.
II. Near End-of-life Cardiac Implantable Electronic Devices Battery Depletion
End-of-life CIEDs due to advanced battery wear should be replaced with newer and more modern units before elective noncardiac surgeries. These devices may present adverse behavior when subjected to extreme operating conditions (repeated interrogations and schedules), which may occur during surgery. In addition, these CIEDs can enter the end-of-life mode, changing the behavior and even disabling several important functions to save battery, which could be important in the perioperative period.
III. Safe Cardiac Stimulation
For elective noncardiac surgeries, patients should be evaluated by their CIED physicians, which will perform a complete verification of the stimulation system. The physician will determine the need for special programming, report the care that should be taken by the surgeon and anesthesiologist, and describe the possible behaviors of the CIED during surgery or even indicate the need for a stimulus during the procedure to make necessary perioperative schedules, which is usually required in patients at higher risk and with more complex CIED, such as defibrillators.170170 Crossley GH, Poole JE, Rozner MA, Asirvatham SJ, Cheng A, Chung MK, et al. The Heart Rhythm Society (HRS)/American Society of Anesthesiologists (ASA) Expert Consensus Statement on the perioperative management of patients with implantable defibrillators, pacemakers and arrhythmia monitors: facilities and patient management: executive summary this document was developed as a joint project with the American Society of Anesthesiologists (ASA), and in collaboration with the American Heart Association (AHA), and the Society of Thoracic Surgeons (STS). Heart Rhythm. 2011;8(7):e1-18.
The biggest concern usually involves those patients scheduled for major surgeries with the use of electric scalpels. In such cases, a safety evaluation must be performed always in a pacemaker evaluation unit and by a qualified physician. The physician should program the pacemaker in asynchronous mode only in cases where the patient depends on pacing and has no arrhythmia history (avoiding competition between pacemaker pace and self-pacing). The physician should also advise the surgical team to use bipolar or ultrasonic scalpel when possible, as these types of devices interfere less with the CIED.
The report should contain at least the recommendations described below for surgeries without the presence of the physician who programmed the pacemaker:
-
Continuous cardiac monitoring with an ECG and a pulse oximeter (heart rhythm monitoring is possible even when using an electric scalpel).
-
Use a bipolar electric scalpel. If it is not possible, use a unipolar scalpel and place the dispersive electrode (scalpel plate) away from the pacemaker (see below). Subsequently, prepare the skin in the region and eliminate oils by using an alcohol. If the dispersive electrode is reusable, apply a thin and homogeneous layer of electrolytic paste on its surface.
-
The dispersive electrode should be placed away from the CIED, preferably close to the surgical region to minimize the electric field. Thus, in an abdominal or pelvic surgery, the dispersive electrode should be placed close to the coccyx; in a right-hand surgery, the dispersive electrode should be placed on the right forearm; and in a head surgery, the dispersive electrode should be placed on the neck (nape). The CIED and its electrodes should be always away from the electric field generated by the electric scalpel.
-
Ground the scalpel by connecting it to an efficient ground wire.
-
Limit the use of the electric scalpel as much as possible to short and irregular intervals and evaluate the ECG or pulse. During this procedure, the ECG monitor is usually unreadable. Monitoring can be performed using plethysmography, which does not interfere with the electric scalpel.
-
If bradycardia or tachycardia occurs while using the electric scalpel (due to electromagnetic interference), place a magnet on the pacemaker every time the electric scalpel is used and then remove it immediately. The magnetic response of each pacemaker may be different and it may not exist in some cases (if it was programmed to be turned off). A good practice is to perform a few tests before surgery, but the patient must be continuously monitored to observe the magnetic response of the device. In addition, the magnetic behavior of each patient’s pacemaker should be reported by the specialist physician, as this depends on the program of the device.171171 Jacob S, Panaich SS, Maheshwari R, Haddad JW, Padanilam BJ, John SK. Clinical applications of magnets on cardiac rhythm management devices. Europace. 2011;13(9):1222-30. In defibrillators, placing a magnet on the device may turn off antitachycardia therapies, leaving the patient unprotected.
-
The patient should be advised to return to the pacemaker assessment clinic after the postoperative recovery period so that the normal set-up of the generator is re-established and the pacemaker functions are re-evaluated.
In patients with resynchronizers, the presence of a greater number of electrodes in the heart undeniably increases the possibility of complications due to external interferences on the stimulation system. Most stimulation electrodes used in the venous system of the left ventricle are used in unipolar mode. Therefore, they are more susceptible to external interferences, particularly those produced by the electric scalpel. However, there is a current trend of using bipolar and even multi-polar electrodes. Notably, many unipolar implants that have already been implanted will remain active for many years. The presence of more electrodes and unipolar electrodes forces physicians to take rigorous measures and pay more attention to signs of interference in the multisite stimulation system.
IV. Patients with Implantable Cardioverter Defibrillator
The complexity and diversity of the behavior of ICD, the risk of serious arrhythmias during surgery, and the potential electromagnetic interferences from an electric scalpel with the release of inappropriate shocks lead us to recommend, whenever possible, the presence of the specialist in the operating room with the ICD equipment. The equipment enables to program the ICD during the procedure in accordance to the clinical and metabolic needs of the patient. The antitachycardia function should be turned off, and the patient must be properly monitored. Turning off the function makes the patient unprotected. The physician should be prepared to treat a high-risk arrhythmia by using an external defibrillator and antiarrhythmic drugs. Following the experts’ advice, this type of patient must stay in the ICU during the postoperative period to allow monitoring during the critical stage. At the end of the surgery, the ICD parameters should be re-established and even adjusted to the patient’s clinical condition. The antitachycardia function of the ICD must be switched back on.
V. Emergency Electrical Cardioversion or Defibrillation
During the perioperative period, patients with CIED may present complications that require application of electrical cardioversion or defibrillation. Although generators can theoretically withstand shocks, it is advisable to avoid them whenever possible.172 When necessary, some care should be taken to preserve the pacemaker or defibrillator, the electrodes, and the heart-electrode interface, as described below:
-
If the patient has an implantable defibrillator, internal cardioversion is recommended because it uses a small amount of energy, biphasic pulse, and internal safety features of the device itself.
-
For external shocks, prefer biphasic cardioverters with adhesive pads. Place them in an anteroposterior position (embracing the left ventricle) in accordance to the polarity given by the manufacturer. The classic arrangement of the pads (between the base and tip of the heart - parallel to the electrodes) should be avoided because of the risk of myocardial injury due to contact with the electrode tip.
-
Adhere the pads in the chest as far as possible from the generator and the electrodes.
-
Use as little energy as possible. Modern biphasic external cardioverters should be preferred, whenever possible, because they use less energy;
-
Place a magnet over the pacemaker generator. Older pacemakers invariably switch off when a magnet is placed over them and become asynchronous. In current devices, the magnetic response is programmable and may exhibit different behavior. Therefore, placing a magnet over the generator does not guarantee protection during cardioversion.
-
Placing a magnet over the ICD is not recommended because the antitachycardic function can be switched off if it remains over the ICD for more than 30 seconds.
-
After the procedure, re-evaluate the sensitivity and command thresholds. Consider reassessing the device in 24 hours, and monitor the patient during this period.
VI. Lithotripsy
Shocks generated by lithotripsy have been related to transitory events of loss of sensitivity and command of the CIED, as well as reversion to the safe mode; however, these situations are extremely rare.173173 Küfer R, Thamasett S, Volkmer B, Hautmann RE, Gschwend JE. New-generation lithotripters for treatment of patients with implantable cardioverter defibrillator: experimental approach and review of literature. J Endourol. 2001;15(5):479-84. When lithotripsy is required in patients with pacemaker and/or defibrillator, direct the focus away from the area of the apparatus and electrodes.
Turn off atrial stimulation when ECG-triggered lithotripsy is used to avoid the device from synchronization with the atrium. Programming the atrial channel with less energy and in the bipolar mode may be another option, keeping the bicameral stimulation more physiological. A test can be performed before the application to observe the behavior and the interaction of the devices. Do not immerse the part of the body that contains the pacemaker or ICD when performing immersion lithotripsy.
It is also recommended to monitor the patient throughout the procedure and, whenever possible, the physician should stay in the room with the CIED programmer to adjust the program of the device as needed. Since lithotripsy is usually outpatient, the patient may perform a regular assessment of the CIED and the specialist can be requested to provide specific guidelines for the procedure. Placing a magnet over the CIED during lithotripsy should not be a rule because, as previously discussed, the device may have different behaviors and may deactivate therapies.
VII. Magnetic Resonance Imaging
Magnetic resonance imaging should not be performed on patients with older CIEDs. There is a risk of dysfunction of the prosthesis, electrodes, and even displacement due to the magnetic field generated.174174 Gimbel JR. Magnetic resonance imaging of implantable cardiac rhythm devices at 3.0 tesla. Pacing Clin Electrophysiol. 2008;31(7):795-801.
The recent advancement of the CIED industry has led to the production of devices that support the field of resonance, including tests of the chest area with a field strength of up to 1.5 Tesla. In this case, both the CIED and electrodes need to be compatible with this technology. Some patients with new devices but with old electrodes (connected or abandoned) could not undergo magnetic resonance imaging.175175 Nazarian S, Beinart R, Halperin HR. Magnetic resonance imaging and implantable devices. Circ Arrhythm Electrophysiol. 2013;6(2):419-28.
Despite the development in this field, even patients with CIED and compatible electrodes require the presence of a physician and a programmer during the test because a specific program is required, which should be deactivated at the end of the procedure. The most appropriate recommendations in these cases are previous evaluation of the patient in a pacemaker evaluation unit and guidance from the specialist on whether the patient should undergo testing. It is important to note that not only the images present artifacts due to the presence of the prosthesis but the patient may also experience local discomfort. This local discomfort is frequently described as burning and palpitations or dizziness related to inhibitions/deflagrations of the CIED.
VIII. Radiotherapy
Radiotherapy can be used if the radiation focus is not directed to the CIED. If the device is close to the radiation focus, the area should be covered with a lead screen. If the irradiated site is located exactly in the region of the implant or very close to it and many radiotherapy sessions are necessary, reimplantation of the CIED away from the irradiation site should be evaluated.
Direct radiotherapy on the CIED may cause transient or definitive dysfunction of the device and premature battery wear.176176 Zweng A, Schuster R, Hawlicek R, Weber HS. Life-threatening pacemaker dysfunction associated with therapeutic radiation: a case report. Angiology. 2009;60(4):509-12.,177177 McCollough CH, Zhang J, Primak AN, Clement WJ, Buysman JR. Effects of CT irradiation on implantable cardiac rhythm management devices. Radiology. 2007;243(3):766-74. Each radiotherapy application may put the CIED in safety mode, even if local protection measures are taken; thus, evaluation of the CIED is required after each radiotherapy session.178178 Makkar A, Prisciandaro J, Agarwal S, Lusk M, Horwood L, Moran J, et al. Effect of radiation therapy on permanent pacemaker and implantable cardioverter-defibrillator function. Heart Rhythm. 2012;9(12):1964-8.
Electrodes may also be affected with radiotherapy, especially at the site of contact with the endocardium, which may suffer fibrosis and loss of control. This phenomenon can occur from days to months after radiotherapy. Therefore, particular attention should be given to these patients, especially those that depend on stimulation. Under these conditions, a greater frequency of electronic evaluations (weekly/monthly) should be stipulated after the procedure. CIEDs that enable remote evaluation can facilitate this monitoring.179179 Hurkmans CW, Knegjens JL, Oei BS, Maas AJ, Uiterwaal GJ, van der Borden AJ, et al; Dutch Society of Radiotherapy and Oncology (NVRO). Management of radiation oncology patients with a pacemaker or ICD: a new comprehensive practical guideline in The Netherlands. Dutch Society of Radiotherapy and Oncology (NVRO). Radiat Oncol. 2012;7:198.
IX. Dental Procedures
Dental procedures in patients with CIEDs are increasingly common in dental practice. In addition to the risk of infection in prostheses, interaction between the equipment used in the dental treatment and the CIED, particularly the electric scalpel, is also possible.180180 Roedig JJ, Shah J, Elayi CS, Miller CS. Interference of cardiac pacemaker and implantable cardioverter-defibrillator activity during electronic dental device use. J Am Dent Assoc. 2010;141(5):521-6. In this situation, care taken should be the same as covered in item 4.G.III for general surgeries.
In patients with ICD, the device may interpret the thermocautery interference as an arrhythmia and release low- or high-energy therapy, placing both the patient and the dental surgeon at risk of receiving an inappropriate shock. Placing a magnet on the generator does not provide adequate protection and should be avoided.
In dental procedures, where the use of thermocautery is mandatory and the patient has ICD, it is essential to disable the antitachycardia therapy, keeping only the pacemaker function.
To prevent untreated risk of arrhythmias in this condition, the patient should be monitored and an external defibrillator should be available on site. The decision to perform the procedure in a hospital environment should always be considered due to the presence of necessary equipment for electrical emergencies, besides the support of the arrhythmologist. General, simple, and routine dentistry procedures carried out in dental practices do not require additional precaution, in addition to the usual therapeutic recommendations. Analgesia should be effective, and the use of anesthetics with vasoconstrictors at recommended doses (vasoconstrictor concentration and amount) should not be avoided. According to case studies and systematic reviews, these anesthetics do not interfere with cardiovascular parameters and do not predispose to coronary events, and when they induce arrhythmias, the risk is low.181181 Godzieba A, Smektala T, Jedrzejewski M, Sporniak-Tutak K. Clinical assessment of the safe use local anaesthesia with vasoconstrictor agents in cardiovascular compromised patients: a systematic review. Med Sci Monit. 2014;20:393-8.
X. Small Outpatient Surgical Procedures under Local Anesthesia
Minor surgeries may be performed with the usual care for patients with CIED provided that the thermocautery is not used. Analgesia should be efficient in dental treatments, and local anesthetics with vasoconstrictors at the usual doses can be administered to patients with cardiopathies because of the low risk of complications.
The cardiologist should, whenever possible, provide guidance in advance to the person responsible for the surgical procedure. If this is not possible, the use of the thermocautery should be avoided. Placing a magnet over the CIED does not guarantee protection in all cases and is not recommended in all situations.
XI. Recommendations
The operative period was divided into preoperative evaluation; preoperative preparation; and intraoperative and postoperative care. The recommendations were grouped to facilitate follow-up of patients with CIED. The suggested sequence should be followed for each patient.
XI.C. Postoperative182182 Hu R, Cowie DA. Pacemaker-driven tachycardia induced by electrocardiograph monitoring in the recovery room. Anaesth Intensive Care. 2006;34(2):266-8.,183183 Pinski SL, Trohman RG. Interference with cardiac pacing. Cardiol Clin. 2000;18(1):219-39.
5. Interventions and Procedures with Specific Features in the Perioperative Period
A) Transplants
I. Liver
Liver transplantation remains the procedure of choice for the treatment of terminal liver disease. However, changes occurring both intraoperatively and post-transplantation have increased the existing cardiovascular morbidity in these patients. This may be due to several risk factors that affect the population of the same age group (such as age, diabetes, male gender, smoking, previous history of CAD) or it may be related to liver disease and its etiology, such as alcohol-related cardiomyopathy, deposition of amyloid substances, and alterations due to cirrhosis-associated cardiomyopathy.184184 Raval Z, Harinstein ME, Skaro AI, Erdogan A, DeWolf AM, Shah SJ, et al. Cardiovascular risk assessment of the liver transplant candidate. J Am Coll Cardiol. 2011;58(3):223-31.
Studies have shown that cardiac events can occur in up to 70% of post-transplant patients, depending on the criteria.185185 Dec GW, Kondo N, Farrell ML, Dienstag J, Cosimi AB, Semigran MJ. Cardiovascular complications following liver transplantation. Clin Transplant. 1995;9(6):463-71. Among the most common are arrhythmias, pulmonary edema, and systolic ventricular dysfunction, but sudden death and myocardial infarction may also occur.186186 Mandell MS, Lindenfeld J, Tsou MY, Zimmerman M. Cardiac evaluation of liver transplant candidates. World J Gastroenterol. 2008;14(22):3445-51.
Therefore, careful investigation of heart disease in candidates for liver transplantation is required.187187 Zaky A, Bendjelid K. Appraising cardiac dysfunction in liver transplantation: an ongoing challenge. Liver Int. 2015;35(1):12-29. However, due to liver disease, cardiological investigation in these patients is difficult because the hemodynamic changes and limitations resulting from the disease do not allow the same sensitivity and specificity in cardiology tests, when compared to other populations.188188 Rugina M, Predescu L, Salagean M, Gheorghe L, Gheorghe C, Tulbure D, et al. Pre-liver transplantation, cardiac assessment. Chirurgia (Bucur). 2012;107(3):283-90.
Approximately 50% of patients with cirrhosis show an increase in the QT interval.189189 Bernardi M, Maggioli C, Dibra V, Zaccherini G. QT interval prolongation in liver cirrhosis: innocent bystander or serious threat? Expert Rev Gastroenterol Hepatol. 2012;6(1):57-66. β-adrenergic receptors respond only slightly to sympathetic stimuli, leading to dubious responses in studies of dobutamine echocardiography.190190 Umphrey LG, Hurst RT, Eleid MF, Lee KS, Reuss CS, Hentz JG, et al. Preoperative dobutamine stress echocardiographic findings and subsequent short-term adverse cardiac events after orthotopic liver transplantation. Liver Transpl. 2008;14(6):886-92. The hyperdynamic state and its consequent chronic vasodilatation impair the vasodilator-induced response, such as dipyridamole in myocardial scintigraphy. Terminal liver disease is often accompanied by renal dysfunction, which impairs the use of contrast agents, such as in coronary angiography or coronary Angio-CT.
However, there are tests and approaches that have become routinely used in the preoperative evaluation of liver transplant candidates due to their cost-effectiveness. Moreover, some cardiovascular comorbidity characteristics of cirrhotic patients should be ruled out because they lead to high morbidity and mortality in the perioperative period. The most important characteristics to note are as follows:
I. A. Cardiomyopathy Associated with Cirrhosis
It is characterized by the triad: systolic dysfunction, mainly due to a deficit in the contractile response induced by stress, and ejection fraction at rest below 55%; diastolic dysfunction, typically with E/A < 1 and prolonged isovolumetric relaxation time; and electrophysiological changes, particularly increased QT interval, chronotropic deficit and bradycardia, changes in ventricular repolarization, increased left atrium and myocardial mass, and increased levels of BNP, NTpro-BNP, and TnI.187187 Zaky A, Bendjelid K. Appraising cardiac dysfunction in liver transplantation: an ongoing challenge. Liver Int. 2015;35(1):12-29.,188188 Rugina M, Predescu L, Salagean M, Gheorghe L, Gheorghe C, Tulbure D, et al. Pre-liver transplantation, cardiac assessment. Chirurgia (Bucur). 2012;107(3):283-90.,191191 Møller S, Henriksen JH. Cirrhotic cardiomyopathy. J Hepatol. 2010;53(1):179-90.
Although these findings increase morbidity and mortality in liver transplant candidates, no benefit has been demonstrated in the specific treatment of these alterations.
I. B. Cardiomyopathy Associated with Alcohol
Cardiomyopathy associated with alcohol accounts 21-32% of patients with dilated cardiomyopathy in some medical centers. Excessive ingestion of alcohol leads to myocyte apoptosis, reduced calcium sensitivity, depressed myocyte contractile function, and myocardial fibrosis.192192 Capasso JM, Li P, Guideri G, Malhotra A, Cortese R, Anversa P. Myocardial mechanical, biochemical, and structural alterations induced by chronic ethanol ingestion in rats. Circ Res. 1992;71(2):346-56. Considering that alcoholic cirrhosis is among the major causes of liver disease, concomitant occurrence of cirrhosis and dilated cardiomyopathy is relatively common.
Interruption of alcohol intake in the early phase of this cardiomyopathy may lead to partial or total recovery of ventricular function, which reduces cardiovascular morbidity in these patients.193193 La Vecchia LL, Bedogni F, Bozzola L, Bevilacqua P, Ometto R, Vincenzi M. Prediction of recovery after abstinence in alcoholic cardiomyopathy: role of hemodynamic and morphometric parameters. Clin Cardiol. 1996;19(1):45-50.
I. C. Port-Pulmonary Hypertension
The hyperdynamic state of the patient with portal hypertension may cause vasoconstriction and remodeling of the pulmonary vessels, leading to pulmonary hypertension (PH). These changes affect 5-10% of the transplant candidates and, depending on the pulmonary artery average pressure, may be mild (> 25 and < 35 mmHg), moderate (> 35 and < 45 mmHg), and severe (> 45 mmHg).194194 Swanson KL, Krowka MJ. Screen for portopulmonary hypertension, especially in liver transplant candidates. Cleve Clin J Med. 2008;75(2):121-2, 125-30.
Although there are studies on endothelin receptor antagonists and phosphodiesterase inhibitors, there are no definitive guidelines for moderate to severe PH. Perioperative mortality in the latter is close to 100%, therefore representing a contraindication for isolated liver transplantation, and combined lung-liver transplantation may be indicated in specific medical centers.195195 Porres-Aguilar M, Zuckerman MJ, Figueroa-Casas JB, Krowka MJ. Portopulmonary hypertension: state of the art. Ann Hepatol. 2008;7(4):321-30.
I. D. Hepatopulmonary Syndrome
Although sometimes confused with PH, hepatopulmonary syndrome presents several different characteristics. It is defined as hypoxia in the presence of hepatic disease that worsens with upright posture, with evidence of intrapulmonary vasodilation. Hypoxia is due to the accumulation of pulmonary vasodilators, particularly nitric oxide, leading to intrapulmonary arteriovenous shunt.196196 Grace JA, Angus PW. Hepatopulmonary syndrome: update on recent advances in pathophysiology, investigation, and treatment. J Gastroenterol Hepatol. 2013;28(2):213-9.
Unlike for PH, the selected treatment for hepatopulmonary syndrome is liver transplantation, although non-definitive data correlates the degree of hypoxia with perioperative mortality.197197 Gupta S, Castel H, Rao RV, Picard M, Lilly L, Faughnan ME, et al. Improved survival after liver transplantation in patients with hepatopulmonary syndrome. Am J Transplant. 2010;10(2):354-63.
I. E. Coronary Artery Disease
As previously mentioned, the risk factors for CAD are either similar or more in cirrhotic patients than in the general population, especially diabetes. Although CAD increases the morbidity and mortality of these patients, the degree of impairment of stenosis does not seem to correlate with worse prognosis.
Computerized coronary tomography with quantification of the calcium score has been recently shown to be useful, and a calcium score above 400 has a high predictive value for early cardiovascular events in these patients.198198 Kong YG, Kang JW, Kim YK, Seo H, Lim TH, Hwang S, et al. Preoperative coronary calcium score is predictive of early postoperative cardiovascular complications in liver transplant recipients. Br J Anaesth. 2015;114(3):437-43. However, the use of this test cannot be routinely indicated for this population.
The choice of treatment for these patients should consider that lack of intervention may lead to an excessive risk during and after surgery. However, the best treatment is not established and should be customized for each patient.
An important controversy concerns the use of drug eluting stents that requires antiplatelet agents for a longer time in patients with thrombocytopenia, and the risk of bleeding is always present.199199 Ehtisham J, Altieri M, Salamé E, Saloux E, Ollivier I, Hamon M. Coronary artery disease in orthotopic liver transplantation: pretransplant assessment and management. Liver Transpl. 2010;16(5):550-7.
Coronary artery bypass grafting (CABG) should be, whenever possible, postponed until after transplantation because of the high probability of hemorrhagic events or worsening of the hepatic condition with the surgery.200200 Bizouarn P, Ausseur A, Desseigne P, Le Teurnier Y, Nougarede B, Train M, et al. Early and late outcome after elective cardiac surgery in patients with cirrhosis. Ann Thorac Surg. 1999;67(5):1334-8. Myocardial revascularization before the transplant should be only performed in patients for whom the risk of death due to CAD exceeds the risk of death due to liver disease.
Finally, it is worth mentioning that the cardiologist is part of the multidisciplinary team that accompanies these patients. For this reason, a possible contraindication of the procedure should always be discussed and customized with the multiprofessional team and the patient.
II. Kidney
Patients with terminal renal disease are one of the highest cardiovascular risk groups, with mortality rates from cardiovascular disease 5 to 100 times higher than those found in the general population.201201 K/DOQI Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. 2005;45(4 Suppl 3):S1-S153. Cardiovascular disease is the leading cause of death after renal transplantation, particularly due to CAD.202202 United States Renal Data System. 2015 USRDS annual data report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD. 2015. In the first 30 days after successful kidney transplantation, approximately half of the deaths are due to MI.203203 Ojo AO, Hanson JA, Wolfe RA, Leichtman AB, Agodoa LY, Port FK. Long-term survival in renal transplant recipients with graft function. Kidney Int. 2000;57(1):307-13. Similarly, in the late follow-up, chronic ischemic heart disease accounts for more than a third of deaths in patients with a functioning graft.204204 Wheeler DC, Steiger J. Evolution and etiology of cardiovascular diseases in renal transplant recipients. Transplantation. 2000;70(11 Suppl):SS41-5.
Therefore, the preoperative evaluation of renal transplant candidates aims not only to reduce cardiovascular risk in the short term, related to the surgical procedure, but also to reduce cardiovascular events in late follow-up.205205 Lentine KL, Costa SP, Weir MR, Robb JF, Fleisher LA, Kasiske BL, et al; American Heart Association Council on the Kidney in Cardiovascular Disease and Council on Peripheral Vascular Disease; American Heart Association; American College of Cardiology Foundation. Cardiac disease evaluation and management among kidney and liver transplantation candidates: a scientific statement from the American Heart Association and the American College of Cardiology Foundation: endorsed by the American Society of Transplant Surgeons, American Society of Transplantation, and National Kidney Foundation. Circulation. 2012;126(5):617-63. During the evaluation of renal transplant candidates, the identification and presence of CAD are of fundamental importance because they allow the medical team to establish more precisely the risk-benefit of transplantation, the possible need for coronary intervention in the preoperative period, the use of cardioprotective measures in the perioperative period, and the control of risk factors in the postoperative period.
This section aims to provide the cardiologist with the most appropriate methods to determine cardiovascular risk in a very special population of patients, almost always excluded from the risk stratification studies. The main aim is to identify those most likely to be diagnosed with CAD among kidney transplant candidates. Thus, the recommendations included in this section should be applied only to asymptomatic patients or patients with atypical symptoms. For those individuals with clinical evidence and/or diagnostic investigations suggestive of coronary disease, further investigation and treatment should follow the proposed rules for the general population.
Identification of relevant CAD is challenging in renal transplant candidates. Patients with terminal renal disease often have atypical symptoms, or are even asymptomatic, in the presence of advanced CAD.206206 Hakeem A, Bhatti S, Chang SM. Screening and risk stratification of coronary artery disease in end-stage renal disease. JACC Cardiovasc Imaging. 2014;7(7):715-28. The use of non-invasive methods, such as exercise ECG testing, MPS, and stress echocardiography, all routinely performed in the general population has lower sensitivity and specificity than in individuals with normal renal function, providing numerous false negative results.207207 Lindley EM, Hall AK, Hess J, Abraham J, Smith B, Hopkins PN, et al. Cardiovascular Risk Assessment and Management in Prerenal Transplantation Candidates. Am J Cardiol. 2016;117(1):146-50.
208 Kahn MR, Fallahi A, Kim MC, Esquitin R, Robbins MJ. Coronary artery disease in a large renal transplant population: implications for management. Am J Transplant. 2011;11(12):2665-74.-209209 De Lima JJ, Sabbaga E, Vieira ML, de Paula FJ, Ianhez LE, Krieger EM, et al. Coronary angiography is the best predictor of events in renal transplant candidates compared with noninvasive testing. Hypertension. 2003;42(3):263-8. On the other hand, coronary angiography should not be performed indiscriminately because it is an invasive method, with risk of complications and high cost. In addition, the prevalence of significant CAD in patients routinely assessed invasively is less than 50%.207207 Lindley EM, Hall AK, Hess J, Abraham J, Smith B, Hopkins PN, et al. Cardiovascular Risk Assessment and Management in Prerenal Transplantation Candidates. Am J Cardiol. 2016;117(1):146-50.,209209 De Lima JJ, Sabbaga E, Vieira ML, de Paula FJ, Ianhez LE, Krieger EM, et al. Coronary angiography is the best predictor of events in renal transplant candidates compared with noninvasive testing. Hypertension. 2003;42(3):263-8.,210210 Charytan D, Kuntz RE, Mauri L, DeFilippi C. Distribution of coronary artery disease and relation to mortality in asymptomatic hemodialysis patients. Am J Kidney Dis. 2007;49(3):409-16.
Observational studies show that patients with terminal chronic kidney disease and CAD undergoing PCI or CABG have a risk of cardiovascular events similar to those with terminal chronic kidney disease without significant CAD. Those with obstructive coronary disease who did not undergo myocardial revascularization had significantly higher rates of cardiovascular events.207207 Lindley EM, Hall AK, Hess J, Abraham J, Smith B, Hopkins PN, et al. Cardiovascular Risk Assessment and Management in Prerenal Transplantation Candidates. Am J Cardiol. 2016;117(1):146-50.,208208 Kahn MR, Fallahi A, Kim MC, Esquitin R, Robbins MJ. Coronary artery disease in a large renal transplant population: implications for management. Am J Transplant. 2011;11(12):2665-74.
Therefore, it is necessary to define a strategy that allows identification of patients more likely to have relevant CAD and who should therefore be referred for angiographic study. With this, we would reduce the number of patients inadequately classified as being of low cardiovascular risk due to failure in the preoperative risk stratification and consequently their exposure to a higher risk of cardiovascular events.
Risk Stratification of the Presence of Coronary Artery Disease
The clinical parameters most strongly associated with ischemic heart disease after kidney transplantation are age > 50 years, DM, and previous evidence of cardiovascular disease (clinical history and/or tests).211211 Pascual J, Abramowicz D, Cochat P, Claas F, Dudley C, Harden P, et al. European renal best practice guideline on the management and evaluation of the kidney donor and recipient. Nefrologia. 2014;34(3):293-301. The prevalence of relevant CAD (stenosis ≥ 70%) increases with the number of risk factors. These three risk factors have been the basis for the formulation of algorithms to investigate coronary disease in patients with chronic kidney disease. Other factors considered as predictors of cardiovascular events in this population are systemic arterial hypertension, left ventricular hypertrophy, smoking, dyslipidemia, and dialysis for more than one year.212212 Abbud-Filho M, Adams PL, Alberú J, Cardella C, Chapman J, Cochat P, et al. A report of the Lisbon Conference on the care of the kidney transplant recipient. Transplantation. 2007;83(8 Suppl):S1-22.
Based on the results of existing studies, we proposed a risk stratification model for asymptomatic chronic renal patients from a cardiovascular perspective, evaluated for renal transplantation, according to the presence or absence of the three previously mentioned risk factors.213213 Gowdak LH, Arantes RL, de Paula FJ, Cesar LA, Ianhez LE, Krieger EM, et al. A new proposal for cardiovascular risk stratification in renal transplant candidates: time to review the American Society of Transplantation Guidelines? J Am Coll Cardiol. 2008;51(10 Suppl. A):A363.
214 Gowdak LH, de Paula FJ, César LA, Martinez Filho EE, Ianhez LE, Krieger EM, et al. Screening for significant coronary artery disease in high-risk renal transplant candidates. Coron Artery Dis. 2007;18(7):553-8.
215 V. Clinical algorithms on cardiovascular risk factors in renal patients. Nephrol Dial Transplant. 2000;15 Suppl 5:123-54.-216216 Gowdak LH, de Paula FJ, César LA, Bortolotto LA, de Lima JJ. A new risk score model to predict the presence of significant coronary artery disease in renal transplant candidates. Transplant Res. 2013;2(1):18. If there is any latency between initial stratification and transplantation, we suggest a period of three years for a new stratification if the patient is stable and without new cardiovascular events or symptoms.
B) Bariatric Surgery
With the obesity epidemic and the increasing prevalence of type 2 diabetes, bariatric or metabolic surgical interventions have become a very interesting option. The results of long-term (though not randomized) studies seem to indicate the benefit of these interventions in reducing mortality. However, there are still many uncertainties, in particular, which patient profile may benefit and what type of surgical intervention to perform for each case. Once the bariatric surgical procedure is considered, it is important to pay attention to the contraindications for this type of surgery: type 1 diabetes, drug or alcohol abuse, uncontrolled psychiatric disease, lack of understanding about risks, alternatives, and complications of the intervention, and lack of commitment to the need for nutritional supplementation and clinical follow-up.
In Brazil, four different types of bariatric surgery (besides the intragastric balloon, which is not considered surgical) are approved: gastric bypass, adjustable gastric band, duodenal switch, and vertical gastrectomy. However, there are no conclusive data to support the selection of procedure based, for example, on the higher or lower incidence of complications. On the other hand, several variables, such as age, gender, BMI, presence of comorbidities, and the patient’s desire, should be considered. Thus, for example, the presence of important hiatal hernia contraindicates vertical gastrectomy, the patient with a very high BMI cannot receive an adjustable gastric banding, vertical gastrectomy is less efficient in a patient who continually eats, or gastric bypass will probably work better if the patient is a long-term diabetic.
Regarding the perioperative evaluation for patients with indication for bariatric surgery, in addition to the general recommendations described for obese patients in another item of this guideline (item 9 D), there are some specific considerations that consider studies that observed the occurrence of complications. DeMaria et al. evaluated 2,075 patients undergoing bariatric surgery (all undergoing gastric bypass) using the obesity surgery mortality risk stratification score and found increased risk of death in the presence of certain factors: pulmonary thromboembolism (PTE) or risk for PTE, BMI > 50 kg/m2, male gender, systemic arterial hypertension, and > 45 years of age. The risk for PTE was defined as previous PTE, presence of a vena cava filter, right HF and/or PH, chronic venous stasis, and obstructive sleep apnea syndrome. Basing on these data, the authors developed a risk score based on the number of risk factors: A (0-1), B (2-3), and C (4-5), which correspond to an estimated perioperative mortality risk of 0.31, 1.90, and 7.56%, respectively.217217 DeMaria EJ, Murr M, Byrne TK, Blackstone R, Grant JP, Budak A, et al. Validation of the obesity surgery mortality risk score in a multicenter study proves it stratifies mortality risk in patients undergoing gastric bypass for morbid obesity. Ann Surg. 2007;246(4):578-82. Patients undergoing bariatric surgery in the National Surgical Quality Improvement Program (NSQIP) of the USA were evaluated. Tools were developed and validated for mortality218218 Ramanan B, Gupta PK, Gupta H, Fang X, Forse RA. Development and validation of a bariatric surgery mortality risk calculator. J Am Coll Surg. 2012;214(6):892-900. and morbidity219219 Gupta PK, Franck C, Miller WJ, Gupta H, Forse RA. Development and validation of a bariatric surgery morbidity risk calculator using the prospective, multicenter NSQIP dataset. J Am Coll Surg. 2011;212(3):301-9. risk, specifically for this type of intervention, and this can be accessed and used online:
http://www.surgicalriskcalculator.com/bariatric-surgery-risk-calculator
The largest prospective study performed to date is the longitudinal assessment of bariatric surgery (LABS), with results published in July 2009. A total of 4,776 bariatric surgical interventions were analyzed, and lower complication rates were observed, which is not in agreement with the findings of DeMaria et al.217217 DeMaria EJ, Murr M, Byrne TK, Blackstone R, Grant JP, Budak A, et al. Validation of the obesity surgery mortality risk score in a multicenter study proves it stratifies mortality risk in patients undergoing gastric bypass for morbid obesity. Ann Surg. 2007;246(4):578-82. The authors found a general mortality rate of 0.3% in a period of 30 days and an outcome composed of death, deep venous thrombosis (DVT), PTE, reintervention, and hospitalization > 30 days in 4.3% of the patients. Some predictors of the outcome were similar to those found by DeMaria,217217 DeMaria EJ, Murr M, Byrne TK, Blackstone R, Grant JP, Budak A, et al. Validation of the obesity surgery mortality risk score in a multicenter study proves it stratifies mortality risk in patients undergoing gastric bypass for morbid obesity. Ann Surg. 2007;246(4):578-82. such as BMI > 70 kg/m2, DVT or prior PTE (8.8% of events), and sleep apnea (5.0% of events). The authors also found a correlation between the outcome and diabetes (5.5% of events), and type of surgery and low functional capacity (inability to walk more than 61 meters without dyspnea with 15.9% of events). In this study, the type of surgery with the best outcome was laparoscopic gastric banding (1.0%) compared to laparoscopic Roux-en-Y gastric bypass (4.8%) and open surgery Roux-en-Y gastric bypass (7.8%).220220 Flum DR, Belle SH, King WC, Wahed AS, Berk P, Chapman W, et al. Perioperative safety in the longitudinal assessment of bariatric surgery. N Engl J Med. 2009;361(5):445-54.
Another study with more than 91,000 patients observed that venous thromboembolism occurred in the first 30 days postoperatively in 0.29% of the cases of obese patients undergoing bariatric or metabolic surgery. However, more than 80% of the cases of thromboembolism occurred after hospital discharge. HF, paraplegia, dyspnea at rest, and resurgery were associated with a higher risk of thromboembolism. The authors suggested that routine pharmacological thromboprophylaxis should be considered for high-risk patients (> 0.4%).221221 Aminian A, Andalib A, Khorgami Z, Cetin D, Burguera B, Bartholomew J, et al. Who should get extended thromboprophylaxis after bariatric surgery?: A risk assessment tool to guide indications for post-discharge pharmacoprophylaxis. Ann Surg. 2017;265(1):143-150.
However, there is no consensus with regard to the most appropriate prophylactic measure. A recent meta-analysis found no benefit for any of the different strategies, with enoxaparion ranging from 40 mg per day to 60 mg twice a day.222222 Ikesaka R, Delluc A, Le Gal G, Carrier M. Efficacy and safety of weight-adjusted heparin prophylaxis for the prevention of acute venous thromboembolism among obese patients undergoing bariatric surgery: a systematic review and meta-analysis. Thromb Res. 2014;133(4):682-7.
On the other hand, a study analyzed the strategy of dividing the groups of patients submitted to bariatric surgery (93% gastric bypass) according to the BMI, administering 40 mg twice a day to the group with BMI lower than or equal to 50 kg/m2 and 60 mg twice a day to the group with BMI > 50 kg/m2. The study reported that 74% of the patients reached anti-Xa therapeutic levels and only 1.79% needed blood transfusion.223223 Borkgren-Okonek MJ, Hart RW, Pantano JE, Rantis PC Jr, Guske PJ, Kane JM, et al. Enoxaparin thromboprophylaxis in gastric bypass patients: extended duration, dose stratification, and antifactor Xa activity. Surg Obes Relat Dis. 2008;4(5):625-31.
In addition to the recommendations for obese patients described in another item in this guideline (item 9D), the following recommendations are added for patients with indication for surgical intervention:
I. Indications of Carotid Endarterectomy or Angioplasty According to Symptoms and Degree of Stenosis
II. Indications of Conventional or Endovascular Surgery of Aortic Aneurysm According to Surgical Risk
C) Arterial Vascular Surgeries
Arterial vascular surgeries represent the group of interventions associated with a higher incidence of cardiovascular complications, with rates of almost 50% in some cases, which questions the validity of performing the procedure.224224 Marques AC, Yu PC, Calderaro D, Gualandro DM, Caramelli B. High-risk patients undergoing major vascular surgery: to operate or not to operate? J Am Coll Cardiol. 2007;50(14):1398-9.
On the other hand, it is important to know the indications based on evidences that showed favorable risk-benefit ratio and to identify all variables involved in risk estimation of this type of intervention. This is discussed in more detail in the updated version of the II Guideline for Perioperative Evaluation, with a focus on arterial vascular surgeries, which can be accessed using the link:5050 Marques AC, Bellen BV, Caramelli B, Presti C, Pinho C, Calderaro D, et al; Sociedade Brasileira de Cardiologia. [Update and focus on arterial vascular surgeries from the II Guidelines for Perioperative Evaluation of the Brazilian Society of Cardiology]. Arq Bras Cardiol 2013;101(4 Suppl 2):2-32.,225225 Carmo GA, Calderaro D, Gualandro DM, Casella IB, Yu PC, Marques AC, et al. Carotid stenosis management: a review for the internist. Intern Emerg Med. 2014;9(2):133-42.
The recommendations and general care in this guideline are also necessary for this specific population; however, there are additional specific issues that are addressed below.226226 Rosenfield K, Matsumura JS, Chaturvedi S, Riles T, Ansel GM, Metzger DC, et al; ACT I Investigators. Randomized trial of stent versus surgery for asymptomatic carotid stenosis. N Engl J Med. 2016;374(11):1011-20.,227227 Brott TG, Howard G, Roubin GS, Meschia JF, Mackey A, Brooks W, et al; CREST Investigators. Long-term results of stenting versus endarterectomy for carotid-artery stenosis. N Engl J Med. 2016;374(11):1021-31.
D) Low-risk Procedures
I. Dental
The preparation of dental procedures in patients with heart disease is not based solely on the use of antibiotic prophylaxis, vasoconstrictors, and/or control of postoperative bleeding. The presence of infectious foci in the oral cavity may represent a factor of postoperative complication. The incidence of odontogenic bacteremia increases significantly in the presence of infectious foci, such as in periodontal disease and endodontic lesions.
Although the occurrence of bacteremias is commonly reported during dental procedures, they occur with similar frequency during oral hygiene and chewing.228228 Scannapieco FA. Pneumonia in nonambulatory patients: the role of oral bacteria and oral hygiene. J Am Dent Assoc. 2006;137 Suppl:21S-5S. Erratum in: J Am Dent Assoc. 2008;139(3):252. For this reason, assessment of oral health with elimination of infectious foci and intensive oral hygiene control of hospitalized patients is advisable whenever possible prior to surgical procedures in patients with or without heart disease to reduce perioperative complications.
In general, patients with controlled heart disease under optimized medication can undergo a dental procedure safely with the usual routine care.
Individuals with pacemakers and implantable automatic defibrillators do not present changes with high or low rotation motors, amalgamators, electric pulp tests, electric toothbrushes, endodontic ultrasound, periodontal ultrasound, and radiography. The use of an electric scalpel has specific guidelines discussed in this guideline (item 4.G.III). Further studies are needed to determine the possible effect of the laser on pacemakers.
I. A. Local Anesthetics: to Use or Not to Use Local Vasoconstrictors
The use of local anesthetics with vasoconstrictors in patients with heart disease has generated controversy. The administration of vasoconstrictors in combination with local anesthetics increases the quality and duration of pain control and promotes reduction of bleeding.229229 Brown RS, Rhodus NL. Epinephrine and local anesthesia revisited. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(4):401-8. Local anesthetic without vasoconstrictor has a short duration, rapid absorption (high toxic potential), and inadequate pain control. It can also generate hemodynamic changes and even cardiac arrhythmias, besides promoting mild vasodilation, increasing bleeding.
Lidocaine with epinephrine has been the most widely used local anesthetic worldwide. Although the interaction of epinephrine with β-blockers, tricyclic antidepressants, diuretics, and cocaine has been reported in the literature, the use of two to three 2.0% lidocaine tubes with 1:100,000 epinephrine (36-54 µg epinephrine) is well tolerated in most patients. This also applies to individuals with hypertension or other cardiovascular disease, situations where the use of this vasoconstrictor has more benefits than risks.229229 Brown RS, Rhodus NL. Epinephrine and local anesthesia revisited. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(4):401-8.
I. B. Patients Using Antithrombotic Agents (Antiplatelet Agents and Oral Anticoagulants)
Most dental procedures have low risk of bleeding. Therefore, warfarin should not be discontinued in most patients submitted to dental procedures, including dental extractions.230230 Perry DJ, Noakes TJ, Helliwell PS; British Dental Society. Guidelines for the management of patients on oral anticoagulants requiring dental surgery. Br Dent J. 2007;203(7):389-93. A meta-analysis231231 Wahl MJ. Dental surgery in anticoagulated patients. Arch Intern Med. 1998;158(15):1610-6. and smaller studies232232 Devani P, Lavery KM, Howell CJ. Dental extractions in patients on warfarin: is alteration of anticoagulant regime necessary? Br J Oral Maxillofac Surg. 1998;36(2):107-11.
233 Blinder D, Manor Y, Martinowitz U, Taicher S. Dental extractions in patients maintained on oral anticoagulant therapy: comparison of INR value with occurrence of postoperative bleeding. Int J Oral Maxillofac Surg. 2001;30(6):518-21.-234234 Al-Mubarak S, Rass MA, Alsuwyed A, Alabdulaaly A, Ciancio S. Thromboembolic risk and bleeding in patients maintaining or stopping oral anticoagulant therapy during dental extraction. J Thromb Haemost. 2006;4(3):689-91. have demonstrated safety in performing dental procedures in anticoagulated patients with international normalized ratio (INR) < 4.0 by using local measures to reduce bleeding. Major procedures, and consequently with greater risk of bleeding, such as extraction > 3 teeth, should have customized discussion based on the thrombotic risk of each patient to determine interruption of therapy and possible bridge therapy, as discussed in specific section in this guideline.
To date, evidence of bleeding risk in patients using new anticoagulants (NOACs) in dental procedures is limited.235235 Johnston S. An evidence summary of the management of patients taking direct oral anticoagulants (DOACs) undergoing dental surgery. Int J Oral Maxillofac Surg. 2016;45(5):618-30. There are also no recommendations available for perioperative measures.
Regarding antiplatelet agents, several studies in the literature show the safety of performing dental procedures usually using aspirin or clopidogrel monotherapy.236236 Lillis T, Ziakas A, Koskinas K, Tsirlis A, Giannoglou G. Safety of dental extractions during uninterrupted single or dual antiplatelet treatment. Am J Cardiol. 2011;108(7):964-7.
237 Halley D, Weld-Moore R, Duane B. No evidence for stopping long-term aspirin therapy before tooth extraction. Evid Based Dent. 2015;16(4):118-9.
238 Lu SY, Tsai CY, Lin LH, Lu SN. Dental extraction without stopping single or dual antiplatelet therapy: results of a retrospective cohort study. Int J Oral Maxillofac Surg. 2016;45(10):1293-8.-239239 Zhao B, Wang P, Dong Y, Zhu Y, Zhao H. Should aspirin be stopped before tooth extraction? A meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;119(5):522-30. Although bleeding increases, this is easily controlled with local hemostatic measures.240240 Sánchez-Palomino P, Sánchez-Cobo P, Rodriguez-Archilla A, González-Jaranay M, Moreu G, Calvo-Guirado JL, et al. Dental extraction in patients receiving dual antiplatelet therapy. Med Oral Patol Oral Cir Bucal. 2015;20(5):e616-20.
241 Olmos-Carrasco O, Pastor-Ramos V, Espinilla-Blanco R, Ortiz-Zárate A, García-Avila I, Rodríguez-Alonso E, et al. Hemorrhagic complications of dental extractions in 181 patients undergoing double antiplatelet therapy. J Oral Maxillofac Surg. 2015;73(2):203-10.-242242 Sadeghi-Ghahrody M, Yousefi-Malekshah SH, Karimi-Sari H, Yazdanpanah H, Rezaee-Zavareh MS, Yavarahmadi M. Bleeding after tooth extraction in patients taking aspirin and clopidogrel (Plavix(r)) compared with healthy controls. Br J Oral Maxillofac Surg. 2016;54(5):568-72. Therefore, patients in secondary prevention of cardiovascular events using aspirin or clopidogrel monotherapy should keep using the drugs in the perioperative period of the procedures.
Patients on DAPT with a recent PCI (6 weeks after bare metal stent (BMS) and 6 months after drug eluting stent - DES) or acute coronary syndrome for less than one year should maintain the use of the drugs, if dental procedures are required in the period of highest risk of intra-stent thrombosis. There is already evidence in the literature on the safety of this strategy when local hemostatic measures are increased. Studies with ticagrelor or prasugrel remain scarce,243243 Dézsi BB, Koritsánszky L, Braunitzer G, Hangyási DB, Dézsi CA. Prasugrel versus clopidogrel: a comparative examination of local bleeding after dental extraction in patients receiving dual antiplatelet therapy. J Oral Maxillofac Surg. 2015;73(10):1894-900. but the recommendation is to maintain them in these conditions of DAPT in periods of increased risk of intra-stent thrombosis.
When using antithrombotic therapy, dental procedures may be performed following some precautions.
Specific considerations that may be suggested to dentists
Some precautions and measures may be considered to reduce bleeding in patients taking antithrombotic drugs.
I. C. Use of Antibiotics with Anticoagulants
The use of antibiotics for endocarditis prophylaxis is indicated in patients with previous history of endocarditis or valve disease who will undergo procedures involving manipulation of gingival tissue, periodontal region, or perforation of the oral mucosa, as discussed in a specific section in this guideline (item 7.E.I). Antibiotics often used for this purpose may interfere with the metabolism of oral anticoagulants, particularly warfarin. Patients taking anticoagulants should be alerted to a possible increase in bleeding and control the INR, if necessary. There is no need to change the anticoagulant regimen when a single dose of prophylactic antibiotic is used.
II. Dermatological
Dermatological surgical procedures are low-risk procedures for both cardiovascular and bleeding events. Data from the literature suggest that approximately 50% of patients scheduled for dermatological procedures are using antiplatelet or anticoagulant therapy.244244 O'Neill JL, Taheri A, Solomon JA, Pearce DJ. Postoperative hemorrhage risk after outpatient dermatologic surgery procedures. Dermatol Surg. 2014;40(1):74-6.,245245 Bordeaux JS, Martires KJ, Goldberg D, Pattee SF, Fu P, Maloney ME. Prospective evaluation of dermatologic surgery complications including patients on multiple antiplatelet and anticoagulant medications. J Am Acad Dermatol. 2011;65(3):576-83. In these cases, the surgical team and the anesthesiologist should be informed about the drugs used and the necessary care, including a more time-consuming and cautious hemostasis, because in most cases the risk associated with discontinuation of antithrombotic therapy outweighs the risk of bleeding inherent in the procedure.
Suspension of the use of aspirin for secondary prevention of cardiovascular events is not necessary before performing any dermatological surgical intervention.246246 Dixon AJ, Dixon MP, Dixon JB. Bleeding complications in skin cancer surgery are associated with warfarin but not aspirin therapy. Br J Surg. 2007;94(11):1356-60.,247247 Burger W, Chemnitius JM, Kneissl GD, Rücker G. Low-dose aspirin for secondary cardiovascular prevention - cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation - review and meta-analysis. J Intern Med. 2005;257(5):399-414. For patients using double antiplatelet therapy for stent implantation who are not in the period of greatest thrombotic risk, the recommendation is to suspend the second antiplatelet drug,248248 Palamaras I, Semkova K. Perioperative management of and recommendations for antithrombotic medications in dermatological surgery. Br J Dermatol. 2015;172(3):597-605.,249249 Cook-Norris RH, Michaels JD, Weaver AL, Phillips PK, Brewer JD, Roenigk RK, et al. Complications of cutaneous surgery in patients taking clopidogrel-containing anticoagulation. J Am Acad Dermatol. 2011;65(3):584-91. considering the intervals already described in this guideline (see section on antiplatelet agents - item 7.A.V).
For individuals taking warfarin, the recommendation is to continue its use and adjust the INR to ≤ 3.5 to minimize the risk of bleeding.248248 Palamaras I, Semkova K. Perioperative management of and recommendations for antithrombotic medications in dermatological surgery. Br J Dermatol. 2015;172(3):597-605. However, some studies have not demonstrated the correlation between INR levels and the risk of increased bleeding in patients taking warfarin.250250 Blasdale C, Lawrence CM. Perioperative international normalized ratio level is a poor predictor of postoperative bleeding complications in dermatological surgery patients taking warfarin. Br J Dermatol. 2008;158(3):522-6. Although evidence is scarce, it is recommended that patients taking one of the new oral anticoagulants (NOACs) can perform most of the dermatological procedures during the medications.248248 Palamaras I, Semkova K. Perioperative management of and recommendations for antithrombotic medications in dermatological surgery. Br J Dermatol. 2015;172(3):597-605. This is to ensure that the surgical intervention is scheduled, whenever possible, a few hours before the next dose to avoid the peak serum level of the drug.
III. Endoscopic
Considering the risk analysis of cardiovascular events, endoscopic procedures are low risk.251251 Rogers BH, Silvis SE, Nebel OT, Sugawa C, Mandelstam P. Complications of flexible fiberoptic colonoscopy and polypectomy. Gastrointest Endosc. 1975;22(2):73-7. Thus, suspension of the procedure is not required for cardiovascular intervention, except in severe cardiovascular conditions already mentioned in the section of perioperative evaluation algorithms of this guideline. In addition, most drugs that are included in the cardiovascular therapy do not need to be discontinued and can be ingested with minimal water. In fact, the most important issue is whether the patient makes use of antithrombotic drugs due to the potential risk of endoscopic bleeding and thromboembolic events caused by discontinuation of these drugs.
Bleeding risk in endoscopic procedures* * Adapted from Acosta RD et al.252 UDE: upper digestive endoscopy; ERCP: endoscopic retrograde cholangiopancreatography.
Endoscopic procedures have different bleeding potentials, which is very important to determine the strategy to be used. The risk varies with the type of procedure and is mainly related to the existence of therapeutic interventions. Chart 4 presents the risks of bleeding attributed to common endoscopic procedures in clinical practice.252252 Acosta RD, Abraham NS, Chandrasekhara V, Chathadi KV, Early DS, Eloubeidi MA, et al. The management of antithrombotic agents for patients undergoing GI endoscopy. Gastrointest Endosc. 2016;83(1):3-16. Erratum in: Gastrointest Endosc. 2016 Mar;83(3):678. The risk of thromboembolic events with discontinuation of antithrombotic therapy varies with the therapy proposed and individual patient conditions.
Management of Antiplatelet Agents in Endoscopic Procedures
For endoscopic procedures classified as low risk of bleeding, antiplatelet therapy may be maintained, either in the form of monotherapy (independent of the agent) or DAPT.252252 Acosta RD, Abraham NS, Chandrasekhara V, Chathadi KV, Early DS, Eloubeidi MA, et al. The management of antithrombotic agents for patients undergoing GI endoscopy. Gastrointest Endosc. 2016;83(1):3-16. Erratum in: Gastrointest Endosc. 2016 Mar;83(3):678.
253 Ono S, Fujishiro M, Kodashima S, Takahashi Y, Minatsuki C, Mikami-Matsuda R, et al. Evaluation of safety of endoscopic biopsy without cessation of antithrombotic agents in Japan. J Gastroenterol. 2012;47(7):770-4.
254 Whitson MJ, Dikman AE, von Althann C, Sanyal S, Desai JC, Bamji ND, et al. Is gastroduodenal biopsy safe in patients receiving aspirin and clopidogrel?: a prospective, randomized study involving 630 biopsies. J Clin Gastroenterol. 2011;45(3):228-33.-255255 Veitch AM, Vanbiervliet G, Gershlick AH, Boustiere C, Baglin TP, Smith LA, et al. Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guidelines. Endoscopy. 2016;48(4):385-402. For procedures considered as high risk of bleeding, some points should be considered.
Patients taking DAPT for a recent PCI (6 weeks after BMS stent and 6 months after DES) or acute coronary syndrome in the past year present the highest risk if antiplatelet therapy is discontinued. Therefore, elective high-risk bleeding endoscopic procedures should be postponed, whenever possible, until the end of this period of increased risk. However, for procedures that require to be performed during this period, the most accepted strategy is to maintain aspirin and withdraw the second antiplatelet drug,255255 Veitch AM, Vanbiervliet G, Gershlick AH, Boustiere C, Baglin TP, Smith LA, et al. Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guidelines. Endoscopy. 2016;48(4):385-402.,256256 Becker RC, Scheiman J, Dauerman HL, Spencer F, Rao S, Sabatine M, et al; American College of Cardiology; American College of Gastroenterology. Management of platelet-directed pharmacotherapy in patients with atherosclerotic coronary artery disease undergoing elective endoscopic gastrointestinal procedures. J Am Coll Cardiol. 2009;54(24):2261-76. although evidence for this strategy is limited.
Patients taking aspirin monotherapy for secondary prevention of cardiovascular events may maintain the treatment in the perioperative period of endoscopic procedures, even in those considered to be high risk for bleeding, because most evidence in the literature shows a low risk of significant bleeding in these situations.257257 Kien-Fong Vu C, Chang F, Doig L, Meenan J. A prospective control study of the safety and cellular yield of EUS-guided FNA or Trucut biopsy in patients taking aspirin, nonsteroidal anti-inflammatory drugs, or prophylactic low molecular weight heparin. Gastrointest Endosc. 2006;63(6):808-13.
258 Richter JA, Patrie JT, Richter RP, Henry ZH, Pop GH, Regan KA, et al. Bleeding after percutaneous endoscopic gastrostomy is linked to serotonin reuptake inhibitors, not aspirin or clopidogrel. Gastrointest Endosc. 2011;74(1):22-34.e1.
259 Shiffman ML, Farrel MT, Yee YS. Risk of bleeding after endoscopic biopsy or polypectomy in patients taking aspirin or other NSAIDS. Gastrointest Endosc. 1994;40(4):458-62.
260 Hui AJ, Wong RM, Ching JY, Hung LC, Chung SC, Sung JJ. Risk of colonoscopic polypectomy bleeding with anticoagulants and antiplatelet agents: analysis of 1657 cases. Gastrointest Endosc. 2004;59(1):44-8.
261 Cotton PB, Garrow DA, Gallagher J, Romagnuolo J. Risk factors for complications after ERCP: a multivariate analysis of 11,497 procedures over 12 years. Gastrointest Endosc. 2009;70(1):80-8.
262 Onal IK, Parlak E, Akdogan M, Yesil Y, Kuran SO, Kurt M, et al. Do aspirin and non-steroidal anti-inflammatory drugs increase the risk of post-sphincterotomy hemorrhage--a case-control study. Clin Res Hepatol Gastroenterol. 2013;37(2):171-6.
263 Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;335(13):909-18.
264 Yousfi M, Gostout CJ, Baron TH, Hernandez JL, Keate R, Fleischer DE, et al. Postpolypectomy lower gastrointestinal bleeding: potential role of aspirin. Am J Gastroenterol. 2004;99(9):1785-9.
265 Nelson DB, Freeman ML. Major hemorrhage from endoscopic sphincterotomy: risk factor analysis. J Clin Gastroenterol. 1994;19(4):283-7.-266266 Shalman D, Gerson LB. Systematic review with meta-analysis: the risk of gastrointestinal haemorrhage post-polypectomy in patients receiving anti-platelet, anti-coagulant and/or thienopyridine medications. Aliment Pharmacol Ther. 2015;42(8):949-56. Some studies have demonstrated increased bleeding in procedures, such as submucosal dissection in patients with gastric neoplasia267267 Cho SJ, Choi IJ, Kim CG, Lee JY, Nam BH, Kwak MH, et al. Aspirin use and bleeding risk after endoscopic submucosal dissection in patients with gastric neoplasms. Endoscopy. 2012;44(2):114-21. and mucosectomy in colonic tumors larger than 20 mm,268268 Metz AJ, Bourke MJ, Moss A, Williams SJ, Swan MP, Byth K. Factors that predict bleeding following endoscopic mucosal resection of large colonic lesions. Endoscopy. 2011;43(6):506-11. these procedures should be analyzed individually according to the risk of thrombotic events with suspension of aspirin.255255 Veitch AM, Vanbiervliet G, Gershlick AH, Boustiere C, Baglin TP, Smith LA, et al. Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guidelines. Endoscopy. 2016;48(4):385-402. There is some evidence showing the safety of clopidogrel monotherapy during percutaneous endoscopic gastrostomy, and its maintenance may be considered in this situation.258258 Richter JA, Patrie JT, Richter RP, Henry ZH, Pop GH, Regan KA, et al. Bleeding after percutaneous endoscopic gastrostomy is linked to serotonin reuptake inhibitors, not aspirin or clopidogrel. Gastrointest Endosc. 2011;74(1):22-34.e1. Evidence for the use of prasugrel and ticagrelor in high-risk bleeding endoscopic procedures is scarce.
If antiplatelet therapy is discontinued, the intervals between the suspension and the procedure should follow the recommendations of this guideline in the antiplatelet management section (item 7.A.V.C). Antiplatelet therapy may be resumed after the procedure as soon as hemostasis is achieved. An attack dose may be considered in patients who are at high risk for cardiovascular events.256256 Becker RC, Scheiman J, Dauerman HL, Spencer F, Rao S, Sabatine M, et al; American College of Cardiology; American College of Gastroenterology. Management of platelet-directed pharmacotherapy in patients with atherosclerotic coronary artery disease undergoing elective endoscopic gastrointestinal procedures. J Am Coll Cardiol. 2009;54(24):2261-76.
Management of Anticoagulants in Endoscopic Procedures
For endoscopic procedures classified as low risk of bleeding, anticoagulant therapy with warfarin may be maintained252252 Acosta RD, Abraham NS, Chandrasekhara V, Chathadi KV, Early DS, Eloubeidi MA, et al. The management of antithrombotic agents for patients undergoing GI endoscopy. Gastrointest Endosc. 2016;83(1):3-16. Erratum in: Gastrointest Endosc. 2016 Mar;83(3):678.,253253 Ono S, Fujishiro M, Kodashima S, Takahashi Y, Minatsuki C, Mikami-Matsuda R, et al. Evaluation of safety of endoscopic biopsy without cessation of antithrombotic agents in Japan. J Gastroenterol. 2012;47(7):770-4.,255255 Veitch AM, Vanbiervliet G, Gershlick AH, Boustiere C, Baglin TP, Smith LA, et al. Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guidelines. Endoscopy. 2016;48(4):385-402.,269269 Gerson LB, Gage BF, Owens DK, Triadafilopoulos G. Effect and outcomes of the ASGE guidelines on the periendoscopic management of patients who take anticoagulants. Am J Gastroenterol. 2000;95(7):1717-24. and should be discontinued in those considered to be at high risk of bleeding.260260 Hui AJ, Wong RM, Ching JY, Hung LC, Chung SC, Sung JJ. Risk of colonoscopic polypectomy bleeding with anticoagulants and antiplatelet agents: analysis of 1657 cases. Gastrointest Endosc. 2004;59(1):44-8.,266266 Shalman D, Gerson LB. Systematic review with meta-analysis: the risk of gastrointestinal haemorrhage post-polypectomy in patients receiving anti-platelet, anti-coagulant and/or thienopyridine medications. Aliment Pharmacol Ther. 2015;42(8):949-56. To date, no evidence has been reported regarding the use of new anticoagulants (NOACs) in these situations, suggesting that they should be maintained in low-risk bleeding procedures and suspended in those with high risk for bleeding.252252 Acosta RD, Abraham NS, Chandrasekhara V, Chathadi KV, Early DS, Eloubeidi MA, et al. The management of antithrombotic agents for patients undergoing GI endoscopy. Gastrointest Endosc. 2016;83(1):3-16. Erratum in: Gastrointest Endosc. 2016 Mar;83(3):678.
Intervals for the suspension and resumption of NOACs and warfarin (including consideration of bridge therapy in those patients considered to be at a greatest risk for thromboembolic events) should follow the guidelines in the perioperative management section of this guideline (section 7.D).
IV. Ophthalmologic
Ophthalmologic surgical interventions are relatively frequent procedures in the elderly population. The presence of cardiovascular comorbidities that require the use of antithrombotic drugs and their associated treatment during the perioperative period is a subject of intense debate between ophthalmological surgeons and cardiologists. In Brazil, the fear of hemorrhagic complications, including bruising in the periorbital region, is responsible for the indiscriminate interruption of aspirin and warfarin in 82.7% of patients who undergo glaucoma surgeries.270270 Balbino M, Boin P, Prata TS. Perioperative management of anticoagulant users scheduled for glaucoma surgery: a survey among the Brazilian Glaucoma Society members. Arq Bras Oftalmol. 2013;76(6):363-5.
The limited evidence regarding the occurrence of complications shows that this fear is not reasonable. The rate of hemorrhagic complications described in observational studies is low and without major consequences, particularly in cataract surgeries using conventional anesthetic techniques.271271 Katz J, Feldman MA, Bass EB, Lubomski LH, Tielsch JM, Petty BG, et al; Study of Medical Testing for Cataract Surgery Team. Risks and benefits of anticoagulant and antiplatelet medication use before cataract surgery. Ophthalmology. 2003;110(9):1784-8. Erratum in: Ophthalmology. 2003;110(12):2309.
272 Kallio H, Paloheimo M, Maunuksela EL. Haemorrhage and risk factors associated with retrobulbar/peribulbar block: a prospective study in 1383 patients. Br J Anaesth. 2000;85(5):708-11.
273 Jamula E, Anderson J, Douketis JD. Safety of continuing warfarin therapy during cataract surgery: a systematic review and meta-analysis. Thromb Res. 2009;124(3):292-9.
274 Calenda E, Lamothe L, Genevois O, Cardon A, Muraine M. Peribulbar block in patients scheduled for eye procedures and treated with clopidogrel. J Anesth. 2012;26(5):779-82.-275275 Kumar N, Jivan S, Thomas P, McLure H. Sub-Tenon's anesthesia with aspirin, warfarin, and clopidogrel. J Cataract Refract Surg. 2006;32(6):1022-5.
Some ophthalmologic surgical interventions, such as trabeculectomy276276 Law SK, Song BJ, Yu F, Kurbanyan K, Yang TA, Caprioli J. Hemorrhagic complications from glaucoma surgery in patients on anticoagulation therapy or antiplatelet therapy. Am J Ophthalmol. 2008;145(4):736-46.,277277 Cobb CJ, Chakrabarti S, Chadha V, Sanders R. The effect of aspirin and warfarin therapy in trabeculectomy. Eye (Lond). 2007;21(5):598-603. and vitrectomy,278278 Chauvaud D. [Anticoagulation and vitreoretinal surgery]. Bull Acad Natl Med. 2007;191(4-5):879-84.,279279 Fu AD, McDonald HR, Williams DF, Cantrill HL, Ryan EH, Johnson RN, et al. Anticoagulation with warfarin in vitreoretinal surgery. Retina. 2007;27(3):290-5. which are used to treat glaucoma and retinal diseases, respectively, present a greater hemorrhagic risk. Nevertheless, the evidence does not demonstrate an increased risk of significant hemorrhagic complications in these surgeries with the use of aspirin.277277 Cobb CJ, Chakrabarti S, Chadha V, Sanders R. The effect of aspirin and warfarin therapy in trabeculectomy. Eye (Lond). 2007;21(5):598-603.,280280 Ryan A, Saad T, Kirwan C, Keegan DJ, Acheson RW. Maintenance of perioperative antiplatelet and anticoagulant therapy for vitreoretinal surgery. Clin Exp Ophthalmol. 2013;41(4):387-95.,281281 Narendran N, Williamson TH. The effects of aspirin and warfarin therapy on haemorrhage in vitreoretinal surgery. Acta Ophthalmol Scand. 2003;81(1):38-40. In such cases, the decision should be customized, but maintaining this agent is generally recommended in the perioperative period.282282 Kong KL, Khan J. Ophthalmic patients on antithrombotic drugs: a review and guide to perioperative management. Br J Ophthalmol. 2015;99(8):1025-30.
Patients receiving a DAPT for a recent PCI (6 weeks after BMS stent and 6 months after DES) or acute coronary syndrome in the past year are those at highest risk of events due to discontinuation of antiplatelet therapy. Therefore, ophthalmologic procedures, whenever possible, should be postponed until this period of greatest risk ends.
For procedures that required to be performed in this period, the strategy depends on the hemorrhagic risk of the intervention. For interventions with low hemorrhagic risk (intravitreal injections, cataract, and peribulbar anesthesia), aspirin and P2Y12 receptor inhibitors should be maintained. For interventions with higher hemorrhagic risk, such as vitrectomy and trabulectomy, the most accepted recommendation is the maintenance of aspirin and suspension of the second antiplatelet, considering the intervals already described in a specific section of this guideline (item 7.A.V.C). However, the evidence for this strategy is limited.
Similar to patients taking ASA monotherapy, evidence in the literature favors the maintenance of clopidogrel monotherapy in the perioperative period of cataract surgeries.274274 Calenda E, Lamothe L, Genevois O, Cardon A, Muraine M. Peribulbar block in patients scheduled for eye procedures and treated with clopidogrel. J Anesth. 2012;26(5):779-82.,275275 Kumar N, Jivan S, Thomas P, McLure H. Sub-Tenon's anesthesia with aspirin, warfarin, and clopidogrel. J Cataract Refract Surg. 2006;32(6):1022-5. Evidence is more limited in glaucoma and retinal surgeries. The recommendation is to suspend clopidogrel in the perioperative period of these interventions, considering the 5-day period between the suspension and the procedure.
With regard to patients taking warfarin, the evidence in the literature favors their maintenance in surgeries with lower hemorrhagic risk, such as cataract surgeries, ensuring that the INR is in the therapeutic range.271271 Katz J, Feldman MA, Bass EB, Lubomski LH, Tielsch JM, Petty BG, et al; Study of Medical Testing for Cataract Surgery Team. Risks and benefits of anticoagulant and antiplatelet medication use before cataract surgery. Ophthalmology. 2003;110(9):1784-8. Erratum in: Ophthalmology. 2003;110(12):2309.,272272 Kallio H, Paloheimo M, Maunuksela EL. Haemorrhage and risk factors associated with retrobulbar/peribulbar block: a prospective study in 1383 patients. Br J Anaesth. 2000;85(5):708-11. A meta-analysis of observational studies including patients submitted to cataract surgery and using warfarin found a bleeding incidence of around 10%. This incidence was mostly self-limiting, subconjunctival, and with no visual loss.273273 Jamula E, Anderson J, Douketis JD. Safety of continuing warfarin therapy during cataract surgery: a systematic review and meta-analysis. Thromb Res. 2009;124(3):292-9. On the contrary, in glaucoma and retinal disease surgeries, warfarin should be discontinued. Perioperative management should follow the strategy described in this guideline in the perioperative anticoagulation management section (item 7.D), considering the individual risk of thrombotic events of the patients.
To date, evidence of risk of bleeding during ophthalmologic surgeries in patients using new anticoagulants (NOACs) is limited. No recommendations have been established for their perioperative management.
Recommendations, particularly for patients with coronary stents and mechanical valvular prostheses, should be customized, considering the relationship between thrombotic and hemorrhagic risks. For patients recommended to maintain anticoagulant and/or antiplatelet agents, the surgeon should be informed of the need to ensure adequate hemostasis. A suggestion that can be considered and discussed with the anesthesiologist, who makes the final decision, is the use of a specific type of anesthesia that is less associated with hemorrhagic complications.275275 Kumar N, Jivan S, Thomas P, McLure H. Sub-Tenon's anesthesia with aspirin, warfarin, and clopidogrel. J Cataract Refract Surg. 2006;32(6):1022-5. For antiplatelets, if the decision is to interrupt the drug, it should be restarted postoperatively as soon as possible. In addition, the procedure must be performed in a hospital with competence for urgent hemodynamic intervention (PCI), if necessary.
6. Considerations for High-Risk Patients
A) When the Cardiovascular Risk is Very High - to Perform Surgery or Not to Perform Surgery?
After the patient, the surgeon is the most interested person to define whether a surgery should be performed based on the balance between the risk of complications and the benefit of the intervention. The surgeon generally does not perform surgery if there is a high risk of surgical complications, which is sometimes against the expectations of the patient and his family.283283 Wall A. The surgeon as stakeholder: making the case not to operate. Narrat Inq Bioeth. 2015;5(2):195-200.
However, there are situations in which perioperative evaluation concludes that the risk of cardiaovascular complications, such as myocardial infarction and stroke is high. In this case, it is important that the cardiologist knows the prognosis of the underlying disease to determine whether the risk-benefit ratio is unfavorable and whether the intervention should not be performed. Such information regarding the prognosis of the underlying disease should be requested to the surgeon who requested the evaluation. Class of recommendation I, Level of evidence C.
Noncardiac surgery should be contraindicated when there is objective information that the risk of serious cardiovascular complications, such as cardiac death, nonfatal infarction, and stroke, does not exceed the risk of death from the underlying disease. Class of recommendation IIa, Level of evidence C.
B) Hospital Choice
An important part of the perioperative evaluation by the cardiologist is the analysis of the health institute where the surgical procedure will be performed. Studies have demonstrated that a hospital with a cohesive multiprofessional team who focuses on prompt diagnosis and therapeutics of the complications has a positive influence on the perioperative results.284284 Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288(16):1987-93.
285 Sasichay-Akkadechanunt T, Scalzi CC, Jawad AF. The relationship between nurse staffing and patient outcomes. J Nurs Adm. 2003;33(9):478-85.
286 Carayon P, Gürses AP. A human factors engineering conceptual framework of nursing workload and patient safety in intensive care units. Intensive Crit Care Nurs. 2005;21(5):284-301.-287287 Bucholz EM, Butala NM, Ma S, Normand ST, Krumholz HM. Life Expectancy after Myocardial Infarction, According to Hospital Performance. N Engl J Med. 2016;375(14):1332-42.
In addition, there is evidence that hospitals with a higher number of procedures have lower perioperative mortality compared with those with fewer procedures, even after adjusting for other variables.288288 Birkmeyer JD, Siewers AE, Finlayson EV, Stukel TA, Lucas FL, Batista I, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346(15):1128-37.
In conclusion, in the evaluation of surgical risk, it is imperative to analyze the variables related to the health institute where the procedure will be performed. The analysis provides our patients with more comprehensive counseling. Class of recommendation I, Level of evidence C.
7. Measures to Reduce Surgical Risk from a Cardiovascular Perspective
A) Perioperative Drug Therapy
I. β-blockers
The recommendations regarding the use of β-blockers in the perioperative period of noncardiac surgical interventions have been under intense debate in recent years because of the results of large clinical studies. These studies presented limitations that generate discussions in the academic and care communities.
Pioneering studies in the 1990s suggested that perioperative use of β-blockers could reduce cardiovascular mortality and morbidity in a broad spectrum of patients. Three randomized trials conducted between 2005 and 2006 did not confirm the protective effect of β-blockers in the vascular perioperative period of low- or intermediate-risk patients, highlighting the potential harm, given the association with a higher incidence of bradycardia and hypotension.289289 Brady AR, Gibbs JS, Greenhalgh RM, Powell JT, Sydes MR; POBBLE trial investigators. Perioperative beta-blockade (POBBLE) for patients undergoing infrarenal vascular surgery: results of a randomized double-blind controlled trial. J Vasc Surg. 2005;41(4):602-9.
290 Juul AB, Wetterslev J, Gluud C, Kofoed-Enevoldsen A, Jensen G, Callesen T, et al; DIPOM Trial Group. Effect of perioperative beta blockade in patients with diabetes undergoing major non-cardiac surgery: randomised placebo controlled, blinded multicentre trial. BMJ. 2006;332(7556):1482.-291291 Yang H, Raymer K, Butler R, Parlow J, Roberts R. The effects of perioperative beta-blockade: results of the Metoprolol after Vascular Surgery (MaVS) study, a randomized controlled trial. Am Heart J. 2006;152(5):983-90.
The benefit of β-blockers was later questioned in meta-analyses.292292 Devereaux PJ, Beattie WS, Choi PT, Badner NH, Guyatt GH, Villar JC, et al. How strong is the evidence for the use of perioperative beta blockers in non-cardiac surgery? Systematic review and meta-analysis of randomised controlled trials. BMJ. 2005;331(7512):313-21.,293293 Wiesbauer F, Schlager O, Domanovits H, Wildner B, Maurer G, Muellner M, et al. Perioperative beta-blockers for preventing surgery-related mortality and morbidity: a systematic review and meta-analysis. Anesth Analg. 2007;104(1):27-41. On the other hand, the largest retrospective study on the use of β-blockers in the perioperative period, which analyzed more than 780,000 patients submitted to noncardiac surgery, showed that the impact of β-blockers depends on the estimation of cardiac risk. In high-risk patients, β-blockers are associated with lower mortality, whereas in low-risk patients, no benefit was found and the β-blockers could be harmful.294294 Lindenauer PK, Pekow P, Wang K, Mamidi DK, Gutierrez B, Benjamin EM. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Engl J Med. 2005;353(4):349-61. In 2008, the POISE study was conducted. In this study, 8,351 patients who were mostly having an intermediate risk of complications were randomized to receive metoprolol succinate or placebo starting 2-4 hours prior to noncardiac surgery, with doses up to 400 mg in the first 24 hours. The results showed a lower incidence of MI, reversed cardiac arrest, and cardiac mortality in the group with β-blockers. However, the authors observed two times higher incidence of stroke and greater overall mortality in this group. The high incidence of hypotension and bradycardia was strongly associated with higher mortality and stroke.295295 Devereaux PJ, Yang H, Yusuf S, Guyatt G, Leslie K, Villar JC, et al; POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet. 2008;371(9627):1839-47.
Careful analysis of these data shows a great heterogeneity among studies, mainly regarding the dosage of β-blockers used and time of onset. There are studies that initiated β-blockers a few hours before the surgery, with no time to determine the doses conferring adequate heart rate control.289289 Brady AR, Gibbs JS, Greenhalgh RM, Powell JT, Sydes MR; POBBLE trial investigators. Perioperative beta-blockade (POBBLE) for patients undergoing infrarenal vascular surgery: results of a randomized double-blind controlled trial. J Vasc Surg. 2005;41(4):602-9.
290 Juul AB, Wetterslev J, Gluud C, Kofoed-Enevoldsen A, Jensen G, Callesen T, et al; DIPOM Trial Group. Effect of perioperative beta blockade in patients with diabetes undergoing major non-cardiac surgery: randomised placebo controlled, blinded multicentre trial. BMJ. 2006;332(7556):1482.-291291 Yang H, Raymer K, Butler R, Parlow J, Roberts R. The effects of perioperative beta-blockade: results of the Metoprolol after Vascular Surgery (MaVS) study, a randomized controlled trial. Am Heart J. 2006;152(5):983-90. In other studies, some patients continued to receive β-blockers despite the occurrence of bradycardia and/or hypotension and most importantly without time for hemodynamic adaptation.295295 Devereaux PJ, Yang H, Yusuf S, Guyatt G, Leslie K, Villar JC, et al; POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet. 2008;371(9627):1839-47.
On the other hand, there are studies that started β-blockers earlier, at least one week before the surgery, to determine the adequate dose.296296 Poldermans D, Boersma E, Bax JJ, Thomson IR, van de Ven LL, Blankensteijn JD, et al. The effect of bisoprolol on perioperative mortality and myocardial infarction in high-risk patients undergoing vascular surgery. Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. N Engl J Med. 1999;341(24):1789-94. These were the studies that showed benefit. In 2008, even before the publication of the POISE study, an interesting publication reviewed data from the two main meta-analyses previously cited292292 Devereaux PJ, Beattie WS, Choi PT, Badner NH, Guyatt GH, Villar JC, et al. How strong is the evidence for the use of perioperative beta blockers in non-cardiac surgery? Systematic review and meta-analysis of randomised controlled trials. BMJ. 2005;331(7512):313-21.,293293 Wiesbauer F, Schlager O, Domanovits H, Wildner B, Maurer G, Muellner M, et al. Perioperative beta-blockers for preventing surgery-related mortality and morbidity: a systematic review and meta-analysis. Anesth Analg. 2007;104(1):27-41. based on the heart rate control obtained for each study. The authors divided the data into two groups according to degree of heart rate control, and observed that the trials in which patients achieve the most effective control of heart rate were associated with a reduced incidence of postoperative MI, suggesting that effective control of heart rate is important for achieving cardioprotection.297297 Beattie WS, Wijeysundera DN, Karkouti K, McCluskey S, Tait G. Does tight heart rate control improve beta-blocker efficacy? An updated analysis of the noncardiac surgical randomized trials. Anesth Analg. 2008;106(4):1039-48.
Thus, once the specific indications have been evaluated, the use of β-blockers in the perioperative period must always comply with safety principles. The time of onset should be as early as possible (at least one week before the surgery) to ensure adequate time to evaluate the hemodynamic response of each patient, avoiding bradycardia and hypotension. Low doses should be prescribed, with progressive titration to a HR of 55 to 65 bpm, without hypotension (SBP > 100 mmHg). During the perioperative period, frequent monitoring of HR and BP must be done. If HR < 50 bpm or SBP < 100 mmHg is detected, the β-blockers should be suspended until hemodynamic and chronotropic balance is restored. On the other hand, from the point of view of effectiveness, the benefit of the β-blockers is associated with adequate heart rate control. Therefore, we should target for a HR of 55 to 65 bpm in the pre- and postoperative periods.
Finally, β-blockers should not be withdraw in the perioperative period of patients who receive them chronically for various indications. Acute β-blocker suspension is associated with a significant increase in postoperative mortality.298298 Hoeks SE, Scholte Op Reimer WJ, van Urk H, Jörning PJ, Boersma E, Simoons ML, et al. Increase of 1-year mortality after perioperative beta-blocker withdrawal in endovascular and vascular surgery patients. Eur J Vasc Endovasc Surg. 2007;33(1):13-9.
II. Statins
In addition to reducing cholesterol levels, statins have a pleiotropic effect of reducing inflammation and stabilizing plaques of atherosclerosis. The use of statins to prevent cardiovascular events after vascular surgeries is well established and is based on prospective, randomized, placebo-controlled studies.
In 2004, in the first randomized study published, the authors demonstrated that the use of 20 mg of atorvastatin is associated with a large decrease in major cardiovascular events (death, MI, stroke, unstable angina) in the perioperative period and after 6 months of follow-up. This effect occurred regardless of baseline cholesterol levels.299299 Durazzo AE, Machado FS, Ikeoka DT, De Bernoche C, Monachini MC, Puech-Leão P, et al. Reduction in cardiovascular events after vascular surgery with atorvastatin: a randomized trial. J Vasc Surg. 2004;39(5):967-75.
In 2009, the use of 80 mg of slow-release fluvastatin in 250 patients submitted to vascular surgeries was shown to reduce the occurrence of postoperative myocardial ischemia and the combined outcome of MI and cardiac death in a period of 30 days compared to the placebo group (247 patients).300300 Schouten O, Boersma E, Hoeks SE, Benner R, van Urk H, van Sambeek MR, et al; Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Fluvastatin and perioperative events in patients undergoing vascular surgery. N Engl J Med. 2009;361(10):980-9.
This result was confirmed in a recent meta-analysis involving 23,536 patients, in which the use of statins in the perioperative vascular period reduces overall mortality and MI and stroke rates.301301 Antoniou GA, Hajibandeh S, Vallabhaneni SR, Brennan JA, Torella F. Meta-analysis of the effects of statins on perioperative outcomes in vascular and endovascular surgery. J Vasc Surg. 2015;61(2):519-32.e1. The specific benefits of statins for each type of vascular procedure can be found in a specific guideline for vascular surgeries.5050 Marques AC, Bellen BV, Caramelli B, Presti C, Pinho C, Calderaro D, et al; Sociedade Brasileira de Cardiologia. [Update and focus on arterial vascular surgeries from the II Guidelines for Perioperative Evaluation of the Brazilian Society of Cardiology]. Arq Bras Cardiol 2013;101(4 Suppl 2):2-32. The administration of 20 mg of atorvastatin (or 40 mg of simvastatin) in patients submitted to vascular surgery should be preferably performed two weeks before the procedure and maintained for 30 days. Subsequently, the dose should be adjusted to the individual LDL goal of each patient.
On the other hand, evidence on the use of statins for the prevention of cardiovascular complications in nonvascular surgeries is obtained from retrospective studies. Lindenauer et al.302302 Lindenauer PK, Pekow P, Wang K, Gutierrez B, Benjamin EM. Lipid-lowering therapy and in-hospital mortality following major noncardiac surgery. JAMA. 2004;291(17):2092-9. evaluated 780,591 patients submitted to noncardiac surgeries (92% nonvascular surgeries) in a retrospective cohort study with 77,082 patients (9.9%) receiving statins. In this study, the patients who received statins had lower mortality during hospital stays. Another retrospective case-control study with only nonvascular surgeries, including 989 patients who died postoperatively within 30 days and 1879 controls, showed that the use of statins is also associated with a reduction in mortality (OR = 0.4; CI 0.24-0.68).303303 Noordzij PG, Poldermans D, Schouten O, Schreiner F, Feringa HH, Dunkelgrun M, et al. Beta-blockers and statins are individually associated with reduced mortality in patients undergoing noncardiac, nonvascular surgery. Coron Artery Dis. 2007;18(1):67-72. In a retrospective cohort that included 752 patients submitted to nonvascular surgeries, the authors demonstrated a reduction in the combined outcome of nonfatal MI, AF, and mortality in a period of 30 days in patients using statins.304304 Raju MG, Pachika A, Punnam SR, Gardiner JC, Shishehbor MH, Kapadia SR, et al. Statin therapy in the reduction of cardiovascular events in patients undergoing intermediate-risk noncardiac, nonvascular surgery. Clin Cardiol. 2013;36(8):456-61. Recently, in an analysis of the patients included in the VISION study,305305 Devereaux PJ, Chan MT, Alonso-Coello P, Walsh M, Berwanger O, Villar JC, et al; Vascular Events In Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA. 2012;307(21):2295-304. Erratum in: JAMA. 2012;307(24):2590. Berwanger et al.306306 Berwanger O, Le Manach Y, Suzumura EA, Biccard B, Srinathan SK, Szczeklik W, et al; VISION Investigators. Association between pre-operative statin use and major cardiovascular complications among patients undergoing non-cardiac surgery: the VISION study. Eur Heart J. 2016;37(2):177-85. evaluated 2,842 patients receiving statins and 4,492 patients without statins. They compared the occurrence of mortality, isolated elevation of troponin levels (defined as troponin increased levels, without MI or other cause), and stroke in a period of 30 days by using propensity score matching. About 10% of the patients were submitted to vascular surgeries and the rest to nonvascular procedures. Patients receiving statins showed reduction in the risk of the combined outcome (RR 0.83; 95% CI 0.73-0.95; p = 0.007). The use of statins reduced overall mortality (RR 0.58; 95% CI 0.40-0.83; p = 0.003), cardiovascular mortality (RR 0.42, 95% CI 0.23-0.76; p = 0.004), and the occurrence of isolated increase of troponin levels (RR 0.86, 95% CI 0.73-0.98; p = 0.02). There was no reduction in noncardiovascular mortality and in the rate of MI or stroke. It should be noted that, despite propensity score matching, the patients in the statin group had CAD, diabetes, peripheral vascular disease, aspirin use, and ACE inhibitors/angiotensin receptor blockers more frequently than the patients in the group without statins. Although presenting more risk factors, the patients in the statin group had fewer cardiovascular events.306306 Berwanger O, Le Manach Y, Suzumura EA, Biccard B, Srinathan SK, Szczeklik W, et al; VISION Investigators. Association between pre-operative statin use and major cardiovascular complications among patients undergoing non-cardiac surgery: the VISION study. Eur Heart J. 2016;37(2):177-85. Basing on these studies, we can conclude that the patients with higher cardiovascular risk and those using statins due to comorbidities (CAD, diabetes, peripheral vascular disease) may benefit with the administration of statins in perioperative nonvascular surgeries.
Statins are often withdraw postoperatively. The main reasons for statin withdrawal are as follows: postoperative ileus and inability to administer oral medications, hemodynamic instability, concern with the occurrence of side effects, and lack of awareness of the importance of maintaining statins.307307 Fallouh N, Chopra V. Statin withdrawal after major noncardiac surgery: risks, consequences, and preventative strategies. J Hosp Med. 2012;7(7):573-9.
Perioperative statin suspension in patients who use this medication on a chronic basis is an independent predictor of cardiovascular events following vascular surgeries.308308 Schouten O, Hoeks SE, Welten GM, Davignon J, Kastelein JJ, Vidakovic R, et al. Effect of statin withdrawal on frequency of cardiac events after vascular surgery. Am J Cardiol. 2007;100(2):316-20.,309309 Le Manach Y, Godet G, Coriat P, Martinon C, Bertrand M, Fléron MH, et al. The impact of postoperative discontinuation or continuation of chronic statin therapy on cardiac outcome after major vascular surgery. Anesth Analg. 2007;104(6):1326-33. The use of statins in the perioperative period is safe. Although patients using statins have a higher baseline CPK level, the occurrence of increases above 5 times their reference value or rhabdomyolysis is rare.310310 Schouten O, Kertai MD, Bax JJ, Durazzo AE, Biagini E, Boersma E, et al. Safety of perioperative statin use in high-risk patients undergoing major vascular surgery. Am J Cardiol. 2005;95(5):658-60. Therefore, in patients who already use statins, it should be maintained in the perioperative period.
III. Alpha-agonists
Alpha2-agonists modulate the response of catecholamines to surgery and anesthesia, decreasing the release of noradrenaline and reducing blood pressure and heart rate. The first randomized studies that used clonidine to prevent cardiovascular complications following noncardiac surgeries demonstrated a reduction in myocardial ischemia, but without a reduction in clinical events or mortality.311311 Ellis JE, Drijvers G, Pedlow S, Laff SP, Sorrentino MJ, Foss JF, et al. Premedication with oral and transdermal clonidine provides safe and efficacious postoperative sympatholysis. Anesth Analg. 1994;79(6):1133-40.,312312 Stühmeier KD, Mainzer B, Cierpka J, Sandmann W, Tarnow J. Small, oral dose of clonidine reduces the incidence of intraoperative myocardial ischemia in patients having vascular surgery. Anesthesiology. 1996;85(4):706-12. On the other hand, a meta-analysis demonstrated that α2-agonists reduce mortality and MI in patients submitted to vascular surgeries, but not in those submitted to nonvascular surgeries.313313 Wijeysundera DN, Naik JS, Beattie WS. Alpha-2 adrenergic agonists to prevent perioperative cardiovascular complications: a meta-analysis. Am J Med. 2003;114(9):742-52.
The European Mivazerol Trial (EMIT) evaluated the use of mivazerol in 1,897 patients with CAD submitted to noncardiac surgeries. The authors found a decrease in general mortality and MI or cardiac death only in the subgroup of patients submitted to vascular surgeries.314314 Oliver MF, Goldman L, Julian DG, Holme I. Effect of mivazerol on perioperative cardiac complications during non-cardiac surgery in patients with coronary heart disease: the European Mivazerol Trial (EMIT). Anesthesiology. 1999;91(4):951-61.
A randomized study with 190 patients demonstrated reductions in myocardial ischemia and mortality with the use of perioperative prophylactic clonidine in patients with CAD or risk factors for CAD,315315 Wallace AW, Galindez D, Salahieh A, Layug EL, Lazo EA, Haratonik KA, et al. Effect of clonidine on cardiovascular morbidity and mortality after noncardiac surgery. Anesthesiology. 2004;101(2):284-93. but these results were not confirmed.
Recently, the POISE-2 study included 10,010 patients submitted to noncardiac surgery in 23 countries. The patients were randomized to receive clonidine or placebo in the perioperative period of noncardiac surgeries. The use of clonidine did not reduce the incidence of death or MI in a period of 30 days (HR 1.08, 95% CI 0.93-1.26; p = 0.29). Furthermore, patients on clonidine more frequently presented clinically significant hypotension (HR 1.3, 95% CI 1.24-1.4, p < 0.001) and reversed cardiac arrest (HR 3.2, 95% CI 1.17-8.76, p = 0.02).316316 Devereaux PJ, Sessler DI, Leslie K, Kurz A, Mrkobrada M, Alonso-Coello P, et al; POISE-2 Investigators. Clonidine in patients undergoing noncardiac surgery. N Engl J Med. 2014;370(16):1504-13.
Therefore, the introduction of clonidine in the preoperative period is not recommended to reduce the risk of cardiovascular events.
IV. Calcium Channel Blockers
Evidence for the use of calcium channel blockers with the aim to reduce cardiovascular risk in the perioperative period of noncardiac surgeries is scarce. In a meta-analysis of 11 studies involving 1,007 patients, there was no reduction in mortality or MI with verapamil, diltiazem, or dihydropyridine.317317 Wijeysundera DN, Beattie WS. Calcium channel blockers for reducing cardiac morbidity after noncardiac surgery: a meta-analysis. Anesth Analg. 2003;97(3):634-41. Another study evaluated 1,000 patients submitted to aortic aneurysm surgeries, and the results demonstrated an increase in perioperative mortality with the use of calcium channel blockers.318318 Kertai MD, Westerhout CM, Varga KS, Acsady G, Gal J. Dihydropiridine calcium-channel blockers and perioperative mortality in aortic aneurysm surgery. Br J Anaesth. 2008;101(4):458-65.
Therefore, the use of calcium channel blockers to prevent cardiovascular events in the perioperative period of noncardiac surgeries is not recommended.
V. Antiplatelet Agents
Operating patients who use antiplatelet therapy implies an increased risk of bleeding;247247 Burger W, Chemnitius JM, Kneissl GD, Rücker G. Low-dose aspirin for secondary cardiovascular prevention - cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation - review and meta-analysis. J Intern Med. 2005;257(5):399-414. however, the suspension is known to be associated with rebound effect319319 Beving H, Zhao C, Albåge A, Ivert T. Abnormally high platelet activity after discontinuation of acetylsalicylic acid treatment. Blood Coagul Fibrinolysis. 1996;7(1):80-4. and clinical atherothrombotic events.247247 Burger W, Chemnitius JM, Kneissl GD, Rücker G. Low-dose aspirin for secondary cardiovascular prevention - cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation - review and meta-analysis. J Intern Med. 2005;257(5):399-414.,320320 Biondi-Zoccai GG, Lotrionte M, Agostoni P, Abbate A, Fusaro M, Burzotta F, et al. A systematic review and meta-analysis on the hazards of discontinuing or not adhering to aspirin among 50,279 patients at risk for coronary artery disease. Eur Heart J. 2006;27(22):2667-74. In general, the decision should be based on the discussion between the surgical, clinical, and anesthetic teams. The team should consider the risk of exacerbation of bleeding inherent to the surgical procedure and, on the other hand, the thrombotic burden that led to the prescription of the antiplatelet agent.
V. A. Acetylsalicylic Acid
POISE-2 study, which was published in 2014, is the largest randomized, placebo-controlled study evaluating the impact of ASA in the perioperative period.321321 Devereaux PJ, Mrkobrada M, Sessler DI, Leslie K, Alonso-Coello P, Kurz A, et al; POISE-2 Investigators. Aspirin in patients undergoing noncardiac surgery. N Engl J Med. 2014;370(16):1494-503. In this study, 10,010 patients with risk factors for perioperative complications receiving ASA or placebo were evaluated. Patients who never took ASA were included, as well as patients who were already on chronic use, randomized to placebo, or continued ASA at the study doses of 200 mg immediately prior to surgery and 100 mg daily for 30 days. The authors did not show a significant difference in the primary outcome (death or MI) or in the secondary outcome of the study (death, MI or stroke). No difference was observed based on the history of use of pre-randomization ASA. On the other hand, they observed a higher incidence of bleeding in the ASA group: 4.6% × 3.8%, p = 0.04, especially at the surgical site.
Some considerations should be made regarding the clinical profile of patients who mostly (almost 70% of the population) had no history of cardiovascular disease and used ASA for primary prevention. Another extremely relevant fact is the non-inclusion of patients with PCI with DES in the last year or BMS in the last 6 weeks. Most surgeries in the study were orthopedic, general, or gynecological, with 605 vascular procedures, for which the main results of the study are maintained.321321 Devereaux PJ, Mrkobrada M, Sessler DI, Leslie K, Alonso-Coello P, Kurz A, et al; POISE-2 Investigators. Aspirin in patients undergoing noncardiac surgery. N Engl J Med. 2014;370(16):1494-503. Thus, the most practical applicability of POISE-2 results is to recommend the non-use of ASA in the perioperative period of individuals in primary prevention. For patients who are already using ASA for primary prevention and are scheduled for noncardiac surgery, suspension of antiplatelet treatment 7 days before is recommended.
Oscarsson et al.322322 Oscarsson A, Gupta A, Fredrikson M, Järhult J, Nyström M, Pettersson E, et al. To continue or discontinue aspirin in the perioperative period: a randomized, controlled clinical trial. Br J Anaesth. 2010;104(3):305-12. conducted a much smaller study than POISE-2. It included 210 patients. The study design was interesting because it did not investigate the initiation of ASA, but the suspension or maintenance in the noncardiac perioperative period of patients chronically using ASA. Patients scheduled for vascular surgeries were not included (the authors thought that it was unethical to withdraw the antiplatelet treatment in the vascular perioperative period). They observed a lower incidence of cardiovascular events in the group that maintained ASA, without a higher incidence of bleeding. Anecdotally, the subjective notion of the surgeon on the bleeding tendency due to impaired hemostasis during the surgery did not allow discriminating patients receiving placebo or antiplatelets.322322 Oscarsson A, Gupta A, Fredrikson M, Järhult J, Nyström M, Pettersson E, et al. To continue or discontinue aspirin in the perioperative period: a randomized, controlled clinical trial. Br J Anaesth. 2010;104(3):305-12.
In the STRATAGEM study, the patients using ASA only for secondary cardiovascular prevention were randomized to receive 75 mg of ASA or placebo in the perioperative period. The results showed no increased incidence of bleeding or significant difference in thrombotic complications.323323 Mantz J, Samama CM, Tubach F, Devereaux PJ, Collet JP, Albaladejo P, et al; Stratagem Study Group. Impact of preoperative maintenance or interruption of aspirin on thrombotic and bleeding events after elective non-cardiac surgery: the multicentre, randomized, blinded, placebo-controlled, STRATAGEM trial. Br J Anaesth. 2011;107(6):899-910. However, this study included only 20% of the planned patients, which hinders definitive conclusions for patients at higher risk.
In the vascular perioperative period, evidence suggests the beneficial use of ASA for protection of infrainguinal grafts, but without conclusion about systemic outcomes. On the other hand, Calderaro et al.324324 Calderaro D, Pastana AF, Flores da Rocha TR, Yu PC, Gualandro DM, DeLuccia N, et al. Aspirin responsiveness safely lowers perioperative cardiovascular risk. J Vasc Surg. 2013;58(6):1593-9. analyzed patients in the elective vascular perioperative who were already on chronic use of ASA and observed that those individuals with lower platelet responsivity up to 100 mg daily (according to the aggregability test after stimulation with arachidonic acid) presented more than twice the systemic atherothrombotic events, when compared to the more responsive individuals, without an increase in bleeding rate.324324 Calderaro D, Pastana AF, Flores da Rocha TR, Yu PC, Gualandro DM, DeLuccia N, et al. Aspirin responsiveness safely lowers perioperative cardiovascular risk. J Vasc Surg. 2013;58(6):1593-9.
For patients receiving ASA for secondary prevention, it is recommended to maintain it at a maximum dose of 100 mg daily. Meta-analysis data suggest that this ratio is favorable for most perioperative patients.247247 Burger W, Chemnitius JM, Kneissl GD, Rücker G. Low-dose aspirin for secondary cardiovascular prevention - cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation - review and meta-analysis. J Intern Med. 2005;257(5):399-414. Neurosurgeries due to high morbidity and mortality associated with bleeding, even small ones, represent an absolute indication for ASA suspension 7 days before.247247 Burger W, Chemnitius JM, Kneissl GD, Rücker G. Low-dose aspirin for secondary cardiovascular prevention - cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation - review and meta-analysis. J Intern Med. 2005;257(5):399-414.
Patients scheduled for transurethral resection of the prostate using the conventional technique should also suspend ASA owing to the high risk of bleeding.247247 Burger W, Chemnitius JM, Kneissl GD, Rücker G. Low-dose aspirin for secondary cardiovascular prevention - cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation - review and meta-analysis. J Intern Med. 2005;257(5):399-414. Urologists recently acknowledged that ASA can be maintained using the hemostatic technique called laser green-light in patients scheduled for transurethral resection.325325 Culkin DJ, Exaire EJ, Green D, Soloway MS, Gross AJ, Desai MR, et al. Anticoagulation and antiplatelet therapy in urological practice: ICUD/AUA review paper. J Urol. 2014;192(4):1026-34.,326326 Lee DJ, Rieken M, Halpern J, Zhao F, Pueschel H, Chughtai B, et al. Laser vaporization of the prostate with the 180-W XPS-Greenlight Laser in patients with ongoing platelet aggregation inhibition and oral anticoagulation. Urology. 2016;91:167-73. This example demonstrates the benefit of new techniques for more complex patients and the constant need for a multidisciplinary approach to the perioperative decision process. At present, there is no recommendation for routine ASA withdrawal for transrectal prostate biopsy, an extremely common urological procedure.325325 Culkin DJ, Exaire EJ, Green D, Soloway MS, Gross AJ, Desai MR, et al. Anticoagulation and antiplatelet therapy in urological practice: ICUD/AUA review paper. J Urol. 2014;192(4):1026-34.
There is no recommendation to start ASA before noncardiac surgeries. If we evaluate patients with established vascular disease but who erroneously omit using antiplatelets, it is the opinion of this guideline by consensus of the specialists that this therapy should be implemented at the time of hospital discharge. However, no study has supported the administration of the drug before surgery.
V. B. Dual Antiplatelet Therapy
Approximately 20% of patients submitted to PCI will require noncardiac surgery in the subsequent 2 years.327327 Hawn MT, Graham LA, Richman JR, Itani KM, Plomondon ME, Altom LK, et al. The incidence and timing of noncardiac surgery after cardiac stent implantation. J Am Coll Surg. 2012;214(4):658-66.,328328 Tokushige A, Shiomi H, Morimoto T, Ono K, Furukawa Y, Nakagawa Y, et al; CREDO-Kyoto PCI/CABG Registry Cohort-2 Investigators. Incidence and outcome of surgical procedures after coronary artery bypass grafting compared with those after percutaneous coronary intervention: a report from the Coronary Revascularization Demonstrating Outcome Study in Kyoto PCI/CABG Registry Cohort-2. Circ Cardiovasc Interv. 2014;7(4):482-91. This implies perioperative management not only of ASA but also of the second antiplatelet agent (clopidogrel, prasugrel or ticagrelor), particularly in cases with less than one year between interventions. This is a common and quite complex situation because evidence on the safety of maintaining DAPT in the noncardiac perioperative period is scarce and indirect. The evidence is mainly extrapolated from the cardiac surgery data, which reveals a great increase in the rate of bleeding.329329 Yende S, Wunderink RG. Effect of clopidogrel on bleeding after coronary artery bypass surgery. Crit Care Med. 2001;29(12):2271-5.,330330 Hongo RH, Ley J, Dick SE, Yee RR. The effect of clopidogrel in combination with aspirin when given before coronary artery bypass grafting. J Am Coll Cardiol. 2002;40(2):231-7. On the other hand, the potential for treatment suspension is also quite high, especially after PCI, with DAPT suspension being one of the main predictors of stent thrombosis.331331 Grines CL, Bonow RO, Casey DE, Gardner TJ, Lockhart PB, Moliterno DJ, et al; American Heart Association.; American College of Cardiology.; Society for Cardiovascular Angiography and Interventions.; American College of Surgeons.; American Dental Association.; American College of Physicians. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. J Am Coll Cardiol. 2007;49(6):734-9. An interesting study was conducted in France evaluating 1,134 patients with PCI who required subsequent noncardiac surgery. The study identified DAPT suspension for more than 5 days before the surgery as one of the independent predictors of perioperative cardiovascular complications.332332 Albaladejo P, Marret E, Samama CM, Collet JP, Abhay K, Loutrel O, et al. Non-cardiac surgery in patients with coronary stents: the RECO study. Heart. 2011;97(19):1566-72.
The best way to deal with DAPT in the perioperative period is to maintain the optimal duration of this therapy and not to perform elective surgeries during this period (see the topic of prophylactic myocardial revascularization in this guideline - item 7.B): 6 weeks after PCI with BMS; 6 months after DES or one year after PCI in the context of acute coronary syndromes. Some elective procedures, such as oncological treatment, cannot be postponed without consequences. In this situation, it is recommended to maintain ASA alone and suspend clopidogrel. Clopidogrel should be suspended 5 days before the surgery and restarted as soon as possible, ideally before completing 10 days without DAPT. The postoperative deadline for restarting the drug depends on adequate hemostasis control and should be individually established between the surgical and clinical teams. Basing on the evidence of relative safety of withdrawal of the second antiplatelet in up to 10 days, we recommend not to exceed a total of 10 days without DAPT outside the perioperative context.333333 Eisenberg MJ, Richard PR, Libersan D, Filion KB. Safety of short-term discontinuation of antiplatelet therapy in patients with drug-eluting stents. Circulation. 2009;119(12):1634-42.
Evidence is even scarcer for the newer antiplatelet drugs. The TRITON-TIMI 38 study included patients receiving prasugrel or clopidogrel associated with ASA and requiring cardiac surgery. Prasugrel showed higher rates of bleeding than clopidogrel, even with suspension of clopidogrel or prasugrel for up to 7 days.334334 Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, et al; TRITON-TIMI 38 Investigators. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357(20):2001-15. This observation supports the recommendation to discontinue prasugrel 7 days before noncardiac surgeries.
Although pharmacokinetic data support the suspension of ticagrelor for a shorter period,335335 Gurbel PA, Bliden KP, Butler K, Tantry US, Gesheff T, Wei C, et al. Randomized double-blind assessment of the ONSET and OFFSET of the antiplatelet effects of ticagrelor versus clopidogrel in patients with stable coronary artery disease: the ONSET/OFFSET study. Circulation. 2009;120(25):2577-85. the current recommendation is still 5 days. Sub-analysis of patients who required myocardial revascularization in the PLATO study (patients randomized to ASA + ticagrelor vs. ASA + clopidogrel) demonstrated less bleeding with ticagrelor than with clopidogrel. This finding is in agreement with the idea of a faster platelet activity recovery after suspension of ticagrelor in comparison with clopidogrel.336336 Held C, Asenblad N, Bassand JP, Becker RC, Cannon CP, Claeys MJ, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes undergoing coronary artery bypass surgery: results from the PLATO (Platelet Inhibition and Patient Outcomes) trial. J Am Coll Cardiol. 2011;57(6):672-84.,337337 Varenhorst C, Alström U, Scirica BM, Hogue CW, Åsenblad N, Storey RF, et al. Factors contributing to the lower mortality with ticagrelor compared with clopidogrel in patients undergoing coronary artery bypass surgery. J Am Coll Cardiol. 2012;60(17):1623-30.
The new drug eluting stents are less thrombogenic; thus, the ideal interval for noncardiac surgery is shortened to 6 months in cases of elective PCI (see specific session of prophylactic myocardial revascularization in this guideline - item 7.B). Notably, maintenance of DAPT can be considered for some procedures performed in compressible sites or by endovascular technique depending on multidisciplinary consensus.
Patients at very high risk of stent thrombosis, such as diabetic or with PCI involving grafts, or in the context of acute coronary syndromes or complicated PCI, may be considered for “bridge” therapy with parenteral antiplatelet consisting of glycoprotein IIb/IIIa inhibitors.338338 Savonitto S, D'Urbano M, Caracciolo M, Barlocco F, Mariani G, Nichelatti M, et al. Urgent surgery in patients with a recently implanted coronary drug-eluting stent: a phase II study of 'bridging' antiplatelet therapy with tirofiban during temporary withdrawal of clopidogrel. Br J Anaesth. 2010;104(3):285-91. There is no recommendation for “bridge” therapy with LMWH because recent clinical evidence has demonstrated the harm of such measure, in addition to the pharmacological need of inhibition of platelet activity rather than coagulation.339339 Capodanno D, Musumeci G, Lettieri C, Limbruno U, Senni M, Guagliumi G, et al. Impact of bridging with perioperative low-molecular-weight heparin on cardiac and bleeding outcomes of stented patients undergoing non-cardiac surgery. Thromb Haemost. 2015;114(2):423-31.
B) Myocardial Revascularization
The first studies that analyzed the role of myocardial revascularization before noncardiac surgery suggested that it could be indicated to reduce perioperative cardiovascular risk.340340 Eagle KA, Rihal CS, Mickel MC, Holmes DR, Foster ED, Gersh BJ. Cardiac risk of noncardiac surgery: influence of coronary disease and type of surgery in 3368 operations. CASS Investigators and University of Michigan Heart Care Program. Coronary Artery Surgery Study. Circulation. 1997;96(6):1882-7.,341341 Hassan SA, Hlatky MA, Boothroyd DB, Winston C, Mark DB, Brooks MM, et al. Outcomes of noncardiac surgery after coronary bypass surgery or coronary angioplasty in the Bypass Angioplasty Revascularization Investigation (BARI). Am J Med. 2001;110(4):260-6. This strategy aimed at reducing the risk of ischemic events related to severe and fixed coronary stenosis(342). Nevertheless, the events related to the instability of atherosclerotic plaques are not reduced. Atherosclerotic plaque rupture is a pathophysiological mechanism known to be involved in the genesis of ischemic events in the perioperative context.6868 Gualandro DM, Campos CA, Calderaro D, Yu PC, Marques AC, Pastana AF, et al. Coronary plaque rupture in patients with myocardial infarction after noncardiac surgery: frequent and dangerous. Atherosclerosis. 2012;222(1):191-5.
Recent evidence in the literature has failed to demonstrate the beneficial role of prophylactic myocardial revascularization (CABG or PCI) in patients with stable CAD in the preoperative period in noncardiac surgeries.343343 McFalls EO, Ward HB, Moritz TE, Goldman S, Krupski WC, Littooy F, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med. 2004;351(27):2795-804.,344344 Wong EY, Lawrence HP, Wong DT. The effects of prophylactic coronary revascularization or medical management on patient outcomes after noncardiac surgery--a meta-analysis. Can J Anaesth. 2007;54(9):705-17. In addition, the development of drug therapy and consequent perioperative pharmacoprotection have made the potential benefits of prophylactic myocardial revascularization increasingly restricted. Therefore, indications for preoperative myocardial revascularization in noncardiac surgeries are identical to those outside the perioperative context.345345 Cesar LA, Ferreira JF, Armaganijan D, Gowdak LH, Mansur AP, Bodanese LC, et al; Sociedade Brasileira de Cardiologia. Guideline for stable coronary artery disease. Arq Bras Cardiol. 2014;103(2 Suppl 2):1-56. The indications aimed not only to reduce perioperative ischemic events but also to improve long-term prognosis.
In cases with unequivocal indication of myocardial revascularization in patients who are in the preoperative period of noncardiac surgeries, information, such as clinical stability of the patient, prognosis of the underlying disease that led to the indication of the surgical procedure, and the potential risk of bleeding of this procedure, should be considered in decision-making. In these cases, the interval between myocardial revascularization and noncardiac surgery is an important factor, particularly in cases of PCI.346346 Kaluza GL, Joseph J, Lee JR, Raizner ME, Raizner AE. Catastrophic outcomes of noncardiac surgery soon after coronary stenting. J Am Coll Cardiol. 2000;35(5):1288-94.
347 Nuttall GA, Brown MJ, Stombaugh JW, Michon PB, Hathaway MF, Lindeen KC, et al. Time and cardiac risk of surgery after bare-metal stent percutaneous coronary intervention. Anesthesiology. 2008;109(4):588-95.
348 Rabbitts JA, Nuttall GA, Brown MJ, Hanson AC, Oliver WC, Holmes DR, et al. Cardiac risk of noncardiac surgery after percutaneous coronary intervention with drug-eluting stents. Anesthesiology. 2008;109(4):596-604.-349349 Calderaro D, Marques AC, Yu PC, Gualandro DM, Caramelli B. Bare metal stenting and noncardiac surgery, how long should we wait? Am J Cardiol. 2010;105(7):1040-1.
When the surgery must be performed during the endothelization period of the stent, the risk of stent thrombosis and the risk of hemorrhagic complications associated with the use of double antiplatelet therapy increase. In the perioperative period, the French registry of more than 1,000 patients submitted to noncardiac surgery after PCI with stent (DES in one third of them) reaffirmed that one of the main predictors of cardiac complications is the suspension of DAPT more than 5 days before the surgery, regardless of the type of stent.332332 Albaladejo P, Marret E, Samama CM, Collet JP, Abhay K, Loutrel O, et al. Non-cardiac surgery in patients with coronary stents: the RECO study. Heart. 2011;97(19):1566-72. Therefore, elective operations must be performed whenever possible after the end of this high-risk period.
In contrast to what we observed in the context of isolated coronary disease, DES present an enormous fear in the perioperative period and a potentially higher risk than BMS because of the greater and more lasting thrombogenicity associated to them. Thus, when noncardiac surgery is required in a near future (formerly a year, with paclitaxel stents or first-generation sirolimus stents), the use of DES is contraindicated.331331 Grines CL, Bonow RO, Casey DE, Gardner TJ, Lockhart PB, Moliterno DJ, et al; American Heart Association.; American College of Cardiology.; Society for Cardiovascular Angiography and Interventions.; American College of Surgeons.; American Dental Association.; American College of Physicians. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. J Am Coll Cardiol. 2007;49(6):734-9. Consequently, when the surgical procedure needs to be performed shortly, PCI with BMS or even balloon PCI without stent should be considered, provided they present favorable primary outcome.
With most modern DES, recent evidence suggests that the duration of DAPT can be shortened to 6 months350350 Wijeysundera DN, Wijeysundera HC, Yun L, Wasowicz M, Beattie WS, Velianou JL, et al. Risk of elective major noncardiac surgery after coronary stent insertion: a population-based study. Circulation. 2012;126(11):1355-62.
351 Hawn MT, Graham LA, Richman JS, Itani KM, Henderson WG, Maddox TM. Risk of major adverse cardiac events following noncardiac surgery in patients with coronary stents. JAMA. 2013;310(14):1462-72. Erratum in: JAMA. 2014;311(5):528.-352352 D'Ascenzo F, Moretti C, Bianco M, Bernardi A, Taha S, Cerrato E, et al. Meta-analysis of the duration of dual antiplatelet therapy in patients treated with second-generation drug-eluting stents. Am J Cardiol. 2016;117(11):1714-23. and exceptionally 3 months.353353 Feres F, Costa RA, Abizaid A, Leon MB, Marin-Neto JA, Botelho RV, et al; OPTIMIZE Trial Investigators. Three vs twelve months of dual antiplatelet therapy after zotarolimus-eluting stents: the OPTIMIZE randomized trial. JAMA. 2013;310(23):2510-22.,354354 Levine GN, Bates ER, Bittl JA, Brindis RG, Fihn SD, Fleisher LA, et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2016;68(10):1082-115. On the other hand, when PCI is performed to treat acute coronary syndromes, especially in cases of MI, duration of DAPT should be one year, regardless of the type of stent implanted.354354 Levine GN, Bates ER, Bittl JA, Brindis RG, Fihn SD, Fleisher LA, et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2016;68(10):1082-115.
Recommendations for the Safety Interval between Elective Myocardial Revascularization and Noncardiac Surgery
Recommendations for the Safety Interval between Myocardial Revascularization (Cabg or Pci) in the Context of Acute Coronary Syndromes and Noncardiac Surgery
Contextualizing these most recent data on shortening the duration of DAPT in the perioperative period, Holcomb et al. demonstrated that the risk of complications following noncardiac surgeries is significantly reduced from the 6th month of PCI with DES.355355 Holcomb CN, Graham LA, Richman JS, Rhyne RR, Itani KM, Maddox TM, et al. The incremental risk of noncardiac surgery on adverse cardiac events following coronary stenting. J Am Coll Cardiol. 2014;64(25):2730-9. The authors analyzed more than 20,000 cases of noncardiac surgeries after coronary PCI, with approximately half of them with DES. Notably, they also introduced another important concept of interventional treatment of acute coronary disease in the perioperative period. When PCI was performed in the context of MI even after one year, the risk of thrombotic complications is still greater than in cases where PCI was performed electively.356356 Holcomb CN, Hollis RH, Graham LA, Richman JS, Valle JA, Itani KM, et al. Association of Coronary Stent Indication With Postoperative Outcomes Following Noncardiac Surgery. JAMA Surg. 2016;151(5):462-9.
C) Prophylaxis for Venous Thromboembolism
The adequate prophylaxis for venous thromboembolism in the perioperative evaluation involves detailed knowledge of the risk factors of each patient together with the risks inherent to the surgical procedure.
It is important to consider that most hospitalized patients have one or more risk factors for venous thromboembolism357357 Excellence NIfHaC. Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in inpatients undergoing surgery. NICE clinical guideline No. 46:1-160. [Accessed in 2008 Mar 31]. Available from: http://www.nice.org.uk/CG046
http://www.nice.org.uk/CG046...
358 Anderson FA, Wheeler HB, Goldberg RJ, Hosmer DW, Forcier A. The prevalence of risk factors for venous thromboembolism among hospital patients. Arch Intern Med. 1992;152(8):1660-4.
359 Rosendaal FR. Risk factors for venous thrombotic disease. Thromb Haemost. 1999;82(2):610-9.
360 Rosendaal FR. Venous thrombosis: a multicausal disease. Lancet. 1999;353(9159):1167-73.
361 Heit JA, O'Fallon WM, Petterson TM, Lohse CM, Silverstein MD, Mohr DN, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med. 2002;162(11):1245-8.
362 Anderson FA, Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I9-16.
363 Samama MM, Dahl OE, Quinlan DJ, Mismetti P, Rosencher N. Quantification of risk factors for venous thromboembolism: a preliminary study for the development of a risk assessment tool. Haematologica. 2003;88(12):1410-21.
364 Edmonds MJ, Crichton TJ, Runciman WB, Pradhan M. Evidence-based risk factors for postoperative deep vein thrombosis. ANZ J Surg. 2004;74(12):1082-97.
365 Kucher N, Tapson VF, Goldhaber SZ; DVT FREE Steering Committee. Risk factors associated with symptomatic pulmonary embolism in a large cohort of deep vein thrombosis patients. Thromb Haemost. 2005;93(3):494-8.-366366 Gangireddy C, Rectenwald JR, Upchurch GR, Wakefield TW, Khuri S, Henderson WG, et al. Risk factors and clinical impact of postoperative symptomatic venous thromboembolism. J Vasc Surg. 2007;45(2):335-41. and that these factors have a cumulative character (Chart 5).360360 Rosendaal FR. Venous thrombosis: a multicausal disease. Lancet. 1999;353(9159):1167-73.
The incidence of confirmed thromboembolism in hospitalized patients without adequate thromboprophylaxis may vary widely, depending on the type of surgery performed, as outlined in table 2.367367 Gould MK, Garcia DA, Wren SM, Karanicolas PJ, Arcelus JI, Heit JA, et al; American College of Chest Physicians. Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e227S-77S. Erratum in: Chest. 2012;141(5):1369.
There is strong evidence in the literature that adequate thromboprophylaxis in surgical patients is cost-effective, with an optimal cost-benefit ratio.368368 Geerts WH, Pineo GF, Heit JA, Bergqvist D, Lassen MR, Colwell CW, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 Suppl):338S-400S. Despite the evidence available, with more than 20 guidelines recommending its use since 1986, it is not frequently applied, compromising patient safety.369369 Ahmad HA, Geissler A, MacLellan DG. Deep venous thrombosis prophylaxis: are guidelines being followed? ANZ J Surg. 2002;72(5):331-4.,370370 Deheinzelin D, Braga AL, Martins LC, Martins MA, Hernandez A, Yoshida WB, et al; Trombo Risc Investigators. Incorrect use of thromboprophylaxis for venous thromboembolism in medical and surgical patients: results of a multicentric, observational and cross-sectional study in Brazil. J Thromb Haemost. 2006;4(6):1266-70.
Mechanical thromboprophylaxis should be the primary method to prevent VTE in patients at high risk of bleeding. When pharmacological prophylaxis is indicated, the doses recommended by each manufacturer should be followed. In general, we consider the following doses: UFH, 5,000 IU, subcutaneously (SC), 12/12h or 8/8h; LMWH (dalteparin 5,000 IU, SC, 1x/day; tinzaparin 4,500 IU, SC, 1x/day; enoxaparin 40 mg, SC, 1x/day); and fondaparinux, 2.5 mg, SC, 1x/day (in individuals > 50 kg). Aspirin should not be used alone in any group of patients as thromboprophylaxis for VTE.
Evaluation of renal function is fundamentally important when considering the use and dose of LMWH, fondaparinux, or other thrombotic agents excreted by the kidneys, especially in elderly, diabetic, or at high risk of bleeding individuals. In such circumstances, the use of antithrombotic drugs with renal metabolism should be avoided. Smaller doses of the drug should be used, or serum levels of the drug and its anticoagulant effect should be monitored.
I. Recommendations for Prophylaxis in Non-Orthopedic Surgeries
We now use more objective scores to assess the risk of thromboembolism associated with each type of surgery to better guide prophylaxis. One of these scores that can stratify the risk for venous thromboembolism with greater accuracy is the Caprini risk assessment model.371371 Caprini JA. Thrombosis risk assessment as a guide to quality patient care. Dis Mon. 2005;51(2-3):70-8.,372372 Caprini JA, Arcelus JI, Hasty JH, Tamhane AC, Fabrega F. Clinical assessment of venous thromboembolic risk in surgical patients. Semin Thromb Hemost. 1991;17 Suppl 3:304-12. In this model, a score is assigned to each clinical or laboratory variable (Chart 6). Based on the number of these variables and the score obtained, the categories of risk are defined (very low, low, moderate, and high) according to the risk of VTE (Chart 7).367367 Gould MK, Garcia DA, Wren SM, Karanicolas PJ, Arcelus JI, Heit JA, et al; American College of Chest Physicians. Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e227S-77S. Erratum in: Chest. 2012;141(5):1369.
Caprini risk assessment model:371371 Caprini JA. Thrombosis risk assessment as a guide to quality patient care. Dis Mon. 2005;51(2-3):70-8.,372372 Caprini JA, Arcelus JI, Hasty JH, Tamhane AC, Fabrega F. Clinical assessment of venous thromboembolic risk in surgical patients. Semin Thromb Hemost. 1991;17 Suppl 3:304-12. risk stratification of general, abdominal, pelvic, urological, gynecological, vascular, and plastic and reconstructive surgeries
Venous thromboembolism risk stratification in the absence of mechanical or pharmacological prophylaxis according to Caprini risk score
In addition to the risk of venous thromboembolism, according to risk factors attributed to the condition of the patient or to the surgical procedure, it is important to analyze risk factors for bleeding that may modify the choice of the best thromboprophylaxis. Risk factors for severe bleeding complications are described in chart 8.367367 Gould MK, Garcia DA, Wren SM, Karanicolas PJ, Arcelus JI, Heit JA, et al; American College of Chest Physicians. Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e227S-77S. Erratum in: Chest. 2012;141(5):1369.
A. General Risk Factors
Chart 8 - Risk factors for severe hemorrhagic complications A. General risk factors
I. A. General, Abdominal and Pelvic, Urological, Gynecological, Vascular, and Plastic and Reconstructive Surgeries
Next, we present the recommendations for specific non-orthopedic surgeries. The recommendations are no longer guided by the Caprini risk score, but according to the risk characteristics of each surgery.
II. Recommendations for Prophylaxis for Orthopedic Surgeries
The risk of VTE associated with major orthopedic surgeries (hip and knee prosthesis surgeries and hip fracture surgery) is one of the highest of all surgical specialties. The combined risk of VTE in a postoperative period of 35 days in untreated patients is currently estimated at 4.3%.373373 Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, et al; American College of Chest Physicians. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e278S-325S. Table 3 describes the components of this risk.373373 Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, et al; American College of Chest Physicians. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e278S-325S. Next, we present the recommendations for prophylaxis for VTE in major orthopedic surgeries.
Estimated frequency of symptomatic, nonfatal venous thromboembolism after major orthopedic surgeries
For patients submitted to major orthopedic surgeries, regardless of the possibility of using IPC or duration of treatment, LMWH is preferred compared with other antiplatelet agents suggested as alternatives. When using LMWH, it is suggested to start administration at least 12 hours before surgery or at least 12 hours after the surgical procedure.373373 Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, et al; American College of Chest Physicians. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e278S-325S.
Doses of new anticoagulants in hip and knee prosthesis surgeries (adjust doses in patients with decreased renal function)
Whenever possible, mechanical prophylaxis should be associated with IPC during hospital stay (Class of Recommendation IIa, Level of evidence C). In addition, use of apixaban or dabigatran is preferred for patients rejecting IPC or multiple subcutaneous injections.373373 Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, et al; American College of Chest Physicians. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e278S-325S.
The doses of the new anticoagulants used in the studies for prophylaxis of VTE in major orthopedic surgeries are outlined in chart 9.
D) Anticoagulation Management in the Perioperative Period
The major challenges of anticoagulation management in the perioperative period are the interruption of anticoagulation, which temporarily increases the risk of thromboembolism and its maintenance during invasive procedures, which may increase the risk of hemorrhagic complications. Both challenges increase the risk of death.374374 Douketis JD. Perioperative management of patients who are receiving warfarin therapy: an evidence-based and practical approach. Blood. 2011;117(19):5044-9.
375 Spyropoulos AC, Douketis JD. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood. 2012;120(15):2954-62.
376 Torn M, Rosendaal FR. Oral anticoagulation in surgical procedures: risks and recommendations. Br J Haematol. 2003;123(4):676-82.
377 Kakkar VV, Cohen AT, Edmonson RA, Phillips MJ, Cooper DJ, Das SK, et al. Low molecular weight versus standard heparin for prevention of venous thromboembolism after major abdominal surgery. The Thromboprophylaxis Collaborative Group. Lancet. 1993;341(8840):259-65.
378 Jaffer AK. Perioperative management of warfarin and antiplatelet therapy. Cleve Clin J Med. 2009;76 Suppl 4:S37-44.-379379 Gallego P, Apostolakis S, Lip GY. Bridging evidence-based practice and practice-based evidence in periprocedural anticoagulation. Circulation. 2012;126(13):1573-6.
When assessing perioperative thromboembolic risk, recognizing the different risk situations for thromboembolism is necessary. One of them is the patient receiving anticoagulation for the prevention of venous thromboembolism (VTE). Another risk situation is the patient receiving anticoagulation in the presence of mechanical cardiac prostheses and/or AF for the prevention of arterial thromboembolism. Table 4 presents a proposal for the risk stratification of these patients. High-risk patients are those with >10% annual risk of thromboembolism; moderate risk, 5-10% annual risk of thromboembolism; and low risk, < 5% annual risk of thromboembolism.380380 Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704.
In addition to assessment of thromboembolic risk, we should consider the risk of bleeding that certain surgical procedures present during the use of antithrombotic medications. The risk of bleeding associated with each type of surgical procedure is shown in chart 10.375375 Spyropoulos AC, Douketis JD. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood. 2012;120(15):2954-62. In general, we divided the procedures in those with high risk of severe bleeding in 2 to 4 days (2 to 4%) and those with low risk (0 to 2%). Severe bleeding is generally defined as a bleeding that results in death or is intracranial or requires reoperation to be stagnant or causes a decrease in hemoglobin ≥ 2 g/dL or requires transfusion of ≥ 2 units of red blood cells.381381 Mehran R, Rao SV, Bhatt DL, Gibson CM, Caixeta A, Eikelboom J, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123(23):2736-47.
In addition to assessment of the risk of bleeding based on the type of surgical procedure, there are clinical conditions inherent to each patient that may confer a greater risk of bleeding. There are scores that can quantify the risk of bleeding based on the clinical features of patients undergoing antiplatelet therapy, such as the HAS-BLED score, which is summarized in chart 11.382382 Omran H, Bauersachs R, Rübenacker S, Goss F, Hammerstingl C. The HAS-BLED score predicts bleedings during bridging of chronic oral anticoagulation. Results from the national multicentre BNK Online bRiDging REgistRy (BORDER). Thromb Haemost. 2012;108(1):65-73. A HAS-BLED score ≥ 3 is associated to higher risk of bleeding (HR 11.8, 95% CI 5.6-24.9).
I. Warfarin380380 Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704.,384384 Lorga Filho AM, Azmus AD, Soeiro AM, Quadros AS, Avezum A, Marques AC, et al; Sociedade Brasileira de Cardiologia. [Brazilian guidelines on platelet antiaggregants and anticoagulants in cardiology]. Arq Bras Cardiol. 2013;101(3 Suppl 3):1-95.
Warfarin is a vitamin K antagonist; its anticoagulant effect takes days to disappear (half-life from 36 to 42 hours) and may require similar time to reach adequate levels after surgery. Thus, patients at high risk for thromboembolism may require “bridge therapy” with parenteral antiplatelet agents, such as UFH and subcutaneous LMWHs. These two agents present faster onset and a shorter half-life, which would allow the possibility of suspending warfarin as close to the surgical procedure as possible, minimizing thromboembolic risk as much as possible.
Since the metabolism of warfarin may be influenced by several factors, such as patient age, renal function, and drug interactions, the INR should be measured on the day before surgery to ensure that it is <1.5. If the INR is >1.5, reverse it with oral vitamin K administration (1 to 2 mg) and re-evaluate it the following day.
The decision to suspend or not to suspend warfarin before the surgical procedure will depend on the combined analysis of thromboembolic risk (Table 4), risk of bleeding (Chart 11), and the patient’s own risk.
I. B. Patients with Moderate Risk of Thromboembolism
There is little evidence on the best course of action in patients with moderate risk of thromboembolism regarding whether to use or not to use bridge therapy. Thus, the choice should be based on the individual characteristics of each patient and the proposed surgery. Whether the patient requires bridge therapy is decided by the attending physician.
I. D. Urgent or Emergency Procedures385385 Machado FS. Perioperatório do paciente em uso de anticoagulante. In: Machado FS, Martins MA, Caramelli B. (editores). Perioperatório: procedimentos clínicos: Sarvier; 2004. p. 105-9.
The therapeutic measures used for the reversal of oral anticoagulation with warfarin will depend on how quickly normalization of prothrombin time, measured by the INR, is reached. For surgeries that can wait 18-24 hours, suspension of warfarin associated with intravenous vitamin K1 at a dose of 2.5-5 mg usually normalizes the INR when it is within the therapeutic range.380380 Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704.
If rapid normalization of INR is needed, it is necessary to replace the deficient coagulation factors with fresh frozen plasma (FFP) and prothrombin complex concentrate. The Resolution - RDC No. 10 of January 23, 2004 from the Brazillian Health Regulatory Agency (ANVISA) states that “for the correction of hemorrhage due to coumarin antiplatelet agents or rapid reversal of the effects of coumarins”, the product of choice is the prothrombin complex. As this type of concentrate is not yet broadly available in Brazilian hospitals, the use of FFP is an acceptable alternative.386386 Ministério da Saúde. Agência Nacional de Vigilância Sanitária (ANVISA). RDC nº10, de 23 de janeiro de 2004. Diretrizes para o uso de plasma fresco congelado PFC e plasma virus inativo. Diário Oficial da União, Poder Executivo, Brasília (DF) de 26 de janeiro de 2004. [Citado em 2004 jan 10]. Disponível em: http://pegasus.fmrp.usp.br/projeto/legislacao/rdc%2010%20e%2023%2001%2004.pdf
http://pegasus.fmrp.usp.br/projeto/legis...
For the FFP, the recommended dose is 15 mL/kg of body weight and volume overload should be avoided.387387 O'Shaughnessy DF, Atterbury C, Bolton Maggs P, Murphy M, Thomas D, Yates S, et al; British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol. 2004;126(1):11-28. No standard procedure has been established for the prothrombin concentrate. Table 5 shows the doses used in health services in the United Kingdom. However, regardless of what is used to replace vitamin K-dependent factors, using vitamin K1 (2.5-5.0 mg, oral or slow venous administration) is necessary to maintain normal prothrombin values during the preoperative period.380380 Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704.
Dose of prothrombin complex concentrate to be administered for reversal of anticoagulation according to the INR
II. Dabigatran375375 Spyropoulos AC, Douketis JD. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood. 2012;120(15):2954-62.,384384 Lorga Filho AM, Azmus AD, Soeiro AM, Quadros AS, Avezum A, Marques AC, et al; Sociedade Brasileira de Cardiologia. [Brazilian guidelines on platelet antiaggregants and anticoagulants in cardiology]. Arq Bras Cardiol. 2013;101(3 Suppl 3):1-95.,388388 Schulman S, Crowther MA. How I treat with anticoagulants in 2012: new and old anticoagulants, and when and how to switch. Blood. 2012;119(13):3016-23.
389 Lai A, Davidson N, Galloway SW, Thachil J. Perioperative management of patients on new oral anticoagulants. Br J Surg. 2014;101(7):742-9. Erratum in: Br J Surg. 2014;101(12):1624.
390 Stangier J, Rathgen K, Stähle H, Gansser D, Roth W. The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects. Br J Clin Pharmacol. 2007;64(3):292-303.-391391 Fonseca NM, Alves RR, Pontes JP; Sociedade Brasileira de Anestesiologia. SBA recommendations for regional anesthesia safety in patients taking anticoagulants. Braz J Anesthesiol. 2014;64(1):1-15.
Dabigatran is an anticoagulant drug that acts as a direct inhibitor of thrombin, reversibly blocking the conversion of fibrinogen to fibrin (factor IIa). It is a drug that acts rapidly. Its concentration peaks after 30-120 minutes. Dabigatran has a half-life of 12-17 hours and is predominantly renally excreted (80%).
This drug is approved for preventing stroke in patients with non-valvular AF, in the treatment of VTE (DVT/PE), and for the prevention of recurrent VTE and VTE in major orthopedic surgeries. However, its use is not authorized for the prevention of arterial thromboembolism in patients with mechanical valve prostheses. Because of its rapid action and shorter half-life, there is no need for bridge therapy associated with this drug.
One of the concerns associated with the use of dabigatran is the lack of specific antidotes until recently. The available possibilities were limited to the use of the prothrombin complex and hemodialysis, which had limited success. The first antidote for thrombin inhibitors (dabigatran), the idarucizumab, was FDA approved in the USA in October 2015. Idarucizumab completely reversed the anticoagulant effect of dabigatran in phase I and phase III studies. Another promising agent under study is Arapazine (PER-977), which has been shown to reverse the anticoagulant action of dabigatran, as well as rivaroxaban, apixaban, and LMWH.392392 Tummala R, Kavtaradze A, Gupta A, Ghosh RK. Specific antidotes against direct oral anticoagulants: a comprehensive review of clinical trials data. Int J Cardiol. 2016;214:292-8.
III. Rivaroxaban375375 Spyropoulos AC, Douketis JD. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood. 2012;120(15):2954-62.,384384 Lorga Filho AM, Azmus AD, Soeiro AM, Quadros AS, Avezum A, Marques AC, et al; Sociedade Brasileira de Cardiologia. [Brazilian guidelines on platelet antiaggregants and anticoagulants in cardiology]. Arq Bras Cardiol. 2013;101(3 Suppl 3):1-95.,388388 Schulman S, Crowther MA. How I treat with anticoagulants in 2012: new and old anticoagulants, and when and how to switch. Blood. 2012;119(13):3016-23.,389389 Lai A, Davidson N, Galloway SW, Thachil J. Perioperative management of patients on new oral anticoagulants. Br J Surg. 2014;101(7):742-9. Erratum in: Br J Surg. 2014;101(12):1624.,391391 Fonseca NM, Alves RR, Pontes JP; Sociedade Brasileira de Anestesiologia. SBA recommendations for regional anesthesia safety in patients taking anticoagulants. Braz J Anesthesiol. 2014;64(1):1-15.
Rivaroxaban is a drug that acts as a factor Xa inhibitor, blocking its enzymatic function of converting prothrombin to thrombin. It is also a fast-acting substance. Its concentration peaks after 2-4 hours and has a short half-life (5-9 hours in young people and 11-13 hours in the elderly). This drug undergoes liver metabolism and renal excretion (66%).
Rivaroxaban is approved for the prevention of stroke in patients with non-valvular AF, in the treatment of VTE (DVT/PE), in the prevention of recurrent VTE, and in the prevention of VTE in major orthopedic surgeries. However, its use is not authorized for the prevention of arterial thromboembolism in patients with mechanical valve prostheses. Since it is fast-acting and has a shorter half-life, there is no need for bridge therapy associated with this drug.
In the past, only the prothrombin complex was available to reverse the effect of rivaroxaban since there were no specific antidotes available. Currently, Andexanet alfa (PRT064445) is a specific antidote against factor Xa inhibitors. It shows a rapid reversal of the anticoagulant effect of apixaban and rivaroxaban in minutes, as observed in two recent parallel phase III studies, ANEXA-A and ANEEXA-R, respectively. Currently, ANNEXA-4, a phase IV study, is being performed. Another promising agent under study is Arapazine (PER-977), which shows an effect in reversing the anticoagulant action of dabigatran, as well as rivaroxaban, apixaban, and LMWH.392392 Tummala R, Kavtaradze A, Gupta A, Ghosh RK. Specific antidotes against direct oral anticoagulants: a comprehensive review of clinical trials data. Int J Cardiol. 2016;214:292-8.
IV. Apixaban375375 Spyropoulos AC, Douketis JD. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood. 2012;120(15):2954-62.,388388 Schulman S, Crowther MA. How I treat with anticoagulants in 2012: new and old anticoagulants, and when and how to switch. Blood. 2012;119(13):3016-23.,389389 Lai A, Davidson N, Galloway SW, Thachil J. Perioperative management of patients on new oral anticoagulants. Br J Surg. 2014;101(7):742-9. Erratum in: Br J Surg. 2014;101(12):1624.,391391 Fonseca NM, Alves RR, Pontes JP; Sociedade Brasileira de Anestesiologia. SBA recommendations for regional anesthesia safety in patients taking anticoagulants. Braz J Anesthesiol. 2014;64(1):1-15.
Apixaban is also a factor Xa inhibitor that blocks the conversion of prothrombin to thrombin. It has a rapid onset of action. Its concentration peaks after 3 hours and has a short half-life (8-15 hours). This drug undergoes liver metabolism and renal (27%) and fecal excretion. Apixaban is approved for the prevention of stroke in patients with non-valvular AF, prevention of VTE in major orthopedic surgeries, and treatment of DVT and PE. Its use is not authorized for the prevention of arterial thromboembolism in patients with mechanical valve prostheses. Due to its rapid onset of action and shorter half-life, there is no need for bridge therapy associated with this drug.
Currently, Andexanet alfa (PRT064445) is the specific antidote against factor Xa inhibitors. It shows a rapid reversal of the anticoagulant effect of apixaban and rivaroxaban in minutes, as observed in two recent parallel phase III studies, ANNEXA-A and ANEEXA-R, respectively. A phase IV study, ANNEXA-4, is underway. Another promising agent under study is Arapazine (PER-977), which shows an effect in reversing the anticoagulant action of dabigatran, as well as rivaroxaban, apixaban, and LMWH.392392 Tummala R, Kavtaradze A, Gupta A, Ghosh RK. Specific antidotes against direct oral anticoagulants: a comprehensive review of clinical trials data. Int J Cardiol. 2016;214:292-8.
V. Edoxaban393393 Zalpour A, Oo TH. Update on edoxaban for the prevention and treatment of thromboembolism: clinical applications based on current evidence. Adv Hematol. 2015;2015:920361.
Edoxaban is also a factor Xa inhibitor. It has a rapid onset of action. Its concentration peaks in 1-2 hours. This drug has a short half-life (10-14 hours) and undergoes renal (50%) and biliary and intestinal (50%) excretion. Edoxaban is indicated for the prevention of arterial thromboembolic phenomena in patients with non-valvular AF and in the treatment of DVT or PE, but it has not yet been released in Brazil.
At present, there are no studies investigating specific antidotes for edoxaban. An option would be to use the prothrombin complex for the occurrence of bleeding that necessitates the reversal of its effect. Because it is the newest oral anticoagulant, studies evaluating its use in the perioperative period are very limited.
In principle, the most accepted approach is interruption of edoxaban 24 hours before surgeries with low risk of bleeding and interruption 48-72 hours before surgeries associated with high risk of bleeding (Chart 10).
E) Prophylaxis of Infective Endocarditis
Despite advances in health care, infective endocarditis remains a disease of high morbidity and mortality.394394 Bin Abdulhak AA, Baddour LM, Erwin PJ, Hoen B, Chu VH, Mensah GA, et al. Global and regional burden of infective endocarditis, 1990-2010: a systematic review of the literature. Glob Heart. 2014;9(1):131-43.,395395 Werdan K, Dietz S, Löffler B, Niemann S, Bushnaq H, Silber RE, et al. Mechanisms of infective endocarditis: pathogen-host interaction and risk states. Nat Rev Cardiol. 2014;11(1):35-50. In the last decades, we have witnessed major debates on which strategies are truly effective in reducing its prevalence.
The main cause for the occurrence of endocarditis is endothelial lesion due to cardiac anatomic predisposition. Consequently, there is deposition of platelets and fibrin in the endocardium, generating non-bacterial thrombotic endocarditis. The presence of circulating microorganisms in the bloodstream may result in infective endocarditis. Other predisposing factors are the presence of vascular devices and/or infectious agent of high virulence. These can cause the disease even in individuals with a structurally normal heart.395395 Werdan K, Dietz S, Löffler B, Niemann S, Bushnaq H, Silber RE, et al. Mechanisms of infective endocarditis: pathogen-host interaction and risk states. Nat Rev Cardiol. 2014;11(1):35-50. Bacteria are the most common etiological agents. Thus, several studies have evaluated the risk of spontaneous bacteremia related to routine activities and invasive procedures.
I. Dental Procedures
Early studies correlated dental extraction with the presence of transient bacteremia.396396 Overholser CD, Moreillon P, Glauser MP. Experimental bacterial endocarditis after dental extractions in rats with periodontitis. J Infect Dis. 1987;155(1):107-12.,397397 Okell CC, Elliott SD. Bacteraemia and oral sepsis with special reference to the aetiology of subacute endocarditis. Lancet. 1935;2:869-72. Others indicated that endodontic and periodontal manipulation may lead to similar levels of bacteremia.398398 Beechen II, Laston DJ, Garbarino VE. Transitory bacteraemia as related to the operation of vital pulpotomy. Oral Surg Oral Med Oral Path. 1956;8(9):902-5.
399 Bender IB, Seltzer S, Yermish M. The incidence of bacteremia in endodontic manipulation: preliminary report. 1960. J Endod. 2003;29(11):697-700.-400400 Forner L, Larsen T, Kilian M, Holmstrup P. Incidence of bacteremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J Clin Periodontol. 2006;33(6):401-7. Based on this, experimental animal models confirmed the reduction of bacteremia after dental manipulation with the use of prophylactic antibiotic therapy.401401 Glauser MP, Bernard JP, Moreillon P, Francioli P. Successful single-dose amoxicillin prophylaxis against experimental streptococcal endocarditis: evidence for two mechanisms of protection. J Infect Dis. 1983;147(3):568-75.,402402 Shanson DC, Akash S, Harris M, Tadayon M. Erythromycin stearate, 1.5 g, for the oral prophylaxis of streptococcal bacteraemia in patients undergoing dental extraction: efficacy and tolerance. J Antimicrob Chemother. 1985;15(1):83-90. Since then, this recommendation has been established for individuals with an anatomical predisposition to endocarditis.
More recently, the impact of prophylaxis on the prevention of endocarditis has been questioned. Clinical trials showed a low prevalence of infectious endocarditis (IE) presumably related to dental treatments, ranging from 2.7 to 13%.403403 Van der Meer JT, Van Wijk W, Thompson J, Vandenbroucke JP, Valkenburg HA, Michel MF. Efficacy of antibiotic prophylaxis for prevention of native-valve endocarditis. Lancet. 1992;339(8786):135-9.
404 Strom BL, Abrutyn E, Berlin JA, Kinman JL, Feldman RS, Stolley PD, et al. Dental and cardiac risk factors for infective endocarditis. A population-based, case-control study. Ann Intern Med. 1998;129(10):761-9.-405405 Duval X, Alla F, Hoen B, Danielou F, Larrieu S, Delahaye F, et al. Estimated risk of endocarditis in adults with predisposing cardiac conditions undergoing dental procedures with or without antibiotic prophylaxis. Clin Infect Dis. 2006;42(12):e102-7. Moreover, it has been shown that daily activities, such as mastication, tooth brushing, and flossing are related to transient bacteremia.400400 Forner L, Larsen T, Kilian M, Holmstrup P. Incidence of bacteremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J Clin Periodontol. 2006;33(6):401-7.,406406 Roberts GJ. Dentists are innocent! "Everyday" bacteremia is the real culprit: a review and assessment of the evidence that dental surgical procedures are a principal cause of bacterial endocarditis in children. Pediatr Cardiol. 1999;20(5):317-25.
407 Lucas V, Roberts GJ. Odontogenic bacteremia following tooth cleaning procedures in children. Pediatr Dent. 2000;22(2):96-100.
408 Seymour RA, Lowry R, Whitworth JM, Martin MV. Infective endocarditis, dentistry and antibiotic prophylaxis; time for a rethink? Br Dent J. 2000;189(11):610-6.-409409 Lockhart PB, Brennan MT, Sasser HC, Fox PC, Paster BJ, Bahrani-Mougeot FK. Bacteremia associated with toothbrushing and dental extraction. Circulation. 2008;117(24):3118-25. Other arguments against the use of prophylaxis are risk of anaphylaxis associated with the use of penicillin, efficacy proven only in experimental studies, and possibility of induction of bacterial resistance.408408 Seymour RA, Lowry R, Whitworth JM, Martin MV. Infective endocarditis, dentistry and antibiotic prophylaxis; time for a rethink? Br Dent J. 2000;189(11):610-6.,410410 Lee P, Shanson D. Results of a UK survey of fatal anaphylaxis after oral amoxicillin. J Antimicrob Chemother. 2007;60(5):1172-3.
Based on these arguments, the recommendation not to use prophylaxis for endocarditis has been instituted in the United Kingdom by the National Institute for Health and Clinical Excellence (NICE) since 2008.411411 Prophylaxis against infective endocarditis: antimicrobial prophylaxis against infective endocarditis in adults and children undergoing interventional procedures (CG64). National Institute for Health and Care Excellence (NICE) http://wwwniceorguk/guidance/CG64 [Internet].
http://wwwniceorguk/guidance/CG64...
In France, prophylaxis has been recommended for high-risk individuals only since 2002.412412 Danchin N, Duval X, Leport C. Prophylaxis of infective endocarditis: French recommendations 2002. Heart. 2005;91(6):715-8. The same recommendation has been made by the American Heart Association (AHA) since 2007413413 Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M, et al; American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee; American Heart Association Council on Cardiovascular Disease in the Young; American Heart Association Council on Clinical Cardiology; American Heart Association Council on Cardiovascular Surgery and Anesthesia; Quality of Care and Outcomes Research Interdisciplinary Working Group. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116(15):1736-54. Erratum in: Circulation. 2007;116(15):e376-7. and the European Society of Cardiology (ESC) since 2009.414414 Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075-128. The population considered to be at high risk is composed of individuals with a greater chance of developing complications and die due to illness (severe IE risk conditions). The individuals described in chart 12 are considered at risk of IE.413413 Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M, et al; American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee; American Heart Association Council on Cardiovascular Disease in the Young; American Heart Association Council on Clinical Cardiology; American Heart Association Council on Cardiovascular Surgery and Anesthesia; Quality of Care and Outcomes Research Interdisciplinary Working Group. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116(15):1736-54. Erratum in: Circulation. 2007;116(15):e376-7.,414414 Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075-128.
Recent observational studies have shown no increase in the number of endocarditis following recommendations for prophylaxis in high-risk individuals in France and the United States.415415 Duval X, Delahaye F, Alla F, Tattevin P, Obadia JF, Le Moing V, et al; AEPEI Study Group. Temporal trends in infective endocarditis in the context of prophylaxis guideline modifications: three successive population-based surveys. J Am Coll Cardiol. 2012;59(22):1968-76.
416 Desimone DC, Tleyjeh IM, Correa de Sa DD, Anavekar NS, Lahr BD, Sohail MR, et al; Mayo Cardiovascular Infections Study Group. Incidence of infective endocarditis caused by viridans group streptococci before and after publication of the 2007 American Heart Association's endocarditis prevention guidelines. Circulation. 2012;126(1):60-4.-417417 Pasquali SK, He X, Mohamad Z, McCrindle BW, Newburger JW, Li JS, et al. Trends in endocarditis hospitalizations at US children's hospitals: impact of the 2007 American Heart Association Antibiotic Prophylaxis Guidelines. Am Heart J. 2012;163(5):894-9. However, an observational study in the United Kingdom showed an increase in the incidence of infective endocarditis since the NICE recommendations in 2008.418418 Dayer MJ, Jones S, Prendergast B, Baddour LM, Lockhart PB, Thornhill MH. Incidence of infective endocarditis in England, 2000-13: a secular trend, interrupted time-series analysis. Lancet. 2015;385(9974):1219-28. In this country, a study performed in 2012 revealed that most cardiologists and cardiac surgeons believed that prophylaxis should be performed in cases of valve prosthesis and previous endocarditis.419419 Dayer MJ, Chambers JB, Prendergast B, Sandoe JA, Thornhill MH. NICE guidance on antibiotic prophylaxis to prevent infective endocarditis: a survey of clinicians' attitudes. QJM. 2013;106(3):237-43. In the USA, following the new AHA recommendations in 2007, one study showed an increase in the incidence of hospitalizations for streptococcal endocarditis.420420 Pant S, Patel NJ, Deshmukh A, Golwala H, Patel N, Badheka A, et al. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J Am Coll Cardiol. 2015;65(19):2070-6. On the other hand, the limitations imposed on observational cohorts should be considered.
Considering that most patients with valvular heart disease in Brazil present characteristics different from those currently observed in the USA and European countries (young people with rheumatic sequelae and higher lethality due to endocarditis) and the lack of prophylaxis studies in Brazil, prophylaxis is recommended for patients with native valve injury, although they do not have a valve prosthesis. Another difference of our population compared to the American and European populations is the higher prevalence of individuals with low access to health care and therefore with lower dental hygiene and higher risk of bacteremia after invasive dental procedures.400400 Forner L, Larsen T, Kilian M, Holmstrup P. Incidence of bacteremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J Clin Periodontol. 2006;33(6):401-7.,421421 Strom BL, Abrutyn E, Berlin JA, Kinman JL, Feldman RS, Stolley PD, et al. Risk factors for infective endocarditis: oral hygiene and nondental exposures. Circulation. 2000;102(23):2842-8.
Although cited in the international literature, a significant adverse effect of antimicrobial therapy is a rare event. Therefore, use of prophylaxis for endocarditis is recommended prior to dental procedures involving the manipulation of gingival tissue, periodontal region, or oral mucosa perforation (Chart 13) for all individuals with anatomically relevant valve disease (Chart 12). The antibiotic should be given as a single dose 30-60 minutes before the procedure (Table 6).
It should be noted that infective endocarditis is a more frequent result of bacteremia from daily activities than after dental procedures. There is no doubt that maintaining good oral health is the best strategy to prevent endocarditis. In individuals with periodontal and endodontic diseases, the incidence and magnitude of bacteremia in daily care and during procedures are higher compared to individuals with healthy teeth.421421 Strom BL, Abrutyn E, Berlin JA, Kinman JL, Feldman RS, Stolley PD, et al. Risk factors for infective endocarditis: oral hygiene and nondental exposures. Circulation. 2000;102(23):2842-8. Thus, we recommend emphasizing daily dental care and biannual dental evaluation.
II. Respiratory Tract Procedures
Patients submitted to an incision or biopsy of the respiratory tract mucosa, such as otorhinolaryngological surgeries, should receive an antibiotic treatment scheme similar to the one used before dental treatment with high risk of bacteremia. There is no recommendation for prophylaxis for bronchoscopy, laryngoscopy, and orotracheal intubation. For infection treatments, such as abscess drainage, antibiotic prophylaxis with antistreptococcal action should also be administered.414414 Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075-128.
Recommendations for Prophylaxis of Infectious Endocarditis before Genitourinary and Gastrointestinal Tract Procedures
III. Genitourinary and Gastrointestinal Tract Procedures
Despite limited evidence, it is believed that patients at high risk for infective endocarditis (Chart 12) would probably benefit from prophylaxis before genitourinary or gastrointestinal procedures. Patients with non-high-risk valvular heart disease may also benefit from prophylaxis before these procedures (Chart 12). The recommended antibiotic treatment scheme for this group is in table 7.
IV. Dermatological and Skeletal Muscle Procedures
For treatment of infections, such as abscess drainage, antibiotic prophylaxis should be administered with antistaphylococcal and antistreptococcal action.414414 Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075-128.
V. Piercing and Tattooing
The number of reports of infective endocarditis related to piercing and tattooing has increased, mainly associated with tongue piercing, but the risk was not estimated.422422 Yu CH, Minnema BJ, Gold WL. Bacterial infections complicating tongue piercing. Can J Infect Dis Med Microbiol. 2010;21(1):e70-4. Therefore, patients should be warned about this risk.
F) Surveillance for Cardiovascular Complications
Early detection of cardiovascular events is critical to reduce mortality after noncardiac surgeries. MI can occur in the absence of chest pain and is thus necessary to develop monitoring strategies for its diagnosis.
ST-segment monitoring, serial 12-lead ECG, and measurement of cardiac troponin levels are methods used to monitor complications. Studies evaluating the use of continuous ST-segment monitoring have shown that this method has a large sensitivity (between 55 and 100%) and specificity (between 37 and 85%) range for the detection of perioperative ischemia (intra- and postoperatively) because its effectiveness depends on the technique used and the baseline features of the population.423423 Landesberg G, Mosseri M, Wolf Y, Vesselov Y, Weissman C. Perioperative myocardial ischemia and infarction: identification by continuous 12-lead electrocardiogram with online ST-segment monitoring. Anesthesiology. 2002;96(2):264-70.
424 Landesberg G. Monitoring for myocardial ischemia. Best Pract Res Clin Anaesthesiol. 2005;19(1):77-95.
425 Raby KE, Barry J, Creager MA, Cook EF, Weisberg MC, Goldman L. Detection and significance of intraoperative and postoperative myocardial ischemia in peripheral vascular surgery. JAMA. 1992;268(2):222-7.-426426 Zakowski MI, Ramanathan S, Baratta JB, Cziner D, Goldstein MJ, Kronzon I, et al. Electrocardiographic changes during cesarean section: a cause for concern? Anesth Analg. 1993;76(1):162-7. The occurrence of postoperative ischemia detected with continuous monitoring in patients submitted to vascular surgeries has prognostic implication and is an independent predictor of long-term cardiovascular events.427427 Mangano DT, Browner WS, Hollenberg M, Li J, Tateo IM. Long-term cardiac prognosis following noncardiac surgery. The Study of Perioperative Ischemia Research Group. JAMA. 1992;268(2):233-9.,428428 Landesberg G, Shatz V, Akopnik I, Wolf YG, Mayer M, Berlatzky Y, et al. Association of cardiac troponin, CK-MB, and postoperative myocardial ischemia with long-term survival after major vascular surgery. J Am Coll Cardiol. 2003;42(9):1547-54. However, since measurement of perioperative troponin levels (a simpler test) became available, the use of automatic monitoring for diagnosis and prognosis of perioperative myocardial ischemia has been discontinued. It has not been studied further and is therefore not recommended.
In the absence of electrocardiographic changes or clinical condition suggestive of ischemia or echocardiographic changes compatible with MI, increases in conventional troponin levels following noncardiac surgeries is associated with a higher rate of cardiovascular events in the short and long term, as shown in several studies.428428 Landesberg G, Shatz V, Akopnik I, Wolf YG, Mayer M, Berlatzky Y, et al. Association of cardiac troponin, CK-MB, and postoperative myocardial ischemia with long-term survival after major vascular surgery. J Am Coll Cardiol. 2003;42(9):1547-54.
429 Lopez-Jimenez F, Goldman L, Sacks DB, Thomas EJ, Johnson PA, Cook EF, et al. Prognostic value of cardiac troponin T after noncardiac surgery: 6-month follow-up data. J Am Coll Cardiol. 1997;29(6):1241-5.
430 Bursi F, Babuin L, Barbieri A, Politi L, Zennaro M, Grimaldi T, et al. Vascular surgery patients: perioperative and long-term risk according to the ACC/AHA guidelines, the additive role of post-operative troponin elevation. Eur Heart J. 2005;26(22):2448-56.
431 Barbagallo M, Casati A, Spadini E, Bertolizio G, Kepgang L, Tecchio T, et al. Early increases in cardiac troponin levels after major vascular surgery is associated with an increased frequency of delayed cardiac complications. J Clin Anesth. 2006;18(4):280-5.
432 Winkel TA, Schouten O, van Kuijk JP, Verhagen HJ, Bax JJ, Poldermans D. Perioperative asymptomatic cardiac damage after endovascular abdominal aneurysm repair is associated with poor long-term outcome. J Vasc Surg. 2009;50(4):749-54. Erratum in: J Vasc Surg. 2010;51(1):289.-433433 Kim LJ, Martinez EA, Faraday N, Dorman T, Fleisher LA, Perler BA, et al. Cardiac troponin I predicts short-term mortality in vascular surgery patients. Circulation. 2002;106(18):2366-71. In a meta-analysis of patients submitted to vascular surgeries in 2011, the authors demonstrated that increases in TnI levels postoperatively without MI features was a mortality predictor in a period of 30 days, with a mortality rate of 11.6%. Patients with normal troponin levels and patients with MI had mortality rates of 2.3% and 21.6%, respectively.434434 Redfern G, Rodseth RN, Biccard BM. Outcomes in vascular surgical patients with isolated postoperative troponin leak: a meta-analysis. Anaesthesia. 2011;66(7):604-10. In 2012, in the VISION study involving 15,133 patients, the authors demonstrated a significant association between the peak of fourth-generation troponin T (TnT) and mortality rate in a period of 30 days.305305 Devereaux PJ, Chan MT, Alonso-Coello P, Walsh M, Berwanger O, Villar JC, et al; Vascular Events In Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA. 2012;307(21):2295-304. Erratum in: JAMA. 2012;307(24):2590. Although there is no sufficient evidence regarding the best strategy to manage cases of increase in troponin levels, we recommend performing a non-invasive or invasive complementary investigation with cardiac risk stratification based on the specific evaluation of the cardiologist before hospital discharge.
The use of hs-Tn kits significantly improved the accuracy to rapidly confirm or exclude diagnosis of MI in patients with chest pain in the emergency room.100100 Lipinski MJ, Baker NC, Escárcega RO, Torguson R, Chen F, Aldous SJ, et al. Comparison of conventional and high-sensitivity troponin in patients with chest pain: a collaborative meta-analysis. Am Heart J. 2015;169(1):6-16.e6.,435435 Reichlin T, Hochholzer W, Bassetti S, Steuer S, Stelzig C, Hartwiger S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361(9):858-67. However, its interpretation is still a challenge in the perioperative period. Since 2011, observational studies have evaluated the behavior of hs-TnT in the postoperative period. The studies found an increase of hs-TnT levels above the 99th percentile (14 ng/L) in 45-60% of patients after noncardiac surgeries.103103 Nagele P, Brown F, Gage BF, Gibson DW, Miller JP, Jaffe AS, et al. High-sensitivity cardiac troponin T in prediction and diagnosis of myocardial infarction and long-term mortality after noncardiac surgery. Am Heart J. 2013;166(2):325-32.e1.,104104 Gillmann HJ, Meinders A, Grosshennig A, Larmann J, Bünte C, Calmer S, et al. Perioperative levels and changes of high-sensitivity troponin T are associated with cardiovascular events in vascular surgery patients. Crit Care Med. 2014;42(6):1498-506.,106106 Kavsak PA, Walsh M, Srinathan S, Thorlacius L, Buse GL, Botto F, et al. High sensitivity troponin T concentrations in patients undergoing noncardiac surgery: a prospective cohort study. Clin Biochem. 2011;44(12):1021-4.,107107 Alcock RF, Kouzios D, Naoum C, Hillis GS, Brieger DB. Perioperative myocardial necrosis in patients at high cardiovascular risk undergoing elective non-cardiac surgery. Heart. 2012;98(10):792-8. In some studies, this increase is related to mortality in the long term.103103 Nagele P, Brown F, Gage BF, Gibson DW, Miller JP, Jaffe AS, et al. High-sensitivity cardiac troponin T in prediction and diagnosis of myocardial infarction and long-term mortality after noncardiac surgery. Am Heart J. 2013;166(2):325-32.e1. Recently, a study correlated the increase of hs-TnT with noncardiac complications in a period of 30 days after abdominal surgeries.436436 Noordzij PG, van Geffen O, Dijkstra IM, Boerma D, Meinders AJ, Rettig TC, et al. High-sensitive cardiac troponin T measurements in prediction of non-cardiac complications after major abdominal surgery. Br J Anaesth. 2015;114(6):909-18.
Only one study with 135 patients investigated the hs-TnI in the perioperative period. The authors observed a correlation between increases in hs-TnI levels and mortality.437437 Lee GR, Jhanji S, Tarrant H, James S, Pearse RM, Fitzgibbon M. Peri-operative troponin monitoring using a prototype high-sensitivity cardiac troponin I (hs-cTnI) assay: comparisons with hs-cTnT and contemporary cTnI assays. Ann Clin Biochem. 2014;51(Pt 2):258-68. To date, the relevance of isolated increases in hs-Tn levels in the postoperative period remains uncertain. Several conditions may be related to a baseline (chronic) increase in hs-Tn, such as advanced age, HF, CAD, valve diseases, chronic renal failure, or other chronic noncardiac diseases. Therefore, hs-Tn should be dosed preoperatively to determine its baseline value (see item 3.E.I). Even so, no reference value has been established for the value of the variation (delta) that correlates with cardiovascular events or mortality.438438 Gualandro DM, Puelacher C, Mueller C. High-sensitivity cardiac troponin in acute conditions. Curr Opin Crit Care. 2014;20(5):472-7. Whether an increase in perioperative hs-TnT is related only to general mortality or cardiovascular events is difficult to differentiate. Thus, it is harder in clinical practice to determine whether performing additional cardiovascular risk stratification measures will improve the prognosis of the patients.
On the other hand, whenever the patient shows increased troponin levels alone, alternative diagnoses that may lead to increases in troponin and are frequent in the perioperative period, such as pulmonary thromboembolism (PTE), acute pericarditis, decompensated HF, arrhythmias, myocarditis, sepsis, shock, or renal failure, should be avoided.439439 Roongsritong C, Warraich I, Bradley C. Common causes of troponin elevations in the absence of acute myocardial infarction: incidence and clinical significance. Chest. 2004;125(5):1877-84. We recommend the use of the flowchart shown in figure 2 for the evaluation of patients with hs-Tn levels above the 99th percentile after surgery.
Most cardiovascular events occur until the third postoperative day. The use of serial 12-lead ECG during this period is a simple and effective method for detecting events. In a study involving 3,564 patients more than 50 years old, detection of ischemia using postoperative ECG is an independent predictor of cardiovascular events. However, a negative ECG for ischemia does not reduce the risk of events.440440 Rinfret S, Goldman L, Polanczyk CA, Cook EF, Lee TH. Value of immediate postoperative electrocardiogram to update risk stratification after major noncardiac surgery. Am J Cardiol. 2004;94(8):1017-22. In another study comparing serial ECG with 3-lead Holter in 55 patients submitted to vascular surgeries, the ECG is as effective as the Holter for detecting myocardial ischemia.441441 Böttiger BW, Motsch J, Teschendorf P, Rehmert GC, Gust R, Zorn M, et al. Postoperative 12-lead ECG predicts peri-operative myocardial ischaemia associated with myocardial cell damage. Anaesthesia. 2004;59(11):1083-90. Troponin dosage associated with serial ECG until the third postoperative period is the best strategy for the diagnosis of MI.442442 Martinez EA, Nass CM, Jermyn RM, Rosenbaum SH, Akhtar S, Chan DW, et al. Intermittent cardiac troponin-I screening is an effective means of surveillance for a perioperative myocardial infarction. J Cardiothorac Vasc Anesth. 2005;19(5):577-82. Notably, these ECG studies were performed before the availability of highly sensitive troponins.
8. Diagnosis and Treatment of Cardiovascular Complications in the Perioperative Period
A) Acute Coronary Syndromes in the Perioperative
MI is the most feared cardiac complication in the perioperative period, occurring in 0.3-3% of low-risk patients with no history of CAD and reaching 33% in high-risk patients with a history of CAD.6969 Gualandro DM, Calderaro D, Yu PC, Caramelli B. Acute myocardial infarction after noncardiac surgery. Arq Bras Cardiol. 2012;99(5):1060-7. MI shows high mortality rates (40-50%),443443 Becker RC, Underwood DA. Myocardial infarction in patients undergoing noncardiac surgery. Cleve Clin J Med. 1987;54(1):25-8. probably related to the existence of comorbidities, diagnostic difficulty, and limitations to use of antithrombotic and antiplatelet drugs. About 50% of perioperative MI is due to instability of atherosclerosis plaques, and the remainder is due to imbalances between supply and consumption of oxygen,6868 Gualandro DM, Campos CA, Calderaro D, Yu PC, Marques AC, Pastana AF, et al. Coronary plaque rupture in patients with myocardial infarction after noncardiac surgery: frequent and dangerous. Atherosclerosis. 2012;222(1):191-5. which should be considered not only in acute treatment but also in the establishment of prevention strategies.
Although clinical consequences of perioperative MI are extremely serious, diagnosis is often not obvious and requires a high degree of clinical suspicion. Most perioperative ischemic events occur within the first three days after the surgical procedure. The classic clinical feature of precordial pain is absent in more than half of the patients,6868 Gualandro DM, Campos CA, Calderaro D, Yu PC, Marques AC, Pastana AF, et al. Coronary plaque rupture in patients with myocardial infarction after noncardiac surgery: frequent and dangerous. Atherosclerosis. 2012;222(1):191-5.,6969 Gualandro DM, Calderaro D, Yu PC, Caramelli B. Acute myocardial infarction after noncardiac surgery. Arq Bras Cardiol. 2012;99(5):1060-7.,444444 Devereaux PJ, Xavier D, Pogue J, Guyatt G, Sigamani A, Garutti I, et al; POISE (PeriOperative ISchemic Evaluation) Investigators. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: a cohort study. Ann Intern Med. 2011;154(8):523-8. which is partially explained by the residual effect of analgesics or sedatives used in that period. In addition, when chest pain is present, it is often attributed to other more obvious etiologies, such as incisional pain or position of the patient. Other manifestations, such as dyspnea and nausea, have alternative explanations in this period (atelectasis, medication effect). Thus, perioperative MI is frequently undervalued by the medical team. Since it is difficult to interpret the clinical findings, analysis of complementary tests is fundamental for the diagnosis of perioperative myocardial ischemia. Among these, the ECG, the markers of myocardial necrosis, and the transthoracic echocardiogram should be considered.
Regarding the analysis of ECG, ischemic alterations should be distinguished from other causes of ECG alterations, such as electrolytic imbalances, hypothermia, drug effects, and incorrect positioning of the leads. Evolutionary pattern should also be considered in the analysis of ECG. It is important to compare the changes in the traces before and after the event.
Among the markers of myocardial necrosis, troponin is undoubtedly the most used due to its high sensitivity and specificity in the diagnosis of myocardial injury. However, this marker is increased in other situations of myocardial injury, in addition to the one caused by obstructive coronary disease. Other complications commonly present in the postoperative period of noncardiac surgeries are pulmonary embolism, HF, arrhythmias, and sepsis, which also increase the levels of markers of myocardial necrosis and should be considered in the differential diagnosis. In addition, patients with renal failure commonly present increases in troponin levels, particularly TnT, but show a steady evolutionary behavior without the typical increase and decrease pattern of MI. On the other hand, CKMB dosage is less useful for the diagnosis of perioperative MI because of its lower sensitivity and specificity compared to troponin. This marker may increase after skeletal muscle injury during surgery, and its relationship with CPK has low reliability in the identification of perioperative myocardial injury.428428 Landesberg G, Shatz V, Akopnik I, Wolf YG, Mayer M, Berlatzky Y, et al. Association of cardiac troponin, CK-MB, and postoperative myocardial ischemia with long-term survival after major vascular surgery. J Am Coll Cardiol. 2003;42(9):1547-54.
Transthoracic echocardiography is an important tool for the diagnosis. Although a normal test does not exclude the diagnosis, presence of a new alteration in segmental contractility in patients with suspected myocardial ischemia corroborates the diagnosis. It can also provide indirect data for alternative diagnoses, such as pulmonary embolism and non-ischemic HF.
It is important to note that analysis of isolated data cannot confirm or exclude the diagnosis of perioperative myocardial ischemia. Although recent publications define very clearly the criteria for the diagnosis of myocardial infarction, perioperative MI remains without well-defined criteria.445445 Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et al. Third universal definition of myocardial infarction. J Am Coll Cardiol. 2012;60(16):1581-98. The diagnostic strategy proposed by this guideline for the identification of patients with perioperative MI is presented in figure 3.
In 2014, the authors of this study proposed prognostic criteria for patients with isolated troponin increases postoperatively based on data from the VISION study.446446 Botto F, Alonso-Coello P, Chan MT, Villar JC, Xavier D, Srinathan S, et al; Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Writing Group, on behalf of The Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Investigators.; Appendix 1. The Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Study Investigators Writing Group.; Appendix 2. The Vascular events In noncardiac Surgery patIents cOhort evaluatioN Operations Committee.; Vascular events In noncardiac Surgery patIents cOhort evaluatioN VISION Study Investigators. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120(3):564-78. Patients were diagnosed if they presented increases in fourth-generation TnT above the 99th percentile (30 ng/L) without another alternative diagnosis that could explain this result. Although the authors did not use the universal definition of MI, they created the first prognostic score for these patients. They found that age above 75 years (1 point), presence of anterior wall ischemia on ECG (1 point), and alterations in ST-segment (2 points) are independent predictors of mortality in a period of 30 days (Table 8).446446 Botto F, Alonso-Coello P, Chan MT, Villar JC, Xavier D, Srinathan S, et al; Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Writing Group, on behalf of The Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Investigators.; Appendix 1. The Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Study Investigators Writing Group.; Appendix 2. The Vascular events In noncardiac Surgery patIents cOhort evaluatioN Operations Committee.; Vascular events In noncardiac Surgery patIents cOhort evaluatioN VISION Study Investigators. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120(3):564-78.
Despite the frequency and prognostic importance, data in the literature are limited with regard to the treatment of perioperative myocardial ischemia. Most of the interventions represent extrapolations of well-established data for acute coronary syndromes not related to surgical procedures. However, all therapeutic strategies require measures that lead to an increased risk of postoperative bleeding. Thus, individualized measures and constant interaction with the surgical team are required.
The treatment of MI with no alterations in ST-segment (most cases of perioperative MI) initially requires correction of triggering factors and may perpetuate the ischemic process. Correction of anemia, hypovolemia, and pressure oscillations is the primary measure to be considered in this situation. To achieve consistency with the pathophysiology of the event, stabilization of the coronary plaque should be considered an important measure in the treatment. The extrapolated recommendations for the treatment of spontaneous acute coronary syndrome, antiplatelet treatment with ASA and clopidogrel, and anticoagulation with UFH or LMWH are used.447447 Nicolau JC, Timerman A, Marin-Neto JA, Piegas LS, Barbosa CJ, Franci A, et al; Sociedade Brasileira de Cardiologia. [Guidelines of Sociedade Brasileira de Cardiologia for unstable angina and non-ST-segment elevation myocardial infarction (II edition, 2007) 2013-2014 update]. Arq Bras Cardiol. 2014;102(3 Suppl 1):1-61. However, one should always weigh the risk of bleeding and the benefit of anticoagulation. Despite the absence of randomized studies in the perioperative period, it is prudent to give preference to UFH in cases of increased risk of bleeding because its effect can be quickly reversed in cases of bleeding. Patients of higher ischemic risk, i.e., those more than 75 years or with anterior wall ischemia on the ECG or clinical or hemodynamic instability, should be referred for early invasive strategy and revascularization. The remaining patients should be submitted to stratification before discharge. Such practice is fundamental to control the alarming morbidity and mortality in the short and long term.6969 Gualandro DM, Calderaro D, Yu PC, Caramelli B. Acute myocardial infarction after noncardiac surgery. Arq Bras Cardiol. 2012;99(5):1060-7.,448448 Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, et al; American College of Cardiology.; American Heart Association Task Force on Practice Guidelines.; Society for Cardiovascular Angiography and Interventions.; Society of Thoracic Surgeons.; American Association for Clinical Chemistry. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139-228. Erratum in: J Am Coll Cardiol. 2014;64(24):2713-4.
MI with ST-segment alterations occurs in a minority of cases and presupposes total occlusion of the coronary artery, requiring immediate intervention. In contrast to MI not related to surgical interventions, thrombolytic therapy is strongly contraindicated in the perioperative period because of prohibitive risk of bleeding. Thus, coronary angiography with primary PCI is the treatment of choice for these patients. This strategy is safe and feasible in those patients considered to be without contraindications to heparin and antiplatelet therapy, which are required during and after the procedure, respectively.6969 Gualandro DM, Calderaro D, Yu PC, Caramelli B. Acute myocardial infarction after noncardiac surgery. Arq Bras Cardiol. 2012;99(5):1060-7.,449449 Berger PB, Bellot V, Bell MR, Horlocker TT, Rihal CS, Hallett JW, et al. An immediate invasive strategy for the treatment of acute myocardial infarction early after noncardiac surgery. Am J Cardiol. 2001;87(9):1100-2, A6, A9.
B) Acute Atrial Fribrilation/Flutter
In the perioperative period, patients may present a variable risk of developing AF. The definition is based on the risk factors of the patient (male gender, advanced age, presence of cardiovascular comorbidities) and type of surgery (thoracic, mainly esophageal and lung surgeries). The reasons for higher occurrence of AF in thoracic surgeries are elevated levels of catecholamines, hypervolemia, right ventricular overload, pericarditis, and marked systemic inflammatory response.
The incidence of AF in the perioperative period of noncardiac surgeries (POAF) varies with the characteristics of the patients and the type of surgery. The incidence can vary from 3% in adults > 45 years up to 30% in thoracic surgeries. It usually presents between the second and fourth postoperative days.450450 Frendl G, Sodickson AC, Chung MK, Waldo AL, Gersh BJ, Tisdale JE, et al; American Association of Thoracic Surgery. 2014 AATS guidelines for the prevention and management of perioperative atrial fibrillation and flutter for thoracic surgical procedures. Executive summary. J Thorac Cardiovasc Surg. 2014;148(3):772-91. High ventricular response AF is the most common presentation and may compromise hemodynamics, which may result in hypotension, HF, and myocardial infarction.451451 Bhave PD, Goldman LE, Vittinghoff E, Maselli J, Auerbach A. Incidence, predictors, and outcomes associated with postoperative atrial fibrillation after major noncardiac surgery. Am Heart J. 2012;164(6):918-24. The triggering factors of atrial arrhythmia are increased sympathetic activity caused by surgical stress, pain, and anemia, in addition to hypotension and hypo or hypervolemia. Hypoxia also causes AF due to vasoconstriction of the pulmonary veins and increases in right atrial pressure and atrial myocardial ischemia.452452 Kanji S, Williamson DR, Yaghchi BM, Albert M, McIntyre L, Canadian Critical Care Trials Group. Epidemiology and management of atrial fibrillation in medical and noncardiac surgical adult intensive care unit patients. J Crit Care. 2012;27(3):326.e1-8.
Atrial flutter (FLU) may have the same mechanism of AF but may also occur only due to autonomic imbalance, similar to other paroxysmal supraventricular tachycardias. Due to association with cardioembolic events and hemodynamic impairment as in AF, FLU can be diagnosed and managed in a similar manner.
Diagnosis is performed using 12-lead ECG or detection on a cardiac monitor for more than 30 seconds.450450 Frendl G, Sodickson AC, Chung MK, Waldo AL, Gersh BJ, Tisdale JE, et al; American Association of Thoracic Surgery. 2014 AATS guidelines for the prevention and management of perioperative atrial fibrillation and flutter for thoracic surgical procedures. Executive summary. J Thorac Cardiovasc Surg. 2014;148(3):772-91. The initial measure for AF/FLU is to identify the triggering factors and to correct them early. Most POAFs have spontaneous reversal in 24 hours. If arrhythmia persists, the initial aim is to control the heart rate, which may remain between 80 and 110 bpm or up to 120 and 130 bpm according to clinical decision (hemodynamic stability and transient situations of increased adrenergic stress). The most commonly used medications for heart rate control are metoprolol, diltiazem, and digoxin (or deslanosid C, if only the venous route is available).453453 Danelich IM, Lose JM, Wright SS, Asirvatham SJ, Ballinger BA, Larson DW, et al. Practical management of postoperative atrial fibrillation after noncardiac surgery. J Am Coll Surg. 2014;219(4):831-41.
Digital use requires slow titration, adequate electrolytic control (calcium, potassium, and magnesium), and monitoring renal function or, in specific cases, digoxinemia. Its efficacy may be compromised by the degree of sympathetic activity in the perioperative period. Diltiazem should not be used in patients with hypotension or with ventricular dysfunction because of its negative inotropic effect. In these patients, the use of β-blockers is preferred.452452 Kanji S, Williamson DR, Yaghchi BM, Albert M, McIntyre L, Canadian Critical Care Trials Group. Epidemiology and management of atrial fibrillation in medical and noncardiac surgical adult intensive care unit patients. J Crit Care. 2012;27(3):326.e1-8.,454454 January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, et al; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267. Erratum in: Circulation. 2014;130(23):e272-4. Some studies indicated the use of venous magnesium or chloride sulfate, which can reverse arrhythmia because of its effect on T- and L-type calcium channels by reducing atrial automatism and heart rate control (inhibition of AV conduction), with a lower hypotensive or inotropic negative effect.455455 Ho KM, Sheridan DJ, Paterson T. Use of intravenous magnesium to treat acute onset atrial fibrillation: a meta-analysis. Heart. 2007;93(11):1433-40.
During the surgical period, patients present hypercoagulability associated with the risk of bleeding. Thus, most consensuses recommend anticoagulation for the prevention of arterial embolism only after 48 hours of persistent arrhythmia.452452 Kanji S, Williamson DR, Yaghchi BM, Albert M, McIntyre L, Canadian Critical Care Trials Group. Epidemiology and management of atrial fibrillation in medical and noncardiac surgical adult intensive care unit patients. J Crit Care. 2012;27(3):326.e1-8.,454454 January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, et al; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267. Erratum in: Circulation. 2014;130(23):e272-4. Clinical scores used to determine the risk of ischemic event and bleeding were not evaluated in the perioperative period. However, the American directive of 2014 recommends the routine use of CHA2DS2-VASC scores for embolic risk and HAS-BLED for bleeding risk.454454 January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, et al; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267. Erratum in: Circulation. 2014;130(23):e272-4. Considering surgical recovery, anemia, hemodynamic stability, and surgical wound, special attention should be given to the risk of bleeding.
C) Acute Heart Failure
The influence of chronic HF on perioperative risk is well known, with an increase in death of 63% and a readmission rate of 51% in a period of 30 days, compared to patients with CAD but without HF.126126 Hammill BG, Curtis LH, Bennett-Guerrero E, O'Connor CM, Jollis JG, Schulman KA, et al. Impact of heart failure on patients undergoing major noncardiac surgery. Anesthesiology. 2008;108(4):559-67. However, publications on acute perioperative HF in noncardiac surgeries are limited. On the other hand, when HF has recently been diagnosed and it is possible to extrapolate that patients are at least moderately symptomatic or with signs of congestion, there is a clear recommendation for an elective surgery to be postponed until symptoms subside and the reverse remodeling process begins (improvement of ventricular dysfunction and reduction of diastolic volume), following administration and optimization of drugs, such as ACE inhibitors or angiotensin II receptor blockers (ARBs) aldosterone antagonists, and β-blockers.456456 Upshaw J, Kiernan MS. Preoperative cardiac risk assessment for noncardiac surgery in patients with heart failure. Curr Heart Fail Rep. 2013;10(2):147-56.
We can analyze the presence of acute HF through evaluation of natriuretic peptides. Levels of B-type natriuretic peptide (BNP) or amino terminal portion of ProBNP (NT-proBNP) in the circulation increase when there is ventricular dysfunction. They are particularly increased if ventricular wall tension or fiber stretching exists and are therefore significantly increased in acute HF. Mildly or moderately increased levels have already shown an important relation with morbidity and mortality. In a study of 297 patients more than 50 years old submitted to emergency procedures, Farzi et al.457457 Farzi S, Stojakovic T, Marko T, Sankin C, Rehak P, Gumpert R, et al. Role of N-terminal pro B-type natriuretic peptide in identifying patients at high risk for adverse outcome after emergent non-cardiac surgery. Br J Anaesth. 2013;110(4):554-60. observed a sevenfold increase in the risk of cardiovascular events (nonfatal MI, acute HF, or cardiovascular death) during hospitalization in patients with NT-proBNP above 1,740 mg/mL and patients with NT-proBNP > 1,600 pg/mL showed a fourfold increase in the rate of combined events. The importance of this study relies on the fact that high NT-proBNP levels are compatible with the expected values in patients with acute HF (usually > 1,800 pg/mL defines the patient with acute dyspnea of cardiac cause). Another study evaluated patients with hip fracture submitted to emergency surgery and analyzed the relationship between NT-proBNP and the risk of death. High (> 2,370 pg/mL) and intermediate (806-2,370 pg/mL) NT-proBNP levels are associated with a significantly higher mortality compared to patients with low levels (< 806 pg/mL) - (15 vs. 11 vs. 2%, p = 0.04). In the long term, mortality is also higher in these two groups (69% vs. 49% vs. 27%, p < 0.001).458458 Nordling P, Kiviniemi T, Strandberg M, Strandberg N, Airaksinen J. Predicting the outcome of hip fracture patients by using N-terminal fragment of pro-B-type natriuretic peptide. BMJ Open. 2016;6(2):e009416. Patients with such increased levels of natriuretic peptides in the preoperative period are probably no longer adequately compensated for HF at the time of surgery and this may be one of the causes of postoperative acute HF.
A multicenter study compared 5,094 patients with worsening HF to 5,094 patients without HF, paired by baseline characteristics, submitted to noncardiac surgery. Worsening HF in the perioperative period was associated with a twofold increase in mortality in a period of 30 days (p < 0.001), 1.5-fold increase in postoperative morbidity (p < 0.001), increased risk of developing renal failure, need for mechanical ventilation for more than 48 hours, pneumonia, cardiac arrest, unplanned intubation, sepsis, and urinary tract infection (all p < 0.05). BNP or NT-proBNP was not evaluated in this series, and the incidence of myocardial infarction was similar in both groups (p = 0.7).459459 Maile MD, Engoren MC, Tremper KK, Jewell E, Kheterpal S. Worsening preoperative heart failure is associated with mortality and noncardiac complications, but not myocardial infarction after noncardiac surgery: a retrospective cohort study. Anesth Analg. 2014;119(3):522-32.
Therefore, patients who are not compensated for HF should not be submitted to elective surgeries because they have a very high risk of developing HF. Studies evaluating the real incidence, cause, diagnosis, and treatment of acute postoperative HF are required. Diagnosis of acute postoperative HF is clinical, and the dosage of natriuretic peptides can be performed in cases of diagnostic uncertainty. The echocardiogram should be performed to evaluate the presence of basic structural heart disease. Treatment should be performed in the same manner as that of acute HF outside the perioperative period. The possible causes of acute postoperative HF are acute CAD, persistently positive perioperative water balance volume overload, involuntary suspension of drugs used to treat chronic HF, renal failure, infection, PTE, and arrhythmias, among others.
Among these causes, MI is more common in the first 72 hours of the postoperative period.6969 Gualandro DM, Calderaro D, Yu PC, Caramelli B. Acute myocardial infarction after noncardiac surgery. Arq Bras Cardiol. 2012;99(5):1060-7.,444444 Devereaux PJ, Xavier D, Pogue J, Guyatt G, Sigamani A, Garutti I, et al; POISE (PeriOperative ISchemic Evaluation) Investigators. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: a cohort study. Ann Intern Med. 2011;154(8):523-8. It may manifest as acute HF or acute pulmonary edema and not as chest pain.446446 Botto F, Alonso-Coello P, Chan MT, Villar JC, Xavier D, Srinathan S, et al; Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Writing Group, on behalf of The Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Investigators.; Appendix 1. The Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Study Investigators Writing Group.; Appendix 2. The Vascular events In noncardiac Surgery patIents cOhort evaluatioN Operations Committee.; Vascular events In noncardiac Surgery patIents cOhort evaluatioN VISION Study Investigators. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120(3):564-78. MI should always be actively investigated with ECG and serial troponin collection. The echocardiogram may also help in the diagnosis by showing new changes in segmental contractility.
D) Venous Thromboembolism
I. Diagnosis of Venous Thromboembolism
DVT and PTE are two manifestations of the same disease, the venous thromboembolism (VTE). There are clinical probability scores that can be used for the diagnosis of VTE. One of the most used is the Wells score (Table 9 for DVT and table 10 for PTE).460460 Wells PS, Anderson DR, Rodger M, Ginsberg JS, Kearon C, Gent M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer. Thromb Haemost. 2000;83(3):416-20.,461461 Wells PS, Anderson DR, Bormanis J, Guy F, Mitchell M, Gray L, et al. Value of assessment of pretest probability of deep-vein thrombosis in clinical management. Lancet. 1997;350(9094):1795-8.
I. A. Deep Venous Thrombosis
DVT of the lower limbs is subdivided into two categories, namely, distal venous thrombosis (calf veins) and proximal vein (popliteal, femoral, or iliac veins). Proximal venous thrombosis is the most commonly associated with PTE. The diagnosis is performed with history and clinical examination (edema, pain, and erythema involving the site) and confirmed by imaging tests. The proposed flowchart for the diagnosis of DVT is shown in figure 4.
Venous Doppler is the test of choice, with a positive predictive value of 94% and has the advantage of being conducted at the bedside.462,463 However, venous Doppler has limitations in detecting isolated thrombi in the iliac veins and in the portion of the femoral vein in the adductor canal.
D-dimer dosage should not be used alone for the diagnosis of VTE. D-Dimer is a product of fibrin degradation and is increased (> 500 ng/mL equivalent units of fibrinogen) in virtually all VTE patients. However, this test has high sensitivity and low specificity and may be increased in the elderly, patients with neoplasms, renal failure, pregnancy, and patients recently submitted to surgeries.464464 Di Nisio M, Squizzato A, Rutjes AW, Büller HR, Zwinderman AH, Bossuyt PM. Diagnostic accuracy of D-dimer test for exclusion of venous thromboembolism: a systematic review. J Thromb Haemost. 2007;5(2):296-304. Erratum in: J Thromb Haemost. 2013;11(10):1942.
Iodinated contrast venography can be used when the venous Doppler cannot be performed or gave an uncertain result. Venography can cause discomfort to the patient, besides the greater difficulty in obtaining an adequate study. It has an accuracy similar to the venous Doppler.465465 Lensing AW, Büller HR, Prandoni P, Batchelor D, Molenaar AH, Cogo A, et al. Contrast venography, the gold standard for the diagnosis of deep-vein thrombosis: improvement in observer agreement. Thromb Haemost. 1992;67(1):8-12.
Magnetic resonance venography (MRV) has the same accuracy as contrast venography (100% sensitivity and 96% specificity). Its major limitation is the high cost, but it is an option when the patient has allergy to iodinated contrast.466466 Carpenter JP, Holland GA, Baum RA, Owen RS, Carpenter JT, Cope C. Magnetic resonance venography for the detection of deep venous thrombosis: comparison with contrast venography and duplex Doppler ultrasonography. J Vasc Surg. 1993;18(5):734-41.
Angio-CT of the chest with PTE protocol allows visualization of the pulmonary arteries and subdiaphragmatic deep veins, including the lower limbs, in the same test without the need for additional doses of iodinated contrast.467467 Duwe KM, Shiau M, Budorick NE, Austin JH, Berkmen YM. Evaluation of the lower extremity veins in patients with suspected pulmonary embolism: a retrospective comparison of helical CT venography and sonography. 2000 ARRS Executive Council Award I. American Roentgen Ray Society. AJR Am J Roentgenol. 2000;175(6):1525-31. In some studies, Angio-CT venography is comparable to venous Doppler for the diagnosis of femoral-popliteal venous thrombosis.468468 Garg K, Kemp JL, Wojcik D, Hoehn S, Johnston RJ, Macey LC, et al. Thromboembolic disease: comparison of combined CT pulmonary angiography and venography with bilateral leg sonography in 70 patients. AJR Am J Roentgenol. 2000;175(4):997-1001. However, to date, the use of Angio-CT remains a potential test for simplifying the diagnosis of DVT. Future studies are still required to establish its accuracy.
I. B. Pulmonary Thromboembolism
Acute PTE is a common and often fatal disease. Clinical evaluation and diagnostic tests are required before the start of anticoagulation (Figure 5).
The diagnosis is performed with history and physical examination, ranging from the absence of symptoms to shock or sudden death. The most common symptoms identified in the PIOPED II (Prospective Investigation of Pulmonary Embolism Diagnosis II) study469469 Stein PD, Beemath A, Matta F, Weg JG, Yusen RD, Hales CA, et al. Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II. Am J Med. 2007;120(10):871-9. are dyspnea (73%), pleuritic pain, and cough (37%). Dyspnea is often sudden. Approximately 10% of patients present with symptoms of pulmonary infarction, usually due to small and peripheral embolisms. However, in a systematic review of 28 studies with a total of 5,233 patients with DVT, one-third had asymptomatic PTE.470470 Stein PD, Matta F, Musani MH, Diaczok B. Silent pulmonary embolism in patients with deep venous thrombosis: a systematic review. Am J Med. 2010;123(5):426-31.
The incidence of shock is 8%. Massive PTE can be accompanied by right ventricular failure, with increased jugular venous pressure, presence of a third sound on the right side, cyanosis, and obstructive shock. However, patients with severe PH and underlying cardiopulmonary diseases may present shock with small PTE.
Complementary Tests
Arterial blood gas: this test is usually altered. However, it is neither sensitive nor specific for the diagnosis of PTE. Hypoxemia is present in 74% of cases.
BNP and troponin: they may be increased but are not sensitive or specific tests for the diagnosis of PTE. They have prognostic implications, being indicative of the severity of PTE.
D-dimer: D-dimer, as well as for DVT, is a sensitive but not very specific test.
ECG: ECG alterations in patients with PTE are common, although not specific. Tachycardia and ST-segment and T-wave alterations are the most frequent findings (70% of cases of PTE). Classical alterations considered as suggestive of PTE (S1 Q3 T3, right ventricular overload, and incomplete right branch block) are not frequent (< 10%). Electrocardiographic changes that are associated with a worse prognosis are atrial arrhythmias (e.g., AF), bradycardia (< 50 bpm) or tachycardia (> 100 bpm), new right branch block, Q waves in lower leads (DII, DIII, and aVF), ST-segment changes in anterior wall, and T-wave and standard S1 Q3 T3 inversion.
Chest X-ray: Chest X-ray is a common test, but it has low sensitivity and specificity. However, it can detect atelectasis or parenchymal abnormalities (18-69%), pleural effusion (47%), and cardiomegaly (> 50%). Peripheral wedge-shaped opacity in peripheral lung regions and abrupt cut-off of pulmonary arterioles with distal hypoperfusion are rare but are highly suspected of PTE. Chest X-ray may be normal in 12-22% of patients with PTE.
Angio-CT with protocol for PTE: for most patients with PTE, it is the selected diagnostic test due to its high sensitivity (> 90%) and specificity (> 95%) for PTE, especially when associated with D-dimer dosage,471 in patients with moderate to high probability. Demonstration of filling failure in any branch of the pulmonary artery using contrast is a diagnosis of PTE.
Ventilation/perfusion (V/Q) scintigraphy: this test is reserved for patients with suspected PTE when Angio-CT is contraindicated (renal insufficiency, creatinine clearance < 60 mL/min/m22 Dunkelgrun M, Boersma E, Schouten O, Koopman-van Gemert AW, van Poorten F, Bax JJ, et al; Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Bisoprolol and fluvastatin for the reduction of perioperative cardiac mortality and myocardial infarction in intermediate-risk patients undergoing noncardiovascular surgery: a randomized controlled trial (DECREASE-IV). Ann Surg. 2009;249(6):921-6., contrast allergy, or morbid obesity) or when Angio-CT is inconclusive or negative, but in disagreement with the high clinical suspicion. V/Q scintigraphy is a sensitive test for the diagnosis of PTE, but it is not specific due to its high incidence of false-positive results. Accuracy is higher when chest X-ray is normal. V/Q scintigraphy is selected for the diagnosis of PTE during pregnancy. A high probability V/Q scintigraphy is sufficient for the diagnosis of PTE, whereas a normal scintigraphy is sufficient to exclude PTE. Low or intermediate probabilities are not sufficient for diagnosis.
Pulmonary digital angiography with iodinated contrast: this test was the historical gold standard for the diagnosis of PTE. With the development of Angio-CT, it is reserved for patients with suspected PTE when Angio-CT or V/Q scintigraphy is not conclusive. In a retrospective analysis of 20 cases of the PIOPED II study,472 digital angiography was shown to be less sensitive than Angio-CT for the diagnosis of small emboli. It has morbidity of 5% and mortality of < 2%. Exposure to radiation is greater than in Angio-CT. Demonstration of filling failure and abrupt cut-off of pulmonary arterial vessel are diagnoses of embolization.
Pulmonary angiography by nuclear magnetic resonance: this test is not very sensitive (77-84%). It is reserved for cases in which other methods cannot be performed.
Echocardiogram: this test does not diagnose PTE. However, presumptive diagnosis can be performed using the echocardiogram in patients with high clinical suspicion and hemodynamic instability. Approximately 30-40% of patients with PTE have echocardiographic changes, indicative of right ventricular overload, especially in those with massive PTE, such as right ventricular dilatation, right ventricular dysfunction, and tricuspid insufficiency.
II. Treatment of Venous Thromboembolism
There is limited evidence for the best treatment for venous thromboembolism in the perioperative period. This is because surgeries may have different bleeding risks, clinical situations may be extremely heterogeneous, and conventional therapy may not be the most appropriate after a specific surgical procedure. Thus, we will present the usual recommended treatment, regardless of the perioperative context, but it is important to customize the decisions in conjunction with the surgeon.
The main pillar of venous thromboembolism treatment (deep vein thrombosis and PTE) is anticoagulant therapy, which should be a long-term therapy, with a duration of at least 3 months.380380 Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704. However, there are clinical situations that require the use of anticoagulant therapy for longer periods, which has become known as extended anticoagulant therapy and implies its use for an indefinite period.380380 Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704.
II. A. Selection of Anticoagulant
Several recent studies have examined the efficacy of new anticoagulants in acute and long-term treatment of VTE and compared to warfarin. These studies showed that the reduction in the risk of recurrence of VTE is similar with both therapies, including cancer patients.473473 Büller HR, Décousus H, Grosso MA, Mercuri M, Middeldorp S, Prins MH, et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med. 2013;369(15):1406-15. Erratum in: N Engl J Med. 2014;370(4):390.
474 Schulman S, Kakkar AK, Goldhaber SZ, Schellong S, Eriksson H, Mismetti P, et al; RE-COVER II Trial Investigators. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation. 2014;129(7):764-72.
475 Agnelli G, Buller HR, Cohen A, Curto M, Gallus AS, Johnson M, et al; AMPLIFY Investigators. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013; 369(9):799-808.
476 Büller HR, Prins MH, Lensin AW, Decousus H, Jacobson BF, Minar E, et al; EINSTEIN-PE Investigators. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366(14):1287-97.-477477 Castellucci LA, Cameron C, Le Gal G, Rodger MA, Coyle D, Wells PS, et al. Clinical and safety outcomes associated with treatment of acute venous thromboembolism: a systematic review and meta-analysis. JAMA. 2014;312(11):1122-35. The reduction in the risk of recurrence of VTE with the different new anticoagulants (dabigatran, rivaroxaban, apixaban, and edoxaban) is not directly compared among them, but it appeared to be equally effective based on indirect comparisons.477477 Castellucci LA, Cameron C, Le Gal G, Rodger MA, Coyle D, Wells PS, et al. Clinical and safety outcomes associated with treatment of acute venous thromboembolism: a systematic review and meta-analysis. JAMA. 2014;312(11):1122-35. In fact, in the recommendations, the order of the new anticoagulants cited in the text refers to the chronology of the publication of the phase III studies on VTE and is not the order of preference.
The new anticoagulants have lower bleeding rates and provide greater convenience for patients and health professionals in relation to fixed dose. They have less drug and food interactions and do not require serial blood tests to ensure a specific therapeutic range. Given these advantages, the new anticoagulants are now preferred compared to warfarin for initial and long-term treatments of VTE in patients without cancer.
In cancer patients, a recent randomized study compared the use of LMWH (tinzaparin) and warfarin for the treatment of 900 cancer patients with DVT during the first 6 months. The study demonstrated that LMWH is more effective than warfarin, without alterations in death rates and major bleeding.478478 Lee AY, Kamphuisen PW, Meyer G, Bauersachs R, Janas MS, Jarner MF, et al; CATCH Investigators. Tinzaparin vs warfarin for treatment of acute venous thromboembolism in patients with active cancer: a randomized clinical trial. JAMA. 2015;314(7):677-86. Other studies have also shown that the reduction of the risk of recurrence of VTE in cancer patients is higher with the use of LMWH compared to warfarin.479479 Carrier M, Cameron C, Delluc A, Castellucci L, Khorana AA, Lee AY. Efficacy and safety of anticoagulant therapy for the treatment of acute cancer-associated thrombosis: a systematic review and meta-analysis. Thromb Res. 2014;134(6):1214-9.,480480 Bochenek T, Nizankowski R. The treatment of venous thromboembolism with low-molecular-weight heparins. A meta-analysis. Thromb Haemost. 2012;107(4):699-716.
Therefore, warfarin is preferentially used in patients with VTE without cancer and LMWH in patients with VTE and cancer. No study has directly compared the new anticoagulants and LMWH in cancer patients. However, based on indirect comparisons, LMWH appears to be more effective than the new anticoagulants in patients with VTE and cancer.479479 Carrier M, Cameron C, Delluc A, Castellucci L, Khorana AA, Lee AY. Efficacy and safety of anticoagulant therapy for the treatment of acute cancer-associated thrombosis: a systematic review and meta-analysis. Thromb Res. 2014;134(6):1214-9.
It is important to emphasize that parenteral anticoagulation was given before the use of dabigatran and edoxaban in previous studies. It was not used prior to rivaroxaban and apixaban. It was used before and for a period with warfarin until the desired INR was reached.
II. B. Duration of the Anticoagulant Therapy
The studies that determined the appropriate duration of treatment for VTE basically compared four treatment duration options: 4 or 6 weeks; 3 months; more than 3 months, although limited to 6 to 12 months; and extended or indefinite duration therapy. These four treatment duration protocols were tested in different available studies in four profiles of VTE patients with different estimates of recurrence risk after suspending anticoagulant therapy:
(1) VTE caused by surgery (major transient risk factor with 3% recurrence in 5 years);481481 Iorio A, Kearon C, Filippucci E, Marcucci M, Macura A, Pengo V, et al. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk factor: a systematic review. Arch Intern Med. 2010;170(19):1710-6. (2) VTE caused by a transient non-surgical risk factor (estrogen therapy, pregnancy, lower limb lesions, flights > 8 hours, with a risk of recurrence of 15% in 5 years); (3) idiopathic VTE with no transient risk factors or cancer (30% recurrence in 5 years);482482 Boutitie F, Pinede L, Schulman S, Agnelli G, Raskob G, Julian J, et al. Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism on risk of recurrence after stopping treatment: analysis of individual participants' data from seven trials. BMJ. 2011;342:d3036.,483483 Prandoni P, Noventa F, Ghirarduzzi A, Pengo V, Bernardi E, Pesavento R, et al. The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute proximal deep vein thrombosis or pulmonary embolism. A prospective cohort study in 1,626 patients. Haematologica. 2007;92(2):199-205. (4) VTE associated with cancer (15% annual recurrence).484484 Palareti G, Legnani C, Lee A, Manotti C, Hirsh J, D'Angelo A, et al. A comparison of the safety and efficacy of oral anticoagulation for the treatment of venous thromboembolic disease in patients with or without malignancy. Thromb Haemost. 2000;84(5):805-10.,485485 Prandoni P, Lensing AW, Cogo A, Cuppini S, Villalta S, Carta M, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. 1996;125(1):1-7.
Another important factor that guides the duration of anticoagulant therapy in VTE is the risk of bleeding that can be categorized as low (absence of risk factors for bleeding, with a 0.8% annual risk for major bleeding), moderate (one risk factor for bleeding, with a 1.6% annual risk for major bleeding), or high (two or more risk factors for bleeding, with a ≥6.5% annual risk for major bleeding). The risk factors for bleeding during anticoagulant therapy are described in chart 14.486486 Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-52.
It is important to note that for all patients using extended or indefinite anticoagulant therapy, treatment should be reassessed at least annually.
II. C. When and How to Prescribe Anticoagulants in Patients With Distal Dvt of The Lower Limbs
It is still unclear whether the benefits of anticoagulation outweigh the risks of anticoagulant treatment for distal isolated DVT because of the low risk of progression and recurrence of VTE.380380 Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704. About 15% of distal isolated DVT will develop with thrombus progression to the popliteal vein and risk of PTE.487487 Masuda EM, Kistner RL, Musikasinthorn C, Liquido F, Geling O, He Q. The controversy of managing calf vein thrombosis. J Vasc Surg. 2012;55(2):550-61.
The following risk factors favor thrombus extension in distal isolated DVT and support the use of anticoagulant therapy over imaging follow-up: positive D-dimer, extensive thrombosis involving multiple veins, proximal vein thrombosis, absence of reversible trigger factor for DVT, active cancer, previous history of VTE, and hospitalized patient.488488 Kearon C. Natural history of venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I22-30.
489 Macdonald PS, Kahn SR, Miller N, Obrand D. Short-term natural history of isolated gastrocnemius and soleal vein thrombosis. J Vasc Surg. 2003;37(3):523-7.
490 Parisi R, Visonà A, Camporese G, Verlato F, Lessiani G, Antignani PL, et al. Isolated distal deep vein thrombosis: efficacy and safety of a protocol of treatment. Treatment of Isolated Calf Thrombosis (TICT) Study. Int Angiol. 2009;28(1):68-72.
491 Palareti G. How I treat isolated distal deep vein thrombosis (IDDVT). Blood. 2014;123(12):1802-9.-492492 Galanaud JP, Sevestre MA, Genty C, Kahn SR, Pernod G, Rolland C, et al; OPTIMEV-SFMV investigators. Incidence and predictors of venous thromboembolism recurrence after a first isolated distal deep vein thrombosis. J Thromb Haemost. 2014;12(4):436-43.
II. D. Role of Catheter-directed Thrombolysis in Deep Venous Thrombosis of the Lower Limb
Evidence is scarce with regard to the use of catheter-directed thrombolysis for the treatment of proximal DVT of the lower limb, causing substantial uncertainty that the benefits outweigh the risks associated with the procedure.380380 Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704.
II. E. Role of the Inferior Vena Cava Filter
Evidence shows the inconsistent benefit of using the inferior vena cava filter to prevent recurrence of VTE in anticoagulated patients. The most recent randomized study, PREPIC,493493 Mismetti P, Laporte S, Pellerin O, Ennezat PV, Couturaud F, Elias A, et al; PREPIC2 Study Group. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone on risk of recurrent pulmonary embolism: a randomized clinical trial. JAMA. 2015;313(16):1627-35. demonstrated that inferior vena cava filter implantation during 3 months does not reduce the recurrence of PTE, including fatal PTE, in anticoagulated patients with PTE and DVT, with additional risk factors for recurrence of VTE
II. F. Role of Compression Stockings
A recent multicenter, placebo-controlled, study has shown that in contrast to two previous smaller studies, the routine use of compression stockings does not reduce the risk of post-thrombotic syndrome nor does it add any other important benefit.494494 Kahn SR, Shapiro S, Wells PS, Rodger MA, Kovacs MJ, Anderson DR, et al; SOX trial investigators. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet. 2014;383(9920):880-8.
II. G. Subsegmental Pulmonary Thromboembolism Treatment
With technological development of pulmonary angiotomographies, diagnostic identification of subsegmental PTEs increases and the best therapeutic management in these cases is uncertain. Changes are often small and may correspond to false positives, and true subsegmental PTE is generally associated with small DVTs. The risk of progression or recurrence of VTE in the absence of anticoagulation is small in relation to larger PTEs.486486 Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-52.
Imaging of DVT should be performed on the lower limbs, as well as on the upper limbs and central venous catheters. If DVT is detected, anticoagulant therapy should be introduced, but if no DVT is detected, the need for anticoagulation in these patients is uncertain.486486 Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-52.
In these cases, it is important to evaluate the risk factors for recurrence or progression of VTE, which include the following: patients hospitalized or with reduced mobility for other reasons; patients with active cancer, especially those with metastatic disease or those treated with chemotherapy; or patients with non-reversible risk factors, such as recent surgery. Similarly, important clinical symptoms that cannot be attributed to another cause or a low functional reserve favor the use of anticoagulant therapy, whereas the presence of a high risk of bleeding favors the preference for clinical follow-up.
II. H. Home Treatment of Pulmonary Thromboembolism
Recent meta-analyses evaluated the possibility and safety of home treatment for pulmonary embolism.495495 Piran S, Le Gal G, Wells PS, Gandara E, Righini M, Rodger MA, et al. Outpatient treatment of symptomatic pulmonary embolism: a systematic review and meta-analysis. Thromb Res. 2013;132(5):515-9.
496 Vinson DR, Zehtabchi S, Yealy DM. Can selected patients with newly diagnosed pulmonary embolism be safely treated without hospitalization? A systematic review. Ann Emerg Med. 2012;60(5):651-62.e4. Erratum in: Ann Emerg Med. 2015;65(2):177.-497497 Zondag W, Kooiman J, Klok FA, Dekkers OM, Huisman MV. Outpatient versus inpatient treatment in patients with pulmonary embolism: a meta-analysis. Eur Respir J. 2013;42(1):134-44. It is recommended that patients candidate for home treatment meet all the following criteria:380380 Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704. clinically stable with good cardiopulmonary reserve; no contraindications, such as recent bleeding, severe renal or hepatic failure, or severe thrombocytopenia (< 70,000/mm3); willingness to follow the treatment; and feel safe to be treated at home.
II. I. Systemic Thrombolysis for Pulmonary Thromboembolism
Systemic thrombolytic therapy is associated with a faster decrease in pulmonary artery pressure, increased arterial oxygenation, and resolution of filling faults on CT, accelerating the resolution of PTE. However, such therapy is associated with increased bleeding risks. Patients who will benefit the most are those who have the highest risk of death associated with PTE and the lowest risk of bleeding.380380 Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704.
Recently, three randomized trials evaluated the use of systemic thrombolytic therapy in 1,200 patients with acute PTE and improved the evidence regarding this topic.498498 Kline JA, Nordenholz KE, Courtney DM, Kabrhel C, Jones AE, Rondina MT, et al. Treatment of submassive pulmonary embolism with tenecteplase or placebo: cardiopulmonary outcomes at 3 months: multicenter double-blind, placebo-controlled randomized trial. J Thromb Haemost. 2014;12(4):459-68.
499 Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M; "MOPETT" Investigators. Moderate pulmonary embolism treated with thrombolysis (from the "MOPETT" Trial). Am J Cardiol. 2013;111(2):273-7.-500500 Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, et al; PEITHO Investigators. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402-11.
It is important to note that patients recently submitted to a surgery will always have an at least moderate risk of bleeding (Chart 14) and the possibility of using systemic thrombolytic therapy for the treatment of acute PTE needs to carefully assess the risks and benefits and should be discussed with the surgeon.
II. J. Pulmonary Thromboembolism Therapy with Catheter Intervention486486 Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-52.
II. K. T Recurrent Pulmonary Thromboembolism During Anticoagulant Therapy486486 Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-52.
9. Evaluation of Comorbidities
A) Diabetes Mellitus
I. Preoperative
DM affects 6.2% of the Brazilian adult population,501501 IBGE. Diretoria de Pesquisas, Coordenação de Trabalho e Rendimento, Pesquisa Nacional de Saúde 2013. Disponível em ftp://ftp.ibge.gov.br/PNS/2013/pns2013.pdf
ftp://ftp.ibge.gov.br/PNS/2013/pns2013.p...
with a progressive increase in prevalence according to age, affecting more than 19% of individuals more than 65 years. These patients have a high incidence of CDs. Glycemic control is one of the most important aspects to be considered in the perioperative evaluation of patients with DM. There is substantial observational evidence that links hyperglycemia to unfavorable surgical outcomes, such as infection, longer hospital stay, disability after discharge, and mortality.
In Brazil, approximately 90% and 73% of type 1 and type 2 DM patients, respectively, are outside the recommended targets for glycemic control (glycated hemoglobin lower than 7.0%). Therefore, it is expected that most individuals in preoperative evaluation need specific guidelines regarding glycemic control.
Preoperative evaluation becomes an additional opportunity to adjust medication doses, educate an individual, and improve metabolic control. A staggered scheme (insulin to correct capillary glycemia) should be avoided as an exclusive therapy for prolonged periods because it is ineffective for most patients. In addition, this scheme favors glycemic variability, attempting to correct the “problem” (hyperglycemia) after it has already occurred and may even be deleterious, predisposing to diabetic ketoacidosis in patients with type 1 DM.
Specific Glossary
-
Prandial insulin: dose of fast (regular) or ultrafast (lispro, aspart, glulisine) insulin used to control postprandial blood glucose, used before meals.
-
Basal insulin: dose of intermediate (NPH) or slow (detemir, glargine, and degludec) insulin used to control glucose during fasting and interprandial periods. Used in several schemes: fasting, sleeping, and pre-meals, divided into 1 to 2 doses per day (detemir and glargine) and 1 to 4 doses per day (NPH).
-
Correction or supplemental insulin: dose of fast (regular) or ultrafast (lispro, aspart, glulisine) insulin used to treat hyperglycemia that occurs before or between meals or when the patient is fasting (Table 11).
-
Staggered scheme: known as “insulin on demand”, “insulin according to dextro or HGT”. Fast (regular) or ultrafast (lispro, aspart, glulisine) dose scheme according to capillary glycemia to treat hyperglycemia.
-
Basal scheme: use of intermediate or slow insulin alone.
-
Basal-bolus or basal-prandial scheme: use of combined basal and prandial insulins.
A free Brazilian application was developed at the Hospital das Clínicas (HCFMUSP) to assist physicians and nurses in performing intensive glycemic control in hospitalized patients. InsulinApp is a tool developed for smartphones and tablets that calculates hospital doses of insulin necessary for a patient in a few minutes.508 It is available free of charge from both Google Play (Android) and Apple (iOS) under the name InsulinAPP.
Special Considerations for Patients with Type 1 Diabetes Mellitus
Pre-assessment and in-hospital monitoring with specialist is recommended, if available.
Monitor capillary glycemia: pre-meal and at 10 pm while maintaining usual diet; every 4 hours during the fast; and every hour or two hours if using continuous intravenous insulinization.
Never substitute basal-bolus insulin in the preoperative period by staggered scheme alone - risk of diabetic ketoacidosis.
In medium to major surgeries or with a surgical time of more than 1 hour, ideally use continuous intravenous insulin pump as soon as fasting starts or on the morning of surgery, maintaining the therapy during the intraoperative and postoperative periods.
If venous insulinization is not possible to perform, the following can be used:
-
- Maintain the insulin the evening before surgery.
-
- In the morning of the day of surgery - reduce basal insulin as described in chart 16.
-
- Remove prandial insulin, maintaining basal insulin, capillary glycemia every 3 or 4 hours, and start staggered scheme (prefer ultrafast insulin).
-
- Install glucose intake the morning of the surgery (before breakfast time). - maintain intake from 5 to 10 g/h. The number of grams per hour depends on the glycemic control.
Emergency Surgery in Patients with Diabetes Mellitus
Evaluate blood glucose before surgery.
Correct hypoglycemia and maintain glucose supply at 5 to 10 g/h of glucose. Preferably, control hyperglycemia with intravenous insulin and maintain blood glucose levels between 100 and 180 mg/dL.
Attention to potassium correction.
General Recommendations for Patients with Diabetes Mellitus502502 Rydén L, Grant PJ, Anker SD, Berne C, Cosentino F, Danchin N, et al. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD: the Task Force on diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and developed in collaboration with the European Association for the Study of Diabetes (EASD). Eur Heart J. 2013;34(39):3035-87. Erratum in: Eur Heart J. 2014;35(27):1824.
503 Umpierrez GE, Smiley D, Jacobs S, Peng L, Temponi A, Mulligan P, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care. 2011;34(2):256-61.
504 Buchleitner AM, Martínez-Alonso M, Hernández M, Solà I, Mauricio D. Perioperative glycaemic control for diabetic patients undergoing surgery. Cochrane Database Syst Rev. 2012 Sept 12;(9):CD007315.
505 Noordzij PG, Boersma E, Schreiner F, Kertai MD, Feringa HH, Dunkelgrun M, et al. Increased preoperative glucose levels are associated with perioperative mortality in patients undergoing noncardiac, nonvascular surgery. Eur J Endocrinol. 2007;156(1):137-42.
506 Bruno A, Gregori D, Caropreso A, Lazzarato F, Petrinco M, Pagano E. Normal glucose values are associated with a lower risk of mortality in hospitalized patients. Diabetes Care. 2008;31(11):2209-10.-507507 Griesdale DE, de Souza RJ, van Dam RM, Heyland DK, Cook DJ, Malhotra A, et al. Intensive insulin therapy and mortality among critically ill patients: a meta-analysis including NICE-SUGAR study data. CMAJ. 2009;180(8):821-7.
Postoperative Recommendations511511 Marik PE, Preiser JC. Toward understanding tight glycemic control in the ICU: a systematic review and metaanalysis. Chest. 2010;137(3):544-51.,512512 Jacobi J, Bircher N, Krinsley J, Agus M, Braithwaite SS, Deutschman C, et al. Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit Care Med. 2012;40(12):3251-76.
II. Postoperative
In 2001, an important study demonstrated a clinical benefit of strict glycemic control in the postoperative period for the first time in surgical patients: lower rates of in-hospital mortality, polyneuropathy, infections, and acute renal failure, and shorter time of mechanical ventilation and of stay in ICUs.509509 van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345(19):1359-67. Regarding patients with diabetes, the clinical benefit associated with strict glycemic control was also observed, but there was no impact on the reduction of mortality. Based on this study, the recommendation was strict glycemic control in the postoperative period for patients undergoing noncardiac surgery.
Another large randomized multicenter trial (NICE-SUGAR)510510 Finfer S, Chittock DR, Su SY, Blair D, Foster D, Dhingra V, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283-97. involving more than 6,000 patients, with approximately one-third of surgical patients and two-thirds of clinical patients, compared strict glycemic control (81-108 mg/dL) with conventional glycemic control (144-180 mg/dL). Surprisingly, the group of patients randomized to strict control presented higher mortality rates in a period of 90 days (27.5%) compared to the conventional group (24.9%). No differences were found in other minor outcomes between the groups. The group with the strict glycemic control presented higher hypoglycemia levels (<40 mg/dL) compared to the control group.
B) Thyroid Diseases
Hormonal disorders may be responsible for considerable perioperative morbidity and mortality,513 in addition to technical difficulties in managing the airways of patients with goiter.
Tetraiodothyronine (T4) represents 80-90% of thyroid hormone production, and 40% is peripherally converted to triiodothyronine (T3), which is five times more potent. About 50% of T4 is converted to 3,5-triiodothyronine (reverse T3), which has no biological activity. Only 0.2% of T3 and 0.3% of T4 circulate in the free and biologically active form. The rest binds to plasma proteins (albumin, pre-albumin, thyroglobulin). T3 and T3r are converted in the liver, kidneys, and central nervous system into inactive compounds. Severe systemic diseases, trauma, and drugs can block the peripheral conversion of T4 to T3, leading to euthyroid syndrome of the critical patient, which represents a physiological mechanism to save energy in critical situations.
During thyroid surgery, specific complications may occur in the perioperative period. Patients with large goiters may present complications in intubation and extubation (up to 35% have some of airway obstruction), recurrent laryngeal lesion, tracheomalacia, and glottal edema. Hypocalcemia may occur up to 36 hours after thyroidectomy in 20% of cases. Only 3% are permanently hypocalcemic, and calcium must be replaced intravenously at this stage.
I. Hypothyroidism
In epidemiological studies, the overall incidence of hypothyroidism varies from 0.1 to 2%. The prevalence of subclinical hypothyroidism is higher, ranging from 4 to 10% in the adult population and tending to be higher in women more than 65 years. Most of the population, even asymptomatic, has thyroid alterations. Some clinical conditions present a potential risk for the development of perioperative complications and a rapid decline in thyroid function, such as age > 65 years; hypothalamic or pituitary disease; coexisting autoimmune disease; irradiation of the neck, thyroid surgery, or radioiodine therapy; significant hyperlipidemia; hyponatremia; high levels of muscle enzyme; macrocytic anemia; and pleural or pericardial effusion.
If these risk conditions are present, screening for thyroid disease may be useful in the preoperative period. The recommended test is TSH because 95% of the causes of hypothyroidism are of primary thyroid etiology.
No randomized study has demonstrated the benefit of patients with hypothyroidism being euthyroid in the preoperative period compared to hypothyroid and postoperative morbidity and mortality. Current evidence shows that if there is a prior diagnosis and time, the patient should be euthyroid in the preoperative period. However, if the patient has subclinical or mild hypothyroidism and the operation is urgent, the surgical procedure should not be postponed. In elective surgeries, treatment can begin, but we should not wait until TSH normalized.
Patients with clinical or moderate hypothyroidism and scheduled for urgent surgery should undergo the surgical procedure and initiate treatment in the immediate postoperative period. Patients with moderate hypothyroidism and elective surgeries should wait for euthyroidism to undergo the surgery. These patients do not necessarily need to achieve normalized TSH levels because 10 to 20% have a slow TSH decay. The most important criterion is that progressive increase and normalization of free T4 levels occur, which should exist within seven days, or treatment should continue to further increase the levels.
Patients with severe hypothyroidism or myxedema coma should only be operated if the surgery is an emergency. If the surgery is elective, previous treatment of hypothyroidism and acquisition of normal thyroid function should be considered. Treatment should be given in the form of T4 and T3. The doses used are as follows: T4 with an attack dose of 200-300 mcg intravenously, followed by 50 mcg per day; T3 dose of 5-20 mcg intravenously, followed by 2.5-10 mcg every 8 hours, depending on age and cardiovascular comorbidities.
In the postoperative period of any patient with hypothyroidism, if the patient does not resume eating in 5-7 days, 80% of the total dose of T4 should be given intravenously or intramuscularly once a day. The dose is 20% lower due to bioavailability.
II. Hyperthyroidism
Thyrotoxicosis affects 2% of women and 0.2% of men. The prevalence of clinical and subclinical hyperthyroidism in the USA is 0.2 and 1%, respectively. The most common causes are Graves-Basedow’s disease, toxic nodular goiter, thyroiditis, and iatrogenic. Adrenergic effects pose a high risk for perioperative complications, such as cardiac arrhythmias (8-15% AF). These are related to the increase in the number and/or sensitivity of β-adrenergic receptors. In addition, studies showed that more pronounced hyperthyroidism indicates greater chance of AF. The mortality in hyperthyroidism is related to the occurrence of cardiovascular events.513513 Mostbeck A, Galvan G, Bauer P, Eber O, Atefie K, Dam K, et al. The incidence of hyperthyroidism in Austria from 1987 to 1995 before and after an increase in salt iodization in 1990. Eur J Nucl Med. 1998;25(4):367-74.,517517 Graham GW, Unger BP, Coursin DB. Perioperative management of selected endocrine disorders. Int Anesthesiol Clin. 2000;38(4):31-67.
518 Murkin JM. Anesthesia and hypothyroidism: a review of thyroxine physiology, pharmacology, and anesthetic implications. Anesth Analg. 1982;61(4):371-83.
519 Bennett-Guerrero E, Kramer DC, Schwinn DA. Effect of chronic and acute thyroid hormone reduction on perioperative outcome. Anesth Analg. 1997;85(1):30-6.
520 Pronovost PH, Parris KH. Perioperative management of thyroid disease. Prevention of complications related to hyperthyroidism and hypothyroidism. Postgrad Med. 1995;98(2):83-6, 96-8.-521521 Stehling LC. Anesthetic management of the patient with hyperthyroidism. Anesthesiology. 1974;41(6):585-95.
For the diagnosis, there should be laboratory confirmation of clinical suspicion. TSH level should be low, and free T4 level should be normal (subclinical hyperthyroidism) or high. Several situations may increase the total T4 levels by increasing the T4-binding protein. However, they do not affect free T4, which has biological activity: pregnancy, cirrhosis, acromegaly, Cushing’s syndrome, use of lithium, contraceptives, propranolol, amiodarone, and iodinated contrast agents. In these situations, there is no real hyperthyroidism, only a compensatory increase in free T4, a consequence of the increase in TBG, a T4-binding protein.
II. C. Recommendations for Urgent or Emergency Surgical Procedures for Patients with Hyperthyreoidism
II. A. Clinical Manifestations in Hyperthyroid Patients with Perioperative Consequences
-
Cardiovascular: increased cardiac inotropism and chronotropism with decreased systemic vascular resistance (SVR), left ventricular hypertrophy, increased incidence of angina, HF, arrhythmias, and embolic events.
-
Hematologic: anemia, thrombocytopenia, neutropenia, increase of factor III, decrease of vitamin K-dependent factors, bleeding.
-
Gastrointestinal: inadequate absorption of drugs.
-
Metabolic/renal: hypercalcemia, hypoalbuminemia, ketoacidosis, increased drug clearance.
-
Pulmonary: myopathy with ventilatory dysfunction.
-
Endocrine: increased production and use of cortisol, glucose intolerance, weight loss, and protein catabolism.
II. D. Treatment of Thyrotoxic Storm
Treatment of thyrotoxic storm includes hydration, cooling, inotropes (if necessary), administration of PTU attack dose (1,000 mg oral) and maintenance (200 mg every 6 hours), ventilatory support, oral metabolic control, hydrocortisone attack dose of 300 mg intravenously and maintenance of 100 mg every 8 hours, iodine as oral Lugol or intravenous iodine at a dose of 1 g every 8 hours, and, if necessary, plasmapheresis, dialysis, or cholestyramine to remove hormones from the circulation.
C) Adrenal Insufficiency
Increased level of cortisol during acute stress is an important protective response. However, the metabolic stress caused by surgery can trigger acute adrenal insufficiency (AAI) in individuals with clinical and subclinical disorders. AAI affects the hypothalamic-pituitary-adrenal axis, and the results can be catastrophic, leading to multiple complications and even patient death.
Physical stress increases adrenocorticotropic hormone (ACTH) and cortisol secretion. The increase in cortisol, noradrenaline, and adrenaline levels characterize the stress-induced hormonal changes, minimal in small surgical stress and progressively higher in moderate and severe stress, lasting no more than 24 hours in uncomplicated interventions. The intraoperative period and mainly the anesthetic recovery and extubation periods are the major determinants for axis activation, with increases in plasma cortisol levels, which return to basal values in 24 to 48 hours.522522 Udelsman R, Norton JA, Jelenich SE, Goldstein DS, Linehan WM, Loriaux DL, et al. Responses of the hypothalamic-pituitary-adrenal and renin-angiotensin axes and the sympathetic system during controlled surgical and anesthetic stress. J Clin Endocrinol Metab. 1987;64(5):986-94. With the increasing demand for endogenous corticosteroids, individuals with impaired function and compromised adrenal reserve may have AAI. Thus, early identification of these individuals for adequate perioperative planning is essential to avoid complications.
I. Clinical Conditions of Primary Adrenal Insufficiency
Hypotension and hemodynamic shock (which may be resistant to vasopressors), with multiple organ dysfunction; hypoglycemia; tachycardia; hydroelectrolytic disorders: hyponatremia, hyperkalemia (in primary adrenal insufficiency - AI), hypercalcemia, acidosis; cardiac hypocontractility; anemia, eosinophilia, and neutropenia; nausea, vomiting, weakness, orthostatic hypotension, dehydration, abdominal or flank pain (acute adrenal hemorrhage), fatigue, weight loss; vitiligo, alteration of skin pigmentation, hypogonadism, hypothyroidism.
Diagnosis of AF should not be trusted if there is unexplained hypotension or refractory shock to volume and drugs in the intraoperative or postoperative period, discrepancy between disease severity and patient condition, high fever without apparent cause (negative cultures) or unresponsive to antibiotic therapy, unexplained mental changes, apathy, or depression without specific psychiatric disorder. In such cases, AAI should be initiated, and subsequent diagnostic confirmation should be obtained.
II. Identification of Patients at Risk for Adrenal Insufficiency
Patients with diagnosis of AI,523523 Oelkers W. Adrenal insufficiency. N Engl J Med. 1996;335(16):1206-12. patients at risk for AI524524 Grinspoon Sk MMEVEDCRM. Adrenocortical insufficiency - clinical aspects. In: Vaughn Edj CRM, editor. Adrenal disorders. New York: Thieme Medical; 1989. p. 171-89. and patients with relative hypoadrenalism (limited adrenocortical reserve): pituitary tumors (macroadenomas); radiation therapy of the pituitary region; previous pituitary surgical intervention; postoperative period of Cushing’s disease surgery, bilateral adrenalectomy or unilateral adrenalectomy in case of another adrenal attack; chronic corticosteroid users (> 5 mg of prednisone or equivalent for more than 21 days or dose > 7.5 mg for more than 14 days); patients with type 1 DM or autoimmune diseases (Hashimoto’s thyroiditis, ovarian or primary testicular failure, hypoparathyroidism, vitiligo, autoimmune polyglandular syndrome); individuals with suggestive clinical conditions (darkening of the skin, weakness, fatigue, nausea, vomiting, depression, hypotension, electrolytic imbalances, hypoglycemia, fever).
Evaluation of the hypothalamic-pituitary-adrenal axis for confirmation of AI should be made by measuring serum cortisol level at 8 AM. Perioperative corticosteroid replacement may be indicated depending on the result (Chart 17). If < 5 mcg/dL, replacement should be performed; 5-10 mcg/dL, perform simple cortrosyn test and measure serum ACTH levels to complement evaluation because it can be a false positive, that is, have an acute response and have no reserve. In this case, empirical therapy with steroids should be started. In cortisol level > 10 mcg /dL, replacement is not necessary.
IV. D. Treatment of AI Based on the Extent of the Surgery
-
Small (local anesthesia or hernia): maintain usual dose of corticoid in the morning without a new attack dose; maintain regular dose for 24 hours perioperatively.
-
Medium (total hip prosthesis): maintain regular dose of corticoid + 50 mg of hydrocortisone in bolus at induction; maintain regular dose for 24 hours perioperatively.
-
Large (colectomy, esophagectomy, peripheral revascularization, pancreatectomy): maintain regular dose of corticoid + 100 mg of hydrocortisone in bolus at induction; maintain 50 mg of hydrocortisone 8/8h in the 24-hour perioperative period.
IV. Recommendations for Doses of Corticoid Supplementation525525 Axelrod L. Perioperative management of patients treated with glucocorticoids. Endocrinol Metab Clin North Am. 2003;32(2):367-83.
526 Cooper MS, Stewart PM. Corticosteroid insufficiency in acutely ill patients. N Engl J Med. 2003;348(8):727-34.-527527 Salem M, Tainsh RE, Bromberg J, Loriaux DL, Chernow B. Perioperative glucocorticoid coverage. A reassessment 42 years after emergence of a problem. Ann Surg. 1994;219(4):416-25.
D) Obesity
Obesity has reached pandemic proportions. In Brazil, more than half of the population is overweight. According to the Risk and Protection Factors for Chronic Diseases by Telephone Survey (VIGITEL), 52.2% Brazilians are overweight.528528 Vigitel Brasil 2014: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção da Saúde. - Brasília : Ministério da Saúde, 2015. Approximately 30% of surgical patients are obese.
Obesity is related to several morbidities that influence perioperative evaluation and management, such as atherosclerotic disease, HF, systemic arterial hypertension, PH, DVT, and low functional capacity. Excess weight is also associated with problems in the respiratory system, such as reduced functional residual capacity, atelectasis, and pulmonary shunts. The association results in a risk of rapid desaturation due to the combination of high basal metabolic rate and oxygen demand. Furthermore, sleep disorders, such as obstructive apnea and alveolar hypoventilation, are special concerns in the perioperative period of the obese.
Weight is not only related to the greater risk of complications but also to the distribution of fat mass. Centripetal fat distribution (trunk and abdomen) is associated with metabolic syndrome, sleep disturbances, and unfavorable anatomy for intubation. Classifying the degree and type of obesity and screening for sleep-disordered breathing are essential steps to identify specific functional limitations and guide perioperative decisions.
The World Health Organization classifies obesity in grades: obesity grade 1: BMI 30-34.9 kg/m2; obesity grade 2: BMI 35-39.9 kg/m2; obesity grade 3: BMI ≥ 40 kg/m2. Classifications used in bariatric surgeries still categorize obesity in grades 4 and 5 when BMI exceeds 50 and 60 kg/m2, respectively.
The STOP-Bang questionnaire (Chart 18)529529 Chung F, Chau E, Yang Y, Liao P, Hall R, Mokhlesi B. Serum bicarbonate level improves specificity of STOP-Bang screening for obstructive sleep apnea. Chest. 2013;143(5):1284-93.,530530 Chung F, Subramanyam R, Liao P, Sasaki E, Shapiro C, Sun Y. High STOP-Bang score indicates a high probability of obstructive sleep apnoea. Br J Anaesth. 2012;108(5):768-75. is a validated tool to track sleep disorders in the preoperative evaluation of obese individuals. Scores from 5 to 8 identify patients with a high probability of moderate to severe obstructive sleep apnea.
I. Peculiarities in the Evaluation of Surgical Risk in Obese Patients217217 DeMaria EJ, Murr M, Byrne TK, Blackstone R, Grant JP, Budak A, et al. Validation of the obesity surgery mortality risk score in a multicenter study proves it stratifies mortality risk in patients undergoing gastric bypass for morbid obesity. Ann Surg. 2007;246(4):578-82.,531531 Poirier P, Alpert MA, Fleisher LA, Thompson PD, Sugerman HJ, Burke LE, et al; American Heart Association Obesity Committee of Council on Nutrition, Physical Activity and Metabolism, Council on Cardiopulmonary Perioperative and Critical Care, Council on Cardiovascular Surgery and Anesthesia, Council on Cardiovas. Cardiovascular evaluation and management of severely obese patients undergoing surgery: a science advisory from the American Heart Association. Circulation. 2009;120(1):86-95.
Clinical history limited by the difficulty to differentiate between dyspnea and cardiogenic and pulmonary origins of the low functional capacity of the obese. Physical examination and detailed analysis of the cardiopulmonary system is limited due to obesity. Few risk scores used in the perioperative evaluation include obesity and quantify the risk associated with this variable.
Higher prevalence of comorbidities that are risk factors for atherosclerosis and myocardial ischemia (hypertension, DM, and dyslipidemia); increased risk of thromboembolic events and infection of the surgical wound; greater difficulty in measuring blood pressure and acquiring venous access; longer mechanical ventilation time and longer hospitalization time; increased risk of renal failure; greater sensitivity to opioids and sedatives; increased risk of aspiration of gastric contents; higher probability of presenting hypoxemia due to hypoventilation, pulmonary restriction, postoperative atelectasis, increased occurrence of central and obstructive sleep apnea and hypercapnia; higher mortality in intensive care in severely obese patients. Specific regimens for venous thromboprophylaxis in obese patients are shown in table 12.
II. Specific Recommendations for Preoperative Evaluation in Elective Surgeries of Obese Patients531531 Poirier P, Alpert MA, Fleisher LA, Thompson PD, Sugerman HJ, Burke LE, et al; American Heart Association Obesity Committee of Council on Nutrition, Physical Activity and Metabolism, Council on Cardiopulmonary Perioperative and Critical Care, Council on Cardiovascular Surgery and Anesthesia, Council on Cardiovas. Cardiovascular evaluation and management of severely obese patients undergoing surgery: a science advisory from the American Heart Association. Circulation. 2009;120(1):86-95.
532 Chung F, Yegneswaran B, Liao P, Chung SA, Vairavanathan S, Islam S, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812-21.-533533 Schumann R, Jones SB, Ortiz VE, Connor K, Pulai I, Ozawa ET, et al. Best practice recommendations for anesthetic perioperative care and pain management in weight loss surgery. Obes Res. 2005;13(2):254-66.
III. Recommendations to Reduce the Risk of Obese Patients531531 Poirier P, Alpert MA, Fleisher LA, Thompson PD, Sugerman HJ, Burke LE, et al; American Heart Association Obesity Committee of Council on Nutrition, Physical Activity and Metabolism, Council on Cardiopulmonary Perioperative and Critical Care, Council on Cardiovascular Surgery and Anesthesia, Council on Cardiovas. Cardiovascular evaluation and management of severely obese patients undergoing surgery: a science advisory from the American Heart Association. Circulation. 2009;120(1):86-95.,533533 Schumann R, Jones SB, Ortiz VE, Connor K, Pulai I, Ozawa ET, et al. Best practice recommendations for anesthetic perioperative care and pain management in weight loss surgery. Obes Res. 2005;13(2):254-66.,535535 McCullough PA, Gallagher MJ, Dejong AT, Sandberg KR, Trivax JE, Alexander D, et al. Cardiorespiratory fitness and short-term complications after bariatric surgery. Chest. 2006;130(2):517-25.
536 Rocha AT, de Vasconcellos AG, da Luz Neto ER, Araújo DM, Alves ES, Lopes AA. Risk of venous thromboembolism and efficacy of thromboprophylaxis in hospitalized obese medical patients and in obese patients undergoing bariatric surgery. Obes Surg. 2006;16(12):1645-55.-537537 Stroh C, Birk D, Flade-Kuthe R, Frenken M, Herbig B, Höhne S, et al; Study Group Obesity Surgery. Evidence of thromboembolism prophylaxis in bariatric surgery-results of a quality assurance trial in bariatric surgery in Germany from 2005 to 2007 and review of the literature. Obes Surg. 2009;19(7):928-36.
E) Hematologic Diseases
I. Anemias
As doenças hematológicas podem aumentar a morbidade e aHematologic diseases may increase the morbidity and mortality of individuals submitted to surgical procedures. Anemia is the most common hematological problem found in the preoperative period. It is generally defined according to WHO criteria:540540 WHO. (1968) Nutritional anaemias. Report of a WHO scientific group. Geneva, World Health Organization, 1968. (WHO Technical Report Series, No.405). Available at http://whqlibdoc.who.int/trs/WHO_TRS_405.pdf1968.
http://whqlibdoc.who.int/trs/WHO_TRS_405...
,541541 WHO. (2011) Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva, World Health Organization, 2011 (WHO/NMH/NHD/MNM/11.1) Available from: http://www.who.int/vmnis/indicators/haemoglobin.pdf. 2011.
http://www.who.int/vmnis/indicators/haem...
hemoglobin concentration < 13 g/dL for men and < 12 g/dL for women. It is often a sign of underlying disease that can affect the surgical outcome. Studies involving many patients indicated that preoperative anemia is an independent risk factor for morbidity, mortality, and transfusion requirement, with an association between extent of anemia and outcome.542542 Pedersen AB, Mehnert F, Overgaard S, Johnsen SP. Allogeneic blood transfusion and prognosis following total hip replacement: a population-based follow up study. BMC Musculoskelet Disord. 2009;10:167.
543 Glance LG, Dick AW, Mukamel DB, Fleming FJ, Zollo RA, Wissler R, et al. Association between intraoperative blood transfusion and mortality and morbidity in patients undergoing noncardiac surgery. Anesthesiology. 2011;114(2):283-92.
544 Musallam KM, Tamim HM, Richards T, Spahn DR, Rosendaal FR, Habbal A, et al. Preoperative anaemia and postoperative outcomes in non-cardiac surgery: a retrospective cohort study. Lancet. 2011;378(9800):1396-407.
545 Ferraris VA, Davenport DL, Saha SP, Austin PC, Zwischenberger JB. Surgical outcomes and transfusion of minimal amounts of blood in the operating room. Arch Surg. 2012;147(1):49-55.-546546 Kotzé A, Harris A, Baker C, Iqbal T, Lavies N, Richards T, et al. British Committee for Standards in Haematology Guidelines on the Identification and Management of Pre-Operative Anaemia. Br J Haematol. 2015;171(3):322-31. Anemia leads to overload of the cardiovascular system, increasing cardiac output. Individuals with CD have less tolerance to anemia, and its presence can intensify the conditions of myocardial ischemia and underlying HF. Therefore, identification of anemia in the preoperative period assists in the identification of patients at risk of adverse outcome in the postoperative period. Whenever possible, anemia should be identified, investigated, and corrected before surgery, although there is no randomized evidence that its correction alters the perioperative risk. On the other hand, there is randomized evidence that the correction of anemia in the preoperative period decreases the need for blood transfusion and consequently the postoperative transfusion risk.546546 Kotzé A, Harris A, Baker C, Iqbal T, Lavies N, Richards T, et al. British Committee for Standards in Haematology Guidelines on the Identification and Management of Pre-Operative Anaemia. Br J Haematol. 2015;171(3):322-31.
The available guidelines for perioperative blood transfusion are limited, but the risks and benefits of this measure should always be questioned.547547 Patel MS, Carson JL. Anemia in the preoperative patient. Med Clin North Am. 2009;93(5):1095-104. Traditional practices, such as correction of preoperative anemia for normal or near-normal values of hemoglobin concentration (Hb ≥ 12 g/dL) to prepare patients for surgery, are not supported in the literature and are not recommended in clinical practice.546546 Kotzé A, Harris A, Baker C, Iqbal T, Lavies N, Richards T, et al. British Committee for Standards in Haematology Guidelines on the Identification and Management of Pre-Operative Anaemia. Br J Haematol. 2015;171(3):322-31.
Numerous studies and reviews have attempted to establish transfusion triggers for patients with anemia by evaluating two strategies: “restrictive” (usually Hb < 7.0 g/dL) and “liberal” (usually Hb ≥ 7.0 g/dL).548548 Carson JL, Carless PA, Hebert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012 Apr 18;(4):CD002042.
549 Holst LB, Petersen MW, Haase N, Perner A, Wetterslev J. Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of randomised trials with meta-analysis and trial sequential analysis. BMJ. 2015;350:h1354.
550 Fominskiy E, Putzu A, Monaco F, Scandroglio AM, Karaskov A, Galas FR, et al. Liberal transfusion strategy improves survival in perioperative but not in critically ill patients. A meta-analysis of randomised trials. Br J Anaesth. 2015;115(4):511-9.-551551 Docherty AB, O'Donnell R, Brunskill S, Trivella M, Doree C, Holst L, et al. Effect of restrictive versus liberal transfusion strategies on outcomes in patients with cardiovascular disease in a non-cardiac surgery setting: systematic review and meta-analysis. BMJ. 2016;352:i1351. Most meta-analyses included perioperative patients of various natures: critical and clinical patients, as well as adults and children. The meta-analysis of Carson et al.548548 Carson JL, Carless PA, Hebert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012 Apr 18;(4):CD002042. included 6,264 patients. These surgical and clinical patients involved adults and children. The authors concluded that the existing evidence supported the use of restrictive transfusion therapy in most patients, but that the effects of the restrictive strategy in high-risk groups, such as acute coronary syndrome, needed to be tested in future large studies. In the meta-analysis of Holst et al.,549549 Holst LB, Petersen MW, Haase N, Perner A, Wetterslev J. Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of randomised trials with meta-analysis and trial sequential analysis. BMJ. 2015;350:h1354. 9,813 patients from 31 randomized controlled trials were included. These trials consisted of twenty perioperative and acute blood loss studies, eight critical patient studies, two trauma studies, and one study with patients with leukemia undergoing bone marrow transplantation. According to the authors, the results were not affected by the inclusion of studies with high risk or unclear risk. The restrictive strategy was associated with the reduction in the number of transfused red cell concentrate units and the number of transfused patients; however, mortality, overall morbidity, and myocardial infarction remained unchanged. The restrictive strategy is safe in most clinical settings, and liberal transfusion does not show any benefit to the patients analyzed in this review.549549 Holst LB, Petersen MW, Haase N, Perner A, Wetterslev J. Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of randomised trials with meta-analysis and trial sequential analysis. BMJ. 2015;350:h1354.
In the meta-analysis of Docherty et al.,551551 Docherty AB, O'Donnell R, Brunskill S, Trivella M, Doree C, Holst L, et al. Effect of restrictive versus liberal transfusion strategies on outcomes in patients with cardiovascular disease in a non-cardiac surgery setting: systematic review and meta-analysis. BMJ. 2016;352:i1351. they specifically investigated the effect of restrictive versus liberal strategy in patients with CD undergoing noncardiac surgery. A total of 3,033 patients were included: 1,514 with restrictive transfusion and 1,519 with liberal transfusion. The risk of acute coronary syndrome was higher in patients with a restrictive strategy compared to patients with a liberal strategy, but the effects on mortality and other outcomes were uncertain in a period of 30 days. The authors concluded that it may not be safe to use a transfusion trigger below 8 g/dL in these patients.551551 Docherty AB, O'Donnell R, Brunskill S, Trivella M, Doree C, Holst L, et al. Effect of restrictive versus liberal transfusion strategies on outcomes in patients with cardiovascular disease in a non-cardiac surgery setting: systematic review and meta-analysis. BMJ. 2016;352:i1351.
Perioperative mortality in a period of 90 days was investigated in a recent review with meta-analysis, which included only perioperative adult patients and critically ill patients. Twenty-seven studies with 11,021 patients were included in the review: 17 in the perioperative period (9 in orthopedic surgery, 5 in cardiac, 1 in vascular, 1 in oncologic, and 1 in obstetric) and 10 in critically ill patients. Overall, there was no difference in mortality between the liberal and restrictive strategies. However, in the perioperative period, mortality was reduced in adult patients randomized to receive the liberal strategy compared to those who received the restrictive strategy with 7,552 patients. In critical patients, there was no difference between the groups. The heterogeneity between the studies was low. It was concluded that blood transfusion had a different statistically significant effect on the survival of patients in different clinical contexts.550550 Fominskiy E, Putzu A, Monaco F, Scandroglio AM, Karaskov A, Galas FR, et al. Liberal transfusion strategy improves survival in perioperative but not in critically ill patients. A meta-analysis of randomised trials. Br J Anaesth. 2015;115(4):511-9.
In an isolated study, Carson et al.552552 Carson JL, Terrin ML, Noveck H, Sanders DW, Chaitman BR, Rhoads GG, et al; FOCUS Investigators. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365(26):2453-62. included 2,016 patients aged ≥ 50 years. The patients had a history or risk factors for CD, with a hemoglobin concentration below 10 g/dL after hip surgery. They were randomized to liberal (transfusion trigger above 10 g/dL) or restrictive (symptoms of anemia or Hb < 8 g/dL) strategy to determine whether a higher transfusion trigger would improve the recovery of patients submitted to orthopedic hip fracture surgery. The authors concluded that the liberal and restrictive strategies did not reduce death rates, did not improve recovery in a period of 60 days of follow-up, and did not reduce hospital morbidity in older patients at high cardiovascular risk.552552 Carson JL, Terrin ML, Noveck H, Sanders DW, Chaitman BR, Rhoads GG, et al; FOCUS Investigators. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365(26):2453-62.
Another isolated study was conducted at John Hopkins Hospital including 10,163 patients submitted to vascular or gastrointestinal cardiothoracic surgery. The authors aimed to determine the transfusion practices and the effect of the use of transfusion on the perioperative outcome. They concluded that the use of the liberal transfusion trigger (Hb ≥ 7.0 g/dL) after major surgeries was more common than the restrictive practice (trigger < 7.0 g/dL) and that patients with restrictive transfusion had no increased risk of complications compared to patients with liberal transfusion.553553 Kim Y, Spolverato G, Lucas DJ, Ejaz A, Xu L, Wagner D, et al. Red cell transfusion triggers and postoperative outcomes after major surgery. J Gastrointest Surg. 2015;19(11):2062-73.
Recommendations for Perioperative Management In Patients with Sickle Cell Disease (SS/SC/Sβtal)556556 Vichinsky EP, Haberkern CM, Neumayr L, Earles AN, Black D, Koshy M, et al. A comparison of conservative and aggressive transfusion regimens in the perioperative management of sickle cell disease. The Preoperative Transfusion in Sickle Cell Disease Study Group. N Engl J Med. 1995;333(4):206-13.
557 Haberkern CM, Neumayr LD, Orringer EP, Earles AN, Robertson SM, Black D, et al. Cholecystectomy in sickle cell anemia patients: perioperative outcome of 364 cases from the National Preoperative Transfusion Study. Preoperative Transfusion in Sickle Cell Disease Study Group. Blood. 1997;89(5):1533-42.
558 Riddington C, Williamson L. Preoperative blood transfusions for sickle cell disease. Cochrane Database Syst Rev. 2001;(3):CD003149.
559 Lottenberg R, Hassell KL. An evidence-based approach to the treatment of adults with sickle cell disease. Hematology Am Soc Hematol Educ Program. 2005:58-65.
560 Yawn BP, Buchanan GR, Afenyi-Annan AN, Ballas SK, Hassell KL, James AH, et al. Management of sickle cell disease: summary of the 2014 evidence-based report by expert panel members. JAMA. 2014;312(10):1033-48. Erratum in: JAMA. 2014;312(18):1932. JAMA. 2015;313(7):729.-561561 Estcourt LJ, Fortin PM, Trivella M, Hopewell S. Preoperative blood transfusions for sickle cell disease. Cochrane Database Syst Rev. 2016 Apr 6;4:CD003149.
Therefore, the optimal transfusion trigger remains undetermined. Hemoglobin level is probably not the answer because some patients require higher values and others tolerate values lower than 7 g/dL.554554 Tisherman SA. Determining when patients need transfusions. JAMA Surg. 2015;150(10):956. The transfusion triggers used in isolated studies and in studies that were part of large reviews with meta-analysis are not homogeneous.
Therefore, the decision on blood transfusion should be based not only on hemoglobin levels, but also on the suspicion of organic ischemia, the risk or presence of bleeding, the status of the intravascular volume, and the susceptibility to complications due to inadequate oxygenation.555555 American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Practice guidelines for perioperative blood transfusion and adjuvant therapies: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Anesthesiology. 2006;105(1):198-208. Common sense, careful observation of the patient, and clinical context should guide the decision of the best strategy for each case. It should be noted that blood transfusion is not a risk-free procedure and that a dose-dependent relationship exists between transfusions and complications.545545 Ferraris VA, Davenport DL, Saha SP, Austin PC, Zwischenberger JB. Surgical outcomes and transfusion of minimal amounts of blood in the operating room. Arch Surg. 2012;147(1):49-55. Thus, even if selecting the liberal strategy, hemoglobin correction towards normal values is not necessary. One unit of erythrocyte concentrate increases the hemoglobin rate by approximately 1.0 g/dL and the hematocrit by approximately 3.0%. The optimal rate of administration of red blood cell concentrate should consider the clinical situation. Most patients can receive a packed red blood cell unit every one to two hours. Patients at risk of volume overload should receive 1.0 mL/kg/h. After transfusion of each unit, the patient should be reevaluated and the hemoglobin level must be determined.547547 Patel MS, Carson JL. Anemia in the preoperative patient. Med Clin North Am. 2009;93(5):1095-104.
II. Thrombocytopenia
Several studies have demonstrated a strong correlation between thrombocytopenia and hemorrhagic risk, as well as the effectiveness of platelet transfusion in reducing this risk. However, controversy still exists about the appropriate value to indicate for transfusion of platelet concentrates.562562 Squires JE. Indications for platelet transfusion in patients with thrombocytopenia. Blood Transfus. 2015;13(2):221-6. Patients scheduled for invasive surgical procedures may present benefits with a higher platelet count with 50,000 platelets/mm3.562562 Squires JE. Indications for platelet transfusion in patients with thrombocytopenia. Blood Transfus. 2015;13(2):221-6.
563 Hunt BJ, Allard S, Keeling D, Norfolk D, Stanworth SJ, Pendry K; British Committee for Standards in Haematology. A practical guideline for the haematological management of major haemorrhage. Br J Haematol. 2015;170(6):788-803.-564564 American Society of Anesthesiologists Task Force on Perioperative Blood Management. Practice guidelines for perioperative blood management: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Management*. Anesthesiology. 2015;122(2):241-75. In neurosurgeries, there is no evidence-based data to determine a safe minimum platelet count, with several consensuses indicating 100,000 platelets/mm3.565565 British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of platelets transfusions. Br J Haematol. 2003;122:10-23.
566 Johansson PI, Stensballe J. Hemostatic resuscitation for massive bleeding: the paradigm of plasma and platelets--a review of the current literature. Transfusion. 2010;50(3):701-10.-567567 Stroncek DF, Rebulla P. Platelet transfusions. Lancet. 2007;370(9585):427-38.
III. Hereditary Antiphospholipid Antibodies and Thrombophilias
Antiphospholipid antibodies are a family of autoantibodies directed against plasma phospholipid-binding proteins.569569 Barbhaiya M, Erkan D. Primary thrombosis prophylaxis in antiphospholipid antibody-positive patients: where do we stand? Curr Rheumatol Rep. 2011;13(1):59-69. Antiphospholipid syndrome is characterized by thrombosis (arterial and/or venous) and/or gestational morbidity in patients with persistent antiphospholipid antibodies.570570 Erkan D, Aguiar CL, Andrade D, Cohen H, Cuadrado MJ, Danowski A, et al. 14th International Congress on Antiphospholipid Antibodies: task force report on antiphospholipid syndrome treatment trends. Autoimmun Rev. 2014;13(6):685-96.
However, there are patients with a persistent presence of antiphospholipid antibodies without vaso-occlusive manifestations, only gestational morbidity and manifestations are not considered as criteria for the antiphospholipid syndrome (thrombocytopenia, livedo reticularis, cardiac valve disease).569569 Barbhaiya M, Erkan D. Primary thrombosis prophylaxis in antiphospholipid antibody-positive patients: where do we stand? Curr Rheumatol Rep. 2011;13(1):59-69. In addition, not every positive test for antiphospholipid antibodies is clinically significant and not every patient with positive antiphospholipid antibodies has the same thrombotic risk.569569 Barbhaiya M, Erkan D. Primary thrombosis prophylaxis in antiphospholipid antibody-positive patients: where do we stand? Curr Rheumatol Rep. 2011;13(1):59-69. To better estimate the thrombotic risk in patients with positive antiphospholipid antibody tests, some variables should be considered including persistently positive laboratory tests and presence of additional thrombotic risk factors.569569 Barbhaiya M, Erkan D. Primary thrombosis prophylaxis in antiphospholipid antibody-positive patients: where do we stand? Curr Rheumatol Rep. 2011;13(1):59-69.
Recommendations for Platelet Transfusion568568 Liumbruno GM, Bennardello F, Lattanzio A, Piccoli P, Rossetti G; Italian Society of Transfusion Medicine and Immunohaematology (SIMTI) Working Party. Recommendations for the transfusion management of patients in the peri-operative period. I. The pre-operative period. Blood Transfus. 2011;9(1):19-40.
Recommendations for Perioperative Use of Anticoagulants in Patients with Thrombophilia (Acquired or Hereditary)
Although several studies have evaluated thrombotic risk in asymptomatic patients with persistent antiphospholipid antibodies, most of them included patients with systemic lupus erythematosus. The annual risk of the first thrombotic event in these laboratory-positive individuals, but without other associated autoimmune diseases and other thrombotic risk factors, is low (less than 1% per year). In the presence of another autoimmune disease, the risk increases to less than 4% per year. Based on the hypothesis of the association of “two injuries”, antiphospholipid antibodies induce a prothrombotic and proinflammatory phenotype in endothelial cells that is not capable of causing thrombosis alone. However, the presence of a triggering event or “second injury”, such as infection, surgeries, estrogen use, and prolonged immobilization, may trigger a vaso-occlusive event.569569 Barbhaiya M, Erkan D. Primary thrombosis prophylaxis in antiphospholipid antibody-positive patients: where do we stand? Curr Rheumatol Rep. 2011;13(1):59-69.
Therefore, pharmacological antithrombotic prophylaxis is associated with mechanical measures in patients with positive antiphospholipid antibodies and in a period of greater vaso-occlusive risk (surgeries, immobilization, hospitalization).569569 Barbhaiya M, Erkan D. Primary thrombosis prophylaxis in antiphospholipid antibody-positive patients: where do we stand? Curr Rheumatol Rep. 2011;13(1):59-69. Patients with antiphospholipid syndrome under anticoagulant treatment have a higher thrombotic risk when submitted to surgical procedures.367367 Gould MK, Garcia DA, Wren SM, Karanicolas PJ, Arcelus JI, Heit JA, et al; American College of Chest Physicians. Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e227S-77S. Erratum in: Chest. 2012;141(5):1369.
The term thrombophilia describes the tendency to develop venous thromboembolism due to a state of hypercoagulability caused by the presence of inherited or acquired abnormalities of coagulation or fibrinolysis.571571 Martinelli I, De Stefano V, Mannucci PM. Inherited risk factors for venous thromboembolism. Nat Rev Cardiol. 2014;11(3):140-56. Hereditary thrombophilias do not present the same thrombotic risk. Severe thrombophilias are those resulting from deficiencies of natural anticoagulants (antithrombin, protein C, and protein S), abnormalities in homozygous, and presence of multiple defects. Presence of factor V Leiden in heterozygosity and the mutation G20210A in heterozygosis are considered mild thrombophilias. On the other hand, the presence of family history of venous thromboembolism events is a strong risk factor for venous thromboembolism, regardless of the presence of genetic alterations.571571 Martinelli I, De Stefano V, Mannucci PM. Inherited risk factors for venous thromboembolism. Nat Rev Cardiol. 2014;11(3):140-56. Documentation of the presence of an inherited thrombophilic alteration implies the need for primary anticoagulant prophylaxis in situations where an increased risk of venous thromboembolism exists, such as surgical procedures.571571 Martinelli I, De Stefano V, Mannucci PM. Inherited risk factors for venous thromboembolism. Nat Rev Cardiol. 2014;11(3):140-56.
IV. Hemophilia A (Factor Viii Deficiency) and B (Factor IX Deficiency)572572 Srivastava A, Brewer AK, Mauser-Bunschoten EP, Key NS, Kitchen S, Llinas A, et al; Treatment Guidelines Working Group on Behalf of The World Federation Of Hemophilia. Guidelines for the management of hemophilia. Haemophilia. 2013;19(1):e1-47.
Surgical procedures should be performed in conjunction with a team experienced in the treatment of hemophilia. Before performing the surgical procedure, ensure that sufficient concentrate of the deficient factor is available.
The procedures must be performed in a medical center with adequate laboratory support, with capacity to monitor the deficient factor. Preoperative laboratory evaluation should always include the search for inhibitors for the deficient factor;
The surgical procedure should be performed at the beginning of the week and at the beginning of the day to provide optimal laboratory and blood bank support. For the intraoperative period, the plasma level of the deficient factor should be corrected for hemostatically safe values through the use of specific factor concentrate.
In the postoperative period, maintain the plasma concentration of the deficient factor for adequate time and concentration according to the type and size of the surgery.
Efficacy of hemostasis should be assessed using the criteria defined by the International Society of Thrombosis and Hemostasis (ISTH).
V. Von Willebrand Disease573573 Nichols WL, Hultin MB, James AH, Manco-Johnson MJ, Montgomery RR, Ortel TL, et al. von Willebrand disease (VWD): evidence-based diagnosis and management guidelines, the National Heart, Lung, and Blood Institute (NHLBI) Expert Panel report (USA). Haemophilia. 2008;14(2):171-232.,574574 Laffan MA, Lester W, O'Donnell JS, Will A, Tait RC, Goodeve A, et al. The diagnosis and management of von Willebrand disease: a United Kingdom Haemophilia Centre Doctors Organization guideline approved by the British Committee for Standards in Haematology. Br J Haematol. 2014;167(4):453-65.
In the postoperative period, the minimum plasma levels of FVIII:C and von Willebrand factor:ristocetin cofactor (vWF:RCo) will vary according to the type and surgical extent.
F) Renal Failure
Patients with renal failure are more prone to postoperative complications, prolonged hospitalization time, higher costs during hospitalization, and higher mortality than those without renal dysfunction.4545 Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043-9.,575575 Dimick JB, Pronovost PJ, Cowan JA, Lipsett PA. Complications and costs after high-risk surgery: where should we focus quality improvement initiatives? J Am Coll Surg. 2003;196(5):671-8.
576 LeMaire SA, Miller CC 3rd, Conklin LD, Schmittling ZC, Köksoy C, Coselli JS. A new predictive model for adverse outcomes after elective thoracoabdominal aortic aneurysm repair. Ann Thorac Surg. 2001;71(4):1233-8.
577 O'Brien MM, Gonzales R, Shroyer AL, Grunwald GK, Daley J, Henderson WG, et al. Modest serum creatinine elevation affects adverse outcome after general surgery. Kidney Int. 2002;62(2):585-92.-578578 O'Hare AM, Feinglass J, Sidawy AN, Bacchetti P, Rodriguez RA, Daley J, et al. Impact of renal insufficiency on short-term morbidity and mortality after lower extremity revascularization: data from the Department of Veterans Affairs' National Surgical Quality Improvement Program. J Am Soc Nephrol. 2003;14(5):1287-95. Renal failure or preoperative dialysis has been consistently associated with postoperative complications and high mortality.
In preoperative evaluation, renal function can be assessed using the Cockroft-Gault formula, or glomerular filtration can be estimated using the MDRD equation. Estimated glomerular filtration of less than 60 mL/min /1.73 m22 Dunkelgrun M, Boersma E, Schouten O, Koopman-van Gemert AW, van Poorten F, Bax JJ, et al; Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Bisoprolol and fluvastatin for the reduction of perioperative cardiac mortality and myocardial infarction in intermediate-risk patients undergoing noncardiovascular surgery: a randomized controlled trial (DECREASE-IV). Ann Surg. 2009;249(6):921-6. is a risk factor for cardiac and noncardiac complications in the postoperative period and is associated with mortality up to two times higher compared to patients with normal renal function577577 O'Brien MM, Gonzales R, Shroyer AL, Grunwald GK, Daley J, Henderson WG, et al. Modest serum creatinine elevation affects adverse outcome after general surgery. Kidney Int. 2002;62(2):585-92.,578578 O'Hare AM, Feinglass J, Sidawy AN, Bacchetti P, Rodriguez RA, Daley J, et al. Impact of renal insufficiency on short-term morbidity and mortality after lower extremity revascularization: data from the Department of Veterans Affairs' National Surgical Quality Improvement Program. J Am Soc Nephrol. 2003;14(5):1287-95. Lee et al.4545 Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043-9. developed and validated a prognostic model for cardiovascular complications after noncardiac surgeries. The risk factors identified were (increasing risk) history of congestive HF, coronary ischemic disease, high risk surgery (abdominal aortic aneurysm, other vascular, thoracic, abdominal, and orthopedic surgeries), insulin-dependent DM, preoperative creatinine > 2.0 mg/dL, and cerebrovascular disease.
The development of acute renal injury (ARI) is a serious complication in the postoperative period and occurs, depending on the type of surgery, in 1-30% of the cases, with mortality around 50%.579579 Ea B. Epidemiologia. Insuficiência renal aguda: fisiopatologia, clínica e tratamento. Schor N SOBM, editor. São Paulo: Sarvier; 1997.
580 Chertow GM, Lazarus JM, Christiansen CL, Cook EF, Hammermeister KE, Grover F, et al. Preoperative renal risk stratification. Circulation. 1997;95(4):878-84.-581581 Lima EQ, Dirce MT, Castro I, Yu L. Mortality risk factors and validation of severity scoring systems in critically ill patients with acute renal failure. Ren Fail. 2005;27(5):547-56. There is evidence that small changes in serum creatinine are associated with increased morbidity and mortality in clinical and surgical patients.582582 Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, et al; Acute Kidney Injury Network. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31.
583 Barrantes F, Tian J, Vazquez R, Amoateng-Adjepong Y, Manthous CA. Acute kidney injury criteria predict outcomes of critically ill patients. Crit Care Med. 2008;36(5):1397-403.
584 Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365-70.-585585 Lassnigg A, Schmidlin D, Mouhieddine M, Bachmann LM, Druml W, Bauer P, et al. Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol. 2004;15(6):1597-605.
In the latest international guidelines, ARI is considered when a patient presents an increase of 0.3 mg/dL in serum creatinine in 48 hours or a 50% increase in baseline value within 7 days associated or not with the reduction of urinary volume to values below 0.5 mL/kg/h over a 6-hour period.586586 Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter, Suppl. 2012;2:1-138.
In a study with 75,952 noncardiac surgeries, the authors identified the following risk factors for ARI in the postoperative period: age ≥ 56 years, male, emergency surgery, intraperitoneal surgery, DM with oral medication or insulin, decompensated HF, hypertension, “mild” renal failure (preoperative creatinine between 1.2 and 1.9 mg/dL), and “moderate” renal failure (creatinine ≥ 2.0 mg/dL). Patients with 6 or more risk factors had an ARI incidence of 9% in the postoperative period and mortality eight times higher than the patients who did not present renal dysfunction.587587 Kheterpal S, Tremper KK, Heung M, Rosenberg AL, Englesbe M, Shanks AM, et al. Development and validation of an acute kidney injury risk index for patients undergoing general surgery: results from a national data set. Anesthesiology. 2009;110(3):505-15.
The prevention of ARI in the postoperative period depends on the following care: identifying risk factors for its development (mainly preoperative renal failure), avoiding the use of nephrotoxic drugs, maintaining adequate hydration, and avoiding hypotension. Even relatively short periods of intraoperative hypotension (MAP lower than 60 mmHg for more than 20 minutes or 55 mmHg for more than 10 minutes) are associated with an increased risk of ARI.588588 Sun LY, Wijeysundera DN, Tait GA, Beattie WS. Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. Anesthesiology. 2015;123(3):515-23.
Attempts to prevent ARI with drugs, such as diuretics and vasoactive amines, have not shown efficacy.589589 Lassnigg A, Donner E, Grubhofer G, Presterl E, Druml W, Hiesmayr M. Lack of renoprotective effects of dopamine and furosemide during cardiac surgery. J Am Soc Nephrol. 2000;11(1):97-104.,590590 Solomon R, Werner C, Mann D, D'Elia J, Silva P. Effects of saline, mannitol, and furosemide to prevent acute decreases in renal function induced by radiocontrast agents. N Engl J Med. 1994;331(21):1416-20. Potentially nephrotoxic drugs should be avoided or used appropriately with correction for the level of renal function. Aminoglycoside antibiotics, amphotericin B, radiological contrast, and non-hormonal anti-inflammatories are examples of nephrotoxic drugs commonly used in the perioperative period. The use of anti-inflammatories should be avoided, particularly in patients at risk: advanced age, previous renal failure, HF, dehydration, concomitant use of ACE inhibitors, and diuretics or other nephrotoxic agent.591591 Harris RC Jr. Cyclooxygenase-2 inhibition and renal physiology. Am J Cardiol. 2002;89(6A):10D-7D.,592592 Ott E, Nussmeier NA, Duke PC, Feneck RO, Alston RP, Snabes MC, et al; Multicenter Study of Perioperative Ischemia (McSPI) Research Group; Ischemia Research and Education Foundation (IREF) Investigators. Efficacy and safety of the cyclooxygenase 2 inhibitors parecoxib and valdecoxib in patients undergoing coronary artery bypass surgery. J Thorac Cardiovasc Surg. 2003;125(6):1481-92. ACE inhibitors and angiotensin II receptor blockers (ARBs) are potentially nephrotoxic drugs, and prescription should be evaluated in the perioperative period. In a recent work with orthopedic patients, use of ACE inhibitors or ARBs is associated with a higher risk of developing ARI in the postoperative period.593593 Bell S, Dekker FW, Vadiveloo T, Marwick C, Deshmukh H, Donnan PT, et al. Risk of postoperative acute kidney injury in patients undergoing orthopaedic surgery--development and validation of a risk score and effect of acute kidney injury on survival: observational cohort study. BMJ. 2015;351:h5639.
In the preoperative evaluation of patients with chronic renal failure on dialysis or renal transplants, some aspects are relevant. Many of these patients have known risk factors for coronary ischemic disease, such as advanced age, systemic arterial hypertension, or DM. Patients on a renal replacement therapy program should undergo dialysis before surgery to prevent hypervolemia, correct electrolyte and acid-base imbalances, and reduce the risk of bleeding due to uremia. In renal transplant patients, immunosuppression should be carefully adjusted by the nephrologist in the perioperative period because of the risk of acute rejection and nephrotoxicity.
The risk of postoperative complications is well defined in patients with renal failure. In these cases, the evaluation of the nephrologist should be considered. It should always be noted that creatinine is a poorly sensitive marker of renal function. Therefore, creatinine < 1.2 mg/dL does not necessarily mean normal renal function, particularly in elderly patients or patients with reduced muscle mass. The preoperative evaluation is an opportunity to communicate with the patient and the clinical-surgical team to define measures to prevent deterioration of renal function and for subsequent follow-up aimed at delaying the progression of chronic renal failure.
G) Pulmonary Hypertension
PH is a clinical condition that results from increased right ventricular afterload, leading to pressure increase in the pulmonary vascular territory and progressive right ventricular dysfunction.594594 Ventetuolo CE, Klinger JR. Management of acute right ventricular failure in the intensive care unit. Ann Am Thorac Soc. 2014;11(5):811-22.,595595 Hoeper MM, Bogaard HJ, Condliffe R, Frantz R, Khanna D, Kurzyna M, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D42-50. The diagnosis of PH involves right chamber catheterization and measurement of pulmonary artery pressure. Hypertensive condition is defined by a mean pulmonary arterial pressure (PAPm) greater than or equal to 25 mmHg.596596 Costa EL, Jardim C, Bogossian HB, Amato MB, Carvalho CR, Souza R. Acute vasodilator test in pulmonary arterial hypertension: evaluation of two response criteria. Vascul Pharmacol. 2005;43(3):143-7.
There are several mechanisms or clinical conditions that can lead to PH from direct involvement of the pulmonary vasculature to left heart disease, pulmonary parenchymal diseases, or even associated with chronic PTE.597597 Gavilanes F, Alves Jr JL, Fernandes C, Prada LF, Jardim CV, Morinaga LT, et al. Left ventricular dysfunction in patients with suspected pulmonary arterial hypertension. J Bras Pneumol. 2014;40(6):609-16.,598598 Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D34-41. Erratum in: J Am Coll Cardiol. 2014;63(7):746.
The pathophysiology of the decompensation of PH depends on the functional characteristics of the right ventricle. Due to the normal mechanical features of the pulmonary circulation (high complacency and low resistance), there is no tolerance for afterloading increases. The increase of the afterload generates distension of the free wall of the RV and consequent decoupling of the muscular fibers (Frank-Starling’s Law), impairing the efficiency of the RV systole.594594 Ventetuolo CE, Klinger JR. Management of acute right ventricular failure in the intensive care unit. Ann Am Thorac Soc. 2014;11(5):811-22.,599599 Hoeper MM, Granton J. Intensive care unit management of patients with severe pulmonary hypertension and right heart failure. Am J Respir Crit Care Med. 2011;184(10):1114-24.,600600 Green EM, Givertz MM. Management of acute right ventricular failure in the intensive care unit. Curr Heart Fail Rep. 2012;9(3):228-35.
There are several causes of RV failure including natural evolution of PH, regardless of the underlying cause, as well as other decompensations, such as infectious cardiac arrhythmias601601 Tongers J, Schwerdtfeger B, Klein G, Kempf T, Schaefer A, Knapp JM, et al. Incidence and clinical relevance of supraventricular tachyarrhythmias in pulmonary hypertension. Am Heart J. 2007;153(1):127-32. and surgical stress.602602 Minai OA, Yared JP, Kaw R, Subramaniam K, Hill NS. Perioperative risk and management in patients with pulmonary hypertension. Chest. 2013;144(1):329-40.
The surgical procedure is related to significant morbidity and mortality in patients with PH.603603 Kosarek L, Fox C, Baluch AR, Kaye AD. Pulmonary hypertension and current anesthetic implications. Middle East J Anaesthesiol. 2009;20(3):337-46.,604604 Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J. 2015;46(4):903-75. Erratum in: Eur Respir J. 2015;46(6):1855-6 Mortality is estimated between 4% and 24% in several cases, depending on the stage of the disease and the surgical procedure that the patient underwent.605605 Blaise G, Langleben D, Hubert B. Pulmonary arterial hypertension: pathophysiology and anesthetic approach. Anesthesiology. 2003;99(6):1415-32. When only cardiac surgeries are considered, mortality is higher than 25%, because there is a high risk of ischemia and RV dysfunction, particularly at the time of cardiopulmonary bypass.602602 Minai OA, Yared JP, Kaw R, Subramaniam K, Hill NS. Perioperative risk and management in patients with pulmonary hypertension. Chest. 2013;144(1):329-40.
During surgery, several factors may impair RV function due to reduction of coronary perfusion with consequent ischemia and elevation of pulmonary vascular resistance (PVR), leading to increased afterload (Chart 19).602602 Minai OA, Yared JP, Kaw R, Subramaniam K, Hill NS. Perioperative risk and management in patients with pulmonary hypertension. Chest. 2013;144(1):329-40.
Ideally, perioperative evaluation of these patients should be performed by a multidisciplinary team. The need for the surgery in question should be carefully evaluated, considering the risks and benefits and avoiding emergency procedures that may increase morbidity and mortality.
Preoperative evaluation is complex because it should include assessment of baseline conditions related to the genesis of PH, as well as the associated hemodynamics. In this manner, evaluation is based on clinical data obtained with chest X-ray, pulmonary function test, ECG, echocardiogram, and measurement of biomarkers, such as BNP.
Performing right cardiac catheterization to effectively assess ventricular function through direct measurement of cardiac output, as well as levels of atrial and ventricular filling pressures, may be required, depending on the clinical condition of the patient and the procedure to be performed. This comprehensive evaluation aims to better control PH, with optimization of diuretic therapy, as well as the use of specific medications in patients with pulmonary arterial hypertension.602602 Minai OA, Yared JP, Kaw R, Subramaniam K, Hill NS. Perioperative risk and management in patients with pulmonary hypertension. Chest. 2013;144(1):329-40.
Some specific conditions deserve particular attention. Patients with chronic PTE should maintain anticoagulant therapy throughout the perioperative period. The transition from oral anticoagulants to anticoagulants with a known half-life (e.g., enoxaparin or UFH in an infusion pump) is recommended. As for anticoagulated patients, due to pulmonary arterial hypertension, the perioperative suspension of this medication does not imply an additional risk and can be performed aiming at greater procedural safety.602602 Minai OA, Yared JP, Kaw R, Subramaniam K, Hill NS. Perioperative risk and management in patients with pulmonary hypertension. Chest. 2013;144(1):329-40.,603603 Kosarek L, Fox C, Baluch AR, Kaye AD. Pulmonary hypertension and current anesthetic implications. Middle East J Anaesthesiol. 2009;20(3):337-46. In these patients, the use of specific drugs to control PH, such as endothelin receptor antagonists, phosphodiesterase type 5 inhibitors, and prostanoids, should be maintained; if necessary, substitution with inhaled or intravenous formulations is possible.602602 Minai OA, Yared JP, Kaw R, Subramaniam K, Hill NS. Perioperative risk and management in patients with pulmonary hypertension. Chest. 2013;144(1):329-40.,604604 Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J. 2015;46(4):903-75. Erratum in: Eur Respir J. 2015;46(6):1855-6
Regional anesthesia (blocks or epidural) is apparently better tolerated in patients with PH than general anesthesia.606606 Meyer S, McLaughlin VV, Seyfarth HJ, Bull TM, Vizza CD, Gomberg-Maitland M, et al. Outcomes of noncardiac, nonobstetric surgery in patients with PAH: an international prospective survey. Eur Respir J. 2013;41(6):1302-7. In the intraoperative period, care must be taken to manage the fluids administered (avoiding excess or lack of volume, which may deteriorate cardiac output), as well as analgesic control. Hypotension should be avoided to maintain adequate coronary perfusion of the RV. For this, monitoring with invasive blood pressure and pulmonary artery catheter is useful, as well as vasoactive drugs that maintain SVR without significantly interfering with PVR.602602 Minai OA, Yared JP, Kaw R, Subramaniam K, Hill NS. Perioperative risk and management in patients with pulmonary hypertension. Chest. 2013;144(1):329-40.,603603 Kosarek L, Fox C, Baluch AR, Kaye AD. Pulmonary hypertension and current anesthetic implications. Middle East J Anaesthesiol. 2009;20(3):337-46.
Mechanical ventilation during the surgical procedure should be protective with low tidal volume (6 mL/kg with steady pressure < 30 cmH2O), avoiding hypoxia. It must give preference to the management of FiO2 over the increase of PEEP, not to compromise venous return and decrease RV preload, as well as a potential increase in PVR.602602 Minai OA, Yared JP, Kaw R, Subramaniam K, Hill NS. Perioperative risk and management in patients with pulmonary hypertension. Chest. 2013;144(1):329-40. It is possible to use inhaled nitric oxide considering its short half-life, low repercussion in systemic hemodynamics, and significant auxiliary role in the control of PVR.596596 Costa EL, Jardim C, Bogossian HB, Amato MB, Carvalho CR, Souza R. Acute vasodilator test in pulmonary arterial hypertension: evaluation of two response criteria. Vascul Pharmacol. 2005;43(3):143-7.
Considering all the complexity related to the right ventricular dysfunction, patients with PH scheduled for noncardiac operations should have the preoperative evaluation and surgical procedure preferably performed in a specialized center for the treatment of various forms of PH.5353 Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleischmann KE, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery); American Society of Echocardiography.; American Society of Nuclear Cardiology; Heart Rhythm Society; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society for Vascular Medicine and Biology; Society for Vascular Surgery. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery): developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. Circulation. 2007;116(17):e418-99. Erratum in: Circulation. 2008;117(5):e154. Circulation. 2008;118(9): e143-4.
H) Asthma and Chronic Obstructive Pulmonary Disease
Perioperative pulmonary complications largely contribute to perioperative morbidity and mortality. Some series estimate that pulmonary complications may be present in up to 70% of cases in the postoperative period, depending on the type of surgery and clinical profile of the patient.607607 Wightman JA. A prospective survey of the incidence of postoperative pulmonary complications. Br J Surg. 1968;55(2):85-91.,608608 Mohr DN, Jett JR. Preoperative evaluation of pulmonary risk factors. J Gen Intern Med. 1988;3(3):277-87. In addition, pulmonary complications are among the ones that increase hospitalization costs and lead to longer hospitalization.608608 Mohr DN, Jett JR. Preoperative evaluation of pulmonary risk factors. J Gen Intern Med. 1988;3(3):277-87.
The definition of postoperative pulmonary complication greatly varies. The most common are atelectasis, infections (including acute bronchitis and pneumonia), prolonged mechanical ventilation and respiratory failure, exacerbation of chronic lung disease, and bronchospasm.609609 Hall JC, Tarala RA, Hall JL, Mander J. A multivariate analysis of the risk of pulmonary complications after laparotomy. Chest. 1991;99(4):923-7.,610610 Gracey DR, Divertie MB, Didier EP. Preoperative pulmonary preparation of patients with chronic obstructive pulmonary disease: a prospective study. Chest. 1979;76(2):123-9.
Risk factors related to patients that are associated with a higher incidence of pulmonary complications are diagnosis of COPD, asthma, active smoking, obstructive sleep apnea, PH, and upper airway infection.607607 Wightman JA. A prospective survey of the incidence of postoperative pulmonary complications. Br J Surg. 1968;55(2):85-91.,611611 Kroenke K, Lawrence VA, Theroux JF, Tuley MR, Hilsenbeck S. Postoperative complications after thoracic and major abdominal surgery in patients with and without obstructive lung disease. Chest. 1993;104(5):1445-51.
612 Price LC, Montani D, Jaïs X, Dick JR, Simonneau G, Sitbon O, et al. Noncardiothoracic nonobstetric surgery in mild-to-moderate pulmonary hypertension. Eur Respir J. 2010;35(6):1294-302.-613613 Tait AR, Malviya S. Anesthesia for the child with an upper respiratory tract infection: still a dilemma? Anesth Analg. 2005;100(1):59-65. Regarding the factors associated with the procedure, the surgical site should be emphasized (the closer to the diaphragm, the greater the risk of complications),610610 Gracey DR, Divertie MB, Didier EP. Preoperative pulmonary preparation of patients with chronic obstructive pulmonary disease: a prospective study. Chest. 1979;76(2):123-9. but also the duration of the procedure (greater risk with surgeries lasting more than 3 to 4 hours),614614 Brooks-Brunn JA. Predictors of postoperative pulmonary complications following abdominal surgery. Chest. 1997;111(3):564-71. type of anesthesia (general anesthesia with a greater risk than neuroaxial block)615615 Rodgers A, Walker N, Schug S, McKee A, Kehlet H, van Zundert A, et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ. 2000;321(7275):1493. and type of neuromuscular blocker (pancuronium associated with a higher incidence of posterior neuromuscular block than agents with a less prolonged effect).616616 Berg H, Roed J, Viby-Mogensen J, Mortensen CR, Engbaek J, Skovgaard LT, et al. Residual neuromuscular block is a risk factor for postoperative pulmonary complications. A prospective, randomised, and blinded study of postoperative pulmonary complications after atracurium, vecuronium and pancuronium. Acta Anaesthesiol Scand. 1997;41(9):1095-103.
There is a significant difference in the evaluation of patients scheduled for pulmonary resection and patients scheduled for other types of surgery. In the first group, pulmonary function tests, arterial blood gas analysis, chest imaging exams, and cardiopulmonary tests are fundamental.611611 Kroenke K, Lawrence VA, Theroux JF, Tuley MR, Hilsenbeck S. Postoperative complications after thoracic and major abdominal surgery in patients with and without obstructive lung disease. Chest. 1993;104(5):1445-51. Risk predictors, such as ARISCAT, Arozullah, and Gupta, can be used to estimate perioperative pulmonary complications of surgeries without pulmonary resection.617617 Canet J, Gallart L, Gomar C, Paluzie G, Vallès J, Castillo J, et al; ARISCAT Group. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338-50.
618 Arozullah AM, Khuri SF, Henderson WG, Daley J; Participants in the National Veterans Affairs Surgical Quality Improvement Program. Development and validation of a multifactorial risk index for predicting postoperative pneumonia after major noncardiac surgery. Ann Intern Med. 2001;135(10):847-57.-619619 Gupta H, Gupta PK, Fang X, Miller WJ, Cemaj S, Forse RA, et al. Development and validation of a risk calculator predicting postoperative respiratory failure. Chest. 2011;140(5):1207-15.
ARISCAT risk score for estimation of postoperative pulmonary complications617617 Canet J, Gallart L, Gomar C, Paluzie G, Vallès J, Castillo J, et al; ARISCAT Group. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338-50.
The simplest table is ARISCAT617617 Canet J, Gallart L, Gomar C, Paluzie G, Vallès J, Castillo J, et al; ARISCAT Group. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338-50. that predicts the general incidence of postoperative complications (any severity). In this table, independent risk factors receive a weighted score, producing risk ranges for postoperative complications: 0 to 25 points: low risk, 1.6% complication rate; 26 to 44 points: intermediate risk, 13.3% complication rate; and 45 to 123 points: high risk, 42.1% complication rate (Table 13).
Regarding management to reduce pulmonary complications, the recommendations are similar to those outside the surgical context aimed at optimizing pulmonary function and minimizing the occurrence of respiratory complications. Optimization of pulmonary function includes the use of antibiotics when active infection is observed, as well as the use of corticosteroids and/or bronchodilators in patients already taking these drugs or who present residual bronchospasm. Smoking cessation should be recommended preferably more than two months before the surgical procedure.
Specialized physiotherapy care and follow-up are important in this context. Education of the patient regarding pulmonary expansion exercises is fundamental since the preoperative period. In a systematic review of the literature conducted in 2016, the approach with postoperative pulmonary expansion exercises was the only strategy with a Level of evidence A for the reduction of pulmonary complications.620620 Lawrence VA, Cornell JE, Smetana GW; American College of Physicians. Strategies to reduce postoperative pulmonary complications after noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med. 2006;144(8):596-608.
In summary, there is no recommendation for specific reduction of perioperative cardiac complications in patients with COPD/Asthma.
I) Smoking
Smoking is the main avoidable cause of death worldwide. It contributes directly to at least 20% of all deaths, and about 200,000 deaths per year in Brazil. Hospitalizations are an opportunity to sensitize patients to quit smoking, as well as to facilitate monitoring of symptoms of nicotine withdrawal and close follow-up of tolerance and efficacy of treatments eventually established.
Reduction of mortality risks and various postoperative complications in smoking is also focused in the perioperative care management, given the significant effect of smoking on postoperative healing, infection rates, surgical bleeding, pain control, and respiratory, cardiocirculatory, and orthopedic complications, among others. History of smoking is associated with longer stays in ICU in the postoperative period and longer hospitalizations.621621 Moores LK. Smoking and postoperative pulmonary complications. An evidence-based review of the recent literature. Clin Chest Med. 2000;21(1):139-46, ix-x.
622 Møller AM, Maaløe R, Pedersen T. Postoperative intensive care admittance: the role of tobacco smoking. Acta Anaesthesiol Scand. 2001;45(3):345-8.
623 Delgado-Rodriguez M, Medina-Cuadros M, Martínez-Gallego G, Gómez-Ortega A, Mariscal-Ortiz M, Palma-Pérez S, et al. A prospective study of tobacco smoking as a predictor of complications in general surgery. Infect Control Hosp Epidemiol. 2003;24(1):37-43.
624 Bettin CC, Gower K, McCormick K, Wan JY, Ishikawa SN, Richardson DR, et al. Cigarette smoking increases complication rate in forefoot surgery. Foot Ankle Int. 2015;36(5):488-93.
625 McCunniff PT, Young ES, Ahmadinia K, Ahn UM, Ahn NU. Smoking is associated with increased blood loss and transfusion use after lumbar spinal surgery. Clin Orthop Relat Res. 2016;474(4):1019-25.-626626 Lau D, Berger MS, Khullar D, Maa J. The impact of smoking on neurosurgical outcomes. J Neurosurg. 2013;119(5):1323-30. Despite this, discussion about smoking during the preoperative preparation of the patient is mostly absent, which is partly due to the lack of knowledge of the doctors on the ideal timing for cessation of smoking. Recognizing the right time during a surgical risk assessment to address the issue of smoking and initiating treatment as early as possible can have significant reductions in clinical and surgical complications and lower costs to the health system.
I. Cessation of Smoking During Hospitalization
Cessation of smoking during hospitalization offers an opportunity to access withdrawal symptoms more readily, titer medication doses more safely, and monitor the effectiveness of the therapeutic program more reliably.
The reasons that drive patients to stop smoking during hospitalization, which are part of health treatment or merely resulting from the condition of staying in a tobacco-free environment, should be seen as an important step. Measures of support and follow-up indispensable for the patient to remain abstinent should be implemented.
If such efforts are not organized in a structured program that involves the identification of smokers at the time of hospitalization, the medical center responsible for therapeutic interventions (informational, cognitive-behavioral, and medication), follow-up during hospitalization, and post-discharge follow-up, such efforts become ineffective in the medium and long term.
II. Cessation of Smoking in the Preoperative Period
The negative effects of smoking on surgical outcomes are multifactorial. However, they are mainly due to the direct effects of nicotine carbon monoxide (CO) and increased oxidative and inflammatory stress. CO and nicotine increase heart rate, blood pressure, and tissue oxygen demand, as well as decrease oxygen transport capacity. Because of the vasoconstricting effect of nicotine, it increases the risk of tissue ischemia in surgery and in other areas, such as the coronary artery.627627 Rejali M, Rejali AR, Zhang L. Effects of nicotine on the cardiovascular system. Vasc Dis Prev. 2005;2:135-44.
The irritant and proinflammatory effect of numerous components of cigarette smoke on the airways also increase the susceptibility of smoking patients to respiratory infections, local healing complications in lung surgeries, and longer periods under mechanical ventilation.628628 Ngaage DL, Martins E, Orkell E, Griffin S, Cale AR, Cowen ME, et al. The impact of the duration of mechanical ventilation on the respiratory outcome in smokers undergoing cardiac surgery. Cardiovasc Surg. 2002;10(4):345-50.
Smoking is also associated with the need for higher doses of anesthetics and neuromuscular blockers,629629 Teiriä H, Rautoma P, Yli-Hankala A. Effect of smoking on dose requirements for vecuronium. Br J Anaesth. 1996;76(1):154-5. increased incidence of thromboembolic events, and slower repair processes in orthopedic surgeries.630630 Sherwin MA, Gastwirth CM. Detrimental effects of cigarette smoking on lower extremity wound healing. J Foot Surg. 1990;29(1):84-7.
Patients scheduled for surgeries are usually more motivated to quit smoking and are thus susceptible to a therapeutic approach to quit smoking. With the regulation of hospitals (and other enclosed spaces for public and private use) as tobacco-free environments, and with the increasing availability of effective therapeutic resources to help the patient to stop smoking, the preoperative period becomes a perfect time to stop smoking before elective surgical hospitalization.
The ideal time to stop smoking before surgery had been controversial. This was partly due to the great methodological heterogeneity of studies that evaluated the different periods to stop smoking, the difficulty of controlling confounding variables in the samples of patients, the great variation in the postoperative follow-up time, and the multiplicity of outcomes studied.
A review of prospective studies on the impact of smoking cessation in the preoperative period on the occurrence of postoperative complications (respiratory, infectious, general mortality and length of hospital stay) was conducted by Cropley and Theadom.631631 Theadom A, Cropley M. Effects of preoperative smoking cessation on the incidence and risk of intraoperative and postoperative complications in adult smokers: a systematic review. Tob Control. 2006;15(5):352-8. They concluded that although there is great methodological limitation of the studies evaluated, there are several benefits of smoking cessation before surgical hospitalizations. They reported that longer abstinence period results in greater benefit. It should also be mentioned that there is no ideal period to recommend preoperative smoking abstinence, in terms of reduction of surgical complications and risk in the medium and long term. Cessation of smoking should not be postponed due to the unsustainable assumption that risk increases when cessation occurs less than two months before surgery.
In 2009, a retrospective cohort study evaluated data from 7,990 lung resection surgeries due to neoplasia. The study concluded that the risks of in-hospital mortality and respiratory complications after lung resection were higher in smokers and clearly reduced by smoking cessation in the preoperative period. The ideal interval between cessation of smoking and surgery could not be identified, which reinforced the recommendation for counseling (and treatment) for smoking cessation, regardless of the proximity of the surgery. This corroborates the results presented in the study published in 2001 by Nakagawa et al.632632 Nakagawa M, Tanaka H, Tsukuma H, Kishi Y. Relationship between the duration of the preoperative smoke-free period and the incidence of postoperative pulmonary complications after pulmonary surgery. Chest. 2001;120(3):705-10. They found a clear and increasing reduction in the risk of postoperative complications after four weeks of preoperative smoking cessation.
III. Therapeutic Strategies
As in general situations, the treatment of nicotine dependence in patients scheduled for surgery and in hospitalized patients is based on cognitive-behavioral interventions (brief approach, individual counseling, provision of informational materials, and group therapy), systematized or not, and in the pharmacological support.
Regarding the “intensity” of the non-pharmacological approach, a systematic review published in 2012 evaluated several studies in hospitalized patients.633633 Rigotti NA, Clair C, Munafò MR, Stead LF. Interventions for smoking cessation in hospitalised patients. Cochrane Database Syst Rev. 2012 May 16;(5):CD001837. The study showed a dose-response relationship between the intervention and the cessation rate. Moreover, structured counseling programs initiated at the hospital and extended for at least one month after discharge are more effective compared to single-point approaches during hospitalization (RR 1.37; 95% CI 1.27-1.48; 25 studies).
Prospective studies evaluating the effectiveness of implementing a structured counseling, cognitive-behavioral approach, pharmacologic support, and post-discharge follow-up of hospitalized smokers showed success rates of about 35-44% in six months634634 Simon JA, Carmody TP, Hudes ES, Snyder E, Murray J. Intensive smoking cessation counseling versus minimal counseling among hospitalized smokers treated with transdermal nicotine replacement: a randomized trial. Am J Med. 2003;114(7):555-62.,635635 Reid RD, Pipe AL, Quinlan B. Promoting smoking cessation during hospitalization for coronary artery disease. Can J Cardiol. 2006;22(9):775-80. and approximately 33% after 12 months, with studies showing success rates above 50% after one year in hospitalized coronary patients.636636 Smith PM, Burgess E. Smoking cessation initiated during hospital stay for patients with coronary artery disease: a randomized controlled trial. CMAJ. 2009;180(13):1297-303.
Given the need to specify, in cases of surgical and hospitalized patients, cessation of smoking and the control of nicotine withdrawal symptoms in a shorter period, nicotine replacement therapy (NRT), isolated or combined, is the most frequent approach selected. The usual transdermal nicotine prescription schemes (6 to 8 weeks of 21 mg/24h or 15 mg/16h, 2 weeks of 14 mg/24h or 10 mg/16h and 2 weeks of 7 mg/24h or 5 mg/16h, depending on the presentation selected) are recommended, in association with rapid forms of ad libitum replacement (in Brazil, chewing gum and tablets are available, both in presentations of 2 and 4 mg per unit) for craving episodes. The addition of NRT to an intensive counseling intervention (more than one session, post-discharge) increased smoking cessation rates compared to intensive counseling alone (RR 1.54, 95% CI 1.34-1, 79, six studies).637637 Mazza R, Lina M, Boffi R, Invernizzi G, De Marco C, Pierotti M. Taking care of smoker cancer patients: a review and some recommendations. Ann Oncol. 2010;21(7):1404-9.
The same systematic review did not show evidence of benefit of adding bupropion (RR 1.04, 95% CI 0.75-1.45, three studies) or varenicline (RR 1.29, 95% CI 0.95-1.76, two studies) to intensive counseling. Regarding bupropion, new studies, such as the randomized placebo-controlled trial conducted by Eisenberg et al.,638638 Eisenberg MJ, Grandi SM, Gervais A, O'Loughlin J, Paradis G, Rinfret S, et al; ZESCA Investigators. Bupropion for smoking cessation in patients hospitalized with acute myocardial infarction: a randomized, placebo-controlled trial. J Am Coll Cardiol. 2013;61(5):524-32. failed to demonstrate the superiority of bupropion over placebo in hospitalized patients. In the same year, a study published by Smith et al.639639 Smith BJ, Carson KV, Brinn MP, Labiszewski NA, Peters MJ, Fitridge R, et al. Smoking Termination Opportunity for inPatients (STOP): superiority of a course of varenicline tartrate plus counselling over counselling alone for smoking cessation: a 12-month randomised controlled trial for inpatients. Thorax. 2013;68(5):485-6. evaluated the addition of varenicline to counseling through a randomized, placebo-controlled, protocol. The result showed a significant superiority of pharmacological intervention compared to the control group (RR 1.45; 95% CI 1.03-2.03; p = 0.03).
Although there is potential benefit of other pharmacological approaches to smoking cessation in hospitalized patients, NRT remains the standard of care at the same doses and schemes normally recommended for other clinical situations. The use of customized doses (above 21 mg/day) of nicotine replacement to reach plasma levels of nicotine closer to the arterial concentrations of an active smoker and aimed at better control of withdrawal symptoms in heavy smokers has been tested and is safe up to doses higher than 42 mg per day,640640 Dale LC, Hurt RD, Offord KP, Lawson GM, Croghan IT, Schroeder DR. High-dose nicotine patch therapy. Percentage of replacement and smoking cessation. JAMA. 1995;274(17):1353-8.
641 Hatsukami D, Mooney M, Murphy S, LeSage M, Babb D, Hecht S. Effects of high dose transdermal nicotine replacement in cigarette smokers. Pharmacol Biochem Behav. 2007;86(1):132-9.
642 Zevin S, Jacob P 3rd, Benowitz NL. Dose-related cardiovascular and endocrine effects of transdermal nicotine. Clin Pharmacol Ther. 1998;64(1):87-95.-643643 Benowitz NL, Zevin S, Jacob P 3rd. Suppression of nicotine intake during ad libitum cigarette smoking by high-dose transdermal nicotine. J Pharmacol Exp Ther. 1998;287(3):958-62. even in individuals who persisted smoking. However, the heterogeneity of the studies and the small number of volunteers included do not provide sufficient evidence of an increase in long-term smoking abstinence rates.
The possible association of NRT with non-nicotinic drug (such as bupropion) or the choice of varenicline monotherapy is theoretically an acceptable option, but they do not find great support in specific studies in these special situations.640640 Dale LC, Hurt RD, Offord KP, Lawson GM, Croghan IT, Schroeder DR. High-dose nicotine patch therapy. Percentage of replacement and smoking cessation. JAMA. 1995;274(17):1353-8.
641 Hatsukami D, Mooney M, Murphy S, LeSage M, Babb D, Hecht S. Effects of high dose transdermal nicotine replacement in cigarette smokers. Pharmacol Biochem Behav. 2007;86(1):132-9.
642 Zevin S, Jacob P 3rd, Benowitz NL. Dose-related cardiovascular and endocrine effects of transdermal nicotine. Clin Pharmacol Ther. 1998;64(1):87-95.-643643 Benowitz NL, Zevin S, Jacob P 3rd. Suppression of nicotine intake during ad libitum cigarette smoking by high-dose transdermal nicotine. J Pharmacol Exp Ther. 1998;287(3):958-62.
NRT is not superior over bupropion in patients with a history of recent (below six weeks) high-risk acute coronary syndrome and patients with complex ventricular arrhythmias. Published studies are controversial in identifying additional benefits (in addition to the control of withdrawal symptoms) from the drug treatment compared to the counseling program and behavioral approach alone.
For hospitalized patients, we propose a treatment based on the flowchart in figure 6.
In-hospital patient algorithm.
* < 20 CIGARETTES/DAY: 14 mg patches; 20-30 cigarettes/day: 21 mg patches; 31-40 cigarettes/day: 21 mg + 7 mg patches; > 40 cigarettes/day: 21 mg + 14 mg patches. For all cases, consider the association with nicotine gum or tablet of 4 mg ad libitum. † consider titration of transdermal nicotine dose (avoid doses above 42 mg/day) or substitute for varenicline. ‡ outpatient return in a maximum of one month, with follow-up for a time not lesser than one month. Reduce dose of NRT according to the guidelines applicable to general situations.
There is consistent evidence supporting the treatment to stop smoking in subpopulations of hospitalized patients and candidates for surgical procedures. This intervention is extremely effective and inexpensive.
In general, the therapeutic strategies are not much different from the routines suggested for general populations, but there is a preference for NRT.
Hospital admissions and consultations for the evaluation of surgical risks and perioperative care should consider the active approach to cessation of smoking, researching, advising, treating, and following-up these patients.
-
Erratum
In “3rd Guideline for Perioperative Cardiovascular Evaluation of the Brazilian Society of Cardiology”, consider Marcondes-Braga FG as the correct form for the name of the author Fabiana Goulart Marcondes Braga.
-
1Gualandro DM, Yu PC, Calderaro D, Marques AC, Pinho C, Caramelli B, et al. II Guidelines for perioperative evaluation of the Brazilian Society of Cardiology. Arq Bras Cardiol. 2011;96(3 Suppl 1):1-68.
-
2Dunkelgrun M, Boersma E, Schouten O, Koopman-van Gemert AW, van Poorten F, Bax JJ, et al; Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Bisoprolol and fluvastatin for the reduction of perioperative cardiac mortality and myocardial infarction in intermediate-risk patients undergoing noncardiovascular surgery: a randomized controlled trial (DECREASE-IV). Ann Surg. 2009;249(6):921-6.
-
3Poldermans D, Schouten O, Vidakovic R, Bax JJ, Thomson IR, Hoeks SE, et al; DECREASE Study Group. A clinical randomized trial to evaluate the safety of a noninvasive approach in high-risk patients undergoing major vascular surgery: the DECREASE-V Pilot Study. J Am Coll Cardiol. 2007;49(17):1763-9.
-
4Goei D, van Kuijk JP, Flu WJ, Hoeks SE, Chonchol M, Verhagen HJ, et al. Usefulness of repeated N-terminal pro-B-type natriuretic peptide measurements as incremental predictor for long-term cardiovascular outcome after vascular surgery. Am J Cardiol. 2011;107(4):609-14.
-
5Dakik HA, Kobrossi S, Tamim H. The yield of routine pre-operative cardiovascular evaluation in stable patients scheduled for elective non-cardiac surgery. Int J Cardiol. 2015;186:325-7.
-
6Heinisch RH, Barbieri CF, Nunes Filho JR, Oliveira GL, Heinisch LM. Prospective assessment of different indices of cardiac risk for patients undergoing noncardiac surgeries. Arq Bras Cardiol. 2002;79(4):327-38.
-
7Hlatky MA, Boineau RE, Higginbotham MB, Lee KL, Mark DB, Califf RM, et al. A brief self-administered questionnaire to determine functional capacity (the Duke Activity Status Index). Am J Cardiol. 1989;64(10):651-4.
-
8Melin AA, Schmid KK, Lynch TG, Pipinos II, Kappes S, Longo GM, et al. Preoperative frailty Risk Analysis Index to stratify patients undergoing carotid endarterectomy. J Vasc Surg. 2015;61(3):683-9.
-
9Rinkinen J, Agarwal S, Beauregard J, Aliu O, Benedict M, Buchman SR, et al. Morphomic analysis as an aid for preoperative risk stratification in patients undergoing major head and neck cancer surgery. J Surg Res. 2015;194(1):177-84.
-
10Scandrett KG, Zuckerbraun BS, Peitzman AB. Operative risk stratification in the older adult. Surg Clin North Am. 2015;95(1):149-72.
-
11Amrock LG, Deiner S. The implication of frailty on preoperative risk assessment. Curr Opin Anaesthesiol. 2014;27(3):330-5.
-
12Amrock LG, Neuman MD, Lin HM, Deiner S. Can routine preoperative data predict adverse outcomes in the elderly? Development and validation of a simple risk model incorporating a chart-derived frailty score. J Am Coll Surg. 2014;219(4):684-94.
-
13Dunne MJ, Abah U, Scarci M. Frailty assessment in thoracic surgery. Interact Cardiovasc Thorac Surg. 2014;18(5):667-70.
-
14Hasselager R, Gögenur I. Core muscle size assessed by perioperative abdominal CT scan is related to mortality, postoperative complications, and hospitalization after major abdominal surgery: a systematic review. Langenbecks Arch Surg. 2014;399(3):287-95.
-
15Revenig LM, Canter DJ, Taylor MD, Tai C, Sweeney JF, Sarmiento JM, et al. Too frail for surgery? Initial results of a large multidisciplinary prospective study examining preoperative variables predictive of poor surgical outcomes. J Am Coll Surg. 2013;217(4):665-70.e1.
-
16Robinson TN, Wu DS, Pointer L, Dunn CL, Cleveland JC, Moss M. Simple frailty score predicts postoperative complications across surgical specialties. Am J Surg. 2013;206(4):544-50.
-
17Lee JS, He K, Harbaugh CM, Schaubel DE, Sonnenday CJ, Wang SC, et al; Michigan Analytic Morphomics Group (MAMG). Frailty, core muscle size, and mortality in patients undergoing open abdominal aortic aneurysm repair. J Vasc Surg. 2011;53(4):912-7.
-
18Makary MA, Segev DL, Pronovost PJ, Syin D, Bandeen-Roche K, Patel P, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210(6):901-8.
-
19Goldman L, Caldera DL, Nussbaum SR, Southwick FS, Krogstad D, Murray B, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med. 1977;297(16):845-50.
-
20Butman SM, Ewy GA, Standen JR, Kern KB, Hahn E. Bedside cardiovascular examination in patients with severe chronic heart failure: importance of rest or inducible jugular venous distension. J Am Coll Cardiol. 1993;22(4):968-74.
-
21Munro J, Booth A, Nicholl J. Routine preoperative testing: a systematic review of the evidence. Health Technol Assess. 1997;1(12):i-iv; 1-62.
-
22American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Practice advisory for preanesthesia evaluation: a report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2002;96(2):485-96.
-
23Health NIf, Care E. NICE Guideline: Routine preoperative tests for elective surgery. United Kingdom; 2016. [Access in 2016 Nov 12]. Available from: https://www.nice.org.uk/guidance/ng45/resources/routine-preoperative-tests-for-elective-surgery-1837454508997
» https://www.nice.org.uk/guidance/ng45/resources/routine-preoperative-tests-for-elective-surgery-1837454508997 -
24Schein OD, Katz J, Bass EB, Tielsch JM, Lubomski LH, Feldman MA, et al. The value of routine preoperative medical testing before cataract surgery. Study of Medical Testing for Cataract Surgery. N Engl J Med. 2000;342(3):168-75.
-
25Lira RP, Nascimento MA, Moreira-Filho DC, Kara-José N, Arieta CE. Are routine preoperative medical tests needed with cataract surgery? Rev Panam Salud Publica. 2001;10(1):13-7.
-
26Cavallini GM, Saccarola P, D'Amico R, Gasparin A, Campi L. Impact of preoperative testing on ophthalmologic and systemic outcomes in cataract surgery. Eur J Ophthalmol. 2004;14(5):369-74.
-
27Keay L, Lindsley K, Tielsch J, Katz J, Schein O. Routine preoperative medical testing for cataract surgery. Cochrane Database Syst Rev. 2012 Mar 14;(3):CD007293.
-
28Chen CL, Lin GA, Bardach NS, Clay TH, Boscardin WJ, Gelb AW, et al. Preoperative medical testing in Medicare patients undergoing cataract surgery. N Engl J Med. 2015;372(16):1530-8.
-
29Chung F, Yuan H, Yin L, Vairavanathan S, Wong DT. Elimination of preoperative testing in ambulatory surgery. Anesth Analg. 2009;108(2):467-75.
-
30Benarroch-Gampel J, Sheffield KM, Duncan CB, Brown KM, Han Y, Townsend CM, et al. Preoperative laboratory testing in patients undergoing elective, low-risk ambulatory surgery. Ann Surg. 2012;256(3):518-28.
-
31Czoski-Murray C, Lloyd Jones M, McCabe C, Claxton K, Oluboyede Y, Roberts J, et al. What is the value of routinely testing full blood count, electrolytes and urea, and pulmonary function tests before elective surgery in patients with no apparent clinical indication and in subgroups of patients with common comorbidities: a systematic review of the clinical and cost-effective literature. Health Technol Assess. 2012;16(50):i-xvi, 1-159.
-
32Goldberger AL, O'Konski M. Utility of the routine electrocardiogram before surgery and on general hospital admission. Critical review and new guidelines. Ann Intern Med. 1986;105(4):552-7.
-
33Liu LL, Dzankic S, Leung JM. Preoperative electrocardiogram abnormalities do not predict postoperative cardiac complications in geriatric surgical patients. J Am Geriatr Soc. 2002;50(7):1186-91.
-
34van Klei WA, Bryson GL, Yang H, Kalkman CJ, Wells GA, Beattie WS. The value of routine preoperative electrocardiography in predicting myocardial infarction after noncardiac surgery. Ann Surg. 2007;246(2):165-70.
-
35Noordzij PG, Boersma E, Bax JJ, Feringa HH, Schreiner F, Schouten O, et al. Prognostic value of routine preoperative electrocardiography in patients undergoing noncardiac surgery. Am J Cardiol. 2006;97(7):1103-6.
-
36Payne CJ, Payne AR, Gibson SC, Jardine AG, Berry C, Kingsmore DB. Is there still a role for preoperative 12-lead electrocardiography? World J Surg. 2011;35(12):2611-6.
-
37Biteker M, Duman D, Tekkesin AI. Predictive value of preoperative electrocardiography for perioperative cardiovascular outcomes in patients undergoing noncardiac, nonvascular surgery. Clin Cardiol. 2012;35(8):494-9.
-
38Feely MA, Collins CS, Daniels PR, Kebede EB, Jatoi A, Mauck KF. Preoperative testing before noncardiac surgery: guidelines and recommendations. Am Fam Physician. 2013;87(6):414-8.
-
39García-Miguel FJ, Serrano-Aguilar PG, López-Bastida J. Preoperative assessment. Lancet. 2003;362(9397):1749-57.
-
40Silvestri L, Gullo A. Pre-operative chest radiograph. The challenge continues. Minerva Anestesiol. 2004;70(6):437-42.
-
41Joo HS, Wong J, Naik VN, Savoldelli GL. The value of screening preoperative chest x-rays: a systematic review. Can J Anaesth. 2005;52(6):568-74.
-
42Gilbert K, Larocque BJ, Patrick LT. Prospective evaluation of cardiac risk indices for patients undergoing noncardiac surgery. Ann Intern Med. 2000;133(5):356-9.
-
43Press MJ, Chassin MR, Wang J, Tuhrim S, Halm EA. Predicting medical and surgical complications of carotid endarterectomy: comparing the risk indexes. Arch Intern Med. 2006;166(8):914-20.
-
44Smeili LA, Lotufo PA. Incidence and predictors of cardiovascular complications and death after vascular surgery. Arq Bras Cardiol. 2015;105(5):510-8.
-
45Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043-9.
-
46Guidelines for assessing and managing the perioperative risk from coronary artery disease associated with major noncardiac surgery. American College of Physicians. Ann Intern Med. 1997;127(4):309-12.
-
47Palda VA, Detsky AS. Perioperative assessment and management of risk from coronary artery disease. Ann Intern Med. 1997;127(4):313-28.
-
48Pinho C, Grandini PC, Gualandro DM, Calderaro D, Monachini M, Caramelli B. Multicenter study of perioperative evaluation for noncardiac surgeries in Brazil (EMAPO). Clinics (Sao Paulo). 2007;62(1):17-22.
-
49Ford MK, Beattie WS, Wijeysundera DN. Systematic review: prediction of perioperative cardiac complications and mortality by the revised cardiac risk index. Ann Intern Med. 2010;152(1):26-35.
-
50Marques AC, Bellen BV, Caramelli B, Presti C, Pinho C, Calderaro D, et al; Sociedade Brasileira de Cardiologia. [Update and focus on arterial vascular surgeries from the II Guidelines for Perioperative Evaluation of the Brazilian Society of Cardiology]. Arq Bras Cardiol 2013;101(4 Suppl 2):2-32.
-
51Bertges DJ, Goodney PP, Zhao Y, Schanzer A, Nolan BW, Likosky DS, et al; Vascular Study Group of New England. The Vascular Study Group of New England Cardiac Risk Index (VSG-CRI) predicts cardiac complications more accurately than the Revised Cardiac Risk Index in vascular surgery patients. J Vasc Surg. 2010;52(3):674-83, 83.e1-83.e3.
-
52Bilimoria KY, Liu Y, Paruch JL, Zhou L, Kmiecik TE, Ko CY, et al. Development and evaluation of the universal ACS NSQIP surgical risk calculator: a decision aid and informed consent tool for patients and surgeons. J Am Coll Surg. 2013;217(5):833-42.e1-3.
-
53Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleischmann KE, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery); American Society of Echocardiography.; American Society of Nuclear Cardiology; Heart Rhythm Society; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society for Vascular Medicine and Biology; Society for Vascular Surgery. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery): developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. Circulation. 2007;116(17):e418-99. Erratum in: Circulation. 2008;117(5):e154. Circulation. 2008;118(9): e143-4.
-
54Reilly DF, McNeely MJ, Doerner D, Greenberg DL, Staiger TO, Geist MJ, et al. Self-reported exercise tolerance and the risk of serious perioperative complications. Arch Intern Med. 1999;159(18):2185-92.
-
55Marques AC, Calderaro D, Yu PC, Gualandro DM, Carmo GA, Azevedo FR, et al. Impact of cardiology referral: clinical outcomes and factors associated with physicians' adherence to recommendations. Clinics (Sao Paulo). 2014;69(10):666-71.
-
56Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
-
57Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130(24):e278-333.
-
58Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al; American Society of Echocardiography's Nomenclature and Standards Committee.; Task Force on Chamber Quantification.; American College of Cardiology Echocardiography Committee.; American Heart Association.; European Association of Echocardiography, European Society of Cardiology. Recommendations for chamber quantification. Eur J Echocardiogr. 2006;7(2):79-108.
-
59Mor-Avi V, Lang RM, Badano LP, Belohlavek M, Cardim NM, Derumeaux G, et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. J Am Soc Echocardiogr. 2011;24(3):277-313.
-
60Cowie B. Focused transthoracic echocardiography predicts perioperative cardiovascular morbidity. J Cardiothorac Vasc Anesth. 2012;26(6):989-93.
-
61Wijeysundera DN, Beattie WS, Karkouti K, Neuman MD, Austin PC, Laupacis A. Association of echocardiography before major elective non-cardiac surgery with postoperative survival and length of hospital stay: population based cohort study. BMJ. 2011;342:d3695.
-
62McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al; ESC Committee for Practice Guidelines. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2012;14(8):803-69. Erratum in: Eur J Heart Fail. 2013;15(3):361-2.
-
63Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Barón-Esquivias G, Baumgartner H, et al; ESC Committee for Practice Guidelines (CPG).; Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC).; European Association for Cardio-Thoracic Surgery (EACTS). Guidelines on the management of valvular heart disease (version 2012): the Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur J Cardiothorac Surg. 2012;42(4):S1-44.
-
64Calleja AM, Dommaraju S, Gaddam R, Cha S, Khandheria BK, Chaliki HP. Cardiac risk in patients aged >75 years with asymptomatic, severe aortic stenosis undergoing noncardiac surgery. Am J Cardiol. 2010;105(8):1159-63.
-
65Kristensen SD, Knuuti J, Saraste A, Anker S, Bøtker HE, Hert SD, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J. 2014;35(35):2383-431.
-
66Habib G, Hoen B, Tornos P, Thuny F, Prendergast B, Vilacosta I, et al; ESC Committee for Practice Guidelines. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J. 2009;30(19):2369-413.
-
67Samarendra P, Mangione MP. Aortic stenosis and perioperative risk with noncardiac surgery. J Am Coll Cardiol. 2015;65(3):295-302.
-
68Gualandro DM, Campos CA, Calderaro D, Yu PC, Marques AC, Pastana AF, et al. Coronary plaque rupture in patients with myocardial infarction after noncardiac surgery: frequent and dangerous. Atherosclerosis. 2012;222(1):191-5.
-
69Gualandro DM, Calderaro D, Yu PC, Caramelli B. Acute myocardial infarction after noncardiac surgery. Arq Bras Cardiol. 2012;99(5):1060-7.
-
70Padma S, Sundaram PS. Current practice and recommendation for presurgical cardiac evaluation in patients undergoing noncardiac surgeries. World J Nucl Med. 2014;13(1):6-15.
-
71Wijeysundera DN, Beattie WS, Austin PC, Hux JE, Laupacis A. Non-invasive cardiac stress testing before elective major non-cardiac surgery: population based cohort study. BMJ. 2010;340:b5526.
-
72Grayburn PA, Hillis LD. Cardiac events in patients undergoing noncardiac surgery: shifting the paradigm from noninvasive risk stratification to therapy. Ann Intern Med. 2003;138(6):506-11.
-
73Kertai MD, Boersma E, Bax JJ, Heijenbrok-Kal MH, Hunink MG, L'talien GJ, et al. A meta-analysis comparing the prognostic accuracy of six diagnostic tests for predicting perioperative cardiac risk in patients undergoing major vascular surgery. Heart. 2003;89(11):1327-34.
-
74Morris CK, Ueshima K, Kawaguchi T, Hideg A, Froelicher VF. The prognostic value of exercise capacity: a review of the literature. Am Heart J. 1991;122(5):1423-31.
-
75Vacanti LJ, Sposito AC, Séspedes L, Sarpi M, Ramires JA, Bortnick AE. In comparison to the myocardial perfusion scintigraphy, a treadmill stress test is a viable, efficient and cost effective option to predict cardiovascular events in elderly patients. Arq Bras Cardiol. 2007;88(5):531-6.
-
76Etchells E, Meade M, Tomlinson G, Cook D. Semiquantitative dipyridamole myocardial stress perfusion imaging for cardiac risk assessment before noncardiac vascular surgery: a meta-analysis. J Vasc Surg. 2002;36(3):534-40.
-
77Shaw LJ, Eagle KA, Gersh BJ, Miller DD. Meta-analysis of intravenous dipyridamole-thallium-201 imaging (1985 to 1994) and dobutamine echocardiography (1991 to 1994) for risk stratification before vascular surgery. J Am Coll Cardiol. 1996;27(4):787-98.
-
78Kayano D, Nakajima K, Ohtake H, Kinuya S. Gated myocardial perfusion SPECT for preoperative risk stratification in patients with noncardiac vascular disease. Ann Nucl Med. 2009;23(2):173-81.
-
79Mathias W Jr, Arruda A, Santos FC, Arruda AL, Mattos E, Osório A, et al. Safety of dobutamine-atropine stress echocardiography: A prospective experience of 4,033 consecutive studies. J Am Soc Echocardiogr. 1999;12(10):785-91.
-
80Chuah SC, Pellikka PA, Roger VL, McCully RB, Seward JB. Role of dobutamine stress echocardiography in predicting outcome in 860 patients with known or suspected coronary artery disease. Circulation. 1998;97(15):1474-80.
-
81Dagianti A, Penco M, Agati L, Sciomer S, Rosanio S, Fedele F. Stress echocardiography: comparison of exercise, dipyridamole and dobutamine in detecting and predicting the extent of coronary artery disease. J Am Coll Cardiol. 1995;26(1):18-25.
-
82Das MK, Pellikka PA, Mahoney DW, Roger VL, Oh JK, McCully RB, et al. Assessment of cardiac risk before nonvascular surgery: dobutamine stress echocardiography in 530 patients. J Am Coll Cardiol. 2000;35(6):1647-53.
-
83Illuminati G, Ricco JB, Greco C, Mangieri E, Calio F, Ceccanei G, et al. Systematic preoperative coronary angiography and stenting improves postoperative results of carotid endarterectomy in patients with asymptomatic coronary artery disease: a randomised controlled trial. Eur J Vasc Endovasc Surg. 2010;39(2):139-45.
-
84Leschka S, Alkadhi H, Plass A, Desbiolles L, Grünenfelder J, Marincek B, et al. Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J. 2005;26(15):1482-7.
-
85Mollet NR, Cademartiri F, Krestin GP, McFadden EP, Arampatzis CA, Serruys PW, et al. Improved diagnostic accuracy with 16-row multi-slice computed tomography coronary angiography. J Am Coll Cardiol. 2005;45(1):128-32.
-
86Sheth T, Amlani S, Ellins ML, Mehta S, Velianou J, Cappelli G, et al. Computed tomographic coronary angiographic assessment of high-risk coronary anatomy in patients with suspected coronary artery disease and intermediate pretest probability. Am Heart J. 2008;155(5):918-23.
-
87Raff GL, Gallagher MJ, O'Neill WW, Goldstein JA. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005;46(3):552-7.
-
88Ahn JH, Park JR, Min JH, Sohn JT, Hwang SJ, Park Y, et al. Risk stratification using computed tomography coronary angiography in patients undergoing intermediate-risk noncardiac surgery. J Am Coll Cardiol. 2013;61(6):661-8.
-
89Sheth T, Chan M, Butler C, Chow B, Tandon V, Nagele P, et al; Coronary Computed Tomographic Angiography and Vascular Events in Noncardiac Surgery Patients Cohort Evaluation Study Investigators. Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study. BMJ. 2015;350:h1907.
-
90Ghadri JR, Fiechter M, Veraguth K, Gebhard C, Pazhenkottil AP, Fuchs TA, et al. Coronary calcium score as an adjunct to nuclear myocardial perfusion imaging for risk stratification before noncardiac surgery. J Nucl Med. 2012;53(7):1081-6.
-
91Lange RA. Pre-operative risk assessment with cardiac computed tomography: all dressed up and nowhere to go. J Am Coll Cardiol. 2013;61(6):669-71.
-
92Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1-75.
-
93Aboyans V, Criqui MH, Abraham P, Allison MA, Creager MA, Diehm C, et al; American Heart Association Council on Peripheral Vascular Disease; Council on Epidemiology and Prevention; Council on Clinical Cardiology; Council on Cardiovascular Nursing; Council on Cardiovascular Radiology and Intervention, and Council on Cardiovascular Surgery and Anesthesia. Measurement and interpretation of the ankle-brachial index: a scientific statement from the American Heart Association. Circulation. 2012;126(24):2890-909. Erratum in: Circulation. 2013;127(1):e264.
-
94Fowkes FG, Murray GD, Butcher I, Heald CL, Lee RJ, Chambless LE, et al; Ankle Brachial Index Collaboration. Ankle brachial index combined with Framingham Risk Score to predict cardiovascular events and mortality: a meta-analysis. JAMA. 2008;300(2):197-208.
-
95Carmo GA, Calderaro D, Yu PC, Gualandro DM, Marques AC, Bittar CS, et al. Perioperative cardiovascular evaluation: heads or tails? Rev Assoc Med Bras (1992). 2012;58(4):505-12.
-
96Flu WJ, van Kuijk JP, Voûte MT, Kuiper R, Verhagen HJ, Bax JJ, et al. Asymptomatic low ankle-brachial index in vascular surgery patients: a predictor of perioperative myocardial damage. Eur J Vasc Endovasc Surg. 2010;39(1):62-9.
-
97Fisher BW, Ramsay G, Majumdar SR, Hrazdil CT, Finegan BA, Padwal RS, et al. The ankle-to-arm blood pressure index predicts risk of cardiac complications after noncardiac surgery. Anesth Analg. 2008;107(1):149-54.
-
98Carmo GA, Calderaro D, Gualandro DM, Pastana AF, Yu PC, Marques AC, et al. The ankle-brachial index is associated with cardiovascular complications after noncardiac surgery. Angiology. 2016;67(2):187-92.
-
99Heim C, Geel A, Münzer T, Angehrn W, Roelli H, Niederhauser H. [Perioperative myocardial infarction and cardiac complications after noncardiac surgery in patients with prior myocardial infarction. II: Perioperative long-term ECG--clinical relevance practicability]. Anaesthesist. 1996;45(3):220-4.
-
100Lipinski MJ, Baker NC, Escárcega RO, Torguson R, Chen F, Aldous SJ, et al. Comparison of conventional and high-sensitivity troponin in patients with chest pain: a collaborative meta-analysis. Am Heart J. 2015;169(1):6-16.e6.
-
101Jarolim P. High sensitivity cardiac troponin assays in the clinical laboratories. Clin Chem Lab Med. 2015;53(5):635-52.
-
102Twerenbold R, Wildi K, Jaeger C, Gimenez MR, Reiter M, Reichlin T, et al. Optimal cutoff levels of more sensitive cardiac troponin assays for the early diagnosis of myocardial infarction in patients with renal dysfunction. Circulation. 2015;131(23):2041-50.
-
103Nagele P, Brown F, Gage BF, Gibson DW, Miller JP, Jaffe AS, et al. High-sensitivity cardiac troponin T in prediction and diagnosis of myocardial infarction and long-term mortality after noncardiac surgery. Am Heart J. 2013;166(2):325-32.e1.
-
104Gillmann HJ, Meinders A, Grosshennig A, Larmann J, Bünte C, Calmer S, et al. Perioperative levels and changes of high-sensitivity troponin T are associated with cardiovascular events in vascular surgery patients. Crit Care Med. 2014;42(6):1498-506.
-
105Weber M, Luchner A, Manfred S, Mueller C, Liebetrau C, Schlitt A, et al. Incremental value of high-sensitive troponin T in addition to the revised cardiac index for peri-operative risk stratification in non-cardiac surgery. Eur Heart J. 2013;34(11):853-62. Erratum in: Eur Heart J. 2013;34(24):1853.
-
106Kavsak PA, Walsh M, Srinathan S, Thorlacius L, Buse GL, Botto F, et al. High sensitivity troponin T concentrations in patients undergoing noncardiac surgery: a prospective cohort study. Clin Biochem. 2011;44(12):1021-4.
-
107Alcock RF, Kouzios D, Naoum C, Hillis GS, Brieger DB. Perioperative myocardial necrosis in patients at high cardiovascular risk undergoing elective non-cardiac surgery. Heart. 2012;98(10):792-8.
-
108Biccard BM, Naidoo P, de Vasconcellos K. What is the best pre-operative risk stratification tool for major adverse cardiac events following elective vascular surgery? A prospective observational cohort study evaluating pre-operative myocardial ischaemia monitoring and biomarker analysis. Anaesthesia. 2012;67(4):389-95.
-
109Sankar A, Beattie WS, Wijeysundera DN. How can we identify the high-risk patient? Curr Opin Crit Care. 2015;21(4):328-35.
-
110Karthikeyan G, Moncur RA, Levine O, Heels-Ansdell D, Chan MT, Alonso-Coello P, et al. Is a pre-operative brain natriuretic peptide or N-terminal pro-B-type natriuretic peptide measurement an independent predictor of adverse cardiovascular outcomes within 30 days of noncardiac surgery? A systematic review and meta-analysis of observational studies. J Am Coll Cardiol. 2009;54(17):1599-606.
-
111Biccard BM, Naidoo P. The role of brain natriuretic peptide in prognostication and reclassification of risk in patients undergoing vascular surgery. Anaesthesia. 2011;66(5):379-85.
-
112Rodseth RN, Lurati Buse GA, Bolliger D, Burkhart CS, Cuthbertson BH, Gibson SC, et al. The predictive ability of pre-operative B-type natriuretic peptide in vascular patients for major adverse cardiac events: an individual patient data meta-analysis. J Am Coll Cardiol. 2011;58(5):522-9.
-
113Ryding AD, Kumar S, Worthington AM, Burgess D. Prognostic value of brain natriuretic peptide in noncardiac surgery: a meta-analysis. Anesthesiology. 2009;111(2):311-9.
-
114Beattie WS, Wijeysundera DN. Perioperative cardiac biomarkers: the utility and timing. Curr Opin Crit Care. 2013;19(4):334-41.
-
115Rodseth RN, Biccard BM, Le Manach Y, Sessler DI, Lurati Buse GA, Thabane L, et al. The prognostic value of pre-operative and post-operative B-type natriuretic peptides in patients undergoing noncardiac surgery: B-type natriuretic peptide and N-terminal fragment of pro-B-type natriuretic peptide: a systematic review and individual patient data meta-analysis. J Am Coll Cardiol. 2014;63(2):170-80.
-
116Livhits M, Ko CY, Leonardi MJ, Zingmond DS, Gibbons MM, de Virgilio C. Risk of surgery following recent myocardial infarction. Ann Surg. 2011;253(5):857-64.
-
117Dix P, Howell S. Survey of cancellation rate of hypertensive patients undergoing anaesthesia and elective surgery. Br J Anaesth. 2001;86(6):789-93.
-
118Browner WS, Li J, Mangano DT. In-hospital and long-term mortality in male veterans following noncardiac surgery. The Study of Perioperative Ischemia Research Group. JAMA. 1992;268(2):228-32.
-
119Kang JL, Chung TK, Lancaster RT, Lamuraglia GM, Conrad MF, Cambria RP. Outcomes after carotid endarterectomy: is there a high-risk population? A National Surgical Quality Improvement Program report. J Vasc Surg. 2009;49(2):331-8, 9.e1.
-
120Dodson GM, Bentley WE 4th, Awad A, Muntazar M, Goldberg ME. Isolated perioperative hypertension: clinical implications & contemporary treatment strategies. Curr Hypertens Rev. 2014;10(1):31-6.
-
121Ghignone M, Calvillo O, Quintin L. Anesthesia and hypertension: the effect of clonidine on perioperative hemodynamics and isoflurane requirements. Anesthesiology. 1987;67(1):3-10.
-
122Sellevold OF, Raeder J, Stenseth R. Undiagnosed phaeochromocytoma in the perioperative period. Case reports. Acta Anaesthesiol Scand. 1985;29(5):474-9.
-
123Deague JA, Wilson CM, Grigg LE, Harrap SB. Physiological relationships between central vascular haemodynamics and left ventricular structure. Clin Sci (Lond). 2001;101(1):79-85.
-
124Mosterd A, Hoes AW. Clinical epidemiology of heart failure. Heart. 2007;93(9):1137-46.
-
125Gaui EN, Oliveira GM, Klein CH. Mortality by heart failure and ischemic heart disease in Brazil from 1996 to 2011. Arq Bras Cardiol. 2014;102(6):557-65.
-
126Hammill BG, Curtis LH, Bennett-Guerrero E, O'Connor CM, Jollis JG, Schulman KA, et al. Impact of heart failure on patients undergoing major noncardiac surgery. Anesthesiology. 2008;108(4):559-67.
-
127Healy KO, Waksmonski CA, Altman RK, Stetson PD, Reyentovich A, Maurer MS. Perioperative outcome and long-term mortality for heart failure patients undergoing intermediate- and high-risk noncardiac surgery: impact of left ventricular ejection fraction. Congest Heart Fail. 2010;16(2):45-9.
-
128Biccard BM, Lurati Buse GA, Burkhart C, Cuthbertson BH, Filipovic M, Gibson SC, et al. The influence of clinical risk factors on pre-operative B-type natriuretic peptide risk stratification of vascular surgical patients. Anaesthesia. 2012;67(1):55-9.
-
129Rajagopalan S, Croal BL, Reeve J, Bachoo P, Brittenden J. N-terminal pro-B-type natriuretic peptide is an independent predictor of all-cause mortality and MACE after major vascular surgery in medium-term follow-up. Eur J Vasc Endovasc Surg. 2011;41(5):657-62.
-
130Polanczyk CA, Goldman L, Marcantonio ER, Orav EJ, Lee TH. Supraventricular arrhythmia in patients having noncardiac surgery: clinical correlates and effect on length of stay. Ann Intern Med. 1998;129(4):279-85.
-
131Sprung J, Abdelmalak B, Gottlieb A, Mayhew C, Hammel J, Levy PJ, et al. Analysis of risk factors for myocardial infarction and cardiac mortality after major vascular surgery. Anesthesiology. 2000;93(1):129-40.
-
132Tarasoutchi F, Montera MW, Grinberg M, Piñeiro DJ, Sánchez CR, Bacelar AC, et al. [Brazilian Guidelines for Valve Disease - SBC 2011 / I Guideline Inter-American Valve Disease - 2011 SIAC]. Arq Bras Cardiol. 2011;97(5 Suppl 1):1-67.
-
133Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Guyton RA, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(22):e57-185. Erratum in: J Am Coll Cardiol. 2014;63(22):2489.
-
134Freeman RV, Otto CM. Spectrum of calcific aortic valve disease: pathogenesis, disease progression, and treatment strategies. Circulation. 2005;111(24):3316-26.
-
135Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368(9540):1005-11.
-
136Skinner JF, Pearce ML. Surgical risk in the cardiac patient. J Chronic Dis. 1964;17:57-72.
-
137Detsky AS, Abrams HB, McLaughlin JR, Drucker DJ, Sasson Z, Johnston N, et al. Predicting cardiac complications in patients undergoing non-cardiac surgery. J Gen Intern Med. 1986;1(4):211-9.
-
138Rohde LE, Polanczyk CA, Goldman L, Cook EF, Lee RT, Lee TH. Usefulness of transthoracic echocardiography as a tool for risk stratification of patients undergoing major noncardiac surgery. Am J Cardiol. 2001;87(5):505-9.
-
139Zahid M, Sonel AF, Saba S, Good CB. Perioperative risk of noncardiac surgery associated with aortic stenosis. Am J Cardiol. 2005;96(3):436-8.
-
140Mizuno R, Yamagami ST, Higashi T, Nakada Y, Takeda Y, Okayama S, et al. Major non-cardiac surgery is a risk factor for rapid hemodynamic progression of non-rheumatic aortic stenosis. Circ J. 2015;79(4):867-72.
-
141Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al; PARTNER Trial Investigators. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-607.
-
142Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, et al; PARTNER Trial Investigators. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-98.
-
143Torsher LC, Shub C, Rettke SR, Brown DL. Risk of patients with severe aortic stenosis undergoing noncardiac surgery. Am J Cardiol. 1998;81(4):448-52.
-
144Reyes VP, Raju BS, Wynne J, Stephenson LW, Raju R, Fromm BS, et al. Percutaneous balloon valvuloplasty compared with open surgical commissurotomy for mitral stenosis. N Engl J Med. 1994;331(15):961-7.
-
145Lai HC, Lee WL, Wang KY, Ting CT, Hung CJ, Liu TJ. Impact of chronic advanced aortic regurgitation on the perioperative outcome of noncardiac surgery. Acta Anaesthesiol Scand. 2010;54(5):580-8.
-
146Bajaj NS, Agarwal S, Rajamanickam A, Parashar A, Poddar KL, Griffin BP, et al. Impact of severe mitral regurgitation on postoperative outcomes after noncardiac surgery. Am J Med. 2013;126(6):529-35.
-
147Scanavacca MI, de Brito FS, Maia I, Hachul D, Gizzi J, Lorga A, et al; Sociedade Brasileira de Cardiologia. [Guidelines for the evaluation and treatment of patients with cardiac arrhythmias]. Arq Bras Cardiol. 2002;79 Suppl 5:1-50.
-
148Blomström-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, et al; European Society of Cardiology Committee, NASPE-Heart Rhythm Society. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias--executive summary. a report of the American college of cardiology/American heart association task force on practice guidelines and the European society of cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J Am Coll Cardiol. 2003;42(8):1493-531.
-
149Pedersen CT, Kay GN, Kalman J, Borggrefe M, Della-Bella P, Dickfeld T, et al; EP-Europace,UK. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm. 2014;11(10):e166-96.
-
150Mahla E, Rotman B, Rehak P, Atlee JL, Gombotz H, Berger J, et al. Perioperative ventricular dysrhythmias in patients with structural heart disease undergoing noncardiac surgery. Anesth Analg. 1998;86(1):16-21.
-
151Chatterjee A, Hage FG. Guidelines in review: 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Nucl Cardiol. 2015;22(1):158-61.
-
152January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, et al; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267.
-
153Bengali R, Wellens HJ, Jiang Y. Perioperative management of the Wolff-Parkinson-White syndrome. J Cardiothorac Vasc Anesth. 2014;28(5):1375-86.
-
154Martinelli Filho M, Moreira DA, Lorga AM, Sosa E, Atié J, Pimenta J, et al. [Guideline of atrial fibrillation]. Arq Bras Cardiol. 2003;81 Suppl 6:3-24.
-
155Bessissow A, Khan J, Devereaux PJ, Alvarez-Garcia J, Alonso-Coello P. Postoperative atrial fibrillation in non-cardiac and cardiac surgery: an overview. J Thromb Haemost. 2015;13 Suppl 1:S304-12.
-
156Tisdale JE, Wroblewski HA, Kesler KA. Prophylaxis of atrial fibrillation after noncardiac thoracic surgery. Semin Thorac Cardiovasc Surg. 2010;22(4):310-20.
-
157Tisdale JE, Wroblewski HA, Wall DS, Rieger KM, Hammoud ZT, Young JV, et al. A randomized, controlled study of amiodarone for prevention of atrial fibrillation after transthoracic esophagectomy. J Thorac Cardiovasc Surg. 2010;140(1):45-51.
-
158Tisdale JE, Wroblewski HA, Wall DS, Rieger KM, Hammoud ZT, Young JV, et al. A randomized trial evaluating amiodarone for prevention of atrial fibrillation after pulmonary resection. Ann Thorac Surg. 2009;88(3):886-93.
-
159Riber LP, Christensen TD, Jensen HK, Hoejsgaard A, Pilegaard HK. Amiodarone significantly decreases atrial fibrillation in patients undergoing surgery for lung cancer. Ann Thorac Surg. 2012;94(2):339-44.
-
160Khalil MA, Al-Agaty AE, Ali WG, Abdel Azeem MS. A comparative study between amiodarone and magnesium sulfate as antiarrhythmic agents for prophylaxis against atrial fibrillation following lobectomy. J Anesth. 2013;27(1):56-61.
-
161Chopra V, Wesorick DH, Sussman JB, Greene T, Rogers M, Froehlich JB, et al. Effect of perioperative statins on death, myocardial infarction, atrial fibrillation, and length of stay: a systematic review and meta-analysis. Arch Surg. 2012;147(2):181-9.
-
162Staikou C, Chondrogiannis K, Mani A. Perioperative management of hereditary arrhythmogenic syndromes. Br J Anaesth. 2012;108(5):730-44.
-
163Tabib A, Loire R, Miras A, Thivolet-Bejui F, Timour Q, Bui-Xuan B, et al. Unsuspected cardiac lesions associated with sudden unexpected perioperative death. Eur J Anaesthesiol. 2000;17(4):230-5.
-
164Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al; Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Europace. 2015;17(11):1601-87.
-
165Gauss A, Hübner C, Radermacher P, Georgieff M, Schütz W. Perioperative risk of bradyarrhythmias in patients with asymptomatic chronic bifascicular block or left bundle branch block: does an additional first-degree atrioventricular block make any difference? Anesthesiology. 1998;88(3):679-87. Erratum in: Anesthesiology 1998;88(6):1697.
-
166Gauss A, Hübner C, Meierhenrich R, Röhm HJ, Georgieff M, Schütz W. Perioperative transcutaneous pacemaker in patients with chronic bifascicular block or left bundle branch block and additional first-degree atrioventricular block. Acta Anaesthesiol Scand. 1999;43(7):731-6.
-
167Martinelli Filho M, Zimerman LI, Lorga AM, Vasconcelos JT, Rassi A Jr. Guidelines for implantable electronic cardiac devices of the Brazilian Society of Cardiology. Arq Bras Cardiol. 2007;89(6):e210-e38.
-
168Gammage MD. Temporary cardiac pacing. Heart. 2000;83(6):715-20.
-
169Wong DT, Middleton W. Electrocautery-induced tachycardia in a rate-responsive pacemaker. Anesthesiology. 2001;94(4):710-1.
-
170Crossley GH, Poole JE, Rozner MA, Asirvatham SJ, Cheng A, Chung MK, et al. The Heart Rhythm Society (HRS)/American Society of Anesthesiologists (ASA) Expert Consensus Statement on the perioperative management of patients with implantable defibrillators, pacemakers and arrhythmia monitors: facilities and patient management: executive summary this document was developed as a joint project with the American Society of Anesthesiologists (ASA), and in collaboration with the American Heart Association (AHA), and the Society of Thoracic Surgeons (STS). Heart Rhythm. 2011;8(7):e1-18.
-
171Jacob S, Panaich SS, Maheshwari R, Haddad JW, Padanilam BJ, John SK. Clinical applications of magnets on cardiac rhythm management devices. Europace. 2011;13(9):1222-30.
-
172McMullan J, Valento M, Attari M, Venkat A. Care of the pacemaker/implantable cardioverter defibrillator patient in the ED. Am J Emerg Med. 2007;25(7):812-22.
-
173Küfer R, Thamasett S, Volkmer B, Hautmann RE, Gschwend JE. New-generation lithotripters for treatment of patients with implantable cardioverter defibrillator: experimental approach and review of literature. J Endourol. 2001;15(5):479-84.
-
174Gimbel JR. Magnetic resonance imaging of implantable cardiac rhythm devices at 3.0 tesla. Pacing Clin Electrophysiol. 2008;31(7):795-801.
-
175Nazarian S, Beinart R, Halperin HR. Magnetic resonance imaging and implantable devices. Circ Arrhythm Electrophysiol. 2013;6(2):419-28.
-
176Zweng A, Schuster R, Hawlicek R, Weber HS. Life-threatening pacemaker dysfunction associated with therapeutic radiation: a case report. Angiology. 2009;60(4):509-12.
-
177McCollough CH, Zhang J, Primak AN, Clement WJ, Buysman JR. Effects of CT irradiation on implantable cardiac rhythm management devices. Radiology. 2007;243(3):766-74.
-
178Makkar A, Prisciandaro J, Agarwal S, Lusk M, Horwood L, Moran J, et al. Effect of radiation therapy on permanent pacemaker and implantable cardioverter-defibrillator function. Heart Rhythm. 2012;9(12):1964-8.
-
179Hurkmans CW, Knegjens JL, Oei BS, Maas AJ, Uiterwaal GJ, van der Borden AJ, et al; Dutch Society of Radiotherapy and Oncology (NVRO). Management of radiation oncology patients with a pacemaker or ICD: a new comprehensive practical guideline in The Netherlands. Dutch Society of Radiotherapy and Oncology (NVRO). Radiat Oncol. 2012;7:198.
-
180Roedig JJ, Shah J, Elayi CS, Miller CS. Interference of cardiac pacemaker and implantable cardioverter-defibrillator activity during electronic dental device use. J Am Dent Assoc. 2010;141(5):521-6.
-
181Godzieba A, Smektala T, Jedrzejewski M, Sporniak-Tutak K. Clinical assessment of the safe use local anaesthesia with vasoconstrictor agents in cardiovascular compromised patients: a systematic review. Med Sci Monit. 2014;20:393-8.
-
182Hu R, Cowie DA. Pacemaker-driven tachycardia induced by electrocardiograph monitoring in the recovery room. Anaesth Intensive Care. 2006;34(2):266-8.
-
183Pinski SL, Trohman RG. Interference with cardiac pacing. Cardiol Clin. 2000;18(1):219-39.
-
184Raval Z, Harinstein ME, Skaro AI, Erdogan A, DeWolf AM, Shah SJ, et al. Cardiovascular risk assessment of the liver transplant candidate. J Am Coll Cardiol. 2011;58(3):223-31.
-
185Dec GW, Kondo N, Farrell ML, Dienstag J, Cosimi AB, Semigran MJ. Cardiovascular complications following liver transplantation. Clin Transplant. 1995;9(6):463-71.
-
186Mandell MS, Lindenfeld J, Tsou MY, Zimmerman M. Cardiac evaluation of liver transplant candidates. World J Gastroenterol. 2008;14(22):3445-51.
-
187Zaky A, Bendjelid K. Appraising cardiac dysfunction in liver transplantation: an ongoing challenge. Liver Int. 2015;35(1):12-29.
-
188Rugina M, Predescu L, Salagean M, Gheorghe L, Gheorghe C, Tulbure D, et al. Pre-liver transplantation, cardiac assessment. Chirurgia (Bucur). 2012;107(3):283-90.
-
189Bernardi M, Maggioli C, Dibra V, Zaccherini G. QT interval prolongation in liver cirrhosis: innocent bystander or serious threat? Expert Rev Gastroenterol Hepatol. 2012;6(1):57-66.
-
190Umphrey LG, Hurst RT, Eleid MF, Lee KS, Reuss CS, Hentz JG, et al. Preoperative dobutamine stress echocardiographic findings and subsequent short-term adverse cardiac events after orthotopic liver transplantation. Liver Transpl. 2008;14(6):886-92.
-
191Møller S, Henriksen JH. Cirrhotic cardiomyopathy. J Hepatol. 2010;53(1):179-90.
-
192Capasso JM, Li P, Guideri G, Malhotra A, Cortese R, Anversa P. Myocardial mechanical, biochemical, and structural alterations induced by chronic ethanol ingestion in rats. Circ Res. 1992;71(2):346-56.
-
193La Vecchia LL, Bedogni F, Bozzola L, Bevilacqua P, Ometto R, Vincenzi M. Prediction of recovery after abstinence in alcoholic cardiomyopathy: role of hemodynamic and morphometric parameters. Clin Cardiol. 1996;19(1):45-50.
-
194Swanson KL, Krowka MJ. Screen for portopulmonary hypertension, especially in liver transplant candidates. Cleve Clin J Med. 2008;75(2):121-2, 125-30.
-
195Porres-Aguilar M, Zuckerman MJ, Figueroa-Casas JB, Krowka MJ. Portopulmonary hypertension: state of the art. Ann Hepatol. 2008;7(4):321-30.
-
196Grace JA, Angus PW. Hepatopulmonary syndrome: update on recent advances in pathophysiology, investigation, and treatment. J Gastroenterol Hepatol. 2013;28(2):213-9.
-
197Gupta S, Castel H, Rao RV, Picard M, Lilly L, Faughnan ME, et al. Improved survival after liver transplantation in patients with hepatopulmonary syndrome. Am J Transplant. 2010;10(2):354-63.
-
198Kong YG, Kang JW, Kim YK, Seo H, Lim TH, Hwang S, et al. Preoperative coronary calcium score is predictive of early postoperative cardiovascular complications in liver transplant recipients. Br J Anaesth. 2015;114(3):437-43.
-
199Ehtisham J, Altieri M, Salamé E, Saloux E, Ollivier I, Hamon M. Coronary artery disease in orthotopic liver transplantation: pretransplant assessment and management. Liver Transpl. 2010;16(5):550-7.
-
200Bizouarn P, Ausseur A, Desseigne P, Le Teurnier Y, Nougarede B, Train M, et al. Early and late outcome after elective cardiac surgery in patients with cirrhosis. Ann Thorac Surg. 1999;67(5):1334-8.
-
201K/DOQI Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. 2005;45(4 Suppl 3):S1-S153.
-
202United States Renal Data System. 2015 USRDS annual data report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD. 2015.
-
203Ojo AO, Hanson JA, Wolfe RA, Leichtman AB, Agodoa LY, Port FK. Long-term survival in renal transplant recipients with graft function. Kidney Int. 2000;57(1):307-13.
-
204Wheeler DC, Steiger J. Evolution and etiology of cardiovascular diseases in renal transplant recipients. Transplantation. 2000;70(11 Suppl):SS41-5.
-
205Lentine KL, Costa SP, Weir MR, Robb JF, Fleisher LA, Kasiske BL, et al; American Heart Association Council on the Kidney in Cardiovascular Disease and Council on Peripheral Vascular Disease; American Heart Association; American College of Cardiology Foundation. Cardiac disease evaluation and management among kidney and liver transplantation candidates: a scientific statement from the American Heart Association and the American College of Cardiology Foundation: endorsed by the American Society of Transplant Surgeons, American Society of Transplantation, and National Kidney Foundation. Circulation. 2012;126(5):617-63.
-
206Hakeem A, Bhatti S, Chang SM. Screening and risk stratification of coronary artery disease in end-stage renal disease. JACC Cardiovasc Imaging. 2014;7(7):715-28.
-
207Lindley EM, Hall AK, Hess J, Abraham J, Smith B, Hopkins PN, et al. Cardiovascular Risk Assessment and Management in Prerenal Transplantation Candidates. Am J Cardiol. 2016;117(1):146-50.
-
208Kahn MR, Fallahi A, Kim MC, Esquitin R, Robbins MJ. Coronary artery disease in a large renal transplant population: implications for management. Am J Transplant. 2011;11(12):2665-74.
-
209De Lima JJ, Sabbaga E, Vieira ML, de Paula FJ, Ianhez LE, Krieger EM, et al. Coronary angiography is the best predictor of events in renal transplant candidates compared with noninvasive testing. Hypertension. 2003;42(3):263-8.
-
210Charytan D, Kuntz RE, Mauri L, DeFilippi C. Distribution of coronary artery disease and relation to mortality in asymptomatic hemodialysis patients. Am J Kidney Dis. 2007;49(3):409-16.
-
211Pascual J, Abramowicz D, Cochat P, Claas F, Dudley C, Harden P, et al. European renal best practice guideline on the management and evaluation of the kidney donor and recipient. Nefrologia. 2014;34(3):293-301.
-
212Abbud-Filho M, Adams PL, Alberú J, Cardella C, Chapman J, Cochat P, et al. A report of the Lisbon Conference on the care of the kidney transplant recipient. Transplantation. 2007;83(8 Suppl):S1-22.
-
213Gowdak LH, Arantes RL, de Paula FJ, Cesar LA, Ianhez LE, Krieger EM, et al. A new proposal for cardiovascular risk stratification in renal transplant candidates: time to review the American Society of Transplantation Guidelines? J Am Coll Cardiol. 2008;51(10 Suppl. A):A363.
-
214Gowdak LH, de Paula FJ, César LA, Martinez Filho EE, Ianhez LE, Krieger EM, et al. Screening for significant coronary artery disease in high-risk renal transplant candidates. Coron Artery Dis. 2007;18(7):553-8.
-
215V. Clinical algorithms on cardiovascular risk factors in renal patients. Nephrol Dial Transplant. 2000;15 Suppl 5:123-54.
-
216Gowdak LH, de Paula FJ, César LA, Bortolotto LA, de Lima JJ. A new risk score model to predict the presence of significant coronary artery disease in renal transplant candidates. Transplant Res. 2013;2(1):18.
-
217DeMaria EJ, Murr M, Byrne TK, Blackstone R, Grant JP, Budak A, et al. Validation of the obesity surgery mortality risk score in a multicenter study proves it stratifies mortality risk in patients undergoing gastric bypass for morbid obesity. Ann Surg. 2007;246(4):578-82.
-
218Ramanan B, Gupta PK, Gupta H, Fang X, Forse RA. Development and validation of a bariatric surgery mortality risk calculator. J Am Coll Surg. 2012;214(6):892-900.
-
219Gupta PK, Franck C, Miller WJ, Gupta H, Forse RA. Development and validation of a bariatric surgery morbidity risk calculator using the prospective, multicenter NSQIP dataset. J Am Coll Surg. 2011;212(3):301-9.
-
220Flum DR, Belle SH, King WC, Wahed AS, Berk P, Chapman W, et al. Perioperative safety in the longitudinal assessment of bariatric surgery. N Engl J Med. 2009;361(5):445-54.
-
221Aminian A, Andalib A, Khorgami Z, Cetin D, Burguera B, Bartholomew J, et al. Who should get extended thromboprophylaxis after bariatric surgery?: A risk assessment tool to guide indications for post-discharge pharmacoprophylaxis. Ann Surg. 2017;265(1):143-150.
-
222Ikesaka R, Delluc A, Le Gal G, Carrier M. Efficacy and safety of weight-adjusted heparin prophylaxis for the prevention of acute venous thromboembolism among obese patients undergoing bariatric surgery: a systematic review and meta-analysis. Thromb Res. 2014;133(4):682-7.
-
223Borkgren-Okonek MJ, Hart RW, Pantano JE, Rantis PC Jr, Guske PJ, Kane JM, et al. Enoxaparin thromboprophylaxis in gastric bypass patients: extended duration, dose stratification, and antifactor Xa activity. Surg Obes Relat Dis. 2008;4(5):625-31.
-
224Marques AC, Yu PC, Calderaro D, Gualandro DM, Caramelli B. High-risk patients undergoing major vascular surgery: to operate or not to operate? J Am Coll Cardiol. 2007;50(14):1398-9.
-
225Carmo GA, Calderaro D, Gualandro DM, Casella IB, Yu PC, Marques AC, et al. Carotid stenosis management: a review for the internist. Intern Emerg Med. 2014;9(2):133-42.
-
226Rosenfield K, Matsumura JS, Chaturvedi S, Riles T, Ansel GM, Metzger DC, et al; ACT I Investigators. Randomized trial of stent versus surgery for asymptomatic carotid stenosis. N Engl J Med. 2016;374(11):1011-20.
-
227Brott TG, Howard G, Roubin GS, Meschia JF, Mackey A, Brooks W, et al; CREST Investigators. Long-term results of stenting versus endarterectomy for carotid-artery stenosis. N Engl J Med. 2016;374(11):1021-31.
-
228Scannapieco FA. Pneumonia in nonambulatory patients: the role of oral bacteria and oral hygiene. J Am Dent Assoc. 2006;137 Suppl:21S-5S. Erratum in: J Am Dent Assoc. 2008;139(3):252.
-
229Brown RS, Rhodus NL. Epinephrine and local anesthesia revisited. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(4):401-8.
-
230Perry DJ, Noakes TJ, Helliwell PS; British Dental Society. Guidelines for the management of patients on oral anticoagulants requiring dental surgery. Br Dent J. 2007;203(7):389-93.
-
231Wahl MJ. Dental surgery in anticoagulated patients. Arch Intern Med. 1998;158(15):1610-6.
-
232Devani P, Lavery KM, Howell CJ. Dental extractions in patients on warfarin: is alteration of anticoagulant regime necessary? Br J Oral Maxillofac Surg. 1998;36(2):107-11.
-
233Blinder D, Manor Y, Martinowitz U, Taicher S. Dental extractions in patients maintained on oral anticoagulant therapy: comparison of INR value with occurrence of postoperative bleeding. Int J Oral Maxillofac Surg. 2001;30(6):518-21.
-
234Al-Mubarak S, Rass MA, Alsuwyed A, Alabdulaaly A, Ciancio S. Thromboembolic risk and bleeding in patients maintaining or stopping oral anticoagulant therapy during dental extraction. J Thromb Haemost. 2006;4(3):689-91.
-
235Johnston S. An evidence summary of the management of patients taking direct oral anticoagulants (DOACs) undergoing dental surgery. Int J Oral Maxillofac Surg. 2016;45(5):618-30.
-
236Lillis T, Ziakas A, Koskinas K, Tsirlis A, Giannoglou G. Safety of dental extractions during uninterrupted single or dual antiplatelet treatment. Am J Cardiol. 2011;108(7):964-7.
-
237Halley D, Weld-Moore R, Duane B. No evidence for stopping long-term aspirin therapy before tooth extraction. Evid Based Dent. 2015;16(4):118-9.
-
238Lu SY, Tsai CY, Lin LH, Lu SN. Dental extraction without stopping single or dual antiplatelet therapy: results of a retrospective cohort study. Int J Oral Maxillofac Surg. 2016;45(10):1293-8.
-
239Zhao B, Wang P, Dong Y, Zhu Y, Zhao H. Should aspirin be stopped before tooth extraction? A meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;119(5):522-30.
-
240Sánchez-Palomino P, Sánchez-Cobo P, Rodriguez-Archilla A, González-Jaranay M, Moreu G, Calvo-Guirado JL, et al. Dental extraction in patients receiving dual antiplatelet therapy. Med Oral Patol Oral Cir Bucal. 2015;20(5):e616-20.
-
241Olmos-Carrasco O, Pastor-Ramos V, Espinilla-Blanco R, Ortiz-Zárate A, García-Avila I, Rodríguez-Alonso E, et al. Hemorrhagic complications of dental extractions in 181 patients undergoing double antiplatelet therapy. J Oral Maxillofac Surg. 2015;73(2):203-10.
-
242Sadeghi-Ghahrody M, Yousefi-Malekshah SH, Karimi-Sari H, Yazdanpanah H, Rezaee-Zavareh MS, Yavarahmadi M. Bleeding after tooth extraction in patients taking aspirin and clopidogrel (Plavix(r)) compared with healthy controls. Br J Oral Maxillofac Surg. 2016;54(5):568-72.
-
243Dézsi BB, Koritsánszky L, Braunitzer G, Hangyási DB, Dézsi CA. Prasugrel versus clopidogrel: a comparative examination of local bleeding after dental extraction in patients receiving dual antiplatelet therapy. J Oral Maxillofac Surg. 2015;73(10):1894-900.
-
244O'Neill JL, Taheri A, Solomon JA, Pearce DJ. Postoperative hemorrhage risk after outpatient dermatologic surgery procedures. Dermatol Surg. 2014;40(1):74-6.
-
245Bordeaux JS, Martires KJ, Goldberg D, Pattee SF, Fu P, Maloney ME. Prospective evaluation of dermatologic surgery complications including patients on multiple antiplatelet and anticoagulant medications. J Am Acad Dermatol. 2011;65(3):576-83.
-
246Dixon AJ, Dixon MP, Dixon JB. Bleeding complications in skin cancer surgery are associated with warfarin but not aspirin therapy. Br J Surg. 2007;94(11):1356-60.
-
247Burger W, Chemnitius JM, Kneissl GD, Rücker G. Low-dose aspirin for secondary cardiovascular prevention - cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation - review and meta-analysis. J Intern Med. 2005;257(5):399-414.
-
248Palamaras I, Semkova K. Perioperative management of and recommendations for antithrombotic medications in dermatological surgery. Br J Dermatol. 2015;172(3):597-605.
-
249Cook-Norris RH, Michaels JD, Weaver AL, Phillips PK, Brewer JD, Roenigk RK, et al. Complications of cutaneous surgery in patients taking clopidogrel-containing anticoagulation. J Am Acad Dermatol. 2011;65(3):584-91.
-
250Blasdale C, Lawrence CM. Perioperative international normalized ratio level is a poor predictor of postoperative bleeding complications in dermatological surgery patients taking warfarin. Br J Dermatol. 2008;158(3):522-6.
-
251Rogers BH, Silvis SE, Nebel OT, Sugawa C, Mandelstam P. Complications of flexible fiberoptic colonoscopy and polypectomy. Gastrointest Endosc. 1975;22(2):73-7.
-
252Acosta RD, Abraham NS, Chandrasekhara V, Chathadi KV, Early DS, Eloubeidi MA, et al. The management of antithrombotic agents for patients undergoing GI endoscopy. Gastrointest Endosc. 2016;83(1):3-16. Erratum in: Gastrointest Endosc. 2016 Mar;83(3):678.
-
253Ono S, Fujishiro M, Kodashima S, Takahashi Y, Minatsuki C, Mikami-Matsuda R, et al. Evaluation of safety of endoscopic biopsy without cessation of antithrombotic agents in Japan. J Gastroenterol. 2012;47(7):770-4.
-
254Whitson MJ, Dikman AE, von Althann C, Sanyal S, Desai JC, Bamji ND, et al. Is gastroduodenal biopsy safe in patients receiving aspirin and clopidogrel?: a prospective, randomized study involving 630 biopsies. J Clin Gastroenterol. 2011;45(3):228-33.
-
255Veitch AM, Vanbiervliet G, Gershlick AH, Boustiere C, Baglin TP, Smith LA, et al. Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guidelines. Endoscopy. 2016;48(4):385-402.
-
256Becker RC, Scheiman J, Dauerman HL, Spencer F, Rao S, Sabatine M, et al; American College of Cardiology; American College of Gastroenterology. Management of platelet-directed pharmacotherapy in patients with atherosclerotic coronary artery disease undergoing elective endoscopic gastrointestinal procedures. J Am Coll Cardiol. 2009;54(24):2261-76.
-
257Kien-Fong Vu C, Chang F, Doig L, Meenan J. A prospective control study of the safety and cellular yield of EUS-guided FNA or Trucut biopsy in patients taking aspirin, nonsteroidal anti-inflammatory drugs, or prophylactic low molecular weight heparin. Gastrointest Endosc. 2006;63(6):808-13.
-
258Richter JA, Patrie JT, Richter RP, Henry ZH, Pop GH, Regan KA, et al. Bleeding after percutaneous endoscopic gastrostomy is linked to serotonin reuptake inhibitors, not aspirin or clopidogrel. Gastrointest Endosc. 2011;74(1):22-34.e1.
-
259Shiffman ML, Farrel MT, Yee YS. Risk of bleeding after endoscopic biopsy or polypectomy in patients taking aspirin or other NSAIDS. Gastrointest Endosc. 1994;40(4):458-62.
-
260Hui AJ, Wong RM, Ching JY, Hung LC, Chung SC, Sung JJ. Risk of colonoscopic polypectomy bleeding with anticoagulants and antiplatelet agents: analysis of 1657 cases. Gastrointest Endosc. 2004;59(1):44-8.
-
261Cotton PB, Garrow DA, Gallagher J, Romagnuolo J. Risk factors for complications after ERCP: a multivariate analysis of 11,497 procedures over 12 years. Gastrointest Endosc. 2009;70(1):80-8.
-
262Onal IK, Parlak E, Akdogan M, Yesil Y, Kuran SO, Kurt M, et al. Do aspirin and non-steroidal anti-inflammatory drugs increase the risk of post-sphincterotomy hemorrhage--a case-control study. Clin Res Hepatol Gastroenterol. 2013;37(2):171-6.
-
263Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;335(13):909-18.
-
264Yousfi M, Gostout CJ, Baron TH, Hernandez JL, Keate R, Fleischer DE, et al. Postpolypectomy lower gastrointestinal bleeding: potential role of aspirin. Am J Gastroenterol. 2004;99(9):1785-9.
-
265Nelson DB, Freeman ML. Major hemorrhage from endoscopic sphincterotomy: risk factor analysis. J Clin Gastroenterol. 1994;19(4):283-7.
-
266Shalman D, Gerson LB. Systematic review with meta-analysis: the risk of gastrointestinal haemorrhage post-polypectomy in patients receiving anti-platelet, anti-coagulant and/or thienopyridine medications. Aliment Pharmacol Ther. 2015;42(8):949-56.
-
267Cho SJ, Choi IJ, Kim CG, Lee JY, Nam BH, Kwak MH, et al. Aspirin use and bleeding risk after endoscopic submucosal dissection in patients with gastric neoplasms. Endoscopy. 2012;44(2):114-21.
-
268Metz AJ, Bourke MJ, Moss A, Williams SJ, Swan MP, Byth K. Factors that predict bleeding following endoscopic mucosal resection of large colonic lesions. Endoscopy. 2011;43(6):506-11.
-
269Gerson LB, Gage BF, Owens DK, Triadafilopoulos G. Effect and outcomes of the ASGE guidelines on the periendoscopic management of patients who take anticoagulants. Am J Gastroenterol. 2000;95(7):1717-24.
-
270Balbino M, Boin P, Prata TS. Perioperative management of anticoagulant users scheduled for glaucoma surgery: a survey among the Brazilian Glaucoma Society members. Arq Bras Oftalmol. 2013;76(6):363-5.
-
271Katz J, Feldman MA, Bass EB, Lubomski LH, Tielsch JM, Petty BG, et al; Study of Medical Testing for Cataract Surgery Team. Risks and benefits of anticoagulant and antiplatelet medication use before cataract surgery. Ophthalmology. 2003;110(9):1784-8. Erratum in: Ophthalmology. 2003;110(12):2309.
-
272Kallio H, Paloheimo M, Maunuksela EL. Haemorrhage and risk factors associated with retrobulbar/peribulbar block: a prospective study in 1383 patients. Br J Anaesth. 2000;85(5):708-11.
-
273Jamula E, Anderson J, Douketis JD. Safety of continuing warfarin therapy during cataract surgery: a systematic review and meta-analysis. Thromb Res. 2009;124(3):292-9.
-
274Calenda E, Lamothe L, Genevois O, Cardon A, Muraine M. Peribulbar block in patients scheduled for eye procedures and treated with clopidogrel. J Anesth. 2012;26(5):779-82.
-
275Kumar N, Jivan S, Thomas P, McLure H. Sub-Tenon's anesthesia with aspirin, warfarin, and clopidogrel. J Cataract Refract Surg. 2006;32(6):1022-5.
-
276Law SK, Song BJ, Yu F, Kurbanyan K, Yang TA, Caprioli J. Hemorrhagic complications from glaucoma surgery in patients on anticoagulation therapy or antiplatelet therapy. Am J Ophthalmol. 2008;145(4):736-46.
-
277Cobb CJ, Chakrabarti S, Chadha V, Sanders R. The effect of aspirin and warfarin therapy in trabeculectomy. Eye (Lond). 2007;21(5):598-603.
-
278Chauvaud D. [Anticoagulation and vitreoretinal surgery]. Bull Acad Natl Med. 2007;191(4-5):879-84.
-
279Fu AD, McDonald HR, Williams DF, Cantrill HL, Ryan EH, Johnson RN, et al. Anticoagulation with warfarin in vitreoretinal surgery. Retina. 2007;27(3):290-5.
-
280Ryan A, Saad T, Kirwan C, Keegan DJ, Acheson RW. Maintenance of perioperative antiplatelet and anticoagulant therapy for vitreoretinal surgery. Clin Exp Ophthalmol. 2013;41(4):387-95.
-
281Narendran N, Williamson TH. The effects of aspirin and warfarin therapy on haemorrhage in vitreoretinal surgery. Acta Ophthalmol Scand. 2003;81(1):38-40.
-
282Kong KL, Khan J. Ophthalmic patients on antithrombotic drugs: a review and guide to perioperative management. Br J Ophthalmol. 2015;99(8):1025-30.
-
283Wall A. The surgeon as stakeholder: making the case not to operate. Narrat Inq Bioeth. 2015;5(2):195-200.
-
284Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288(16):1987-93.
-
285Sasichay-Akkadechanunt T, Scalzi CC, Jawad AF. The relationship between nurse staffing and patient outcomes. J Nurs Adm. 2003;33(9):478-85.
-
286Carayon P, Gürses AP. A human factors engineering conceptual framework of nursing workload and patient safety in intensive care units. Intensive Crit Care Nurs. 2005;21(5):284-301.
-
287Bucholz EM, Butala NM, Ma S, Normand ST, Krumholz HM. Life Expectancy after Myocardial Infarction, According to Hospital Performance. N Engl J Med. 2016;375(14):1332-42.
-
288Birkmeyer JD, Siewers AE, Finlayson EV, Stukel TA, Lucas FL, Batista I, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346(15):1128-37.
-
289Brady AR, Gibbs JS, Greenhalgh RM, Powell JT, Sydes MR; POBBLE trial investigators. Perioperative beta-blockade (POBBLE) for patients undergoing infrarenal vascular surgery: results of a randomized double-blind controlled trial. J Vasc Surg. 2005;41(4):602-9.
-
290Juul AB, Wetterslev J, Gluud C, Kofoed-Enevoldsen A, Jensen G, Callesen T, et al; DIPOM Trial Group. Effect of perioperative beta blockade in patients with diabetes undergoing major non-cardiac surgery: randomised placebo controlled, blinded multicentre trial. BMJ. 2006;332(7556):1482.
-
291Yang H, Raymer K, Butler R, Parlow J, Roberts R. The effects of perioperative beta-blockade: results of the Metoprolol after Vascular Surgery (MaVS) study, a randomized controlled trial. Am Heart J. 2006;152(5):983-90.
-
292Devereaux PJ, Beattie WS, Choi PT, Badner NH, Guyatt GH, Villar JC, et al. How strong is the evidence for the use of perioperative beta blockers in non-cardiac surgery? Systematic review and meta-analysis of randomised controlled trials. BMJ. 2005;331(7512):313-21.
-
293Wiesbauer F, Schlager O, Domanovits H, Wildner B, Maurer G, Muellner M, et al. Perioperative beta-blockers for preventing surgery-related mortality and morbidity: a systematic review and meta-analysis. Anesth Analg. 2007;104(1):27-41.
-
294Lindenauer PK, Pekow P, Wang K, Mamidi DK, Gutierrez B, Benjamin EM. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Engl J Med. 2005;353(4):349-61.
-
295Devereaux PJ, Yang H, Yusuf S, Guyatt G, Leslie K, Villar JC, et al; POISE Study Group. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet. 2008;371(9627):1839-47.
-
296Poldermans D, Boersma E, Bax JJ, Thomson IR, van de Ven LL, Blankensteijn JD, et al. The effect of bisoprolol on perioperative mortality and myocardial infarction in high-risk patients undergoing vascular surgery. Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. N Engl J Med. 1999;341(24):1789-94.
-
297Beattie WS, Wijeysundera DN, Karkouti K, McCluskey S, Tait G. Does tight heart rate control improve beta-blocker efficacy? An updated analysis of the noncardiac surgical randomized trials. Anesth Analg. 2008;106(4):1039-48.
-
298Hoeks SE, Scholte Op Reimer WJ, van Urk H, Jörning PJ, Boersma E, Simoons ML, et al. Increase of 1-year mortality after perioperative beta-blocker withdrawal in endovascular and vascular surgery patients. Eur J Vasc Endovasc Surg. 2007;33(1):13-9.
-
299Durazzo AE, Machado FS, Ikeoka DT, De Bernoche C, Monachini MC, Puech-Leão P, et al. Reduction in cardiovascular events after vascular surgery with atorvastatin: a randomized trial. J Vasc Surg. 2004;39(5):967-75.
-
300Schouten O, Boersma E, Hoeks SE, Benner R, van Urk H, van Sambeek MR, et al; Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. Fluvastatin and perioperative events in patients undergoing vascular surgery. N Engl J Med. 2009;361(10):980-9.
-
301Antoniou GA, Hajibandeh S, Vallabhaneni SR, Brennan JA, Torella F. Meta-analysis of the effects of statins on perioperative outcomes in vascular and endovascular surgery. J Vasc Surg. 2015;61(2):519-32.e1.
-
302Lindenauer PK, Pekow P, Wang K, Gutierrez B, Benjamin EM. Lipid-lowering therapy and in-hospital mortality following major noncardiac surgery. JAMA. 2004;291(17):2092-9.
-
303Noordzij PG, Poldermans D, Schouten O, Schreiner F, Feringa HH, Dunkelgrun M, et al. Beta-blockers and statins are individually associated with reduced mortality in patients undergoing noncardiac, nonvascular surgery. Coron Artery Dis. 2007;18(1):67-72.
-
304Raju MG, Pachika A, Punnam SR, Gardiner JC, Shishehbor MH, Kapadia SR, et al. Statin therapy in the reduction of cardiovascular events in patients undergoing intermediate-risk noncardiac, nonvascular surgery. Clin Cardiol. 2013;36(8):456-61.
-
305Devereaux PJ, Chan MT, Alonso-Coello P, Walsh M, Berwanger O, Villar JC, et al; Vascular Events In Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA. 2012;307(21):2295-304. Erratum in: JAMA. 2012;307(24):2590.
-
306Berwanger O, Le Manach Y, Suzumura EA, Biccard B, Srinathan SK, Szczeklik W, et al; VISION Investigators. Association between pre-operative statin use and major cardiovascular complications among patients undergoing non-cardiac surgery: the VISION study. Eur Heart J. 2016;37(2):177-85.
-
307Fallouh N, Chopra V. Statin withdrawal after major noncardiac surgery: risks, consequences, and preventative strategies. J Hosp Med. 2012;7(7):573-9.
-
308Schouten O, Hoeks SE, Welten GM, Davignon J, Kastelein JJ, Vidakovic R, et al. Effect of statin withdrawal on frequency of cardiac events after vascular surgery. Am J Cardiol. 2007;100(2):316-20.
-
309Le Manach Y, Godet G, Coriat P, Martinon C, Bertrand M, Fléron MH, et al. The impact of postoperative discontinuation or continuation of chronic statin therapy on cardiac outcome after major vascular surgery. Anesth Analg. 2007;104(6):1326-33.
-
310Schouten O, Kertai MD, Bax JJ, Durazzo AE, Biagini E, Boersma E, et al. Safety of perioperative statin use in high-risk patients undergoing major vascular surgery. Am J Cardiol. 2005;95(5):658-60.
-
311Ellis JE, Drijvers G, Pedlow S, Laff SP, Sorrentino MJ, Foss JF, et al. Premedication with oral and transdermal clonidine provides safe and efficacious postoperative sympatholysis. Anesth Analg. 1994;79(6):1133-40.
-
312Stühmeier KD, Mainzer B, Cierpka J, Sandmann W, Tarnow J. Small, oral dose of clonidine reduces the incidence of intraoperative myocardial ischemia in patients having vascular surgery. Anesthesiology. 1996;85(4):706-12.
-
313Wijeysundera DN, Naik JS, Beattie WS. Alpha-2 adrenergic agonists to prevent perioperative cardiovascular complications: a meta-analysis. Am J Med. 2003;114(9):742-52.
-
314Oliver MF, Goldman L, Julian DG, Holme I. Effect of mivazerol on perioperative cardiac complications during non-cardiac surgery in patients with coronary heart disease: the European Mivazerol Trial (EMIT). Anesthesiology. 1999;91(4):951-61.
-
315Wallace AW, Galindez D, Salahieh A, Layug EL, Lazo EA, Haratonik KA, et al. Effect of clonidine on cardiovascular morbidity and mortality after noncardiac surgery. Anesthesiology. 2004;101(2):284-93.
-
316Devereaux PJ, Sessler DI, Leslie K, Kurz A, Mrkobrada M, Alonso-Coello P, et al; POISE-2 Investigators. Clonidine in patients undergoing noncardiac surgery. N Engl J Med. 2014;370(16):1504-13.
-
317Wijeysundera DN, Beattie WS. Calcium channel blockers for reducing cardiac morbidity after noncardiac surgery: a meta-analysis. Anesth Analg. 2003;97(3):634-41.
-
318Kertai MD, Westerhout CM, Varga KS, Acsady G, Gal J. Dihydropiridine calcium-channel blockers and perioperative mortality in aortic aneurysm surgery. Br J Anaesth. 2008;101(4):458-65.
-
319Beving H, Zhao C, Albåge A, Ivert T. Abnormally high platelet activity after discontinuation of acetylsalicylic acid treatment. Blood Coagul Fibrinolysis. 1996;7(1):80-4.
-
320Biondi-Zoccai GG, Lotrionte M, Agostoni P, Abbate A, Fusaro M, Burzotta F, et al. A systematic review and meta-analysis on the hazards of discontinuing or not adhering to aspirin among 50,279 patients at risk for coronary artery disease. Eur Heart J. 2006;27(22):2667-74.
-
321Devereaux PJ, Mrkobrada M, Sessler DI, Leslie K, Alonso-Coello P, Kurz A, et al; POISE-2 Investigators. Aspirin in patients undergoing noncardiac surgery. N Engl J Med. 2014;370(16):1494-503.
-
322Oscarsson A, Gupta A, Fredrikson M, Järhult J, Nyström M, Pettersson E, et al. To continue or discontinue aspirin in the perioperative period: a randomized, controlled clinical trial. Br J Anaesth. 2010;104(3):305-12.
-
323Mantz J, Samama CM, Tubach F, Devereaux PJ, Collet JP, Albaladejo P, et al; Stratagem Study Group. Impact of preoperative maintenance or interruption of aspirin on thrombotic and bleeding events after elective non-cardiac surgery: the multicentre, randomized, blinded, placebo-controlled, STRATAGEM trial. Br J Anaesth. 2011;107(6):899-910.
-
324Calderaro D, Pastana AF, Flores da Rocha TR, Yu PC, Gualandro DM, DeLuccia N, et al. Aspirin responsiveness safely lowers perioperative cardiovascular risk. J Vasc Surg. 2013;58(6):1593-9.
-
325Culkin DJ, Exaire EJ, Green D, Soloway MS, Gross AJ, Desai MR, et al. Anticoagulation and antiplatelet therapy in urological practice: ICUD/AUA review paper. J Urol. 2014;192(4):1026-34.
-
326Lee DJ, Rieken M, Halpern J, Zhao F, Pueschel H, Chughtai B, et al. Laser vaporization of the prostate with the 180-W XPS-Greenlight Laser in patients with ongoing platelet aggregation inhibition and oral anticoagulation. Urology. 2016;91:167-73.
-
327Hawn MT, Graham LA, Richman JR, Itani KM, Plomondon ME, Altom LK, et al. The incidence and timing of noncardiac surgery after cardiac stent implantation. J Am Coll Surg. 2012;214(4):658-66.
-
328Tokushige A, Shiomi H, Morimoto T, Ono K, Furukawa Y, Nakagawa Y, et al; CREDO-Kyoto PCI/CABG Registry Cohort-2 Investigators. Incidence and outcome of surgical procedures after coronary artery bypass grafting compared with those after percutaneous coronary intervention: a report from the Coronary Revascularization Demonstrating Outcome Study in Kyoto PCI/CABG Registry Cohort-2. Circ Cardiovasc Interv. 2014;7(4):482-91.
-
329Yende S, Wunderink RG. Effect of clopidogrel on bleeding after coronary artery bypass surgery. Crit Care Med. 2001;29(12):2271-5.
-
330Hongo RH, Ley J, Dick SE, Yee RR. The effect of clopidogrel in combination with aspirin when given before coronary artery bypass grafting. J Am Coll Cardiol. 2002;40(2):231-7.
-
331Grines CL, Bonow RO, Casey DE, Gardner TJ, Lockhart PB, Moliterno DJ, et al; American Heart Association.; American College of Cardiology.; Society for Cardiovascular Angiography and Interventions.; American College of Surgeons.; American Dental Association.; American College of Physicians. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. J Am Coll Cardiol. 2007;49(6):734-9.
-
332Albaladejo P, Marret E, Samama CM, Collet JP, Abhay K, Loutrel O, et al. Non-cardiac surgery in patients with coronary stents: the RECO study. Heart. 2011;97(19):1566-72.
-
333Eisenberg MJ, Richard PR, Libersan D, Filion KB. Safety of short-term discontinuation of antiplatelet therapy in patients with drug-eluting stents. Circulation. 2009;119(12):1634-42.
-
334Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, et al; TRITON-TIMI 38 Investigators. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357(20):2001-15.
-
335Gurbel PA, Bliden KP, Butler K, Tantry US, Gesheff T, Wei C, et al. Randomized double-blind assessment of the ONSET and OFFSET of the antiplatelet effects of ticagrelor versus clopidogrel in patients with stable coronary artery disease: the ONSET/OFFSET study. Circulation. 2009;120(25):2577-85.
-
336Held C, Asenblad N, Bassand JP, Becker RC, Cannon CP, Claeys MJ, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes undergoing coronary artery bypass surgery: results from the PLATO (Platelet Inhibition and Patient Outcomes) trial. J Am Coll Cardiol. 2011;57(6):672-84.
-
337Varenhorst C, Alström U, Scirica BM, Hogue CW, Åsenblad N, Storey RF, et al. Factors contributing to the lower mortality with ticagrelor compared with clopidogrel in patients undergoing coronary artery bypass surgery. J Am Coll Cardiol. 2012;60(17):1623-30.
-
338Savonitto S, D'Urbano M, Caracciolo M, Barlocco F, Mariani G, Nichelatti M, et al. Urgent surgery in patients with a recently implanted coronary drug-eluting stent: a phase II study of 'bridging' antiplatelet therapy with tirofiban during temporary withdrawal of clopidogrel. Br J Anaesth. 2010;104(3):285-91.
-
339Capodanno D, Musumeci G, Lettieri C, Limbruno U, Senni M, Guagliumi G, et al. Impact of bridging with perioperative low-molecular-weight heparin on cardiac and bleeding outcomes of stented patients undergoing non-cardiac surgery. Thromb Haemost. 2015;114(2):423-31.
-
340Eagle KA, Rihal CS, Mickel MC, Holmes DR, Foster ED, Gersh BJ. Cardiac risk of noncardiac surgery: influence of coronary disease and type of surgery in 3368 operations. CASS Investigators and University of Michigan Heart Care Program. Coronary Artery Surgery Study. Circulation. 1997;96(6):1882-7.
-
341Hassan SA, Hlatky MA, Boothroyd DB, Winston C, Mark DB, Brooks MM, et al. Outcomes of noncardiac surgery after coronary bypass surgery or coronary angioplasty in the Bypass Angioplasty Revascularization Investigation (BARI). Am J Med. 2001;110(4):260-6.
-
342Dawood MM, Gutpa DK, Southern J, Walia A, Atkinson JB, Eagle KA. Pathology of fatal perioperative myocardial infarction: implications regarding pathophysiology and prevention. Int J Cardiol. 1996;57(1):37-44.
-
343McFalls EO, Ward HB, Moritz TE, Goldman S, Krupski WC, Littooy F, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med. 2004;351(27):2795-804.
-
344Wong EY, Lawrence HP, Wong DT. The effects of prophylactic coronary revascularization or medical management on patient outcomes after noncardiac surgery--a meta-analysis. Can J Anaesth. 2007;54(9):705-17.
-
345Cesar LA, Ferreira JF, Armaganijan D, Gowdak LH, Mansur AP, Bodanese LC, et al; Sociedade Brasileira de Cardiologia. Guideline for stable coronary artery disease. Arq Bras Cardiol. 2014;103(2 Suppl 2):1-56.
-
346Kaluza GL, Joseph J, Lee JR, Raizner ME, Raizner AE. Catastrophic outcomes of noncardiac surgery soon after coronary stenting. J Am Coll Cardiol. 2000;35(5):1288-94.
-
347Nuttall GA, Brown MJ, Stombaugh JW, Michon PB, Hathaway MF, Lindeen KC, et al. Time and cardiac risk of surgery after bare-metal stent percutaneous coronary intervention. Anesthesiology. 2008;109(4):588-95.
-
348Rabbitts JA, Nuttall GA, Brown MJ, Hanson AC, Oliver WC, Holmes DR, et al. Cardiac risk of noncardiac surgery after percutaneous coronary intervention with drug-eluting stents. Anesthesiology. 2008;109(4):596-604.
-
349Calderaro D, Marques AC, Yu PC, Gualandro DM, Caramelli B. Bare metal stenting and noncardiac surgery, how long should we wait? Am J Cardiol. 2010;105(7):1040-1.
-
350Wijeysundera DN, Wijeysundera HC, Yun L, Wasowicz M, Beattie WS, Velianou JL, et al. Risk of elective major noncardiac surgery after coronary stent insertion: a population-based study. Circulation. 2012;126(11):1355-62.
-
351Hawn MT, Graham LA, Richman JS, Itani KM, Henderson WG, Maddox TM. Risk of major adverse cardiac events following noncardiac surgery in patients with coronary stents. JAMA. 2013;310(14):1462-72. Erratum in: JAMA. 2014;311(5):528.
-
352D'Ascenzo F, Moretti C, Bianco M, Bernardi A, Taha S, Cerrato E, et al. Meta-analysis of the duration of dual antiplatelet therapy in patients treated with second-generation drug-eluting stents. Am J Cardiol. 2016;117(11):1714-23.
-
353Feres F, Costa RA, Abizaid A, Leon MB, Marin-Neto JA, Botelho RV, et al; OPTIMIZE Trial Investigators. Three vs twelve months of dual antiplatelet therapy after zotarolimus-eluting stents: the OPTIMIZE randomized trial. JAMA. 2013;310(23):2510-22.
-
354Levine GN, Bates ER, Bittl JA, Brindis RG, Fihn SD, Fleisher LA, et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2016;68(10):1082-115.
-
355Holcomb CN, Graham LA, Richman JS, Rhyne RR, Itani KM, Maddox TM, et al. The incremental risk of noncardiac surgery on adverse cardiac events following coronary stenting. J Am Coll Cardiol. 2014;64(25):2730-9.
-
356Holcomb CN, Hollis RH, Graham LA, Richman JS, Valle JA, Itani KM, et al. Association of Coronary Stent Indication With Postoperative Outcomes Following Noncardiac Surgery. JAMA Surg. 2016;151(5):462-9.
-
357Excellence NIfHaC. Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in inpatients undergoing surgery. NICE clinical guideline No. 46:1-160. [Accessed in 2008 Mar 31]. Available from: http://www.nice.org.uk/CG046
» http://www.nice.org.uk/CG046 -
358Anderson FA, Wheeler HB, Goldberg RJ, Hosmer DW, Forcier A. The prevalence of risk factors for venous thromboembolism among hospital patients. Arch Intern Med. 1992;152(8):1660-4.
-
359Rosendaal FR. Risk factors for venous thrombotic disease. Thromb Haemost. 1999;82(2):610-9.
-
360Rosendaal FR. Venous thrombosis: a multicausal disease. Lancet. 1999;353(9159):1167-73.
-
361Heit JA, O'Fallon WM, Petterson TM, Lohse CM, Silverstein MD, Mohr DN, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med. 2002;162(11):1245-8.
-
362Anderson FA, Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I9-16.
-
363Samama MM, Dahl OE, Quinlan DJ, Mismetti P, Rosencher N. Quantification of risk factors for venous thromboembolism: a preliminary study for the development of a risk assessment tool. Haematologica. 2003;88(12):1410-21.
-
364Edmonds MJ, Crichton TJ, Runciman WB, Pradhan M. Evidence-based risk factors for postoperative deep vein thrombosis. ANZ J Surg. 2004;74(12):1082-97.
-
365Kucher N, Tapson VF, Goldhaber SZ; DVT FREE Steering Committee. Risk factors associated with symptomatic pulmonary embolism in a large cohort of deep vein thrombosis patients. Thromb Haemost. 2005;93(3):494-8.
-
366Gangireddy C, Rectenwald JR, Upchurch GR, Wakefield TW, Khuri S, Henderson WG, et al. Risk factors and clinical impact of postoperative symptomatic venous thromboembolism. J Vasc Surg. 2007;45(2):335-41.
-
367Gould MK, Garcia DA, Wren SM, Karanicolas PJ, Arcelus JI, Heit JA, et al; American College of Chest Physicians. Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e227S-77S. Erratum in: Chest. 2012;141(5):1369.
-
368Geerts WH, Pineo GF, Heit JA, Bergqvist D, Lassen MR, Colwell CW, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 Suppl):338S-400S.
-
369Ahmad HA, Geissler A, MacLellan DG. Deep venous thrombosis prophylaxis: are guidelines being followed? ANZ J Surg. 2002;72(5):331-4.
-
370Deheinzelin D, Braga AL, Martins LC, Martins MA, Hernandez A, Yoshida WB, et al; Trombo Risc Investigators. Incorrect use of thromboprophylaxis for venous thromboembolism in medical and surgical patients: results of a multicentric, observational and cross-sectional study in Brazil. J Thromb Haemost. 2006;4(6):1266-70.
-
371Caprini JA. Thrombosis risk assessment as a guide to quality patient care. Dis Mon. 2005;51(2-3):70-8.
-
372Caprini JA, Arcelus JI, Hasty JH, Tamhane AC, Fabrega F. Clinical assessment of venous thromboembolic risk in surgical patients. Semin Thromb Hemost. 1991;17 Suppl 3:304-12.
-
373Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, et al; American College of Chest Physicians. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e278S-325S.
-
374Douketis JD. Perioperative management of patients who are receiving warfarin therapy: an evidence-based and practical approach. Blood. 2011;117(19):5044-9.
-
375Spyropoulos AC, Douketis JD. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood. 2012;120(15):2954-62.
-
376Torn M, Rosendaal FR. Oral anticoagulation in surgical procedures: risks and recommendations. Br J Haematol. 2003;123(4):676-82.
-
377Kakkar VV, Cohen AT, Edmonson RA, Phillips MJ, Cooper DJ, Das SK, et al. Low molecular weight versus standard heparin for prevention of venous thromboembolism after major abdominal surgery. The Thromboprophylaxis Collaborative Group. Lancet. 1993;341(8840):259-65.
-
378Jaffer AK. Perioperative management of warfarin and antiplatelet therapy. Cleve Clin J Med. 2009;76 Suppl 4:S37-44.
-
379Gallego P, Apostolakis S, Lip GY. Bridging evidence-based practice and practice-based evidence in periprocedural anticoagulation. Circulation. 2012;126(13):1573-6.
-
380Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-94S. Erratum in: Chest. 2012;142(6):1698-704.
-
381Mehran R, Rao SV, Bhatt DL, Gibson CM, Caixeta A, Eikelboom J, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123(23):2736-47.
-
382Omran H, Bauersachs R, Rübenacker S, Goss F, Hammerstingl C. The HAS-BLED score predicts bleedings during bridging of chronic oral anticoagulation. Results from the national multicentre BNK Online bRiDging REgistRy (BORDER). Thromb Haemost. 2012;108(1):65-73.
-
383Lip GY. Implications of the CHA(2)DS(2)-VASc and HAS-BLED Scores for thromboprophylaxis in atrial fibrillation. Am J Med. 2011;124(2):111-4.
-
384Lorga Filho AM, Azmus AD, Soeiro AM, Quadros AS, Avezum A, Marques AC, et al; Sociedade Brasileira de Cardiologia. [Brazilian guidelines on platelet antiaggregants and anticoagulants in cardiology]. Arq Bras Cardiol. 2013;101(3 Suppl 3):1-95.
-
385Machado FS. Perioperatório do paciente em uso de anticoagulante. In: Machado FS, Martins MA, Caramelli B. (editores). Perioperatório: procedimentos clínicos: Sarvier; 2004. p. 105-9.
-
386Ministério da Saúde. Agência Nacional de Vigilância Sanitária (ANVISA). RDC nº10, de 23 de janeiro de 2004. Diretrizes para o uso de plasma fresco congelado PFC e plasma virus inativo. Diário Oficial da União, Poder Executivo, Brasília (DF) de 26 de janeiro de 2004. [Citado em 2004 jan 10]. Disponível em: http://pegasus.fmrp.usp.br/projeto/legislacao/rdc%2010%20e%2023%2001%2004.pdf
» http://pegasus.fmrp.usp.br/projeto/legislacao/rdc%2010%20e%2023%2001%2004.pdf -
387O'Shaughnessy DF, Atterbury C, Bolton Maggs P, Murphy M, Thomas D, Yates S, et al; British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol. 2004;126(1):11-28.
-
388Schulman S, Crowther MA. How I treat with anticoagulants in 2012: new and old anticoagulants, and when and how to switch. Blood. 2012;119(13):3016-23.
-
389Lai A, Davidson N, Galloway SW, Thachil J. Perioperative management of patients on new oral anticoagulants. Br J Surg. 2014;101(7):742-9. Erratum in: Br J Surg. 2014;101(12):1624.
-
390Stangier J, Rathgen K, Stähle H, Gansser D, Roth W. The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects. Br J Clin Pharmacol. 2007;64(3):292-303.
-
391Fonseca NM, Alves RR, Pontes JP; Sociedade Brasileira de Anestesiologia. SBA recommendations for regional anesthesia safety in patients taking anticoagulants. Braz J Anesthesiol. 2014;64(1):1-15.
-
392Tummala R, Kavtaradze A, Gupta A, Ghosh RK. Specific antidotes against direct oral anticoagulants: a comprehensive review of clinical trials data. Int J Cardiol. 2016;214:292-8.
-
393Zalpour A, Oo TH. Update on edoxaban for the prevention and treatment of thromboembolism: clinical applications based on current evidence. Adv Hematol. 2015;2015:920361.
-
394Bin Abdulhak AA, Baddour LM, Erwin PJ, Hoen B, Chu VH, Mensah GA, et al. Global and regional burden of infective endocarditis, 1990-2010: a systematic review of the literature. Glob Heart. 2014;9(1):131-43.
-
395Werdan K, Dietz S, Löffler B, Niemann S, Bushnaq H, Silber RE, et al. Mechanisms of infective endocarditis: pathogen-host interaction and risk states. Nat Rev Cardiol. 2014;11(1):35-50.
-
396Overholser CD, Moreillon P, Glauser MP. Experimental bacterial endocarditis after dental extractions in rats with periodontitis. J Infect Dis. 1987;155(1):107-12.
-
397Okell CC, Elliott SD. Bacteraemia and oral sepsis with special reference to the aetiology of subacute endocarditis. Lancet. 1935;2:869-72.
-
398Beechen II, Laston DJ, Garbarino VE. Transitory bacteraemia as related to the operation of vital pulpotomy. Oral Surg Oral Med Oral Path. 1956;8(9):902-5.
-
399Bender IB, Seltzer S, Yermish M. The incidence of bacteremia in endodontic manipulation: preliminary report. 1960. J Endod. 2003;29(11):697-700.
-
400Forner L, Larsen T, Kilian M, Holmstrup P. Incidence of bacteremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J Clin Periodontol. 2006;33(6):401-7.
-
401Glauser MP, Bernard JP, Moreillon P, Francioli P. Successful single-dose amoxicillin prophylaxis against experimental streptococcal endocarditis: evidence for two mechanisms of protection. J Infect Dis. 1983;147(3):568-75.
-
402Shanson DC, Akash S, Harris M, Tadayon M. Erythromycin stearate, 1.5 g, for the oral prophylaxis of streptococcal bacteraemia in patients undergoing dental extraction: efficacy and tolerance. J Antimicrob Chemother. 1985;15(1):83-90.
-
403Van der Meer JT, Van Wijk W, Thompson J, Vandenbroucke JP, Valkenburg HA, Michel MF. Efficacy of antibiotic prophylaxis for prevention of native-valve endocarditis. Lancet. 1992;339(8786):135-9.
-
404Strom BL, Abrutyn E, Berlin JA, Kinman JL, Feldman RS, Stolley PD, et al. Dental and cardiac risk factors for infective endocarditis. A population-based, case-control study. Ann Intern Med. 1998;129(10):761-9.
-
405Duval X, Alla F, Hoen B, Danielou F, Larrieu S, Delahaye F, et al. Estimated risk of endocarditis in adults with predisposing cardiac conditions undergoing dental procedures with or without antibiotic prophylaxis. Clin Infect Dis. 2006;42(12):e102-7.
-
406Roberts GJ. Dentists are innocent! "Everyday" bacteremia is the real culprit: a review and assessment of the evidence that dental surgical procedures are a principal cause of bacterial endocarditis in children. Pediatr Cardiol. 1999;20(5):317-25.
-
407Lucas V, Roberts GJ. Odontogenic bacteremia following tooth cleaning procedures in children. Pediatr Dent. 2000;22(2):96-100.
-
408Seymour RA, Lowry R, Whitworth JM, Martin MV. Infective endocarditis, dentistry and antibiotic prophylaxis; time for a rethink? Br Dent J. 2000;189(11):610-6.
-
409Lockhart PB, Brennan MT, Sasser HC, Fox PC, Paster BJ, Bahrani-Mougeot FK. Bacteremia associated with toothbrushing and dental extraction. Circulation. 2008;117(24):3118-25.
-
410Lee P, Shanson D. Results of a UK survey of fatal anaphylaxis after oral amoxicillin. J Antimicrob Chemother. 2007;60(5):1172-3.
-
411Prophylaxis against infective endocarditis: antimicrobial prophylaxis against infective endocarditis in adults and children undergoing interventional procedures (CG64). National Institute for Health and Care Excellence (NICE) http://wwwniceorguk/guidance/CG64 [Internet].
» http://wwwniceorguk/guidance/CG64 -
412Danchin N, Duval X, Leport C. Prophylaxis of infective endocarditis: French recommendations 2002. Heart. 2005;91(6):715-8.
-
413Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, Levison M, et al; American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee; American Heart Association Council on Cardiovascular Disease in the Young; American Heart Association Council on Clinical Cardiology; American Heart Association Council on Cardiovascular Surgery and Anesthesia; Quality of Care and Outcomes Research Interdisciplinary Working Group. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116(15):1736-54. Erratum in: Circulation. 2007;116(15):e376-7.
-
414Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075-128.
-
415Duval X, Delahaye F, Alla F, Tattevin P, Obadia JF, Le Moing V, et al; AEPEI Study Group. Temporal trends in infective endocarditis in the context of prophylaxis guideline modifications: three successive population-based surveys. J Am Coll Cardiol. 2012;59(22):1968-76.
-
416Desimone DC, Tleyjeh IM, Correa de Sa DD, Anavekar NS, Lahr BD, Sohail MR, et al; Mayo Cardiovascular Infections Study Group. Incidence of infective endocarditis caused by viridans group streptococci before and after publication of the 2007 American Heart Association's endocarditis prevention guidelines. Circulation. 2012;126(1):60-4.
-
417Pasquali SK, He X, Mohamad Z, McCrindle BW, Newburger JW, Li JS, et al. Trends in endocarditis hospitalizations at US children's hospitals: impact of the 2007 American Heart Association Antibiotic Prophylaxis Guidelines. Am Heart J. 2012;163(5):894-9.
-
418Dayer MJ, Jones S, Prendergast B, Baddour LM, Lockhart PB, Thornhill MH. Incidence of infective endocarditis in England, 2000-13: a secular trend, interrupted time-series analysis. Lancet. 2015;385(9974):1219-28.
-
419Dayer MJ, Chambers JB, Prendergast B, Sandoe JA, Thornhill MH. NICE guidance on antibiotic prophylaxis to prevent infective endocarditis: a survey of clinicians' attitudes. QJM. 2013;106(3):237-43.
-
420Pant S, Patel NJ, Deshmukh A, Golwala H, Patel N, Badheka A, et al. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J Am Coll Cardiol. 2015;65(19):2070-6.
-
421Strom BL, Abrutyn E, Berlin JA, Kinman JL, Feldman RS, Stolley PD, et al. Risk factors for infective endocarditis: oral hygiene and nondental exposures. Circulation. 2000;102(23):2842-8.
-
422Yu CH, Minnema BJ, Gold WL. Bacterial infections complicating tongue piercing. Can J Infect Dis Med Microbiol. 2010;21(1):e70-4.
-
423Landesberg G, Mosseri M, Wolf Y, Vesselov Y, Weissman C. Perioperative myocardial ischemia and infarction: identification by continuous 12-lead electrocardiogram with online ST-segment monitoring. Anesthesiology. 2002;96(2):264-70.
-
424Landesberg G. Monitoring for myocardial ischemia. Best Pract Res Clin Anaesthesiol. 2005;19(1):77-95.
-
425Raby KE, Barry J, Creager MA, Cook EF, Weisberg MC, Goldman L. Detection and significance of intraoperative and postoperative myocardial ischemia in peripheral vascular surgery. JAMA. 1992;268(2):222-7.
-
426Zakowski MI, Ramanathan S, Baratta JB, Cziner D, Goldstein MJ, Kronzon I, et al. Electrocardiographic changes during cesarean section: a cause for concern? Anesth Analg. 1993;76(1):162-7.
-
427Mangano DT, Browner WS, Hollenberg M, Li J, Tateo IM. Long-term cardiac prognosis following noncardiac surgery. The Study of Perioperative Ischemia Research Group. JAMA. 1992;268(2):233-9.
-
428Landesberg G, Shatz V, Akopnik I, Wolf YG, Mayer M, Berlatzky Y, et al. Association of cardiac troponin, CK-MB, and postoperative myocardial ischemia with long-term survival after major vascular surgery. J Am Coll Cardiol. 2003;42(9):1547-54.
-
429Lopez-Jimenez F, Goldman L, Sacks DB, Thomas EJ, Johnson PA, Cook EF, et al. Prognostic value of cardiac troponin T after noncardiac surgery: 6-month follow-up data. J Am Coll Cardiol. 1997;29(6):1241-5.
-
430Bursi F, Babuin L, Barbieri A, Politi L, Zennaro M, Grimaldi T, et al. Vascular surgery patients: perioperative and long-term risk according to the ACC/AHA guidelines, the additive role of post-operative troponin elevation. Eur Heart J. 2005;26(22):2448-56.
-
431Barbagallo M, Casati A, Spadini E, Bertolizio G, Kepgang L, Tecchio T, et al. Early increases in cardiac troponin levels after major vascular surgery is associated with an increased frequency of delayed cardiac complications. J Clin Anesth. 2006;18(4):280-5.
-
432Winkel TA, Schouten O, van Kuijk JP, Verhagen HJ, Bax JJ, Poldermans D. Perioperative asymptomatic cardiac damage after endovascular abdominal aneurysm repair is associated with poor long-term outcome. J Vasc Surg. 2009;50(4):749-54. Erratum in: J Vasc Surg. 2010;51(1):289.
-
433Kim LJ, Martinez EA, Faraday N, Dorman T, Fleisher LA, Perler BA, et al. Cardiac troponin I predicts short-term mortality in vascular surgery patients. Circulation. 2002;106(18):2366-71.
-
434Redfern G, Rodseth RN, Biccard BM. Outcomes in vascular surgical patients with isolated postoperative troponin leak: a meta-analysis. Anaesthesia. 2011;66(7):604-10.
-
435Reichlin T, Hochholzer W, Bassetti S, Steuer S, Stelzig C, Hartwiger S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361(9):858-67.
-
436Noordzij PG, van Geffen O, Dijkstra IM, Boerma D, Meinders AJ, Rettig TC, et al. High-sensitive cardiac troponin T measurements in prediction of non-cardiac complications after major abdominal surgery. Br J Anaesth. 2015;114(6):909-18.
-
437Lee GR, Jhanji S, Tarrant H, James S, Pearse RM, Fitzgibbon M. Peri-operative troponin monitoring using a prototype high-sensitivity cardiac troponin I (hs-cTnI) assay: comparisons with hs-cTnT and contemporary cTnI assays. Ann Clin Biochem. 2014;51(Pt 2):258-68.
-
438Gualandro DM, Puelacher C, Mueller C. High-sensitivity cardiac troponin in acute conditions. Curr Opin Crit Care. 2014;20(5):472-7.
-
439Roongsritong C, Warraich I, Bradley C. Common causes of troponin elevations in the absence of acute myocardial infarction: incidence and clinical significance. Chest. 2004;125(5):1877-84.
-
440Rinfret S, Goldman L, Polanczyk CA, Cook EF, Lee TH. Value of immediate postoperative electrocardiogram to update risk stratification after major noncardiac surgery. Am J Cardiol. 2004;94(8):1017-22.
-
441Böttiger BW, Motsch J, Teschendorf P, Rehmert GC, Gust R, Zorn M, et al. Postoperative 12-lead ECG predicts peri-operative myocardial ischaemia associated with myocardial cell damage. Anaesthesia. 2004;59(11):1083-90.
-
442Martinez EA, Nass CM, Jermyn RM, Rosenbaum SH, Akhtar S, Chan DW, et al. Intermittent cardiac troponin-I screening is an effective means of surveillance for a perioperative myocardial infarction. J Cardiothorac Vasc Anesth. 2005;19(5):577-82.
-
443Becker RC, Underwood DA. Myocardial infarction in patients undergoing noncardiac surgery. Cleve Clin J Med. 1987;54(1):25-8.
-
444Devereaux PJ, Xavier D, Pogue J, Guyatt G, Sigamani A, Garutti I, et al; POISE (PeriOperative ISchemic Evaluation) Investigators. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: a cohort study. Ann Intern Med. 2011;154(8):523-8.
-
445Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et al. Third universal definition of myocardial infarction. J Am Coll Cardiol. 2012;60(16):1581-98.
-
446Botto F, Alonso-Coello P, Chan MT, Villar JC, Xavier D, Srinathan S, et al; Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Writing Group, on behalf of The Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Investigators.; Appendix 1. The Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Study Investigators Writing Group.; Appendix 2. The Vascular events In noncardiac Surgery patIents cOhort evaluatioN Operations Committee.; Vascular events In noncardiac Surgery patIents cOhort evaluatioN VISION Study Investigators. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120(3):564-78.
-
447Nicolau JC, Timerman A, Marin-Neto JA, Piegas LS, Barbosa CJ, Franci A, et al; Sociedade Brasileira de Cardiologia. [Guidelines of Sociedade Brasileira de Cardiologia for unstable angina and non-ST-segment elevation myocardial infarction (II edition, 2007) 2013-2014 update]. Arq Bras Cardiol. 2014;102(3 Suppl 1):1-61.
-
448Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, et al; American College of Cardiology.; American Heart Association Task Force on Practice Guidelines.; Society for Cardiovascular Angiography and Interventions.; Society of Thoracic Surgeons.; American Association for Clinical Chemistry. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139-228. Erratum in: J Am Coll Cardiol. 2014;64(24):2713-4.
-
449Berger PB, Bellot V, Bell MR, Horlocker TT, Rihal CS, Hallett JW, et al. An immediate invasive strategy for the treatment of acute myocardial infarction early after noncardiac surgery. Am J Cardiol. 2001;87(9):1100-2, A6, A9.
-
450Frendl G, Sodickson AC, Chung MK, Waldo AL, Gersh BJ, Tisdale JE, et al; American Association of Thoracic Surgery. 2014 AATS guidelines for the prevention and management of perioperative atrial fibrillation and flutter for thoracic surgical procedures. Executive summary. J Thorac Cardiovasc Surg. 2014;148(3):772-91.
-
451Bhave PD, Goldman LE, Vittinghoff E, Maselli J, Auerbach A. Incidence, predictors, and outcomes associated with postoperative atrial fibrillation after major noncardiac surgery. Am Heart J. 2012;164(6):918-24.
-
452Kanji S, Williamson DR, Yaghchi BM, Albert M, McIntyre L, Canadian Critical Care Trials Group. Epidemiology and management of atrial fibrillation in medical and noncardiac surgical adult intensive care unit patients. J Crit Care. 2012;27(3):326.e1-8.
-
453Danelich IM, Lose JM, Wright SS, Asirvatham SJ, Ballinger BA, Larson DW, et al. Practical management of postoperative atrial fibrillation after noncardiac surgery. J Am Coll Surg. 2014;219(4):831-41.
-
454January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, et al; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267. Erratum in: Circulation. 2014;130(23):e272-4.
-
455Ho KM, Sheridan DJ, Paterson T. Use of intravenous magnesium to treat acute onset atrial fibrillation: a meta-analysis. Heart. 2007;93(11):1433-40.
-
456Upshaw J, Kiernan MS. Preoperative cardiac risk assessment for noncardiac surgery in patients with heart failure. Curr Heart Fail Rep. 2013;10(2):147-56.
-
457Farzi S, Stojakovic T, Marko T, Sankin C, Rehak P, Gumpert R, et al. Role of N-terminal pro B-type natriuretic peptide in identifying patients at high risk for adverse outcome after emergent non-cardiac surgery. Br J Anaesth. 2013;110(4):554-60.
-
458Nordling P, Kiviniemi T, Strandberg M, Strandberg N, Airaksinen J. Predicting the outcome of hip fracture patients by using N-terminal fragment of pro-B-type natriuretic peptide. BMJ Open. 2016;6(2):e009416.
-
459Maile MD, Engoren MC, Tremper KK, Jewell E, Kheterpal S. Worsening preoperative heart failure is associated with mortality and noncardiac complications, but not myocardial infarction after noncardiac surgery: a retrospective cohort study. Anesth Analg. 2014;119(3):522-32.
-
460Wells PS, Anderson DR, Rodger M, Ginsberg JS, Kearon C, Gent M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer. Thromb Haemost. 2000;83(3):416-20.
-
461Wells PS, Anderson DR, Bormanis J, Guy F, Mitchell M, Gray L, et al. Value of assessment of pretest probability of deep-vein thrombosis in clinical management. Lancet. 1997;350(9094):1795-8.
-
462Donnelly R, Hinwood D, London NJ. ABC of arterial and venous disease. Non-invasive methods of arterial and venous assessment. BMJ. 2000;320(7236):698-701.
-
463Mattos MA, Londrey GL, Leutz DW, Hodgson KJ, Ramsey DE, Barkmeier LD, et al. Color-flow duplex scanning for the surveillance and diagnosis of acute deep venous thrombosis. J Vasc Surg. 1992;15(2):366-75.
-
464Di Nisio M, Squizzato A, Rutjes AW, Büller HR, Zwinderman AH, Bossuyt PM. Diagnostic accuracy of D-dimer test for exclusion of venous thromboembolism: a systematic review. J Thromb Haemost. 2007;5(2):296-304. Erratum in: J Thromb Haemost. 2013;11(10):1942.
-
465Lensing AW, Büller HR, Prandoni P, Batchelor D, Molenaar AH, Cogo A, et al. Contrast venography, the gold standard for the diagnosis of deep-vein thrombosis: improvement in observer agreement. Thromb Haemost. 1992;67(1):8-12.
-
466Carpenter JP, Holland GA, Baum RA, Owen RS, Carpenter JT, Cope C. Magnetic resonance venography for the detection of deep venous thrombosis: comparison with contrast venography and duplex Doppler ultrasonography. J Vasc Surg. 1993;18(5):734-41.
-
467Duwe KM, Shiau M, Budorick NE, Austin JH, Berkmen YM. Evaluation of the lower extremity veins in patients with suspected pulmonary embolism: a retrospective comparison of helical CT venography and sonography. 2000 ARRS Executive Council Award I. American Roentgen Ray Society. AJR Am J Roentgenol. 2000;175(6):1525-31.
-
468Garg K, Kemp JL, Wojcik D, Hoehn S, Johnston RJ, Macey LC, et al. Thromboembolic disease: comparison of combined CT pulmonary angiography and venography with bilateral leg sonography in 70 patients. AJR Am J Roentgenol. 2000;175(4):997-1001.
-
469Stein PD, Beemath A, Matta F, Weg JG, Yusen RD, Hales CA, et al. Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II. Am J Med. 2007;120(10):871-9.
-
470Stein PD, Matta F, Musani MH, Diaczok B. Silent pulmonary embolism in patients with deep venous thrombosis: a systematic review. Am J Med. 2010;123(5):426-31.
-
471Anderson DR, Kahn SR, Rodger MA, Kovacs MJ, Morris T, Hirsch A, et al. Computed tomographic pulmonary angiography vs ventilation-perfusion lung scanning in patients with suspected pulmonary embolism: a randomized controlled trial. JAMA. 2007;298(23):2743-53.
-
472Wittram C, Waltman AC, Shepard JA, Halpern E, Goodman LR. Discordance between CT and angiography in the PIOPED II study. Radiology. 2007;244(3):883-9.
-
473Büller HR, Décousus H, Grosso MA, Mercuri M, Middeldorp S, Prins MH, et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med. 2013;369(15):1406-15. Erratum in: N Engl J Med. 2014;370(4):390.
-
474Schulman S, Kakkar AK, Goldhaber SZ, Schellong S, Eriksson H, Mismetti P, et al; RE-COVER II Trial Investigators. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation. 2014;129(7):764-72.
-
475Agnelli G, Buller HR, Cohen A, Curto M, Gallus AS, Johnson M, et al; AMPLIFY Investigators. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013; 369(9):799-808.
-
476Büller HR, Prins MH, Lensin AW, Decousus H, Jacobson BF, Minar E, et al; EINSTEIN-PE Investigators. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366(14):1287-97.
-
477Castellucci LA, Cameron C, Le Gal G, Rodger MA, Coyle D, Wells PS, et al. Clinical and safety outcomes associated with treatment of acute venous thromboembolism: a systematic review and meta-analysis. JAMA. 2014;312(11):1122-35.
-
478Lee AY, Kamphuisen PW, Meyer G, Bauersachs R, Janas MS, Jarner MF, et al; CATCH Investigators. Tinzaparin vs warfarin for treatment of acute venous thromboembolism in patients with active cancer: a randomized clinical trial. JAMA. 2015;314(7):677-86.
-
479Carrier M, Cameron C, Delluc A, Castellucci L, Khorana AA, Lee AY. Efficacy and safety of anticoagulant therapy for the treatment of acute cancer-associated thrombosis: a systematic review and meta-analysis. Thromb Res. 2014;134(6):1214-9.
-
480Bochenek T, Nizankowski R. The treatment of venous thromboembolism with low-molecular-weight heparins. A meta-analysis. Thromb Haemost. 2012;107(4):699-716.
-
481Iorio A, Kearon C, Filippucci E, Marcucci M, Macura A, Pengo V, et al. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk factor: a systematic review. Arch Intern Med. 2010;170(19):1710-6.
-
482Boutitie F, Pinede L, Schulman S, Agnelli G, Raskob G, Julian J, et al. Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism on risk of recurrence after stopping treatment: analysis of individual participants' data from seven trials. BMJ. 2011;342:d3036.
-
483Prandoni P, Noventa F, Ghirarduzzi A, Pengo V, Bernardi E, Pesavento R, et al. The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute proximal deep vein thrombosis or pulmonary embolism. A prospective cohort study in 1,626 patients. Haematologica. 2007;92(2):199-205.
-
484Palareti G, Legnani C, Lee A, Manotti C, Hirsh J, D'Angelo A, et al. A comparison of the safety and efficacy of oral anticoagulation for the treatment of venous thromboembolic disease in patients with or without malignancy. Thromb Haemost. 2000;84(5):805-10.
-
485Prandoni P, Lensing AW, Cogo A, Cuppini S, Villalta S, Carta M, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. 1996;125(1):1-7.
-
486Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic therapy for VTE disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315-52.
-
487Masuda EM, Kistner RL, Musikasinthorn C, Liquido F, Geling O, He Q. The controversy of managing calf vein thrombosis. J Vasc Surg. 2012;55(2):550-61.
-
488Kearon C. Natural history of venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I22-30.
-
489Macdonald PS, Kahn SR, Miller N, Obrand D. Short-term natural history of isolated gastrocnemius and soleal vein thrombosis. J Vasc Surg. 2003;37(3):523-7.
-
490Parisi R, Visonà A, Camporese G, Verlato F, Lessiani G, Antignani PL, et al. Isolated distal deep vein thrombosis: efficacy and safety of a protocol of treatment. Treatment of Isolated Calf Thrombosis (TICT) Study. Int Angiol. 2009;28(1):68-72.
-
491Palareti G. How I treat isolated distal deep vein thrombosis (IDDVT). Blood. 2014;123(12):1802-9.
-
492Galanaud JP, Sevestre MA, Genty C, Kahn SR, Pernod G, Rolland C, et al; OPTIMEV-SFMV investigators. Incidence and predictors of venous thromboembolism recurrence after a first isolated distal deep vein thrombosis. J Thromb Haemost. 2014;12(4):436-43.
-
493Mismetti P, Laporte S, Pellerin O, Ennezat PV, Couturaud F, Elias A, et al; PREPIC2 Study Group. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone on risk of recurrent pulmonary embolism: a randomized clinical trial. JAMA. 2015;313(16):1627-35.
-
494Kahn SR, Shapiro S, Wells PS, Rodger MA, Kovacs MJ, Anderson DR, et al; SOX trial investigators. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet. 2014;383(9920):880-8.
-
495Piran S, Le Gal G, Wells PS, Gandara E, Righini M, Rodger MA, et al. Outpatient treatment of symptomatic pulmonary embolism: a systematic review and meta-analysis. Thromb Res. 2013;132(5):515-9.
-
496Vinson DR, Zehtabchi S, Yealy DM. Can selected patients with newly diagnosed pulmonary embolism be safely treated without hospitalization? A systematic review. Ann Emerg Med. 2012;60(5):651-62.e4. Erratum in: Ann Emerg Med. 2015;65(2):177.
-
497Zondag W, Kooiman J, Klok FA, Dekkers OM, Huisman MV. Outpatient versus inpatient treatment in patients with pulmonary embolism: a meta-analysis. Eur Respir J. 2013;42(1):134-44.
-
498Kline JA, Nordenholz KE, Courtney DM, Kabrhel C, Jones AE, Rondina MT, et al. Treatment of submassive pulmonary embolism with tenecteplase or placebo: cardiopulmonary outcomes at 3 months: multicenter double-blind, placebo-controlled randomized trial. J Thromb Haemost. 2014;12(4):459-68.
-
499Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M; "MOPETT" Investigators. Moderate pulmonary embolism treated with thrombolysis (from the "MOPETT" Trial). Am J Cardiol. 2013;111(2):273-7.
-
500Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, et al; PEITHO Investigators. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402-11.
-
501IBGE. Diretoria de Pesquisas, Coordenação de Trabalho e Rendimento, Pesquisa Nacional de Saúde 2013. Disponível em ftp://ftp.ibge.gov.br/PNS/2013/pns2013.pdf
» ftp://ftp.ibge.gov.br/PNS/2013/pns2013.pdf -
502Rydén L, Grant PJ, Anker SD, Berne C, Cosentino F, Danchin N, et al. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD: the Task Force on diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and developed in collaboration with the European Association for the Study of Diabetes (EASD). Eur Heart J. 2013;34(39):3035-87. Erratum in: Eur Heart J. 2014;35(27):1824.
-
503Umpierrez GE, Smiley D, Jacobs S, Peng L, Temponi A, Mulligan P, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care. 2011;34(2):256-61.
-
504Buchleitner AM, Martínez-Alonso M, Hernández M, Solà I, Mauricio D. Perioperative glycaemic control for diabetic patients undergoing surgery. Cochrane Database Syst Rev. 2012 Sept 12;(9):CD007315.
-
505Noordzij PG, Boersma E, Schreiner F, Kertai MD, Feringa HH, Dunkelgrun M, et al. Increased preoperative glucose levels are associated with perioperative mortality in patients undergoing noncardiac, nonvascular surgery. Eur J Endocrinol. 2007;156(1):137-42.
-
506Bruno A, Gregori D, Caropreso A, Lazzarato F, Petrinco M, Pagano E. Normal glucose values are associated with a lower risk of mortality in hospitalized patients. Diabetes Care. 2008;31(11):2209-10.
-
507Griesdale DE, de Souza RJ, van Dam RM, Heyland DK, Cook DJ, Malhotra A, et al. Intensive insulin therapy and mortality among critically ill patients: a meta-analysis including NICE-SUGAR study data. CMAJ. 2009;180(8):821-7.
-
508Toyoshima MT, de Souza AB, Admoni SN, Cukier P, Lottenberg SA, Latronico AC, et al. New digital tool to facilitate subcutaneous insulin therapy orders: an inpatient insulin dose calculator. Diabetol Metab Syndr. 2015;7:114.
-
509van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345(19):1359-67.
-
510Finfer S, Chittock DR, Su SY, Blair D, Foster D, Dhingra V, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283-97.
-
511Marik PE, Preiser JC. Toward understanding tight glycemic control in the ICU: a systematic review and metaanalysis. Chest. 2010;137(3):544-51.
-
512Jacobi J, Bircher N, Krinsley J, Agus M, Braithwaite SS, Deutschman C, et al. Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit Care Med. 2012;40(12):3251-76.
-
513Mostbeck A, Galvan G, Bauer P, Eber O, Atefie K, Dam K, et al. The incidence of hyperthyroidism in Austria from 1987 to 1995 before and after an increase in salt iodization in 1990. Eur J Nucl Med. 1998;25(4):367-74.
-
514Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, et al. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. 2002;87(2):489-99.
-
515LeFevre ML; U.S. Preventive Services Task Force. Screening for thyroid dysfunction: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;162(9):641-50.
-
516Garber JR, Cobin RH, Gharib H, Hennessey JV, Klein I, Mechanick JI, et al; American Association Of Clinical Endocrinologists And American Thyroid Association Taskforce On Hypothyroidism In Adults. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Thyroid. 2012;22(12):1200-35. Erratum in: Thyroid. 2013;23(2):251. Thyroid. 2013;23(1):129.
-
517Graham GW, Unger BP, Coursin DB. Perioperative management of selected endocrine disorders. Int Anesthesiol Clin. 2000;38(4):31-67.
-
518Murkin JM. Anesthesia and hypothyroidism: a review of thyroxine physiology, pharmacology, and anesthetic implications. Anesth Analg. 1982;61(4):371-83.
-
519Bennett-Guerrero E, Kramer DC, Schwinn DA. Effect of chronic and acute thyroid hormone reduction on perioperative outcome. Anesth Analg. 1997;85(1):30-6.
-
520Pronovost PH, Parris KH. Perioperative management of thyroid disease. Prevention of complications related to hyperthyroidism and hypothyroidism. Postgrad Med. 1995;98(2):83-6, 96-8.
-
521Stehling LC. Anesthetic management of the patient with hyperthyroidism. Anesthesiology. 1974;41(6):585-95.
-
522Udelsman R, Norton JA, Jelenich SE, Goldstein DS, Linehan WM, Loriaux DL, et al. Responses of the hypothalamic-pituitary-adrenal and renin-angiotensin axes and the sympathetic system during controlled surgical and anesthetic stress. J Clin Endocrinol Metab. 1987;64(5):986-94.
-
523Oelkers W. Adrenal insufficiency. N Engl J Med. 1996;335(16):1206-12.
-
524Grinspoon Sk MMEVEDCRM. Adrenocortical insufficiency - clinical aspects. In: Vaughn Edj CRM, editor. Adrenal disorders. New York: Thieme Medical; 1989. p. 171-89.
-
525Axelrod L. Perioperative management of patients treated with glucocorticoids. Endocrinol Metab Clin North Am. 2003;32(2):367-83.
-
526Cooper MS, Stewart PM. Corticosteroid insufficiency in acutely ill patients. N Engl J Med. 2003;348(8):727-34.
-
527Salem M, Tainsh RE, Bromberg J, Loriaux DL, Chernow B. Perioperative glucocorticoid coverage. A reassessment 42 years after emergence of a problem. Ann Surg. 1994;219(4):416-25.
-
528Vigitel Brasil 2014: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção da Saúde. - Brasília : Ministério da Saúde, 2015.
-
529Chung F, Chau E, Yang Y, Liao P, Hall R, Mokhlesi B. Serum bicarbonate level improves specificity of STOP-Bang screening for obstructive sleep apnea. Chest. 2013;143(5):1284-93.
-
530Chung F, Subramanyam R, Liao P, Sasaki E, Shapiro C, Sun Y. High STOP-Bang score indicates a high probability of obstructive sleep apnoea. Br J Anaesth. 2012;108(5):768-75.
-
531Poirier P, Alpert MA, Fleisher LA, Thompson PD, Sugerman HJ, Burke LE, et al; American Heart Association Obesity Committee of Council on Nutrition, Physical Activity and Metabolism, Council on Cardiopulmonary Perioperative and Critical Care, Council on Cardiovascular Surgery and Anesthesia, Council on Cardiovas. Cardiovascular evaluation and management of severely obese patients undergoing surgery: a science advisory from the American Heart Association. Circulation. 2009;120(1):86-95.
-
532Chung F, Yegneswaran B, Liao P, Chung SA, Vairavanathan S, Islam S, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812-21.
-
533Schumann R, Jones SB, Ortiz VE, Connor K, Pulai I, Ozawa ET, et al. Best practice recommendations for anesthetic perioperative care and pain management in weight loss surgery. Obes Res. 2005;13(2):254-66.
-
534Mandal S, Hart N. Respiratory complications of obesity. Clin Med (Lond). 2012;12(1):75-8.
-
535McCullough PA, Gallagher MJ, Dejong AT, Sandberg KR, Trivax JE, Alexander D, et al. Cardiorespiratory fitness and short-term complications after bariatric surgery. Chest. 2006;130(2):517-25.
-
536Rocha AT, de Vasconcellos AG, da Luz Neto ER, Araújo DM, Alves ES, Lopes AA. Risk of venous thromboembolism and efficacy of thromboprophylaxis in hospitalized obese medical patients and in obese patients undergoing bariatric surgery. Obes Surg. 2006;16(12):1645-55.
-
537Stroh C, Birk D, Flade-Kuthe R, Frenken M, Herbig B, Höhne S, et al; Study Group Obesity Surgery. Evidence of thromboembolism prophylaxis in bariatric surgery-results of a quality assurance trial in bariatric surgery in Germany from 2005 to 2007 and review of the literature. Obes Surg. 2009;19(7):928-36.
-
538Nielsen KC, Guller U, Steele SM, Klein SM, Greengrass RA, Pietrobon R. Influence of obesity on surgical regional anesthesia in the ambulatory setting: an analysis of 9,038 blocks. Anesthesiology. 2005;102(1):181-7.
-
539Nightingale CE, Margarson MP, Shearer E, Redman JW, Lucas DN, Cousins JM, et al; Association of Anaesthetists of Great Britain; Ireland Society for Obesity and Bariatric Anaesthesia. Peri-operative management of the obese surgical patient 2015: Association of Anaesthetists of Great Britain and Ireland Society for Obesity and Bariatric Anaesthesia. Anaesthesia. 2015;70(7):859-76.
-
540WHO. (1968) Nutritional anaemias. Report of a WHO scientific group. Geneva, World Health Organization, 1968. (WHO Technical Report Series, No.405). Available at http://whqlibdoc.who.int/trs/WHO_TRS_405.pdf1968.
» http://whqlibdoc.who.int/trs/WHO_TRS_405.pdf -
541WHO. (2011) Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva, World Health Organization, 2011 (WHO/NMH/NHD/MNM/11.1) Available from: http://www.who.int/vmnis/indicators/haemoglobin.pdf 2011.
» http://www.who.int/vmnis/indicators/haemoglobin.pdf -
542Pedersen AB, Mehnert F, Overgaard S, Johnsen SP. Allogeneic blood transfusion and prognosis following total hip replacement: a population-based follow up study. BMC Musculoskelet Disord. 2009;10:167.
-
543Glance LG, Dick AW, Mukamel DB, Fleming FJ, Zollo RA, Wissler R, et al. Association between intraoperative blood transfusion and mortality and morbidity in patients undergoing noncardiac surgery. Anesthesiology. 2011;114(2):283-92.
-
544Musallam KM, Tamim HM, Richards T, Spahn DR, Rosendaal FR, Habbal A, et al. Preoperative anaemia and postoperative outcomes in non-cardiac surgery: a retrospective cohort study. Lancet. 2011;378(9800):1396-407.
-
545Ferraris VA, Davenport DL, Saha SP, Austin PC, Zwischenberger JB. Surgical outcomes and transfusion of minimal amounts of blood in the operating room. Arch Surg. 2012;147(1):49-55.
-
546Kotzé A, Harris A, Baker C, Iqbal T, Lavies N, Richards T, et al. British Committee for Standards in Haematology Guidelines on the Identification and Management of Pre-Operative Anaemia. Br J Haematol. 2015;171(3):322-31.
-
547Patel MS, Carson JL. Anemia in the preoperative patient. Med Clin North Am. 2009;93(5):1095-104.
-
548Carson JL, Carless PA, Hebert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012 Apr 18;(4):CD002042.
-
549Holst LB, Petersen MW, Haase N, Perner A, Wetterslev J. Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of randomised trials with meta-analysis and trial sequential analysis. BMJ. 2015;350:h1354.
-
550Fominskiy E, Putzu A, Monaco F, Scandroglio AM, Karaskov A, Galas FR, et al. Liberal transfusion strategy improves survival in perioperative but not in critically ill patients. A meta-analysis of randomised trials. Br J Anaesth. 2015;115(4):511-9.
-
551Docherty AB, O'Donnell R, Brunskill S, Trivella M, Doree C, Holst L, et al. Effect of restrictive versus liberal transfusion strategies on outcomes in patients with cardiovascular disease in a non-cardiac surgery setting: systematic review and meta-analysis. BMJ. 2016;352:i1351.
-
552Carson JL, Terrin ML, Noveck H, Sanders DW, Chaitman BR, Rhoads GG, et al; FOCUS Investigators. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365(26):2453-62.
-
553Kim Y, Spolverato G, Lucas DJ, Ejaz A, Xu L, Wagner D, et al. Red cell transfusion triggers and postoperative outcomes after major surgery. J Gastrointest Surg. 2015;19(11):2062-73.
-
554Tisherman SA. Determining when patients need transfusions. JAMA Surg. 2015;150(10):956.
-
555American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Practice guidelines for perioperative blood transfusion and adjuvant therapies: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Anesthesiology. 2006;105(1):198-208.
-
556Vichinsky EP, Haberkern CM, Neumayr L, Earles AN, Black D, Koshy M, et al. A comparison of conservative and aggressive transfusion regimens in the perioperative management of sickle cell disease. The Preoperative Transfusion in Sickle Cell Disease Study Group. N Engl J Med. 1995;333(4):206-13.
-
557Haberkern CM, Neumayr LD, Orringer EP, Earles AN, Robertson SM, Black D, et al. Cholecystectomy in sickle cell anemia patients: perioperative outcome of 364 cases from the National Preoperative Transfusion Study. Preoperative Transfusion in Sickle Cell Disease Study Group. Blood. 1997;89(5):1533-42.
-
558Riddington C, Williamson L. Preoperative blood transfusions for sickle cell disease. Cochrane Database Syst Rev. 2001;(3):CD003149.
-
559Lottenberg R, Hassell KL. An evidence-based approach to the treatment of adults with sickle cell disease. Hematology Am Soc Hematol Educ Program. 2005:58-65.
-
560Yawn BP, Buchanan GR, Afenyi-Annan AN, Ballas SK, Hassell KL, James AH, et al. Management of sickle cell disease: summary of the 2014 evidence-based report by expert panel members. JAMA. 2014;312(10):1033-48. Erratum in: JAMA. 2014;312(18):1932. JAMA. 2015;313(7):729.
-
561Estcourt LJ, Fortin PM, Trivella M, Hopewell S. Preoperative blood transfusions for sickle cell disease. Cochrane Database Syst Rev. 2016 Apr 6;4:CD003149.
-
562Squires JE. Indications for platelet transfusion in patients with thrombocytopenia. Blood Transfus. 2015;13(2):221-6.
-
563Hunt BJ, Allard S, Keeling D, Norfolk D, Stanworth SJ, Pendry K; British Committee for Standards in Haematology. A practical guideline for the haematological management of major haemorrhage. Br J Haematol. 2015;170(6):788-803.
-
564American Society of Anesthesiologists Task Force on Perioperative Blood Management. Practice guidelines for perioperative blood management: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Management*. Anesthesiology. 2015;122(2):241-75.
-
565British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of platelets transfusions. Br J Haematol. 2003;122:10-23.
-
566Johansson PI, Stensballe J. Hemostatic resuscitation for massive bleeding: the paradigm of plasma and platelets--a review of the current literature. Transfusion. 2010;50(3):701-10.
-
567Stroncek DF, Rebulla P. Platelet transfusions. Lancet. 2007;370(9585):427-38.
-
568Liumbruno GM, Bennardello F, Lattanzio A, Piccoli P, Rossetti G; Italian Society of Transfusion Medicine and Immunohaematology (SIMTI) Working Party. Recommendations for the transfusion management of patients in the peri-operative period. I. The pre-operative period. Blood Transfus. 2011;9(1):19-40.
-
569Barbhaiya M, Erkan D. Primary thrombosis prophylaxis in antiphospholipid antibody-positive patients: where do we stand? Curr Rheumatol Rep. 2011;13(1):59-69.
-
570Erkan D, Aguiar CL, Andrade D, Cohen H, Cuadrado MJ, Danowski A, et al. 14th International Congress on Antiphospholipid Antibodies: task force report on antiphospholipid syndrome treatment trends. Autoimmun Rev. 2014;13(6):685-96.
-
571Martinelli I, De Stefano V, Mannucci PM. Inherited risk factors for venous thromboembolism. Nat Rev Cardiol. 2014;11(3):140-56.
-
572Srivastava A, Brewer AK, Mauser-Bunschoten EP, Key NS, Kitchen S, Llinas A, et al; Treatment Guidelines Working Group on Behalf of The World Federation Of Hemophilia. Guidelines for the management of hemophilia. Haemophilia. 2013;19(1):e1-47.
-
573Nichols WL, Hultin MB, James AH, Manco-Johnson MJ, Montgomery RR, Ortel TL, et al. von Willebrand disease (VWD): evidence-based diagnosis and management guidelines, the National Heart, Lung, and Blood Institute (NHLBI) Expert Panel report (USA). Haemophilia. 2008;14(2):171-232.
-
574Laffan MA, Lester W, O'Donnell JS, Will A, Tait RC, Goodeve A, et al. The diagnosis and management of von Willebrand disease: a United Kingdom Haemophilia Centre Doctors Organization guideline approved by the British Committee for Standards in Haematology. Br J Haematol. 2014;167(4):453-65.
-
575Dimick JB, Pronovost PJ, Cowan JA, Lipsett PA. Complications and costs after high-risk surgery: where should we focus quality improvement initiatives? J Am Coll Surg. 2003;196(5):671-8.
-
576LeMaire SA, Miller CC 3rd, Conklin LD, Schmittling ZC, Köksoy C, Coselli JS. A new predictive model for adverse outcomes after elective thoracoabdominal aortic aneurysm repair. Ann Thorac Surg. 2001;71(4):1233-8.
-
577O'Brien MM, Gonzales R, Shroyer AL, Grunwald GK, Daley J, Henderson WG, et al. Modest serum creatinine elevation affects adverse outcome after general surgery. Kidney Int. 2002;62(2):585-92.
-
578O'Hare AM, Feinglass J, Sidawy AN, Bacchetti P, Rodriguez RA, Daley J, et al. Impact of renal insufficiency on short-term morbidity and mortality after lower extremity revascularization: data from the Department of Veterans Affairs' National Surgical Quality Improvement Program. J Am Soc Nephrol. 2003;14(5):1287-95.
-
579Ea B. Epidemiologia. Insuficiência renal aguda: fisiopatologia, clínica e tratamento. Schor N SOBM, editor. São Paulo: Sarvier; 1997.
-
580Chertow GM, Lazarus JM, Christiansen CL, Cook EF, Hammermeister KE, Grover F, et al. Preoperative renal risk stratification. Circulation. 1997;95(4):878-84.
-
581Lima EQ, Dirce MT, Castro I, Yu L. Mortality risk factors and validation of severity scoring systems in critically ill patients with acute renal failure. Ren Fail. 2005;27(5):547-56.
-
582Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, et al; Acute Kidney Injury Network. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31.
-
583Barrantes F, Tian J, Vazquez R, Amoateng-Adjepong Y, Manthous CA. Acute kidney injury criteria predict outcomes of critically ill patients. Crit Care Med. 2008;36(5):1397-403.
-
584Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365-70.
-
585Lassnigg A, Schmidlin D, Mouhieddine M, Bachmann LM, Druml W, Bauer P, et al. Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol. 2004;15(6):1597-605.
-
586Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney inter, Suppl. 2012;2:1-138.
-
587Kheterpal S, Tremper KK, Heung M, Rosenberg AL, Englesbe M, Shanks AM, et al. Development and validation of an acute kidney injury risk index for patients undergoing general surgery: results from a national data set. Anesthesiology. 2009;110(3):505-15.
-
588Sun LY, Wijeysundera DN, Tait GA, Beattie WS. Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. Anesthesiology. 2015;123(3):515-23.
-
589Lassnigg A, Donner E, Grubhofer G, Presterl E, Druml W, Hiesmayr M. Lack of renoprotective effects of dopamine and furosemide during cardiac surgery. J Am Soc Nephrol. 2000;11(1):97-104.
-
590Solomon R, Werner C, Mann D, D'Elia J, Silva P. Effects of saline, mannitol, and furosemide to prevent acute decreases in renal function induced by radiocontrast agents. N Engl J Med. 1994;331(21):1416-20.
-
591Harris RC Jr. Cyclooxygenase-2 inhibition and renal physiology. Am J Cardiol. 2002;89(6A):10D-7D.
-
592Ott E, Nussmeier NA, Duke PC, Feneck RO, Alston RP, Snabes MC, et al; Multicenter Study of Perioperative Ischemia (McSPI) Research Group; Ischemia Research and Education Foundation (IREF) Investigators. Efficacy and safety of the cyclooxygenase 2 inhibitors parecoxib and valdecoxib in patients undergoing coronary artery bypass surgery. J Thorac Cardiovasc Surg. 2003;125(6):1481-92.
-
593Bell S, Dekker FW, Vadiveloo T, Marwick C, Deshmukh H, Donnan PT, et al. Risk of postoperative acute kidney injury in patients undergoing orthopaedic surgery--development and validation of a risk score and effect of acute kidney injury on survival: observational cohort study. BMJ. 2015;351:h5639.
-
594Ventetuolo CE, Klinger JR. Management of acute right ventricular failure in the intensive care unit. Ann Am Thorac Soc. 2014;11(5):811-22.
-
595Hoeper MM, Bogaard HJ, Condliffe R, Frantz R, Khanna D, Kurzyna M, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D42-50.
-
596Costa EL, Jardim C, Bogossian HB, Amato MB, Carvalho CR, Souza R. Acute vasodilator test in pulmonary arterial hypertension: evaluation of two response criteria. Vascul Pharmacol. 2005;43(3):143-7.
-
597Gavilanes F, Alves Jr JL, Fernandes C, Prada LF, Jardim CV, Morinaga LT, et al. Left ventricular dysfunction in patients with suspected pulmonary arterial hypertension. J Bras Pneumol. 2014;40(6):609-16.
-
598Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D34-41. Erratum in: J Am Coll Cardiol. 2014;63(7):746.
-
599Hoeper MM, Granton J. Intensive care unit management of patients with severe pulmonary hypertension and right heart failure. Am J Respir Crit Care Med. 2011;184(10):1114-24.
-
600Green EM, Givertz MM. Management of acute right ventricular failure in the intensive care unit. Curr Heart Fail Rep. 2012;9(3):228-35.
-
601Tongers J, Schwerdtfeger B, Klein G, Kempf T, Schaefer A, Knapp JM, et al. Incidence and clinical relevance of supraventricular tachyarrhythmias in pulmonary hypertension. Am Heart J. 2007;153(1):127-32.
-
602Minai OA, Yared JP, Kaw R, Subramaniam K, Hill NS. Perioperative risk and management in patients with pulmonary hypertension. Chest. 2013;144(1):329-40.
-
603Kosarek L, Fox C, Baluch AR, Kaye AD. Pulmonary hypertension and current anesthetic implications. Middle East J Anaesthesiol. 2009;20(3):337-46.
-
604Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J. 2015;46(4):903-75. Erratum in: Eur Respir J. 2015;46(6):1855-6
-
605Blaise G, Langleben D, Hubert B. Pulmonary arterial hypertension: pathophysiology and anesthetic approach. Anesthesiology. 2003;99(6):1415-32.
-
606Meyer S, McLaughlin VV, Seyfarth HJ, Bull TM, Vizza CD, Gomberg-Maitland M, et al. Outcomes of noncardiac, nonobstetric surgery in patients with PAH: an international prospective survey. Eur Respir J. 2013;41(6):1302-7.
-
607Wightman JA. A prospective survey of the incidence of postoperative pulmonary complications. Br J Surg. 1968;55(2):85-91.
-
608Mohr DN, Jett JR. Preoperative evaluation of pulmonary risk factors. J Gen Intern Med. 1988;3(3):277-87.
-
609Hall JC, Tarala RA, Hall JL, Mander J. A multivariate analysis of the risk of pulmonary complications after laparotomy. Chest. 1991;99(4):923-7.
-
610Gracey DR, Divertie MB, Didier EP. Preoperative pulmonary preparation of patients with chronic obstructive pulmonary disease: a prospective study. Chest. 1979;76(2):123-9.
-
611Kroenke K, Lawrence VA, Theroux JF, Tuley MR, Hilsenbeck S. Postoperative complications after thoracic and major abdominal surgery in patients with and without obstructive lung disease. Chest. 1993;104(5):1445-51.
-
612Price LC, Montani D, Jaïs X, Dick JR, Simonneau G, Sitbon O, et al. Noncardiothoracic nonobstetric surgery in mild-to-moderate pulmonary hypertension. Eur Respir J. 2010;35(6):1294-302.
-
613Tait AR, Malviya S. Anesthesia for the child with an upper respiratory tract infection: still a dilemma? Anesth Analg. 2005;100(1):59-65.
-
614Brooks-Brunn JA. Predictors of postoperative pulmonary complications following abdominal surgery. Chest. 1997;111(3):564-71.
-
615Rodgers A, Walker N, Schug S, McKee A, Kehlet H, van Zundert A, et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ. 2000;321(7275):1493.
-
616Berg H, Roed J, Viby-Mogensen J, Mortensen CR, Engbaek J, Skovgaard LT, et al. Residual neuromuscular block is a risk factor for postoperative pulmonary complications. A prospective, randomised, and blinded study of postoperative pulmonary complications after atracurium, vecuronium and pancuronium. Acta Anaesthesiol Scand. 1997;41(9):1095-103.
-
617Canet J, Gallart L, Gomar C, Paluzie G, Vallès J, Castillo J, et al; ARISCAT Group. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338-50.
-
618Arozullah AM, Khuri SF, Henderson WG, Daley J; Participants in the National Veterans Affairs Surgical Quality Improvement Program. Development and validation of a multifactorial risk index for predicting postoperative pneumonia after major noncardiac surgery. Ann Intern Med. 2001;135(10):847-57.
-
619Gupta H, Gupta PK, Fang X, Miller WJ, Cemaj S, Forse RA, et al. Development and validation of a risk calculator predicting postoperative respiratory failure. Chest. 2011;140(5):1207-15.
-
620Lawrence VA, Cornell JE, Smetana GW; American College of Physicians. Strategies to reduce postoperative pulmonary complications after noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med. 2006;144(8):596-608.
-
621Moores LK. Smoking and postoperative pulmonary complications. An evidence-based review of the recent literature. Clin Chest Med. 2000;21(1):139-46, ix-x.
-
622Møller AM, Maaløe R, Pedersen T. Postoperative intensive care admittance: the role of tobacco smoking. Acta Anaesthesiol Scand. 2001;45(3):345-8.
-
623Delgado-Rodriguez M, Medina-Cuadros M, Martínez-Gallego G, Gómez-Ortega A, Mariscal-Ortiz M, Palma-Pérez S, et al. A prospective study of tobacco smoking as a predictor of complications in general surgery. Infect Control Hosp Epidemiol. 2003;24(1):37-43.
-
624Bettin CC, Gower K, McCormick K, Wan JY, Ishikawa SN, Richardson DR, et al. Cigarette smoking increases complication rate in forefoot surgery. Foot Ankle Int. 2015;36(5):488-93.
-
625McCunniff PT, Young ES, Ahmadinia K, Ahn UM, Ahn NU. Smoking is associated with increased blood loss and transfusion use after lumbar spinal surgery. Clin Orthop Relat Res. 2016;474(4):1019-25.
-
626Lau D, Berger MS, Khullar D, Maa J. The impact of smoking on neurosurgical outcomes. J Neurosurg. 2013;119(5):1323-30.
-
627Rejali M, Rejali AR, Zhang L. Effects of nicotine on the cardiovascular system. Vasc Dis Prev. 2005;2:135-44.
-
628Ngaage DL, Martins E, Orkell E, Griffin S, Cale AR, Cowen ME, et al. The impact of the duration of mechanical ventilation on the respiratory outcome in smokers undergoing cardiac surgery. Cardiovasc Surg. 2002;10(4):345-50.
-
629Teiriä H, Rautoma P, Yli-Hankala A. Effect of smoking on dose requirements for vecuronium. Br J Anaesth. 1996;76(1):154-5.
-
630Sherwin MA, Gastwirth CM. Detrimental effects of cigarette smoking on lower extremity wound healing. J Foot Surg. 1990;29(1):84-7.
-
631Theadom A, Cropley M. Effects of preoperative smoking cessation on the incidence and risk of intraoperative and postoperative complications in adult smokers: a systematic review. Tob Control. 2006;15(5):352-8.
-
632Nakagawa M, Tanaka H, Tsukuma H, Kishi Y. Relationship between the duration of the preoperative smoke-free period and the incidence of postoperative pulmonary complications after pulmonary surgery. Chest. 2001;120(3):705-10.
-
633Rigotti NA, Clair C, Munafò MR, Stead LF. Interventions for smoking cessation in hospitalised patients. Cochrane Database Syst Rev. 2012 May 16;(5):CD001837.
-
634Simon JA, Carmody TP, Hudes ES, Snyder E, Murray J. Intensive smoking cessation counseling versus minimal counseling among hospitalized smokers treated with transdermal nicotine replacement: a randomized trial. Am J Med. 2003;114(7):555-62.
-
635Reid RD, Pipe AL, Quinlan B. Promoting smoking cessation during hospitalization for coronary artery disease. Can J Cardiol. 2006;22(9):775-80.
-
636Smith PM, Burgess E. Smoking cessation initiated during hospital stay for patients with coronary artery disease: a randomized controlled trial. CMAJ. 2009;180(13):1297-303.
-
637Mazza R, Lina M, Boffi R, Invernizzi G, De Marco C, Pierotti M. Taking care of smoker cancer patients: a review and some recommendations. Ann Oncol. 2010;21(7):1404-9.
-
638Eisenberg MJ, Grandi SM, Gervais A, O'Loughlin J, Paradis G, Rinfret S, et al; ZESCA Investigators. Bupropion for smoking cessation in patients hospitalized with acute myocardial infarction: a randomized, placebo-controlled trial. J Am Coll Cardiol. 2013;61(5):524-32.
-
639Smith BJ, Carson KV, Brinn MP, Labiszewski NA, Peters MJ, Fitridge R, et al. Smoking Termination Opportunity for inPatients (STOP): superiority of a course of varenicline tartrate plus counselling over counselling alone for smoking cessation: a 12-month randomised controlled trial for inpatients. Thorax. 2013;68(5):485-6.
-
640Dale LC, Hurt RD, Offord KP, Lawson GM, Croghan IT, Schroeder DR. High-dose nicotine patch therapy. Percentage of replacement and smoking cessation. JAMA. 1995;274(17):1353-8.
-
641Hatsukami D, Mooney M, Murphy S, LeSage M, Babb D, Hecht S. Effects of high dose transdermal nicotine replacement in cigarette smokers. Pharmacol Biochem Behav. 2007;86(1):132-9.
-
642Zevin S, Jacob P 3rd, Benowitz NL. Dose-related cardiovascular and endocrine effects of transdermal nicotine. Clin Pharmacol Ther. 1998;64(1):87-95.
-
643Benowitz NL, Zevin S, Jacob P 3rd. Suppression of nicotine intake during ad libitum cigarette smoking by high-dose transdermal nicotine. J Pharmacol Exp Ther. 1998;287(3):958-62.
Publication Dates
-
Publication in this collection
Jan-Feb 2017