Abstract
Background:
Plasma levels of brain natriuretic peptides have better diagnostic accuracy compared to clinical-radiologic judgment for acute heart failure. In acute coronary syndromes (ACS), the prognostic value of acute heart failure is incorporated into predictive models through Killip classification. It is not established whether NT-proBNP could increment prognostic prediction.
Objective:
To evaluate whether NT-proBNP, as a measure of left ventricular dysfunction, improves the in-hospital prognostic value of the GRACE score in ACS.
Methods:
Patients admitted due to acute chest pain, with electrocardiogram and/or troponin criteria for ACS were included in the study. The plasma level of NT-proBNP was measured at hospital admission and the primary endpoint was defined as cardiovascular death during hospitalization. P-value < 0.05 was considered as significant.
Results:
Among 352 patients studied, cardiovascular mortality was 4.8%. The predictive value of NT-proBNP for cardiovascular death was shown by a C-statistic of 0.78 (95% CI = 0.65-0.90). After adjustment for the GRACE model subtracted by Killip variable, NT-proBNP remained independently associated with cardiovascular death (p = 0.015). However, discrimination by the GRACE-BNP logistic model (C-statistics = 0.83; 95%CI = 0.69-0.97) was not superior to the traditional GRACE Score with Killip (C-statistic = 0.82; 95%CI = 0.68-0.97). The GRACE-BNP model did not provide improvement in the classification of patients to high risk by the GRACE Score (net reclassification index = - 0.15; p = 0.14).
Conclusion:
Despite the statistical association with cardiovascular death, there was no evidence that NT-proBNP increments the prognostic value of GRACE score in ACS.
Keywords:
Acute Coronary Syndrome; Heart Failure; Natriuretic Peptide, Brain; Mortality; Ventricular Dysfunction, Left; Biomarkers
Resumo
Fundamento:
Os níveis plasmáticos de peptídeos natriuréticos cerebrais têm melhor precisão diagnóstica em comparação com a avaliação clínico-radiológica para insuficiência cardíaca aguda. Nas síndromes coronárias agudas (SCA), o valor prognóstico da insuficiência cardíaca aguda é incorporado nos modelos preditivos através da classificação de Killip. Não está estabelecido se o NT-proBNP poderia aumentar a previsão prognóstica.
Objetivo:
Avaliar se o NT-proBNP, como medida da disfunção ventricular esquerda, melhora o valor prognóstico intra-hospitalar do escore GRACE na SCA.
Métodos:
Foram incluídos no estudo pacientes admitidos por dor torácica aguda, com eletrocardiograma e/ou critérios de troponina para SCA. O nível plasmático de NT-proBNP foi medido no momento da admissão hospitalar e o desfecho primário foi definido como morte cardiovascular durante a hospitalização. Foi considerado significativo o valor de p < 0,05.
Resultados:
A mortalidade cardiovascular entre os 352 pacientes estudados foi de 4,8%. O valor preditivo do NT-proBNP para morte cardiovascular foi mostrado por uma estatística C de 0,78 (IC 95% = 0,65-0,90). Após o ajuste para o modelo GRACE subtraído pela variável Killip, o NT-proBNP permaneceu independentemente associado à morte cardiovascular (p = 0,015). No entanto, a discriminação pelo modelo logístico GRACE-BNP (estatística C = 0,83; IC 95% = 0,69-0,97) não foi superior ao escore GRACE tradicional com Killip (estatística C = 0,82; IC 95% = 0,68-0,97). O modelo GRACE-BNP não proporcionou melhora na classificação dos pacientes de alto risco pelo Escore GRACE (índice líquido de reclassificação = - 0,15; p = 0,14).
Conclusão:
Apesar da associação estatística com a morte cardiovascular, não houve evidências de que o NT-proBNP aumente o valor prognóstico do escore GRACE na SCA.
Palavras-chave:
Síndrome Coronariana Aguda; Insuficiência Cardíaca; Peptídeo Natriurético Encefálico; Mortalidade; Disfunção Ventricular Esquerda; Biomarcadores
Introduction
Brain natriuretic peptide is a prohormone, biologically measured by its active fragment or its inactive terminal portion (NT-proBNP). These molecules are biomarkers of left ventricular dysfunction, released to the bloodstream by myocytes undergoing wall tension due to volumetric or pressure overload.11 Hall C. Nt-probnp: the mechanism behind the marker. J Card Fail. 2005;11(5 suppl):S81-3. In the detection of heart failure, these peptides present better accuracy than clinical-radiological evaluation, being able to identify sub-clinical levels of decompensation.22 Januzzi JL Jr, Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG, et al. The n-terminal pro-bnp investigation of dyspnea in the emergency department (pride) study. Am J Cardiol. 2005;95(8):948-54.
The presence of left ventricular dysfunction is an important determinant of prognosis in patients with acute coronary syndromes (ACS). In this context, multivariate predictive models33 Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, Cannon CP, et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003;163(19):2345-53.,44 Morrow DA, Antman EM, Charlesworth A, Cairns R, Murphy SA, de Lemos JA, et al. TIMI risk score for st-elevation myocardial infarction: a convenient, bedside, clinical score for risk assessment at presentation: an intravenous npa for treatment of infarcting myocardium early ii trial substudy. Circulation. 2000;102(17):2031-7. take into account the presence of clinically manifested left ventricular dysfunction, well represented by the classification of Killip and Kimball.55 Killip T 3rd, Kimball JT. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol. 1967;20(4):457-4. Two reasons support the hypothesis that the use of plasma biomarkers may increase the prognostic value of these models: the capacity to numerically quantify the degree of cardiac decompensation and the higher sensitivity for subclinical changes, without impairing specificity.22 Januzzi JL Jr, Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG, et al. The n-terminal pro-bnp investigation of dyspnea in the emergency department (pride) study. Am J Cardiol. 2005;95(8):948-54.
In the context of ACS, the concentration of NT-proBNP has a well-documented prognostic accuracy.66 Zeng X, Li L, Su Q. The prognostic value of n-terminal pro-brain natriuretic peptide in non-st elevation acute coronary syndromes: a meta-analysis. Clin Chem Lab Med. 2012;50(4):731-9. However, from a predictive point of view, whether NT-proBNP has an incremental value in relation to probabilistic models that already contain Killip as a predictor variable is a controversial matter.77 Meune C, Drexler B, Haaf P, Reichlin T, Reiter M, Meissner J, et al. The grace score's performance in predicting in-hospital and 1-year outcome in the era of high-sensitivity cardiac troponin assays and b-type natriuretic peptide. Heart. 2011;97(18):1479-83.
8 Timoteo AT, Toste A, Ramos R, Miranda F, Ferreira ML, Oliveira JA, et al. Does admission nt-probnp increase the prognostic accuracy of grace risk score in the prediction of short-term mortality after acute coronary syndromes? Acute Card Care. 2009;11(4):236-42.-99 Guidez T, Marechaux S, Pincon C, Lamour H, Barrailler S, Decourcelle V, et al. Addition of b-type natriuretic peptide to the grace score to predict outcome in acute coronary syndrome: A retrospective (development) and prospective (validation) cohort-based study. Emerg Med J. 2012;29(4):274-9. Among the models validated for risk prediction, GRACE score is the one with the best prognostic accuracy, containing Killip class as the marker of heart failure.1010 Goncalves PA, Ferreira J, Aguiar C, Seabra-Gomes R. TIMI, PURSUIT, and GRACE risk scores: sustained prognostic value and interaction with revascularization in NSTE-ACS. Eur Heart J. 2005;26(9):865-72.
11 Yan AT, Yan RT, Tan M, Casanova A, Labinaz M, Sridhar K, et al. Risk scores for risk stratification in acute coronary syndromes: useful but simpler is not necessarily better. Eur Heart J. 2007;28(9):1072-8.-1212 Correia LC, Freitas R, Bittencourt AP, Souza AC, Almeida MC, Leal J, et al. Prognostic value of grace scores versus timi score in acute coronary syndromes. Arq Bras Cardiol. 2010;94(5):613-9. In this cohort, we tested the hypothesis that NT-proBNP incorporation increases the prognostic value of the GRACE score in patients with ACS. NT-proBNP wasmeasured at admission and the primary outcome was defined as cardiovascular death during hospitalization.
Methods
Sample selection
Patients consecutively admitted to the coronary care unit (CCU) of a tertiary-care hospital, between September 2007 and October 2013, due to suspected ACS (unstable angina and myocardial infarction) were prospectively included in the study. Inclusion criteria was chest discomfort in addition to at least one of the three objective criteria:
-
positive biological marker of myocardial necrosis, defined as troponin T ≥ 0.01 ug/L or troponin I > 0.034 g/L, corresponding to values above the 99th percentile;1313 Apple FS, Quist HE, Doyle PJ, Otto AP, Murakami MM. Plasma 99th percentile reference limits for cardiac troponin and creatine kinase mb mass for use with European Society of Cardiology/American College Of Cardiology consensus recommendations. Clin Chem. 2003;49(8):1331-6.
-
ischemic electrocardiographic alteration, consisting of T wave inversion (≥ 0.1 mV) or ST segment changes (≥ 0.05 mV); and
-
previously documented coronary artery disease, defined as a history of myocardial infarction with Q wave or previous angiography demonstrating coronary obstruction ≥ 70%.
Patients without NT-proBNP dosage or who did not agree to participate in the study were excluded. The protocol was in compliance with the Declaration of Helsinki, was approved by the Research Ethics Committee of the Institution, and all participants provided written informed consent.
NT-proBNP Measurement
NT-proBNP measurement was performed on a blood sample collected at patient’s arrival at the hospital, aiming for a minimum delay between the onset of symptoms and the collection of material. Plasma was frozen at -70 ºC for simultaneous dosing of the samples. The immunoassay method (Biomérieux) was used, considering the following definitions of high NT-proBNP:
-
Values above 450 pg/ml in patients under 50 years of age;
-
Values above 900 pg/ml in patients over 50 years of age.22 Januzzi JL Jr, Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG, et al. The n-terminal pro-bnp investigation of dyspnea in the emergency department (pride) study. Am J Cardiol. 2005;95(8):948-54.
GRACE score
The GRACE score calculation was based on clinical data at admission, electrocardiogram performed within 6 hours of admission, troponin T or troponin I dosages in the first 12 hours, and the first plasmatic creatinine. Elevation of myocardial necrosis markers (as a component of the scores) was defined as troponin above the 99th percentile. The GRACE score includes eight variables: five semi-quantitative, meaning different weight for each age stratum (systolic blood pressure, heart rate, plasma creatinine and Killip class), and three dichotomic ones (ST segment depression, elevation of myocardial necrosis marker, and cardiac arrest at admission). The final score can range from 0 to 372.33 Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, Cannon CP, et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003;163(19):2345-53.
Clinical end-point
The clinical end-point was cardiovascular death during hospitalization, defined by one of the following mechanisms: cardiac failure, arrhythmia or due to complications from treatments related to ACS.
Statistical Analyses
Numerical variables were expressed as mean and standard deviation as they presented normal distribution or small deviation from normality, while median and interquartile range were preferred in case of significant deviation from normality. Categorical variables were expressed in proportions. Preliminary results were accompanied by a 95% confidence interval as a measure of uncertainty. Initially, predictive values of NT-proBNP and Killip class were evaluated by the area under the ROC curve (C-statistic), considering cardiovascular death as an outcome. These two curves were statistically compared by the Hanley-McNeil paired test.1414 Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148(3):839-43. In addition, Kappa Test was used to assess concordance between high NT-proBNP and Killip > I in the definition of heart failure.
Logistic regression was used to assess the incremental value of NT-proBNP to the GRACE Score. The technique of modifying the GRACE Score was used, by replacing Killip for NT-proBNP, and then comparing this GRACE-BNP model to the traditional GRACE. The modification of GRACE was performed in two ways, one numerical and another categorical. In the first case, the regression coefficient of NT-proBNP represented the change in log odds promoted by each unit of NT-proBNP. In this case, the logistic regression equation determined the weight of NT-proBNP (numerical GRACE-BNP). In the second case, a high NT-proBNP added 20 points to the Killip free GRACE, which is the equivalent of Killip II value in the score (categorical GRACE-BNP).
The C-statistics of both models were compared with the traditional GRACE Score by the Hanley-McNeil test. Finally, net reclassification index analysis by Pencina1515 Xanthakis V, Sullivan LM, Vasan RS, Benjamin EJ, Massaro JM, D'Agostino RB, et al. Assessing the incremental predictive performance of novel biomarkers over standard predictors. Stat Med. 2014;33(15):2577-84. was used to evaluate the reclassification value of logistic and categorical GRACE-BNP in relation to the definition of high risk. For this reclassification, the best cutoff points for these new scores were used in the ROC curve.
Regarding sample size definition, two criteria were used. Firstly, aiming to reach a power of 80% to detect a difference of 0.05 between two ROC curves (referring to scores) and predicting a correlation of 0.80 between the scores, it would be necessary to enroll 192 patients. Secondly, in order to insert two variables in a logistic regression model, 10 to 20 events would be necessary.1616 Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373-9.
All of the tests above were considered statistically significant if p-value < 0.05. The SPSS Version 21 was the software used for the analysis.
Results
Sample characteristics
The sample consisted of 352 patients, mean age 63 ± 14 years, 60% male, 26% presenting with ST-segment elevation myocardial infarction. The GRACE score had a median of 104 (IIQ 82 - 131), which corresponds to intermediate risk. The median of NT-proBNP was 340 pg/ml (IIQ 86-1212), elevated in 29% of patients. The median time between symptom onset and NT-pro-BNP dosage was 15.5 hours (IIQ 8.2 - 32.5). The incidence of cardiovascular death in the hospital phase was 4.8%. Sample characteristics are described in Table 1.
NT-proBNP and Killip: Univariate Predictor Value
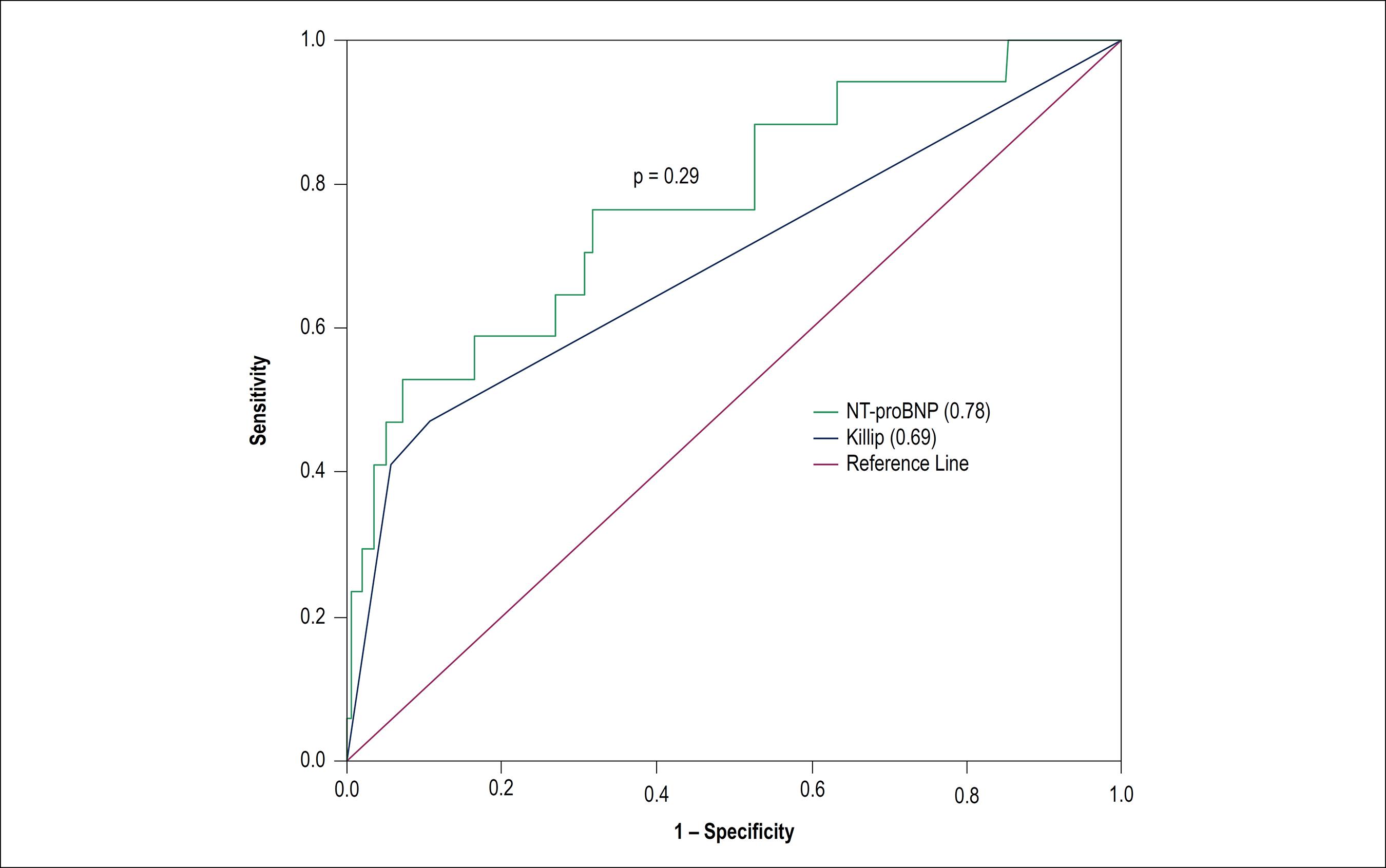
NT-proBNP demonstrated a moderate predictive capacity for cardiovascular death, according to C-statistic of 0.78 (95% CI = 0.65-0.90, p < 0.001), while the Killip score presented C-statistic of 0.69 (95% CI = 0.54-0.84, p = 0.008), with no statistical difference between the two curves (p = 0.29) (Figure 1). The two markers agreed in the definition of heart failure in 75% of the cases (8% with heart failure and 67% without hear failure), meaning low level of agreement according to the Kappa test (k = 0.26; 95% CI = 0.54-0.84; p < 0.001).
The accuracy of NT-pro-BNP in the prediction of death has a value of 0.78 (95% CI 0.65 – 0.9) in the C statistic and in the Killip classification 0.69 (95% CI 0.54 – 0.84).
Independent and Incremental NT-pro-BNP Value
In the logistic regression analysis, numerical NT-proBNP did not maintain statistical significance after adjustment for the traditional GRACE score (p = 0.11). On the other hand, numerical NT-proBNP remained an independent predictor when adjusted for GRACE score without Killip (p = 0.015; for each 500 pg/ml increase in NT-proBNP, a Beta of 0.029 was observed, OR = 1.03; 95% CI = 1.006 - 1.05) (Table 2). Categorical NT-proBNP was not an independent predictor after adjustment for the GRACE score (p = 0.91) or for the GRACE score without Killip (p = 0.36).
Logistic regression model containing GRACE without Killip and numerical NT-proBNP in predicting deaths
For analysis of the incremental value of NT-proBNP to GRACE, we compared the C-statistics of the logistic GRACE-BNP, categorical GRACE-BNP and traditional GRACE score. The results of the analysis were, respectively, 0.83 (95% CI = 0.69-0.97), 0.82 (95% CI = 0.68-0.96), and 0.82 (95% CI = 0.68-0.97). Therefore, no incremental value of the new approaches was identified (Figure 2).
Comparison of the ROC curves between original GRACE (0.82; 95% CI = 0.68-0.97) and GRACE-BNP logistic (0.83; 95% CI = 0.69-0.97) and categorical (0.82; 95% CI = 0.68-0.96) shows similar C-statistics among the three scores.
Reclassification of GRACE Score by NT-pro-BNP
Regarding the net reclassification analysis, of the 17 patients who died, 3 were correctly reclassified by logistic GRACE-BNP from low to high risk, with no incorrect reclassification, resulting in a positive net reclassification index (+ 0.18%). Among the 335 patients who survived, 9 were erroneously reclassified from low to high risk, while there was no correct reclassification. This resulted in a negative net reclassification ratio (-0.02%). In the final analysis, considering all patients, the total net reclassification index (NRI) was - 0.15% (p = 0.14) (Table 03). Reclassification based on categorical GRACE-BNP showed similar results (NRI = 0.08; p = 0.44). (Table 3)
Analysis of net reclassification by the GRACE-BNP numerical score in relation to the GRACE score in the definition of high risk
Discussion
The present study demonstrates the independent prognostic value of numeric NT-proBNP after adjustment to the GRACE score. However, the NT-proBNP did not improve discrimination of the GRACE Score, nor its reclassification ability. Its findings are in line with the notions that not every independent predictor offers incremental value to traditional models.1717 Yeboah J, McClelland RL, Polonsky TS, Burke GL, Sibley CT, O'Leary D, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment in intermediate-risk individuals. JAMA. 2012;308(8):788-95.
In an explanatory point of view, our findings reinforce that the status of cardiac decompensation increases the risk of patients with ACS. On the other hand, from the predictive point of view, refining the prognostic evaluation with a biomarker of heart failure that is more accurate than clinical evaluation was not enough to increase the accuracy of multivariate models. This discussion is intended to debate the potential explanations for the absence of an incremental value, to confront this paper’s results with external evidence, to recognize methodological limitations and to address the relevance of the present results.
Different hypotheses may explain the absence of NT-proBNP incremental value. Three possibilities will be pointed out, which comprises the generic properties of predictors and the specificities of the clinical context in question. First, probabilistic models are created with variables that simultaneously contribute to risk prediction, each with a predictive weight that is proportional to its independent strength of association. The improvement of a single predictor (detection of ventricular dysfunction) among many may not represent a relevant change. In the present case, the incorporation of a marker related to a new phenomenon was not proposed, but rather only the replacement of the evaluation of the phenomenon of heart failure with a theoretically better marker. Second, the predictive capacity of NT-proBNP theoretically lies in its continuous characteristic (numerical variable) and in its ability to identify subclinical ventricular dysfunction. It is possible that the prognostic value of heart failure is not at initial levels, limiting to more advanced and clinically manifested degrees. Finally, the prognostic accuracy of the traditional GRACE Score is already satisfactory, represented by C-statistic above 0.8, making more difficult to improve a marker that functions with good predictive capacity.
Some previous studies have tested the prognostic value of brain natriuretic peptides in ACS. Although there is a disagreement between studies, a careful analysis of the results shows that they all point in the same direction. Three studies conclude positively regarding the prognostic value of this type of marker; however, these studies evaluated the independent predictive value but did not test incremental value (discrimination or reclassification).1818 Almeida R, Mariano L, Gavina C, Pinho T, Vasconcelos M, Ferreira A, et al. The value of nt-probnp in early risk stratification of acute coronary syndromes. Rev Port Cardiol. 2006;25(1):71-5.
19 Bassan F, Bassan R, Esporcatte R, Santos B, Tura B. Very long-term prognostic role of admission bnp in non-st segment elevation acute coronary syndrome. Arq Bras Cardiol. 2016;106(3):218-25.
20 Galvani M, Ottani F, Oltrona L, Ardissino D, Gensini GF, Maggioni AP, et al. N-terminal pro-brain natriuretic peptide on admission has prognostic value across the whole spectrum of acute coronary syndromes. Circulation. 2004;110(2):128-34.
21 Ranjith N, Pegoraro RJ, Naidoo DP, Esterhuizen TM. Prognostic value of n-terminal-pro-brain natriuretic peptide measurements in patients with acute coronary syndromes. Cardiovasc J S Afr. 2006;17(2):60-6.-2222 Vieira C, Nabais S, Ramos V, Braga C, Gaspar A, Azevedo P, et al. Multimarker approach with cystatin c, n-terminal pro-brain natriuretic peptide, c-reactive protein and red blood cell distribution width in risk stratification of patients with acute coronary syndromes. Rev Port Cardiol. 2014;33(3):127-36. In this context, our results are not discordant. However, our negative conclusion resides in a more comprehensive analysis that was not previously done. In concordance, the two studies that evaluated the incremental value of multivariate models presented the same conclusion as ours.77 Meune C, Drexler B, Haaf P, Reichlin T, Reiter M, Meissner J, et al. The grace score's performance in predicting in-hospital and 1-year outcome in the era of high-sensitivity cardiac troponin assays and b-type natriuretic peptide. Heart. 2011;97(18):1479-83.,88 Timoteo AT, Toste A, Ramos R, Miranda F, Ferreira ML, Oliveira JA, et al. Does admission nt-probnp increase the prognostic accuracy of grace risk score in the prediction of short-term mortality after acute coronary syndromes? Acute Card Care. 2009;11(4):236-42.
Two aspects are original in the present work: it was the first study to aggregate the analysis of reclassification proposed by Pencina and the only one to adjust for the GRACE score after removal of Killip, avoiding eventual collinearity between Killip and NT-proBNP which could induce type II error. These approaches bring more veracity to our negative outcome.
Methodological limitations must be recognized here, which may have promoted a false negative result. Firstly, it is known that, ideally, a risk marker should be tested in an environment where the care team is not aware of its outcome. As this marker is already available in our clinical practice, the team became aware of the NT-proBNP result, predisposing to performance bias, which could improve the prognosis of patients with high NT-proBNP. Secondly, although this study had the planned sample size, it lacked additional power for exploratory analyses. For example, it was not possible to test the incremental value of the best NT-proBNP cutoff point. To do so, it would require a sample to identify the best cutoff point and another one to test for its incremental value. However, given our sample size, we chose not to split the sample.
The value of a negative result should be contextualized. Frequently, improper evaluation of markers modifies clinical reasoning with no probabilistic basis. That is, after estimating the risk based on the GRACE score, our evaluation would become less accurate if we mentally increased the risk after observing a high NT-proBNP value. It would be an improper reclassification. Therefore, it must be considered that the GRACE score has better accuracy than NT-proBNP, which should not modify the message of the first. On the other hand, the absence of prognostic value should not discredit the value of BNP in diagnosing symptoms of dyspnea during hospitalization or in monitoring the volemic status of patients who developed acute heart failure.
Conclusion
Despite its association with risk in a univariate approach, it has not been proven that the use of NT-proBNP as a measure of left ventricular dysfunction increases the in-hospital prognostic value of GRACE score in ACS.
-
Sources of FundingThere were no external funding sources for this study.
-
Study AssociationThis study is not associated with any thesis or dissertation work.
-
Ethics approval and consent to participateThis study was approved by the Ethics Committee of the Monte Tabor under the protocol number 36/11. All the procedures in this study were in accordance with the 1975 Helsinki Declaration, updated in 2013. Informed consent was obtained from all participants included in the study.
References
-
1Hall C. Nt-probnp: the mechanism behind the marker. J Card Fail. 2005;11(5 suppl):S81-3.
-
2Januzzi JL Jr, Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG, et al. The n-terminal pro-bnp investigation of dyspnea in the emergency department (pride) study. Am J Cardiol. 2005;95(8):948-54.
-
3Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, Cannon CP, et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003;163(19):2345-53.
-
4Morrow DA, Antman EM, Charlesworth A, Cairns R, Murphy SA, de Lemos JA, et al. TIMI risk score for st-elevation myocardial infarction: a convenient, bedside, clinical score for risk assessment at presentation: an intravenous npa for treatment of infarcting myocardium early ii trial substudy. Circulation. 2000;102(17):2031-7.
-
5Killip T 3rd, Kimball JT. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol. 1967;20(4):457-4.
-
6Zeng X, Li L, Su Q. The prognostic value of n-terminal pro-brain natriuretic peptide in non-st elevation acute coronary syndromes: a meta-analysis. Clin Chem Lab Med. 2012;50(4):731-9.
-
7Meune C, Drexler B, Haaf P, Reichlin T, Reiter M, Meissner J, et al. The grace score's performance in predicting in-hospital and 1-year outcome in the era of high-sensitivity cardiac troponin assays and b-type natriuretic peptide. Heart. 2011;97(18):1479-83.
-
8Timoteo AT, Toste A, Ramos R, Miranda F, Ferreira ML, Oliveira JA, et al. Does admission nt-probnp increase the prognostic accuracy of grace risk score in the prediction of short-term mortality after acute coronary syndromes? Acute Card Care. 2009;11(4):236-42.
-
9Guidez T, Marechaux S, Pincon C, Lamour H, Barrailler S, Decourcelle V, et al. Addition of b-type natriuretic peptide to the grace score to predict outcome in acute coronary syndrome: A retrospective (development) and prospective (validation) cohort-based study. Emerg Med J. 2012;29(4):274-9.
-
10Goncalves PA, Ferreira J, Aguiar C, Seabra-Gomes R. TIMI, PURSUIT, and GRACE risk scores: sustained prognostic value and interaction with revascularization in NSTE-ACS. Eur Heart J. 2005;26(9):865-72.
-
11Yan AT, Yan RT, Tan M, Casanova A, Labinaz M, Sridhar K, et al. Risk scores for risk stratification in acute coronary syndromes: useful but simpler is not necessarily better. Eur Heart J. 2007;28(9):1072-8.
-
12Correia LC, Freitas R, Bittencourt AP, Souza AC, Almeida MC, Leal J, et al. Prognostic value of grace scores versus timi score in acute coronary syndromes. Arq Bras Cardiol. 2010;94(5):613-9.
-
13Apple FS, Quist HE, Doyle PJ, Otto AP, Murakami MM. Plasma 99th percentile reference limits for cardiac troponin and creatine kinase mb mass for use with European Society of Cardiology/American College Of Cardiology consensus recommendations. Clin Chem. 2003;49(8):1331-6.
-
14Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148(3):839-43.
-
15Xanthakis V, Sullivan LM, Vasan RS, Benjamin EJ, Massaro JM, D'Agostino RB, et al. Assessing the incremental predictive performance of novel biomarkers over standard predictors. Stat Med. 2014;33(15):2577-84.
-
16Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373-9.
-
17Yeboah J, McClelland RL, Polonsky TS, Burke GL, Sibley CT, O'Leary D, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment in intermediate-risk individuals. JAMA. 2012;308(8):788-95.
-
18Almeida R, Mariano L, Gavina C, Pinho T, Vasconcelos M, Ferreira A, et al. The value of nt-probnp in early risk stratification of acute coronary syndromes. Rev Port Cardiol. 2006;25(1):71-5.
-
19Bassan F, Bassan R, Esporcatte R, Santos B, Tura B. Very long-term prognostic role of admission bnp in non-st segment elevation acute coronary syndrome. Arq Bras Cardiol. 2016;106(3):218-25.
-
20Galvani M, Ottani F, Oltrona L, Ardissino D, Gensini GF, Maggioni AP, et al. N-terminal pro-brain natriuretic peptide on admission has prognostic value across the whole spectrum of acute coronary syndromes. Circulation. 2004;110(2):128-34.
-
21Ranjith N, Pegoraro RJ, Naidoo DP, Esterhuizen TM. Prognostic value of n-terminal-pro-brain natriuretic peptide measurements in patients with acute coronary syndromes. Cardiovasc J S Afr. 2006;17(2):60-6.
-
22Vieira C, Nabais S, Ramos V, Braga C, Gaspar A, Azevedo P, et al. Multimarker approach with cystatin c, n-terminal pro-brain natriuretic peptide, c-reactive protein and red blood cell distribution width in risk stratification of patients with acute coronary syndromes. Rev Port Cardiol. 2014;33(3):127-36.
Publication Dates
-
Publication in this collection
14 Feb 2020 -
Date of issue
Apr 2020
History
-
Received
13 Nov 2018 -
Reviewed
20 May 2019 -
Accepted
05 June 2019