Abstracts
This study describes the profile of Hospitalisations for Ambulatory Care Sensitive Conditions (ACSCs) in Curitiba from 2005 to 2007. An ecological study was conducted using the data obtained from the Brazilian Hospital Information System (Sistema de Informações Hospitalares). Descriptive statistics was used for analysis. It was observed that there was a trend toward stabilisation in ACSCs in Curitiba, the most frequent causes being angina and heart failure, with an increased frequency in females and individuals aged ≥65 years. The results were similar to those observed in other studies, and almost in their entirety, were highly significant from a statistical point of view. However, the studies should be viewed with caution because it is an indicator presenting some limitations, including the reliability of diagnosis and the use of secondary data.
Hospitalization; Primary Health Care; Quality of Health Care; Evaluation
Este estudo tem como objetivo descrever o perfil das Internações por Condições Sensíveis à Atenção Primária (ICSAP) no município de Curitiba no período de 2005 a 2007. Foi realizado um estudo ecológico, com dados obtidos no Sistema de Informações Hospitalares. Para análise, foi utilizada a estatística descritiva. Observou-se que em Curitiba as ICSAP seguem tendência de estabilização, sendo as causas mais frequentes a angina e a insuficiência cardíaca, maior frequência para o sexo feminino e a faixa etária ≥ 65 anos. Os resultados observados assemelham-se aos de outros estudos e foram, quase na totalidade, altamente significativos do ponto de vista estatístico. Entretanto, devem ser vistos com cuidado, pois se se trata de um indicador que apresenta algumas limitações, dentre as quais a própria confiabilidade do diagnóstico e o uso de dados secundários.
Hospitalização; Atenção Primária à Saúde; Qualidade da Assistência à Saúde; Avaliação
Este estudio tuvo como objetivo describir el perfil de las hospitalizaciones por condiciones sensibles a la Atención Primaria (ICSAP) en el municipio de Curitiba, durante en el período de 2005 a 2007. Fue realizado un estudio ecológico, con datos extraídos del Sistema de Informaciones Hospitalarias. Para el análisis fue utilizado la estadística descriptiva. Se observó que en Curitiba las ICSAP siguen la tendencia de estabilización, siendo las causas más frecuentes la angina de pecho y la insuficiencia cardíaca, con mayor frecuencia para el sexo femenino y el grupo etáreo ≥65 años. Los resultados observados son similares a otros estudios y fueron, casi en su totalidad, altamente significativos desde el punto de vista estadístico. Sin embargo, deben ser analizados cuidadosamente pues se trata de un indicador con algunas limitaciones, entre las que podemos destacar la propia confiabilidad del diagnóstico y el uso de datos secundarios.
Hospitalización; Atención Primaria de Salud; Calidad de la Atención de Salud; Evaluación
INTRODUCTION
The process of implementing the Unified Health System [Sistema Único de Saúde – SUS)] over the last two decades has been marked by many advances. The construction of the system’s universality stands out among them, mainly due to the participation of municipalities, as a result of the decentralisation of responsibilities, powers, and financial resources. Noteworthy is the progress made in Basic Care (BC), of which implementation is the responsibility of municipal management.
With regard to the performance of this care level, the World Health Organisation (WHO), in its 2008 World Health Report, proposed radical changes in Primary Health Care (PHC), ensuring that it would be a response to peoples’ needs and expectations in relation to a broad range of risks and diseases, as well as coordinating a comprehensive response at all health care levels (
11 World Health Organization (WHO). The World Health Report 2008: primary health care (now more than ever) [Internet]. Geneva; 2008 [cited 2012 Feb 19]. Available from: http://www.who.int/whr/2008/en/
http://www.who.int/whr/2008/en/...
) .
Brazil has been discussing the configuration of health care networks in the SUS wherein BC would no longer be just a gateway but would occupy a central position as the coordinator of healthcare within the system. Therefore, it is necessary to not only expand the range of BC services offered but improve their quality as well.
The organisation of health care networks must ensure continuity of care and realise the principle of comprehensive care. Thus, cases that seek health care directly in the various health care levels will require BC, where their needs should be met.
As part of this pursuit, Brazil began to work on the concept of Hospitalisation for Ambulatory Care Sensitive Conditions (ACSCs). The indicator originated in the United States as Ambulatory Care Sensitive Conditions (ACSCs) ( 22 Bermúdez-Tamayo C, Márquez-Calderón S, Rodríguez del Aguila MM, Perea-Milla LE, Ortiz Espinosa J. Características organizativas de la atención primaria y hospitalización por los principals ambulatory care sensitive conditions. Aten Primária. 2004;33(6):305-11. ) and from there, adaptations were made in order to contemplate specific local features, depending on the context being analysed, as with the study carried out in the European context that used the American list ( 33 Caminal Homal J, Starfield B, Sánchez Ruiz E, Casanova Matutano C, Morales M. The role of primary care in preventing ambulatory care sensitive conditions. Eur J Public Health. 2004;14(3):246-51. ) .
Hospitalisations for ACSCs are a new hospital indicator developed in the last decade, which aim to serve as a measure of PHC effectiveness for the care of certain health problems (
44 Caminal Homar J, Casanova Matutano C. La evaluación de la atención primaria y las hospitalizaciones por ambulatory care sensitive conditions: marco conceptual. Aten Primaria. 2003;31(1):61-5.
) . Such have been used in some countries as an indirect indicator for evaluating the access to and quality of care (
55 Nedel FB, Facchini LA, Bastos JL, Martín-Mateo M. Conceptual and methodological aspects in the study of hospitalizations for ambulatory care sensitive conditions. Ciênc Saúde Coletiva. 2011;16 Suppl 1:1145-54.
6 Nedel FB, Facchini LA, Martín-Mateo M, Navarro A. Características da atenção básica associadas ao risco de internar por condições sensíveis à atenção primária: revisão sistemática de literatura. Epidemiol Serv Saúde. 2010;19(1):61-75.
7 Dias-da-Costa JS, Buttenbender, DC, Hoefel AL, Souza LL. Hospitalizações por condições sensíveis à atenção primária nos municípios em gestão plena do sistema no Estado do Rio Grande do Sul, Brasil. Cad Saúde Pública. 2010;26(2):358-64.
8 Rehem TCMSB, Egry EY. Internações por condições sensíveis à Atenção Primária no Estado de São Paulo. Ciênc Saúde Coletiva. 2011;16(12):4755-66.
-
99 Torres RL, Rehem TCMSB, Egry EY, Ciosak SI. The panorama of ambulatory care sensitive conditions in district of São Paulo. Rev Esc Enferm USP [Internet]. 2011 [cited 2012 Feb 12];45(n.spe2):1661-6. Available from: http://www.scielo.br/pdf/reeusp/v45nspe2/en_04.pdf
http://www.scielo.br/pdf/reeusp/v45nspe2...
) .
In Brazil, although this indicator was already being used by some health departments, including the Curitiba Municipal Department, the first ACSCs National List was drafted in 2007 and published in 2008.
The model proposed by Caminal Homar and Casanova Matutano was adopted as a contextual framework and used to compile the list, with adaptations to Brazilian conditions. It assumed that, for some health conditions, timely and quality PHC can avert hospitalisation or reduce its frequency ( 1010 Alfradique ME, Bonolo PF, Dourado I, Costa-Lima MF, Macinko J, Mendonça CS, et al. Internações por condições sensíveis à atenção primária: a construção da lista brasileira como ferramenta para medir o desempenho do sistema de saúde (Projeto ICSAP Brasil). Cad Saúde Pública. 2009;25(6):1337-49. ) .
The process of building the Brazilian list involved researchers and managers for the first phase of validation, consolidation, and review, as well as consulted with the Brazilian Society of Family and Community Medicine (Sociedade Brasileira de Medicina de Família e Comunidade – SBMFC) and the public ( 1010 Alfradique ME, Bonolo PF, Dourado I, Costa-Lima MF, Macinko J, Mendonça CS, et al. Internações por condições sensíveis à atenção primária: a construção da lista brasileira como ferramenta para medir o desempenho do sistema de saúde (Projeto ICSAP Brasil). Cad Saúde Pública. 2009;25(6):1337-49. ) . After necessary adjustments, the Ministry of Health’s (Ministério da Saúde – MS) Department of Health Care (Secretaria de Atenção à Saúde – SAS) published the final version of the Brazilian List of ACSCs as an annex to Directive SAS/MS No. 221, April 17, 2008 ( 1111 Brasil. Ministério da Saúde. Portaria n. 221, de 17 de abril de 2008. Publica em forma do anexo a lista brasileira de internações por condições sensíveis à Atenção Primária. Diário Oficial da União, Brasília, 21 set. 2008. Seção 1, p. 50. ) . This list considers, among other things, the impact of PHC on the reduction of ACSCs at this care level in several countries and the possibility of including hospital indicators to indirectly measure the operation of BC and the Family Health Strategy (Estratégia Saúde da Família – ESF),
Given the above, and considering that the MS Directive further stipulates that the Brazilian list will be used as a tool for evaluating PHC and/or the use of hospital care ( 1111 Brasil. Ministério da Saúde. Portaria n. 221, de 17 de abril de 2008. Publica em forma do anexo a lista brasileira de internações por condições sensíveis à Atenção Primária. Diário Oficial da União, Brasília, 21 set. 2008. Seção 1, p. 50. ) , it is appropriate to conduct studies using this indicator to verify the behaviour of the hospitalisations for ACSCs in Brazil. Therefore, this study aims to identify the profile of ACSCs in the city of Curitiba from 2005 to 2007.
METHOD
This exploratory ecological study takes as its unit of analysis the population of Curitiba hospitalised for ACSCs in the years 2005, 2006, and 2007. The study period corresponds to the period of time immediately prior to the implementation of the national list in 2008, which provides a baseline for potential analysis of the data before and after this milestone. Curitiba was selected because it is one of the pioneer cities in the construction and implementation of an ACSCs list.
The data collected were the hospitalisations of patients living in Curitiba and registered in the Unified Health System’s Hospital Information System (SIH-SUS) from 2005 to 2007. This system processes authorisations for hospitalisations, providing information related to the resources allocated for each hospital that is part of the SUS network and the leading causes of hospitalisations in Brazil. Its information is available via the internet through the products developed by DATASUS.
The selection of ACSCs was based on the Brazilian List published by the Ministry of Health ( 1010 Alfradique ME, Bonolo PF, Dourado I, Costa-Lima MF, Macinko J, Mendonça CS, et al. Internações por condições sensíveis à atenção primária: a construção da lista brasileira como ferramenta para medir o desempenho do sistema de saúde (Projeto ICSAP Brasil). Cad Saúde Pública. 2009;25(6):1337-49. ) , consisting of 19 cause groups, with 74 diagnoses classified according to the 10th Revision of the International Classification of Diseases (ICD-10). From the selection in the HIS-SUS of the codes referred to above, a definition file (DEF) was generated to tabulate sensitive conditions, using the application Tabwin – Version 3.5 developed by DATASUS/MS.
The analysis of ACSCs involved the calculation of four estimates:
-
Proportion of ACSCs: total admissions to the SUS for ACSCs, divided by total hospitalisations of resident patients in the same selected area and time period (2005 to 2007), multiplied by 100.
-
Proportion of hospitalisations of resident patients by primary care-sensitive cause groups: total ACSCs by selected cause group, divided by total ACSCs for resident patients in the same selected area and time period (2005 to 2007), multiplied by 100.
-
Proportion of ACSCs, according to gender: ACSCs numbers of male and female resident patients, divided by total ACSCs for resident patients in the same selected area and time period, multiplied by 100.
-
Proportion of ACSCs according to age: ACSCs numbers of resident patients in selected age groups: 1 year; 1 to 4; 5 to 14; 15 to 24; <25 to 34; 34 to 44; 45 to 54; 55 to 64; ≥ 65, divided by total ACSCs for resident patients in the same selected area and time period, multiplied by 100.
The Epi-Info 6.0 (v.DOS) was used to test the hypotheses for difference in proportions. The Chi-Square test at a significance level of 5% was also used to test the null hypothesis of equal proportions for each of the estimates among the three years studied.
As for the ethical aspects, the study was conducted using non-nominal health data from the public domain that is available on the website DATASUS. Thus, it did not involve any risk to the study population, and the information may benefit SUS users.
RESULTS
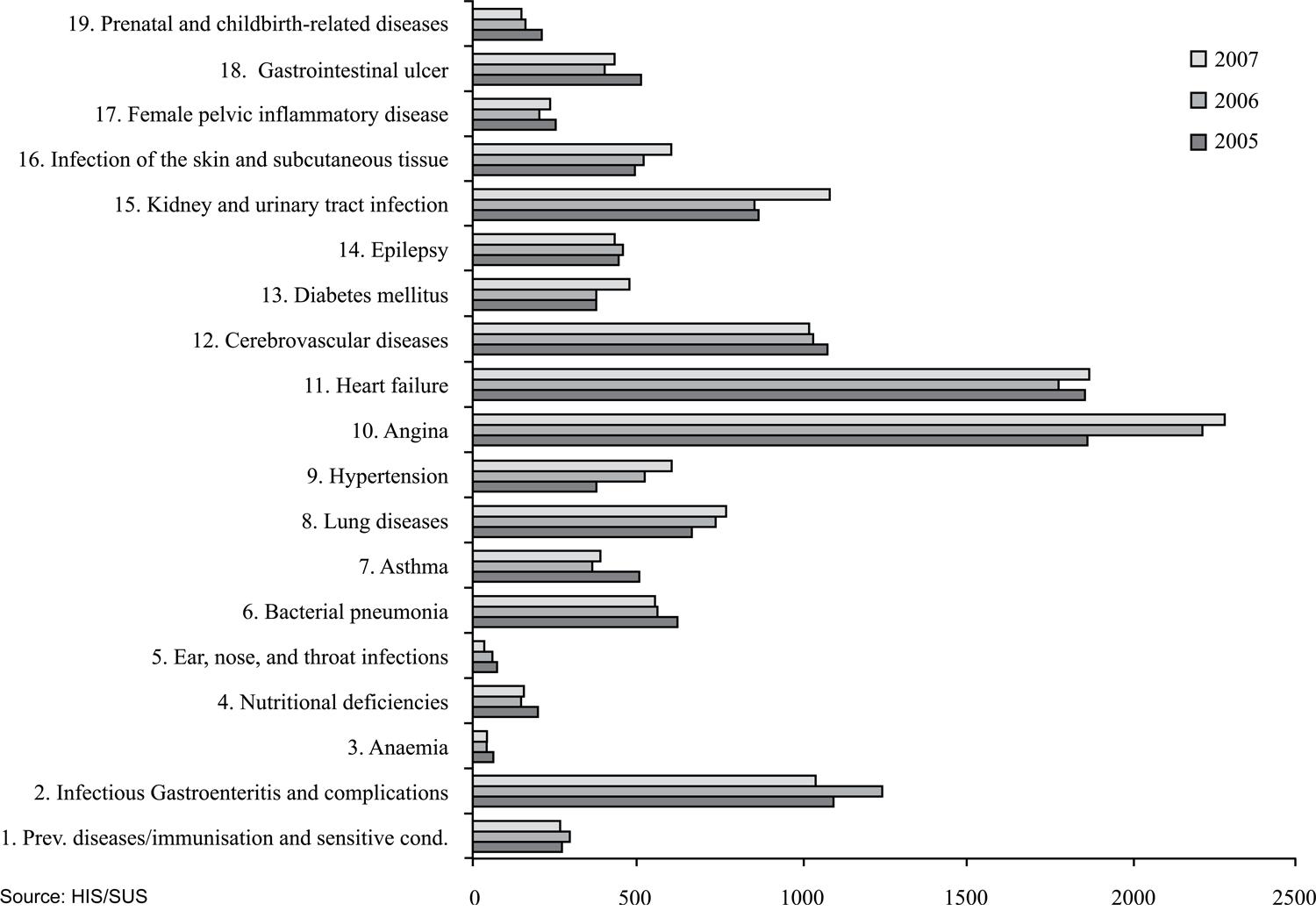
The proportion of ACSCs from the total number of hospitalisations that took place in the city of Curitiba from 2005 to 2007 remained stable: 11,785 (11.52%) in 2005, 11,956 (11.47%) in 2006, and 12,407 (11.54%) in 2007 (p=0.87). Among the cause groups, it is observed that hospitalisations for angina and heart failure were those that occurred most frequently during the three years studied ( Figure 1).
Hospitalisations for ambulatory care sensitive conditions 1according to cause group – Curitiba, PR, 2005 to 2007 1 Resident Patient
Infectious gastroenteritis and its complications were the third leading cause of hospitalisations for ACSCs in 2006, with a decrease in 2007, falling below the value recorded in 2005 (p=0.000001). Another noteworthy aspect relates to the reduction of ACSCs in prenatal and childbirth-related diseases (p=0.00015); ear, nose, and throat infections (p=0.0018); and anaemia (p=0.044). It is also worth noting that there was an increase in ACSCs for infections of the skin and subcutaneous tissue (p=0.022), kidney and urinary tract infection (p=0.000002), diabetes mellitus (p=0.005), hypertension (p=0.000000), and lung diseases (p=0.17) in 2007, compared with those in 2005 and 2006 ( Figure 1 ).
When analysing the data from ACSCs in 2007, it appears that the most frequent hospitalisation was angina, followed by heart failure, kidney and urinary tract infections, infectious gastroenteritis and its complications, and cerebrovascular diseases. Hospitalisations that occurred less frequently were ear, nose, and throat infections, anaemia, prenatal and childbirth-related diseases, nutritional deficiency, and asthma.
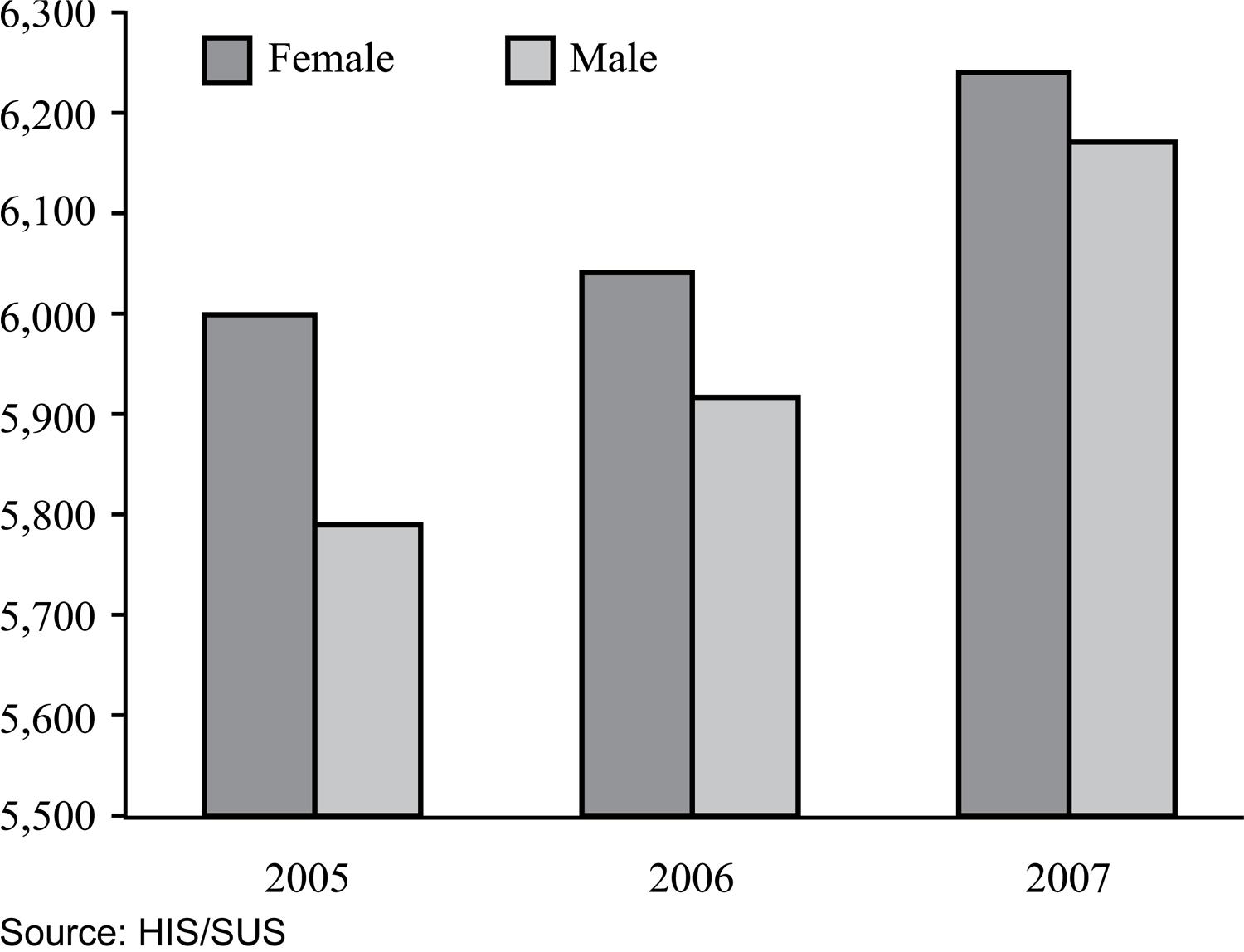
In the estimate according to gender, there was a higher number of female hospitalisations ( Figure 2 ), without any major fluctuations during the three years (p=0.64).
Admissions by ambulatory care sensitive conditions 1 according to gender − Curitiba, PR, 2005 to 2007
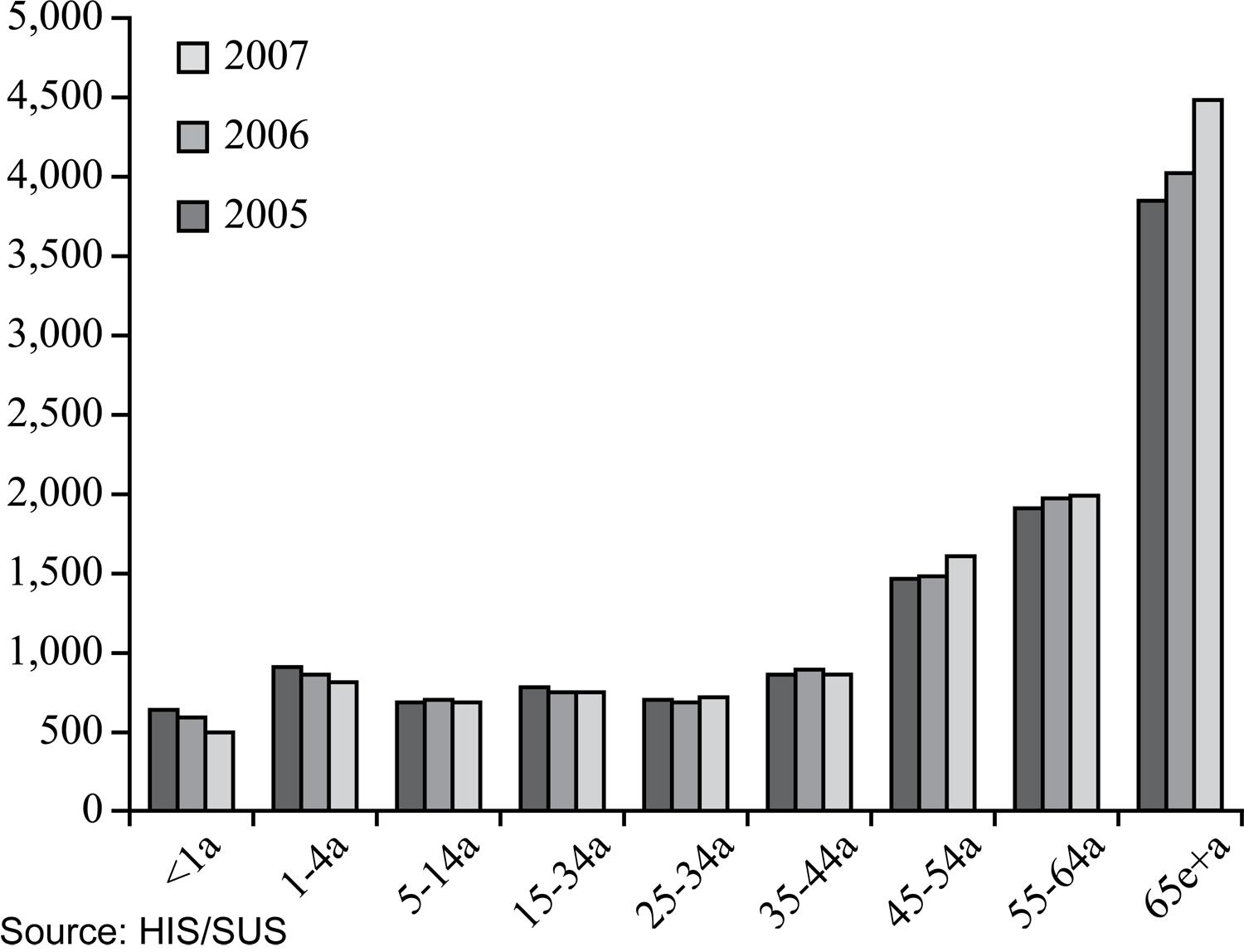
Figure 3 shows a rising curve following the increase in age. In the three years, there was a higher rate of hospitalisations for ACSCs in individuals over 45 years of age, with a rising frequency in the 65 years or older range (p<0.001) over the years. On the other hand, it appears that in the <1-year age group, these hospitalisations have gradually decreased during the study period (p=0.000003).
Hospitalisations for ambulatory care sensitive conditions 1according to age − Curitiba, PR, 2005 to 2007 1 Resident Patient
DISCUSSION
When analysing the results of our study, it can be seen that there was a stabilisation of hospitalisations from 2005 to 2007. This has been observed in other studies conducted in Brazil, where ACSCs have shown a pattern of stability or even reduction ( 1010 Alfradique ME, Bonolo PF, Dourado I, Costa-Lima MF, Macinko J, Mendonça CS, et al. Internações por condições sensíveis à atenção primária: a construção da lista brasileira como ferramenta para medir o desempenho do sistema de saúde (Projeto ICSAP Brasil). Cad Saúde Pública. 2009;25(6):1337-49. , 1212 Rehem TCMSB. Internações Sensíveis à Atenção Primária: limites e possibilidades da lista brasileira de diagnósticos [tese doutorado]. São Paulo: Escola de Enfermagem, Universidade de São Paulo; 2011. - 1313 Rehem TCMSB, Egry EY, Ciosak SI. Internações por condições sensíveis à Atenção Primária no Hospital Geral de uma Microrregião de Saúde do Município de São Paulo, Brasil. Texto Contexto Enferm. 2012;21(3):535-42. ) .
With respect to the main causes of ACSCs in Curitiba in 2007, there was a similarity to a study using the national data in 2006, in which gastroenteritis and its complications, heart failure, kidney and urinary tract infections, and cerebrovascular disease were also among the five leading causes of hospitalisations ( 1010 Alfradique ME, Bonolo PF, Dourado I, Costa-Lima MF, Macinko J, Mendonça CS, et al. Internações por condições sensíveis à atenção primária: a construção da lista brasileira como ferramenta para medir o desempenho do sistema de saúde (Projeto ICSAP Brasil). Cad Saúde Pública. 2009;25(6):1337-49. , 1212 Rehem TCMSB. Internações Sensíveis à Atenção Primária: limites e possibilidades da lista brasileira de diagnósticos [tese doutorado]. São Paulo: Escola de Enfermagem, Universidade de São Paulo; 2011. - 1313 Rehem TCMSB, Egry EY, Ciosak SI. Internações por condições sensíveis à Atenção Primária no Hospital Geral de uma Microrregião de Saúde do Município de São Paulo, Brasil. Texto Contexto Enferm. 2012;21(3):535-42. ) . In this study, it is worth noting that, of the total hospitalisations, births were excluded for they represent a natural outcome of pregnancy and would be influenced by the fertility rate.
In Curitiba, there was an increase in the number of hospitalisations in the group with diabetes mellitus in 2007, compared with those in 2005 and 2006. This fact deserves attention because it differs from that found in another study with Brazilian data, which revealed a reduction in hospitalisations for this cause group ( 1010 Alfradique ME, Bonolo PF, Dourado I, Costa-Lima MF, Macinko J, Mendonça CS, et al. Internações por condições sensíveis à atenção primária: a construção da lista brasileira como ferramenta para medir o desempenho do sistema de saúde (Projeto ICSAP Brasil). Cad Saúde Pública. 2009;25(6):1337-49. ) .
In the literature review, three studies were found to focus on diabetes alone as a PHC-sensitive condition (
1414 Robbins JM, Valdmanis VG, Webb DA. Do public health clinics reduce rehospitalizations?: the urban diabetes study. J Health Care Poor Underserved. 2008;19(2):562-73.
15 Niefeld MR, Braunstein JB, Wu AW, Saudek CD, Weller WE, Anderson GF. Preventable hospitalization among elderly Medicare beneficiaries with type 2 diabetes. Diabetes Care. 2003;26(5):1344-9.
-
1616 Booth GL, Hux JE. Relationship between avoidable hospitalizations for diabetes mellitus and income level. Arch Intern Med. 2003;163(1):101-6.
) . This may raise a few possibilities, one being that this diagnosis, among those that make up the cast of ACSCs, would be the most sensitive to PHC; that is, improving the quality of and access to this care level would result in some level of impact on hospitalisations for this cause. On the other hand, considering the discussion on the management of chronic diseases by primary care (
1717 Mendes EV. O cuidado das condições crônicas na Atenção Primária à Saúde: o imperativo da consolidação da Estratégia Saúde da Família. Brasília: OPAS; 2012.
) , it justifies studies focused on these diagnoses such as diabetes.
By analysing the relationship between ACSCs and care quality offered by the ESF, it was found that hospitalisations for diabetes mellitus showed a declining trend in the population with adequate basic ambulatory care ( 1818 Elias E, Magajenski F. A Atenção Primária à Saúde no Sul de Santa Catarina: uma análise das internações por condições sensíveis à atenção ambulatorial, no período de 1999 a 2004. Rev Bras Epidemiol. 2008;11(4):633-47. ) . The ACSCs data in Brazil showed that, between 1998 and 2002, the expansion of the ESF was associated with a reduction in hospitalisations for diabetes mellitus and respiratory problems, while the expansion of the Community Agents Program (Programa de Agentes Comunitários) was associated with a reduction in hospitalisations for circulatory conditions ( 1919 Guanais F, Macinko J. Primary care and avoidable hospitalizations: evidence from Brazil. J Ambul Care Manage. 2009;32(2):115-22. ) .
In the city of Curitiba, there was an increase in ESF coverage during the years studied, but this study has a limitation for estimating the correlation between ESF coverage and ACSCs because of the short duration for analysing a historical series. Other studies should be performed to expand the historical series in order to allow for the correlation of ESF quality and coverage and for a better assessment of primary care.
When considering prenatal and childbirth-related diseases, the occurrence of hospitalisations for these causes is noteworthy, although they have been decreasing over the years. This is due to the implementation of the Curitiban Mother (Mãe Curitibana) program in 1999, which aimed to improve access to and quality of care for pregnant women from the beginning of pregnancy to post-partum. The occurrence of hospitalisations for this cause group does not necessarily mean a lack of effectiveness of PHC and the Program, but it may be a reflection of the limitations to using ACSCs as an indicator of PHC quality. This is because the determinants for hospitalisations can be multiple and diverse, such as those related to social causes, which remain hidden in the frequency of hospitalisations for a particular cause.
In Spain, PHC doctors have been resisting the evaluation of their clinical practice by means of a hospital indicator. Such resistance is based on the existence of other more relevant factors that are determinants of hospitalisations and beyond the control of PHC practitioners; these include patient characteristics, variability in clinical practice, and hospitalisation policies in these centres ( 2020 Gervas J, Homar JC. Hospitalizations by Ambulatory Care Sensitive Conditions (ACSC) from the general practitioner/family physician’s point of view. Rev Esp Salud Pública. 2007;81(1):7-13. ) .
When it comes to gender, the analysis of the data from Curitiba, similar to those of other studies (
88 Rehem TCMSB, Egry EY. Internações por condições sensíveis à Atenção Primária no Estado de São Paulo. Ciênc Saúde Coletiva. 2011;16(12):4755-66.
9 Torres RL, Rehem TCMSB, Egry EY, Ciosak SI. The panorama of ambulatory care sensitive conditions in district of São Paulo. Rev Esc Enferm USP [Internet]. 2011 [cited 2012 Feb 12];45(n.spe2):1661-6. Available from: http://www.scielo.br/pdf/reeusp/v45nspe2/en_04.pdf
http://www.scielo.br/pdf/reeusp/v45nspe2...
-
1010 Alfradique ME, Bonolo PF, Dourado I, Costa-Lima MF, Macinko J, Mendonça CS, et al. Internações por condições sensíveis à atenção primária: a construção da lista brasileira como ferramenta para medir o desempenho do sistema de saúde (Projeto ICSAP Brasil). Cad Saúde Pública. 2009;25(6):1337-49.
,
1212 Rehem TCMSB. Internações Sensíveis à Atenção Primária: limites e possibilidades da lista brasileira de diagnósticos [tese doutorado]. São Paulo: Escola de Enfermagem, Universidade de São Paulo; 2011.
) , showed a higher number of women hospitalised for ACSCs. This condition is possibly due to the fact that more women seek health services. In this case, besides the Basic Health Units (Unidades Básicas de Saúde – UBS), they also seek alternative hospital services, sometimes due to poor solutions offered by the UBS when facing health problems, which requires referral to another care level.
When analysing age range, ACSCs increase after 45 years of age and most particularly in the population aged 65 years or older. These hospitalisations can be supported by the changing disease patterns in the ageing population, a result of increased life expectancy due to demographic and epidemiological transitions. Another possible explanation may be the fact that the elderly have less access to PHC services because of transportation-related difficulties, lack of the physical condition necessary to get to the UBS, and high degree of dependency on companions, among others, thereby aggravating their health status and making hospital care necessary.
As to the requirements established in Directive No. 221 of April 17, 2008 regarding ACSCs and the evaluation and effectiveness of PHC, studies have been conducted showing that other aspects should be considered besides the access to and effectiveness of this care level. To analyse hospitalisations, it is necessary to take social determinants, the working process of the teams, and the organisation of the healthcare system into account ( 1212 Rehem TCMSB. Internações Sensíveis à Atenção Primária: limites e possibilidades da lista brasileira de diagnósticos [tese doutorado]. São Paulo: Escola de Enfermagem, Universidade de São Paulo; 2011. , 2121 Mendonça CS, Harzheim E, Duncan BB, Nunes LN, Leyh W. Trends in hospitalizations for primary care sensitive conditions following the implantation of Family Health Teams in Belo Horizonte, Brazil. Health Policy Plan. 2011;27(4):348-55. - 2222 Magan P, Alberquilla A, Otero A, Ribera JM. Hospitalizations for ambulatory care sensitive conditions and quality of primary care: their relation with socioeconomic and health care variables in the Madrid regional health service (Spain). Med Care. 2011;49(1):17-23. ) .
With regard to the health care system, it is necessary to simultaneously evaluate the local system and its organisation to be able to assess this care level, as the fundamental role of PHC as an ordering system is not defined by it. In fact, it will play the role that was assigned to it by the model adopted by the organisation of the system. Therefore, within the system where PHC is defined as acting selectively or only as a gateway, rather than ordering flows and counter-flows of users within the system, this care level will not reduce or avert the ACSCs and may be an important bias in making PHC responsible for these hospitalisations. In any case, its use will be of great value in pointing out the system’s weaknesses, signalling the issues that should be analysed by the management in order to organise services to confront these problems.
With respect to the work process, even if PHC work presupposes an interdisciplinary team-based approach for comprehensive actions, the nursing staff can play a key role in reducing or preventing ACSCs. This possibility stems from both the number of staff, including the Community Health Agents, and the duties of the nursing staff, which should prioritize actions for health promotion and disease prevention, as well as the control of common diseases that are on the ACSCs list.
CONCLUSION
This study allowed us to describe the profile of ACSCs in Curitiba and verified that the data observed was, almost entirely, highly statistically significant and similar to those of other Brazilian studies. However, the result of stabilizing the frequency of ACSCs in the municipality of Curitiba in order to evaluate the performance of this care level should be viewed with caution, since it is an indicator that presents some limitations, including the very reliability of diagnosis and use of secondary data.
Expanded studies of historical series should be encouraged to observe the trend since such results are best seen in large samples. It is important to remember that other analyses are indicated to answer evaluative questions that are beyond the objectives of this study.
Despite these aspects, ACSCs assessment studies should be performed, as it is an indicator that indirectly measures PHC functioning and resolution capacity. It may contribute to the reflection of both professionals involved in its execution, as well as SUS managers, on the pursuit of better resolution and care quality, at the same time on their potential to provide feedback on the Brazilian list of ACSCs.
REFERÊNCIAS
-
1World Health Organization (WHO). The World Health Report 2008: primary health care (now more than ever) [Internet]. Geneva; 2008 [cited 2012 Feb 19]. Available from: http://www.who.int/whr/2008/en/
» http://www.who.int/whr/2008/en/ -
2Bermúdez-Tamayo C, Márquez-Calderón S, Rodríguez del Aguila MM, Perea-Milla LE, Ortiz Espinosa J. Características organizativas de la atención primaria y hospitalización por los principals ambulatory care sensitive conditions. Aten Primária. 2004;33(6):305-11.
-
3Caminal Homal J, Starfield B, Sánchez Ruiz E, Casanova Matutano C, Morales M. The role of primary care in preventing ambulatory care sensitive conditions. Eur J Public Health. 2004;14(3):246-51.
-
4Caminal Homar J, Casanova Matutano C. La evaluación de la atención primaria y las hospitalizaciones por ambulatory care sensitive conditions: marco conceptual. Aten Primaria. 2003;31(1):61-5.
-
5Nedel FB, Facchini LA, Bastos JL, Martín-Mateo M. Conceptual and methodological aspects in the study of hospitalizations for ambulatory care sensitive conditions. Ciênc Saúde Coletiva. 2011;16 Suppl 1:1145-54.
-
6Nedel FB, Facchini LA, Martín-Mateo M, Navarro A. Características da atenção básica associadas ao risco de internar por condições sensíveis à atenção primária: revisão sistemática de literatura. Epidemiol Serv Saúde. 2010;19(1):61-75.
-
7Dias-da-Costa JS, Buttenbender, DC, Hoefel AL, Souza LL. Hospitalizações por condições sensíveis à atenção primária nos municípios em gestão plena do sistema no Estado do Rio Grande do Sul, Brasil. Cad Saúde Pública. 2010;26(2):358-64.
-
8Rehem TCMSB, Egry EY. Internações por condições sensíveis à Atenção Primária no Estado de São Paulo. Ciênc Saúde Coletiva. 2011;16(12):4755-66.
-
9Torres RL, Rehem TCMSB, Egry EY, Ciosak SI. The panorama of ambulatory care sensitive conditions in district of São Paulo. Rev Esc Enferm USP [Internet]. 2011 [cited 2012 Feb 12];45(n.spe2):1661-6. Available from: http://www.scielo.br/pdf/reeusp/v45nspe2/en_04.pdf
» http://www.scielo.br/pdf/reeusp/v45nspe2/en_04.pdf -
10Alfradique ME, Bonolo PF, Dourado I, Costa-Lima MF, Macinko J, Mendonça CS, et al. Internações por condições sensíveis à atenção primária: a construção da lista brasileira como ferramenta para medir o desempenho do sistema de saúde (Projeto ICSAP Brasil). Cad Saúde Pública. 2009;25(6):1337-49.
-
11Brasil. Ministério da Saúde. Portaria n. 221, de 17 de abril de 2008. Publica em forma do anexo a lista brasileira de internações por condições sensíveis à Atenção Primária. Diário Oficial da União, Brasília, 21 set. 2008. Seção 1, p. 50.
-
12Rehem TCMSB. Internações Sensíveis à Atenção Primária: limites e possibilidades da lista brasileira de diagnósticos [tese doutorado]. São Paulo: Escola de Enfermagem, Universidade de São Paulo; 2011.
-
13Rehem TCMSB, Egry EY, Ciosak SI. Internações por condições sensíveis à Atenção Primária no Hospital Geral de uma Microrregião de Saúde do Município de São Paulo, Brasil. Texto Contexto Enferm. 2012;21(3):535-42.
-
14Robbins JM, Valdmanis VG, Webb DA. Do public health clinics reduce rehospitalizations?: the urban diabetes study. J Health Care Poor Underserved. 2008;19(2):562-73.
-
15Niefeld MR, Braunstein JB, Wu AW, Saudek CD, Weller WE, Anderson GF. Preventable hospitalization among elderly Medicare beneficiaries with type 2 diabetes. Diabetes Care. 2003;26(5):1344-9.
-
16Booth GL, Hux JE. Relationship between avoidable hospitalizations for diabetes mellitus and income level. Arch Intern Med. 2003;163(1):101-6.
-
17Mendes EV. O cuidado das condições crônicas na Atenção Primária à Saúde: o imperativo da consolidação da Estratégia Saúde da Família. Brasília: OPAS; 2012.
-
18Elias E, Magajenski F. A Atenção Primária à Saúde no Sul de Santa Catarina: uma análise das internações por condições sensíveis à atenção ambulatorial, no período de 1999 a 2004. Rev Bras Epidemiol. 2008;11(4):633-47.
-
19Guanais F, Macinko J. Primary care and avoidable hospitalizations: evidence from Brazil. J Ambul Care Manage. 2009;32(2):115-22.
-
20Gervas J, Homar JC. Hospitalizations by Ambulatory Care Sensitive Conditions (ACSC) from the general practitioner/family physician’s point of view. Rev Esp Salud Pública. 2007;81(1):7-13.
-
21Mendonça CS, Harzheim E, Duncan BB, Nunes LN, Leyh W. Trends in hospitalizations for primary care sensitive conditions following the implantation of Family Health Teams in Belo Horizonte, Brazil. Health Policy Plan. 2011;27(4):348-55.
-
22Magan P, Alberquilla A, Otero A, Ribera JM. Hospitalizations for ambulatory care sensitive conditions and quality of primary care: their relation with socioeconomic and health care variables in the Madrid regional health service (Spain). Med Care. 2011;49(1):17-23.
Publication Dates
-
Publication in this collection
Aug 2013
History
-
Received
10 May 2011 -
Accepted
23 Aug 2012