Abstracts
OBJECTIVE: To demonstrate the relevance of ultrasonography and magnetic resonance imaging findings in the prenatal characterization and prognostic evaluation in cases of congenital diaphragmatic hernia. MATERIALS AND METHODS: Fourteen pregnant women (mean gestational age = 28.7 weeks) who had undergone ultrasonography for suspicion of fetuses with congenital diaphragmatic hernia were assessed by means of magnetic resonance imaging on a 1.5 tesla equipment, following the standard protocol. Two radiologists evaluated the images and the findings were defined by consensus. RESULTS: Twelve fetuses had left diaphragmatic hernia and two, right diaphragmatic hernia. Ultrasonography showed the fetal liver inside the thorax of five fetuses (three with left diaphragmatic hernia, and two with right diaphragmatic hernia) and magnetic resonance imaging in eight fetuses (six with left diaphragmatic hernia, and two with right diaphragmatic hernia). Stomach and small bowel loop herniation was observed in all of the fetuses with left diaphragmatic hernia (n = 12) at both magnetic resonance imaging and ultrasonography. Eight fetuses (seven with left diaphragmatic hernia and one with right diaphragmatic hernia) survived after surgical treatment. CONCLUSION: Ultrasonography and magnetic resonance imaging are complementary imaging methods in the evaluation of congenital diaphragmatic hernia. Magnetic resonance imaging is a helpful diagnostic method complementary to ultrasonography for evaluation of the fetal liver positioning, considering its relevance as a prognostic factor in cases of congenital diaphragmatic hernia.
Fetus; Congenital diaphragmatic hernia; Ultrasonography; Magnetic resonance imaging
OBJETIVO: Demonstrar a significância dos achados da ressonância magnética e da ultra-sonografia na caracterização pré-natal e avaliação do prognóstico de pacientes com hérnia diafragmática congênita. MATERIAIS E MÉTODOS: Catorze gestantes (idade gestacional média de 28,7 semanas) examinadas com ultra-sonografia e apresentando fetos com suspeita de hérnia diafragmática congênita foram avaliadas por meio da ressonância magnética. Os exames foram realizados em aparelho de 1,5 tesla usando seqüências-padrão. Dois radiologistas avaliaram as imagens e estabeleceram os achados por consenso. RESULTADOS: Doze fetos tinham hérnia diafragmática à esquerda e dois, à direita. O fígado fetal foi localizado no interior do tórax de cinco fetos pela ultra-sonografia (três com hérnia diafragmática esquerda e dois com hérnia diafragmática direita) e de oito pela ressonância magnética (seis com hérnia diafragmática esquerda e dois com hérnia diafragmática direita). Herniação do estômago e alças de intestino delgado foi observada em todos os fetos com hérnia diafragmática esquerda (n = 12), tanto pela ultra-sonografia quanto pela ressonância magnética. Oito fetos sobreviveram após cirurgia (sete com hérnia diafragmática esquerda e um com hérnia diafragmática direita). CONCLUSÃO: A ultra-sonografia e a ressonância magnética são métodos de imagens complementares na avaliação das hérnias diafragmáticas congênitas. A ressonância magnética pode auxiliar a ultra-sonografia na avaliação da posição do fígado, o qual representa importante fator prognóstico.
Feto; Hérnia diafragmática congênita; Ultra-sonografia; Ressonância magnética
ORIGINAL ARTICLE
The value of fetal ultrasonography and magnetic resonance imaging in the assessment of diaphragmatic hernias* Mailing address: Dr. Bruno Amim Avenida das Américas, 4666, sala 325, Barra da Tijuca Rio de Janeiro, RJ, Brazil, 22640-120 E-mail: brunoamim@gmail.com
Bruno AmimI; Heron Werner Jr.II; Pedro Augusto DaltroIII; Erika AntunesIV; Tatiana FazecasV; Leise RodriguesV; Fernando GuerraVI; Edson MarchioriVII; Emerson Leandro GasparettoVIII; Romeu Côrtes DominguesIX
IFellow Master degree, Course of Post-graduation in Radiology Universidade Federal do Rio de Janeiro (UFRJ), MD, Trainee at Clínica de Diagnóstico por Imagem (CDPI), Rio de Janeiro, RJ, Brazil
IIMD, Clínica de Diagnóstico por Imagem (CDPI), Rio de Janeiro, RJ, Brazil
IIIMD, Radiologist, Responsible for Pediatric Radiology Unit Clínica de Diagnóstico por Imagem (CDPI), Rio de Janeiro, RJ, Brazil
IVMD, Trainee at Clínica de Diagnóstico por Imagem (CDPI), Rio de Janeiro, RJ, Brazil
VMDs, Radiologists at Clínica de Diagnóstico por Imagem (CDPI), Rio de Janeiro, RJ, Brazil
VIMD, Surgeon at Instituto Fernandes Figueira, Rio de Janeiro, RJ, Brazil
VIITitular Professor of Radiology, Universidade Federal Fluminense (UFF), Niterói, RJ, Adjunct Coordinator for the Course of Post-graduation in Radiology, Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
VIIIAssociate Professor of Radiology at Universidade Federal do Rio de Janeiro (UFRJ), MD, Radiologist, Clínica de Diagnóstico por Imagem (CDPI), Rio de Janeiro, RJ, Brazil
IXMD, Radiologist, Director, Clínica de Diagnóstico por Imagem (CDPI), Rio de Janeiro, RJ, Brazil
Mailing address Mailing address: Dr. Bruno Amim Avenida das Américas, 4666, sala 325, Barra da Tijuca Rio de Janeiro, RJ, Brazil, 22640-120 E-mail: brunoamim@gmail.com
ABSTRACT
OBJECTIVE: To demonstrate the relevance of ultrasonography and magnetic resonance imaging findings in the prenatal characterization and prognostic evaluation in cases of congenital diaphragmatic hernia.
MATERIALS AND METHODS: Fourteen pregnant women (mean gestational age = 28.7 weeks) who had undergone ultrasonography for suspicion of fetuses with congenital diaphragmatic hernia were assessed by means of magnetic resonance imaging on a 1.5 tesla equipment, following the standard protocol. Two radiologists evaluated the images and the findings were defined by consensus.
RESULTS: Twelve fetuses had left diaphragmatic hernia and two, right diaphragmatic hernia. Ultrasonography showed the fetal liver inside the thorax of five fetuses (three with left diaphragmatic hernia, and two with right diaphragmatic hernia) and magnetic resonance imaging in eight fetuses (six with left diaphragmatic hernia, and two with right diaphragmatic hernia). Stomach and small bowel loop herniation was observed in all of the fetuses with left diaphragmatic hernia (n = 12) at both magnetic resonance imaging and ultrasonography. Eight fetuses (seven with left diaphragmatic hernia and one with right diaphragmatic hernia) survived after surgical treatment.
CONCLUSION: Ultrasonography and magnetic resonance imaging are complementary imaging methods in the evaluation of congenital diaphragmatic hernia. Magnetic resonance imaging is a helpful diagnostic method complementary to ultrasonography for evaluation of the fetal liver positioning, considering its relevance as a prognostic factor in cases of congenital diaphragmatic hernia.
Keywords: Fetus; Congenital diaphragmatic hernia; Ultrasonography; Magnetic resonance imaging.
INTRODUCTION
Congenital diaphragmatic hernia (CDH) is a developmental involving the posterolateral diaphragm that manifests at about the 9th gestational week, with herniation of abdominal viscera into the chest cavity. The incidence is about one in 30004000 live births, representing one of the most frequent causes of neonatal morbidity and mortality(13).
CDH etiology is still to be known, but in 30% of cases it is associated with chromosomal anomalies or anatomical malformations(3). Morbidity and mortality are related to pulmonary hypoplasia resulting from mechanical compression of the developing lungs(4), and to the presence of hepatic herniation. However, studies in the literature demonstrate that pulmonary hypoplasia would be a primary defect associated with CDH(5).
The prenatal diagnosis of CDH is established by ultrasonography (US). However, in some cases this method is limited by the presence of artifacts resulting from poor fetal positioning or because of other limitations such as maternal obesity or an insufficiently trained operator(6,7). An accurate diagnosis is critical, particularly in centers where intrauterine therapeutic tracheal occlusion is adopted to promote an increase in bronchoalveolar pressure and pulmonary volume(2). For this reason, magnetic resonance imaging (MRI) used as a supplement to US can be useful to confirm the diagnosis and as an aid in the evaluation of the fetal prognosis(8,9).
The arrival of new MRI techniques has allowed a more detailed study of fetuses considering that, with faster sequences, the images acquisition can be performed during a single respiratory pause of the mother, minimizing fetal motion artifacts, besides eliminating the necessity of sedation(1012). The higher image resolution and contrast of MRI as compared with US allows a more accurate evaluation of the diaphragmatic lesion extent, herniated viscera and the fetal pulmonary maturity(11,12).
The present study was aimed at demonstrating the relevance of MRI and US findings for establishing the prenatal diagnosis in 14 cases of CDH.
MATERIALS AND METHODS
The present study was developed in the Clínica de Diagnóstico por Imagem (CDPI), Rio de Janeiro, RJ, in the period between July/1999 and February/2007, with patients coming from Instituto Fernandes Figueira and private clinics. This study was approved by the Committee for Ethics in Research of the Institution, and all of the patients signed a standard term of free and informed consent. The sample included fourteen pregnant women with ages ranging between 20 and 37 years (mean, 29.5 years) who had been assessed by obstetric sonography between the 13th and 26th gestational weeks (mean, 22.3 weeks), with a suggested diagnosis of CDH. MRI had been requested for diagnostic elucidation.
Previously to the examination, each patient answered a standard questionnaire about possible contraindications for the study and was given information on the procedure. MRI was performed and later supplemented by US. The studies were performed between the 26th and 36th gestational weeks (mean, 28.7 weeks) in a Magnetom Avanto and a 1.5 tesla Magnetom Vision equipment (Siemens; Germany). Images acquisition was performed with a surface coil positioned on the abdomen of the pregnant woman, in T2-weighted sequences HASTE (repetition time [TR] = 1000 ms and echo time [TE] = 8587 ms; field of view (FoV) = 250380 mm; 256 × 112256 mm matrix] in the axial, coronal and sagittal planes of the fetus, and T1-weighted sequences (TR = 201 ms, TE = 4,72 ms; FoV = 250400 mm; 256 × 90256 mm matrix) with 3.0 mm to 7.0 mm slices. Following, the patients were submitted to US scans in Logic 500 and Voluson 730 (General Electric; USA) equipment coupled with 3.5 MHz, 5.0 MHz and volumetric 3D and 4D transducers.
Both MRI and US images were independently reviewed by two experienced radiologists, with the findings (herniated viscera and lesions extent) being defined by consensus. Ultrasonography evaluated the diaphragm integrity through the observation of the fetal stomach inside the chest cavity, causing mediastinal deviation and decrease in pulmonary volume. Color-Doppler US was utilized to visualize the blood flow in supra-hepatic and portal veins, aiming at identifying the presence, or not, of the liver inside the thorax. On MRI images the stomach was identified as a hyperintense structure on T2-weighted sequences, while the intestinal loops were visualized as tubular serpiginous structures with variable signal intensities presumably as a result of the presence or absence of meconium. The fetal liver position was assessed on T1-weighted sequences, defining the presence or absence of herniation.
Additionally, all of the patients underwent follow-up throughout the gestational and postnatal periods. Their gestations were interrupted between the 37th and 38th weeks (mean 37.6 weeks) by vaginal delivery (3 patients) and Cesarean section (11 patients). On average, the fetuses weighted 2933 g (1919 g to 3520 g).
RESULTS
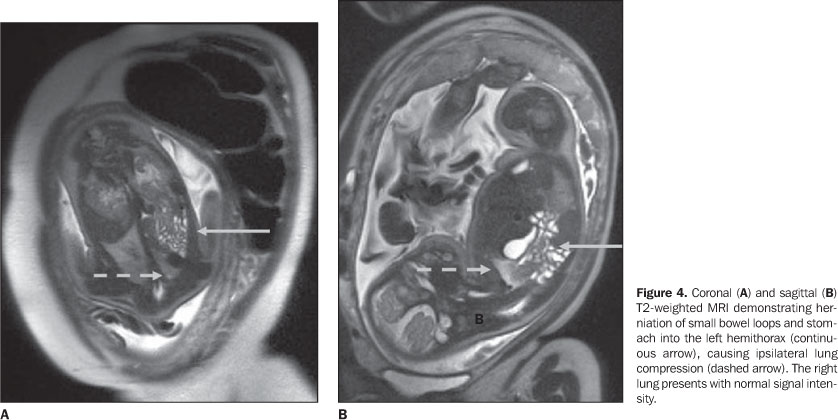
Among the 14 fetuses, 12 presented left-sided (LDH), and two right-sided congenital diaphragmatic hernias (RDH). The fetal liver was found inside the thorax in eight fetuses by MRI (six with LDH and two with RDH), and in five fetuses by US (three with LDH and two with RDH) (Figure 1). The presence of the stomach and bowel loops inside the chest cavity causing right mediastinal shift was observed both on MRI and US in all of the 12 fetuses with LDH, (Figures 2, 3 and 4). A mild left mediastinal shift also was observed on both imaging methods in the two cases of RDH. Additionally, cranial shift of the left kidney was found in one fetus with LDH both on MRI and US images.
Polyhydramnios was found both on US and MRI in five gestations (three in cases of LDH and in the two cases of RDH). One fetus (with RDH) presented microphthalmos which was best visualized on US images. Another fetus (with LDH) showed cerebellar vermis hypoplasia detected both by US and MRI, and interventricular-communication-type cardiac malformation detected only by US. One case of imperforate anus was undetected by both MRI and US. Karyotype alteration was found in two cases, one fetus with 18-trisomy syndrome (46, XX + 18), and another with 46 karyotype, X, der (X), t (X,Y) (p22.3;q12).
Amongst the 14 fetuses studied, six (42.8%) five with LDH and one with RDH progressed to post-natal death, two of them after being submitted to surgical hernia correction. Eight fetuses (57.1%) survived after surgery (seven with LDH and one with RDH). Among these seven fetuses with LDH who survived, six presented with the liver in its usual topography, evidencing the relevant role of hepatic herniation in the determination of the fetal prognosis. Six of the eight surviving children reached the age of seven months, with gastroesophageal reflux being identified in four (three with LDH correction and one with RDH correction), and pneumonia in three (two with LDH correction and one with RDH correction). One children presented retardation of neurological development besides a significant visual deficit.
DISCUSSION
Congenital diaphragmatic hernias result from a developmental defect in the diaphragm because of a failure in the closure of the pleuroperitoneal canal between the 9th and 10th gestational weeks(4). If the pleuroperitoneal canal remains open when the intestines return to the abdomen from the umbilical cord during the tenth week, the abdominal viscera move freely into the thoracic cavity. If the pleuroperitoneal canal closes but fails to become muscularized, the viscera may move into the chest, as a result of the limited intra-abdominal space(4). So, in fetuses with CDH, bronchi are present, but the bronchiolus branching is reduced. The number of alveoli/acinus is normal, but the absolute number of alveoli is reduced because of the lower number of bronchiolus division. The vascular bed also presents altered, with a significant decrease in the number of vessels and muscular hyperplasia. The prognosis in cases involving a child with CDH will be directly related with the extent of pulmonary hyperplasia that is associated with the gestational period where the herniation process was completed(4).
The prenatal diagnosis of CDH by means of US is suggested as the presence of the stomach in the fetal chest is demonstrated(3). Also, cardiomediastinal shift and the presence of left portal vein branches at the level or above the diaphragm can be observed, indicating the liver herniation into the fetal chest(13).
MRI can clearly demonstrate the presence of the stomach and bowel loops in the left hemithorax, particularly on T1-weighted sequences(7,8,14). The herniated liver is best visualized on T1-weighted sequences. The stomach is seen as a structure of low T1 and high T2 signal intensities. Bowel loops appear like serpiginous structures of either high or low T1 and T2 signal intensities. This variable signal intensity is presumably caused by the presence or absence of meconium(7,8). Cardiomediastinal shift to the right and the resulting pulmonary compression are best visualized on axial images. The pulmonary parenchyma can be best visualized on T2-weighted sequences, as a hyperintense structure because the lungs are filled with fluid. In 57% to 86% of cases of CDH, the hepatic parenchyma is partially herniated (liver-up)(3). On MRI, the liver is seen as a structure of high T1 and low T2 signal intensities, so, this method plays a significant role in the evaluation of the fetal prognosis, considering that the presence or absence of part of a herniated liver in the chest cavity corresponds, respectively, to an approximate 57% and 7% mortality rate(3). On axial images, the herniated liver can be easily visualized anteriorly to the stomach. Also, it can be seen in the chest cavity on coronal images both on T1- and T2-weighted sequences. The gastric volvulus also can be identified in the fetal chest, in cases where the greater curvature is superior to the lesser curvature of the stomach(3).
Right-sided congenital diaphragmatic hernias correspond to 12% of all cases of CDH(3,15). The liver is always in the chest cavity, compressing cardiac structures in the left hemithorax. Bowel loops shift into the right hemithorax is less frequent. The mortality rate in cases of this type of hernia is around 80%(3,15). Fetal ascites and hydrothorax also may occur because of hepatic venous obstruction by a Budd-Chiari mechanism, although cervical and cephalic edemas may result from an obstruction of the superior vena cava(3).
Two major indicators in the evaluation of fetal prognosis are the detection of hepatic herniation that is best visualized by MRI, and pulmonary maturity that can be evaluated by means of the lung/cephalic circumference ratio (LCR), or by the pulmonary parenchyma signal intensity. LCR is obtained by means of axial US scans at the level of the four cardiac chambers, in the period between the 24th and 26th gestational weeks. A LCR < 1.0 is associated to 100% mortality, while a LCR > 1.4 is associated to a good prognosis. For a LPC between 1.0 and 1.4, the mortality rate is around 60%(9,16). On MRI, a homogeneous high signal intensity of the fetal pulmonary parenchyma indicates the absence of pulmonary hypoplasia, while low signal intensity suggests the presence of pulmonary hypoplasia(14).
In the present study, a partially herniated liver was found in the chest cavity of eight fetuses by MRI six of them with LDH and two with RDH. Therefore, MRI complemented US that had identified hepatic herniation in five fetuses (three with LDH and two with RDH). Because of the difficulty in identifying the pulmonary parenchyma, MRI demonstrated possible pulmonary hypoplasia in five fetuses (three with LDH and two with RDH). In the present study, marked polyhydramnios was found both by US and MRI in five cases, two of them with RDH and three with LDH (one fetus with 18-trisomy). In this group of fetuses with marked polyhydramnios, only two survived. The presence of microphthalmos associated with RDH was best assessed by US. Besides LDH, the fetus with 18-trisomy presented cerebellar vermis hypoplasia visualized both by US and MRI, and also interventricular communication identified by US.
Finally, US and MRI constitute complementary methods in the evaluation of patients with CDH. MRI plays a significant role as a supplement to US in the diagnosis and prognostic evaluation of CDH, and can easily assess the liver position. Additionally, MRI does not present the typical US limitations represented by the presence of artifacts resulting from poor fetal positioning, beam attenuation in maternal adiposity and operator dependence.
REFERENCES
Received May 8, 2007. Accepted after revision June 19, 2007.
* Study developed at Clínica de Diagnóstico por Imagem (CDPI), Rio de Janeiro, RJ, Brazil.
- 1. Adzick NS, Harrison MR, Glick PL, et al. Diaphragmatic hernia in the fetus: prenatal diagnosis and outcome in 94 cases. J Pediatr Surg. 1985;20: 35761.
- 2. Harrison MR, Mychaliska GB, Albanese CT, et al. Correction of congenital diaphragmatic hernia in utero IX: fetuses with poor prognosis (liver herniation and low lung-to-head ratio) can be saved by fetoscopic temporary tracheal occlusion. J Pediatr Surg. 1998;33:101723.
- 3. Leung JW, Coakley FV, Hricak H, et al. Prenatal MR imaging of congenital diaphragmatic hernia. AJR Am J Roentgenol. 2000;174:160712.
- 4. Harrison MR, Adzick NS, Flake AW. Congenital diaphragmatic hernia: an unsolved problem. Semin Pediatr Surg. 1993;2:10912.
- 5. Ijsselstijn H, Tibboel D. The lungs in congenital diaphragmatic hernia: do we understand? Pediatr Pulmonol. 1998;26:20418.
- 6. Guibaud L, Filiatrault D, Garel L, et al. Fetal congenital diaphragmatic hernia: accuracy of sonography in the diagnosis and prediction of the outcome after birth. AJR Am J Roentgenol. 1996; 166:1195202.
- 7. Hubbard AM, Adzick NS, Crombleholme TM, et al. Congenital chest lesions: diagnosis and characterization with prenatal MR imaging. Radiology. 1999;212:438.
- 8. Hubbard AM, Adzick NS, Crombleholme TM, et al. Left-sided congenital diaphragmatic hernia: value of prenatal MR imaging in preparation for fetal surgery. Radiology. 1997;203:63640.
- 9. Sydorak RM, Harrison MR. Congenital diaphragmatic hernia: advances in prenatal therapy. Clin Perinatol. 2003;30:46579.
- 10. Frates MC, Kumar AJ, Benson CB, et al. Fetal anomalies: comparison of MR imaging and US for diagnosis. Radiology. 2004;232:398404.
- 11. Blasbalg R, Ogawa RE, Costa DN, et al. Como fazer exames com imagens ponderadas em T2 para o estudo do abdome superior? Radiol Bras. 2005;38(5):vvi.
- 12. Francisco VV, D'Ippolito G, Silva GPA, et al. Prevalência de artefatos em exames de ressonância magnética do abdome utilizando a seqüência GRASE: comparável com as melhores seqüências rápidas? Radiol Bras. 2005;38:3238.
- 13. Goldstein RB. Avaliação ultra-sonográfica do tórax fetal. In: Callen PW, editor. Ultra-sonografia em obstetrícia e ginecologia. 4Ş ed. Philadelphia: Guanabara Koogan; 2002. p.40129.
- 14. Kuwashima S, Nishimura G, Iimura F, et al. Low-intensity fetal lungs on MRI may suggest the diagnosis of pulmonary hypoplasia. Pediatr Radiol. 2001;31:66972.
- 15. Hedrick HL, Crombleholme TM, Flake AW, et al. Right congenital diaphragmatic hernia: prenatal assessment and outcome. J Pediatr Surg. 2004;39: 31923.
- 16. Metkus AP, Filly RA, Stringer MD, et al. Sonographic predictors of survival in fetal diaphragmatic hernia. J Pediatr Surg. 1996;31:14852.
Publication Dates
-
Publication in this collection
28 Mar 2008 -
Date of issue
Feb 2008
History
-
Received
08 May 2007 -
Accepted
19 June 2007