Abstract
Introduction:
Human immunodeficiency virus (HIV) the causative agent of Acquired immunodeficiency syndrome (AIDS) is an important cause of renal diseases in sub-Saharan Africa. There is paucity of studies on the burden of chronic kidney disease (CKD) among patients with HIV/AIDS in the North-Central zone of Nigeria.
Methods:
This is a cross-sectional study of 227 newly-diagnosed, antiretroviral naïve patients with HIV/AIDS seen at the HIV clinic of the Medical Out-patient Department (MOPD) of University of Ilorin Teaching Hospital (UITH). They were matched with 108 control group. Laboratory investigations were performed for the participants. CKD was defined as estimated glomerular filtration rate (eGFR) < 60 ml/min/1.73 m2 and/or albumin creatinine ratio (ACR) > 30 mg/g.
Results:
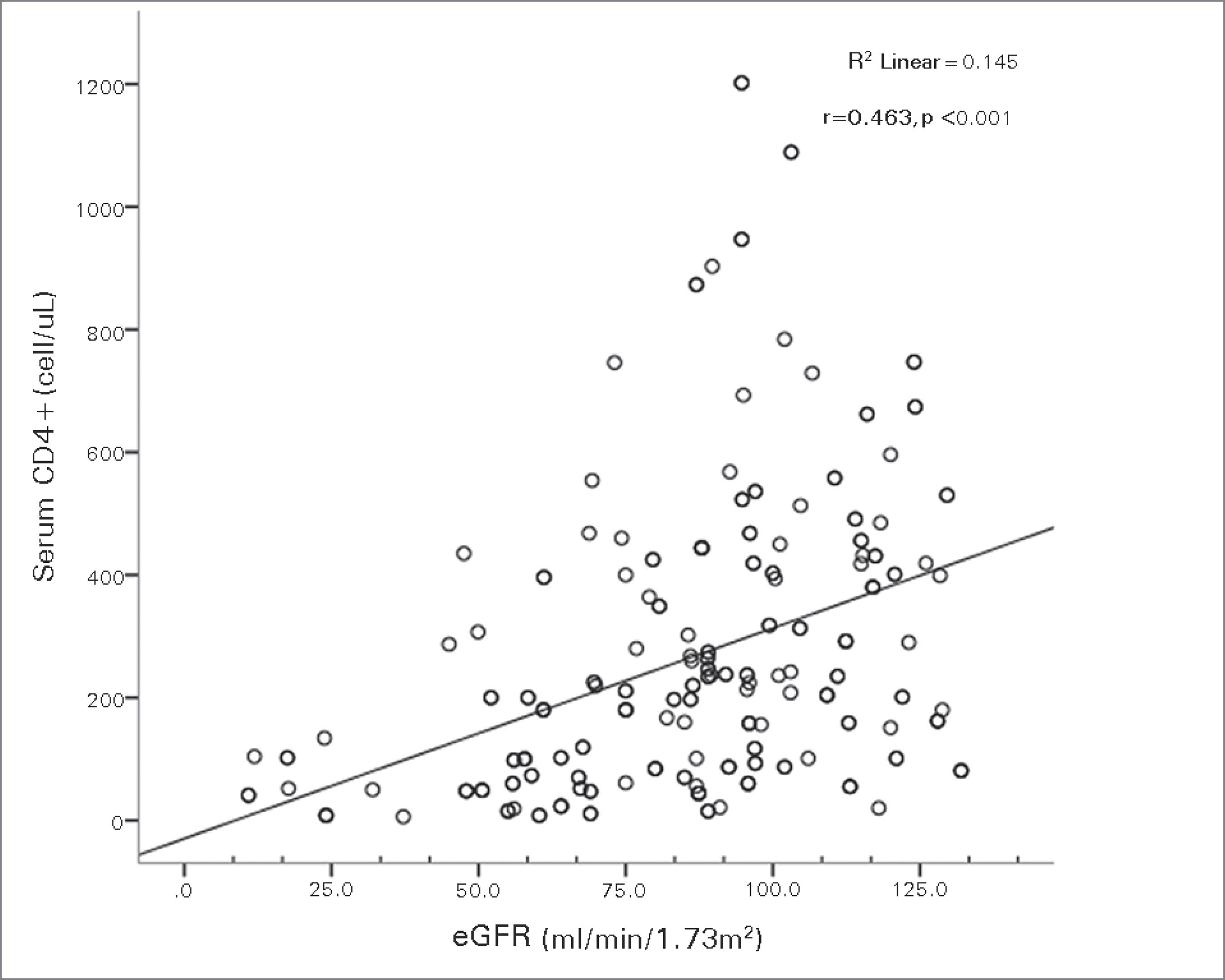
There were 100 (44%) males among the patients and 47 (43.5%) among the control group. The mean ages of the patients and controls were 40.3 ± 10.3 years and 41.8 ± 9.5 years respectively. CKD was observed in 108 (47.6%) among the patients and 18 (16.7%) of the controls (p = 0.01). The median CD4 T-cell count was significantly lower in patients with CKD. Ninety-three (41.0%) of the patients had dipstick proteinuria of > 2 +. The median albumin creatinine ratio (ACR) was significantly higher among the HIV-positive patients (272.3 mg/g) compared with the HIV-negative controls (27.22 mg/g) p = 0.01. The CD4 T-cell count correlates positively with eGFR (r = 0.463, p = 0.001) and negatively with ACR (r = -0.806, p = 0.001).
Conclusions:
CKD is very common among patients with HIV/AIDS in Ilorin. Screening and early intervention for CKD should be part of the protocols in the management of these patients.
Keywords:
AIDS-associated nephropathy; kidney diseases; prevalence
Resumo
Introdução:
o vírus da imunodeficiência humana (HIV), o agente causador da síndrome da imunodeficiência adquirida (AIDS), é uma importante causa de doenças renais na África subsaariana. Há escassez de estudos sobre o impacto da doença renal crônica (DRC) em pacientes com HIV/AIDS na zona centronorte da Nigéria.
Métodos:
Este é um estudo transversal com 227 pacientes recém-diagnosticados com HIV/AIDS, não tratados com agentes antirretrovirais, atendidos no ambulatório de HIV do Hospital Universitário da Universidade de Ilorin (UITH). Eles foram pareados com 108 indivíduos do grupo controle. Os pacientes foram submetidos a investigações laboratoriais. A DRC foi definida como taxa estimada de filtração glomerular (eTFG) ≤ 60 ml/min/1,73m2 e/ou a relação entre albumina e creatinina (RAC) ≥ 30 mg/g
Resultados:
Houve 100 (44%) pacientes do sexo masculino entre os pacientes e 47 (43,5%) entre os indivíduos do grupo controle. As médias de idade dos pacientes e controles foram de 40,3 ± 10,3 anos e 41,8 ± 9,5 anos, respectivamente. A DRC foi observada em 108 indivíduos (47,6%) entre os pacientes e em 18 (16,7%) dos controles (p = 0,01). A contagem mediana de linfócitos T CD4 foi significativamente menor nos pacientes com DRC. Noventa e três (41,0%) dos pacientes tiveram proteinúria ≥ 2 + no exame de dipstick (tiras reagentes). A mediana da relação entre creatinina e albumina (RAC) foi significativamente maior entre os indivíduos HIV-positivos (272,3 mg/g), em comparação com os controles HIV negativos (27,22 mg/g) p = 0,01. A contagem de linfócitos T CD4 correlacionou-se positivamente com a eTFG (r = 0,463, p = 0,001) e negativamente com o RAC (r = -0,806, p = 0,001).
Conclusões:
DRC é muito comum entre os pacientes com HIV/AIDS em Ilorin. Triagem e intervenção precoce para DRC devem fazer parte dos protocolos de tratamento desses pacientes.
Palavras-chave:
doenças renais; nefropatia associada à AIDS; prevalência
Introduction
Human immunodeficiency virus (HIV), the causative agent of acquired immune-deficiency syndrome (AIDS) is a challenging public health problem worldwide. The disease burden is worse in Africa where poverty, ignorance and illiteracy rates are still.11 AIDS Epidemic Update December 2007 [Accessed Mar 15 2015]. Available from: http://data.unaids.org/pub/EPISlides/2007/2007_epiupdate_en.pdf
http://data.unaids.org/pub/EPISlides/200...
,22 Nigeria National Agency for the Control of AIDS. Abuja Nigeria GLOBAL AIDS RESPONSE; Country Progress Report Nigeria GARPR 2012 [Accessed Mar 15 2015]. Available from: http://www.unaids.org/sites/default/files/en/dataanalysis/knowyour-response/countryprogressreports/2012countries/Nigeria%202012%20GARPR%20Report%20Revised.pdf
http://www.unaids.org/sites/default/file...
The kidney is one of the organs that is commonly affected by HIV/AIDS and different types of renal disorders are encountered in all stages of the disease.
The contribution of HIV/AIDS to the prevalence of CKD in Africa and particularly sub-Saharan Africa is quite huge, more importantly as this region has scarce limited resources to adequately manage or control this disease. In Nigeria, reports from the available scattered studies on renal involvement in patients with HIV infection still suggest a paucity of data in spite of the prevalence of HIV/AIDS infection in the Nigerian population. Abnormalities in fluid, electrolyte, and acid-base metabolism in patients infected with HIV have also been recognized.33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
,44 Agaba EI, Agaba PA, Sirisena ND, Anteyi EA, Idoko JA. Renal disease in the acquired immunodeficiency syndrome in north central Nigeria. Niger J Med 2003;12:120-5.
Various histological patterns that characterize the kidney disease in HIV infections including HIV/ AIDS associated nephropathy have been described and documented by few authors.33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
,55 Rao TK, Filippone EJ, Nicastri AD, Landesman SH, Frank E, Chen CK, et al. Associated focal and segmental glomerulosclerosis in the acquired immunodeficiency syndrome. N Engl J Med 1984;310:669-73. PMID: 6700641 DOI: http://dx.doi.org/10.1056/NEJM198403153101101
http://dx.doi.org/10.1056/NEJM1984031531...
6 Pardo V, Aldana M, Colton RM, Fischl MA, Jaffe D, Moskowitz L, et al. Glomerular lesions in the acquired immunodeficiency syndrome. Ann Intern Med 1984;101:429-34. PMID: 6476632 DOI: http://dx.doi.org/10.7326/0003-4819-101-4-429
http://dx.doi.org/10.7326/0003-4819-101-...
7 D'Agati V, Appel GB. Renal pathology of human immunodeficiency virus infection. Semin Nephrol 1998;18:406-21. PMID: 9692353-88 Okpechi I, Swanepoel C, Duffield M, Mahala B, Wearne N, Alagbe S, et al. Patterns of renal disease in Cape Town South Africa: a 10-year review of a single-centre renal biopsy database. Nephrol Dial Transplant 2011;26:1853-61. DOI: http://dx.doi.org/10.1093/ndt/gfq655
http://dx.doi.org/10.1093/ndt/gfq655...
In most of these studies, kidney disease was defined based on the presence of albuminuria and/or low estimated glomerular filtration rate (eGFR).99 Szczech LA, Gange SJ, van der Horst C, Bartlett JA, Young M, Cohen MH, et al. Predictors of proteinuria and renal failure among women with HIV infection. Kidney Int 2002;61:195-202. PMID: 11786101 DOI: http://dx.doi.org/10.1046/j.1523-1755.2002.00094.x
http://dx.doi.org/10.1046/j.1523-1755.20...
10 Naicker S, Fabian J. Risk factors for the development of chronic kidney disease with HIV/AIDS. Clin Nephrol 2010;74:S51-56.-1111 Okafor UH, Unuigbe EI, Ojogwu LI, Oviasu E, Wokoma FS. Renal disease in HIV infected patients at University of Benin Teaching Hospital in Nigeria. Afr Health Sci 2011;11:S28-33. DOI:http://dx.doi.org/10.4314/ahs.v11i3.70067
http://dx.doi.org/10.4314/ahs.v11i3.7006...
Many of these reports have shown that HIV associated nephropathy (HIVAN) is particularly prevalent among the black patient population.1010 Naicker S, Fabian J. Risk factors for the development of chronic kidney disease with HIV/AIDS. Clin Nephrol 2010;74:S51-56.,1212 Avila-Casado C, Fortoul TI, Chugh SS. HIV-associated nephropathy: experimental models. Contrib Nephrol 2011;169:270-85. PMID: 21252526
This study was designed to determine the prevalence and clinical manifestations of CKD in newly diagnosed HIV/AIDS patients in the North-Central region of Nigeria at the University of Ilorin Teaching Hospital (UITH).
Materials and methods
This is a cross sectional study of 227 patients with HIV/AIDS and 108 age and sex-matched control group. The study was conducted over a six month period (June to November 2010), at the HIV clinic of the medical out-patient department (MOPD) of UITH. Ethical approval was obtained from the ethical and research committee of the hospital.
UITH is located in Ilorin, the capital of Kwara State in the North Central geopolitical zone of Nigeria. The population of Ilorin city was estimated to be 847,582 accounting for 36% of the population of Kwara state (2,365,353).1313 Discover Nigeria Facts about Nigeria Kwara State (State of Harmony) [Accessed Jul 27 2014]. Available from: http://zodml.org/Nigeria/Geography/Kwara%20State/
http://zodml.org/Nigeria/Geography/Kwara...
The state has five other adjoining states being serviced partly by the hospital with estimated population of about 20 million.1313 Discover Nigeria Facts about Nigeria Kwara State (State of Harmony) [Accessed Jul 27 2014]. Available from: http://zodml.org/Nigeria/Geography/Kwara%20State/
http://zodml.org/Nigeria/Geography/Kwara...
Majority of the people of Ilorin are indigenous Yoruba and Fulani tribes. Minority groups include Hausa, Igbos and other ethnic groups. The people are mainly traders, civil servants, businessmen and women, students and artisans.
Eligibility for enrolment into the study include individuals who were 18 years and above. Newly-diagnosed antiretroviral-naïve HIV/AIDS patients referred to the HIV clinic of the infectious disease unit in the hospital were recruited consecutively. Individuals with risk factors for chronic kidney disease such as diabetes mellitus (DM), systemic hypertension, pre-existing renal disease, sickle cell disease and patients with HIV who were on highly active antiretroviral therapy or on any other medication that may interfere with kidney functions were excluded from the study. Also excluded were the following; patients with urinary tract infection, hepatitis B or C virus, history of exposure to nephrotoxic agents such as habitual use of non-steroidal anti-inflammatory drugs (NSAID), native medications or herbs and use of mercury/hydroquinone containing soaps or creams. The control group were healthy individuals who presented at the hospital staff clinic for routine medical check-up and voluntary blood donors from the general populace at the blood bank of the hospital. Control group underwent clinical examinations and laboratory investigations.
Written informed consent was obtained from all participants. Pretest counseling was carried out and HIV screening was done for the control group using double ELISA (Determine® Inverse medical Japan Co. Ltd and Uni-GoldTM Trinity Biotech plc. Ireland).
A pretested structured interviewer administered questionnaire was used to collect socio-demographic, relevant clinical information and anthropometric measurements.
Laboratory investigations were performed at the laboratory departments of UITH, and they included complete blood counts, electrolytes (Na +, K +), serum creatinine and urea concentration (by Jaffe's reaction and diacetylmonoxime methods respectively).1414 Greenwald I. The chemistry of Jaffe's reaction for creatinine: V. The isolation of the red coumpound. J Biol Chem 1928;80:103-6.,1515 Marsh WH, Fingerhut B, Miller H. Automated and manual direct methods for the determination of blood urea. Clin Chem 1965;11:624-7.
The value of serum creatinine obtained was used to calculate the glomerular filtration rate (GFR) of each subject, using the modified MDRD formula:
GFR = 186 x (Cr) - 1.154 x (Age) - 0.203 x 0.742 (if female) x 1.210 (if black).1616 Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 1999;130:461-70. DOI:http://dx.doi.org/10.7326/0003-4819-130-6-199903160-00002
http://dx.doi.org/10.7326/0003-4819-130-...
Mid-stream urine samples were collected for urine microscopy to exclude urinary tract infection.
Dipstick urinalysis (Multistix® 10SG by Bayer) was done to detect the presence of protein, red blood cell, pH, specific gravity, leucocytes, glucose, and nitrite in the urine sample.Fasting glycemia was also done to exclude diabetes mellitus.1717 Trinde P. Determination of blood glucose using glucose oxidase with an alternative oxygen acceptor. Ann Clin Biochem 1969;6:24-27. In addition, CD4 + T cell count was analyzed by flow cytometry method using CyFlow® (Partec GmbH, Münster, Germany).
Spot urine samples were collected for albuminuria determination with HemoCue point of care analyzer using immuno-turbidimetric method. Urine creatinine was estimated on the same sample by Jaffe's reaction.1414 Greenwald I. The chemistry of Jaffe's reaction for creatinine: V. The isolation of the red coumpound. J Biol Chem 1928;80:103-6.
Albumin creatinine ratio (ACR) in mg/g was obtained by dividing urine albumin concentration (mg/l) with urine creatinine concentration (g/l).
Operational definitions:
The following definitions were used for the variables in this study;
-
Microalbuminuria was defined as albumin creatinine ratio 30-299 mg/g.1818 Lydakis C, Lip GY. Microalbuminuria and cardiovascular risk. QJM 1998;91:381-91. DOI:http://dx.doi.org/10.1093/qjmed/91.6.381
http://dx.doi.org/10.1093/qjmed/91.6.381... -
Macroalbuminuria or overt albuminuria was defined as ACR of spot urine sample > 300 mg/g.1818 Lydakis C, Lip GY. Microalbuminuria and cardiovascular risk. QJM 1998;91:381-91. DOI:http://dx.doi.org/10.1093/qjmed/91.6.381
http://dx.doi.org/10.1093/qjmed/91.6.381... -
Chronic Kidney Disease was defined as kidney damage based on finding of albuminuria > 30 mg/g and/or eGFR below 60 ml/ml/1.73m2.
-
Dipstick proteinuria of 1 + or greater was taken as significant.
According to the National kidney foundation using the Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines1919 National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 2002;39:S1-266. patients were classified into five stages based on GFR as follows;
Stage 1 (Normal or increased eGFR) = > 90 ml/min/1.73 m2; Stage 2 (Mildly decreased eGFR) = 60 - 89 ml/min/1.73 m2; Stage 3 (Moderately decreased eGFR) = 30 - 59 ml/min/1.73 m2;
Stage 4 (Severely decreased eGFR) = 15 - 29 ml/min/1.73 m2 and Stage 5 (Kidney failure) = < 15 ml/min/1.73 m2.
Data analysis
The data was analyzed using SPSS® version 16 (SPSS Inc, Chicago Il.) computer software package. The frequencies and mean + standard deviation were generated. Student t-test was used to determine differences in means of numerical variable while chi-square test was used for categorical variables. However variables with non-parametric distributions were log transformed and Pearson correlation was carried out to determine association between CD4 T-cell count, eGFR and ACR. A p - value of < 0.05 was taken as statistically significant.
Results
Socio-demographic characteristics of the participants
Among four hundred and thirty eight individuals that participated in the study, three hundred and thirty five (335) individuals had complete and analyzable data. Of these 335 subjects, 227 were HIV-positive patients and 108 were age and sex-matched healthy control group.
There were 100 (44%) males and 127 (56%) females with M: F ratio of 0.8:1 among the cases, while the control group had 47 (43.5%) males and 61 (56.5%) females. The mean ages of the patients and controls were 40.3 ± 10.3 years and 41.8 ± 9.5 years respectively. There was no significant difference in the mean age, p = 0.19. Patients in the age group 30 - 39 years (35.7%) were mostly infected. Majority of the respondents among the cases 187 (82.4%) and the control individuals 92 (85.2%) were married. The proportion of the singles, divorced and separated were 11.9% versus 9.3%, 2.2% versus 1.9% and 1.3 versus 0.9% among the patients and control individuals respectively.
Among the HIV-positive subjects, common symptoms included leg swelling (8.4%), facial swelling (6.2%), oliguria (1.3%) and frothiness of urine (0.9%). Frequently observed signs include wasting (57.7%), pallor (33.5%), peri-orbital and pedal oedema in 4.4% and 3.1% respectively. More of the HIV-positive patients 75 (33%) had multiple sexual exposures compared to the HIV-negative controls 4 (3.7%) p = 0.01. All participants defined themselves as heterosexual and none admitted injecting drug use.
Family history of kidney disease was present in 2 (0.9%) and 1 (0.9%) of the patients and the control group respectively p = 0.97.
Those with family history of hypertension were 5 (2.2%) versus 11 (10.2%) p = 0.01, and diabetes 4 (1.8%) versus 6 (5.6%) p = 0.06, among the patients and the controls respectively. Common electrolyte abnormalities observed among the patients were hyponatraemia in 89 (39.2%) and hyperkalaemia in 10 (4.4%).
CKD was observed in 108 (47.6%) subjects among the patients and 18 (16.7%) of the controls p = 0.001. Table 1 shows that there was significant difference in the mean weight, body mass index (BMI), systolic and diastolic blood pressure among the HIV patients with and without CKD.
Effect of immunosuppression on the kidney
Table 2 revealed that 47.1% of the patients had CD4 T-cell count < 200 cells/µl. Between the HIV infected patients with and without CKD there was a significant difference in the mean value of CD4 + counts (p = 0.01) with a trend in patients with CKD toward having lower CD4 T-cell count and a greater proportion (57.4%) had CD4 T-cell count < 200 cells/µl.
The distributions of CKD among the cases (using their GFR) were as follows; majority, 108 (47.6%) were in stage 1, 82 (36.1%) were in stage 2 while 27 (11.9%) were in stage 3. Seven patients (3.1%) and 3 (1.3%) were in stages 4 and 5 respectively.
There was a statistically significant difference in the mean value of eGFR between patients with HIV, with and without CKD (80.3 ± 30.5 and 92.5 ± 21.1 ml/min/1.73m2 p = 0.001). As shown in table 2, there was a significant difference in the mean value of serum creatinine, ACR and eGFR among the patients with and without CKD.
Fifty (41.4%) of the HIV patients with CKD had 1 + or more of dipstick proteinuria, whereas about 58 (53.7%) had ACR equal or greater than 300mg/g. The median value and interquartile range (IQR) of ACR was 302.72 (303.85) mg/g and 250.00 (317.29) mg/g among the patients with and without CKD respectively. Figure 1 and 2 show that CD4 + counts correlated positively with eGFR (r = 0.463, p = 0.001) and negatively with ACR (r = -0.806, p = 0.001).
Discussion
Renal disease can complicate the course of HIV infection. The need for early screening for CKD and instituting prompt treatment may be beneficial in an attempt to protect the kidney from further disease progression. This becomes more instructive as effective treatment has been shown to alter the progression of HIV infection and its complications.
The mean age of the patients of 40.28 ± 10.26 years (with the most commonly affected age group of 30 - 39 years) was similar to the reports by Bah et al.2020 Bah AO, Kaba ML, Bah MLY, al. E. Renal complications associated with HIV/AIDS infections in Donka National Hospital, Conakry, Guinee. Trop J Nephrol 2007;2(2):89-91. and Agaba et al.44 Agaba EI, Agaba PA, Sirisena ND, Anteyi EA, Idoko JA. Renal disease in the acquired immunodeficiency syndrome in north central Nigeria. Niger J Med 2003;12:120-5. where the mean ages were 40.4 ± 9.6 years and 42.30 ± 11.31 years respectively. It was however higher than 34.6 ± 9.4 years reported by Emem et al.33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
in a study done in Ile Ife in the South-western part of the country. This age group is the peak period of sexual activity and economic productivity, thus a potential for decline in economic contributions which can impart negatively on the family and the society at large.
More females were observed than males in both cases and controls with male to female ratio of 0.8:1 and 0.7:1 respectively. This finding is similar to the study done by Wools-Kaloustian et al.2121 Wools-Kaloustian K, Gupta SK, Muloma E, Owino-Ong'or W, Sidle J, Aubrey RW, et al. Renal disease in an antiretroviral-naïve HIV-infected outpatient population in Western Kenya. Nephrol Dial Transplant 2007;22:2208-12. DOI: http://dx.doi.org/10.1093/ndt/gfm223
http://dx.doi.org/10.1093/ndt/gfm223...
in western Kenya who reported a male to female ratio of 0.5:1 respectively. The finding is also comparable to the report of Han et al.2222 Han TM, Naicker S, Ramdial PK, Assounga AG. A cross-sectional study of HIV-seropositive patients with varying degrees of proteinuria in South Africa. Kidney Int 2006;69:2243-50. PMID:16672914 DOI: http://dx.doi.org/10.1038/sj.ki.5000339
http://dx.doi.org/10.1038/sj.ki.5000339...
where females predominate among the patients with a male to female ratio of 0.3:1. However, Agaba et al.44 Agaba EI, Agaba PA, Sirisena ND, Anteyi EA, Idoko JA. Renal disease in the acquired immunodeficiency syndrome in north central Nigeria. Niger J Med 2003;12:120-5. in Jos, in the North central zone of Nigeria found a male preponderance of 60.5%, which is similar to report by Kwaifa and Bosan2323 Kwaifa SI, Bosan IB. Chronic Kidney disease in HIV infected patients in North Western Nigeria. Trop J Nephr 2008;3:23-8. in Zaria, North western part of Nigeria who documented the proportion of the male to be 58.5%. These differences observed may be due to the fact that the health seeking behavior varies within geographical regions and between sexes with females more likely to seek medical attention earlier than male. In the Northern parts of Nigeria, culture and religion may affect female presentation to the hospital.
The prevalence of chronic kidney disease among these newly diagnosed HIV-positive HAART naïve patients was found to be 47.6%. The prevalence obtained in this study is comparable to the figure reported by Agaba et al.44 Agaba EI, Agaba PA, Sirisena ND, Anteyi EA, Idoko JA. Renal disease in the acquired immunodeficiency syndrome in north central Nigeria. Niger J Med 2003;12:120-5. (51.8%) but the population studied were AIDS patients. The higher figures reported in their study could be a reflection of the advanced nature of patients immunosuppression as studies have shown that renal dysfunction become more pronounced with the progression of HIV disease.2424 Winston JA, Klotman ME, Klotman PE. HIV-associated nephropathy is a late, not early, manifestation of HIV-1 infection. Kidney Int 1999;55:1036-40.
http://dx.doi.org/10.1046/j.1523-1755.19...
The obtained prevalence in this study is also similar to the finding of Ijezie et al.2525 Ijezie IC, Efosa O, Agbaji O, Emmanuel IA, Idoko J, Onwuegbuzie G, et al. Glomerular filtration rate among HIV/AIDS patient at Jos University Teaching hospital Jos. J Med Trop 2010;12:26-29. (50%) in Jos Nigeria.
This value is higher than the figure obtained by Emem et al.33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
(38%), Szczech et al.99 Szczech LA, Gange SJ, van der Horst C, Bartlett JA, Young M, Cohen MH, et al. Predictors of proteinuria and renal failure among women with HIV infection. Kidney Int 2002;61:195-202. PMID: 11786101 DOI: http://dx.doi.org/10.1046/j.1523-1755.2002.00094.x
http://dx.doi.org/10.1046/j.1523-1755.20...
(32%), Janaby et al.2626 Janabi M Y, Chale S, Magao P, et al. Renal abnormalities associated with human immunodeficiency virus infection among police officers in Dar-es-Salaam, Tanzania. XIV International AIDS Conference; 2002 Jul 7-12. Barcelona, Spain. (28.4%) in Tanzania, and Fernando et al.2727 Fernando SK, Finkelstein FO, Moore BA, Weissman S. Prevalence of chronic kidney disease in an urban HIV infected population. Am J Med Sci 2008;335:89-94. DOI:http://dx.doi.org/10.1097/MAJ.0b013e31812e6b34
http://dx.doi.org/10.1097/MAJ.0b013e3181...
(24%). A South African study done between 2003 and 2004, reported a prevalence ranging from 6% to 27% among their patients population.2828 Gerntholtz TE, Goetsch SJ, Katz I. HIV-related nephropathy: a South African perspective. Kidney Int 2006;69:1885-91. PMID: 16625149 DOI: http://dx.doi.org/10.1038/sj.ki.5000351
http://dx.doi.org/10.1038/sj.ki.5000351...
This wide variation could be ascribed in part to differences in study design, the populations studied and the criteria used for the definitions of CKD. While some studies used dipstick proteinuria only2626 Janabi M Y, Chale S, Magao P, et al. Renal abnormalities associated with human immunodeficiency virus infection among police officers in Dar-es-Salaam, Tanzania. XIV International AIDS Conference; 2002 Jul 7-12. Barcelona, Spain. some quantified the amount of proteinuria33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
,2929 Emem CP, Arogundade FA, Sanusi AA. Prevalence of macro-proteinuria in HIV positive patients. Trop J Nephrol. 2006;1(1). and other researchers used serum creatinine as definition of CKD. In addition, very few studies described the histological pattern of kidney disease.33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
,55 Rao TK, Filippone EJ, Nicastri AD, Landesman SH, Frank E, Chen CK, et al. Associated focal and segmental glomerulosclerosis in the acquired immunodeficiency syndrome. N Engl J Med 1984;310:669-73. PMID: 6700641 DOI: http://dx.doi.org/10.1056/NEJM198403153101101
http://dx.doi.org/10.1056/NEJM1984031531...
,66 Pardo V, Aldana M, Colton RM, Fischl MA, Jaffe D, Moskowitz L, et al. Glomerular lesions in the acquired immunodeficiency syndrome. Ann Intern Med 1984;101:429-34. PMID: 6476632 DOI: http://dx.doi.org/10.7326/0003-4819-101-4-429
http://dx.doi.org/10.7326/0003-4819-101-...
,3030 D'Agati V, Appel GB. HIV infection and the kidney. J Am Soc Nephrol 1997;8:138-52.
The study showed that higher proportion of patients had normal or increased GFR. This is similar to the findings of Fernando et al.2727 Fernando SK, Finkelstein FO, Moore BA, Weissman S. Prevalence of chronic kidney disease in an urban HIV infected population. Am J Med Sci 2008;335:89-94. DOI:http://dx.doi.org/10.1097/MAJ.0b013e31812e6b34
http://dx.doi.org/10.1097/MAJ.0b013e3181...
where majority of their patients had stage 1 CKD. Agaba et al.44 Agaba EI, Agaba PA, Sirisena ND, Anteyi EA, Idoko JA. Renal disease in the acquired immunodeficiency syndrome in north central Nigeria. Niger J Med 2003;12:120-5. demonstrated that higher proportion of their patients had chronic renal insufficiency. Better awareness and early presentation of the patients may explain the higher proportion of early stage of CKD found in this study.
It was observed that 16.7% of the control group had CKD and 9.3% were found to have macro-albuminuria. The prevalence of impaired kidney function was estimated to range between 10% and 20% of the adult population in most countries worldwide.3131 Beaglehole R, Yach D. Globalisation and the prevention and control of non-communicable disease: the neglected chronic diseases of adults. Lancet 2003;362:903-8. PMID: 13678979 DOI:http://dx.doi.org/10.1016/S0140-6736(03)14335-8
http://dx.doi.org/10.1016/S0140-6736(03)...
A community screening conducted on healthy dwellers in South West Nigeria to assess the prevalence and pattern of chronic kidney disease by Oluyombo et al.3232 Oluyombo R, Ayodele OE, Akinwusi PO, Okunola OO, Akinsola A, Arogundade FA, et al. A community study of the prevalence, risk factors and pattern of chronic kidney disease in Osun State, South West Nigeria. West Afr J Med 2013;32:85-92. revealed that 18.8% of the 454 participants had evidence of CKD. Our study population was made up of black indigenous people from Nigeria. The predisposition of the black race to CKD has been reported by several authors. The absence of kidney registries in the country made it difficult to ascertain the true burden of CKD. However, the rising incidence of diabetes mellitus, hypertension, obesity and adoption of western lifestyle are some of the contributing factors which may explain the increasing prevalence of CKD among our populace.
Significant number of the patients (41.4%) had dipstick proteinuria of 1 + or more. Kwaifa et al.2323 Kwaifa SI, Bosan IB. Chronic Kidney disease in HIV infected patients in North Western Nigeria. Trop J Nephr 2008;3:23-8. observed the same degree of dipstick proteinuria in 40.9% of their patient population. Similarly, Emem et al.2929 Emem CP, Arogundade FA, Sanusi AA. Prevalence of macro-proteinuria in HIV positive patients. Trop J Nephrol. 2006;1(1). found a comparable figure of 46.7% in their study. Gupta et al.3333 Gupta SK, Mamlin BW, Johnson CS, Dollins MD, Topf JM, Dubé MP. Prevalence of proteinuria and the development of chronic kidney disease in HIV-infected patients. Clin Nephrol 2004;61:1-6. PMID: 14964451 DOI: http://dx.doi.org/10.5414/CNP61001
http://dx.doi.org/10.5414/CNP61001...
revealed that 29% of patients with HIV infection had dipstick proteinuria which was defined as > 1 +. A study involving 411 HIV-infected patients in Brazil showed that only 5.6% had persistent dipstick proteinuria.3434 Cavalcante MA, Coelho SN, Lacerda HR. Prevalence of persistent proteinuria in stable HIV/AIDS patients and its association with HIV nephropathy. Braz J Infect Dis 2007;11:456-61. DOI: http://dx.doi.org/10.1590/S1413-86702007000500003
http://dx.doi.org/10.1590/S1413-86702007...
Result from the Veterans' Affairs Connecticut Health Care System showed that 14% of HIV-infected, ambulatory patients had persistent dipstick proteinuria.3535 Crowley ST, Cantwell B, Abu-Alfa A, Rigsby MO. Prevalence of persistent asymptomatic proteinuria in HIV-infected outpatients and lack of correlation with viral load. Clin Nephrol 2001;55:1-6.
The high figure of dipstick proteinuria reported among the predominant black population can be attributed to the higher prevalence of HIVAN as earlier reported.
One hundred and one (44.5%) HIV-positive patients had microalbuminuria in this study. A comparable figure of 46.7% was observed by Emem et al.33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
Lower figures were documented by Kwaifa et al.2323 Kwaifa SI, Bosan IB. Chronic Kidney disease in HIV infected patients in North Western Nigeria. Trop J Nephr 2008;3:23-8. (33.1%) and Han et al.2222 Han TM, Naicker S, Ramdial PK, Assounga AG. A cross-sectional study of HIV-seropositive patients with varying degrees of proteinuria in South Africa. Kidney Int 2006;69:2243-50. PMID:16672914 DOI: http://dx.doi.org/10.1038/sj.ki.5000339
http://dx.doi.org/10.1038/sj.ki.5000339...
(36.0%) among their patients population, and a much lower values of 11% was documented in the Fat Redistribution and Metabolic Change in HIV Infection Study (FRAM). This variation appears to reflect the epidemiology of the disease with a worse outcome in the black population. Furthermore, the patients were all HAART naïve as compared to other studies in which some were already on the medications.
Recent reports have demonstrated that proteinuria is commonly found in HIV-infected patients.99 Szczech LA, Gange SJ, van der Horst C, Bartlett JA, Young M, Cohen MH, et al. Predictors of proteinuria and renal failure among women with HIV infection. Kidney Int 2002;61:195-202. PMID: 11786101 DOI: http://dx.doi.org/10.1046/j.1523-1755.2002.00094.x
http://dx.doi.org/10.1046/j.1523-1755.20...
,2929 Emem CP, Arogundade FA, Sanusi AA. Prevalence of macro-proteinuria in HIV positive patients. Trop J Nephrol. 2006;1(1).,3333 Gupta SK, Mamlin BW, Johnson CS, Dollins MD, Topf JM, Dubé MP. Prevalence of proteinuria and the development of chronic kidney disease in HIV-infected patients. Clin Nephrol 2004;61:1-6. PMID: 14964451 DOI: http://dx.doi.org/10.5414/CNP61001
http://dx.doi.org/10.5414/CNP61001...
The severity of proteinuria is predictive of CKD progression in the general population.3636 Zandi-Nejad K, Eddy AA, Glassock RJ, Brenner BM. Why is proteinuria an ominous biomarker of progressive kidney disease? Kidney Int Suppl 2004:S76-89. PMID: 15485426 DOI:http://dx.doi.org/10.1111/j.1523-1755.2004.09220.x
http://dx.doi.org/10.1111/j.1523-1755.20...
Proteinuria is associated with faster progression of HIV infection to AIDS and death.3737 Gardner LI, Holmberg SD, Williamson JM, Szczech LA, Carpenter CC, Rompalo AM, et al.; HIV Epidemiology Research Study Group. Development of proteinuria or elevated serum creatinine and mortality in HIV-infected women. J Acquir Immune Defic Syndr 2003;32:203-9. DOI:http://dx.doi.org/10.1097/00126334-200302010-00013
http://dx.doi.org/10.1097/00126334-20030...
,3838 Szczech LA, Hoover DR, Feldman JG, Cohen MH, Gange SJ, Goozé L, et al. Association between renal disease and outcomes among HIV-infected women receiving or not receiving antiretroviral therapy. Clin Infect Dis 2004;39:1199-206. PMID: 15486845 DOI:http://dx.doi.org/10.1086/424013
http://dx.doi.org/10.1086/424013...
Microalbuminuria has been shown to indicate endothelial stress and is predictive of enhanced cardiovascular risk.2626 Janabi M Y, Chale S, Magao P, et al. Renal abnormalities associated with human immunodeficiency virus infection among police officers in Dar-es-Salaam, Tanzania. XIV International AIDS Conference; 2002 Jul 7-12. Barcelona, Spain. Findings from HIV Epidemiology Research Study (HERS)3737 Gardner LI, Holmberg SD, Williamson JM, Szczech LA, Carpenter CC, Rompalo AM, et al.; HIV Epidemiology Research Study Group. Development of proteinuria or elevated serum creatinine and mortality in HIV-infected women. J Acquir Immune Defic Syndr 2003;32:203-9. DOI:http://dx.doi.org/10.1097/00126334-200302010-00013
http://dx.doi.org/10.1097/00126334-20030...
and Women's Interagency HIV Study (WIHS)3838 Szczech LA, Hoover DR, Feldman JG, Cohen MH, Gange SJ, Goozé L, et al. Association between renal disease and outcomes among HIV-infected women receiving or not receiving antiretroviral therapy. Clin Infect Dis 2004;39:1199-206. PMID: 15486845 DOI:http://dx.doi.org/10.1086/424013
http://dx.doi.org/10.1086/424013...
showed that the presence of proteinuria and elevated serum creatinine level were independently associated with increased risk of death among HIV-infected women.
Albumin-creatinine ratio has been shown to detect clinically significant level of proteinuria not detected by dipsticks urinalysis.3939 Siedner MJ, Atta MG, Lucas GM, Perazella MA, Fine DM. Poor validity of urine dipstick as a screening tool for proteinuria in HIV-positive patients. J Acquir Immune Defic Syndr 2008;47:261-3. DOI: http://dx.doi.org/10.1097/QAI.0b013e31815ac4ad
http://dx.doi.org/10.1097/QAI.0b013e3181...
In addition, ACR provides more accurate assessment of proteinuria and has been shown to correlate with 24 hour urinary protein excretion.4040 Price CP, Newall RG, Boyd JC. Use of protein: creatinine ratio measurements on random urine samples for prediction of significant proteinuria: a systematic review. Clin Chem 2005;51:1577-86. DOI: http://dx.doi.org/10.1373/clinchem.2005.049742
http://dx.doi.org/10.1373/clinchem.2005....
This study showed that 30.8% of the patient population had BMI < 18.5 kg/m22 Nigeria National Agency for the Control of AIDS. Abuja Nigeria GLOBAL AIDS RESPONSE; Country Progress Report Nigeria GARPR 2012 [Accessed Mar 15 2015]. Available from: http://www.unaids.org/sites/default/files/en/dataanalysis/knowyour-response/countryprogressreports/2012countries/Nigeria%202012%20GARPR%20Report%20Revised.pdf
http://www.unaids.org/sites/default/file...
and therefore fell into the malnourished group. Some earlier reports by Emem et al.33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
and D'Agatti et al.3030 D'Agati V, Appel GB. HIV infection and the kidney. J Am Soc Nephrol 1997;8:138-52. found that more than 50% of their subjects had BMI < 19 kg/m22 Nigeria National Agency for the Control of AIDS. Abuja Nigeria GLOBAL AIDS RESPONSE; Country Progress Report Nigeria GARPR 2012 [Accessed Mar 15 2015]. Available from: http://www.unaids.org/sites/default/files/en/dataanalysis/knowyour-response/countryprogressreports/2012countries/Nigeria%202012%20GARPR%20Report%20Revised.pdf
http://www.unaids.org/sites/default/file...
. Kwaifa et al.2323 Kwaifa SI, Bosan IB. Chronic Kidney disease in HIV infected patients in North Western Nigeria. Trop J Nephr 2008;3:23-8. however documented a much lower value of 10.2%. These disparities may be as a result of differences in patient selection methods since some of these studies involved patients on antiretroviral (ARV) drugs which might have improved their nutrition status. The malnutrition may be due to impaired oral intake, malabsorption, and wasting syndromes that typify the disease.
The mean systolic and diastolic blood pressures were found to be lower in our patients though comparable to the findings of Agaba et al.44 Agaba EI, Agaba PA, Sirisena ND, Anteyi EA, Idoko JA. Renal disease in the acquired immunodeficiency syndrome in north central Nigeria. Niger J Med 2003;12:120-5. This is probably reflecting the characteristic salt losing nephropathy which is associated with HIV patients.
In this study anemia was prevalent and worse among patients with CKD and low CD4 + counts. This has been reported by earlier studies33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
,2323 Kwaifa SI, Bosan IB. Chronic Kidney disease in HIV infected patients in North Western Nigeria. Trop J Nephr 2008;3:23-8. and suggests the impact of advanced nature of the infection. Anaemia in patients with HIV/AIDS has been shown to vary depending on the stage of the disease, CD4 + counts and level of renal function.2323 Kwaifa SI, Bosan IB. Chronic Kidney disease in HIV infected patients in North Western Nigeria. Trop J Nephr 2008;3:23-8.
Electrolyte abnormalities found in this study were hyponatraemia and hyperkalaemia with a prevalence of 39.2% and 4.4% respectively. This is in agreement with previous reports which showed changes in the serum sodium and potassium including bicarbonates.33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
,44 Agaba EI, Agaba PA, Sirisena ND, Anteyi EA, Idoko JA. Renal disease in the acquired immunodeficiency syndrome in north central Nigeria. Niger J Med 2003;12:120-5.,2323 Kwaifa SI, Bosan IB. Chronic Kidney disease in HIV infected patients in North Western Nigeria. Trop J Nephr 2008;3:23-8. Agaba et al.44 Agaba EI, Agaba PA, Sirisena ND, Anteyi EA, Idoko JA. Renal disease in the acquired immunodeficiency syndrome in north central Nigeria. Niger J Med 2003;12:120-5. showed significantly lower concentrations of serum sodium and bicarbonate among their subjects. This was attributed to the possibilities of inappropriate secretion of antidiuretic hormone and adrenal insufficiency which was reported to be present in about 70% of patients with co-infection of HIV and pulmonary tuberculosis. Other possible causes of electrolyte abnormalities include renal tubular dysfunction, volume depletion, poor intake and use of nephrotoxic drugs.33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
This study demonstrated a linear relationship between the degree of immunosuppression (as measured by CD4 + counts) and the stage of CKD. This is in agreement with previous works.2424 Winston JA, Klotman ME, Klotman PE. HIV-associated nephropathy is a late, not early, manifestation of HIV-1 infection. Kidney Int 1999;55:1036-40.
http://dx.doi.org/10.1046/j.1523-1755.19...
It also showed that HIV patients with CKD had low CD4 T-cell count of < 200 cells/µl similar to previous reports.33 Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
http://dx.doi.org/10.1093/ndt/gfm836...
,99 Szczech LA, Gange SJ, van der Horst C, Bartlett JA, Young M, Cohen MH, et al. Predictors of proteinuria and renal failure among women with HIV infection. Kidney Int 2002;61:195-202. PMID: 11786101 DOI: http://dx.doi.org/10.1046/j.1523-1755.2002.00094.x
http://dx.doi.org/10.1046/j.1523-1755.20...
,2222 Han TM, Naicker S, Ramdial PK, Assounga AG. A cross-sectional study of HIV-seropositive patients with varying degrees of proteinuria in South Africa. Kidney Int 2006;69:2243-50. PMID:16672914 DOI: http://dx.doi.org/10.1038/sj.ki.5000339
http://dx.doi.org/10.1038/sj.ki.5000339...
23 Kwaifa SI, Bosan IB. Chronic Kidney disease in HIV infected patients in North Western Nigeria. Trop J Nephr 2008;3:23-8.-2424 Winston JA, Klotman ME, Klotman PE. HIV-associated nephropathy is a late, not early, manifestation of HIV-1 infection. Kidney Int 1999;55:1036-40.
http://dx.doi.org/10.1046/j.1523-1755.19...
We acknowledge several limitations including the cross-sectional design of the study with a single measurement of serum creatinine and albumin creatinine ratio which may not be a true representation of the obtained CKD prevalence rate. However the combination of the eGFR and/or ACR in definition of CKD is an attempt to reduce potential for misclassification bias in estimating renal function and determining the prevalence. The MDRD equation was used with the aim of improving the prediction of GFR from the plasma creatinine concentration. Though to our knowledge MDRD equation has not been validated in people with HIV in this region.
It is of note that use of serum creatinine in estimating GFR can be affected by muscle wasting, diet and medications which are often present in this group of patient.
Conclusions
The results of this study showed that HIV infected adults have more renal associated abnormalities than controls. In sub-Saharan Africa, where the burden of HIV infection is high and the dearth of resources for kidney care is profound, the high prevalence of CKD in HIV-infected patients documented in this study warrants early detection of kidney involvement in these patients and the need to institute measures that may halt or delay progression to end-stage kidney disease. In addition, incorporation of renal assessment as component of evaluation of patients with HIV/AIDS is suggested as some drugs used in the treatment of HIV/AIDS infection do affect the kidneys and could accelerate undiagnosed kidney disease in these patients.
Erratum
-
In the article “Prevalence of Chronic Kidney Disease in newly diagnosed patients with Human immunodeficiency virus in Ilorin, Nigeria”, published in Jornal Brasileiro de Nefrologia 2015;37:177-84, page 177, which reads: Dada Samuel Ayokunle, Olanrewaju Timothy Olusegun, Aderibigbe Ademola, Chijioke Adindu, Rafiu Mojeed Olaitan, Ajayi Akande Oladimeji should be read as: Samuel Ayokunle Dada, Timothy Olusegun Olanrewaju, Ademola Aderibigbe, Adindu Chijioke, Mojeed Olaitan Rafiu, Akande Oladimeji Ajayi.
REFERÊNCIAS
-
1AIDS Epidemic Update December 2007 [Accessed Mar 15 2015]. Available from: http://data.unaids.org/pub/EPISlides/2007/2007_epiupdate_en.pdf
» http://data.unaids.org/pub/EPISlides/2007/2007_epiupdate_en.pdf -
2Nigeria National Agency for the Control of AIDS. Abuja Nigeria GLOBAL AIDS RESPONSE; Country Progress Report Nigeria GARPR 2012 [Accessed Mar 15 2015]. Available from: http://www.unaids.org/sites/default/files/en/dataanalysis/knowyour-response/countryprogressreports/2012countries/Nigeria%202012%20GARPR%20Report%20Revised.pdf
» http://www.unaids.org/sites/default/files/en/dataanalysis/knowyour-response/countryprogressreports/2012countries/Nigeria%202012%20GARPR%20Report%20Revised.pdf -
3Emem CP, Arogundade F, Sanusi A, Adelusola K, Wokoma F, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant 2008;23:741-6. DOI: http://dx.doi.org/10.1093/ndt/gfm836
» http://dx.doi.org/10.1093/ndt/gfm836 -
4Agaba EI, Agaba PA, Sirisena ND, Anteyi EA, Idoko JA. Renal disease in the acquired immunodeficiency syndrome in north central Nigeria. Niger J Med 2003;12:120-5.
-
5Rao TK, Filippone EJ, Nicastri AD, Landesman SH, Frank E, Chen CK, et al. Associated focal and segmental glomerulosclerosis in the acquired immunodeficiency syndrome. N Engl J Med 1984;310:669-73. PMID: 6700641 DOI: http://dx.doi.org/10.1056/NEJM198403153101101
» http://dx.doi.org/10.1056/NEJM198403153101101 -
6Pardo V, Aldana M, Colton RM, Fischl MA, Jaffe D, Moskowitz L, et al. Glomerular lesions in the acquired immunodeficiency syndrome. Ann Intern Med 1984;101:429-34. PMID: 6476632 DOI: http://dx.doi.org/10.7326/0003-4819-101-4-429
» http://dx.doi.org/10.7326/0003-4819-101-4-429 -
7D'Agati V, Appel GB. Renal pathology of human immunodeficiency virus infection. Semin Nephrol 1998;18:406-21. PMID: 9692353
-
8Okpechi I, Swanepoel C, Duffield M, Mahala B, Wearne N, Alagbe S, et al. Patterns of renal disease in Cape Town South Africa: a 10-year review of a single-centre renal biopsy database. Nephrol Dial Transplant 2011;26:1853-61. DOI: http://dx.doi.org/10.1093/ndt/gfq655
» http://dx.doi.org/10.1093/ndt/gfq655 -
9Szczech LA, Gange SJ, van der Horst C, Bartlett JA, Young M, Cohen MH, et al. Predictors of proteinuria and renal failure among women with HIV infection. Kidney Int 2002;61:195-202. PMID: 11786101 DOI: http://dx.doi.org/10.1046/j.1523-1755.2002.00094.x
» http://dx.doi.org/10.1046/j.1523-1755.2002.00094.x -
10Naicker S, Fabian J. Risk factors for the development of chronic kidney disease with HIV/AIDS. Clin Nephrol 2010;74:S51-56.
-
11Okafor UH, Unuigbe EI, Ojogwu LI, Oviasu E, Wokoma FS. Renal disease in HIV infected patients at University of Benin Teaching Hospital in Nigeria. Afr Health Sci 2011;11:S28-33. DOI:http://dx.doi.org/10.4314/ahs.v11i3.70067
» http://dx.doi.org/10.4314/ahs.v11i3.70067 -
12Avila-Casado C, Fortoul TI, Chugh SS. HIV-associated nephropathy: experimental models. Contrib Nephrol 2011;169:270-85. PMID: 21252526
-
13Discover Nigeria Facts about Nigeria Kwara State (State of Harmony) [Accessed Jul 27 2014]. Available from: http://zodml.org/Nigeria/Geography/Kwara%20State/
» http://zodml.org/Nigeria/Geography/Kwara%20State/ -
14Greenwald I. The chemistry of Jaffe's reaction for creatinine: V. The isolation of the red coumpound. J Biol Chem 1928;80:103-6.
-
15Marsh WH, Fingerhut B, Miller H. Automated and manual direct methods for the determination of blood urea. Clin Chem 1965;11:624-7.
-
16Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 1999;130:461-70. DOI:http://dx.doi.org/10.7326/0003-4819-130-6-199903160-00002
» http://dx.doi.org/10.7326/0003-4819-130-6-199903160-00002 -
17Trinde P. Determination of blood glucose using glucose oxidase with an alternative oxygen acceptor. Ann Clin Biochem 1969;6:24-27.
-
18Lydakis C, Lip GY. Microalbuminuria and cardiovascular risk. QJM 1998;91:381-91. DOI:http://dx.doi.org/10.1093/qjmed/91.6.381
» http://dx.doi.org/10.1093/qjmed/91.6.381 -
19National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 2002;39:S1-266.
-
20Bah AO, Kaba ML, Bah MLY, al. E. Renal complications associated with HIV/AIDS infections in Donka National Hospital, Conakry, Guinee. Trop J Nephrol 2007;2(2):89-91.
-
21Wools-Kaloustian K, Gupta SK, Muloma E, Owino-Ong'or W, Sidle J, Aubrey RW, et al. Renal disease in an antiretroviral-naïve HIV-infected outpatient population in Western Kenya. Nephrol Dial Transplant 2007;22:2208-12. DOI: http://dx.doi.org/10.1093/ndt/gfm223
» http://dx.doi.org/10.1093/ndt/gfm223 -
22Han TM, Naicker S, Ramdial PK, Assounga AG. A cross-sectional study of HIV-seropositive patients with varying degrees of proteinuria in South Africa. Kidney Int 2006;69:2243-50. PMID:16672914 DOI: http://dx.doi.org/10.1038/sj.ki.5000339
» http://dx.doi.org/10.1038/sj.ki.5000339 -
23Kwaifa SI, Bosan IB. Chronic Kidney disease in HIV infected patients in North Western Nigeria. Trop J Nephr 2008;3:23-8.
-
24Winston JA, Klotman ME, Klotman PE. HIV-associated nephropathy is a late, not early, manifestation of HIV-1 infection. Kidney Int 1999;55:1036-40.
» http://dx.doi.org/10.1046/j.1523-1755.1999.0550031036.x -
25Ijezie IC, Efosa O, Agbaji O, Emmanuel IA, Idoko J, Onwuegbuzie G, et al. Glomerular filtration rate among HIV/AIDS patient at Jos University Teaching hospital Jos. J Med Trop 2010;12:26-29.
-
26Janabi M Y, Chale S, Magao P, et al. Renal abnormalities associated with human immunodeficiency virus infection among police officers in Dar-es-Salaam, Tanzania. XIV International AIDS Conference; 2002 Jul 7-12. Barcelona, Spain.
-
27Fernando SK, Finkelstein FO, Moore BA, Weissman S. Prevalence of chronic kidney disease in an urban HIV infected population. Am J Med Sci 2008;335:89-94. DOI:http://dx.doi.org/10.1097/MAJ.0b013e31812e6b34
» http://dx.doi.org/10.1097/MAJ.0b013e31812e6b34 -
28Gerntholtz TE, Goetsch SJ, Katz I. HIV-related nephropathy: a South African perspective. Kidney Int 2006;69:1885-91. PMID: 16625149 DOI: http://dx.doi.org/10.1038/sj.ki.5000351
» http://dx.doi.org/10.1038/sj.ki.5000351 -
29Emem CP, Arogundade FA, Sanusi AA. Prevalence of macro-proteinuria in HIV positive patients. Trop J Nephrol. 2006;1(1).
-
30D'Agati V, Appel GB. HIV infection and the kidney. J Am Soc Nephrol 1997;8:138-52.
-
31Beaglehole R, Yach D. Globalisation and the prevention and control of non-communicable disease: the neglected chronic diseases of adults. Lancet 2003;362:903-8. PMID: 13678979 DOI:http://dx.doi.org/10.1016/S0140-6736(03)14335-8
» http://dx.doi.org/10.1016/S0140-6736(03)14335-8 -
32Oluyombo R, Ayodele OE, Akinwusi PO, Okunola OO, Akinsola A, Arogundade FA, et al. A community study of the prevalence, risk factors and pattern of chronic kidney disease in Osun State, South West Nigeria. West Afr J Med 2013;32:85-92.
-
33Gupta SK, Mamlin BW, Johnson CS, Dollins MD, Topf JM, Dubé MP. Prevalence of proteinuria and the development of chronic kidney disease in HIV-infected patients. Clin Nephrol 2004;61:1-6. PMID: 14964451 DOI: http://dx.doi.org/10.5414/CNP61001
» http://dx.doi.org/10.5414/CNP61001 -
34Cavalcante MA, Coelho SN, Lacerda HR. Prevalence of persistent proteinuria in stable HIV/AIDS patients and its association with HIV nephropathy. Braz J Infect Dis 2007;11:456-61. DOI: http://dx.doi.org/10.1590/S1413-86702007000500003
» http://dx.doi.org/10.1590/S1413-86702007000500003 -
35Crowley ST, Cantwell B, Abu-Alfa A, Rigsby MO. Prevalence of persistent asymptomatic proteinuria in HIV-infected outpatients and lack of correlation with viral load. Clin Nephrol 2001;55:1-6.
-
36Zandi-Nejad K, Eddy AA, Glassock RJ, Brenner BM. Why is proteinuria an ominous biomarker of progressive kidney disease? Kidney Int Suppl 2004:S76-89. PMID: 15485426 DOI:http://dx.doi.org/10.1111/j.1523-1755.2004.09220.x
» http://dx.doi.org/10.1111/j.1523-1755.2004.09220.x -
37Gardner LI, Holmberg SD, Williamson JM, Szczech LA, Carpenter CC, Rompalo AM, et al.; HIV Epidemiology Research Study Group. Development of proteinuria or elevated serum creatinine and mortality in HIV-infected women. J Acquir Immune Defic Syndr 2003;32:203-9. DOI:http://dx.doi.org/10.1097/00126334-200302010-00013
» http://dx.doi.org/10.1097/00126334-200302010-00013 -
38Szczech LA, Hoover DR, Feldman JG, Cohen MH, Gange SJ, Goozé L, et al. Association between renal disease and outcomes among HIV-infected women receiving or not receiving antiretroviral therapy. Clin Infect Dis 2004;39:1199-206. PMID: 15486845 DOI:http://dx.doi.org/10.1086/424013
» http://dx.doi.org/10.1086/424013 -
39Siedner MJ, Atta MG, Lucas GM, Perazella MA, Fine DM. Poor validity of urine dipstick as a screening tool for proteinuria in HIV-positive patients. J Acquir Immune Defic Syndr 2008;47:261-3. DOI: http://dx.doi.org/10.1097/QAI.0b013e31815ac4ad
» http://dx.doi.org/10.1097/QAI.0b013e31815ac4ad -
40Price CP, Newall RG, Boyd JC. Use of protein: creatinine ratio measurements on random urine samples for prediction of significant proteinuria: a systematic review. Clin Chem 2005;51:1577-86. DOI: http://dx.doi.org/10.1373/clinchem.2005.049742
» http://dx.doi.org/10.1373/clinchem.2005.049742
Publication Dates
-
Publication in this collection
Apr-Jun 2015
History
-
Received
23 Oct 2014 -
Accepted
06 Feb 2015