Abstracts
The objective of this study was to assess the prevalence and characteristics of oral lesions and oral self-examination and the association between these variables and life course determinants in a young population. A representative sample (n = 720) of all births occurring in Pelotas, Rio Grande do Sul State, Brazil, in 1982, was investigated and the outcomes were assessed in 2006. Data regarding exploratory variables was collected from other cohort waves. The prevalence of oral lesions was 23.3% (95%CI: 20.3-26.6). A total of 31% of individuals (95%CI: 27.6-34.4) reported never having performed oral self-examination. Multivariable analysis showed that low socio-economic status at birth, lack of oral hygiene instruction from a dentist up to the age of 15 years and smoking habits at the age of 22 year were associated with the presence of oral lesions. Performing oral self-examination was associated with high levels of maternal schooling at birth and having received oral hygiene orientation from a dentist up to the age of 15 years. Socioeconomic and behavioral factors are associated with both presence of oral mucosal lesions and the habit of performing self-examination.
Mouth Diseases; Mouth Mucosa; Self-Examination
El objetivo fue determinar la prevalencia y características de lesiones bucales, autoexamen bucal, y sus asociaciones con determinantes a lo largo de la vida, en una población de adultos jóvenes. Fue investigada una muestra representativa (n = 720) de los nacidos en Pelotas, Río Grande do Sul, Brasil, 1982, y la presencia de lesiones bucales y realización del autoexamen fueron verificadas a los 24 años. Las variables independientes se obtuvieron de otros seguimientos de esta cohorte. La prevalencia de lesiones bucales fue de un 23,3% (IC95%: 20,3-26,6) y un 31% de los individuos (IC95%: 27,6-34,4) relató no haber realizado nunca el autoexamen de la boca. El análisis multivariable mostró que el bajo nivel socioeconómico en el momento del nacimiento, el no haber recibido instrucción de higiene oral hasta los 15 años de edad, y fumar a los 22 años, se asociaron a la presencia de lesiones. La realización del autoexamen bucal se asoció a una mayor escolaridad materna en el nacimiento y al haber recibido orientación de higiene bucal por el dentista a los 15 años. Factores socioeconómicos y de comportamiento están asociados, tanto la presencia de lesiones bucales, como a la realización del autoexamen bucal.
Enfermedades de la Boca; Mucosa Bucal; Autoexamen
O objetivo foi determinar a prevalência e características de lesões bucais, autoexame bucal e suas associações com determinantes ao longo da vida em uma população de adultos jovens. Uma amostra representativa (n = 720) dos nascidos em Pelotas, Rio Grande do Sul, Brasil, em 1982, foi investigada, e a presença de lesões bucais e a realização do autoexame, verificadas aos 24 anos. As variáveis independentes foram obtidas de outros seguimentos dessa coorte. A prevalência de lesões bucais foi de 23,3% (IC95%: 20,3-26,6), e 31% dos indivíduos (IC95%: 27,6-34,4) relataram nunca ter realizado o autoexame da boca. A análise multivariável mostrou que o baixo nível socioeconômico ao nascimento, não ter recebido instrução de higiene oral até os 15 anos de idade e fumar aos 22 anos foram associados à presença de lesões. A realização do autoexame bucal esteve associada à maior escolaridade materna ao nascimento e a ter recebido orientação de higiene bucal pelo dentista aos 15 anos. Fatores socioeconômicos e comportamentais estão associados tanto à presença de lesões bucais quanto à realização do autoexame bucal.
Doenças da Boca; Mucosa Bucal; Auto-Exame
ARTICLE ARTIGO
Factors associated with prevalence of oral lesions and oral self-examination in young adults from a birth cohort in Southern Brazil
Fatores associados à prevalência de lesões bucais e à realização do autoexame bucal em adultos jovens de uma coorte de nascidos vivos do Sul do Brasil
Factores asociados a la prevalencia de lesiones bucales y a la realización del autoexamen bucal en adultos jóvenes de una cohorte de nacidos vivos del sur de Brasil
Sandra Beatriz Chaves TarquinioI; Luisa Jardim Correa de OliveiraI; Marcos Britto CorreaI; Marco Aurélio PeresII; Karen Glazer PeresII; Denise Petrucci GiganteIII; Bernardo Lessa HortaIII; Flávio Fernando DemarcoIII
IPrograma de Pós-graduação em Odontologia, Universidade Federal de Pelotas, Pelotas, Brasil
IICentro de Ciências da Saúde, Universidade Federal de Santa Catarina, Florianópolis, Brasil
IIIPrograma de Pós-graduação em Epidemiologia, Universidade Federal de Pelotas, Pelotas, Brasil
Correspondence Correspondence: S. B. C. Tarquinio Programa de Pós-graduação em Odontologia, Universidade Federal de Pelotas. Rua Gonçalves Chaves 467, 5 o andar, Pelotas, RS 96015-560, Brasil. sbtarquinio@gmail.com
ABSTRACT
The objective of this study was to assess the prevalence and characteristics of oral lesions and oral self-examination and the association between these variables and life course determinants in a young population. A representative sample (n = 720) of all births occurring in Pelotas, Rio Grande do Sul State, Brazil, in 1982, was investigated and the outcomes were assessed in 2006. Data regarding exploratory variables was collected from other cohort waves. The prevalence of oral lesions was 23.3% (95%CI: 20.3-26.6). A total of 31% of individuals (95%CI: 27.6-34.4) reported never having performed oral self-examination. Multivariable analysis showed that low socio-economic status at birth, lack of oral hygiene instruction from a dentist up to the age of 15 years and smoking habits at the age of 22 year were associated with the presence of oral lesions. Performing oral self-examination was associated with high levels of maternal schooling at birth and having received oral hygiene orientation from a dentist up to the age of 15 years. Socioeconomic and behavioral factors are associated with both presence of oral mucosal lesions and the habit of performing self-examination.
Mouth Diseases; Mouth Mucosa; Self-Examination
RESUMO
O objetivo foi determinar a prevalência e características de lesões bucais, autoexame bucal e suas associações com determinantes ao longo da vida em uma população de adultos jovens. Uma amostra representativa (n = 720) dos nascidos em Pelotas, Rio Grande do Sul, Brasil, em 1982, foi investigada, e a presença de lesões bucais e a realização do autoexame, verificadas aos 24 anos. As variáveis independentes foram obtidas de outros seguimentos dessa coorte. A prevalência de lesões bucais foi de 23,3% (IC95%: 20,3-26,6), e 31% dos indivíduos (IC95%: 27,6-34,4) relataram nunca ter realizado o autoexame da boca. A análise multivariável mostrou que o baixo nível socioeconômico ao nascimento, não ter recebido instrução de higiene oral até os 15 anos de idade e fumar aos 22 anos foram associados à presença de lesões. A realização do autoexame bucal esteve associada à maior escolaridade materna ao nascimento e a ter recebido orientação de higiene bucal pelo dentista aos 15 anos. Fatores socioeconômicos e comportamentais estão associados tanto à presença de lesões bucais quanto à realização do autoexame bucal.
Doenças da Boca; Mucosa Bucal; Auto-Exame
RESUMEN
El objetivo fue determinar la prevalencia y características de lesiones bucales, autoexamen bucal, y sus asociaciones con determinantes a lo largo de la vida, en una población de adultos jóvenes. Fue investigada una muestra representativa (n = 720) de los nacidos en Pelotas, Río Grande do Sul, Brasil, 1982, y la presencia de lesiones bucales y realización del autoexamen fueron verificadas a los 24 años. Las variables independientes se obtuvieron de otros seguimientos de esta cohorte. La prevalencia de lesiones bucales fue de un 23,3% (IC95%: 20,3-26,6) y un 31% de los individuos (IC95%: 27,6-34,4) relató no haber realizado nunca el autoexamen de la boca. El análisis multivariable mostró que el bajo nivel socioeconómico en el momento del nacimiento, el no haber recibido instrucción de higiene oral hasta los 15 años de edad, y fumar a los 22 años, se asociaron a la presencia de lesiones. La realización del autoexamen bucal se asoció a una mayor escolaridad materna en el nacimiento y al haber recibido orientación de higiene bucal por el dentista a los 15 años. Factores socioeconómicos y de comportamiento están asociados, tanto la presencia de lesiones bucales, como a la realización del autoexamen bucal.
Enfermedades de la Boca; Mucosa Bucal; Autoexamen
Introduction
Disorders affecting the soft tissues, salivary glands and superficial mucosa are common oral health problems, inciting several symptoms, such as pain, halitosis, xerostomia and oral dysesthesia, which can impair oral functions 1. These conditions can affect an individuals' quality of life by impair mastication, swallowing and speech processes, may affect daily social activities, and can lead to psychological problems 2.
An understanding of the epidemiological aspects, etiology, natural history and risk factors related to oral mucosal pathologies is essential for primary prevention, early diagnosis and prompt treatment of these diseases 3,4. Estimates of prevalence of oral lesions worldwide are highly heterogeneous, ranging from 15% in the Gizan area of Saudi Arabia 5 to 51.1% in Spain 6. Pindborg 4 states that when focusing on the epidemiologic aspects of oral mucosal diseases, researchers should consider the tremendous variety of lesions that characterize this group of pathologies, ranging from excessively rare conditions to very common diseases, and from malignant tumors to the most harmless alterations.
Certain oral disorders have received greater research attention due to their high prevalence in the general population or because of the high risk of death associated with the disease 4. Therefore, lesions such as leukoplakias and erythroplakias (red and white patches, respectively, which are diagnosed by a process of exclusion) have been exhaustively referred to as precancerous lesions 5, due to their prevalence in people who later develop oral cancers 4,7. It is known that oral squamous cell carcinomas generally occur in older men (from the age of 45 to 50 years) with a history of smoking and/or alcohol abuse. Although these carcinomas are less prevalent in young individuals (under the age of 40 years), the incidence of oral tongue squamous cell carcinomas in this particular group has steadily increased since 1973 8. Young patients with oral squamous cell carcinomas and a history of predisposition to cancer may thus have a greater predisposition to this disease than their older counterparts, because they appear to develop the disease despite a shorter exposure time to carcinogenic substances 9.
The majority of the studies about the prevalence of oral lesions are carried out using data from specialized oral health services and limitations exist in comparing this data with information on prevalence of lesions from population-based studies. Furthermore, few population-based studies have been carried out on young adults. In this respect, prospective birth cohort studies allow for the collection of more reliable data about exposure and outcomes over the long-term, which is difficult to investigate using other research approaches 10.
With respect to the detection of these lesions, oral self-examination improves the chances of early diagnosis 11; however, population studies have yet to investigate the prevalence of oral self-examination and the factors associated with its usage.
The aim of this study was to investigate the prevalence and characteristics of oral lesions in young adults who have been continuously followed up since birth. Additionally, the study evaluated the prevalence of self-examination and associations between these variables and demographic, socioeconomic and behavioral variables.
Materials and methods
This is a cross-sectional study nested in a birth cohort. In 1982, all infants born at three maternity hospitals in Pelotas, Rio Grande do Sul State, Brazil, were identified. The 5,914 liveborn infants and their mothers were weighed and measured and the mothers were interviewed shortly after delivery. This population has been followed up several times since then, making this cohort one of the largest and longest-running birth cohorts in the developing world 10. The initial focus of this study was perinatal, infant and early childhood morbidity and mortality. By mid-childhood, the emphasis of the study shifted to childcare, utilization of health services, selected morbidity indicators and child development 10. In 1997, when the members of the cohort had reached adolescence (mean age 15 years), a systematic sample of 70 census tracts of the city (27% of the total) was selected and every household in these tracts was visited. A total of 1,076 cohort members were interviewed during these visits, of which 900 were randomly selected for the Oral Health Study (OHS-97). The latter study consisted of dental examinations to evaluate the presence of dental caries and malocclusion and interviews to obtain information about oral hygiene habits and utilization of dental services in the adolescents.
In 2006 (OHS-06), an attempt was made to follow up the 888 adolescents (98.7%) evaluated under the OHS-97. Subjects were interviewed and examined to evaluate several oral health conditions, including dental caries, periodontal status and soft tissue oral lesions.
The main outcomes evaluated relating to the oral lesions were the type of alteration, site, size, duration and associated symptoms. More than one lesion, each with distinct characteristics, was possible in each person.
Lesions were classified by type according to Hipólito & Martins 12 and Neville et al. 1. Pigmented lesions were defined as displaying a color change in the oral mucosa, such as red, purple, brown, or black staining. The terms papule and nodule were defined as superficial or deep solid and circumscribed elevations of the mucosa. Lesions were classified as white plaques when an elevation of oral mucosa was observed, whose height was lower than its length. Vesicles and blisters were defined as a circumscribed elevation of the oral mucosa containing liquid material. A lesion was categorized as erosion when partial epithelial loss was observed without exposure of the connective tissue. Oral ulcers were defined as open sores inside the mouth.
Some lesions, such as petechiaes, which were obviously caused by tooth brushing or bite trauma, were excluded from the study, due to their high frequency and low relevance in terms of oral health. The developmental defects of the oral maxillofacial region (commissural lip pits, paramedian lip pits, double lip, Fordyce granules, leukoedema, microglossia, macroglossia, ankyloglossia, lingual thyroid, fissured tongue, geographic tongue, hairy tongue, varicosities, lateral soft palate fistulas, exostoses, torus palatinus, and torus mandibularis) were also excluded from the evaluation, as our study relied on the type of lesions and not on the diagnosis. Moreover, the inclusion of this group of alterations, the majority of which do not require any treatment, would lead to an overestimate of the prevalence of oral lesions in a young adult population. For the purpose of analysis, plaques, erosions and pigmented lesions were grouped into a new category classified as potentially malignant oral lesions.
Each lesion was measured with a flexible plastic ruler and categorized according to the following sizes: (1) 5mm or less; (2) 6-10mm; (3) 11-20mm; (4) 21-40mm; (5) greater than 40mm. An individual's perception of the lesion was evaluated using the question, "Had you ever perceived this injury in your mouth?". To assess the existence of symptoms, the question, "Do you relate any of these symptoms to this lesion?" was asked, with the following options: (1) pain; (2) burning sensation; (3) itching; and (4) discomfort. In addition, people were asked if they were used to performing oral self-examinations.
The exploratory variables used in this study were obtained from the different cohort waves. Self-reported skin color was classified in terms of white (Caucasians and people of Asiatic descent), lighter-skinned black people (pardos), and dark-skinned black people (pretos). Level of maternal schooling was categorized into four groups with respect to the number of completed years of study when the cohort member was born: ≥ 12; 9-11; 5-8; and ≤ 4 years. Data regarding family income was collected in 1982 using five categories based on the number of minimum wages (< 1; 1-3; 3; 1-6; 6; 1-10; and > 10). Unfortunately, information on the continuous variable of income was not available. To classify families into tertiles for data analyses, it was necessary to regroup the five categories. A principal component analysis was carried out using four variables in our sample strongly related to income mode of delivery care payment (out-of-pocket, free public health insurance, or private health insurance), schooling, height, and mother's skin color. Each group did not contain exactly the same number of individuals due to ties in the derived score. Information on receipt of oral hygiene instructions from a dentist, obtained through the question, "Have you ever received oral hygiene instructions from a dentist?", was collected when the subject was 15 years of age. Information regarding smoking habits was collected when the subject was 22 years of age through the question, "Have you ever smoked on a daily basis?".
The fieldwork team comprised of six dentists and four final year dental students from the Federal University of Pelotas (UFPel, acronym in Portuguese). All examinations were performed at the individual's home. Patients were examined sitting under artificial illumination (a head lamp). The examiners were properly dressed, and all safety and biohazard measures were adopted. To examine the oral mucosa, examiners used wooden spatulas and buccal mirrors. Prior to the examination, the mucosa was dried with gauzes. All examiners and interviewers were trained and calibrated by an experienced oral pathologist, and inter-examiner reliabilities were calculated using weighted and simple kappa tests when appropriate. The lowest kappa value for oral lesions was 0.60. To ensure data quality, 10% of the interviews were repeated with a short version of the questionnaire, allowing for concordance-level calculation.
The software Stata version 9.0 (Stata Corp., College Station, USA) was used for the analysis. Associations between independent variables and self-examination were determined using the chi square test and chi square test for linear trend when appropriate. Poisson regression with robust variance was used to assess the association between the presence of mucosal oral lesions and independent variables, estimating the prevalence ratio and 95% confidence interval (95%CI). Variables that presented a p-value greater than 0.25 in bivariate analysis were excluded from the final model multivariable analysis using the forward stepwise selection technique.
This project was approved by the UFPel Ethics Committee. All of the examinations and interviews were performed with the individual's authorization through the signing of an informed consent agreement. All individuals presenting oral mucosal lesions were referred to the UFPel Center of Oral Diseases Diagnosis, regardless of whether they needed histopathological diagnosis or not.
Results
A total of 720 individuals were examined in 2006 (equivalent to a response rate of 80% from the OHS-97). Of this total, 52.8% were male, 71.2% were white or yellow, 18.2% were lighter-skinned black, and 10.6% were dark-skinned black. The prevalence of oral lesions was 23.3% (95%CI: 20.3-26.6), and 19.4% of the subjects presented more than one lesion. Prevalence of oral lesions among males and females was 25.1% (95%CI: 21.9-28.4) and 21.2% (95%CI: 18.3-24.5), respectively. Prevalence of lesions was higher among lighter-skinned black subjects [27.9% (95%CI: 24.6-31.3)].
Thirty-two percent (95%CI: 25.6-38.9) of individuals with at least one oral lesion had papules/nodules. Seventeen percent (95%CI: 12.1-22.9) of the subjects had erosions and 26.5% (95%CI: 20.5-33.2) had ulcers. The most commonly affected location was the gingiva [35% (95%CI: 28.4-42.0)], followed by the lips [21% (95%CI: 15.6-27.3)] and tongue [18% (95%CI: 12.9-24.0)].
With regard to the distribution of type of lesion according to location in the mouth, papules/nodules were found predominantly on the gingiva [68.8% (95%CI: 55.9-79.7)], while ulcers and erosions were more prevalent on the lips [35.9% (95%CI: 23.1-50.2)] and tongue [70.6% (95%CI: 52.5-84.9)], respectively.
In relation to lesion size, 61% of lesions were between 0-0.5cm, 12% between 0.6-1.0cm, 8.5% between 1.1-2.0cm, 11% between 2.1-4.0cm, and 3% were larger than 4.0cm.
Thirty-three percent (95%CI: 27.0-40.5) of respondents mentioned feeling discomfort, 22.4% (95%CI: 16.9-28.9) pain, 13.3% (95%CI: 9.1-19.0) burning sensation and 5.5% (95%CI: 2.7-9.6) itching. A total of 27.6% (95%CI: 24.4-31.1) of examined individuals reported having noticed the presence of lesions. When individuals were asked if they performed self-examinations, 68.9% (95%CI: 65.4-72.3) answered yes/always, or sometimes, and 31.1% (95%CI: 27.6-34.5) answered no/never.
Bivariate analysis showed that there was no association between self-examination (Table 1) and gender (p = 0.55), skin color (p = 0.31), familiar income at childbirth (p = 0.09), and smoking habits (p = 0.31). On the other hand, individuals whose mother had a high level of schooling (p = 0.01) and individuals who received oral hygiene orientation from a dentist up to the age of 15 years (p < 0.001) were more likely to perform self-examination than those whose mothers had a low level of schooling or individuals who did not receive oral hygiene orientation.
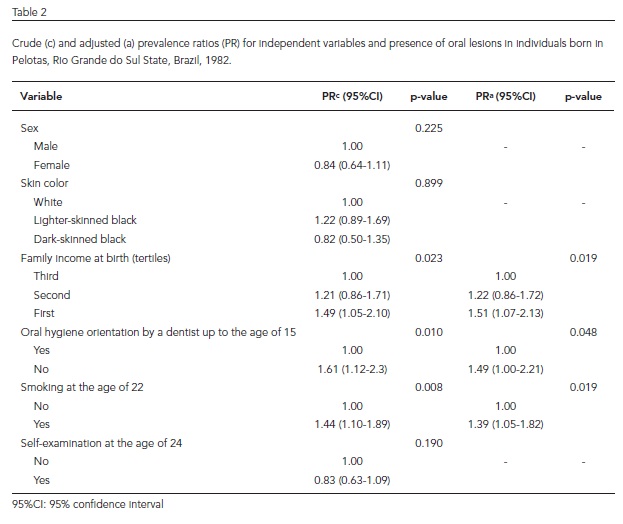
Table 2 shows that there was a positive association between low family income at birth (p = 0.019) and the presence of oral lesions. Lack of oral hygiene orientation up to the age of 15 years (p = 0.048) and smoking habits at the age of 22 years (p = 0.019) were associated with a greater prevalence of oral lesions even after adjustment.
A positive association was observed between the presence of potentially malignant oral mucosal lesions and low family income [prevalence ratio PR = 2.51 (95%CI: 1.09-5.77)]. Although smoking habits was shown to be a risk factor for the presence of potentially malignant lesions, this association lost significance after adjustment. In addition, the habit of self-examination was shown to have a protective effect (95%CI: 0.28-0.88) even after adjustment (Table 3).
Discussion
To the best of our knowledge, this is one of very few population-based studies to investigate oral mucosal lesions in a young adult population. Our findings suggest that these lesions are frequently found in this age group but generally receive little attention from professionals and researchers. However, the prevalence rates observed by the majority of other studies are higher than those found by this study 13,14. This can be explained by the fact that most of these other surveys analyzed individuals with known signs of oral disease seeking help from professionals working in specialized oral health services, therefore leading to a higher prevalence rate than that found in the general population.
Another possible explanation for the lower prevalence of oral lesions in our study is the exclusion of certain conditions that are generally included by other surveys, such as Fordyce granules, leukoedema, fissured tongue, geographic tongue and lingual varicosities 5,6. These conditions were excluded by this study because they are classified as being within the normal spectrum of developmental conditions 1, and are therefore not strictly defined as oral lesions. In addition, we registered the clinical features of the lesions as opposed to their specific diagnosis.
In our study, there was a similar distribution of lesions between men and women. Evidence in the literature regarding this matter is controversial with some studies showing higher prevalence of oral lesions among males 15 and other studies reporting higher prevalence of benign oral mucosal lesions in females 5. It is important to note that the effective comparison of the results of these studies is hindered due to significant variability among the populations examined and the use of different methodologies.
Papules and nodules, predominantly located in the gingiva, were the most common types of alterations found by this study. This site is generally affected by reactive and non-neoplastic oral lesions, such as pyogenic granuloma, fibroma, peripheral ossifying fibroma, peripheral giant cell granuloma, and inflammatory fibrous hyperplasia 1. The most prevalent of these gingival lesions in younger adults between the age of 20 and 29 years, the age group covered by this study, is pyogenic granuloma 14. It is also possible that these papules were due to periodontal or endodontic fistulas.
Lips and ulcers were the second-most prevalent site and type of alteration, respectively. The occurrence of traumatic ulcerations and recurrent aphthous ulcerations, predominantly in the labial mucosa, is relatively common among young adults 1. The third-most prevalent site in our study was the tongue. In another investigation, which examined subjects from different age groups, almost one-third of the total number of oral lesions were found on the tongue 6. In our study, the most common lesions found on the tongue were erosions. Since geographic tongue was excluded from the study, possible diagnostic hypotheses for erosion at this site include traumatic, allergic and infectious lesions 1; however this is outside the scope of our investigation.
In the present study, family income at birth was a risk factor for the presence of oral lesions. This association may be explained by the critical period theory which proposes that exposure to social deprivation during a critical period of development during early stages of life has a long-term effect on adult health, regardless of circumstances in adult life 16. In addition, another recent study of this cohort showed that adult oral health is also influenced by childhood living condi-tions 17. Similarly, a significant positive association was observed between lack of oral hygiene orientation (up to the age of 15 years) and smoking habits (at the age of 22 years) and the presence of oral lesions. Oral hygiene orientation is generally related to good general health, which helps to prevent inflammatory and reactive diseases, and possibly neoplastic conditions 18.
On analyzing the prevalence of smoking habits from adolescence to adult life in the 1982 birth cohort, Menezes et al. 19 found that prevalence of smoking habits increased with age in both sexes, and was particularly notable in individuals with lower socioeconomic status. Tobacco consumption is a major risk factor for certain oral diseases, such as periodontal problems and malignancies 20,21. An initial analysis of the data showed a possible association between smoking habits and the presence of potentially malignant lesions (plaques, erosions and pigmented lesions); however this association was lost significance after adjustment. A limitation of the present analysis is that other lesions may be listed under these clinical aspects and a definitive diagnosis can only be established after a histological examination. Moreover, much more work is needed to understand the etiology of oral cancer in young adults, as some studies have shown that this segment of the population does not maintain smoking and alcohol consumption habits over a long period of time, which is recognized as a risk factor in older age groups 22. Other risk factors, such as genetic alterations, HPV infection and marijuana use, have been listed as risk factors in the etiology of these early lesions 23,24,25.
Our study also observed an association between self-examination and the level of maternal schooling and oral hygiene orientation. In the revised literature, just one study investigated the importance of oral self-examination 26. This process can improve the prevention of certain oral diseases and ensure early diagnosis, allowing for more effective treatment, and may also be an important step in the cure of cancer. Individuals whose mothers had lower levels of education were less likely to perform self-examination than individuals with mothers with higher levels of schooling at birth. A higher level of maternal education may facilitate access to information and therefore more highly educated mothers can better instruct their children regarding the importance of self-examination and the prevention of oral diseases. Others studies have shown an association between schooling and skin self-examination 27. Maternal educational level is also a strong socioeconomic indicator, since a higher level of education is normally associated with a better job, wages and living conditions. It is also a strong determinant of future employment and income 28 and of the knowledge and skills an individual attains during the education process. Therefore, maternal educational level may affect a person's cognitive functioning, making the individual more receptive to health education messages 28, and this could explain the association found by our study. Other studies of birth cohorts, including the one investigated by this study, have shown an association between this indicator and other oral health problems 29,30. A recent study of the same 1982 birth cohort showed that individuals who received orientations on oral hygiene from a dentist up to the age of 15 years had a lower rate of tooth loss at the age of 24 years 29. These findings suggest that individuals who make dental visits during childhood and adolescence demonstrate better healthcare, including the habit of performing self-examinations.
However, no association was found between family income at birth and self-examination. This can be explained in part by the fact that income is related to material resources and circumstances that have a direct impact on health, such as access to health services 28. Nevertheless, we believe that the habit of self-examination is more related to the capacity to receive and assimilate educational messages than to access to oral health services.
Since the present study was carried out with a birth cohort that has been continuously followed up since 1982 10, this investigation is less susceptible to information bias. The internal validity of the study is a consequence of high examiner repeatability, a low number of missing data, and the fact that the examiners and interviewers carried out blinded assessments.
The present epidemiologic survey was carried out by general dentists to evaluate different oral health conditions, including the presence of oral lesions. Considering that the calibration of the examiners for the diagnosis of a range of oral lesions is complex and difficult, and knowing that the diagnosis of these conditions frequently requires histopathological analysis and complementary examinations, the lesions were registered according to the type of oral mucosa alteration observed. Because this study was based on home visits, it would have been impossible for the experienced oral pathologist, whose findings served as a gold standard during the calibration process, to conduct all of the house visits, and therefore a less specific but reliable registration of diagnosis was chosen for the lesions.
Finally, considering the implications of our findings from a public health perspective, the prevalence of oral mucosal lesions found in our study can be considered high. However, most of these lesions were not potentially malignant. This is to be expected considering the age group that was investigated, since it is well-known that oral cancer is more common after the age of 40 years 1. On the other hand, taking into account the protective effect of oral hygiene orientation observed in our study, the high percentage of smokers in this population, and the association of smoking with the presence of oral lesions, governments should design strategies to promote healthy habits from early life into old age. In addition, both public and private health service clinicians should promote oral self-examination habits in individuals as a simple and low-cost strategy to ensure early detection of these lesions. Considering that oral cancer is one of the five most important public oral health problems in this country, the Brazilian government has made stomatology mandatory in public Specialized Dental Centers (CEO, acronym in Portuguese) in an attempt to ensure early diagnosis not only of cancerous lesions but also of other mucosal disorders 31. This strategy, coupled with effective primary care, is an important step toward improving oral health in Brazil during the coming years.
Conclusion
The prevalence of oral lesions in 24-year-old adults in Pelotas was 23.3%. Lower family income at birth and smoking habits at the age of 22 years were risk factors for the presence of oral lesions, while receiving oral hygiene instructions from a dentist up to the age of 15 years was a protective factor for this outcome. Individuals whose mothers had a higher educational level at birth and who received oral hygiene instructions from a dentist up to the age of 15 years were more likely to perform oral self-examinations. Therefore, a dentist has the essential task of orienting individuals to prevent the occurrence of oral lesions, as well as other oral conditions. Self-examination of the oral cavity should be encouraged to improve the prevention, diagnosis and early treatment of oral lesions.
Contributors
M. B. Correa participated in data collection, analysis and interpretation, and in the drafting and final revision of this article. S. B. C. Tarquinio contributed to study conception and design, data collection and interpretation, and to the drafting and final approval of this article. L. J. C. Oliveira contributed to the conception of this article, data collection and interpretation, and to the drafting and final revision of this article. M. A. Peres, K. G. Peres, D. P. Gigante, B. L. Horta e F. F. Demarco participated in study conception, design and planning, data collection, and in the drafting and final revision of this article.
Acknowledgments
The authors would like to thank the Pelotas cohort study program and the CNPq (process number 479621/20047 and 476985/20045) for its financial support.
Submitted on 07/Jun/2012
Final version resubmitted on 06/Sep/2012
Approved on 25/Sep/2012
ERRATUM
Correa MB, Tarquinio SBC, Oliveira LJC, Peres MA, Peres KG, Gigante DP, Horta BL, Demarco FF. Factors associated with prevalence of oral lesions and oral self-examination in Young adults from a birth cohort in Southern Brazil. Cad Saúde Pública 2013; 29(1):155-164.
A revista foi informada sobre erros na publicação da ordem de autoria e do nome do autor de correspondência. A ordem correta e a autora de correspondência são:
The journal was informed about errors in the publication of the order of authorship and the corresponding author's name. The correct order and the corresponding author are:
La revista fue informada acerca de los errores en la publicación de la orden de la autoría y el nombre del autor correspondiente. El orden correcto y el autor de correspondencia son:
Sandra Beatriz Chaves Tarquinio
Luisa Jardim Correa de Oliveira
Marcos Britto Correa
Marco Aurélio Peres
Karen Glazer Peres
Denise Petrucci Gigante
Bernardo Lessa Horta
Flávio Fernando Demarco
Correspondence
S. B. C. Tarquinio
Programa de Pós-graduação em Odontologia, Universidade Federal de Pelotas.
Rua Gonçalves Chaves 467, 5o andar, Pelotas, RS 96015-560, Brasil.
- 1. Neville BW, Damn DD, Allen CM, Bouquot JE. Patologia oral e maxilofacial. Rio de Janeiro: Editora Guanabara Koogan; 2009.
- 2. Lopez-Jornet P, Camacho-Alonso F, Bergugo ML. Measuring the impact of oral mucosa disease on quality of life. Eur J Dermatol 2009; 19:603-6.
- 3. Lima GS, Fontes ST, Araújo LMA, Etges A, Tarquinio SBC, Gomes APN. A survey of oral and maxilofacial biopsies in children. A single-center retrospective study of 20 years in Pelotas-Brazil. J Appl Oral Sci. 2008; 16:397-402.
- 4. Pindborg JJ. Epidemiology and public health aspects of the oral mucosa. J Dent Res 1977; 56:14-9.
- 5. Al-Mobeeriek A, Aldosari AM. Prevalence of oral lesions among Saudi dental patients. Ann Saudi Med 2009; 29:365-8.
- 6. Garcí-Pola-Vallejo MJ, Martinez Díaz-Canel AI,García Martin JM, González García M. Risk factors of oral soft tissue lesions in an adult Spanish population. Community Dent Oral Epidemiol 2002; 30:277-85.
- 7. Kleinman DV, Swango PA, Niessen LC. Epidemiologic studies of oral mucosal conditions methodologic issues. Community Dent Oral Epidemiol 1991; 19:119-40.
- 8. Shiboski CH, Schmidt BL, Jordan RC. Tongue and tonsil carcinoma. Cancer 2005; 103:1843-9.
- 9. Popovtzer A, Shpitzer T, Bahar G, Marshak G, Ulanovski D, Feinmesser R. Squamous cell carcinoma of the oral tongue in young patients. Laryngoscope 2004; 114:915-7.
- 10. Victora CG, Barros FC. Cohort profile: the 1982 Pelotas (Brazil) birth cohort study. Int J Epidemiol 2006; 35:237-42.
- 11. MacCarthy D, Flint SR, Healy C, Stassen LF. Oral and neck examination for early detection of oral cancer: a practical guide. J Ir Dent Assoc 2011; 57:195-9.
- 12. Hipólito RA, Martins CR. Prevalence of oral mucosal alterations in Brazilian adolescents held in two juvenile re-education centers. Ciênc Saúde Coletiva 2010; 15:3233-43.
- 13. Castellanos JL, Díaz-Guzmán L, Guanajuato L. Lesions of the oral mucosa: an epidemiological study. Int Dent J 2008; 105:79-85.
- 14. Salum FG, Yurgel LS, Cherubine K, De Figueiredo MA, Medeiros IC, Nicola FS. Pyogenic granuloma, peripheral giant cell granuloma and peripheral ossifying fibroma: retrospective analysis of 138 cases. Minerva Stomatol 2008; 57: 227-32.
- 15. Jahanbani J, Sandvik L, Lyberg T, Ahlfors E. Evaluation of oral mucosal lesions in 598 referred Iranian patients. Open Dent J 2009; 3:42-7.
- 16. Barker DJP. Mothers, babies, and disease in later life. London: BMJ Publishing Group; 1994.
- 17. Peres MA, Peres KG, Thomson WM, Broadbent JM, Gigante DP, Horta BL. The influence of family income trajectories from birth to adulthood on adult oral health: findings from the 1982 Pelotas birth cohort. Am J Public Health 2011; 101:730-6.
- 18. Meurman JH. Infectious and dietary risk factors of oral cancer. Oral Oncol 2010; 46:411-3.
- 19. Menezes AM, Minten GC, Hallal PC, Victora CG, Horta BL, Gigante DP, et al. Smoking prevalence in the 1982 birth cohort: from adolescence to adult life, Pelotas, Southern Brazil. Rev Saúde Pública 2008; 42:78-85.
- 20. Franco EL, Kowalski LP, Oliveira BV, Curado MP, Pereira RN, Silva ME, et al. Risk factors for oral cancer in Brazil: a case control study. Int J Cancer. 1989; 43:992-1000.
- 21. Vokes EE, Weichselbaum RR, Lippman SM, Hong WK. Head and neck cancer. N Engl J Med 1993; 328:184-94.
- 22. Llewellyn CD, Johnson NW, Warnakulasuriya KAAS. Risk factors for squamous cell carcinoma of the oral cavity in young people: a comprehensive literature review. Oral Oncol 2001; 37:401-18.
- 23. Santos-Silva AR, Ribeiro AC, Soubhia AM, Miyahara GI, Carlos R, Speight PM, et al. High incidences of DNA ploidy abnormalities in tongue squamous cell carcinoma of young patients: an international collaborative study. Histopathology 2011; 58:1127-35.
- 24. Toner M, O'Reagan EM. Head and neck squamous cell carcinoma in the young: a spectrum or a distinct group? Part 2. Head and Neck Pathol 2009; 3:249-51.
- 25. Tremblay S, Pintor Dos Reis P, Bradley G, Galloni NN, Perez-Ordonez B, Freeman J, et al. Young patients with oral squamous cell carcinoma: study of the involvement of GSTP1 and deregulation of the Fanconi anemia genes. Arch Otolaryngol Head Neck Surg 2006; 132:958-66.
- 26. Mathew AL, Pai KM, Sholapurkar AA, Vengal M. The prevalence of oral mucosal lesions in patients visiting a dental school in Southern India. Indian J Dent Res 2008; 19:99-103.
- 27. Kasparian NA, McLoone JK, Meiser B. Skin cancer-related prevention and screening behaviors: a review of literature. J Behav Med 2009; 32:406-28.
- 28. Galobardes B, Shaw M, Lawlor DA, Lynch JW, Smith GD. Indicators of socioeconomic position (part 1). J Epidemiol Community Health 2006; 60:7-12.
- 29. Correa MB, Peres MA, Peres KG, Horta BL, Gigante DP, Demarco FF. Life-course determinants of need for dental prostheses at age 24. J Dent Res 2010; 89:733-8.
- 30. Peres MA, Peres KG, Barros AJD, Victora CG. The relation between family socioeconomic trajectories from childhood to adolescence and dental caries and associated oral behaviours. J Epidemiol Community Health 2007; 61:141-5.
- 31. Coordenação Nacional de Saúde Bucal, Departamento de Atenção Básica, Secretaria de Atenção à Saúde, Ministério da Saúde. Saúde bucal. Brasília: Ministério da Saúde; 2006. (Cadernos de Atenção Básica, 17) (Série A, Normas e Manuais Técnicos).
Correspondence:
Publication Dates
-
Publication in this collection
29 Jan 2013 -
Date of issue
Jan 2013
History
-
Received
07 June 2012 -
Accepted
25 Sept 2012 -
Reviewed
06 Sept 2012