
Abstracts
Social support is an important predictor for the maintenance of physical activity in adolescence. Thus, the social-ecological approach values the impact of individuals or groups interaction with available resources in the social environment for adopting an active lifestyle. This study analyzes social support from family and friends for adolescents to practice physical activity. Guided by the Social-Ecological Theory, an observational cross-sectional structural equations modeling was applied to 2,710 Brazilians adolescents aged from 14 to 18 years. We identified that the greater the social support from friends (β = 0.30; RMSEA = 0.065; CFI = 0.953; TLI = 0.922; SRMR = 0.048) and family, the greater the adolescents physical activity (β = 0.27; RMSEA = 0.015; CFI = 0.997; TLI = 0.995; SRMR = 0.013). However, support from both sources indicated no adequate adjustment values in the same study model. Our findings suggest that adolescents who perceive social support from family members or friends practice more physical activity, confirming that social support is important for physical activity promotion.
Keywords:
Adolescent; Motor Activity; Interpersonal Relations; Social Support
O apoio social é um preditor importante da manutenção de atividade física na adolescência, sendo que a abordagem da ecologia social valoriza o impacto da interação entre indivíduos ou grupos com recursos disponíveis no ambiente social para adotar um estilo de vida saudável. Portanto, o estudo analisa as relações de apoio social de familiares e amigos para a prática de atividade física por adolescentes. Com base na Teoria de Ecologia Social, os autores aplicam a modelagem de equações estruturais com uma perspectiva observacional e desenho transversal, com 2.710 adolescentes brasileiros entre 14 e 18 anos de idade. Foi possível mostrar que níveis maiores de apoio social dos amigos (β = 0,30; RMSEA = 0,065; CFI = 0,953; TLI = 0,922; SRMR = 0,048) e dos familiares estão associados com maior atividade física nos adolescentes (β = 0,27; RMSEA = 0,015; CFI = 0,997; TLI = 0,995; SRMR = 0,013). Entretanto, o apoio de ambas as fontes no mesmo modelo analítico não indicou bons valores de ajuste. Os achados sugerem que os adolescentes que recebem apoio social de familiares ou amigos apresentam melhores níveis de atividade física, confirmando o apoio social como importante fator de promoção da prática de atividade física.
Palavras-chave:
Adolescente; Atividade Motora; Relações Interpessoais; Apoio Social
El apoyo social es un importante predictor para el mantenimiento de la actividad física en la adolescencia, por ello, el enfoque socioecológico valora el impacto de la interacción entre individuos, o grupos con recursos disponibles en el entorno social, con el fin de adoptar un estilo de vida activo. Por lo tanto, este estudio analiza el apoyo social de las relaciones de familia y amigos para la práctica de actividad física de adolescentes. Utilizando la Teoría Ecológica Social, aplicamos modelos de ecuaciones, desde una perspectiva observacional con diseño transversal, en la que participaron 2.710 brasileños adolescentes, de 14 a 18 años de edad. Fue posible identificar que cuanto mayor era el apoyo social de los amigos (β = 0,30; RMSEA = 0,065; CFI = 0,953; TLI = 0,922; SRMR = 0,048), al igual que el apoyo social de la familia, mayor era la actividad física de los adolescentes (β = 0,27; RMSEA = 0,015; CFI = 0,997; TLI = 0,995; SRMR = 0,013). Sin embargo, el respaldo de ambas fuentes en el mismo modelo de análisis no indicó valores de ajuste adecuados. Los resultados sugieren que los adolescentes que percibieron un apoyo social de los miembros de la familia o amigos tienen niveles mejores de actividad física. Este resultado confirma que el apoyo social es un importante promotor de la práctica de actividad física.
Palabras-clave:
Adolescent; Atividad Motora; Relaciones Interpersonales; Apoyo Social
Introduction
The World Health Organization (WHO) 11. World Health Organization. Global status report on noncommunicable diseases. Geneva: World Health Organization; 2014. found that physical inactivity is the fourth leading risk factor for death worldwide, second only to high blood pressure, tobacco use, and high blood glucose. Adolescence is considered a decisive period for adopting adequate physical activity behaviors, as these benefit bone health, prevent chronic noncommunicable diseases 22. Ho FKW, Louvie LHT, Chow CB, Wong WH, Ip P. Activity improves mental health through resilience in Hong Kong Chinese adolescents. BMC Pediatr 2015; 15:48-57.,33. Marques A, Calmeiro L, Loureiro N, Frasquilho D, Matos MG. Health complaints among adolescents: associations with more screen-based behaviours and less physical activity. J Adolesc 2015; 44:150-7.,44. Kapcakova J, Vaselska ZD, Geckova AM, Djk JP, Rejonoveld S. Is being a boy and feeling fat a barrier for physical activity? The association between body image, gender and physical activity among adolescents. Int J Environ Res Public Health 2014; 11:1167-76., and are considered a determining factor in active behavior throughout life 55. Bélanger M, Sabiston CM, Barnett TA, O'Loughlin E, Ward S, Contreras G, et al. Number of years of participation in some, but not all, types of physical activity during adolescence predicts level of physical activity in adulthood: results from a 13-year study. Int J Behav Nut Phys Act 2015; 12:76..
The literature shows that social support is an important predictor for the maintenance of physical activity in adolescence 66. Laird Y, Fawkner S, Kelly P, Mcnamee L, Niven A. The role of social support on physical activity behaviour in adolescent girls: a systematic review and meta-analysis. Int J Behav Nut Phys Act 2016; 13:79.,77. Yao CA, Rhodes RE. Parental correlates in child and adolescente physical activity: a meta-analysis. Int J Behav Nut Phys Act 2015; 12:10.,88. Mendonça G, Cheng LA, Mélo EN, Farias Junior JC. Physical activity and social support in adolescent: a systematic review. Health Educ Res 2014; 29:822-39.,99. Silva P, Lott R, Mota J, Welk G. Direct and indirect effects of social support on youth physical activity behavior. Pedriatr Exerc Sci 2014; 26:86-94.. As a facilitator to physical activity, this construct substantiates theoretical models such as social cognitive, behavior modification, social learning, and social ecological theories 1010. Elder JP, Ayala GX, Harris S. Teories and intervention approaches to health-behavior change in primary care. Am J Prev Med 1990; 17:275-84.. Theoretical models studies on health promotion allows us to understand lifestyle behaviors, such as physical activity.
Among these models, the social-ecological approach values the impact of individuals or groups interaction with available resources in the social environment for adopting an active lifestyle 99. Silva P, Lott R, Mota J, Welk G. Direct and indirect effects of social support on youth physical activity behavior. Pedriatr Exerc Sci 2014; 26:86-94.,1111. Belanger-Gravel A, Gauvin L, Fagarge F, Lafete M. Correlates and moderators of physical activity in parent-twee dyads: a socio-ecological perspective. Public Health 2015; 129:1218-23.,1212. Simpkins SD, Schaefer DR, Prince CD, Vest AE. Adolescent friendships, BMI, and physical activity: untangling selection and influence through longitudinal social network analysis. J Res Adolesc 2012; 23:537-49.,1313. Reimers AK, Jekauc D, Mess F, Mewes N, Woll A. Validity and reliability of a self-report instrument to assess social support and physical environmental correlates of physical activity in adolescents. BMC Public Health 2012; 12:705.. Personal attributes within the social environment and the creation of an interpersonal network are key references for developing positive and negative habits related to physical activity during adolescence 99. Silva P, Lott R, Mota J, Welk G. Direct and indirect effects of social support on youth physical activity behavior. Pedriatr Exerc Sci 2014; 26:86-94.,1414. Yunes MAM, Juliano MC. A bioecologia do desenvolvimento humano e suas interfaces com educação ambiental. Cadernos de Educação 2010; 37:347-79.. Thus, we may understand social support as a complex and multidimensional construct that helps comprehending how different relationships either positively or negatively influence the way individuals deal with possible adversities during their development 1515. Marôco JP, Campos JADB, Vinagre MG, Pais-Ribeiro JL. Adaptação transcultural Brasil-Portugal da escala de satisfação com o suporte social para estudantes do Ensino Superior. Psicol Reflex Crít 2014; 27:247-56..
Family setting is considered an important source of support for the practice of physical activity during adolescence 88. Mendonça G, Cheng LA, Mélo EN, Farias Junior JC. Physical activity and social support in adolescent: a systematic review. Health Educ Res 2014; 29:822-39.,99. Silva P, Lott R, Mota J, Welk G. Direct and indirect effects of social support on youth physical activity behavior. Pedriatr Exerc Sci 2014; 26:86-94.,1111. Belanger-Gravel A, Gauvin L, Fagarge F, Lafete M. Correlates and moderators of physical activity in parent-twee dyads: a socio-ecological perspective. Public Health 2015; 129:1218-23.,1616. Spurr S, Bally J, Trinder K. Predictors of physical activity in positive deviant adolescentes. J Pediatr Nurs 2016; 31:311-8. for facilitating active behavior by different mechanisms - encouraging situations that favor physical activity, proposing different practice strategies, and providing instrumental support and company during the physical activity 1717. Cheng LA, Mendonça G, Farias Junior JC. Physical activity in adolescents: analysis of social influence of parents and friends. J Pediatr (Rio J.) 2014; 90:35-41.,1818. Beets M, Cardinal B, Aldeman B. Parental social support and the physical activity-related behaviors of youth: a review. Health Educ Behav 2010; 37:621-64.. Another important source of social support are friends; as adolescents spend a considerable amount of time with their colleagues, with whom they coexist in common settings such as school and clubs 1919. Sawaka KJ, McCormack GR, Nettel-Agurre A, Hawe P, Doylw-Baker PK. Friendship networks and physical activity and sedentary behavior among youth: a systematized review. Int J Behav Nutr Phys Act 2013; 10:130.,2020. Fritzgerald A, Fritzgerald N, Aherne C. Do peer matter? A review of peer and/or friends' influence on physical activity among American adolescents. J Adolesc 2012; 53:941-58., they may also be considered relevant shapers of active behaviors.
Regardless of the presence of social support from family and friends, promoting the practice of physical activity among adolescents is an important matter. Yet, few studies employed methods of analysis that enable the evaluation of a complex mechanism, such as the social support construct, by decomposing effects. Active behavior development processes within a context may vary according to individual personal attributes and perceived social environment (family and friends) 1111. Belanger-Gravel A, Gauvin L, Fagarge F, Lafete M. Correlates and moderators of physical activity in parent-twee dyads: a socio-ecological perspective. Public Health 2015; 129:1218-23.,1212. Simpkins SD, Schaefer DR, Prince CD, Vest AE. Adolescent friendships, BMI, and physical activity: untangling selection and influence through longitudinal social network analysis. J Res Adolesc 2012; 23:537-49.,2121. Daviso KK, Nishi A, Kranz S, Wyckoff L, May JJ, Earle-Richadson GB, et al. Association among social capital, parenting for active lifestyle, and youth physical in rural families living in upstate New York. Soc Sci Med 2012; 75:1488-96..
Understanding the perceived social support from family and friends for the practice of physical activity among different adolescent populations is necessary to provide subsidies, promote, and increase physical activity levels within this age group. Previous studies on this topic begin by direct relationship analyses; accordingly, structural equation modeling allows us to test mediation models under a theoretical construction using observational data. Considering that, this study aims to analyze the relationship between social support from family and friends and the practice of physical activity in adolescents from a region in Southern Brazil.
Methods
An observational cross-sectional study was conducted with 24,353 adolescents aged between 14 and 18 years, enrolled in 67 public high schools in Greater Florianópolis, Santa Catarina State, Brazil. Using random, cluster, and proportional methods, sampling was calculated according to the number of adolescents enrolled in the public school system. Based on the proportion distribution formula proposed by Luiz & Magnanini 2222. Luiz RR, Magnanini MMF. A lógica da determinação do tamanho da amostra em investigações epidemiológicas. Cad Saúde Colet (Rio J.) 2000; 8:9-28., we adopted a 3% sample error, 95% confidence interval, 50% prevalence, and 2.0 design effect, resulting in a required sample of 2,048 students.
With the approval of the Human Research Ethics Committee of the Santa Catarina State University (UDESC; permit n. 501.582), the schools and classes that would compose the sample were randomly selected. Due to the type of clustering, 25 public schools were systematically selected and proportionally distributed among the 13 municipalities that compose the Greater Florianopolis by region and population density. In total, 19 schools were randomly selected and six automatically recruited for being the only ones within their municipality. Then, 126 classes were selected with proportional distribution per grade and study shift (morning, afternoon, etc.). All students were invited to participate in the study upon presentation of the signed free and informed consent form, resulting in a final sample of 2,710 adolescents.
A short version of the International Physical Activity Questionnaire (IPAQ) was used to verify adolescent’s physical activity level. The instrument was proposed by the International Consensus Group on Physical Activity Measurement, founded by the WHO, with representatives in 25 countries, including Brazil 2323. Guedes DP, Lopes CC, Guedes JERP. Reprodutibilidade e validade do Questionário Internacional de Atividade Física em adolescentes. Rev Bras Med Esporte 2005; 11:151-8.. It addresses questions on how much time did participants spend on vigorous and moderate physical activities and walks during the last seven days. Adolescents were classified into “meeting the recommendations” and “not meeting the recommendations”, according to WHO recommendation of 60 minutes of daily moderate and vigorous physical activity 11. World Health Organization. Global status report on noncommunicable diseases. Geneva: World Health Organization; 2014..
Social support for the practice of physical activity was measured using the Social Support for Exercise Behaviors survey instrument - created by a group coordinated by James F. Sallis 2424. Sallis JF, Grossman RM, Pinkis RB, Patterson TL, Nader PR. The development of scales to measure social support for diet and exercise behaviors. Prev Med 1987; 16:825-36. and validated for Brazilian adolescents by Reis & Sallis 2525. Reis RS, Sallis JF. Validade e reprodutibilidade da versão brasileira da Escala de Suporte Social para o Exercício em Adolescentes. Rev Bras Ciênc Mov 2005; 13:7-15.. It comprises two scales: perceived support from family and perceived support from friends, both composed of 13 statements regarding support for the practice of physical activity. In this survey, adolescents must assign a score to each statement on an ordinal scale (0 = never; 1 = almost never; 2 = sometimes; 3 = frequent; 4 = very frequent). The final score is the sum of each scale assigned scores.
Our study sample was characterized using descriptive statistics, with means, standard deviations, and frequency distributions. The Spearman’s correlation was used to verify collinearity between social support from family and friends. All analyses were performed using the IBM SPSS statistics 20.0 software (https://www.ibm.com). A structural equation modeling analysis was conducted to evaluate direct associations between social support from family and friends and the practice of physical activity in adolescents. Parameters were estimated by the Asymptotically Distribution Free (ADF) method using the Stata 13 software (http://www.stata.com).
Adjustment evaluation was performed using the following parameters: root mean square error of approximation (RMSEA) - where values below 0.08 indicate adequate adjustment; goodness of fit index (GFI); Tucker-Lewis Index (TLI), where values must be equal to or greater than 0.90 to indicate adequate-fitting model 2626. Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation models. Newbury Park: Sage; 1993. p. 136-62.; and a standardized root mean square residual (SRMR) below 0.05 2727. Hair JF, Anderson RE, Tathan RL, Black WC. Análise multivariada de dados. 5ª Ed. Porto Alegre: Bookman; 2005..
Initially, a confirmatory factor analysis was conducted to analyze family social support and friends social support. After confirmation, both constructs were treated as latent variables with three plots including indicators with common characteristics: the first included indicators related to emotional support, the second to informational support, and the third to tangible 2828. Heaney CA, Israel BA. Social networks and social support. In: Glanz K, Rimer BK, Viswanath K, editors. Health behavior and health education: theory, research and practice. 4th Ed. San Francisco: Jossey-Bass; 2008. p. 189-206.,2929. Stroebe W, Stroebe M. The social psychology of social support. In: Higgins ET, Kruglanski Aw, editors. Social psychology: handbook of basic principles. New York: Guilford Press; 1996. p. 597-621.. Then, the measurement model was analyzed to verify whether the latent variables (social support from family and social support from friends) were correlated.
After that, the structural model was initially developed including three constructs: physical activity, perceived social support from family, and perceived social support from friends. Physical activity was treated as an indicator, based on WHO classification of physical activity (whether or not meeting the recommendations), and perceived social support from family and friends as latent variables. Different models were created including a single source of social support within each. We adopted this strategy because the measurement model showed that, when jointly analyzed, the two social support scales failed in adequately fitting quality indicators. The gender indicator was also included in all models for demonstrating powerful interactive effects on adolescents’ physical activity, as different physical activity levels between girls and boys are widely reported in the literature 3030. Carney J, Veldhuizen S, Kwan M, Hay J, Faught BE. Biological age and sex-related declines in physical activity during adolescence. Med Sci Sport Exerc 2013; 46:730-5..
Results
The sample comprised 2,710 adolescents, among which 57.9% were female and mean age was 16.90 (SD = 1.02) years. Regarding physical activity classification, 57.8% of the adolescents did not meet WHO recommendations for weekly physical activity. As for perceived social support, the mean was relatively low for family support, 12.15 (SD = 10.52) points, and for friends support, 14.55 (SD = 11.51), on a scale ranging from 0 to 52.
Polychoric correlation tested the internal consistency between the items of each scale on perceived social support. According to data presented in Table 1, all items were correlated (p > 0.05), confirming the instrument good internal consistency.
The confirmatory analysis of each social support scale verified adequate adjustment indexes for social support from family (RMSEA = 0.032; TLI = 0.908; CFI = 0.941; SRMR = 0.029) and friends (RMSEA = 0.036; TLI = 0.909; CFI = 0.939; SRMR = 0.045) (Figure 1).

Confirmatory factor analysis of Social Support for Exercise Behaviors for family and friends scales.
As for measurement model between perceived social support from family and perceived social support from friends, we found no adequate adjustment values (RMSEA = 0.172; CFT = 0.768; TLI = 0.565; SRMR = 0.068) (Figure 2).

Measurement model between perceived social support from family and perceived social support from friends.
By including perceived social support from family and friends and physical activity in the structural equations modeling analysis and considering gender as an indicator of physical activity we found inadequate adjustment indexes, indicating that the general model was not confirmed (RMSEA = 0.159; CFT = 0.513; TLI = 0.318; SRMR = 0.236) (Figure 3).

Final model for analysis between physical activity and perceived social support from family and friends.
We found adequate adjustment values in the model for physical activity and perceived family social support (Figure 4). These results indicate a direct relationship between social support and physical activity classification (β = 0.27; p < 0.001), as well as gender (β = 0.12; p < 0.001). The model reached a considerably high explanatory value (r2 = 0.88) and adequate adjustment indicators (RMSEA = 0.015; CFI = 0.997; TLI = 0.995; SRMR = 0.013).

The model with perceived social support from friends, physical activity, and gender, presented in Figure 5, show adequate adjustment index values (RMSEA = 0.065; CFI = 0.953; TLI = 0.922; SRMR = 0.048), confirming the relationship between social support (β = 0.20; p < 0.001) and gender (β = 0.085; p < 0.001) with physical activity. The model had a strong explanatory power (r2 = 0.88).

Discussion
Our main results indicate that, when subjected to a structural model, the perceived social support from family and friends influence adolescents’ physical activity, reinforcing the ecological approach to studies on health-related behaviors by the premise that different social settings foster different types of behaviors. Our data confirm that physical activity practiced by adolescents tend to be influenced by their social environments 66. Laird Y, Fawkner S, Kelly P, Mcnamee L, Niven A. The role of social support on physical activity behaviour in adolescent girls: a systematic review and meta-analysis. Int J Behav Nut Phys Act 2016; 13:79.,1111. Belanger-Gravel A, Gauvin L, Fagarge F, Lafete M. Correlates and moderators of physical activity in parent-twee dyads: a socio-ecological perspective. Public Health 2015; 129:1218-23.,1212. Simpkins SD, Schaefer DR, Prince CD, Vest AE. Adolescent friendships, BMI, and physical activity: untangling selection and influence through longitudinal social network analysis. J Res Adolesc 2012; 23:537-49.,2121. Daviso KK, Nishi A, Kranz S, Wyckoff L, May JJ, Earle-Richadson GB, et al. Association among social capital, parenting for active lifestyle, and youth physical in rural families living in upstate New York. Soc Sci Med 2012; 75:1488-96..
The constructs of social support from family and friends presented adequate values in the confirmatory factor analysis. All items composing the instrument evaluate the same construct: the perceived social support for each scale, family and friends. Such construct is supported by the unifactorial structure test of the scale applied to adolescents, since items correlations were statistically significant among each other, as well as scales total score 2626. Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation models. Newbury Park: Sage; 1993. p. 136-62.,3131. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling 1999; 6:1-55.. The confirmatory analysis of Social Support for Exercise Behaviors items helped validating the instrument for Brazilian adolescents 22. Ho FKW, Louvie LHT, Chow CB, Wong WH, Ip P. Activity improves mental health through resilience in Hong Kong Chinese adolescents. BMC Pediatr 2015; 15:48-57., showing an adequate reliability and internal consistency for this population.
In this study, adolescents with a higher perceived social support from family presented higher levels of physical activity, corroborating results reported in the literature, which indicates that family social support plays an important role in active behavior during adolescence 77. Yao CA, Rhodes RE. Parental correlates in child and adolescente physical activity: a meta-analysis. Int J Behav Nut Phys Act 2015; 12:10.,88. Mendonça G, Cheng LA, Mélo EN, Farias Junior JC. Physical activity and social support in adolescent: a systematic review. Health Educ Res 2014; 29:822-39.. This may be explained by the fact that families, especially parents, teach skills and defend beliefs that help adolescents shape important attitudes and behaviors towards physical activity 3232. Edwardson CL, Gorely T. Parental influences on different types and intensities of physical activity in youth: a systematic review. Psychol Sport Exerc 2010; 11:522-35.. Family setting is considered the most conducive structure to healthy development changes during adolescence 1111. Belanger-Gravel A, Gauvin L, Fagarge F, Lafete M. Correlates and moderators of physical activity in parent-twee dyads: a socio-ecological perspective. Public Health 2015; 129:1218-23.. Although adolescence experiences vary according to the contexts, the family promotes transformations in behavioral patterns 3333. Portugal APM, Alberto IMM. Caracterização da comunicação entre progenitores e filhos adolescentes: estudo das variáveis sociodemograficas. Ciênc Saúde Colet 2015; 20:1389-400. and adolescents who perceive their support for practicing physical activity end up by adopting healthy habits and becoming physically active.
Another relevant finding in this study was that the high perceived social support from friends was directly related to higher levels of physical activity, corroborating other studies on this subject 99. Silva P, Lott R, Mota J, Welk G. Direct and indirect effects of social support on youth physical activity behavior. Pedriatr Exerc Sci 2014; 26:86-94.,1717. Cheng LA, Mendonça G, Farias Junior JC. Physical activity in adolescents: analysis of social influence of parents and friends. J Pediatr (Rio J.) 2014; 90:35-41.,3434. Lopes VP, Gabbard C, Rodrigues LP. Effects of psychosocial variables in the similarity and interdependence of physical activity levels among adolescent best friend dyads. J Sports Sci 2016; 34:821-8.. A review performed by Mendonça et al. 88. Mendonça G, Cheng LA, Mélo EN, Farias Junior JC. Physical activity and social support in adolescent: a systematic review. Health Educ Res 2014; 29:822-39. found friends to be the most consistent source of social support in the association between overall physical activity and social support. Friends influence in the practice of physical activity may result from social norms, imposed by themselves, to suit the group 1919. Sawaka KJ, McCormack GR, Nettel-Agurre A, Hawe P, Doylw-Baker PK. Friendship networks and physical activity and sedentary behavior among youth: a systematized review. Int J Behav Nutr Phys Act 2013; 10:130.. That occurs because adolescents adopt behaviors based on those of friends within their social environment, as friendship networks are built according to shared interests, attitudes, and behaviors 1212. Simpkins SD, Schaefer DR, Prince CD, Vest AE. Adolescent friendships, BMI, and physical activity: untangling selection and influence through longitudinal social network analysis. J Res Adolesc 2012; 23:537-49.,1919. Sawaka KJ, McCormack GR, Nettel-Agurre A, Hawe P, Doylw-Baker PK. Friendship networks and physical activity and sedentary behavior among youth: a systematized review. Int J Behav Nutr Phys Act 2013; 10:130.,3434. Lopes VP, Gabbard C, Rodrigues LP. Effects of psychosocial variables in the similarity and interdependence of physical activity levels among adolescent best friend dyads. J Sports Sci 2016; 34:821-8..
We found a peculiarity regarding the employed structural models, whereby analyses on social support from family and friends, when in the same structural model, failed in presenting acceptable adjustment indexes. This may be technically justified by the fact that the measurement model (the previous step) between the two scales showed inadequate adjustment indicators values; if indicators are inadequate in the measurement model, the structural model will follow the same trend 2727. Hair JF, Anderson RE, Tathan RL, Black WC. Análise multivariada de dados. 5ª Ed. Porto Alegre: Bookman; 2005.. These results theoretically indicate that adolescents who perceive receiving support for practicing physical activity from at least one of the sources tend to present better physical activity levels. Another important factor is the way through which support is provided. Family members tend to encourage their children to practice physical activity through different means, such as providing transportation and equipment; in turn, friends tend to offer greater social support by inviting colleagues to practice physical activities 88. Mendonça G, Cheng LA, Mélo EN, Farias Junior JC. Physical activity and social support in adolescent: a systematic review. Health Educ Res 2014; 29:822-39., which may lead to a disparity in the overall individual models.
We found considerably low averages of perceived social support from family and friends among adolescents, as well as a low factorial load of the direct relationship between social support from both family and friends and physical activity. Meta-analysis studies on this subject 66. Laird Y, Fawkner S, Kelly P, Mcnamee L, Niven A. The role of social support on physical activity behaviour in adolescent girls: a systematic review and meta-analysis. Int J Behav Nut Phys Act 2016; 13:79.,77. Yao CA, Rhodes RE. Parental correlates in child and adolescente physical activity: a meta-analysis. Int J Behav Nut Phys Act 2015; 12:10. found positive effects (although relatively modest) on the association between social support and physical activity among adolescents. Their results suggest that support from family and friends influences physical activity; however, the low associations suggest that social support explains part of the variation in activity-related behavior in adolescents 66. Laird Y, Fawkner S, Kelly P, Mcnamee L, Niven A. The role of social support on physical activity behaviour in adolescent girls: a systematic review and meta-analysis. Int J Behav Nut Phys Act 2016; 13:79..
Our study has some limitations. Physical activity, for example, was measured in a general manner (sum of moderate and vigorous physical activity), possibly underestimating activity levels. Physical activity was also evaluated using a subjective method and, even though the employed instrument has acceptable measurement properties to monitor habitual physical activity levels in adolescents older than 14 years 2323. Guedes DP, Lopes CC, Guedes JERP. Reprodutibilidade e validade do Questionário Internacional de Atividade Física em adolescentes. Rev Bras Med Esporte 2005; 11:151-8., self-reporting evaluation imply a potential bias regarding subjectivity. Even so, questionnaires were deemed the best choice for the logistics of evaluating large sample sizes and are widely used in epidemiological studies.
Our study strength is using an analysis. model that estimates the strength of all hypostatized relationships in a theoretical scheme, besides using the confirmatory analysis to verify whether the items that comprise the instrument really evaluate the same construct - social support. Only individual models with social support from family or friends had adequate adjustment indexes, possibly indicating that social support and its effects on adolescents are inherent to social environments.
Conclusion
Considering the investigated factors, we identified that social support from family or friends was associated with the practice of physical activity among adolescents from a region in Southern Brazil, as they presented better physical activity levels when they perceived support from at least one of these sources. Thus, the data indicate that the construct is an important promoter of physical activity and should be considered in intervention programs focused on promoting better physical activity levels in this age group. Our results are important to better understand adolescents’ active behavior, which, although individual, is also influenced by context characteristics and social relationships.
Understanding the determinants of physical activity is essential to support new strategies to reduce sedentary behavior. Supporting or promoting social environment for the development of healthy habits and lifestyles has been a prevention strategy adopted in different public health areas. Thus, physical activity promotion programs should develop strategies focused not only on the individual, but also in increasing the support from social networks involving this group.
Acknowledgments
To Brazilian Graduate Studies Coordinating Board (CAPES) for the financial support. To Dr. Juliana Silva, who contributed to the research design and development.
References
-
1World Health Organization. Global status report on noncommunicable diseases. Geneva: World Health Organization; 2014.
-
2Ho FKW, Louvie LHT, Chow CB, Wong WH, Ip P. Activity improves mental health through resilience in Hong Kong Chinese adolescents. BMC Pediatr 2015; 15:48-57.
-
3Marques A, Calmeiro L, Loureiro N, Frasquilho D, Matos MG. Health complaints among adolescents: associations with more screen-based behaviours and less physical activity. J Adolesc 2015; 44:150-7.
-
4Kapcakova J, Vaselska ZD, Geckova AM, Djk JP, Rejonoveld S. Is being a boy and feeling fat a barrier for physical activity? The association between body image, gender and physical activity among adolescents. Int J Environ Res Public Health 2014; 11:1167-76.
-
5Bélanger M, Sabiston CM, Barnett TA, O'Loughlin E, Ward S, Contreras G, et al. Number of years of participation in some, but not all, types of physical activity during adolescence predicts level of physical activity in adulthood: results from a 13-year study. Int J Behav Nut Phys Act 2015; 12:76.
-
6Laird Y, Fawkner S, Kelly P, Mcnamee L, Niven A. The role of social support on physical activity behaviour in adolescent girls: a systematic review and meta-analysis. Int J Behav Nut Phys Act 2016; 13:79.
-
7Yao CA, Rhodes RE. Parental correlates in child and adolescente physical activity: a meta-analysis. Int J Behav Nut Phys Act 2015; 12:10.
-
8Mendonça G, Cheng LA, Mélo EN, Farias Junior JC. Physical activity and social support in adolescent: a systematic review. Health Educ Res 2014; 29:822-39.
-
9Silva P, Lott R, Mota J, Welk G. Direct and indirect effects of social support on youth physical activity behavior. Pedriatr Exerc Sci 2014; 26:86-94.
-
10Elder JP, Ayala GX, Harris S. Teories and intervention approaches to health-behavior change in primary care. Am J Prev Med 1990; 17:275-84.
-
11Belanger-Gravel A, Gauvin L, Fagarge F, Lafete M. Correlates and moderators of physical activity in parent-twee dyads: a socio-ecological perspective. Public Health 2015; 129:1218-23.
-
12Simpkins SD, Schaefer DR, Prince CD, Vest AE. Adolescent friendships, BMI, and physical activity: untangling selection and influence through longitudinal social network analysis. J Res Adolesc 2012; 23:537-49.
-
13Reimers AK, Jekauc D, Mess F, Mewes N, Woll A. Validity and reliability of a self-report instrument to assess social support and physical environmental correlates of physical activity in adolescents. BMC Public Health 2012; 12:705.
-
14Yunes MAM, Juliano MC. A bioecologia do desenvolvimento humano e suas interfaces com educação ambiental. Cadernos de Educação 2010; 37:347-79.
-
15Marôco JP, Campos JADB, Vinagre MG, Pais-Ribeiro JL. Adaptação transcultural Brasil-Portugal da escala de satisfação com o suporte social para estudantes do Ensino Superior. Psicol Reflex Crít 2014; 27:247-56.
-
16Spurr S, Bally J, Trinder K. Predictors of physical activity in positive deviant adolescentes. J Pediatr Nurs 2016; 31:311-8.
-
17Cheng LA, Mendonça G, Farias Junior JC. Physical activity in adolescents: analysis of social influence of parents and friends. J Pediatr (Rio J.) 2014; 90:35-41.
-
18Beets M, Cardinal B, Aldeman B. Parental social support and the physical activity-related behaviors of youth: a review. Health Educ Behav 2010; 37:621-64.
-
19Sawaka KJ, McCormack GR, Nettel-Agurre A, Hawe P, Doylw-Baker PK. Friendship networks and physical activity and sedentary behavior among youth: a systematized review. Int J Behav Nutr Phys Act 2013; 10:130.
-
20Fritzgerald A, Fritzgerald N, Aherne C. Do peer matter? A review of peer and/or friends' influence on physical activity among American adolescents. J Adolesc 2012; 53:941-58.
-
21Daviso KK, Nishi A, Kranz S, Wyckoff L, May JJ, Earle-Richadson GB, et al. Association among social capital, parenting for active lifestyle, and youth physical in rural families living in upstate New York. Soc Sci Med 2012; 75:1488-96.
-
22Luiz RR, Magnanini MMF. A lógica da determinação do tamanho da amostra em investigações epidemiológicas. Cad Saúde Colet (Rio J.) 2000; 8:9-28.
-
23Guedes DP, Lopes CC, Guedes JERP. Reprodutibilidade e validade do Questionário Internacional de Atividade Física em adolescentes. Rev Bras Med Esporte 2005; 11:151-8.
-
24Sallis JF, Grossman RM, Pinkis RB, Patterson TL, Nader PR. The development of scales to measure social support for diet and exercise behaviors. Prev Med 1987; 16:825-36.
-
25Reis RS, Sallis JF. Validade e reprodutibilidade da versão brasileira da Escala de Suporte Social para o Exercício em Adolescentes. Rev Bras Ciênc Mov 2005; 13:7-15.
-
26Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation models. Newbury Park: Sage; 1993. p. 136-62.
-
27Hair JF, Anderson RE, Tathan RL, Black WC. Análise multivariada de dados. 5ª Ed. Porto Alegre: Bookman; 2005.
-
28Heaney CA, Israel BA. Social networks and social support. In: Glanz K, Rimer BK, Viswanath K, editors. Health behavior and health education: theory, research and practice. 4th Ed. San Francisco: Jossey-Bass; 2008. p. 189-206.
-
29Stroebe W, Stroebe M. The social psychology of social support. In: Higgins ET, Kruglanski Aw, editors. Social psychology: handbook of basic principles. New York: Guilford Press; 1996. p. 597-621.
-
30Carney J, Veldhuizen S, Kwan M, Hay J, Faught BE. Biological age and sex-related declines in physical activity during adolescence. Med Sci Sport Exerc 2013; 46:730-5.
-
31Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling 1999; 6:1-55.
-
32Edwardson CL, Gorely T. Parental influences on different types and intensities of physical activity in youth: a systematic review. Psychol Sport Exerc 2010; 11:522-35.
-
33Portugal APM, Alberto IMM. Caracterização da comunicação entre progenitores e filhos adolescentes: estudo das variáveis sociodemograficas. Ciênc Saúde Colet 2015; 20:1389-400.
-
34Lopes VP, Gabbard C, Rodrigues LP. Effects of psychosocial variables in the similarity and interdependence of physical activity levels among adolescent best friend dyads. J Sports Sci 2016; 34:821-8.
Publication Dates
-
Publication in this collection
11 Jan 2021 -
Date of issue
2021
History
-
Received
08 Oct 2019 -
Reviewed
26 Apr 2020 -
Accepted
08 May 2020

 Note: S + F (item of the instrument Social Support for Exercise Behaviors, for family) + item number; S + A (item of the instrument Social Support for Exercise Behaviors, for friends) + item number.
Note: S + F (item of the instrument Social Support for Exercise Behaviors, for family) + item number; S + A (item of the instrument Social Support for Exercise Behaviors, for friends) + item number.
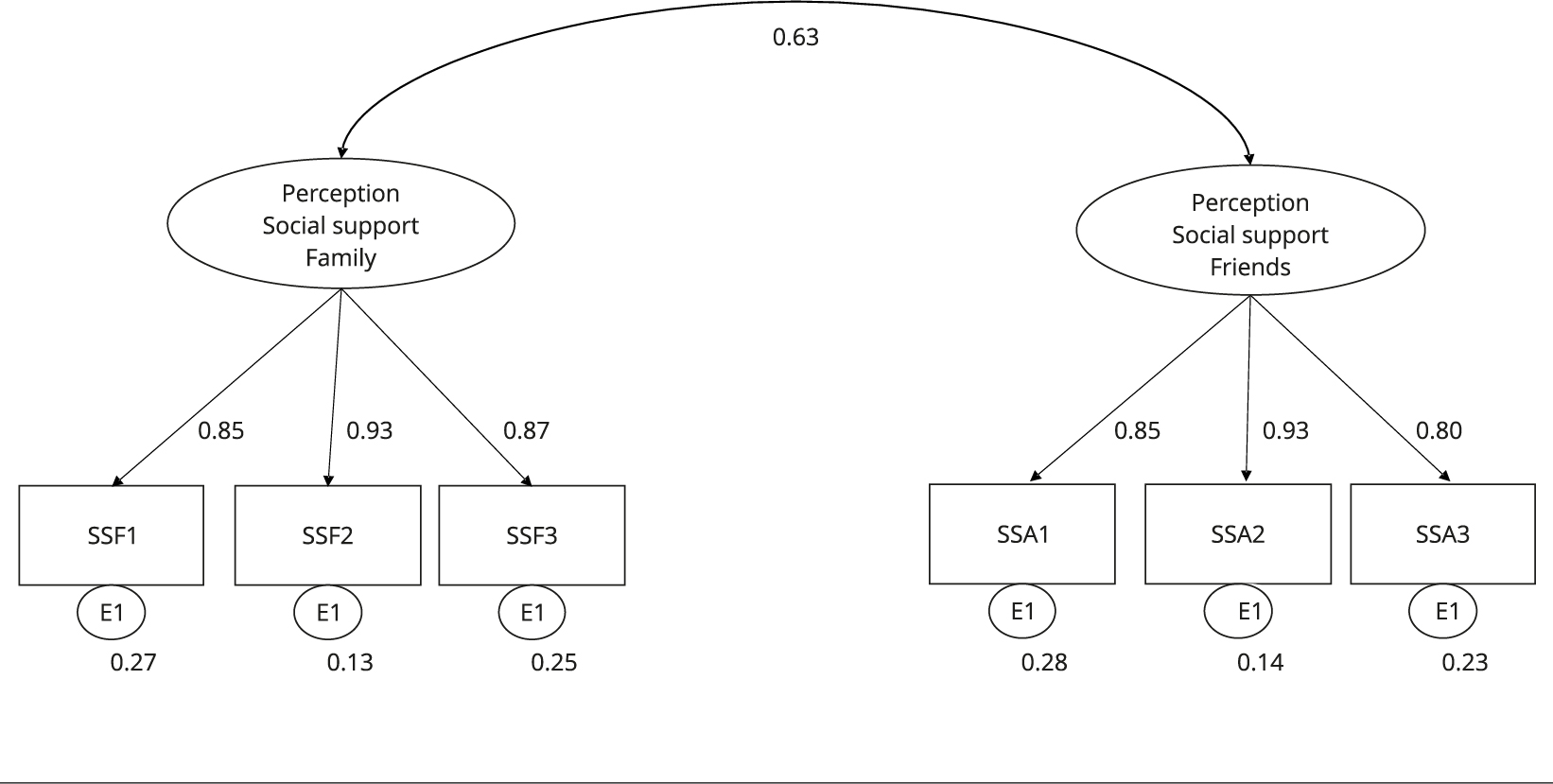 SSA: parcel item of the instrument Social Support for Exercise Behaviors, for friends; SSF: parcel item of the instrument Social Support for Exercise Behaviors, for family.
SSA: parcel item of the instrument Social Support for Exercise Behaviors, for friends; SSF: parcel item of the instrument Social Support for Exercise Behaviors, for family.
 SSA: parcel item of the instrument Social Support for Exercise Behaviors, for friends; SSF: parcel item of the instrument Social Support for Exercise Behaviors, for family.
SSA: parcel item of the instrument Social Support for Exercise Behaviors, for friends; SSF: parcel item of the instrument Social Support for Exercise Behaviors, for family.
 SSF: parcel item of the instrument Social Support for Exercise Behaviors, for family.
SSF: parcel item of the instrument Social Support for Exercise Behaviors, for family.
 SSA: parcel item of the instrument Social Support for Exercise Behaviors, for friends.
SSA: parcel item of the instrument Social Support for Exercise Behaviors, for friends.