Abstract
Sternoclavicular dislocations account for less than 5% of all dislocations of the scapular belt. Most cases of anterior dislocation of the sternoclavicular joint do not present symptoms. However, some patients may develop chronic anterior instability and remain symptomatic, and surgical treatment is indicated in these cases. There is a scarcity of reports in the literature relating to reconstruction using the long palmar tendon in cases of traumatic anterior instability. Although rare, these injuries deserve rapid diagnosis and efficient treatment in order to avoid future complications. The aim of this report was to report on a case of a motocross competitor who developed chronic traumatic anterior instability of the sternoclavicular joint and underwent surgical reconstruction using the autogenous long palmar tendon. The patient was a 33-year-old man with a history of anterior dislocation of the sternoclavicular subsequent to a fall during a maneuver in a motocross competition. Conservative treatment was instituted initially, consisting of use of a functional sling to treat the symptoms for 3 weeks, along with physiotherapeutic rehabilitation for 3 months. We chose to use a modification of the "figure of eight" technique based on the studies by Spencer and Kuhn. A longitudinal incision of approximately 10 cm was made at the level of the sternoclavicular joint. The graft from the ipsilateral long palmar tendon was passed through the orifices in the form of a modified "figure of eight" and its ends were sutured together. The patient was immobilized using an American sling for 4 weeks. After 6 months of follow-up, the patient no longer presented pain or instability when movement of the sternoclavicular joint was required. Minor discomfort and slight prominence of the sternoclavicular joint continued to be present but did not affect the patient's activities. Thus, the patient was able to return to racing 6 months after the operation. Our study presented a case of chronic anterior dislocation of the sternoclavicular joint that was successfully treated by using a modification of the "figure of eight" reconstruction technique. This technique was shown to be safe and effective, and it allowed the patient to fully return to his sports activities.
Keywords:
Dislocation; Tendon transfer; Shoulder
RESUMO
As luxações esternoclaviculares representam menos de 5% de todas as luxações da cintura escapular. A maioria dos casos de luxação anterior da articulação esternoclavicular não apresenta sintomas. Entretanto, alguns pacientes podem desenvolver instabilidade anterior crônica e permanecer sintomáticos. Nesses casos é indicado o tratamento cirúrgico. A literatura é escassa em relação à reconstrução com uso do tendão palmar longo nos casos de instabilidade anterior traumática. Embora raras, essas lesões merecem diagnóstico rápido e tratamento eficaz para evitar complicações futuras. O objetivo deste trabalho foi relatar um caso de um atleta de motocross que evoluiu com instabilidade anterior traumática crônica da articulação esternoclavicular e foi submetido a reconstrução cirúrgica com o uso do tendão palmar longo autógeno. Paciente masculino, 33 anos, com história de luxação anterior da articulação esternoclavicular após queda durante manobra em um campeonato de motocross. Inicialmente foi empregado o tratamento conservador, com uso de tipoia funcional por três semanas, e sintomático, além da reabilitação com fisioterapia por três meses. Optamos por usar uma modificação da técnica do "oito", baseados nos estudos de Spencer e Kuhn. A incisão longitudinal de aproximadamente 10 cm foi feita no nível da articulação esternoclavicular. O enxerto do tendão palmar longo ipsilateral foi passado pelos orifícios em forma de "oito" modificado e suas extremidades foram suturadas conjuntamente. O paciente foi imobilizado com tipoia americana por quatro semanas. No fim de seis meses de seguimento não apresentava dor ou instabilidade quando solicitada a articulação esternoclavicular. Um discreto desconforto e ligeira saliência da articulação esternoclavicular permaneceu, mas não afetaram suas atividades, o que permitiu ao paciente voltar às pistas de corrida com seis meses de pós-operatório. Nosso estudo apresentou um caso de luxação anterior crônica da articulação esternoclavicular tratado com sucesso com o uso de uma modificação da técnica de reconstrução em "oito". Essa técnica mostrou ser segura e eficaz e permitiu um retorno total às atividades esportivas do paciente.
Palavras-chave:
Luxação; Transferência de tendão; Ombro
Introduction
Sternoclavicular dislocations account for fewer than 5% of all dislocations of the scapular belt. Most cases of anterior dislocation of the sternoclavicular joint do not present symptoms. However, some patients may develop chronic anterior instability and may continue to present symptoms. In these cases, surgical treatment is indicated. 11 . Bae DS, Kocher MS, Waters PM, Micheli LM, Griffey M, Dichtel L. Chronic recurrent anterior sternoclavicular joint instability: results of surgical management. J Pediatr Orthop. 2006;26(1):71-4. 22 . Rockwood CA Jr, Groh GI, Wirth MA, Grassi FA. Resection arthroplasty of the sternoclavicular joint. J Bone Joint Surg Am. 1997;79(3):387-93. and 33 . Groh GI, Wirth MA, Rockwood CA Jr. Treatment of traumatic posterior sternoclavicular dislocations. J Shoulder Elbow Surg. 2011;20(1):107-13.
The sternoclavicular joint is more commonly dislocated anteriorly, given that the force required to dislocate the clavicle posteriorly is 50% greater because of the higher resistance of the posterior joint capsule. Many techniques for reconstructing the sternoclavicular joint have been described, such as intramedullary suturing, medial resection of the clavicle, fixation using a plate, reinforcement using the subclavian tendon and reinforcement using the semitendinosus tendon. 44 . Abiddin Z, Sinopidis C, Grocock CJ, Yin Q, Frostick SP. Suture anchors for treatment of sternoclavicular joint instability. J Shoulder Elbow Surg. 2006;15(3):315-8. 55 . Armstrong AL, Dias JJ. Reconstruction for instability of the sternoclavicular joint using the tendon of the sternocleidomastoid muscle. J Bone Joint Surg Br. 2008;90(5):610-3. and 66 . Singer G, Ferlic P, Kraus T, Eberl R. Reconstruction of the sternoclavicular joint in active patients with the figure-of-eight technique using hamstrings. J Shoulder Elbow Surg. 2013;22(1):64-9.
The literature relating to reconstruction using the long palmar tendon in cases of traumatic anterior instability is sparse. Although rare, these lesions deserve to be diagnosed rapidly with efficient treatment in order to avoid future complications.
The objective of this study was to report a case of a motocross competitor who evolved with chronic traumatic anterior instability of the sternoclavicular joint and underwent surgical reconstruction using the autogenous long palmar tendon.
Case report
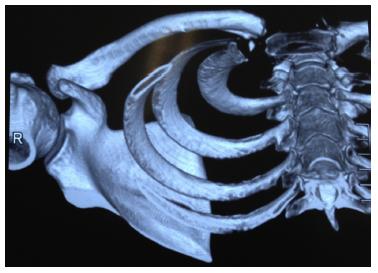
The patient was a 33-year-old man with a history of anterior dislocation of the sternoclavicular joint after a fall during a maneuver in a motocross championship. The trauma mechanism was a fall from a height of approximately two meters with the arm abducted and extended. Conservative treatment was used initially, with use of a functional sling for 3 weeks and treatment of the symptoms, along with physiotherapy for 3 months. However, the patient evolved with pain, discomfort and instability of the sternoclavicular joint when he raised his arm above his head, along with difficulty in swallowing when he flexed his neck anteriorly. He did not present any limitation on range of motion. During the physical examination, the anterior dislocation was visible when abduction and extension movements were made and also when the proximal end of the clavicle was manipulated ( Fig. 1). Imaging examinations showed anterior dislocation of the clavicle and the presence of small periarticular bone fragments ( Fig. 2, Fig. 3, Fig. 4and Fig. 5).
Photograph illustrating the chronic dislocation of the sternoclavicular joint of the right shoulder. Note the medial prominence of the middle third of the ipsilateral clavicle.
Radiograph in serendipity view, on which anterior displacement of the right sternoclavicular joint can be seen.
Image from computed tomography with 3D reconstruction, showing the displacement of the sternoclavicular joint and bone fragments.
Image from computed tomography with 3D reconstruction (view from above), showing the displacement of the sternoclavicular joint.
Image from computed tomography with 3D reconstruction (view from below), showing the displacement of the sternoclavicular joint.
Surgical technique
We chose to use a modification of the "figure of eight" technique, 77 . Kawaguchi K, Tanaka S, Yoshitomi H, Nagai I, Sato W, Karita T, et al. Double figure-of-eight reconstruction technique for chronic anterior sternoclavicular joint dislocation. Knee Surg Sports Traumatol Arthrosc. 2015;23(5):1559-62.based on the studies by Spencer et al., 88 . Spencer EE, Kuhn JE, Huston LJ, Carpenter JE, Hughes RE. Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg. 2002;11(1):43-7. and 99 . Spencer EE Jr, Kuhn JE. Biomechanical analysis of reconstructions for sternoclavicular joint instability. J Bone Joint Surg Am. 2004;86(1):98-105.who used cadavers to compare the resistance of three different reconstruction techniques: reconstruction using the semitendinosus tendon in a "figure of eight"; reinforcement using the subclavian tendon; and reconstruction of the intramedullary ligament. They concluded that reconstruction in a "figure of eight" was the technique that was most resistant to anterior sternoclavicular dislocation.
General anesthesia was induced with the patient in the dorsal decubitus position with the trunk inclined at 40°. A longitudinal incision of 10 cm was made at the level of the sternoclavicular joint. The joint was then completely dislocated anteriorly in order to separate out the disk of the clavicle. The joint space and the adjacent tissues were filled with scar tissue and the anterior and posterior sternoclavicular ligament and the costoclavicular ligament had been torn. The scar tissue was removed and subtle subperiosteal dissection of the proximal clavicle was performed in order to avoid damage to the brachiocephalic trunk and other posterior structures. This restored the mobility of the clavicle and enabled reduction. We removed a 20 cm length of the ipsilateral long palmar tendon ( Fig. 6) and performed the repair by means of a Krakow suture, using high-resistance polyethylene thread. Two 3.5 mm tunnels (anterosuperior and anteroinferior) were made at the proximal end of the clavicle and sternum, 15 mm from the joint face. The holes were put into communication in the intramedullary region and were brought to the exterior through the joint face on both sides. The graft was passed through the orifices in a modified figure of eight and its ends were sutured together ( Fig. 7and Fig. 8). The stability of the sternoclavicular joint was then tested through shoulder movements and maximum extension was avoided.
Intraoperative view showing the passage of the tendon through the bone tunnels at the medial end of the clavicle and the joint end of the sternum.
Postoperative period
The patient was immobilized by means of an American sling for 4 weeks. After this period, the sling was withdrawn and active movements were allowed. After 8 weeks, a program of muscle strengthening and exercises against resistance was started.
At the end of 6 months of follow-up, the patient did not present any pain or instability when use of the sternoclavicular joint was required ( Fig. 9). Mild discomfort and slight prominence of the sternoclavicular joint remained, but these did not affect the patient's activities. Thus, he was able to return to his racing activities 6 months after the operation.
Six months after the operation, showing good reduction of the right sternoclavicular joint. The prominence of the right clavicle can no longer be seen.
Discussion
This study sought to demonstrate a modification of the "figure of eight" reconstruction technique for anterior dislocation of the sternoclavicular joint. This reconstruction used the long palmar tendon and avoided the semitendinosus tendon, which would have led to greater morbidity. The patient presented excellent stability of the sternoclavicular after 2 years of follow-up, with complete restoration of his range of motion and improvement of his symptoms, including the uncommon difficulty in swallowing that he presented.
The majority of the cases of anterior dislocation of the sternoclavicular joint are treated conservatively. However, these injuries may often evolve to chronic instability. No additional treatment should be applied if the patient does not complain of pain or discomfort (rare in cases of anterior dislocation). 1010 . Bak K, Fogh K. Reconstruction of the chronic anterior unstable sternoclavicular joint using a tendon autograft: medium-term to long-term follow-up results. J Shoulder Elbow Surg. 2014;23(2):245-50. and 1111 . De Jong KP, Sukul DM. Anterior sternoclavicular dislocation: a long-term follow-up study. J Orthop Trauma. 1990;4(4):420-3.Each case needs to be carefully evaluated, in order to differentiate chronic dislocation from chronic instability. Surgical interventions may be beneficial for patients with chronic anterior dislocation of the sternoclavicular joint who present instability, discomfort or pain. 33 . Groh GI, Wirth MA, Rockwood CA Jr. Treatment of traumatic posterior sternoclavicular dislocations. J Shoulder Elbow Surg. 2011;20(1):107-13.
Studies have shown good functional results from using autologous grafts from the long palmar tendon for reconstruction of the sternoclavicular joint. 1212 . Eskola A, Vainionpää S, Vastamäki M, Slätis P, Rokkanen P. Operation for old sternoclavicular dislocation. Results in 12 cases. J Bone Joint Surg Br. 1989;71(1):63-5. 1313 . Eskola A. Sternoclavicular dislocation. A plea for open treatment. Acta Orthop Scand. 1986;57(3):227-8. and 1414 . Castropil W, Ramadan LB, Bitar AC, Schor B, De Oliveira D'Elia C. Sternoclavicular dislocation - reconstruction with semitendinosus tendon autograft: a case report. Knee Surg Sports Traumatol Arthrosc. 2008;16(9):865-8.This technique is biological and therefore subject to fewer complications than if plates and other implants are used. Even if plates produce good results, they may cause the complications that are inherent to non-biological implants, along with the possible need for their removal. Use of allografts also leads to the risk of infection. We chose to use the long palmar tendon because this presents low morbidity at the donor site, and is also easily removed. We are aware that the long palmar tendon is absent in around 30% of individuals, and our second choice would be the semitendinosus.
Several techniques for reconstructing the sternoclavicular joint have been introduced, including fixation with plates, fixation with anchors, fixation of the capsule and joint disk, reconstruction in a "figure of eight" using a graft from an autologous tendon and reconstruction using a graft from the sternocleidomastoid fascia. 11 . Bae DS, Kocher MS, Waters PM, Micheli LM, Griffey M, Dichtel L. Chronic recurrent anterior sternoclavicular joint instability: results of surgical management. J Pediatr Orthop. 2006;26(1):71-4. 44 . Abiddin Z, Sinopidis C, Grocock CJ, Yin Q, Frostick SP. Suture anchors for treatment of sternoclavicular joint instability. J Shoulder Elbow Surg. 2006;15(3):315-8. and 1515 . Friedrich L, Afifi FK, Skarvan J, Friederich NF, Hirschmann MT. Combined gracilis tendon autograft reconstruction and discus repair of a chronic anterior-superior sternoclavicular joint dislocation. Knee Surg Sports Traumatol Arthrosc. 2012;20(10):1978-82.Resection of the medial portion of the clavicle has also been reported. The ideal treatment still remains unknown, given that few studies have presented long-term results. Friedrich et al. 1515 . Friedrich L, Afifi FK, Skarvan J, Friederich NF, Hirschmann MT. Combined gracilis tendon autograft reconstruction and discus repair of a chronic anterior-superior sternoclavicular joint dislocation. Knee Surg Sports Traumatol Arthrosc. 2012;20(10):1978-82.reported good clinical results through using the autologous gracilis tendon as the graft in "figure of eight" reconstruction for a case of chronic anterosuperior sternoclavicular dislocation. Bae et al. 11 . Bae DS, Kocher MS, Waters PM, Micheli LM, Griffey M, Dichtel L. Chronic recurrent anterior sternoclavicular joint instability: results of surgical management. J Pediatr Orthop. 2006;26(1):71-4.reported that good stabilization was achieved in nine patients who underwent reconstruction of the sternoclavicular joint with the graft interlaced in a "figure of eight", through predrilled tunnels. Few studies have reported any advantage from "figure of eight" reconstruction, in relation to primary stability. Spencer and Kuhn9 conducted a study using cadavers with the aim of comparing the resistance of three different reconstruction techniques: reconstruction using the semitendinosus tendon in a "figure of eight"; reinforcement using the subclavian tendon; and reconstruction of the intramedullary ligament. They concluded that reconstruction in a "figure of eight" was the most resistant technique for cases of anterior sternoclavicular dislocation. Furthermore, a recent systematic review of clinical reports showed that the reconstruction technique involving a tendon graft in a "figure of eight" was more resistant than other techniques for treating chronic instability of the sternoclavicular joint.
The autologous grafts commonly used in reconstructions of the sternoclavicular joint are the gracilis, semitendinosus, long palmar and plantar tendons. 1212 . Eskola A, Vainionpää S, Vastamäki M, Slätis P, Rokkanen P. Operation for old sternoclavicular dislocation. Results in 12 cases. J Bone Joint Surg Br. 1989;71(1):63-5. 1414 . Castropil W, Ramadan LB, Bitar AC, Schor B, De Oliveira D'Elia C. Sternoclavicular dislocation - reconstruction with semitendinosus tendon autograft: a case report. Knee Surg Sports Traumatol Arthrosc. 2008;16(9):865-8. and 1515 . Friedrich L, Afifi FK, Skarvan J, Friederich NF, Hirschmann MT. Combined gracilis tendon autograft reconstruction and discus repair of a chronic anterior-superior sternoclavicular joint dislocation. Knee Surg Sports Traumatol Arthrosc. 2012;20(10):1978-82.Autologous grafts are used in order to avoid the risks of infection and to facilitate tissue integration, with the aim of obtaining a positive result over the long term. Among autologous grafts, we believe that the gracilis tendon and the long palmar tendon (which we used) are the ideal grafts, since their diameter results in lower morbidity. The medium-term results from our patient confirmed these findings, given that there was no morbidity in the donor area.
One potentially dangerous step in our technique was the drilling of the tunnels in the sternum and clavicular, because of the risk of injuring prime structures that are posterior to this. 1010 . Bak K, Fogh K. Reconstruction of the chronic anterior unstable sternoclavicular joint using a tendon autograft: medium-term to long-term follow-up results. J Shoulder Elbow Surg. 2014;23(2):245-50.Therefore, the exit points in the sternum and clavicle need to be protected through using a spacer, so as to avoid this type of injury.
Conclusion
Our study presented a case of chronic anterior dislocation of the sternoclavicular joint that was successfully treated using a modification of the "figure of eight" reconstruction. This technique was shown to be safe and efficient, and it allowed the patient to fully return to his sports activities.
References
-
1Bae DS, Kocher MS, Waters PM, Micheli LM, Griffey M, Dichtel L. Chronic recurrent anterior sternoclavicular joint instability: results of surgical management. J Pediatr Orthop. 2006;26(1):71-4.
-
2Rockwood CA Jr, Groh GI, Wirth MA, Grassi FA. Resection arthroplasty of the sternoclavicular joint. J Bone Joint Surg Am. 1997;79(3):387-93.
-
3Groh GI, Wirth MA, Rockwood CA Jr. Treatment of traumatic posterior sternoclavicular dislocations. J Shoulder Elbow Surg. 2011;20(1):107-13.
-
4Abiddin Z, Sinopidis C, Grocock CJ, Yin Q, Frostick SP. Suture anchors for treatment of sternoclavicular joint instability. J Shoulder Elbow Surg. 2006;15(3):315-8.
-
5Armstrong AL, Dias JJ. Reconstruction for instability of the sternoclavicular joint using the tendon of the sternocleidomastoid muscle. J Bone Joint Surg Br. 2008;90(5):610-3.
-
6Singer G, Ferlic P, Kraus T, Eberl R. Reconstruction of the sternoclavicular joint in active patients with the figure-of-eight technique using hamstrings. J Shoulder Elbow Surg. 2013;22(1):64-9.
-
7Kawaguchi K, Tanaka S, Yoshitomi H, Nagai I, Sato W, Karita T, et al. Double figure-of-eight reconstruction technique for chronic anterior sternoclavicular joint dislocation. Knee Surg Sports Traumatol Arthrosc. 2015;23(5):1559-62.
-
8Spencer EE, Kuhn JE, Huston LJ, Carpenter JE, Hughes RE. Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg. 2002;11(1):43-7.
-
9Spencer EE Jr, Kuhn JE. Biomechanical analysis of reconstructions for sternoclavicular joint instability. J Bone Joint Surg Am. 2004;86(1):98-105.
-
10Bak K, Fogh K. Reconstruction of the chronic anterior unstable sternoclavicular joint using a tendon autograft: medium-term to long-term follow-up results. J Shoulder Elbow Surg. 2014;23(2):245-50.
-
11De Jong KP, Sukul DM. Anterior sternoclavicular dislocation: a long-term follow-up study. J Orthop Trauma. 1990;4(4):420-3.
-
12Eskola A, Vainionpää S, Vastamäki M, Slätis P, Rokkanen P. Operation for old sternoclavicular dislocation. Results in 12 cases. J Bone Joint Surg Br. 1989;71(1):63-5.
-
13Eskola A. Sternoclavicular dislocation. A plea for open treatment. Acta Orthop Scand. 1986;57(3):227-8.
-
14Castropil W, Ramadan LB, Bitar AC, Schor B, De Oliveira D'Elia C. Sternoclavicular dislocation - reconstruction with semitendinosus tendon autograft: a case report. Knee Surg Sports Traumatol Arthrosc. 2008;16(9):865-8.
-
15Friedrich L, Afifi FK, Skarvan J, Friederich NF, Hirschmann MT. Combined gracilis tendon autograft reconstruction and discus repair of a chronic anterior-superior sternoclavicular joint dislocation. Knee Surg Sports Traumatol Arthrosc. 2012;20(10):1978-82.
-
☆
Work performed in the Department of Orthopedics and Traumatology, Hospital Santa Casa de Misericórdia de Vitória, Vitória, ES, Brazil.
Publication Dates
-
Publication in this collection
Aug 2015
History
-
Received
29 June 2014 -
Accepted
29 July 2014