INTRODUCTION
Signet-ring cell (SRC) carcinomas are poorly-differentiated malignant tumors that may affect the stomach and the colon, but very rarely occur in other digestive organs11 Gardner HA, Matthews J, Ciano PS: A signet-ring cell carcinoma of the ampulla of Vater. Arch Pathol Lab Med 1990; 114:1071-1072.,33 Karabulut Z, Yildirim Y, Abaci I, Ilgici D, Ozyilkan O: Signet-ring cell carcinoma of the gallbladder: a case report. Adv Ther 2008; 25:520-23.. Although SCR distal bile duct cholangiocarcinomas have been very rarely reported22 Hiraki M, Yakushiji H, Hashiguchil K et al. Signet ring cell carcinoma of the lower bile duct with rapid growth: report of a case. Hepatogastroenterology2007; 54:1922-1924.,44 Lee EY, Kim C, Kim MJ, et al. Signet ring cell carcinoma of theextrahepatic bile duct. Gut Liver 2010;4:402-6.,77 Ogata S, Kimura K, Hatsuse K et al. Poorly differentiated adenocarcinoma with signet-ring cell carcinoma of the extrahepatic bile duct in a 42-year-old Japanese female: a case report. Acta Med Okayama 2010;64:63-5. we herein first report the occurrence of a SRC hilar cholangiocarcinoma.
CASE REPORT
A 66-year-old caucasian woman was admitted with a 40-day history of fatigue, anorexia, jaundice, itching and pale stools. She had undergone external percutaneous transhepatic drainage and had been treated for cholangitis with antibiotics. The patient had no palpable masses and her past medical history was unremarkable. Total bilirubin and liver enzymes were mildly elevated, and CBC was normal. Abdominal computed tomography showed a 4.0 x 0.5 cm tumor on the confluence of the right and left hepatic bile ducts with moderately dilated intrahepatic ducts. It also revealed a 2 cm tumor in the left kidney. Additional workup was negative for metastases.
Laparotomy was performed and revealed a hardened mass involving the common bile duct from above the implantation of the cystic duct to the confluence of the right and left hepatic ducts. Resection of the biliary tree was then carried out from the supraduodenal portion of the common bile duct to the first 2 cm of the right and left hepatic ducts, with en-bloc regional lymphadenectomy. A Roux-en-Y jejunal loop was taken to the hepatic hilum and right, left and caudate bile ducts were sewn to a single jejunal loop.
Macroscopic exam of the bile duct tumor revealed a 5.5x0.8cm surgical specimen that was firm and scirrhous tumor located on the confluence of the right and left hepatic ducts (Klatskin tumor). Bile duct confluence had a narrow lumen but no stones or mucin. Gallbladder had no stones or wall thickening.
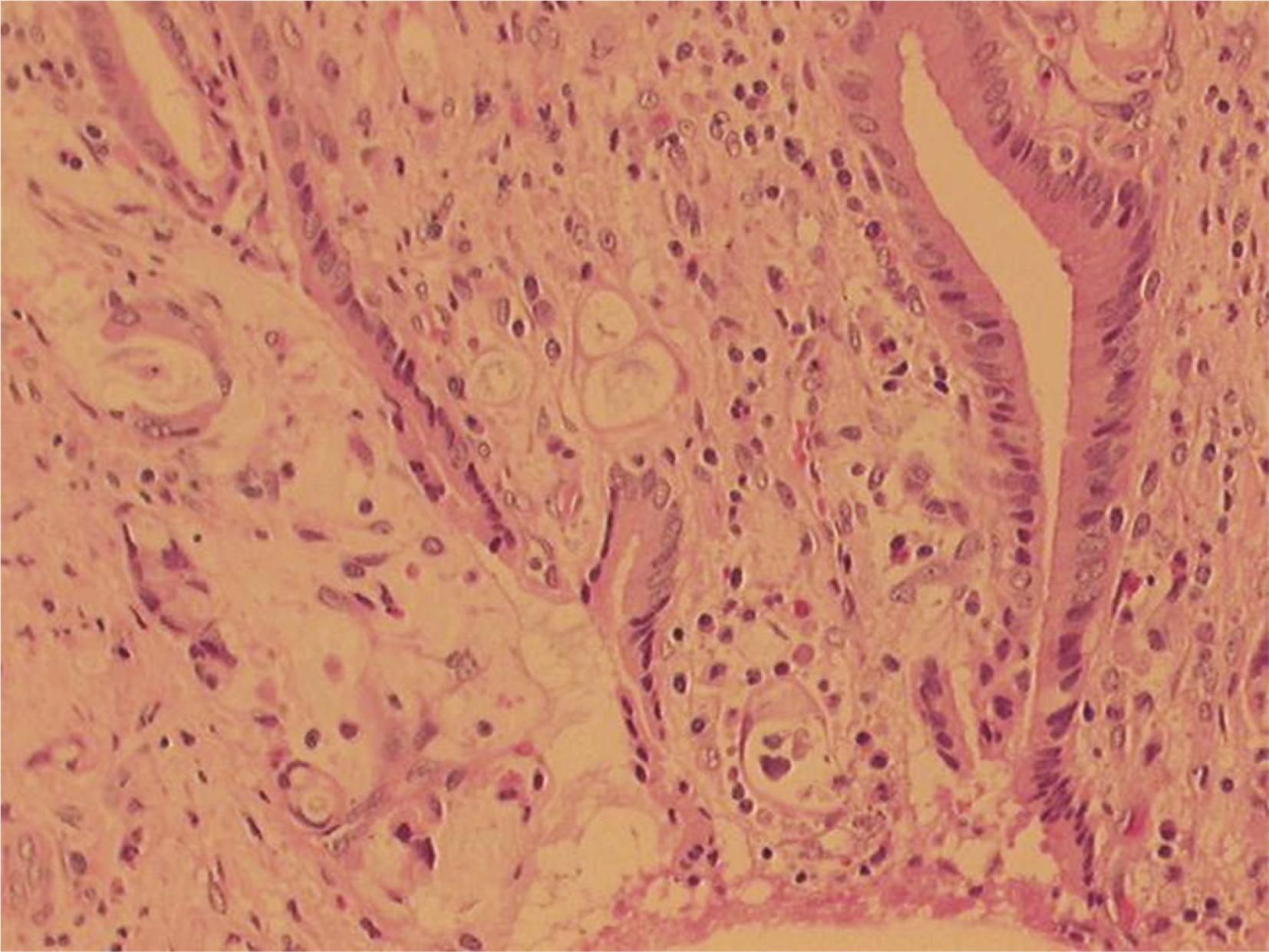
Pathology report revealed a poorly differentiated SRC hilar cholangiocarcinoma (UICC T4N0M0) with free proximal and distal margins and microscopically focally positive circumferential margins (Figure 1). Resected lymph nodes had no metastases.
Histological analysis: bile duct tumor with signetring cells (hematoxylin-eosin, x200); histological examination of the tumor revealed solid and infiltrative growth by pleomorphic round undifferentiated tumor cells with signet-ring morphology
The immunohistochemical profile confirmed the biliary origin of the SRC cancer (Figure 2A, 2B and 2C).
As frozen section of the intraoperative incisional biopsy of the left kidney tumor was suggestive of angiomyolipoma, nephrectomy was not performed at that time.
Postoperative course was complicated by a biliary leak, and patient was discharged home on 27th postoperative day. As the definitive pathology report for the kidney tumor revealed a clear cell renal carcinoma; the patient underwent a left radical nephrectomy after completely recovered from the first operation. Pathology report confirmed the diagnosis of renal cell carcinoma with free margins. Postoperative course was uneventful. Nevertheless, the patient died of local recurrence of SRC carcinoma 15 months after the first operation.
DISCUSSION
Three previous cases of primary biliary SRCC that have been reported in the English-language literature, all consisting of distal bile duct SRCCs occurring in Asian patients22 Hiraki M, Yakushiji H, Hashiguchil K et al. Signet ring cell carcinoma of the lower bile duct with rapid growth: report of a case. Hepatogastroenterology2007; 54:1922-1924.,44 Lee EY, Kim C, Kim MJ, et al. Signet ring cell carcinoma of theextrahepatic bile duct. Gut Liver 2010;4:402-6.,77 Ogata S, Kimura K, Hatsuse K et al. Poorly differentiated adenocarcinoma with signet-ring cell carcinoma of the extrahepatic bile duct in a 42-year-old Japanese female: a case report. Acta Med Okayama 2010;64:63-5.. Two of those patients underwent surgical resection of the primary tumor (pancreaticoduodenectomy). None of the previous bile duct SRC carcinomas consisted of a hilar cholangiocarcinoma (Klatskin tumor). Thus, to the best of our knowledge, this is the first report of a SRC of a signet-ring hilar cholangiocarcinoma. This is a relevant fact, since hilar cholangiocarcinomas carry a worse prognosis than distal bile duct cancers, being usually more aggressive and less amenable to surgical resection. Additionally, surgical treatment employed for hilar cholangiocarcinoma (bile duct resection with bilioenteric anastomoses) is different to the one used for lower bile duct cancers (pancreaticoduodenectomy).
Although risk factors for cholangiocarcinoma include primary sclerosing cholangitis, congenital biliary malformations, and parasitic liver disease, and hepatolithiasis, none of those was present in the case herein reported. This is the first report the occurrence of a SRC bile duct cancer in a Western patient, and this might be relevant since cholangiocarcinomas in the East possess epidemiology and etiology that are diverse to those bile duct cancers occurring in Western countries. A higher incidence of cholangiocarcinoma in the East has been largely credited to colonization by liver Opisthorchis viverrini and Clonorchis sinensis, liver flukes that may induce inflammatory changes in the biliary tree and are endemic in Asian countries.
Although one could hypothesize that SCR hilar cholangiocarcinomas would arise from gastric ectopic or metaplastic mucosa44 Lee EY, Kim C, Kim MJ, et al. Signet ring cell carcinoma of theextrahepatic bile duct. Gut Liver 2010;4:402-6., no evidence of gastric mucosa was found in the surgical specimen of the case reported herein. It has also been demonstrated that bile duct epithelium may undergo a sequence hyperplasia-metaplasia-dysplasia-carcinoma similarly to the one of intestinal-type gastric adenocarcinomas. Nevertheless, no evidence for such sequence was found in this case. In fact, biliary SRC carcinomas are poorly-differentiated aggressive tumors that may arise de novo as it is thought to occur in SRC gastric carcinomas. As happened in this case, most cholangiocarcinomas share expression of markers of progenitor cells such as CK7 and CK19. Thus, it is suggested that cholangiocarcinomas are monoclonal tumors that may arise from hepatobiliary pluripotent stem cells99 Roskams T (2006). Liver stem cells and their implication in hepatocellular and cholangiocarcinoma. Oncogene 2006; 25: 3818-22..
Another uncommon finding in the case presented here is the association between cholangiocarcinoma and clear cell renal cancer66 Levy BF, Nisar A, Karanjia ND. Cholangiocarcinoma, renal cell carcinoma and parathyroid adenoma found synchronously in a patient on long-term methotrexate. HPB (Oxford) 2006; 8:151-3.,88 Pachar JV, Crooks D, Ermocilla R: Hepatocholangiocarcinomaassociated with renal clear cell carcinoma. Rev Med Panama 1987; 12:37-40.. Although bile duct obstruction could have been attributed to the occurrence of a biliary metastasis from renal cell carcinoma1010 Ueda K, Ohori M, Taka J, Kusano M: Metastatic biliary polypoidthrombus from renal cell carcinoma: report of a case. Surg Today 2002; 32:458-61., immunohistochemical analysis confirmed the biliary epithelial origin in this case (positivity for CK19, CK07, CAM 5.2 and AE1+AE3)55 Lee MJ, Lee HS, Kim WH, Choi Y, Yang M: Expression of mucins andcytokeratins in primary carcinomas of the digestive system. Mod Pathol 2003; 16:403-410.. Renal cell clear carcinomas do not usually stain for all these markers. Although Levy et al.66 Levy BF, Nisar A, Karanjia ND. Cholangiocarcinoma, renal cell carcinoma and parathyroid adenoma found synchronously in a patient on long-term methotrexate. HPB (Oxford) 2006; 8:151-3. described the occurrence of simultaneous intrahepatic cholangiocarcinoma and a left kidney cancer in a patient on long-term use of methotrexate, there was no previous chronic use of any medications in this case88 Pachar JV, Crooks D, Ermocilla R: Hepatocholangiocarcinomaassociated with renal clear cell carcinoma. Rev Med Panama 1987; 12:37-40.. Thus, the association of a renal cell carcinoma with a SRC Klatskin tumor is likely to be fortuitous in this case.
Cholangiocarcinoma is an aggressive malignant tumor and it is possible that the presence of signet-ring cells could confer additional aggressiveness to this tumor. Further studies will be necessary to confirm or refute this hypothesis.
REFERENCES
-
1Gardner HA, Matthews J, Ciano PS: A signet-ring cell carcinoma of the ampulla of Vater. Arch Pathol Lab Med 1990; 114:1071-1072.
-
2Hiraki M, Yakushiji H, Hashiguchil K et al. Signet ring cell carcinoma of the lower bile duct with rapid growth: report of a case. Hepatogastroenterology2007; 54:1922-1924.
-
3Karabulut Z, Yildirim Y, Abaci I, Ilgici D, Ozyilkan O: Signet-ring cell carcinoma of the gallbladder: a case report. Adv Ther 2008; 25:520-23.
-
4Lee EY, Kim C, Kim MJ, et al. Signet ring cell carcinoma of theextrahepatic bile duct. Gut Liver 2010;4:402-6.
-
5Lee MJ, Lee HS, Kim WH, Choi Y, Yang M: Expression of mucins andcytokeratins in primary carcinomas of the digestive system. Mod Pathol 2003; 16:403-410.
-
6Levy BF, Nisar A, Karanjia ND. Cholangiocarcinoma, renal cell carcinoma and parathyroid adenoma found synchronously in a patient on long-term methotrexate. HPB (Oxford) 2006; 8:151-3.
-
7Ogata S, Kimura K, Hatsuse K et al. Poorly differentiated adenocarcinoma with signet-ring cell carcinoma of the extrahepatic bile duct in a 42-year-old Japanese female: a case report. Acta Med Okayama 2010;64:63-5.
-
8Pachar JV, Crooks D, Ermocilla R: Hepatocholangiocarcinomaassociated with renal clear cell carcinoma. Rev Med Panama 1987; 12:37-40.
-
9Roskams T (2006). Liver stem cells and their implication in hepatocellular and cholangiocarcinoma. Oncogene 2006; 25: 3818-22.
-
10Ueda K, Ohori M, Taka J, Kusano M: Metastatic biliary polypoidthrombus from renal cell carcinoma: report of a case. Surg Today 2002; 32:458-61.
-
Financial source: none
Publication Dates
-
Publication in this collection
Apr-Jun 2015
History
-
Received
27 Feb 2014 -
Accepted
08 Jan 2015