Abstract
Introduction:
Non-familial ascending thoracic aorta dilation and aneurysms (TAAs) are silent diseases in elderly patients. Histopathology revealed that functionally polarized infiltrating CD4+ T-cells play a key role in aortic wall weakening.
Objective:
To evaluate the possible associations between phenotype and cytokine production of circulating CD4+ T-lymphocytes and the presence of TAA in patients with aortic valve disease (AVD).
Methods:
We studied blood samples from 10 patients with TAA and 10 patients with AVD. Flow cytometry was used to quantify: a) CD4+ T-lymphocytes surface expression of CD25, CD28, and chemokine receptors (CCR5, CXCR3, CX3CR1); b) fractions of in vitro stimulated CD4+ T-cells producing cytokines (interferon gamma [IFN-γ], interleukin [IL]-17A, IL-21, IL-10); c) CD4+CD25highFoxP3+ regulatory T-cells (Treg) fraction. Enzyme-linked immunosorbent assays (ELISA) were performed for cytokines (IFN-γ, IL-6, IL-10, IL-17A, IL-23, transforming growth factor beta [TGF-β]) and chemokines (RANTES, CX3CL1).
Results:
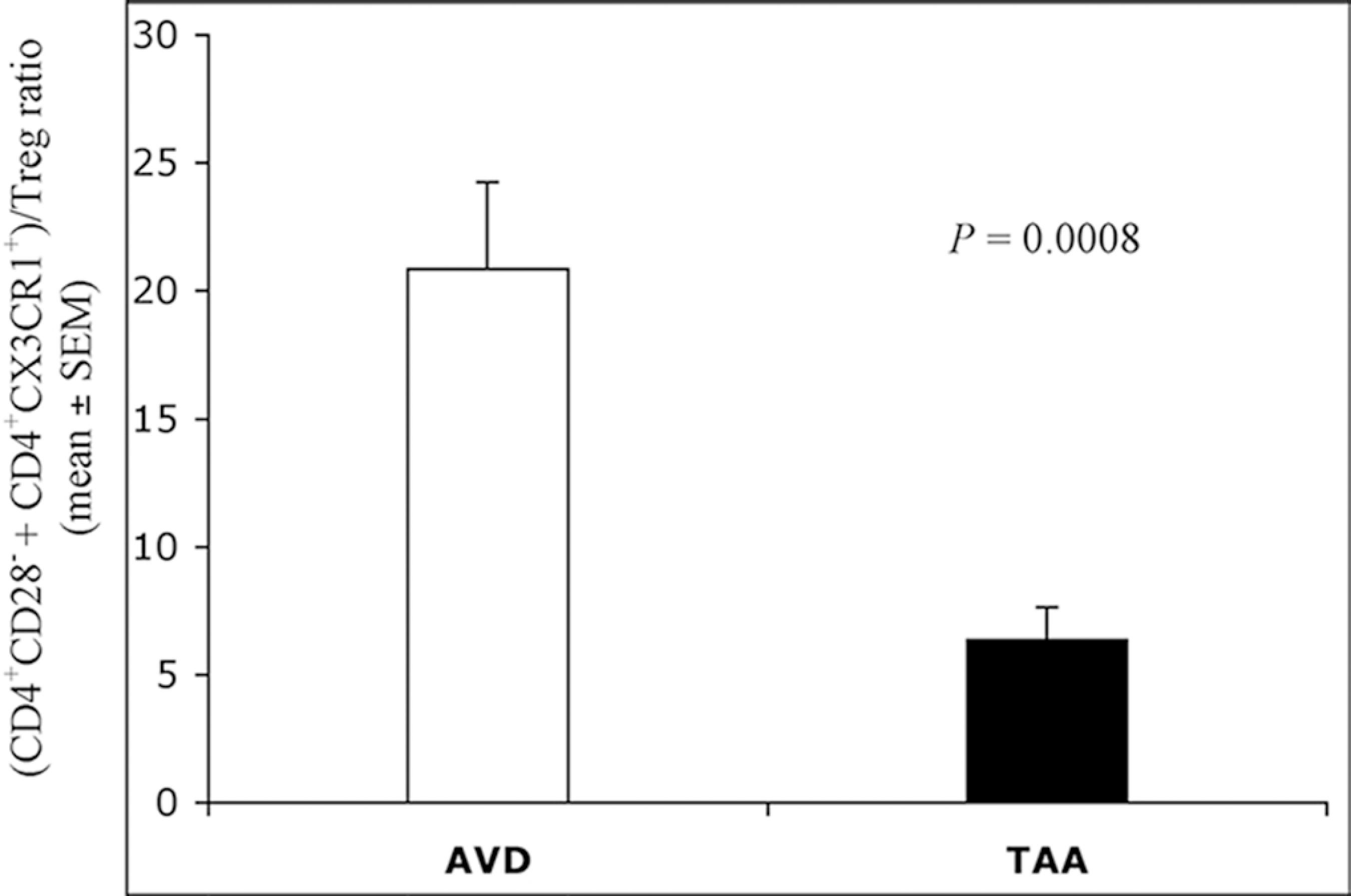
The total CD4+CD28±CD4+/CX3CR1+ T-cells fraction was higher (P=0.0323) in AVD (20.452±4.673) than in TAA patients (8.633±2.030). The frequency ratio of CD4+ T-lymphocytes producing IFN-γ vs. IL-17A+IL-21 cytokine-producing CD4+ T-cells was higher (P=0.0239) in AVD (2.102±0.272) than in TAA (1.365±0.123) patients. The sum of CD4+CD28±CD4+/CX3CR1+ T-cells correlated positively with values of the previous cytokine ratio (P=0.0002, R=0.732). The ratio of CD4+CD28±CD4+/CX3CR1+ T-cells vs. Treg was higher (P=0.0008) in AVD (20.859±3.393) than in TAA (6.367±1.277) patients.
Conclusion:
Our results show that the presence of TAA in subjects with AVD is associated with imbalance between phenotypic and cytokine-producing subsets of circulating CD4+ T-lymphocytes, prevalently oriented towards a pro-fibrotic and IFN-γ counteracting effect to functional polarization.
Keywords
Aortic Aneurysm, Thoracic; CD4-Positive T-Lymphocytes; Flow Cytometry
INTRODUCTION
The non-familial ascending thoracic aortic dilatations and thoracic aortic aneurysms (TAA) are frequent in individuals older than 65 years of age (approximately 6-9%), with a risk of rupture or dissection ranging from 2 to 3.5 cases per 100,000 patients/year[11 Elefteriades JA, Farkas EA. Thoracic aortic aneurysm clinically pertinent controversies and uncertainties. J Am Coll Cardiol. 2010;55(9):841-57.].
The progression from aortic dilatation to aneurysm is a multifactorial process partially undiscovered. Besides other well-known mechanisms[22 Bode-Jänisch S, Schmidt A, Günther D, Stuhrmann M, Fieguth A. Aortic dissecting aneurysms: histopathological findings. Forensic Sci Int. 2012;214(1-3):13-7.], the role of chronic immune-mediated inflammations in defining biomechanical properties of the aortic wall is still to be determined. In particular, the study of cellular and molecular mechanisms leading to aortic fibrosis, considered the histopathological marker of an altered vascular remodeling process[33 Wang X, LeMaire SA, Chen L, Shen YH, Gan Y, Bartsch H, et al. Increased collagen deposition and elevated expression of connective tissue growth factor in human thoracic aortic dissection. Circulation. 2006;114(1 Suppl):I200-5.], might be an important target in understanding the individual's susceptibility to non-syndromic ascending thoracic aortic dilatation and TAA formation. Recent findings in humans confirmed the key role of myofibroblasts (MF) in the extracellular matrix (ECM) proteolysis and deposition (fibrosis)[44 Forte A, Della Corte A, De Feo M, Cerasuolo F, Cipollaro M. Role of myofibroblasts in vascular remodelling: focus on restenosis and aneurysm. Cardiovasc Res. 2010;88(3):395-405.]. MF activity is modulated by a wide array of pro- and anti-fibrotic cytokines and growth factors released by mononuclear immune cells infiltrating the inflamed tissue[55 Wynn TA. Cellular and molecular mechanisms of fibrosis. J Pathol. 2008;214(2):199-210.]. Especially, the cytokines produced by CD4+ T-lymphocytes play a causative role in the initiation and progression of fibrosis associated with pathological conditions such as systemic sclerosis, atherosclerosis, and the use of silicone mammary implants[66 Wick G, Backovic A, Rabensteiner E, Plank N, Schwentner C, Sgonc R. The immunology of fibrosis: innate and adaptive responses. Trends Immunol. 2010;31(3):110-9.]. Given the crucial role of distinct CD4+ T-lymphocyte subsets in normal immune-regulation[77 Abbas AK, Murphy KM, Sher A. Functional diversity of helper T lymphocytes. Nature. 1996;383(6603):787-93.], the evaluation of their dynamic functional balance in terms of cell frequency ratio, either expressing a particular surface phenotype or producing selective signature cytokines, is an important tool to investigate whether a clinical pathological condition and its outcome are associated with a particular T-helper functional perturbation[88 Murphy KM, Stockinger B. Effector T cell plasticity: flexibility in the face of changing circumstances. Nat Immunol. 2010;11(8):674-80.,99 Liuzzo G, Montone RA, Gabriele M, Pedicino D, Giglio AF, Trotta F, et al. Identification of unique adaptive immune system signature in acute coronary syndromes. Int J Cardiol. 2013;168(1):564-7.].
To our knowledge, so far, no studies have related phenotype and function of peripheral blood CD4+ T-lymphocytes with the presence of TAA. Therefore, we have evaluated the presence of possible relationships between this pathological condition and: a) the expression of chemokine receptors and activation markers (CCR5, CXCR3, CX3CR1, CD25) on total blood CD4+ T-cell and on the pro-inflammatory/cytotoxic subset CD4+CD28-, known to be involved in vascular inflammation[1010 Zal B, Kaski JC, Arno G, Akiyu JP, Xu Q, Cole D, et al. Heat-shock protein 60-reactive CD4+CD28null T cells in patients with acute coronary syndromes. Circulation. 2004;109(10):1230-5.]; b) the cytokine production (interferon gamma [IFN-g, interleukin [IL]-17A, IL-21, IL-10) by in vitro stimulated CD4+ T-cells. Moreover, given their both beneficial and harmful roles in several clinical settings, including vascular injury[1111 Schiffrin EL. Immune mechanisms in hypertension and vascular injury. Clin Sci (Lond). 2014;126(4):267-74.], we quantified the circulating fraction of the CD4+CD25highFoxP3+ naturally occurring regulatory T-cells (Treg). On this basis, newly established phenotypic and functional blood CD4+ T-lymphocyte ratios, that overcome the traditional Th1/Th2 paradigm[1212 Gor DO, Rose NR, Greenspan NS. TH1-TH2: a procrustean paradigm. Nat Immunol. 2003;4(6):503-5.], have been calculated and related to the presence of an aortic aneurysm. We also measured the circulating levels of several cytokines (IFN-γ, IL-6, IL-10, IL-17A, IL-23, transforming growth factor beta [TGF-β]) and chemokines (RANTES, CX3CL1) known to influence CD4+ T-cells function and migration[1313 Sallusto F, Mackay CR. Chemoattractants and their receptors in homeostasis and inflammation. Curr Opin Immunol. 2004;16(6):724-31.
14 Nakayamada S, Takahashi H, KannoY, O'Shea JJ. Helper T cell diversity and plasticity. Curr Opin Immunol. 2012;24(3):297-302.-1515 Peters A, Lee Y, Kuchroo VK. The many faces of Th17 cells. Curr Opin Immunol. 2011;23(6):702-6.].
METHODS
Patients and Blood Samples
We have enrolled 20 patients undergoing surgery for aortic valve disease (AVD). TAA group (n=10) included patients undergoing aortic valve surgery with TAA surgery and AVD group (n=10) included patients undergoing surgery only for AVD, like stenosis or regurgitation, or both. Both groups underwent surgery by aortotomy. All patients had an indication for aortic valve surgery, according to current guidelines. TAA surgery was performed, if recommended by current guidelines. Exclusion criteria were the presence of genetic disorders, autoimmune and chronic inflammatory diseases, cancer, or hematological diseases. We enrolled patients with normal, ectasic or entirely aneurysmatic ascending aorta. Comorbidities, risk factors, and medical therapies were recorded, with particular attention to statins and/or angiotensin-converting enzyme (ACE) inhibitors, known to exert also immunomodulating effects[1616 Ulivieri C, Baldari CT. Statins: from cholesterol-lowering drugs to novel immunomodulators for the treatment of Th17-mediated autoimmune diseases. Pharmacol Res. 2014;88:41-52.
17 Platten M, Youssef S, Hur EM, Ho PP, Han MH, Lanz TV, et al. Blocking angiotensin-converting enzyme induces potent regulatory T cells and modulated Th1- and Th17-mediated autoimmunity. Proc Natl Acad Sci U S A. 2009;106(35):14948-53.-1818 Donato Aquaro G, Ait-Ali L, Basso ML, Lombardi M, Pingitore A, Festa P. Elastic properties of aortic wall in patients with bicuspid aortic valve by magnetic resonance imaging. Am J Cardiol. 2011;108(1):81-7.]. Mean and peak aortic gradients were measured by Doppler echocardiography and used to define the grade of stenosis. Aortic valve lesions were classified as predominant stenosis (mean transvalvular gradient ≥40 mmHg and grade of regurgitation <3+/4+), predominant regurgitation (grade of regurgitation 4+/4+ and mean gradient <40 mmHg), and steno-regurgitation, in other cases.
Venous blood was collected at the admission in Vacutainer tubes containing tripotassium ethylenediaminetetraacetic acid (K3-EDTA) or sodium-heparin as anticoagulants. Plasma was obtained after blood centrifugation and immediately frozen at -80°C. The protocol was approved by the local ethics committee and informed consent was obtained from each patient.
Data Acquisition and Analysis
Leukocyte count was carried out with a routine analyzer. Flow cytometry was performed with a FACS scan instrument equipped with a CellQuest software (Becton Dickinson). Quantification of lymphocyte surface markers expression and intracellular cytokines content was based on measurement of fraction (percentage) of positive events. Enzyme-linked immunosorbent assays (ELISA) were performed using the ASYS HITECH Microplate Reader (Eugendorf).
Surface Staining
Blood samples were processed as previously described for monocyte analysis[1919 Sbrana S, Bevilacqua S, Buffa M, Spiller D, Parri MS, Gianetti J, et al. Post-reperfusion changes of monocyte function in coronary blood after extracorporeal circulation. Cytometry B Clin Cytom. 2005;65(1):14-21.]. In brief, K3-EDTA samples were treated with a red cell lysing solution to isolate leukocytes, and then stained with the following combinations of phycoerythrin (PE)/cyanine 5 (Cy5) [PC5]-, fluorescein isothiocyanate (FITC)-, and (PE)-conjugated monoclonal antibodies: CD4/CD28/CD25; CD4/CD28/CCR5; CD4/CD28/CXCR3; CD4/CD28/CX3CR1. Isotype controls were performed. The antibodies used were from Becton Dickinson, Pharmingen, Immunotech, R&D Systems, and MBL International Corporation. The acquisition was stopped after 30,000 CD4+ T-lymphocytes were collected for each sample (Figure 1).
Identification of total CD4+ and CD4+CD28- T-lymphocyte subsets. Top: Selection of total CD4+ T-lymphocytes (R1) based on side scatter (SSC) properties and FL3 (CD4) bright fluorescence (A). R1-derived dot-plot of FL1 (CD28) versus FL3 (CD4) used to identify and quantify (as percentage) the CD4+CD28- T-lymphocyte fraction (R2) (B). Bottom: Example of quantification of CX3CR1 expression. The overlay of the FL2 fluorescence histograms is used to quantify the CX3CR1 positive cells (as percentage, events in M1, filled histograms) on the selected total CD4+ (R1 gated) (C) and CD4+CD28- (R1 + R2 gated) (D) T-cell subsets, when compared with isotype controls (dotted histograms).
Intracellular Cytokines
A whole blood staining procedure for intracellular cytokines detection was carried out as described[2020 Nomura LE, Walker JM, Maecker HT. Optimization of whole blood antigen-specific cytokine assays for CD4(+) T cells. Cytometry. 2000;40(1):60-8.]. In brief, heparinized samples were diluted 1:1 with RPMI (acronym for Roswell Park Memorial Institute) medium complete medium and incubated at a density of 2x106 leukocytes/ml for 5 hours, at 37°C. Phorbol myristate acetate (PMA) (Sigma Chemical Co.) (50 ng/ml) and ionomycin (1 mg/ml) were used as in vitro activators, in the presence of brefeldin A (eBioscience Inc.) (3 mg/ml final) as secretion blocking agent. Samples were then recovered, treated with a red cell lysing solution, and the isolated white blood cells (WBC) were stained with a combination of PC5- and FITC-conjugated monoclonal antibodies against the markers CD3 and CD4, respectively. Then, the cells were fixed with formaldehyde (2%) and permeabilized with saponin (0.5%). Cytokine staining was performed with PE-labeled monoclonal antibodies against IL-17A, IL-21, IFN-γ and IL-10. Isotype controls were performed. The acquisition was stopped after 30,000 CD3+ T-lymphocytes were collected for each sample (Figure 2).
Analysis of intracellular interferon gamma (IFN-y) production by CD4+ T-lymphocytes in activated whole blood samples, as example of cytokine-producing cells quantification by dot-plot quadrant statistics. Top: Selection of CD3+ T-lymphocytes (R1) based on side scatter (SSC) properties and FL3 (CD3) bright fluorescence (A). R1-derived dot-plot of FL2 (IFN-γ) vs. FL1 (CD4) used to select the CD4+ T-lymphocyte fraction (R2) (B). Bottom: Quantification (as percentage) of CD4+ T-cells producing IFN-γ (upper right quadrant, R1 + R2 gated) (D), when compared with isotype control (upper right quadrant, R1 + R2 gated) (C).
CD4+CD25highFoxP3+ Regulatory T-cells
Blood samples were processed as published[2121 Grant J, Bourcier K, Wallace S, Pan D, Conway A, Seyfert-Margolis V, et al. Validated protocol for FoxP3 reveals increased expression in type 1 diabetes patients. Cytometry B Clin Cytom. 2009;76(2):69-78.], with minor modifications. In brief, K3-EDTA samples were lysed as described before and the isolated WBC stained with PC5- and PE-conjugated monoclonal antibodies against the markers CD4 and CD25, respectively. Then, cells were fixed, permeabilized, and stained with an Alexa Fluor 488-conjugated anti-human forkhead-box-P3 (FoxP3) monoclonal antibody (eBioscience Inc.). Isotype controls were performed. Treg cells fraction was quantified into the 2% of CD4+CD25high double positive events, as reported[2222 Baecher-Allan C, Brown JA, Freeman GJ, Hafler DA. CD4+CD25high regulatory cells in human peripheral blood. J Immunol. 2001;167(3):1245-53.]. The acquisition was stopped after 30,000 CD4+ T-lymphocytes were collected for each sample (Figure 3).
Gating sequence used to quantify the frequency of regulatory T-cells (Treg). Top: Identification of CD4+ T-lymphocytes (R1) based on side scatter (SSC) properties and FL3 (CD4) bright fluorescence (A). R1-derived dot-plot of FL2 (CD25) vs. FL3 (CD4) used to select the CD25high positive events at the top 2% of CD4+CD25+ T-cells (R2) (B). Bottom: The overlay of Alexa Fluor-488 FL1 fluorescence histograms is used to quantify the percentage of FoxP3+ cells (events in M1, filled histogram) (C), when compared with isotype control (dotted histogram). By multiplying the above 2 percentages and dividing them by 100, the CD4+CD25highFoxP3+ (Treg) cell fraction is calculated.
ELISA
Plasma levels of IFN-γ, IL-6, IL-10, IL-17A, IL-23, TGF-β, RANTES, and CX3CL1 were quantified by ELISA kits (R&D Systems) according to the manufacturer's protocol. Minimum detectable concentrations were 15.6 pg/ml (IFN-γ, 0.156 pg/ml (IL-6), 0.78 pg/ml (IL-10), 31.25 pg/ml (IL-17A), 39.0 pg/ml (IL-23), 0.031 ng/ml (TGF-β, 0.031 ng/ml (RANTES), and 0.156 ng/ml (CX3CL1).
Statistical Analysis
The calculation of mean values and standard errors of the mean (± SEM), as well as the determination of linear correlations among continuous variables, was carried out with the StatView 5.0 software. The existence of statistically significant differences between groups was explored by analysis of variance (ANOVA) Student's t-test for unpaired data. Chi-squares statistical analysis was used for comparison between nominal variables. P<0.05 was considered statistically significant.
RESULTS
General Findings
Mean aortic diameters were 35.50 ± 1.65 mm (range 27-43 mm) and 48.90 ± 1.18 mm (range 45-56 mm) in AVD and TAA groups, respectively (P<0.0001). At the operation, 8 patients had an isolated ascending aorta replacement and 2 underwent combined aortic root surgery. Clinical and surgical characteristics of patients are reported in Table 1.
The mean frequency (± SEM) of CD4+ T-lymphocytes was 46.39±1.99; their absolute number (number of cells/ml) was 953.34±61.85, accordingly with published CD4+ T-cell reference values during aging[2323 Provinciali M, Moresi R, Donnini A, Lisa RM. Reference values for CD4+ and CD8+ T lymphocytes with naïve or memory phenotype and their association with mortality in the elderly. Gerontology. 2009;55(3):314-21.]. The mean percentage (± SEM) of CD4+ T-cells belonging to the pro-inflammatory/cytotoxic subset CD4+CD28- was 5.56±1.33; this value, if referred to the age's range of our patients, is also in accord with literature data[2424 Weng NP, Akbar AN, Goronzy J. CD28(-) T cells: their role in the age-associated decline of immune function. Trends Immunol. 2009;30(7):306-12.]. Cumulative analysis of surface markers expression on total CD4+ and CD4+CD28- T-cell subsets are reported in Table 2.
Surface marker expression on blood total CD4+and CD4+CD28- T-cell subsets (percentage of positivity, mean ±SEM) (20 patients).
The measurement of plasma cytokines/chemokines is reported in Table 3.
No relationship has been found between the plasma levels of cytokines/chemokines and CD4+ T-cells phenotypes, intracellular cytokines levels, and presence of TAA, respectively. Cumulative quantification of intracellular cytokines is reported in Table 4; also, these data are in accordance with published T-cell cytokines levels in normal aging[2525 Hoffmann F, Albert MH, Arenz S, Bidlingmaier C, Berkowicz N, Sedlaczek S, et al. Intracellular T-cell cytokine levels are age-dependent in healthy children and adults. Eur Cytokine Netw. 2005;16(4):283-8.].
Intracellular cytokine production by "in vitro" stimulated CD4+ T-lymphocytes in whole blood samples (percentage of positivity, mean ± SEM) (20 patients).
Relationships among CD4+ T-cells Phenotypic Subsets
The accumulation of CD28- T-cells in aging is driven by a repeated cellular activation, leading also to a modulation of CD4+ T-cells chemokine receptors expression[2424 Weng NP, Akbar AN, Goronzy J. CD28(-) T cells: their role in the age-associated decline of immune function. Trends Immunol. 2009;30(7):306-12.,2626 Valenzuela HF, Effros RB. Divergent telomerase and CD28 expression patterns in human CD4 and CD8 T cells following repeated encounters with the same antigenic stimulus. Clin Immunol. 2002;105(2):117-25.]. In our patients, a tightly positive correlation between the circulating fraction of CD4+CD28- T-cells and the frequency of CD4+ T-lymphocytes carrying the fractalkine receptor CX3CR1 (CD4+/CX3CR1+) (P<0.0001, R=0.934) has been observed.
Relationships among CD4+ T-cells Phenotype/Function and TAA
The sum of blood CD4+CD28±CD4+/CX3CR1+ T-cells fractions was significantly lower in the TAA group than in the AVD group (Figure 4).
Total fraction (percentage) of circulating CD4+CD28±CD4+/CX3CR1+ T-cells in AVD (white bar) and TAA (black bar) patients. Statistical comparison between percentages (mean ± SEM) was performed with ANOVA Student's t-test for unpaired data. Statistically significant differences (P<0.05) were detected. The functional balance (ratio) between the blood frequency of CD4+ T-lymphocytes producing IFN-γ vs. the total fraction of IL-17A+IL-21 cytokine-producing CD4+ T-cells was significantly lower in the TAA group (Figure 5A).
ANOVA=analysis of variance; AVD=aortic valve disease; IFN-γ=interferon gamma; IL=interleukin; SEM=standard error of the mean; TAA=thoracic aortic aneurysm
For each patient, the sum of CD4+CD28±CD4+/CX3CR1+ T-cell fractions correlated positively with the corresponding values of the above-mentioned cytokine ratio (Figure 5).
(A) Ratio between the blood frequency of CD4+ T-lymphocytes producing IFN-γ vs. the total fraction of IL-17A+IL-21 cytokine-producing CD4+ T-cells in AVD (white bar) and TAA (black bar) patients. Statistical comparison between ratios (mean ± SEM) was performed with ANOVA Student's t-test for unpaired data. Statistically significant differences (P<0.05) were detected. (B) Linear regression between the individual fractions (percentages) of circulating CD4+CD28±CD4+/CX3CR1+ T-cells (x axis) and the corresponding IFN-γ/(IL-17A+IL-21) cytokine ratios (y axis) in all patients.
ANOVA=analysis of variance; AVD=aortic valve disease; IFN-γ=interferon gamma; IL=interleukin; SEM=standard error of the mean; TAA=thoracic aortic aneurysm
The mean value (± SEM) of blood Treg, expressed as a percentage of total CD4+ T-cells, was 1.19±0.09; no statistically significant differences have been observed between the 2 groups of patients. The frequency ratio of CD4+CD28±CD4+/CX3CR1+ T-cells vs. circulating Treg was significantly lower in the TAA group than in the AVD group (Figure 6).
Frequency ratio of blood CD4+CD28±CD4+/CX3CR1+ T-cells vs. Treg in AVD (white bar) and TAA (black bar) patients. Statistical comparison between ratios (mean ± SEM) was performed with ANOVA Student's t-test for unpaired data. Statistically significant differences (P<0.05) were detected.
ANOVA=analysis of variance; AVD=aortic valve disease; SEM=standard error of the mean; TAA=thoracic aortic aneurysm; Treg=regulatory T-cells
CD4+ T-cells Phenotype/Function, Aortic Valve Pathology, and Clinical Features
No correlation has been found between all the above-mentioned phenotypic and functional CD4+ T-cell features and the patients' ages. Student's t-test and linear regression statistical analysis did not show significant associations between immunological parameters and patients' clinical characteristics, such as the prevalent type of valve pathology, aortic valve mean gradient values, associated risk factors, and current medical therapies. The mean functional ratio of IFN-γ vs. IL-17A+IL-21 cytokine-producing CD4+ T-cells was significantly higher (P=0.0228) in female (2.144±279) than in male patients (1.398±0.147). On the other hand, the Chi-squares statistical analysis did not evidence a significant association between sex differences and the presence of TAA.
DISCUSSION
Clinical and experimental studies carried out in abdominal aortic aneurysms by histological and immunohistochemical procedures proved that a predominant Th2-mediated immune response, mainly driven by IL-4, IL-5, or IL-10 cytokines, induces severe aneurysm formations[2727 Shimizu K, Shichiri M, Libby P, Lee RT, Mitchell RN. Th2-predominant inflammation and blockade of IFN-gamma signaling induce aneurysms in allografted aortas. J Clin Invest. 2004;114(2):300-8.]. On the other hand, a prevalent Th1-mediated immune response, sustained by the infiltration of mononuclear cells releasing IFN-γ and IL-12, has been demonstrated to be responsible for transmural inflammation and external vessel wall dilatation in ascending TAA[2828 Tang PC, Yakimov AO, Teesdale MA, Coady MA, Dardik A, Elefteriades JA, et al. Transmural inflammation by interferon-gamma-producing T cells correlates with outward vascular remodeling and intimal expansion of ascending thoracic aortic aneurysm. FASEB J. 2005;19(11):1528-30.]. Nevertheless, independently of their localization, both types of dilating aortic lesions are characterized by common histopathological findings, also including evident modifications of ECM turnover with overexpressed collagen deposition and fibrosis[22 Bode-Jänisch S, Schmidt A, Günther D, Stuhrmann M, Fieguth A. Aortic dissecting aneurysms: histopathological findings. Forensic Sci Int. 2012;214(1-3):13-7.
3 Wang X, LeMaire SA, Chen L, Shen YH, Gan Y, Bartsch H, et al. Increased collagen deposition and elevated expression of connective tissue growth factor in human thoracic aortic dissection. Circulation. 2006;114(1 Suppl):I200-5.-44 Forte A, Della Corte A, De Feo M, Cerasuolo F, Cipollaro M. Role of myofibroblasts in vascular remodelling: focus on restenosis and aneurysm. Cardiovasc Res. 2010;88(3):395-405.]. As known, the ECM remodeling, with fibroblasts activation and development of fibrosis, occurring in pathological conditions, such as systemic sclerosis, atherosclerosis, parasitic infections, and after the use of silicone mammary implants, is suppressed by a locally polarized Th1 IFN-γ-driven immune response[55 Wynn TA. Cellular and molecular mechanisms of fibrosis. J Pathol. 2008;214(2):199-210.,66 Wick G, Backovic A, Rabensteiner E, Plank N, Schwentner C, Sgonc R. The immunology of fibrosis: innate and adaptive responses. Trends Immunol. 2010;31(3):110-9.].
In spite of the histological demonstration of a prevalent Th1-mediated immune response into the wall of dilated and/or aneurysmatic ascending thoracic aortas, so far little is known about the systemic immunological status of these patients. Therefore, in our study, we evaluated several phenotypic and functional features of peripheral blood CD4+ T-lymphocytes in patients undergoing a cardiac operation for aortic valve replacement associated, or not, with elective surgery for TAA.
We have found out that the cumulative CD4+ T-cell fraction calculated by percentage addition of circulating CD4+CD28- T-cells, a subset of cytotoxic T-lymphocytes producing large amount of IFN-γ[2929 van de Berg PJ, van Leeuwen EM, ten Berge IJ, van Lier R. Cytotoxic human CD4(+) T cell. Curr Opin Immunol. 2008;20(3):339-43.], plus CD4+ T-cells carrying the fractalkine receptor CX3CR1 (CD4+/CX3CR1+), preferentially expressed on Th1 IFN-γ-producing cells[3030 Umehara H, Bloom ET, Okazaki T, Domae N, Imai T.. Fractalkine and vascular injury. Trends Immunol. 2001;22(11):602-7.], is significantly lower in the TAA group than in the AVD group.
A prevalent pro-fibrotic IL-17A/IL-21-driven polarization of blood CD4+ T-lymphocytes in the TAA group seems to be demonstrated, in our study, by the significantly lower mean ratio observed between the frequency of CD4+ T-lymphocytes producing the anti-fibrotic IFN-γ vs. the total fraction of IL-17A+IL-21 pro-fibrotic cytokine-producing CD4+ T-cells[66 Wick G, Backovic A, Rabensteiner E, Plank N, Schwentner C, Sgonc R. The immunology of fibrosis: innate and adaptive responses. Trends Immunol. 2010;31(3):110-9.,3131 Monteleone G, Pallone F, MacDonald TT. Interleukin-21: a critical regulator of the balance between effector and regulatory T-cell responses. Trends Immunol. 2008;29(6):290-4.,3232 Tan Z, Qian X, Jiang R, Liu Q, Wang Y, Chen C, et al. IL-17A plays a critical role in the pathogenesis of liver fibrosis through hepatic stellate cell activation. J Immunol. 2013;191(4):1835-44.].
Previous papers demonstrated that human fibrocytes are potent antigen-presenting cells (APC) capable of priming naive T-cells in situ [3333 Chesney J, Bacher M, Bender A, Bucala R. The peripheral blood fibrocyte is a potent antigen-presenting cell capable of priming naive T cells in situ. Proc Natl Acad Sci U S A. 1997;94(12):6307-12.]. Since the requirement of a more broad T-cell/APC cross-talk via CD40-CD40L interactions for generation of Th17- than for Th1 IFN-γ-mediated inflammatory responses[3434 Katzman SD, Gallo E, Hoyer KK, Abbas AK. Differential requirements for Th1 and Th17 responses to a systemic self-antigen. J Immunol. 2011;186(8):4668-73.,3535 Hayashi H, Kawakita A, Okazaki S, Yasutomi M, Murai H, Ohshima Y. IL-17A/F modulates fibrocyte functions in cooperation with CD40-mediated signaling. Inflammation. 2013;36(4):830-8.], our data suggest that the higher extent of fibrotic tissue may orientate aneurysmatic aorta tissue-resident T-cells towards a prevalent production of IL-17A and IL-21, so creating a self-maintaining loop for further fibrocyte priming, collagen production, and pro-fibrotic tissue remodeling.
The close correlation existing between the individual values of the IFN-γ/(IL-17A + IL-21) functional ratio and the CD4+CD28±CD4+/CX3CR1+ T-cell fraction indicates that the association of these last phenotypic T-cell subsets is strictly involved in the establishment of a prevalently IFN-γ-oriented blood CD4+ T-cell polarization in AVD subjects without TAA.
Moreover, while previous papers showed that Treg and IL-10-producing CD4+ T-lymphocytes separately suppress collagen deposition and tissue fibrosis in several chronic inflammatory conditions[55 Wynn TA. Cellular and molecular mechanisms of fibrosis. J Pathol. 2008;214(2):199-210.], apparently cooperating with the anti-fibrotic action of IFN-10-producing CD4+ T-cells, the significantly lower ratio of total CD4+CD28± CD4+/CX3CR1+ T-cell vs. Treg observed in our TAA patients suggests that a tissue IFN-γ counter-acting effect of Treg, mainly sustained by IL-10 production[3636 Cretney E, Kallies A, Nutt SL. Differentiation and function of Foxp3(+) effector regulatory T cells. Trends Immunol. 2013;34(2):74-80.], could be detrimental for this specific pathological condition.
Previous papers have shown that circulating T-cells represent an important repository pool to reveal tissue-resident T-cell functional abnormalities in immune-mediated connective pathologies, such as systemic sclerosis, characterized by a deregulated fibroblast activation leading to fibrosis of internal organs[3737 Brembilla NC, Chizzolini C. T cell abnormalities in systemic sclerosis with a focus on Th17 cells. Eur Cytokine Netw. 2012;23(4):128-39.]. Moreover, it has been demonstrated that the evaluation of balanced dynamic inter-relationships among different phenotypic/functional characteristics of blood CD4+ T-cell subsets can identify unique immunological features correlating with the clinical outcome and therapeutic interventions in selected cardiovascular patients[99 Liuzzo G, Montone RA, Gabriele M, Pedicino D, Giglio AF, Trotta F, et al. Identification of unique adaptive immune system signature in acute coronary syndromes. Int J Cardiol. 2013;168(1):564-7.].
CONCLUSION
We conclude that there is a presence of an immunological imbalance in the form of fibrocyte activation and Treg differentiation leading to the development of an aortic aneurysm in patients with AVD. On this basis, eventually, a targeted therapeutic model could be developed if it is confirmed in a large number of patients with TAA, including subjects with aortic rupture/dissection.
-
This study was carried out at the College of Medical Sciences, Teaching Hospital, Bharatpur, Chitwan, Nepal.
-
Financial support: This study was funded by the National Research Council (CNR) of Italy, RSTL (Curiosity Driven Research Program) DG.RSTL.035.006-035.
-
Fast Track
ACKNOWLEDGMENTS
The authors wish to express their appreciation to the personnel of the "G. Pasquinucci" Heart Hospital operating theater, intensive care unit, and laboratory departments.
REFERENCES
-
1Elefteriades JA, Farkas EA. Thoracic aortic aneurysm clinically pertinent controversies and uncertainties. J Am Coll Cardiol. 2010;55(9):841-57.
-
2Bode-Jänisch S, Schmidt A, Günther D, Stuhrmann M, Fieguth A. Aortic dissecting aneurysms: histopathological findings. Forensic Sci Int. 2012;214(1-3):13-7.
-
3Wang X, LeMaire SA, Chen L, Shen YH, Gan Y, Bartsch H, et al. Increased collagen deposition and elevated expression of connective tissue growth factor in human thoracic aortic dissection. Circulation. 2006;114(1 Suppl):I200-5.
-
4Forte A, Della Corte A, De Feo M, Cerasuolo F, Cipollaro M. Role of myofibroblasts in vascular remodelling: focus on restenosis and aneurysm. Cardiovasc Res. 2010;88(3):395-405.
-
5Wynn TA. Cellular and molecular mechanisms of fibrosis. J Pathol. 2008;214(2):199-210.
-
6Wick G, Backovic A, Rabensteiner E, Plank N, Schwentner C, Sgonc R. The immunology of fibrosis: innate and adaptive responses. Trends Immunol. 2010;31(3):110-9.
-
7Abbas AK, Murphy KM, Sher A. Functional diversity of helper T lymphocytes. Nature. 1996;383(6603):787-93.
-
8Murphy KM, Stockinger B. Effector T cell plasticity: flexibility in the face of changing circumstances. Nat Immunol. 2010;11(8):674-80.
-
9Liuzzo G, Montone RA, Gabriele M, Pedicino D, Giglio AF, Trotta F, et al. Identification of unique adaptive immune system signature in acute coronary syndromes. Int J Cardiol. 2013;168(1):564-7.
-
10Zal B, Kaski JC, Arno G, Akiyu JP, Xu Q, Cole D, et al. Heat-shock protein 60-reactive CD4+CD28null T cells in patients with acute coronary syndromes. Circulation. 2004;109(10):1230-5.
-
11Schiffrin EL. Immune mechanisms in hypertension and vascular injury. Clin Sci (Lond). 2014;126(4):267-74.
-
12Gor DO, Rose NR, Greenspan NS. TH1-TH2: a procrustean paradigm. Nat Immunol. 2003;4(6):503-5.
-
13Sallusto F, Mackay CR. Chemoattractants and their receptors in homeostasis and inflammation. Curr Opin Immunol. 2004;16(6):724-31.
-
14Nakayamada S, Takahashi H, KannoY, O'Shea JJ. Helper T cell diversity and plasticity. Curr Opin Immunol. 2012;24(3):297-302.
-
15Peters A, Lee Y, Kuchroo VK. The many faces of Th17 cells. Curr Opin Immunol. 2011;23(6):702-6.
-
16Ulivieri C, Baldari CT. Statins: from cholesterol-lowering drugs to novel immunomodulators for the treatment of Th17-mediated autoimmune diseases. Pharmacol Res. 2014;88:41-52.
-
17Platten M, Youssef S, Hur EM, Ho PP, Han MH, Lanz TV, et al. Blocking angiotensin-converting enzyme induces potent regulatory T cells and modulated Th1- and Th17-mediated autoimmunity. Proc Natl Acad Sci U S A. 2009;106(35):14948-53.
-
18Donato Aquaro G, Ait-Ali L, Basso ML, Lombardi M, Pingitore A, Festa P. Elastic properties of aortic wall in patients with bicuspid aortic valve by magnetic resonance imaging. Am J Cardiol. 2011;108(1):81-7.
-
19Sbrana S, Bevilacqua S, Buffa M, Spiller D, Parri MS, Gianetti J, et al. Post-reperfusion changes of monocyte function in coronary blood after extracorporeal circulation. Cytometry B Clin Cytom. 2005;65(1):14-21.
-
20Nomura LE, Walker JM, Maecker HT. Optimization of whole blood antigen-specific cytokine assays for CD4(+) T cells. Cytometry. 2000;40(1):60-8.
-
21Grant J, Bourcier K, Wallace S, Pan D, Conway A, Seyfert-Margolis V, et al. Validated protocol for FoxP3 reveals increased expression in type 1 diabetes patients. Cytometry B Clin Cytom. 2009;76(2):69-78.
-
22Baecher-Allan C, Brown JA, Freeman GJ, Hafler DA. CD4+CD25high regulatory cells in human peripheral blood. J Immunol. 2001;167(3):1245-53.
-
23Provinciali M, Moresi R, Donnini A, Lisa RM. Reference values for CD4+ and CD8+ T lymphocytes with naïve or memory phenotype and their association with mortality in the elderly. Gerontology. 2009;55(3):314-21.
-
24Weng NP, Akbar AN, Goronzy J. CD28(-) T cells: their role in the age-associated decline of immune function. Trends Immunol. 2009;30(7):306-12.
-
25Hoffmann F, Albert MH, Arenz S, Bidlingmaier C, Berkowicz N, Sedlaczek S, et al. Intracellular T-cell cytokine levels are age-dependent in healthy children and adults. Eur Cytokine Netw. 2005;16(4):283-8.
-
26Valenzuela HF, Effros RB. Divergent telomerase and CD28 expression patterns in human CD4 and CD8 T cells following repeated encounters with the same antigenic stimulus. Clin Immunol. 2002;105(2):117-25.
-
27Shimizu K, Shichiri M, Libby P, Lee RT, Mitchell RN. Th2-predominant inflammation and blockade of IFN-gamma signaling induce aneurysms in allografted aortas. J Clin Invest. 2004;114(2):300-8.
-
28Tang PC, Yakimov AO, Teesdale MA, Coady MA, Dardik A, Elefteriades JA, et al. Transmural inflammation by interferon-gamma-producing T cells correlates with outward vascular remodeling and intimal expansion of ascending thoracic aortic aneurysm. FASEB J. 2005;19(11):1528-30.
-
29van de Berg PJ, van Leeuwen EM, ten Berge IJ, van Lier R. Cytotoxic human CD4(+) T cell. Curr Opin Immunol. 2008;20(3):339-43.
-
30Umehara H, Bloom ET, Okazaki T, Domae N, Imai T.. Fractalkine and vascular injury. Trends Immunol. 2001;22(11):602-7.
-
31Monteleone G, Pallone F, MacDonald TT. Interleukin-21: a critical regulator of the balance between effector and regulatory T-cell responses. Trends Immunol. 2008;29(6):290-4.
-
32Tan Z, Qian X, Jiang R, Liu Q, Wang Y, Chen C, et al. IL-17A plays a critical role in the pathogenesis of liver fibrosis through hepatic stellate cell activation. J Immunol. 2013;191(4):1835-44.
-
33Chesney J, Bacher M, Bender A, Bucala R. The peripheral blood fibrocyte is a potent antigen-presenting cell capable of priming naive T cells in situ. Proc Natl Acad Sci U S A. 1997;94(12):6307-12.
-
34Katzman SD, Gallo E, Hoyer KK, Abbas AK. Differential requirements for Th1 and Th17 responses to a systemic self-antigen. J Immunol. 2011;186(8):4668-73.
-
35Hayashi H, Kawakita A, Okazaki S, Yasutomi M, Murai H, Ohshima Y. IL-17A/F modulates fibrocyte functions in cooperation with CD40-mediated signaling. Inflammation. 2013;36(4):830-8.
-
36Cretney E, Kallies A, Nutt SL. Differentiation and function of Foxp3(+) effector regulatory T cells. Trends Immunol. 2013;34(2):74-80.
-
37Brembilla NC, Chizzolini C. T cell abnormalities in systemic sclerosis with a focus on Th17 cells. Eur Cytokine Netw. 2012;23(4):128-39.
Publication Dates
-
Publication in this collection
Jan-Feb 2019
History
-
Received
01 Oct 2018 -
Accepted
02 Oct 2018