Abstracts
PURPOSE: To carry out an anatomic study of superior laryngeal nerve in not preserved in formaldehyde and not frozen corpses. METHODS: Thirty-eight male corpses from the Minas Gerais Medico-legal Institute (IML) were studied. In 18 corpses dissection was performed bilaterally and in 20 only on the left side, total number 56 nerves dissected. Their descriptive segments measurements and the anatomic relations with the cervical structures of the region were described. This nerve was statistically analyzed; the variables were corpse side (Friedman´s test (p<0.05), height (Pearson), racial group (Kruskal-Wallis). RESULTS: The superior laryngeal nerve presented a definite anatomical disposition in all the 56 nerves studied, emerging from the nervus vagus inferior ganglion. The superior laryngeal nerve trunk was in average longer in corpses over 25 years old (p<0.05). Significant differences (p<0.05) between the internal and external branches were observed in all racial groups, and the internal branch average was inferior to the external branch average. There were not significant differences between the 18 studied corpses' left and right sides paired measurements. CONCLUSIONS: Concerning emergence, trunk, bifurcation and major branches, the 56 studied nerves disposition had a definite anatomic pattern. The superior laryngeal nerve trunk was in average longer in corpses over 25 years old. In this study, the external branch of the laryngeal nerve was in average longer than the internal branch.
Laryngeal Nerves; Anatomy; Surgery; Cadaver
OBJETIVO: Realizar um estudo anatômico do nervo laríngeo superior através da dissecção em cadáver não formolizado e não congelado. MÉTODOS: 38 cadáveres do sexo masculino, provenientes do Instituto Médico-Legal de Minas Gerais (IML), foram estudados. Em 18 cadáveres a dissecção foi realizada bilateralmente e em 20 somente do lado esquerdo, totalizando 56 nervos. Foram registradas as medidas descritivas dos seus segmentos e as relações anatômicas com as estruturas cervicais da região. Este nervo foi analisado sob o ponto de vista estatístico, com as variáveis: lado (teste de Friedman p<0,05), altura e idade (Pearson) e etnia (Kruskal-Wallis). RESULTADOS: O nervo laríngeo superior apresentou uma disposição anatômica definida em todos os 56 nervos estudados, emergindo do gânglio inferior do nervo vago. O tronco do nervo laríngeo superior foi em média mais longo nos cadáveres acima de 25 anos de idade (p<0,05). Foram observadas diferenças significativas (p<0,05) entre as medidas do ramo interno e do ramo externo em todos os grupos étnicos, sendo que a média do ramo interno foi inferior à média do ramo externo. As medidas pareadas dos lados direito e esquerdo não apresentaram diferenças significativas nos 18 cadáveres estudados. CONCLUSÕES: A disposição dos 56 nervos laríngeos superiores mostrou um padrão anatômico definido, quanto à emergência, ao tronco, à bifurcação e aos ramos principais. O tronco do nervo laríngeo superior foi em média mais longo nos cadáveres acima de 25 anos de idade. O comprimento do ramo externo do nervo laríngeo superior foi em média maior do que o do ramo interno, neste estudo.
Nervos Laríngeos; Anatomia; Cirurgia; Cadáver
ORIGINAL ARTICLE
Superior laryngeal nerve anatomy in corpses not preserved in formaldehyde. Contribution to the operative technique1 1 Research performed at Medicolegal Institute, Minas Gerais, Brazil.
Anatomia do nervo laríngeo superior em cadáver não formalizado. Contribuição para a técnica operatória
Ludércio Rocha de OliveiraI; Alcino Lázaro da SilvaII
IAssistant Professor, Surgery Department, School of Medicine, Minas Gerais, Brazil
IIFull Professor, Digestive System Surgery, Department of Surgery, Federal University of Minas Gerais (UFMG), Brazil
Correspondence Correspondence: Dr. Ludércio Rocha de Oliveira Rua Ceará, 1850/300 30150-311 Belo Horizonte MG Brazil Phone: (55 31)3223-4279
ABSTRACT
PURPOSE: To carry out an anatomic study of superior laryngeal nerve in not preserved in formaldehyde and not frozen corpses.
METHODS: Thirty-eight male corpses from the Minas Gerais Medico-legal Institute (IML) were studied. In 18 corpses dissection was performed bilaterally and in 20 only on the left side, total number 56 nerves dissected. Their descriptive segments measurements and the anatomic relations with the cervical structures of the region were described. This nerve was statistically analyzed; the variables were corpse side (Friedman´s test (p<0.05), height (Pearson), racial group (Kruskal-Wallis).
RESULTS: The superior laryngeal nerve presented a definite anatomical disposition in all the 56 nerves studied, emerging from the nervus vagus inferior ganglion. The superior laryngeal nerve trunk was in average longer in corpses over 25 years old (p<0.05). Significant differences (p<0.05) between the internal and external branches were observed in all racial groups, and the internal branch average was inferior to the external branch average. There were not significant differences between the 18 studied corpses' left and right sides paired measurements.
CONCLUSIONS: Concerning emergence, trunk, bifurcation and major branches, the 56 studied nerves disposition had a definite anatomic pattern. The superior laryngeal nerve trunk was in average longer in corpses over 25 years old. In this study, the external branch of the laryngeal nerve was in average longer than the internal branch.
Key words: Laryngeal Nerves. Anatomy. Surgery. Cadaver.
RESUMO
OBJETIVO: Realizar um estudo anatômico do nervo laríngeo superior através da dissecção em cadáver não formolizado e não congelado.
MÉTODOS: 38 cadáveres do sexo masculino, provenientes do Instituto Médico-Legal de Minas Gerais (IML), foram estudados. Em 18 cadáveres a dissecção foi realizada bilateralmente e em 20 somente do lado esquerdo, totalizando 56 nervos. Foram registradas as medidas descritivas dos seus segmentos e as relações anatômicas com as estruturas cervicais da região. Este nervo foi analisado sob o ponto de vista estatístico, com as variáveis: lado (teste de Friedman p<0,05), altura e idade (Pearson) e etnia (Kruskal-Wallis).
RESULTADOS: O nervo laríngeo superior apresentou uma disposição anatômica definida em todos os 56 nervos estudados, emergindo do gânglio inferior do nervo vago. O tronco do nervo laríngeo superior foi em média mais longo nos cadáveres acima de 25 anos de idade (p<0,05). Foram observadas diferenças significativas (p<0,05) entre as medidas do ramo interno e do ramo externo em todos os grupos étnicos, sendo que a média do ramo interno foi inferior à média do ramo externo. As medidas pareadas dos lados direito e esquerdo não apresentaram diferenças significativas nos 18 cadáveres estudados.
CONCLUSÕES: A disposição dos 56 nervos laríngeos superiores mostrou um padrão anatômico definido, quanto à emergência, ao tronco, à bifurcação e aos ramos principais. O tronco do nervo laríngeo superior foi em média mais longo nos cadáveres acima de 25 anos de idade. O comprimento do ramo externo do nervo laríngeo superior foi em média maior do que o do ramo interno, neste estudo.
Descritores: Nervos Laríngeos. Anatomia. Cirurgia. Cadáver.
Introduction
Since the first human anatomy citations, at the end of the 19 century, when the descriptive and topographic study of the neck region was carried out with the purpose of teaching the students, and for medical-scientific application, the superior laryngeal nerve (SLN), it seems to us, has not been dissected and minutely described in several human anatomy books. The SLN is a mixed nerve (sensory and motor) and responsible, together with the inferior laryngeal nerve (ILN), for the human being voice quality. Its study is of paramount importance with the aim of avoiding its lesion during the surgical act. The knowledge of the SLN anatomy leads to a better tactic organization, with useful surgical technique possibilities, to avoid important laryngeal phonation disorders. Because of the lack of more precise information on the measurements and the importance of the SLN and its relations with the other neck structures, this work has aimed at performing an anatomical study in not preserved in formaldehyde and not frozen corpses, to demonstrate those measurements and the anatomical relations of this nerve, with the cervical structures of interest.
Methods
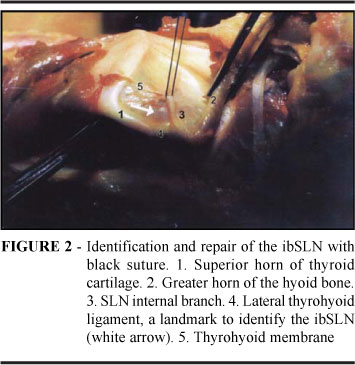
Thirty-eight Brazilian male corpses from the Medico-Legal Institute of the State of Minas Gerais (IML/MG) were used from 1993 to 2000. The ages ranged from 15 to 83 years old, average of 38. 5 ± 17.8 years. Height ranged from 1.50m to 1.80m, average of 1.66 ± 0.06m. As to race, 16 leukoderm (42.1%), 18 pheoderm (47. 4%) and four melanoderm (10. 5%) cadavers were studied. Dissection was performed bilaterally in 18 corpses and performed only on the left side in 20 corpses, in a total of 56 dissected nerves (right side 18, left side 38). In every one of them the thyroid gland has macroscopically shown with normal volume, confirming the inspection and palpation performed prior to dissection. The selected access route was through the combination of two incisions, having as a central landmark the thyroid cartilage prominence (TC). A previous bilateral ascending incision was performed, with the upper concavity and the lateral branches reaching the carotid grooves in front of the mastoid processes. The other incision, combined with the previous one, was started from the TC prominence with the vertical course on the midline of the neck to the sternal furcula. The adopted access route has taken a Y or cup-like shape (Figure 1). The dissection for SLN identification was started by the superior horn of the TC and by the greater horn of the hyoid bone (GHHB). In elevating the superior horn of the TC and the GHHB, promoting a discrete luxation, the superior laryngeal nerve internal branch (ibSLN) and the laryngeal vessels were identified overlying the lateral thyroid ligament.
At this point, the internal branch of the SLN was identified and isolated with black suture (Figure 2). From here on, the dissection of the ibSLN was started towards the bifurcation of the SLN trunk and to the inferior ganglion of the vagus nerve (IGVN), from where emerge. The dissection of the ibSLN was performed in the direction of its distal end up to the B bifurcation, and then, to the SLN trunk and to the IGVN (Figures 3 and 4). The SLN trunk, the vagus nerve (VN) and its inferior ganglion were isolated exposing the B bifurcation in ibSLN and the external branch of the superior laryngeal nerve (ebSLN). These structures were dissected and exposed, taking into consideration the emergence of the ebSLN and its course toward the CTM, in close relationship with the superior thyroid artery (STA), forming a single vasculo-nervous bundle, surrounded by an loose connective tissue (outlined in Figure 4). The distance between the ebSLN and the STA was considered from the point of emission of the first terminal branch of the ebSLN fillet up to the point of implantation of the STA branches in the superior pole of the thyroid gland (SPTG).
In the cases in which the ibSLN and the ebSLN had single penetration (one fillet) into the THM and the CTM, respectively, the C-C1 and D-D1 measurements were taken from 1.5cm before penetrating into the membrane and the muscle, with the points C on the ibSLN and D on the ebSLN being considered virtual ones for the purpose of the measurements B-C of the ibSLN and B-D of the ebSLN and D-STA. Following the complete dissection of the SLN and its branches, a cotton suture was placed on each segment accompanying their courses, and then cut and measured on a millimeter ruler. The C-C1 and D-D1 measurements were taken only on the first fillet of the ibSLN and the ebSLN, respectively, from their point of emergence. For the SLN measurement, the following landmarks were considered:

Click here to enlarge

Statistical analysis: the comparison between the two sides (right and left) with the measurements of the variables of interest, as well as between the measurements B-C1 and B-D1 and the number of fillets C-C1 and D-D1 observed in the ibSLN and ebSLN, was carried out by the Friedman's test. The comparisons among the races were performed with the use of the Kruskal-Wallis test. With the purpose of assessing the measurements among the variables as related to age and height, the Pearson's correlation analysis (r) was used. All the results were considered significant for a significance probability inferior to 5% (p< 0.05).
Results
The comparative analysis of the paired measurements of both the left and the right sides has shown no significant differences (p > 0.05), as presented in Table 1. Table 2 shows the characterization of the measurements concerning the gender. In relation to the measurements B-C, B-D and B-D1, similarities were found between the leukodermas and pheodermas, and both have presented results inferior to the melanodermas. Regarding the number of fillets (C-C1), a significant difference among the races has been evidenced, with the leukoderm and melanoderm races being similar, and both very superior to the pheoderm race. Concerning the age group, significant differences have been found only regarding the A-B measurement, where the younger subjects presented results significantly inferior to those observed in the group over 25 years old. For the other measurements no significant differences were evidenced (Table 3). Comparing the SLN internal and external branches, a significant difference was observed between their B-C1 and B-D1 measurements (p<0.05), with the B-C1 mean being inferior to the B-D1 mean (Table 4). Assessing the relationship of the height with the variables of interest, in each of the age groups, significant correlations have been observed in some situations in the group up to 25 years of age and no correlation was found in the group over 25 years of age. As it can be observed in Table 5, in the group up to 25 years of age, the height was correlated with the measurements B-C, B-D e B-D1. In these situations, the correlation was found to be positive, that is, the increase in height is accompanied by an increase of these measurements. The measurements of the ibSLN (B-C1) and the ebSLN (B-D1), related to the race, have shown a significant difference (p<0,05) in all race groups, with the B-C1 mean being inferior to the B-D1 mean (Table 5). Generally, the number of fillets C-C1 and D-D1 in the ibSLN and ebSLN, has presented a significant difference (p<0.05), with a significantly superior number of C-C1 fillets in the ibSLN being evidenced (Table 6). This same difference has been found when analyzing the different races, as depicted in Table 7.
Discussion
In the bilaterally studied cases, in 18 corpses (36 nerves) significant measurement variations of the SLN segments, in the same cadaver, have not been observed related to the height, race and age, being that the reason why the study was based on the total number of 56 dissected nerves (Table 1). In all cadavers, the SLN has emerged directly from the IGNV, and in two of them the left internal and external branches have emerged directly from the IGNV as anatomical variations. Sappey1 has stated that it is not rare the SLN arising from a higher point or even direct from the vagus nerve. Zarazaga and Cimas2 have identified, in two cases, the SLN arising directly from the vagus nerve. The SLN trunk (A-B), emerging from the IGNV, took a descending oblique and medial course, parallel to the pharynx and bifurcated into ibSLN and ebSLN at point B (Figures 3 and 4) in 54 of the 56 dissected nerves, with a variable distance from the IGNV emergence (A), according to the characterization of the measurements shown in Tables 1, 2 and 3. That segment has shown significant measurement variation related to the age in the groups of cadavers up to 25 years old. The cadavers over the age of 25 (first group) have shown a measurement (A-B) significantly inferior to that of the second group (Table 1). It has not been found in literature any reference on that measurement related to the age group. In 54 of the 56 dissected superior laryngeal nerves, the bifurcation in internal and external branches has occurred in the carotid region or within its limits with the infra-hyoid region, never at the level or after the GHHB. Anatomists and authors like Sappey1, Testut4 quoted in Barros Filho3; Pauchet et al5, Rouvière6; Newman and Becker7; Moore8 have stated that the SLN bifurcation occurs a little behind of the greater horn of the hyoid bone1,3-11. Others like Weissgenner9; Zavaleta10; Barros Filho3 and Espinoza et al11 have reported that the SLN bifurcation occurs above the CMOH3,12-15. The ibSLN has presented an oblique, descendent, anterior and superomedial topography related to the superior laryngeal artery, passing across the lateral thyrohyoid ligament. The anatomical pattern of the ebSLN related to the STA, in all cases, has presented an anterior, internal and slightly posterior course to the STA, being part of the vasculo-nervous bundle in most of its course. The measurements of the main segments B-C do ibSLN and B-D of the ebSLN, as well as the measurement of the total length B-D1 of the ebSLN, have shown similarities between the leukoderm and the pheoderm and both significantly inferior to the melanoderm races (Table 3). The total length (B-C1) of the ibSLN has shown a significant variation related to the total length (B-D1) of the ebSLN in all the race groups. The (B-C1) mean of the ibSLN was lower than the (B-D1) mean of the ebSLN (Tables 4 and 5). Contrary to those findings Gardner et al12; Moosman and De Weese13 and Moore8 stated that the ibSLN is longer than the ebSLN,10,16,17,18. In some cases, the emission of a fillet of the ebSLN to the inferior pharyngeal constrictor muscle (IPCM) was observed, before it penetrating the CTM (Figure 5). The left ebSLN has presented anatomical variation emitting an anastomotic branch with the ILN in only one dissected nerve (Figure 5). Kambic et al14 found the ebSLN emitting a branch to the IPCM in one third of the 80 studied nerves19. The measurements B-C1, C-C1, D-D1, D-STA and the number of fillets (D-D1) have not shown significant variations concerning age, race and height (Tables 2 and 3). The distance D-STA between the ebSLN and the STA together with the SPTG was, in average, 1cm, and intertwining, insinuation and adherence of the ebSLN to the STA have not been found in the 56 studied nerves (Figure 6, Table 2). Moosman and De Weese13 have described that the ebSLN was adherent to the STA in 15% of the cases and running between the branches of the artery in 6% of the cases17. Lekacos et al15 have also reported that the ebSLN runs between the STA branches in 6% to 14% and adherent to it in 15% to 20%20. According to Ligouro et al16 many surgeons do not give value to the SLN believing that, when accidentally injured, or even deliberately cut, sequela21 does not follow. According to Proileau17, the SLN is not recognized, by many, as a larynx nerve and, because of that it is not given the importance it has. Based on what it has been seen about the SLN and its importance for phonation, breathing and even swallowing, it can be stated that the possibility of injury to this nerve and its branches during cervical surgeries is very high and it would result in severe disorders of larynx function. Among the surgeries most commonly performed in the cervical region with a possibility of injuring this nerve we can name: the thyroidectomies, at the moment of the STA ligature, the ebSLN can be easily injured, resulting in voice tone alteration and fatigue, impairing the vocal register and the ability of singing and yelling; in carotid surgery, injury to the SLN trunk may occur, leading to, as consequences, dysphagia, insensitivity and larynx mucosa numbness, as well as the loss of voice quality. In esophagus, vertebral cervical spine, trachea, and oncological surgeries, the surgeon needs to know the SLN anatomy deeply, with the purpose of avoiding an injury, which could be definite and fatal for all the main functions of the larynx. Bastos et al18 have stated that the iatrogeny of the laryngeal nerves in literature ranges from 0,3% to 13,3%23. Cernéa et al 19 have mentioned the risk of injury to this nerve in 15% to 65% of the cases24. Espinoza et al11 have stated that during as thyroidectomies, 15% of ebSLN injury occurs at the moment of the STA15 ligature. Based on the electromyography and acoustic analysis, Teitelbaum and Wenig20 have recorded a SLN injury in 15% to 68% of the patients who underwent thyroid surgery25. The main contribution of this study is calling the attention to the fascinating and peculiar anatomical topography of the SLN, which the surgeons, generally, must know. They should also orient themselves concerning the technical surgery approach, with the purpose of minimizing the high risk of injury of these nerves during the cervical surgical interventions. As a surgical approach, based on what has been found in the present study on the SLN, and with the purpose of avoiding or reducing the iatrogenic injury to the ebSLN, the suggestion is that the surgeon, before ligating the STA in thyroidectomies, performs the luxation of the SPTG, passing the hemostatic forceps in the mediolateral direction, tangent to the SPTG. The forceps passes through the triangular space formed superiorly by the CTM, medially by the trachea and inferolaterally by the SPTG, only occupied by loose tissue (Outlined in Figure 4).This maneuver allows the SPTG, luxated forward and to the side, to enable the STA to keep away from the ebSLN, and the artery may be ligated without major risk to the ebSLN (Figure 6).
Conclusions
The topography of the 56 dissected SLN in 38 male corpses has shown a defined anatomical pattern concerning the emergence, the trunk, the bifurcation, the main branches and the penetration fillets, both in the thyrohyoid membrane, and in the cricothyroid muscle. In all cadavers in which the SLN has been studied bilaterally, its paired measurements have not shown significant variations. The trunk (A-B) of the SLN was, in average, longer in the cadavers of the group over 25 years of age. The measurements of the segments B-C of the ibSLN and B-D and B-D1 of the ebSLN, in the melanoderm cadavers, were significantly longer as related to the other races. The ebSLN length was in average longer than that of the ibSLN in all the 56 studied nerves.
Received: January 16, 2007
Review: February 14, 2007
Accepted: March 15, 2007
Conflict of interest: none
Financial source: none
- 1. Sappey PC. Nerf laryngé supérieur. In: Sappey PC. Traitè d'anatomie; nerologie: organes des sens. 2ed. Paris: Delahaye; 1872. p.350-2.
- 2. Zarazaga J, Cimas L. Relaciones del nervio laringeo superior con el pediculo vasculo nervioso del polo superior de Ia glandula tireoide. Bol Soc Cir Rosário. 1942; 9:95-102.
- 3. Barros Filho NM. Contribuição para a anatomia do ramo externo do nervo laringeo superior; sua aplicação técnica nas tireoidectomias (Tese - Livre Docência). São Paulo: Faculdade de Medicina da Universidade de São Paulo; 1948.
- 4. Testut L. Nerf laryngé supérieur. In: Testut L. Traitè d'anatomie humaine. 2ed. Paris: Gaston Dion; 1911. p.112-5.
- 5. Pauchet V, Soudart P, Labat G, D'Ormont RB. Anesthesie du nerve laryngé supérieur; anatomie. In: Pauchet V, Soudart P, Labat G, D'Ormont RB. L'anesthesie regionale. 4ed. Paris: Gaston Dion; 1927. p.77-8.
- 6. Rouvière H. Nerf laryngé superieur. In: Rouvière H. Anatomie humane descriptive et topographique. 2ed. Paris: Masson; 1927. p.250.
- 7. Newman AN, Becker SP. Superior laryngeal nerve paralysis and benign thyroid disease. Arch Otolaryngol. 1981;107(2):117-9.
- 8. Moore KL. Inervação da laringe. In: Moore KL. Anatomia orientada para clínica. 3ed. Rio de Janeiro: Guanabara Koogan; 1994. p.767-9.
- 9. Weissgenner RJ. Thyroid anatomy and histology: surgical anatomy. Illinois Med J. 1932;61:528-31.
- 10. Zavaleta DE. El laríngeo superior y la cirurgia del tireoide. Rev Assoc Med Argent. 1045;59:765-1.
- 11. Espinoza H, Dhem A. La préservation du rameau external du nerf laryngé supérieur en chirurgie thyroidienne. Ann Otolaryngol. 1989;106(2):127-34.
- 12. Gardner E, Gray D, O'rahilly R. Nervo vago; neurolaríngeo superior. In: Gardner E, Gray D, O'rahilly R. Anatomia; estudo regional do corpo humano. 2ed. Rio de Janeiro: Guanabara Koogan; 1967. p.787-8.
- 13. Moosman DA, De Weese MS. The external laryngeal nerve as related to thyroidectomy. Surg Gynecol Obstet. 1968;127(5):1011-6.
- 14. Kambic V, Zargi M, Radsel Z. Topographic anatomy of the external branch of the superior laryngeal nerve; its importance in head and neck surgery. J Laryngol Otol. 1984;98(11):1121-4.
- 15. Lekacos NL. et al. The superior laryngeal nerve in thyroidectomy. Am Surg. 1987;53(10):610-2.
- 16. Liguoro D. et al. Anatomical basis of the anterior cervical spine approach: topographic study of the nerve structure. Surg Radiol Anat. 1992;14(3):203-8.
- 17. Proileau WH. lnjury of the laryngeal branches of the vagus nerve in thyroid surgery. South Surg. 1933;1:287-92.
- 18. Bastos ES, Cordeiro AC, Toledo AC. Lesões dos nervos laríngeos. In: Bastos ES. Rumos modernos da cirurgia. São Paulo: Fundo Editorial Procieux; 1969. p.178-80.
- 19. Cernéa CR. et al. Surgical anatomy of the external branch of the superior laryngeal nerve. Head Neck. 1992;14(5):380-3.
- 20. Teitelbaum BJ, Wenig BL. Superior laryngeal nerve injury from thyroid surgery. Head Neck. 1995;17(1):36-40.
Publication Dates
-
Publication in this collection
24 May 2007 -
Date of issue
June 2007
History
-
Received
16 Jan 2007 -
Reviewed
14 Feb 2007 -
Accepted
15 Mar 2007