Abstracts
PURPOSE: To elaborate an animal model with the objective of studying the continence of the biological valves surgically performed in the left colon of rats. METHODS: Thirty four rats were operated on and divided into three groups (G). G1 (sham) animals which underwent laparotomy only; G2 (perineal amputation without valves): animals which underwent amputation of the anal sphincter complex combined with a perineal colostomy; G3 (abdominoperineal amputation combined with valves): animals which underwent abdominoperineal amputation combined with three, equidistant and circumferential (360(0)), extra-mucosal seromyotomies, of the descending colon, which were sutured to create biological valves combined with perineal colostomy. Animals were euthanized in the late postoperative period and surgical valves were saved for histopathological study. RESULTS: Surgical procedure provoked intestinal dilation, as well as segmented chambers along the descending colon. Retained fecalomas between the valves and proximal to them were also noted. Six rats died of intestinal obstruction due to fecal impaction at the surgical site. The sequence of events was: stasis, obstruction, distention, perforation, peritonitis and death. Histopathology showed inflammation due to foreign body type reaction around the sutured colon causing partial concentric stenosis, capable of interfering normal mechanical activity of the distal colon. This process resulted in retardation of the intestinal transit. CONCLUSION: Extra-mucosal seromyotomies, with seromuscular suture, can be used as an operative procedure capable of causing retardation in the intestinal transit of rats.
Colostomy; Colorectal Surgery; Animal experimentation; Rats
OBJETIVO: Modelo de experimentação, com confecção de válvulas biológicas no cólon esquerdo de ratos com o objetivo de estudar o grau de continência dessas válvulas. MÉTODOS: Trinta e quatro ratos foram operados e distribuidos em três grupos: G1 (grupo simulado) submetido apenas à laparotomia, G2 (grupo amputado sem válvula) submetido à amputação do conjunto esfincteral mais colostomia perineal e G3 (grupo amputado com válvula) submetido à amputação do conjunto esfincteral, confecção de três seromiotomias extra-mucosas, eqüidistantes e circunferenciais (360(0) - válvulas biológicas), no colon descendente mais colostomia perineal. No pós-operatório tardio, os animais dos três grupos foram submetidos à eutanásia para coleta da peça cirúrgica e estudo histopatológico das válvulas. RESULTADOS: Os resultados mostraram que o procedimento culminou em dilatação intestinal, confirmada pela formação de verdadeiras câmaras de segmentação e pela presença de fecalomas retidos entre as válvulas e cranialmente a elas. Seis ratos morreram em decorrência de obstrução intestinal por impacção de fezes no local operado, na seqüência: obstrução, estase, distensão, perfuração, peritonite e morte. As alterações histopatológicas confirmaram o processo inflamatório com reação do tipo corpo estranho, no perímetro do cólon suturado, proporcionando uma estenose parcial concêntrica, levando à alteração da atividade mecânica do cólon distal, resultando no retardo do trânsito intestinal. CONCLUSÃO: As seromiotomia extramucosas, com sutura seromuscular, podem ser utilizadas como técnica operatória para se obter retardo do trânsito intestinal em ratos.
Colostomia; Cirurgia Colorretal; Experimentação Animal; Ratos
3-ORIGINAL ARTICLE
ALIMENTARY TRACT
Histological study of the left colon of rats after extra-mucosal seromyotomy (continent valves). Evaluation of colonic emptying1 1 Research perfomed at Surgical Laboratory Dr. José Antonio Garcia Coutinho Medical School, Sapucaí Valley University, Pouso Alegre - MG, Brazil.
Estudo histológico do cólon esquerdo de ratos após a confecção de seromiotomias extra-mucosas (válvulas continentes). Avaliação do grau de esvaziamento do conteúdo colônico
Beatriz DeotiI; Alcino Lázaro da SilvaII; Maria Zélia de Oliveira CostaIII; Aline Carvalho DinaliIV
IMs, Fellow PhD degree in Surgery, Federal University of Minas Gerais (UFMG), Brazil
IIProfessor Emeritus of Surgery, UFMG, Brazil
IIIPathologist of the CIAP laboratory, Divinópolis - MG, Brazil
IVGraduate student, UFMG, Brazil
Correspondence Correspondence: Alcino Lázaro da Silva Rua Guaratinga, 151 30315-430 Belo Horizonte MG, Brazil Phone/Fax: (55 31)3221-3072 bardesiro@bol.com.br
ABSTRACT
PURPOSE: To elaborate an animal model with the objective of studying the continence of the biological valves surgically performed in the left colon of rats.
METHODS: Thirty four rats were operated on and divided into three groups (G). G1 (sham) animals which underwent laparotomy only; G2 (perineal amputation without valves): animals which underwent amputation of the anal sphincter complex combined with a perineal colostomy; G3 (abdominoperineal amputation combined with valves): animals which underwent abdominoperineal amputation combined with three, equidistant and circumferential (3600), extra-mucosal seromyotomies, of the descending colon, which were sutured to create biological valves combined with perineal colostomy. Animals were euthanized in the late postoperative period and surgical valves were saved for histopathological study.
RESULTS: Surgical procedure provoked intestinal dilation, as well as segmented chambers along the descending colon. Retained fecalomas between the valves and proximal to them were also noted. Six rats died of intestinal obstruction due to fecal impaction at the surgical site. The sequence of events was: stasis, obstruction, distention, perforation, peritonitis and death. Histopathology showed inflammation due to foreign body type reaction around the sutured colon causing partial concentric stenosis, capable of interfering normal mechanical activity of the distal colon. This process resulted in retardation of the intestinal transit.
CONCLUSION: Extra-mucosal seromyotomies, with seromuscular suture, can be used as an operative procedure capable of causing retardation in the intestinal transit of rats.
Key words: Colostomy. Colorectal Surgery. Animal experimentation. Rats.
RESUMO
OBJETIVO: Modelo de experimentação, com confecção de válvulas biológicas no cólon esquerdo de ratos com o objetivo de estudar o grau de continência dessas válvulas.
MÉTODOS: Trinta e quatro ratos foram operados e distribuidos em três grupos: G1 (grupo simulado) submetido apenas à laparotomia, G2 (grupo amputado sem válvula) submetido à amputação do conjunto esfincteral mais colostomia perineal e G3 (grupo amputado com válvula) submetido à amputação do conjunto esfincteral, confecção de três seromiotomias extra-mucosas, eqüidistantes e circunferenciais (3600 - válvulas biológicas), no colon descendente mais colostomia perineal. No pós-operatório tardio, os animais dos três grupos foram submetidos à eutanásia para coleta da peça cirúrgica e estudo histopatológico das válvulas.
RESULTADOS: Os resultados mostraram que o procedimento culminou em dilatação intestinal, confirmada pela formação de verdadeiras câmaras de segmentação e pela presença de fecalomas retidos entre as válvulas e cranialmente a elas. Seis ratos morreram em decorrência de obstrução intestinal por impacção de fezes no local operado, na seqüência: obstrução, estase, distensão, perfuração, peritonite e morte. As alterações histopatológicas confirmaram o processo inflamatório com reação do tipo corpo estranho, no perímetro do cólon suturado, proporcionando uma estenose parcial concêntrica, levando à alteração da atividade mecânica do cólon distal, resultando no retardo do trânsito intestinal.
CONCLUSÃO: As seromiotomia extramucosas, com sutura seromuscular, podem ser utilizadas como técnica operatória para se obter retardo do trânsito intestinal em ratos.
Descritores: Colostomia. Cirurgia Colorretal. Experimentação Animal. Ratos.
Introduction
The abdominoperineal amputation of the rectum proposed by Miles was a landmark in the history of anorectal surgery1. The procedure provided better survival although patients carried the burden of living with a permanent abdominal colostomy. Many techniques were described thereafter in which a neosphincter was created. However, they have indicated neither adequate applicability nor consistent rehabilitative results. Surgical resection remains the most efficacious treatment modality for rectal cancer. Current literature shows that radiotherapy, chemotherapy, and immunotherapy are supplementary approaches. Lázaro da Silva2 observing that seromyotomy of two muscular layers of the small bowel of rats provoked transit retardation applied the same procedure to the left colon. The objective was to provide relative continence of feces in patients who had undergone abdominoperineal resection, without interfering with the radicalness of the procedure. To this purpose, Miles abdominoperineal rectal amputation is combined with perineal colostomy. This is an alternative procedure to definitive abdominal colostomy for patients who undergo abdominoperineal rectal amputation. Furthermore, the possibility of improving the patient's well being, as well as professional and spouse good relationship are important additional gains. The purpose of this study was to further determine the mechanisms involved in the continence of feces produced by the valves created by seromyotomies.
Methods
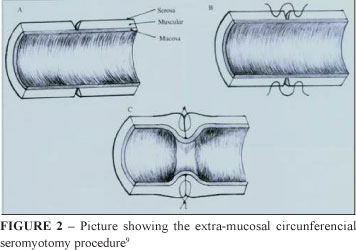
Animal experiments were performed at the Surgical Laboratory of the Dr. José Antonio Garcia Coutinho Medical School, a member school of the Vale do Sapucaí University, Pouso Alegre, Brazil. The research was approved by the Research Ethics Committee of the Dr. José Antonio Garcia Coutinho Medical School, protocol number 86/03. Thirty four male (Rattus novergicus albinos Wistar) rats weighing between 400g and 600g were used in the study. The animals were maintained on 12h light/dark cycles and fed rat chow (Labina® - Purina, São Paulo, Brazil) up to 24 hours before to the operation. Water was given to the animals up to 6hours before the operation. The animals were divided into three groups: Group 1 (G1) sham (n = 8); Group 2 (G2) (n=8); Group 3 (G3) (n=18). The abdominal area was shaved in G1 and G3 rats. All animals were anesthetized with intramuscular Ketamine (0,1ml/100g of weight) and Xylazine (0,1ml/100g of weight) (Laboratório Calier, São Paulo, Brazil) injected in the right thigh. G1 animals (sham) underwent a 5cm median laparotomy followed by manipulation and exposure of the large and small bowel and intraperitoneal injection of 20ml of sterile saline. The bowel was placed back inside the abdominal cavity and the abdominal wall was closed. G2 animals underwent perineal dissection of the rectum and the colon up to the sacrum coccyx union. The anorectal sphincter complex was resected and the descending colon was pulled through the perineal opening where a colostomy was made. G3 animals underwent perineal dissection of the rectum and colon as in G2, after which, a 5cm median laparotomy was performed. The descending colon was mobilized, and three circunferential (3600), extra-mucosal, seromyotomies were performed with a seromuscular suture. The first seromyotomy and suture were located 2cm from the anal verge. The other one was 1cm proximal to the first. The third seromyotomy was located 1cm proximal to the second. A perineal colostomy as described for G2 animals was performed at the end of the operation (Figures 1 and 2).
The animals were euthanized by lethal KCl (10%) intra-cardiac injection on the 40th postoperative day, and a necropsy was performed at that time. The procedure consisted of a median laparotomy, from the xyphoid to the perineum, and resection of the large bowel from the cecum to the anal verge. Resection of the perineal colostomy was performed in G2 and G3 animals. Specimens were stored, for one week, in 10% formaldehyde solution for histopathological analyses. A 4cm long segment was measured from the anal verge or the perineal colostomy (G2 and G3) and cut, from each specimen, for histopathological analyses. Segments cut from each segment were opened longitudinally, in such a way that tissue samples from all three valves were obtained; the strips were used for histopathological analyses which were performed by a single pathologist. All tests were double blind and done in duplicates. Specimens were stained with Hematoxilin and Eosin (H&E) and Masson Trichromic.
The slides were viewed under light microscope and layers of the segment were analyzed. The following parameters were specifically studied: inflammatory reaction, fibrosis, the number of myenteric plexus and the anal sphincter apparatus. Neurons of the myenteric plexus were counted starting at point two located two cm cranially to the anal verge and for an extension of 5mm, in G1 specimens. The same extension was used for counting myenteric plexus in G2 specimens starting one cm cranially to the perineal colostomy. In G3 specimens myenteric plexus neurons were counted in an extension of two cm cranially and two cm distally of the first valve.
Results
Mortality
Six of the 34 G3 rats which were operated died (17,64%). All the animals died of intestinal obstruction.
Macroscopic findings
The first valve was not visualized in any of the G3 animals. The second valve was visualized in nine rats (75%) and the third valve in 12 rats (100%).
Microscopy
G1
No abnormal findings were noted on the mucosa and submucosa layers. At the anal verge area sebaceous glands and hair follicles with tubular glands and goblet cells were noted. Anal sphincter was seen in four rats (50%), sphincter apparatus had normal circular and longitudinal muscular layers. The average number of myenteric plexus identified on 5mm of bowel length was 12.25 and total amplitude (TA) was TA = 10 (Table 1).
G2
Abnormal findings were only noted on the distal part of the large bowel. The mucosa and the submucosa presented granulomatosis reaction. The muscular layer presented no abnormal findings. All rats of this group had foreign body type giant cell reaction on the serosa as well as fibrosis. The average number of myenteric plexus identified on 5mm of bowel length was 12.5 and total amplitude (TA) was TA = 11. No anal sphincter was identified on the rats (Table 2).
G3
The mucosa and the sub-mucosa of the distal portion of the large bowel presented granulomatosis reaction. Important abnormal findings were noted on the mucosa of the perineal colostomy. Giant cell reaction and fibrosis were present, varying from intense to discrete in some cases. Cranial to the perineal colostomy the mucosa was normal in 75% of the rats. Fibrosis, ulceration, and limphocitic infiltration were noted in only one animal each (8.3%). Two animals presented thinning of the mucosa provoked by intense lymphoid reaction (16.6%). In one animal an intra-luminal projection of the mucosa was noted, creating a valve (8.3%) (Table 3 and Figure 3).
The area of the junction between the skin and the bowel on the perineal colostomy presented important submucosal findings. Fibrosis, edema, and ulceration were noted in one animal each (8.3%). Limphocitic infiltration was noted in three rats (25%) and lymphoid hyperplasia in two (16.6%). Transected muscular propria layer was noted in 11 rats of G3 (91.6%) and absent in one animal (8.3%), (Figure 4). In seven rats (58.3%) two areas of muscular propria layer transection were noted and in three rats one layer of transection was noted (25%).
Foreign body type giant cell reaction was noted in the serosa layer of 10 G3 rats (83,3%), (Figure 5). Fibrosis was present in all animals; mild fibrosis in 8 rats (66.6%), and moderate fibrosis in 4 rats (33.3%). The serosa layer was normal in only one animal (Figure 6).
The average number of myenteric plexus identified was 4.4 and total amplitude (TA) was TA = 7. The anal sphincter apparatus was absent in 8 rats (66.6%) and in 4 rats (33.3%) some muscle fibers belonging to the sphincter were identified. The internal sphincter (smooth muscle) was seen in all specimens and the external sphincter (skeletal muscle) was absent in only one animal.
Discussion
The current approach to surgical treatment of rectal and anal tumors is becoming more conservative aiming at the preservation of the anal sphincter and sexual function, without jeopardizing the radicalness of the operation. However, maintenance of the physical and psychological well being of the patients who are candidates to a definitive colostomy became a challenging problem for the surgeon. Orthotopic defection is an important solution to this problem3,4,5,6,7,8,9,10,11. The consequences of a definitive abdominal colostomy and the high social and psychological problems that come along with it are well known. A good physical appearance is an important measure of status in our society. Therefore physical activities in which the body is exposed are becoming more and more common. Furthermore, with the improvement in life expectancy older people are assuming those habits more frequently as well7,12. Many studies3,9,10,11,12,13 have proposed surgical options that would provide orthotopic defection. However, the applicability of those procedures is complex and the outcome is variable. Perineal colostomy combined with circunferential seromyotomy of the left colon, have been shown to form biological valves originated from the invagination of the sutured seromuscular borders. The advantages of this procedure are: there is no need for an anastomosis; it does not interfere with the radicalness of the surgical procedure proposed to the patient; shorter operative time; mucus elimination from the perineal colostomy is minimal because of the small portion of colonic mucosa exposed at the skin edge. Additionally, the lateral and posterior walls of the vagina are reconstructed when those are included in the resection. In terms of personal hygiene the procedure provides more comfortable cleaning because the patient can plan colonic irrigation time and therefore, he has better defecation control. More economy is also to be considered since the patient does not have to spend with colostomy bags. However, the most important advantage of this procedure is its simplicity. Even though perineal colostomy as described above has been safely performed with relatively good results, more studies are necessary to better evaluate the procedure. Two series applied the technique reproducing the original results13. The authors confirmed fecal retention in the distal colon and concluded that this finding was due to alteration of colonic myoelectric activity. In the present study, fecal impaction was a serious complication to the procedure caused the death of five and maybe six rats. Fecal impaction occurred at the site of the valves, provoking stasis, distention, perforation, peritonitis, and death. This was confirmed at the necropsy. Another important complication was segmental necrosis of the colon caused by ligation of the caudal mesenteric artery. Segments that were not supplied by collaterals suffered necrosis and the animals died in the first 12 hours after the procedure. Those animals were excluded from G3 since no further analysis of the procedure could be done. Time of death had large variation in the study (131 days). This shows that the animals had a great capacity of adaptation to the different degrees of colonic dilation. This was an important finding in the study. Colonic dilation was striking in some animals, creating segmented chambers between the valves provoking a translucent aspect on the colon wall. We attribute this finding to partial stenosis at the level of the valves. The most cranial valve presented the greatest flow resistance probably because it was the valve which received the first impact. Distally to that point, fecal matter was already molded into a funnel shape, making it easier for the stenosis to pass the other valves. The colonic dilation located proximally to each valve contributed to the second pathological finding. The increased diameter of the colon provoked flow reduction and stasis of fecal matter, an example of Laplace´s Law14. Seromyotomies (valves) were observed microscopically as areas of interrupted muscular layer associated with fibrosis and foreign body type giant cell reaction. Fibrosis was also noted filling the areas of the myenteric plexus (Auerbach) at the level of the valves, probably interfering with peristalsis transmission. This finding was supported by the smaller number of myoenteric plexus observed in G3. This finding has not been reported in the literature. Seromyotomy was not complete (3600) in one of the slides microscopically observed. However, segmental colonic dilation and fecal retention were noted in the rat during autopsy, demonstrating that fecal retention can be even with an incomplete seromyotomy. The results presented here stimulate the search for a better procedure capable of restoring orthotopic defecation, as physiologically as possible, for patients who would otherwise have to live with a permanent abdominal colostomy.
Conclusion
Seromyotomy of the left colon of rats combined with an invaginating seromuscular suture creates continent valves that provoke fecal retention and histological changes that are capable of controlling defecation.
Received: November 12, 2007
Review: January 15, 2008
Accepted: February 19, 2008
Conflict of interest: none
Financial source: none
- 1. Miles WE. Rectal Surgery. A practical guide to the modern surgical treatment of rectal diseases. London; 1944.
- 2. Lázaro da Silva, A. Tentativa de tratamento do "Dumping" através de um esfincter ileal. Rev Assoc Med Minas Gerais 1974;25(1):32-3.
- 3. Schmidt E, Bruch HP. Traitment chirurgical des incontinences sphincteriennes intestinales par autotransplant libre de musculature lise. J Chir. 1981;118:315-20.
- 4. Torres RA, González A. Operación de Miles con colostomia perineal continente. Rev Argent Cir. 1989;56:166-9.
- 5. Lázaro da Silva A. Amputação abdominoperineal com colostomia perineal. Rev Bras Coloproctol.1991;11:105-8.
- 6. Lázaro da Silva A. Amputacion Abdominoperineal com colostomia perineal. Prensa Med Argent. 1993;82:800-4.
- 7. Lázaro da Silva A. Abdominoperineal excision of the rectum and anal canal with perineal colostomy. Eur J Surg. 1995;161:761-4.
- 8. Gamagami RA, Chiotasso P, Lasorthes F. Continent perineal colostomy after abdominoperineal resection: outcome after 63 cases. Dis Colon Rectum. 1999;42:626-31.
- 9. Veloso SG, Biet R, Rios AM, Leite VHR, Lázaro da Silva A. Eficácia da confecção de válvulas colônicas após ressecção retoanal em ratos. Rev Col Bras Cir. 2001;28:356-63.
- 10. Goldsmith HS. Fecal control following pyloric valve transposition after abdominoperineal resection. Tech Coloproctol. 2003;7:95-101.
- 11. Marchal F, Doucet C, Lechaux D, Lasser P, Lehur PA. Secondary implantation of an artificial sphincter after abdominal resection and pseudocontinent perineal colostomy for rectal cancer. Gastroenterol Clin Biol. 2005;29:425-8.
- 12. Altomare DF, Rinaldi M, Martinelli E, Veglia A, Salustio P. Perineal colostomy following Miles procedure: from reconstructive surgery to the artificial anal sphincter. Osp Ital Chir. 2000;6:572-7.
- 13. Velitchkov NG, Kirov GK, Losanoff JE, Kjossev KT, Grigorov GI, Mironov MB, Klenov IS. Abdominoperineal resection and perineal colostomy for low rectal cancer: the Lázaro da Silva technique. Dis Colon Rectum. 1997;40:530-3.
- 14. Silva Júnior AL, Lázaro da Silva A, Castro LPF. Histopatologia da seromiotomia dupla e sutura seromuscular no cólon descendente de ratos. Rev Col Bras Cir. 1999;26:367-73.
Publication Dates
-
Publication in this collection
12 June 2008 -
Date of issue
June 2008
History
-
Accepted
19 Feb 2008 -
Reviewed
15 Jan 2008 -
Received
12 Nov 2007