Abstracts
PURPOSE: The tension at the aponeurotic edges of abdominal wall defects is an important factor of dehiscence and incisional hernia formation. The purpose of this study is to map and compare the traction force necessary for medial mobilization in various levels of the anterior rectus sheath in cadavers. METHODS: Twenty four adult male cadavers, raging from 22 to 59 years old, with the abdominal wall intact and without prior preservation techniques, were dissected. A complete excision of the linea alba was performed. Traction loops of 10 mm in diameter were made in the anterior rectus sheath and were placed: 2, 4, 6 and 8 cm below the lower edge of the umbilicus and 3, 6 and 9 cm above the upper edge of the umbilicus. Each loop was mobilized 10 mm in the medial direction, using an analog dynamometer. The values obtained in each level were compared using Friedman's analysis of Variance for p < 0.05. RESULTS: The average traction values obtained at the various levels were compared and there was no statistical significant difference. CONCLUSION: There is no variation in tension along the whole extension of the anterior rectus sheath.
Hernia, Ventral; Tensile Strength; Cadaver
OBJETIVO: A tensão na margem da aponeurose de um defeito da parede abdominal é um importante fator de deiscência e formação da hérnia incisional. O objetivo deste estudo é mapear e comparar a força de tração necessária à mobilização medial em vários níveis da lâmina anterior do músculo reto do abdome em cadáveres. MÉTODOS: Vinte e quatro cadáveres adultos masculinos, com idade entre 22 e 59 anos, com a parede abdominal intacta e sem técnicas prévias de conservação, foram dissecados. Uma excisão completa da linha alba foi realizada. Alças de tração de 10 mm de diâmetro foram realizadas na lamina anterior do músculo reto do abdome e estavam localizadas: 2,4,6 e 8 cm abaixo da margem inferior do umbigo e 3,6 e 9 cm da margem superior do umbigo. Cada alça foi mobilizada 10 mm em direção medial, usando um dinamômetro analógico. Os valores obtidos em cada nível foram comparados usando a analise de variância de Friedman com p < 0,05. RESULTADOS: Os valores de tração obtidos nos vários níveis foram comparados e não apresentaram significância estatística. CONCLUSÃO: Não há variação de tensão por toda lamina anterior do músculo reto do abdome.
Hérnia Ventral; Resistência à Tração; Cadaver
9 - ORIGINAL ARTICLE
PLASTIC SURGERY
Mapping traction strength of the anterior rectus sheath in cadaver1 Correspondence: Fabio Xerfan Nahas Division of Plastic Surgery, Department of Surgery Federal University of São Paulo Rua Napoleão de Barros, 715/4º andar 04024-0022 São Paulo - SP Brazil Phone: (55 11)5576-4065 / 5576-4118 fabionahas@uol.com.br
Mapeamento da força de tração da lâmina anterior do músculo reto do abdome em cadáver
Romar Ângelo Barbato SilveiraI; Fábio Xerfan NahasII; Bernardo HochmanIII; Felix Carlos Ocariz BazzanoIV; Carlos Roberto AmorimI; Yara JulianoV; Volney Marques PassosVI; Lydia Masako FerreiraVII
IMaster, Department of Surgery, Post-Graduation Program of Plastic Surgery, UNIFESP, São Paulo, Brazil
IIPhD, Associate Professor, Division of Plastic Surgery, UNIFESP, São Paulo, Brazil
IIIPhD, Affiliate Professor, Division of Plastic Surgery, UNIFESP, São Paulo, Brazil
IVPhD, Associate Professor, Bioethical Post-Graduation, UNIVAS, Pouso Alegre-MG, Brazil
VPhD, Full Professor, Department of Epidemiology, UNIFESP, São Paulo, Brazil
VIMD, UNIVAS, Pouso Alegre-MG, Brazil
VIIPhD, Full Professor, Head of Plastic Surgery Division and Chairwoman of Department of Surgery, UNIFESP, São Paulo, Brazil
Correspondence Correspondence: Fabio Xerfan Nahas Division of Plastic Surgery, Department of Surgery Federal University of São Paulo Rua Napoleão de Barros, 715/4º andar 04024-0022 São Paulo - SP Brazil Phone: (55 11)5576-4065 / 5576-4118 fabionahas@uol.com.br
ABSTRACT
PURPOSE: The tension at the aponeurotic edges of abdominal wall defects is an important factor of dehiscence and incisional hernia formation. The purpose of this study is to map and compare the traction force necessary for medial mobilization in various levels of the anterior rectus sheath in cadavers.
METHODS: Twenty four adult male cadavers, raging from 22 to 59 years old, with the abdominal wall intact and without prior preservation techniques, were dissected. A complete excision of the linea alba was performed. Traction loops of 10 mm in diameter were made in the anterior rectus sheath and were placed: 2, 4, 6 and 8 cm below the lower edge of the umbilicus and 3, 6 and 9 cm above the upper edge of the umbilicus. Each loop was mobilized 10 mm in the medial direction, using an analog dynamometer. The values obtained in each level were compared using Friedman's analysis of Variance for p < 0.05.
RESULTS: The average traction values obtained at the various levels were compared and there was no statistical significant difference.
CONCLUSION: There is no variation in tension along the whole extension of the anterior rectus sheath.
Key words: Hernia, Ventral. Tensile Strength. Cadaver.
RESUMO
OBJETIVO: A tensão na margem da aponeurose de um defeito da parede abdominal é um importante fator de deiscência e formação da hérnia incisional. O objetivo deste estudo é mapear e comparar a força de tração necessária à mobilização medial em vários níveis da lâmina anterior do músculo reto do abdome em cadáveres.
MÉTODOS: Vinte e quatro cadáveres adultos masculinos, com idade entre 22 e 59 anos, com a parede abdominal intacta e sem técnicas prévias de conservação, foram dissecados. Uma excisão completa da linha alba foi realizada. Alças de tração de 10 mm de diâmetro foram realizadas na lamina anterior do músculo reto do abdome e estavam localizadas: 2,4,6 e 8 cm abaixo da margem inferior do umbigo e 3,6 e 9 cm da margem superior do umbigo. Cada alça foi mobilizada 10 mm em direção medial, usando um dinamômetro analógico. Os valores obtidos em cada nível foram comparados usando a analise de variância de Friedman com p < 0,05.
RESULTADOS: Os valores de tração obtidos nos vários níveis foram comparados e não apresentaram significância estatística.
CONCLUSÃO: Não há variação de tensão por toda lamina anterior do músculo reto do abdome.
Descritores: Hérnia Ventral. Resistência à Tração. Cadaver.
Introduction
Laparotomy is one of the most common surgical procedures in medical practice1-6. Median incision is the main access to the abdominal cavity. The incidence of hernias varies from 0 to 6% of all laparotomies7. This complication may be related to factors such as patient's age, malnutrition, obesity, infection, jaundice, anemia, diabetes, renal insufficiency and neoplasias. Other factors such as the use of cytostatics and corticosteroids, as well as mechanical factors that lead to an increase in abdominal pressure7, may also be involved in the incidence of this type of abdominal wall defect.
The tension at the aponeurotic edges of the defect is an important factor of dehiscence and incisional hernia formation. Despite the fact that tension is involved in the physiopathology of incisional hernia, and the existence of a high number of surgical tequniques that have been developed with the purpose of decreasing the tension at the edges of the musculoaponeurotic defect 8-15, few studies about the tension exerted by the musculoaponeurotic components at the edges of incisional hernia were found in the literature. However, no study mapped the tension on the anterior rectus sheath.
The hypothesis tested in this study is as follows: is there any region of lower tension of the anterior layer of the rectus abdominis muscle sheath, which could be preferably corrected with the use of local tissues. On the other hand, areas with higher tension could be preferably corrected with mesh.
Therefore, the objective of this study is to map and compare the traction force necessary for medial mobilization in various levels of the anterior rectus sheath in cadavers.
Methods
The present study was approved by the committee of ethics in research of the Federal University of São Paulo (UNIFESP-EPM). Twenty four adult male cadavers, with the abdominal wall intact and without prior preservation techniques, were dissected from September 2005 to May 2006. Age ranged from 22 to 59 years (mean - 30 years), the time since death varied from 6 - 20 hours (mean - 10 hours). The environmental temperature in the period prior to dissection varied from 20 to 24 °C. The following cadavers were excluded from the study: those who were less than 18 years and more than 60 years old, those with more than 24 hours since death, those that had been submitted to low temperatures or previous laparotomies, those with hernias of the abdominal wall, and cadavers with intraperitoneal disease, which would restrict the mobility of the abdominal wall.
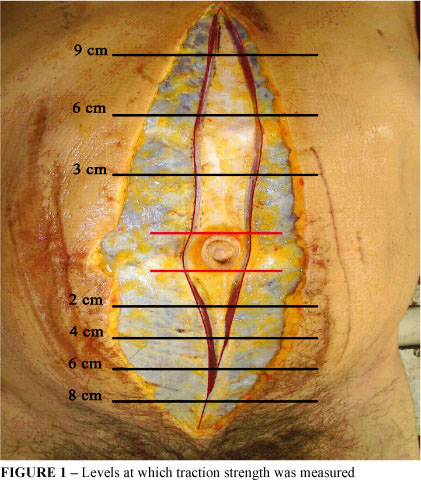
The cadaver was placed in the supine position, and an incision was made from the xiphoid appendix to the symphysis pubis. The subcutaneous tissue was incised down to the linea alba and it was undermined to expose the myoaponeurotic layer. The upper limit of undermining was marked by the tenth rib, and the lower limit by the inguinal ligament. Laterally, the limit of this dissection was the semilunar line. Complete excision of the linea alba was performed throughout its thickness. Traction loops of 10 mm in diameter were made in the anterior rectus sheath, using 2-0 nylon sutures. These loops were fixed to the anterior aponeurosis at a point located 10 mm laterally to the edge of the area where the linea alba was excised. These loops were placed at seven levels: 2, 4, 6 and 8 cm below the lower edge of the umbilicus and 3, 6 and 9 cm above the upper edge of the umbilicus (Figure 1). Each loop at the anterior rectus sheath was mobilized 10 mm in the medial direction, using an analog dynamometer (Crown® Dynamometer, Brazil). After this mobilization, the traction was measured with the dynamometer. The distance of mobilization of the aponeurotic point was measured with an analog pachymeter (Universal® Pachymeter with 20 cm ruler, Japan). (Figure 2)
All traction measurements performed using a dynamometer was repeated by a second researcher. In cases on which there was disagreement, the evaluation of a third researcher was requested.
The measurement closest to that obtained by the third observer was the one considered. The points studied were broken down as shown in Table 1.
The values obtained in each level were inserted in the formula used to calculate the traction index5,6,10. The traction index is the ratio between the traction (force) measured at the aponeurotic point, and the distance on which the point was mobilized. The formula below represents this ratio:

TI - Traction index (kg/cm)
F - Traction force in the point studied
D - Mobilization distance from the aponeurotic point (cm)
The average of the TI obtained at both sides was calculated for each level. The average values for each level in all the cadavers were compared using Friedman's analysis of Variance for p < 0.05.
Results
The average traction values obtained at the various levels were compared, and are shown in Figure 3. There was no statistical significant difference among the studied levels.
Discussion
The physiopathology of incisional hernia is multifactorial and involves the presence of comorbidities as well as a variety of closure techniques. The correction of incisional hernias by primary suture of the musculoaponeurotic edges of the defect is related to a high recurrence rate4. This fact is largely due to excess tension in the suture line. Thus, the aim of the various studies and techniques described for reconstruction of the abdominal wall is to reduce the tension of the suture line. These techniques include the use of synthetic materials (meshes) , use of the hernial sac itself ("Lázaro da Silva" technique)12, advancement of musculoaponeurotic flaps (technique of "components separation")13, muscular, musculocutaneous and musculofasciocutaneous flaps9, use of autologous and heterologous grafts9, and tissue expansion techniques such as progressive pneumoperitoneum and tissue expanders1.
Cadavers at room temperature (22ºC) were used in this study in order to minimize the effects of low temperatures on the tissues, as refrigeration could affect the traction measurements. Therefore, this variable did not influence the results13 . To ensure uniformity of the sample, only male cadavers were studied. No cadavers over 60 years of age were studied, due to the possibility of tissue flaccidity of these individuals.
Excision of the linea alba in the cadavers proved to be an effective experimental method for the study of the physiopathogenesis and treatment of incisional hernias of the median line, and this model is based on the methodology described by Nahas and Ferreira10. The traction measurement was performed at infraumbilical points 2, 4, 6 and 8 cm from the lower edge of the navel, and at points 3, 6 and 9 cm from the upper edge of the navel, in the anterior sheath of the rectus abdominis muscle. The distribution of the aponeurotic points was designed to enable a uniform mapping of the entire anterior rectus sheath. This aponeurosis is an anatomical structure which plays an important role in the closure of median abdominal incisions. This experiment simulated the anatomical reality found by the surgeon when closing a median incision.
Traction strength was expressed numerically by the regional traction coefficients. The traction coefficient5 enables measurements to become comparable, regardless of the traction distance. The comparison of regional coefficients in the various levels of the anterior layer did not reveal any statistical significant difference, which means that there was no difference in resistance to medial traction between the points studied. Therefore, there is no region where anterior aponeurosis could be closed with less tension.
The technique of "components separation"13 was conceived as an effective alternative for reducing the tension of the suture line, with the use of autologous tissues. It was systematically evaluated in cadavers5 and other techniques using different musculoaponeurotic components were developed and evaluated6,14,15 using a methodology described by Nahas et al.5. Although this study does not propose any technical variation, the method was developed based on this study.
The present study enables studies to be guided in the sense of carrying out comparative studies of traction of the anterior and posterior layers of the rectus sheath, which can facilitate the choice of aponeurosis in which reconstruction can be achieved with less tension.
Conclusion
There is no variation in tension along the whole extension of the anterior rectus sheath.
Received: January 20, 2010
Review: March 23, 2010
Accepted: April 28, 2010
Conflict of interest: none
Financial source: none
1 Research performed at Plastic Surgery Post-Graduation. Integration (MINTER) between the Federal University of São Paulo (UNIFESP) and University of the Valley of the Sapucaí (UNIVAS), Brazil.
- 1- Wadstrom J, Gerdim B. Closure of the abdominal wall; how and why? Acta Chir Scand. 1990;156:75-82.
- 2- Ruciski J, Margolis M, Panagopoulos G, Wise L. Closure of abdominal midline fascia: meta-analysis delineates the optimal technique. Am Surg. 2001;67(5):421-6.
- 3- Tognini JRF, Goldenberg S. Síntese da parede abdominal: sutura continua ou com pontos separados? Revisão de literatura. Acta Cir Bras. 1998;13(2):116-22.
- 4- Van Geffen HJAA, Simmermarcher RKJ, Van Vroonhoven TJMV, Werken CVD. Surgical treatment of larger contaminated abdominal wall defects. J Am Coll Surg. 2005;201:206-12.
- 5- Nahas FX, Ishida J, Gemperli R, Ferreira MC. Abdominal wall closure after selective aponeurotic incision and undermining. Ann Plast Surg. 1998;41(6):606-13.
- 6- Amorim CR, Nahas FX, Souza VC, Ely PB, Silveira RAB, Novo NF, Ferreira LM. Traction strength of the posterior and anterior layer of the rectus abdominis muscle sheath in cadavers. Acta Cir Bras. 2007;22(4):254-8.
- 7- Cohen M, Morales R, Fildes J, Barrett J. Staged reconstruction after gunshot wounds to the abdomen. Plast Reconstr Surg. 2001;108:83-92.
- 8- Höer J, Klinge U, Anurov M, Titkova S, Oettinger A, Schumpelick V. Tension banding closure of laparotomies: results of an experimental study in dogs. Langenbecks Arch Surg. 2002;307:309-14.
- 9- Mäkelä JT, Kiviniemi H, Juvonen T, Laitinen S. Factors influencing wound dehiscence after midline laparotomy. Am J Surg. 1995;170:387-90.
- 10- Nahas FX, Ferreira LM. Cadáver as an model to study abdominal wall tension. Acta Cir Bras. 2003;18(special suppl.):37-45.
- 11- Van Geffen HJAA, Simmermarcher RKJ, Bosscha K, Van der Werkwn C, Hillen B. Anatomical considerations for surgery of the anterolateral abdominal wall. Hernia. 2004;8:93-7.
- 12- Lazaro da Silva A. Surgical correction of longitudinal median or paramedian incisional hernia. Surg Gynecol Obstet. 1979;148:579-83.
- 13- Ramirez OM, Ruas E, Dellon L. Components Separation method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg. 1990;86(3):19-26.
- 14- Barbosa MV, Nahas FX, Garcia EB, Ayaviri NA, Juliano Y, Ferreira LM. Use of the anterior sheath for abdominal wall reconstruction: study in cadaver. Scand J Plast Reconst Surg Hand Surg. 2007,41(6)273:7.
- 15- Barbosa MV, Nahas FX, Oliveira Filho RS, Ayaviri NAM, Novo NF, Ferreira LM. A variation in the component separation technique that preserves linea semilunaris: a study in cadavers and a clinical case. J Plast Reconstr Aesthet Surg. 2010;63(3):524-31.
Publication Dates
-
Publication in this collection
26 July 2010 -
Date of issue
Aug 2010
History
-
Accepted
28 Apr 2010 -
Reviewed
23 Mar 2010 -
Received
20 Jan 2010