Abstracts
PURPOSE: To analyze the viability of using SITRACC® (single-portal access) to make partial or total nephrectomy in pigs and also to describe the technical difficulties found during these surgical procedures. METHODS: Ten pigs (Landrace specie) with 20kg in average were distributed in two groups: Group A - total right nephrectomy - and Group B - partial left nephrectomy -. The anesthetic procedure was initially done with thiopental (10mg/kg) and maintained with halothane. The surgical procedures were performed inside the Surgical Technique Room from Pontifical Catholic University of Parana (PUCPR). RESULTS: It was analyzed the surgery duration, time to insert SITRACC®, the volemic loss and the size of the organ. In the first surgeries, the surgical time and blood volume loss were higher (between 15 to 43 minutes and 120 to 400 mL, respectively). The more the procedure was performed, the more the surgeons were used to the technique, so the bleeding and the time of surgery was significantly reduced to 15 minutes and 50 mL of blood loss, respectively. The difficulties found were associated with the nippers, however that was not relevant for the surgical technique. It was also found that the intra-body suture caused an expressive volemic loss. CONCLUSION: The total and partial nephrectomy through umbilical single-access by using SITRACC® was feasible and safe in pigs.
Nephrectomy; Laparoscopy; Swine
OBJETIVO: Analisar a viabilidade do uso do SITRACC® (portal único) para realização de nefrectomia total e parcial em suínos e descrever as dificuldades técnicas encontradas durante os atos cirúrgicos propostos. MÉTODOS: Foram operados 10 porcos da espécie Landrace, com peso médio de 20 Kg, distribuidos em dois grupos: Grupo A: nefrectomia total à direita e Grupo B: nefrectomia parcial à esquerda. A indução anestésica foi realizada com a administração de tiopental (10mg/Kg) e mantida com halotano. Os procedimentos cirúrgicos foram realizados na sala de Técnica Operatória da Pontifícia Universidade Católica do Paraná (PUCPR). RESULTADOS: Foram analisados tempo total de cirurgia, tempo de colocação do SITRACC®, perda volêmica e tamanho da peça. Nas primeiras cirurgias realizadas o tempo cirúrgico e o volume do sangramento foram maiores (entre 15 - 43 minutos e entre 120 - 400 ml, respectivamente); à medida que se adquiriu prática com a técnica, esses apresentaram reduções significativas para menos que 15 minutos e 50 ml, respectivamente. A dificuldade encontrada foi na articulação das pinças, porém, não afetou a técnica cirúrgica. Além disso, houve dificuldade na realização da sutura intracorpórea acarretando uma perda volêmica maior. CONCLUSÃO: A nefrectomia total e parcial por acesso umbilical único com uso do SITRACC® é plenamente viável e segura em suínos.
Nefrectomia; Laparoscopia; Suínos
5 - ORIGINAL ARTICLE
EXPERIMENTAL UROLOGY
Laparoscopic nephrectomy with single-portal access Sitracc® in swines1 Correspondence: Fernando Meyer Pontifícia Universidade Católica do Paraná (PUCPR) Departamento de Urologia Rua Portugal, 307 80510-280 Curitiba - PR Brasil Tel.: (55 41)3074-7478 Fax: (55 41)3015-0303 fmeyer@onda.com.br
Nefrectomia laparoscópica com portal único Sitracc® em suínos
Fernando MeyerI; Daniel Joaquim CoutinhoII; Denise Sbrissia e Silva GouveiaIII; Juliana Navarro LizanaIV; Luiz Felipe DziedrickiV
IPhD, Chairman Full Professor, Urology Division, PUCPR, Head Department of Urology, Cajuru University Hospital, PUCPR, Curitiba-PR, Brazil. Main author, supervised all phases of the study, provided guidelines for the surgical interventions, responsible for conception of the study and critical revision, surgical procedures, manuscript writing, responsible for English language
IIFellow of Surgery, Urology Division, Cajuru University Hospital, PUCPR, Curitiba-PR, Brazil. Helped with technical procedures, data collection, surgical procedures, manuscript writing
IIIMD, Volunteer, Cruz Vermelha Hospital, Curitiba-PR, Brazil. Helped with technical procedures, data collection, surgical procedures, manuscript writing
IVMD, Fellow of Occupational Medicine, PUCPR, Curitiba-PR, Brazil. Surgical procedures, acquisition and interpretation of data, manuscript writing
VMD, Resident, Department of Gynecology and Obstetrics, Santa Brigida Maternity Hospital, Curitiba-PR, Brazil. Surgical procedures, acquisition and interpretation of data, manuscript writing
Correspondence Correspondence: Fernando Meyer Pontifícia Universidade Católica do Paraná (PUCPR) Departamento de Urologia Rua Portugal, 307 80510-280 Curitiba - PR Brasil Tel.: (55 41)3074-7478 Fax: (55 41)3015-0303 fmeyer@onda.com.br
ABSTRACT
PURPOSE: To analyze the viability of using SITRACC® (single-portal access) to make partial or total nephrectomy in pigs and also to describe the technical difficulties found during these surgical procedures.
METHODS: Ten pigs (Landrace specie) with 20kg in average were distributed in two groups: Group A - total right nephrectomy - and Group B - partial left nephrectomy -. The anesthetic procedure was initially done with thiopental (10mg/kg) and maintained with halothane. The surgical procedures were performed inside the Surgical Technique Room from Pontifical Catholic University of Parana (PUCPR).
RESULTS: It was analyzed the surgery duration, time to insert SITRACC®, the volemic loss and the size of the organ. In the first surgeries, the surgical time and blood volume loss were higher (between 15 to 43 minutes and 120 to 400 mL, respectively). The more the procedure was performed, the more the surgeons were used to the technique, so the bleeding and the time of surgery was significantly reduced to 15 minutes and 50 mL of blood loss, respectively. The difficulties found were associated with the nippers, however that was not relevant for the surgical technique. It was also found that the intra-body suture caused an expressive volemic loss.
CONCLUSION: The total and partial nephrectomy through umbilical single-access by using SITRACC® was feasible and safe in pigs.
Key words: Nephrectomy. Laparoscopy. Swine.
RESUMO
OBJETIVO: Analisar a viabilidade do uso do SITRACC® (portal único) para realização de nefrectomia total e parcial em suínos e descrever as dificuldades técnicas encontradas durante os atos cirúrgicos propostos.
MÉTODOS: Foram operados 10 porcos da espécie Landrace, com peso médio de 20 Kg, distribuidos em dois grupos: Grupo A: nefrectomia total à direita e Grupo B: nefrectomia parcial à esquerda. A indução anestésica foi realizada com a administração de tiopental (10mg/Kg) e mantida com halotano. Os procedimentos cirúrgicos foram realizados na sala de Técnica Operatória da Pontifícia Universidade Católica do Paraná (PUCPR).
RESULTADOS: Foram analisados tempo total de cirurgia, tempo de colocação do SITRACC®, perda volêmica e tamanho da peça. Nas primeiras cirurgias realizadas o tempo cirúrgico e o volume do sangramento foram maiores (entre 15 - 43 minutos e entre 120 - 400 ml, respectivamente); à medida que se adquiriu prática com a técnica, esses apresentaram reduções significativas para menos que 15 minutos e 50 ml, respectivamente. A dificuldade encontrada foi na articulação das pinças, porém, não afetou a técnica cirúrgica. Além disso, houve dificuldade na realização da sutura intracorpórea acarretando uma perda volêmica maior.
CONCLUSÃO: A nefrectomia total e parcial por acesso umbilical único com uso do SITRACC® é plenamente viável e segura em suínos.
Descritores: Nefrectomia. Laparoscopia. Suínos.
Introduction
The laparoscopic surgery consists on the pelvic and abdominal cavity visualization through an optic lens connected to a camera. The advantages of the minimally invasive surgery were clearly demonstrated by pioneer surgeons, such as Kurt Semm, who made the first laparoscopic appendectomy in humans in 1980. Eric Muhe was the one who did the first laparoscopic cholecytectomy in humans in 1985. In 1987, laparoscopic cholecystectomy was re-introduced by Philippe Mouret and other pioneers1, however, after the digital era the role world experimented what was called the laparoscopic revolution. The relationship between urology and laparoscopy had a delayed beginning in comparison to the stomach surgery and gynecology. The introduction of the laparoscopic technique in the urology was initially performed by Cortesi et al.2, who had published in 1976 a case of propedeutic laparoscopy in an 18 years old young with bilateral cryptorchid. The definitive introduction of the laparoscopic technique in urology was performed in USA, 1990, by Clayman et al.3, who had done a successful entirely laparoscopic nephrectomy in an octogenary woman with oncocitoma (a renal benign tumor).
In the last decade, there was evidenced some exponential advances and laparoscopic applications in all surgical fields.
The development of the laparoscopic surgery in nephrology represented a considerable benefit for the patients. From the esthetic point of view, this procedure leave less scars, so the abdominal asymmetries due to post lumbotomy - such as hernia and flaccid abdomen - could be avoided.
Since the first laparoscopic nephrectomy, described by Clayman et al.3, the laparoscopy started to represent an attractive option to remove the kidneys affected by benign or malign diseases.
The total laparoscopic nephrectomy has been showing along the years to be a procedure that provides a less hospitalization time for the patients. The effective renal cancer control has no significant efficacy in comparison to an open radical nephrectomy. Moreover, if the patient has a renal function lower than 10%, the best therapy is total surgery, however it appears that since the diagnostic ways have been developing and there is a greater possibility to detect smaller renal tumor mass, it is possible to take into account the partial nephrectomy as indication for the most of cases.
In relation to the radical nephrectomy, which is the classical way of treating the renal tumors, the laparoscopy came as a minimal invasive therapeutic option. It has received world recognition after uncountable works describing the similar results in comparison to the conventional open surgery. It has also demonstrated low rates of complications, besides its many different applications, such as: obesity, local advanced tumors and big tumor masses. The indication of partial nephrectomy by laparoscopy in some occasions, like in patients with 4 cm of renal tumors, unilateral tumor, unilateral tumor with little function or with no function in the contralateral.
In a relatively short period of time though, there were many operations adapted to the minimal invasive method aiming to modify those techniques in a less invasive option. Herewith some modifications have emerged such as: NOTES (Natural Orifice TransEndoscopic Surgery) which natural orifices (mouth, vagina, urethra, etc.) are used to introduce laparoscopic instruments; and the SINGLE-PORT, which uses only a single-access to the peritoneal cavity instead of using many accesses.
In urology, the first procedures using SINGLE-PORT were published by Desai et al.4, who had done pyeloplasty and nephrectomy with a trocar (R-PORT®, Advanced Surgical Concepts, Dublin, Ireland). Some studies indicate that the laparoscopical nephrectomies using SINGLE-PORT have shown less pain, less convalescence and less use of narcotic analgesics5. In Brazil, Martins et al.6, from Estacio de Sa University (Rio de Janeiro) and Positivo University (Parana), supported by EDLO S/A (Canoas-RS) had developed a trocar for using in a single-access abdominal surgery. They nominated it as SITRACC® (Single Trocar Access - Figure 1). This instrument consists on a four way trocar, combined with flexible endoscopy, videosurgery and use of special flexible material. It can be used through the navel, vagina (in experimental phase) or through an access near the indacision place. It is similar to the conventional laparoscopical surgery, but it has a new articulated system which permits the surgeon to work in different movements in the same axis.
Between December 2007 and March 2008, Martins et al.6 had used the SITRACC® to make the cholecystomy in ten female pigs, weighting 30kg in average. All the surgeries were completed without the need of classical laparoscopical convertion, therefore, they concluded that this new procedure is feasible in pigs. The possibility to extend it to humans depends on the improvement of the technique and instruments6.
SITRACC® is a technique that improves the quality of the surgical factor, making it possible to access a single way. The reduction of the injuries by inserting the trocars and the improvement of the scars has been showing the benefits and the relevance to the patient: the esthetic. In contrast with today, in the past, the esthetic factor was not so relevant, but now especially children and women concern about it.
Once the medicine advances, the results have aimed not only the reduction of morbity and mortality, but the patient's global improvement which includes also the emotional aspect in the post-operatory period. Thus, it is given the importance to SITRACC®, which is a new method and gives to patient better psychological improvement in comparison to the classical surgical techniques.
The present experiment aimed to study the use of SITRACC® to make a partial and total nephrectomy in pig. The objective of this work consists on analyzing the use of this new surgical instrument in two different surgical techniques, therefore, it also aims to describe the difficulties found to execute the proposed procedure.
Methods
All the experiments were done according to Brazilian College of Animal Experimentation (COBEA), after approval by the Ethics Committee on Animal Use (CEUA).
Ten pigs, Landrace specie, with 20 kg in average were distributed in two operations groups: Group A (total right nephrectomy) and Group B (partial left nephrectomy).
It was intentioned to use the less number of pigs, so two procedures were done in the same animal: the total and partial nephrectomy. This procedure has as first step using Group A (total right nephrectomy), after it, the second step consisted on changing the animals' position and executing the partial left nephrectomy (with Group B).
The anesthesia was done with thiopental 10 mg/kg and maintained with halothane.
The stages of the surgery consisted on the following sequence: anesthesia induction; fixation of the animal on the surgical table in lateral right decubitus; the abdominal area was cleaned with iodine alcohol; the establishment of the operatory place; incision in approximately 2.5 cm under the umbilical scar; introduction of SITRACC® through the incision (Figure 2); total right nephrectomy according to the laparoscopical technique (Figure 3); hemosthasia and cavity revision; SITRACC® withdrawal together with the right kidney (Figure 4); animal repositioning (lateral right decubitus) to do the partial nephrectomy (Group B); the abdominal area was cleaned with iodine alcohol; the establishment of the operatory place; introduction of SITRACC® through the incision; partial left nephrectomy according to the laparoscopical technique; hemosthasia and cavity revision; SITRACC® withdrawal together with resect renal segment, abdominal sewing with a mononylon string 2-0; and finally the euthanasia.
To execute the euthanasia in pigs, 20 mL of KCl was administrated in a quick dose.
Results
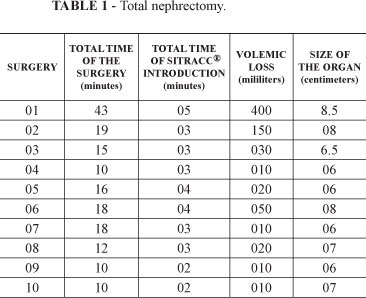
The ten operatory procedures aimed to evaluate the surgical technique in pigs and also to foresee the possible complications associated to this technique in humans. Therefore, the data collected to study it were: total surgery duration; the time of introducing SITRACC®; volemic loss; and the size of the removed organ (Table 1). It had been also demonstrated that as the surgeons become more familiar with the technique, the time of SITRACC® introduction, the surgery time and the bleeding time diminished.
The results indicate the total and partial nephrectomy feasibility by using SITRACC®. It is important to emphasize that adequate training is needed, once the nippers and the other materials differ from what is used in traditional laparoscopic nephrectomy, although, they did not affected the surgical technique (Table 2, Figure 4).
Discussion
In the first procedures, due to the surgical team's lack of experience, it was found difficulties to introduce SITRACC®, which increased the time of surgery (15 to 43 minutes) and the blood loss was also higher due to the delayed arterial renal clamping (120 to 400 mL). The other difficulties of the technique were associated with movements' coordination between the first auxiliary and the surgeon, once the angle between the instruments was reduced. Furthermore, there were difficulties associated to the intra-body suture in the partial nephrectomy, resulting in a higher blood loss.
The surgery number four (Table 2) could not be concluded because the bleeding from the total nephrectomy was excessive, so it has invalidated the technique. In this case the operatory area was compromised and without adequate visibility, thus, making the surgery team finishing the operation before concluding it by euthanasia to reduce the animal's suffering.
As long as the surgeons become familiar with the technique (duration time of 20 minutes) and there were also less volemic loss (50 mL), the problem with the synchronization between the surgeon and the first auxiliary was overcome. The introduction of SITRACC® has also diminished from 5 to 2 minutes in the last operatory procedures.
Conclusions
The total and partial videolaparoscopic nephrectomy by umbilical access with SITRACC® was feasible and safe for the experimental animals. The possibility to make this procedure a minimal invasive surgery may depend on the development and adaptation of new instruments of work. Therefore, this study may be used to future comparisons and surgical indications, because it was firstly evidenced the possibility to use this new technique in swines to facilitate later its use in humans.
Received: October 11, 2011
Review: December 07, 2011
Accepted: January 10, 2012
Conflict of interest: none
Financial source: none
1 Research performed at Operative Technique and Experimental Surgery Division, Department of Urology, Pontifical Catholic University of Parana (PUCPR), Curitiba-PR, Brazil.
- 1. Mouret P. From the first laparoscopic cholecystectomy to the frontiers of laparoscopic surgery. Dig Surg. 1991;8(2)124-5.
- 2. Cortesi N, Baldini A, Ferrari P, Manenti A, Morano FP, Zambarda E. Diagnosis of bilateral abdominal cryptorchidism by laparoscopy. Endoscopy. 1976;8(1)33-4.
- 3. Clayman RV, McDougall EM. Laparoscopic nephrectomy and nephroureterectomy in the octogenarian with a renal tumor. J Laparoendosc Surg. 1994;4(3) 233-6.
- 4. Desai MM, Rao PP, Aron M, Pascal-Haber G, Desai MR, Mishra S, Kaouk JH, Gill IS. Scarless single port transumbilical nephrectomy and pyeloplasty: ûrst clinical report. BJU Int. 2008;101(1)83-8.
- 5. Kommu SS, Kaouk JH, René A. Laparo-endoscopic single-site surgery preliminary advances in renal surgery. BJU Int. 2009;103(8)1024-37.
- 6. Martins MVDC, Skinovsky J, Coelho DE, Torres MF. SITRACC - Single Trocar Access: A New Device for a New Surgical Approach. Bras J Video-Sur. 2008;1(2)61-3
Publication Dates
-
Publication in this collection
26 Mar 2012 -
Date of issue
Mar 2012
History
-
Received
11 Oct 2011 -
Accepted
10 Jan 2012 -
Reviewed
07 Dec 2011