Abstracts
PURPOSE: To determine whether it is possible and the difficulty of anatomical placement of guide wires for reconstruction of the two bands of the anterior cruciate ligament using transtibial technique and to measure the angle and positioning of the anatomic tibial guide wires for this technique. METHODS: Ten cadaver knees were dissected and a guide wire was positioned in the center of origin and insertion of each band. Were collected measurements of the distance from: 1) the entry point of the guide wire on tibial tuberosity; 2) the medial end of the tibia; 3) the tibial articular surface. Were also measured the medial and caudal angles of the guide wires. RESULTS: For the anteromedial band the medial angle was 19±5º and the caudal was 44±4º.The distances were 20±2 mm from anterior tuberosity, 26±5 mm from the tibial plateau and 25±5 mm from the medial end of the tibia. For the posterolateral band the medial angle was 26±5º and the caudal one was 36±8°. The distances were 31±6 mm for the anterior tuberosity, 24±4 mm for the tibial plateau and 17±7 mm from the end of the tibia. CONCLUSIONS: It is possible to position the guide wires of the two bands to reconstruct the anterior cruciate ligament using transtibial technique. The parameters for the proper positioning of the guide wire from anteromedial band is caudal angle of 44º with entry point 20 mm from anterior tuberosity; for the posterolateral band the caudal angle is 36º; from the tibial tuberosity the distance is 31 mm. This technique is difficult to perform leaving its questionable reproducibility.
Anatomy; Knee; Anterior Cruciate Ligament; Cadaver
OBJETIVOS: Determinar se é possível o posicionamento anatômico dos fios-guia para reconstrução das duas bandas do ligamento cruzado anterior pela técnica transtibial, sua dificuldade técnica e medir o posicionamento angular dos parâmetros anatômicos dos fios-guia tibiais para esta técnica. MÉTODOS: Dez joelhos de cadáveres foram dissecados e um fio guia foi posicionado no centro da origem e inserção de cada banda. Foram coletadas as medidas da distância do ponto de entrada do fio-guia à tuberosidade anterior da tíbia, a extremidade medial da tíbia e a superfície articular tibial. Também foram medidos os ângulos mediais e caudais dos fios-guia. RESULTADOS: Para a banda anteromedial o ângulo medial foi de 19±5º e o caudal de 44±4º. As distâncias foram de 20±2 mm da tuberosidade anterior, 26±5 mm do platô tibial e 25±5 mm da extremidade medial da tíbia. Para a banda posterolateral o ângulo medial foi de 26±5° e o caudal de 36±8°. As distâncias foram de 31±6 mm da tuberosidade anterior, 24±4 mm do platô tibial e 17±7 mm da extremidade medial da tíbia. CONCLUSÕES: É possível posicionar os fios-guia para reconstrução das duas bandas do ligamento cruzado anterior pela técnica transtibial. Os parâmetros para o posicionamento adequado do fio-guia da banda anteromedial são ângulo caudal de 44° com ponto de entrada a 20 mm da tuberosidade anterior; para a banda posterolateral o ângulo caudal é de 36° e a distância é de 31 mm da tuberosidade anterior da tíbia. Essa técnica é de difícil execução deixando sua reprodutibilidade questionável.
Anatomia; Joelho; Ligamento Cruzado Anterior; Cadáver
1 - ORIGINAL ARTICLE
ANATOMICAL STUDY
Anatomical study of the positioning of guide wires for the reconstruction of the two bands of the anterior cruciate ligament using transtibial technique1 1 Research performed at Postgraduate Program, Department of Surgery, Evangelic Faculty of Parana (FEPAR) and Department Anatomy, Clinics Hospital, Federal University of Parana (UFPR), Curitiba-PR, Brazil.
Estudo anatômico do posicionamento dos fios-guia para a reconstrução das duas bandas do ligamento cruzado anterior pela técnica transtibial
Christiano Saliba UlianaI; Marcio Fernando Aparecido de MouraII; Mario NambaIII; Edmar Stieven-FilhoIII; Jurandir Marcondes Ribas-FilhoIV; Osvaldo MalafaiaV
IAssistant Professor, Department of Surgery, UFPR, Curitiba-PR, Brazil. Responsible for intellectual, scientific content of the study and critical revision
IIPhD, Assistant Professor, Department of Surgery, UFPR, Curitiba-PR, Brazil. Helped with technical procedures and collection of study
IIIMaster, Assistant Professor, Department of Surgery, UFPR, Curitiba-PR, Brazil. Helped with technical procedures and collection of study
IVFull Professor, Department of Surgery, FEPAR, Curitiba-PR, Brazil. Manuscript writing and critical revision
VFull Professor, Head, Department of Surgery, FEPAR and UFPR, Coordinator of Principles of Surgery, Postgraduate Program, FEPAR, Curitiba-PR, Brazil. Mentor of Master degree Edmar Stieven-Filho. Responsible for conception, scientific content and supervision all phases of the study; manuscript writing; critical revision
Correspondence Correspondence: Christiano Saliba Uliana Rua Desembargador Motta, 2219/601 80420-190 Curitiba - PR Brasil chrisuliana@hotmail.com
ABSTRACT
PURPOSE: To determine whether it is possible and the difficulty of anatomical placement of guide wires for reconstruction of the two bands of the anterior cruciate ligament using transtibial technique and to measure the angle and positioning of the anatomic tibial guide wires for this technique.
METHODS: Ten cadaver knees were dissected and a guide wire was positioned in the center of origin and insertion of each band. Were collected measurements of the distance from: 1) the entry point of the guide wire on tibial tuberosity; 2) the medial end of the tibia; 3) the tibial articular surface. Were also measured the medial and caudal angles of the guide wires.
RESULTS: For the anteromedial band the medial angle was 19±5º and the caudal was 44±4º.The distances were 20±2 mm from anterior tuberosity, 26±5 mm from the tibial plateau and 25±5 mm from the medial end of the tibia. For the posterolateral band the medial angle was 26±5º and the caudal one was 36±8°. The distances were 31±6 mm for the anterior tuberosity, 24±4 mm for the tibial plateau and 17±7 mm from the end of the tibia.
CONCLUSIONS: It is possible to position the guide wires of the two bands to reconstruct the anterior cruciate ligament using transtibial technique. The parameters for the proper positioning of the guide wire from anteromedial band is caudal angle of 44º with entry point 20 mm from anterior tuberosity; for the posterolateral band the caudal angle is 36º; from the tibial tuberosity the distance is 31 mm. This technique is difficult to perform leaving its questionable reproducibility.
Key words: Anatomy. Knee. Anterior Cruciate Ligament. Cadaver.
RESUMO
OBJETIVOS: Determinar se é possível o posicionamento anatômico dos fios-guia para reconstrução das duas bandas do ligamento cruzado anterior pela técnica transtibial, sua dificuldade técnica e medir o posicionamento angular dos parâmetros anatômicos dos fios-guia tibiais para esta técnica.
MÉTODOS: Dez joelhos de cadáveres foram dissecados e um fio guia foi posicionado no centro da origem e inserção de cada banda. Foram coletadas as medidas da distância do ponto de entrada do fio-guia à tuberosidade anterior da tíbia, a extremidade medial da tíbia e a superfície articular tibial. Também foram medidos os ângulos mediais e caudais dos fios-guia.
RESULTADOS: Para a banda anteromedial o ângulo medial foi de 19±5º e o caudal de 44±4º. As distâncias foram de 20±2 mm da tuberosidade anterior, 26±5 mm do platô tibial e 25±5 mm da extremidade medial da tíbia. Para a banda posterolateral o ângulo medial foi de 26±5° e o caudal de 36±8°. As distâncias foram de 31±6 mm da tuberosidade anterior, 24±4 mm do platô tibial e 17±7 mm da extremidade medial da tíbia.
CONCLUSÕES: É possível posicionar os fios-guia para reconstrução das duas bandas do ligamento cruzado anterior pela técnica transtibial. Os parâmetros para o posicionamento adequado do fio-guia da banda anteromedial são ângulo caudal de 44° com ponto de entrada a 20 mm da tuberosidade anterior; para a banda posterolateral o ângulo caudal é de 36° e a distância é de 31 mm da tuberosidade anterior da tíbia. Essa técnica é de difícil execução deixando sua reprodutibilidade questionável.
Descritores: Anatomia. Joelho. Ligamento Cruzado Anterior. Cadáver.
Introduction
Since the 80s, the arthroscopic reconstruction of the ruptured anterior cruciate ligament (ACL) became the gold standard of treatment for this injury1. Although the reconstruction is done with a single band, anatomical studies show that the ACL consists of two bands, one anteromedial and one posterolateral2,3.
Despite excellent results with ACL reconstruction technique by a single band2; long-term studies show 15% to 30% of residual rotational instability, persistence and progression to rebound osteoarthritis in 40% of cases when this technique is used4-7.
One of the techniques which aim to improve the shortcomings of conventional reconstruction is the rebuilding of the two bands of the ACL8. This reconstruction can be done basically in two ways: 1 - first drilling tunnels in the tibia and then doing the same one femoral site, through tibia, known as reconstruction or transtibial monotunel8; 2) to drill the tunnel of the femur and tibia independently of each other, ie, the two tunnels are drilled cortical external to internal, also called outside-in or double incision9.
Transtibial reconstruction is the most performed, but it adds a difficulty to the procedure. The articular tibial tunnel outlet, anatomically well positioned, is not enough for a proper positioning of the graft. The perforating angles must also be correct to allow proper preparation of the femoral tunnel, because the second drilling is through the tunnel previously done10. There are many studies to define the location and angles of guide wires suitable for construction of tunnels for the ACL transtibial technique of dual-band8,10,11.
The aim of this study was: 1) to determine whether it is possible and the difficulty of anatomical placement of guide wires for reconstruction of the two bands of the anterior cruciate ligament using transtibial technique and 2) to measure the angle and positioning of the anatomic tibial guide wires for this technique.
Methods
The study was conducted on the Department of Anatomy of Federal University of Parana, Curitiba-PR, Brazil during April and May of 2011.
Ten dissected cadaver knees were randomly chosen without distinction of sex and age. They were numbered from 1 to 10 according to the chronological sequence of dissection. For measurements of the distances between the points of interest as well as the angles, were used needles, caliper rule, steel wires with two millimeters in diameter, a battery puncher and two paintbrushes for color demarcations.
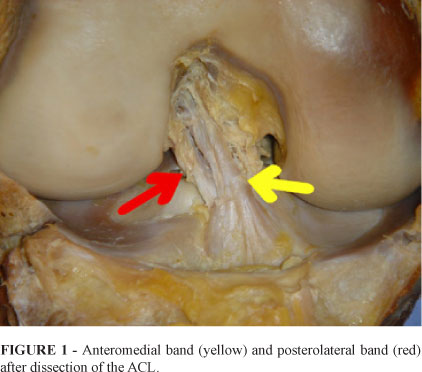
Were identified during the dissection, the anterior cruciate ligament (ACL) and its two bands, the anteromedial and posterolateral, as shown in Figure 1.
The bands were cut and the center of origin and insertion points were marked with colored brushes. Two guide wires were passed, one to anteromedial band (Fam) and another band in posterolateral (FPL). They were passed with free hand through the tibia, until they formed a line that unites the center of the tibial insertion to the center of the femoral origin.
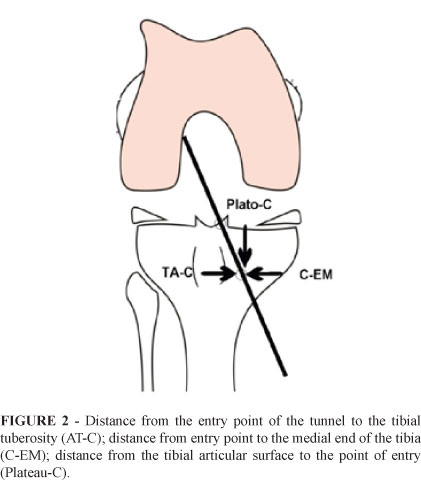
The anatomic relationships of interest, applied to both bands, were:
1. Distance from entry point of the guide wire in tibial anterior tuberosity (AT-C);
2. Distance from entry point of the guide wire in the medial end of the tibia (C-EM);
3. Distance from the tibial articular surface to the entry point of the guide wire (Plateau-C);
4. Length of the tunnel (Figure 2).
To determine the length of the tibial tunnel, was used a caliper rule to measure the difference in total length of the guide wire by measuring the outside wire, when it was getting off the tibial plateau. The angles of interest were:
1. Caudal angle - the angle of the guide wire (Fam or FPL) with the plane of the tibial plateau (axial)
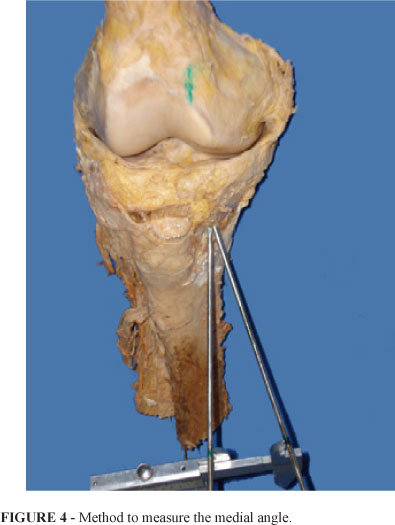
2. Medial angle - guide wire angle (Fam or FPL) in the sagittal plane (Figure 3).
To obtain the value of the medial angle was necessary to establish a triangle formed by the guide wires (Fam or FPL), with another wire placed at the tibial tuberosity and parallel to the axial and sagittal planes (Figure 4).
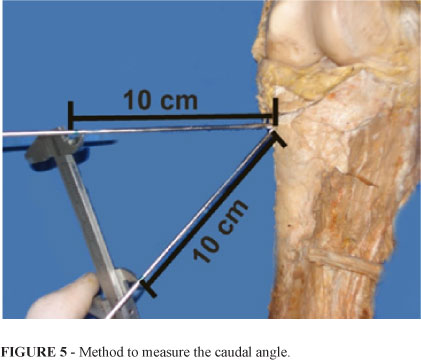
To obtain the value of the caudal angle was necessary to establish a triangle formed by the guide wires (Fam or FPL), with another wire placed parallel to the tibial plateau (axial) (Figure 5).
A triangle was formed by two wires and an imaginary line joining the two 10 cm of its acute angle (Figure 5). The length of the third line determines the angle of the guide wire by trigonometry. These data were extracted with the help of AutoCAD® software for the determination of the angles (Figure 6).
Results
In all cases it was possible to reach the anatomical position by the transtibial technique. In some it was technically difficult and required the passage of the guide wire numerous times, especially for the FPL.
The distance measurements of the guide wire to anatomical landmarks and the caudal and medial angles of the anteromedial band, are shown in Table 1 and the posterolateral band in Table 2.
Discussion
Nowadays the importance of reconstruction of the ACL two bands is always in discussed12. One of the barriers to reconstruction with two bands is the difficulty in its performance, especially by the transtibial technique. For some, the transtibial technique cannot reproduce the correct anatomy of the ACL13. For them the only way to reconstruct the ACL with two bands in its original anatomical position, is drilling tunnels independently9. There are studies that show the possibility of reconstructing the anatomy of the ACL by a double band for the transtibial technique, as well as the present study8,14.
The fact that some authors got the opportunity to reproduce the technique of anatomical reconstruction of the ACL via the transtibial8,14 shows that it is possible to do it, even taking into account the fact that others have failed13. But it is questionable the reproducibility of the technique, because in some cases was very difficult to reproduce the anatomy in laboratories; certainly, in the surgical environment would increase these difficulties.
The wires in the anteromedial band measured 20 mm medial to the tibial tuberosity, 25 mm in tibial plateau and with caudal angulation of 46º. This shows how the tunnel must be superficial in the joint surface to reach the anatomical position. The posterolateral tunnel will be more superficial, due to the fact it is closer to the plateau (24 mm) and in minor caudal angle (36º).
Seibold16 found by MRI enlargement in 100% of cases and communication between the tunnels in 41% one year after surgery. This high rate of communication underlines the close anatomical relationship between the two tibial tunnels. This could cause difficulties in a possible revisional surgery. The data in this study, showing the proximity of the guide wires, corroborates the conclusion of these authors.
In a published anatomical dissection of 50 knees to determine areas of positioning of the two tibial tunnels, was noted significant anatomical variation and the impossibility to locate the tunnel in the center of insertion of each band, because there was not enough space for its realization15. They recommended that the anteromedial tunnel respect a "security zone" of 2 mm from the anterior edge of the remaining stump of the ligament to prevent impingement of the femur. To prepare the posterolateral tunnel is necessary to take special precautions in not cause damage to the posterior horn of the lateral meniscus.
The reconstruction with double band is more difficult when the femoral tunnels are created from the tibial tunnel, carrying greater possibility of error. Facing this problem, to ensure the correct position to the neoligament, femoral anatomical references can be recommended for making femoral bands tunnel in posterolateral and anteromedial position, or a browser can be used8.
Based on the results of this research, it was possible to reproduce the optimal placement of guide wires for the construction of ACL anteromedial and posterolateral tunnels bands via transtibia. For the anteromedial band the angle was 19±5º, the caudal angle was 44±4º. The distances of anatomical points were 20±2 mm from anterior tuberosity, 26±5 mm from the tibial plateau and 25±5 mm from the medial end of the tibia.
For the posteriolateral band the angle was 26±5º, the caudal angle was 36±8º. The distances of anatomical points were 31±6 mm from anterior tuberosity, 24±4 mm from the tibial plateau and 17±7 mm from the end of the tibia. For the anteromedial band, there were no technical difficulties in obtaining an optimal placement. However, for the positioning of the guide wire in the posterolateral band, great difficulties were encountered due to their entry point to be very medial in tibia.
Conclusions
It is possible to position the guide wires of the two bands to reconstruct the anterior cruciate ligament using transtibial technique. The parameters for the proper positioning of the guide wire from anteromedial band is caudal angle of 44º with entry point 20 mm from anterior tuberosity; for the posterolateral band the caudal angle is 36º; from the tibial tuberosity the distance is 31 mm. This technique is difficult to perform leaving its questionable reproducibility.
Received: December 14, 2011
Review: February 15, 2012
Accepted: March 12, 2012
Conflict of interest: none
Financial source: none
- 1. Garofalo R, Mouhsine E, Chambat P, Siegrist O. Anatomic anterior cruciate ligament reconstruction: the two-incision technique. Knee Surg Sports Traumatol Arthrosc. 2006;14(6):510-6.
- 2. Petersen W, Zantop T. Anatomy of the anterior cruciate ligament with regard to its two bundles. Clin Orthop Relat Res. 2007;454:35-47.
- 3. Stieven-Filho E, Garschangen ET, Namba M, Silva JLV, Malafaia O, Cunha LAM. Estudo anatômico das duas bandas do ligamento cruzado anterior com o joelho a 90° de flexão. Rev Col Bras Cir. 2011;38(4)0:338-42.
- 4. Acker JH, Drez D. Analysis of isometric placement of grafts in anterior cruciate ligament reconstruction procedures. Am J Knee Surg 1989;2:65-70.
- 5. Buoncristiani AM, Tjoumakaris FP, Starman JS, Ferretti M, Fu FH. Anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2006;22(9):1000-6.
- 6. Yasuda K, Kondo E, Ichiyama H, Tanabe Y, Tohyama H. Surgical and biomechanical concepts of anatomic anterior cruciate ligament reconstruction. Oper Tech Orthop. 2005;15(2):96-102.
- 7. Girgis FG, Marshall JL, Monajem A. The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Orthop Relat Res. 1975;(106):216-31.
- 8. Yasuda K, Kondo E, Ichiyama H, Kitamura N, Tanabe Y, Tohyama H, Minami A. Anatomic reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament using hamstring tendon grafts. Arthroscopy. 2004;20(10):1015-25.
- 9. Sonnery-Cottet B, Chambat P. Anatomic double bundle: a new concept in anterior cruciate ligament reconstruction using the quadriceps tendon. Arthroscopy. 2006;22(11):1249.e1-4.
- 10. Piasecki DP, Bach BR, Espinoza Orias AA, Verma NN. Anterior cruciate ligament reconstruction: can anatomic femoral placement be achieved with a transtibial technique? Am J Sports Med. 2011;39(6):1306-15.
- 11. Aquino JLB, Said MM, Maziero D, Pliveira JMP, Leando-Merhi VA. Reconstrução esofágica pela esofagocoloplastia no megaesôfago avançado em pacientes gastrectomizados. ABCD Arq Bras Cir Dig. 2009;22(4):197-200.
- 12. Park SJ, Jung YB, Jung HJ, Shin HK, Kim E, Song KS, Kim GS, Cheon HY, Kim S. Outcome of arthroscopic single-bundle versus double-bundle reconstruction of the anterior cruciate ligament: a preliminary 2-year prospective study. Arthroscopy. 2010;26(5):630-6.
- 13. Christel P, Franceschi J, Sbihi A, Colombet P, Djian P, Bellier G. Anatomic anterior cruciate ligament reconstruction: the French experience. Oper Tech Orthop. 2005;15(2):103-10.
- 14. Piasecki DP, Bach BR Jr, Espinoza Orias AA, Verma NN. Anterior cruciate ligament reconstruction: can anatomic femoral placement be achieved with a transtibial technique? Am J Sports Med. 2011;39(6):1306-15.
- 15. Siebold R, Ellert T, Metz S, Metz J. Tibial insertions of the anteromedial and posterolateral bundles of the anterior cruciate ligament: morphometry, arthroscopic landmarks, and orientation model for bone tunnel placement. Arthroscopy. 2008;24(2):154-61.
- 16. Siebold R. Observations on bone tunnel enlargement after double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2007;23(3):291-8.
Publication Dates
-
Publication in this collection
01 June 2012 -
Date of issue
May 2012
History
-
Received
14 Dec 2011 -
Accepted
12 Mar 2012 -
Reviewed
15 Feb 2012