Abstract
Introduction:
Motor vehicles have transformed human life in radical and contradictory ways. At the same time that cars have brought comfort and ease to human life, they are also a main cause of trauma, pain, disability, and death worldwide.
Objective:
To investigate the quality of life and self-esteem of traffic accident victims undergoing physical rehabilitation.
Methods:
This was a controlled, cross-sectional study that compared quality of life and self-esteem among traffic accident victims in physical therapy with other accident victims, physical therapy patients for other causes, and the general population.
Results:
The self-esteem of individuals undergoing physical therapy due to traffic accidents was lower compared to victims of other accidents and those in physical therapy for other reasons (p < 0.05). Regarding quality of life, the study group sample obtained the following mean scores: physical domain 48.1; psychological 52.8; social 68.1; environmental 54.1. These scores were lower than those of traffic accident victims who did not undergo physical therapy and of the general population in all domains (p < 0.05), but higher than that of individuals undergoing physical therapy for other causes, except in the psychological domain.
Conclusion:
Self-esteem and quality of life were low in traffic accident victims undergoing physical therapy. Physical therapy professionals can play an important role in improving these conditions provided they assume a humanized posture, practicing patient-centered rather than disease-centered health actions.
Keywords:
Traffic Accidents; Physical Therapy Specialty; Quality of Life; Self Esteem
Resumo
Introdução:
Os veículos a motor transformaram a vida humana de maneira radical e contraditória. Ao mesmo tempo que trouxeram conforto e facilidades, se tornaram um dos principais causadores de trauma, dor, incapacidades e mortes em escala mundial.
Objetivo:
Investigar a qualidade de vida e autoestima em acidentados de trânsito submetidos à reabilitação física.
Métodos:
Estudo transversal, controlado. Comparou-se a qualidade de vida e a autoestima de vítimas de acidentes de trânsito submetidos a reabilitação fisioterápica com outros acidentados, pacientes de fisioterapia por outras causas e população geral.
Resultados:
Foi significantemente mais baixa a autoestima entre os que faziam fisioterapia devido a acidentes de trânsito do que entre os outros acidentados e os que estavam em reabilitação por outros motivos (p < 0,05). A qualidade de vida do grupo de estudo obteve os seguintes escores médios: Domínio Físico 48,1; Psicológico 52,8; Social 68,1; Ambiental 54,1. Estes escores foram inferiores aos dos grupos de acidentados de trânsito que não fizeram fisioterapia e aos da população geral em todos os domínios (p < 0,05) e superior aos dos submetidos à fisioterapia por outros motivos, exceto no domínio psicológico.
Conclusão:
A autoestima e a qualidade de vida nos acidentados de trânsito submetidos à fisioterapia foram baixas. O profissional de fisioterapia pode ter importante papel na melhora destas condições na medida em que assuma uma postura humanizada, praticando ações de saúde voltadas ao paciente e não à doença.
Palavras-chave:
Acidentes de Trânsito; Fisioterapia; Qualidade de Vida; Autoestima
Introduction
Motor vehicles have transformed human life in radical and contradictory ways. At the same time that cars have brought comfort and ease to human life, they are also a main cause of trauma, pain, disability, and death worldwide. Traffic accidents are a serious social and health problem in most countries. According to World Health Organization estimates, traffic accidents account for 1.2 million fatalities every year, ranking as the second most common cause of death among young people aged 5 to 29 years, and third among people aged 30 to 44 years. Furthermore, it is estimated that every year, 50 million people are injured in traffic accidents 1World Health Organization; Association for Safe International Road Travel. Faces behind figures: voices of road traffic crash victims and their families. Genebra: OMS; 2007..
Traffic in Brazil is among the worst and most dangerous worldwide 2Departamento Nacional de Trânsito. Estatísticas gerais sobre trânsito. Brasília: DENATRAN; 1997.. The large number of vehicles in circulation, their poor organization, problems in supervision and administration, poor condition of vehicles and infrastructure, inappropriate behavior by drivers and impunity of offenders 3Marin L; Queiroz, MS. A atualidade dos acidentes de trânsito na era da velocidade: uma visão geral. Cad Saude Publica. 2000;16(1):7-21. are all factors associated with the poor quality of Brazilian traffic safety. Despite the efforts made to control and prevent accidents, including public policies focused on this public health problem, the situation remains serious in Brazil.
Injuries, trauma, and deaths resulting from traffic accidents generate high costs for society while the economic losses and mental and emotional damages to traffic victims and their families are incalculable 4Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Impacto da violência na saúde dos brasileiros. Brasília; 2005. Portuguese.,5Minayo, MCS. Violência: um problema para a saúde dos brasileiros. In: Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Impacto da violência na saúde dos brasileiros. Brasília; 2005. p. 9-42. Portuguese.. Traffic accidents affect people of all ages, and when they do not cause deaths, they often cause sequelae and disabilities 6Cavalcante, FG; Morita, PA; Rodrigues, S. Sequelas invisíveis dos acidentes de trânsito: o transtorno de estresse pós-traumático como problema de saúde pública. Cienc Saude Colet. 2009;14(5):1763-72., and interfere in their quality of life and performance of daily activities 3Marin L; Queiroz, MS. A atualidade dos acidentes de trânsito na era da velocidade: uma visão geral. Cad Saude Publica. 2000;16(1):7-21.,7Oliveira, NLB; Sousa, RMC. Diagnóstico de lesões e qualidade de vida de motociclistas, vítimas de acidentes de trânsito. Rev Lat Am Enfermagem. 2003;11(6):749-56..
The consequences of accidents to the health system include high demand for services and high costs related to emergency care, relief and rehabilitation, all of which are much more expensive than most conventional medical procedures 8Santos, JLG; Garlet, ER; Figueira, RB; Lima, SBS; Prochnow, AG. Acidentes e Violências: caracterização dos atendimentos no pronto-socorro de um hospital universitário. Saude Soc. 2008;17(3):211-8..
The physical and economic impacts of problems caused by traffic accidents have been thoroughly researched. Traffic accidents have high social importance, with consequences to the lives of those injured and those who live with the injured, and to collective society as a whole. However, some perspectives are less researched. Sequelae, which involve the psychic and social realms, are not apparent in the first moments following a traffic accident 9Thomas, CS. Psychological consequences of traumatic injury. Br J Psychiatry. 2002;180(5):392-3.; rather, they emerge during follow-up monitoring and observation of victims, being referred to as "invisible sequela of traffic accidents" 10Gonçalves, F; Morita, PA; Haddad, S. Sequelas invisíveis dos acidentes de trânsito: o transtorno de estresse pós-traumático como problema de saúde pública. Brasília: IPEA; 2007. Available from:http://tinyurl.com/h6fhk4k.
http://tinyurl.com/h6fhk4k...
, including those that affect quality of life and self-esteem. These sequelae can have a long-term negative effect on the daily lives of traffic accident victims and those around them.
According to the World Health Organization (WHO), quality of life is "individuals" perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns". This concept was constructed in 1990 through a multi-center project, which also originated the WHO Quality of Life - 100 (WHOQOL-100) and its shortened version the WHOQOL-bref 11The WHOQOL group. The World Health Organization quality of life assessment (WHOQOL): development and general psychometric properties. Soc Sci Med. 1998;46(12):1569-85.,12The WHOQOL group. The development of the World Health Organization quality of life assessment instrument (WHOQOL). In: Orley, J; Kuyken, W. Quality of life assessment: international perspectives. Heidelberg (Germany): Springer Verlag; 1994. p. 41-60.. Measuring quality of life is a way to evaluate a patient's perceptions about various aspects of their life, and not merely their state of health.
The concept of self-esteem developed by Rosenberg defines it as an assessment that an individual performs and maintains, expressing attitudes of approval or disapproval 13Rosemberg, M. Society and the adolescent self-image. Princeton (NJ): Princeton University Press; 1965., including beliefs, opinions, attitudes, values and feelings about themselves. High self-esteem does not imply that an individual feels superior to others; rather, that they believe themselves to be important and worthy of respect. High self-esteem is not incompatible with recognition of one's own limitations 13Rosemberg, M. Society and the adolescent self-image. Princeton (NJ): Princeton University Press; 1965..
In Brazil, quality of life and self-esteem have been studied especially regarding worsening chronic health conditions and analysis of therapeutic interventions 14Bampi ,LNS; Guilhem, D; Lima, DD Qualidade de vida em pessoas com lesão medular traumática: um estudo com o WHOQOL-bref. Rev Bras Epidemiol. 2008;11(1):67-77.,15Fleck, MPA; Lima, AFBS; Louzada, S; Schestasky, G; Henriques, A; Borges, VR; et al Associação entre sintomas depressivos e funcionamento social em cuidados primários de saúde. Rev Saude Publica. 2002;36(4):431-8.,16Lima, AFBS. Qualidade de vida em pacientes do sexo masculino dependentes de álcool {master´s thesis}. Porto Alegre (Brazil): Universidade Federal do Rio Grande do Sul; 2001. Portuguese.. Injuries caused by trauma, due to their severity and often irreversibility, require long-term rehabilitation actions, which can lead healing or at least assist in adapting to a new life. Sequelae and other difficulties that people experience in these situations are reflected in quality of life and self-esteem 14Bampi ,LNS; Guilhem, D; Lima, DD Qualidade de vida em pessoas com lesão medular traumática: um estudo com o WHOQOL-bref. Rev Bras Epidemiol. 2008;11(1):67-77.,17Lianza, S; Casalis, MEP; Greve, JMDA; Eichberg, R. A lesão medular. In: Lianza S (Org.). Medicina de Reabilitação. 3rd ed. Rio de Janeiro: Sociedade Brasileira de Medicina Física e de Reabilitação; 2001. p. 299-322. Portuguese., and on their recovery and rehabilitation, and return to everyday activities and work 18Sousa, RMC; Koizumi, MS. As vítimas de traumatismo crânio-encefálico seis meses após o trauma. Acta Paul Enferm. 1998;11(1):63-78.,19Muñoz-Céspedes, JM; Paúl-Lepedriza, N; Pelegrín-Valero, C; Tirapu-Ustarroz, J. Factores de pronóstico en los traumatismos craneoencefálicos. Rev Neurol. 2001;32(4):351-64.,20Oliveira, NLB; Sousa, RMC. Retorno à atividade produtiva de motociclistas vítimas de acidentes de trânsito. Acta Paul Enferm. 2006;19(3):284-9.. An active life contributes to economic and psychological balance, and is instrumental in the rehabilitation process, both as a source of personal satisfaction and self-esteem, as well in the restructuring of social relationships 20Oliveira, NLB; Sousa, RMC. Retorno à atividade produtiva de motociclistas vítimas de acidentes de trânsito. Acta Paul Enferm. 2006;19(3):284-9..
This study aimed to investigate quality of life and self-esteem in traffic accident victims undergoing physical therapy.
Methods
- Design
This was a controlled, cross-sectional study.
- Study scenario
The study was developed in the municipality of Pouso Alegre, in the southeast central Brazilian state of Minas Gerais, at the University Hospital (UH) and the municipal, public physical therapy service (PPS).
- Study sample
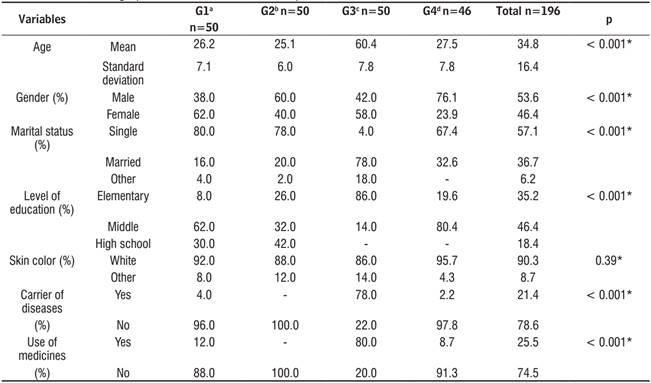
The study used non-probability sampling. The sample consisted of 196 subjects, divided into three groups (G1, G2 and G3) of 50 individuals and one of 46 (G4): the first group (G1) comprised individuals who were not traffic accident victims, and not undergoing physical therapy; the second group (G2) consisted of traffic accident victims who did not need physical therapy; the third group (G3) comprised subjects undergoing physical therapy for various reasons, excluding traffic accidents; the fourth study group (G4) consisted of patients in physical therapy due to injuries caused by traffic accidents. The number of people in the latter was smaller than the others because no other eligible subjects were found.
The study subjects of groups G3 and G4 were invited to participate based on their attendance at the UH and municipal physical therapy services. Groups G1 and G2 were located using medical records from the UH emergency room.
- Eligibility criteria
The eligibility criteria for the study group (G4) were: be a traffic accident victim, with preserved cognition, 18 years of age or older, and undergoing physical therapy; eligibility criteria for G3 included undergoing physical therapy due to causes not included in chapter XX of the ICD-10: external causes of morbidity and mortality and in the G4; the participants of G2 were traffic accident victims that did not require physical therapy, and with no chronic diseases; and for G1, the participants were not traffic accident victims, with no chronic health conditions and were not undergoing physical therapy.
- Research procedures and instruments
After explaining the study goals and procedures, the researcher invited the subjects to participate. Potential participants read and signed an informed consent form, and then answered a closed questionnaire on sociodemographic characteristics and health, composed of closed questions on the following variables: gender; age; schooling; skin color; religion; socioeconomic status; origin; existence, topography and type of injury; external cause; the presence of chronic and/or acute diseases, and occurrence of health treatments.
The second questionnaire was the Rosenberg self-esteem scale, created in 1965 and widely-used. The Rosenberg scale evaluates an individual's personal satisfaction and their satisfaction regarding their personal qualities, capabilities, values, pride and self-respect, positive attitude, and feelings of uselessness and failure. The Rosenberg scale is a Likert-type, one-dimensional measure consisting of ten closed questions with four options: totally agree, agree, disagree and totally disagree, in which each response varies from 1 to 4 points. The higher the score, the higher the self-esteem. For the present study, the Rosenberg scale was cross-culturally adapted and validated for Brazilian Portuguese 21Avanci, JQ; Assis, SG; Santos, NC; Oliveira, RVC. Adaptação transcultural de escala de auto-estima para adolescentes. Psicol Reflex Crit. 2007;20(3):397-405.
The third instrument was the WHOQOL-Bref, which was also translated and validated for Brazilian Portuguese, with satisfactory levels of internal consistency, discriminant validity, criterion validity, concurrent validity and reliability 22Fleck, MPO instrumento de avaliação de qualidade de vida abreviado da Organização Mundial da Saude (WHOQOL-100): características e perspectivas. Cien Saude Colet. 2000;5(1):33-8.. With this instrument, the researchers sought to understand the subjective perceptions of individuals in their cultural, social and environmental context. The WHOQOL-Bref consists of 26 questions that define four domains: 1) physical (pain and discomfort; energy and fatigue; sleep and rest; activities of daily life; dependence on medication or treatments and work capacity); 2) psychological (positive feelings; thinking, learning, memory and concentration; self-esteem; body image and appearance; negative feelings; spirituality, religion and personal beliefs; 3) social relations (personal interactions; social support and care; sexual activity); and 4) environment (physical security and protection; the home environment; financial resources; health and social care: availability and quality; opportunity to acquire new information and skills; participation and opportunities for recreation/leisure; physical environment: pollution/noise/traffic/weather; and transportation).
The score obtained after verification of the WHOQOL-bref resulted in a score on a per-domain basis. The scales have a positive direction (the higher the score, the greater the quality of life). WHOQOL-bref scores range from 4 to 20, based on the use of conversion of raw values into values worked. These values were converted to values between zero and 100, to make it comparable to the WHOQOL-100.
- Database and statistical analysis
The data collected were consolidated in a spreadsheet using Microsoft Excel(r).
The statistical software SPSS(r) version 17, Epi-Info 6.04 and BioEstat 5.0 were used for data analysis, the latter two being publicly-owned. The quantitative variables were described by measures of central tendency (mean) and dispersion (standard deviation). Proportions were used for categorical variables.
The t-test was used to compare the means of the two parametric behavior variables. Analysis of variance (ANOVA) was used for k independent parametric variables. In the case of measures of central tendency of non-parametric variables, the Mann-Whitney or Kruskal-Wallis tests, respectively, were used. Adherence to normality was tested by the Kolmogorov-Smirnov proof. P ≤ 0.05 was considered significant.
- Ethical procedures
This study followed the precepts for research with human beings established by resolution nº 196/96 of 10/10/96, and was approved by the Research Ethics Committee of the Wenceslau Braz School of Nursing under protocol no. 333/2010.
Results
Table 1 shows that the mean age of the study participants was 34.8 years (standard deviation (SD = 16.4). Of the groups of participants undergoing physical therapy for non-traffic injuries, G3 was the oldest (mean age = 60.4 years, SD: 7.8 (p < 0.001). 53.6 percent of the study population consisted of men. The groups of traffic accident victims (in physical therapy or not - G4 and G2) had a higher proportion of men than the other groups (p < 0.001). Except for the group in physical therapy for other reasons (G3), most participants were single (p < 0.001). G3 had significantly less education than the other groups (p < 0.001), and a much larger proportion of people with diseases (p < 0.001) and using medicines (p < 0.001).
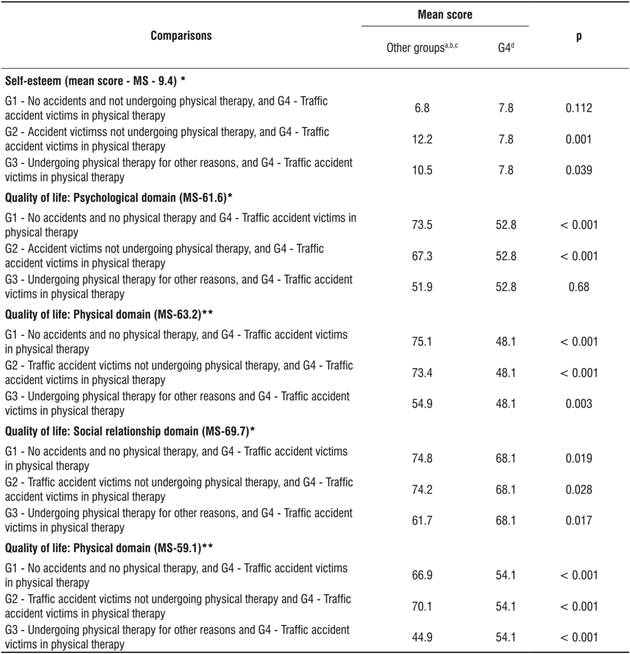
The mean score obtained for the self-esteem scale was 9.4. Table 2 shows that participants who were not traffic accident victims and not undergoing physical therapy (G1), and traffic accident victims undergoing physical therapy (G4) had the lowest levels of self-esteem. They did not present significant differences between their scores. However, the participants with accidents that did not require physical therapy (G2) as well as those in G3 showed significantly higher scores than the other two groups.
Quality of life obtained the following mean scores for the entire sample: Psychological 61.6; Physical 63.2; Social relations 69.7; Environment 59.1 (Table 2). The mean scores of G4 were always lower than the general values.
Evaluation of the psychological domain shows that the participants who suffered from accidents and in physical therapy (G4) had significantly lower mean scores than the individuals in G1, as well as those injured who were not in physical therapy (G2).
Similarly, in the physical domain, the G4 participants had significantly lower mean scores than the others.
The G4 participants obtained their best scores in the domain of social relations, but these were still lower than those of G1 and G2. Overall, the G3 participants had the lowest mean values. The differences between traffic accident victims undergoing physical therapy (G4) were significantly different from the other groups.
In the environment domain, the study group (G4) again had lower scores than all the others, except for G3 (patients in physical therapy for other reasons).
Discussion
This study presented some problems. The four groups initially presented a small number of participants (50 participants), a feature that could compromise the statistical power of the results. Another problem was that the group of patients in physical therapy for causes other than traffic accidents presented sociodemographic characteristics distinct from the others. Also, because it is an under-researched topic, no other studies with a similar approach were found in the literature, and, therefore, comparisons with the literature were done with other studies that did not have the same research goals.
The profile of groups composed of traffic victims was similar for both those undergoing physical therapy (G4) and those who were not (G2). The fact that they were predominantly young, single men with mid-level and higher education follows the pattern described in other studies on traffic accident victims 23Alves, ALA; Salim, FM; Martinez, EZ; Passos, ADC; De Carlo, MMRP; Scarpelini, S; et al. Qualidade de vida de vítimas de trauma seis meses após a alta hospitalar. Rev Saude Publica. 2009;43(1):154-60.,24Mesquita Filho, M; Jorge, MHPM. Características da morbidade por causas externas em serviço de urgência. Rev Bras Epidemiol. 2007;10(4):579-91.,25Gawryszewski, VP; Coelho, HMM; Scarpelini, S; Zan, R; Jorge, MHPM; Rodrigues, EMS. Perfil dos atendimentos a acidentes de transporte terrestre por serviços de emergência em São Paulo, 2005. Rev Saude Publica. 2009;43(2):275-82..
Characteristics of patients receiving physical therapy due to causes other than traffic accidents (G3) were not the same. They had a higher age group, lower education, were married, mostly sick and using medication. Different from accident victims, these were people whose health problems requiring physical therapy were caused predominantly by chronic illnesses that mostly affect the older segment of the population, with socio-demographic characteristics compatible with this age group 26Ferreira, PCS; Tavares, DMS; Martins, NPF; Rodrigue,s LR; Ferreira, LA. Características sociodemográficas e hábitos de vida de idosos com e sem indicativo de depressão. Rev Eletr Enf. 2013;15(1):197-204..
In the present study, the traffic accident victims in physical therapy (G4) and traffic accident victims that did not present injuries (G1) had the lowest self-esteem, with similar results. However, traffic accident victims that did not require physical therapy (G2) and those undergoing physical therapy for other reasons (G3) had significantly higher mean scores than the victims of G4. The studies discussing self-esteem and aging were not consensual 27Shaw, BA; Liang, J; Krause, N. Age and race differences in the trajectories of self-esteem. Psychol Aging. 2010;25(1):84-94.. Some studies point to invariability 28Collins, AL; Smyer, MA. The resilience of self-esteem in late adulthood. J Aging Health. 2005;17(4):471-89., while others indicate a drop 29Robins, RW; Trzesniewski, KH; Tracy, JL; Gosling, SD; Potter, J. Global self-esteem across the life span. Psychol Aging. 2002;17(3):423-34. and even increase 30Gove, WR; Ortega, ST; Style, CB. The maturational and role perspectives on aging and self through the adult years: An empirical evaluation.AJS.1989;94(5):1117-45. of this construct as age increases. Traffic accidents have negative impacts on life, including sequelae and disabilities that can lead to lower self-esteem, especially in more serious cases, such as those for which patients seek physical therapy (G4). The impact of a traumatic event is negatively reflected in the self-esteem of adults 31Simmen-Janevska, K; Brandstätter,V; Maercker, A. The overlooked relationship between motivational abilities and posttraumatic stress: a review. Eur J Psychotraumatol. 2012;3., which may justify the associations found.
In all areas of quality of life (psychological, physical, social relations and environment), the scores of traffic accident victims undergoing physical therapy (G4) were significantly lower than those of traffic accident victims not undergoing physical therapy (G2), as well as those of the group without injuries (G1), data reinforcing the observation that severity of trauma is predictive of damages to quality of life after the accident 32Magalhães, SHT; Loureiro, SR. Acidentes de trânsito e variáveis psicossociais - uma revisão da literatura. Medicina(Ribeirão Preto). 2007;40(3):345-51.. Furthermore, health situation and functional status are key factors in determining the quality of life 33Ritcher, J; Schawarz, M; Bauer, B. Personality characteristics determine health-related quality of life as an outcome indicator of geriatric inpatient rehabilitation. Curr Gerontol Geriatr Res. 2008:474618..
The psychological domain of quality of life had lower scores for those who had suffered traffic accident and were undergoing physical therapy (G4) than for the other traffic accident victims (G2) and the control group (G1). No significant differences were found between traffic accident victims receiving physical therapy (G4) and the group receiving it for other reasons (G3). This situation suggests that the events that led patients to physical therapy, due to decreased mobility and physical disability, influenced decreased psychological performance. In these cases, both the consequences of external causes, such as chronic diseases, impacted this domain, even with important differences between the ages of the two groups. One study by Alves et al. 23Alves, ALA; Salim, FM; Martinez, EZ; Passos, ADC; De Carlo, MMRP; Scarpelini, S; et al. Qualidade de vida de vítimas de trauma seis meses após a alta hospitalar. Rev Saude Publica. 2009;43(1):154-60. that evaluated quality of life of trauma victims treated in an emergency hospital unit six months after hospital discharge found low scores in all areas of the WHOQOL, notably the psychological, physical and social relations domains, data that is similar to the present study.
The lowest score for traffic accident victims undergoing physical therapy (G4) was in the physical domain, with significantly lower scores than the other categories. These results were lower than those found in victims of spinal cord injury, six months after the trauma, where there was influence of age, gender, length of stay and severity of trauma in the scores 14Bampi ,LNS; Guilhem, D; Lima, DD Qualidade de vida em pessoas com lesão medular traumática: um estudo com o WHOQOL-bref. Rev Bras Epidemiol. 2008;11(1):67-77. of the domain, which also diverged from the study by Alves that had lower scores 23Alves, ALA; Salim, FM; Martinez, EZ; Passos, ADC; De Carlo, MMRP; Scarpelini, S; et al. Qualidade de vida de vítimas de trauma seis meses após a alta hospitalar. Rev Saude Publica. 2009;43(1):154-60.. One fact that stood out was that the scores of the G4 were significantly lower than those of patients in physical therapy for non-traumatic causes (G3), composed of patients with chronic diseases and in old age, in constant use of medicines. This fact lead to the assumption that among the traffic victims in physical therapy, there was a greater presence of various facets of the physical domain, including pain, discomfort, low energy, fatigue, impaired sleep and rest than in the other groups, notably, in chronically-ill patients in physical therapy (G3).
Generally, the social relations domain had the highest scores for all groups. This fact may be related to the presence of family support in post-accident conditions including both traumatic and chronic diseases 23Alves, ALA; Salim, FM; Martinez, EZ; Passos, ADC; De Carlo, MMRP; Scarpelini, S; et al. Qualidade de vida de vítimas de trauma seis meses após a alta hospitalar. Rev Saude Publica. 2009;43(1):154-60.. The traffic accident victims in physical therapy (G4) had significantly lower scores than those who did not receive this intervention (G2), and greater than those in physical therapy for non-traumatic causes (G3). As stated above, the participants in the latter group had higher mean age, presence of disease, use of medicines and physical disabilities, all factors that influence social life.
The environment domain followed the results pattern of the previous domain. Accessibility and adaptation to the environment have not been guaranteed in the municipality of the study, similar to what was shown by Alves et al. 23Alves, ALA; Salim, FM; Martinez, EZ; Passos, ADC; De Carlo, MMRP; Scarpelini, S; et al. Qualidade de vida de vítimas de trauma seis meses após a alta hospitalar. Rev Saude Publica. 2009;43(1):154-60.. The average scores of this domain were higher than those obtained in studies on quality of life in patients with traumatic spinal cord injury 14Bampi ,LNS; Guilhem, D; Lima, DD Qualidade de vida em pessoas com lesão medular traumática: um estudo com o WHOQOL-bref. Rev Bras Epidemiol. 2008;11(1):67-77., which is justified by the fact that the mobility of this group was much more limited, and difficulties with the environment much more pronounced.
Conclusion
Self-esteem and quality of life were low among traffic accident victims in physical therapy. Many factors have an important role in this situation. Factors related to the care service, structure of the health system, type and severity of injury, sequelae and pain and access to physical therapy. In addition, the socioeconomic conditions of the victims and their social and family support following trauma are very important.
Physical therapy professionals can play a role in the improvement of self-esteem and quality of life of their patients in a number of domains. One alternative is to practice with a person-centered approach that is not focused solely on the disease, attending to an individual's search for humanized care that considers technical knowledge and can enhance the social and human dimensions of health needs 34Almeida, ALJ; Guimarães, RB. O lugar social do fisioterapeuta brasileiro. Fisioter Pesqui. 2009:16(1):82-8.. With a more supportive approach, the professional can interact with the patient on issues that influence their daily life and its quality. The production of knowledge and actions contextualized to the patient's life, helping them to perceive shared responsibility for maintenance of their health 34Almeida, ALJ; Guimarães, RB. O lugar social do fisioterapeuta brasileiro. Fisioter Pesqui. 2009:16(1):82-8., and solidarity and discussion of alternatives that can contribute to their well-being and adaptation, can be fundamental contributions by physiotherapists to the quality of life of users of their services.
This study brought numerous and relevant contributions to the knowledge of a situation that remains under-researched: self-esteem and quality of life of traffic accident victims in physical therapy. The data presented in the present study is very important in the development of activities and programs focused on this sector, in addition to the professional reorientation of those already working in the area. This study advanced research on a subject on which there is still much to learn, and it is hope that it will be a trigger for other future studies, ranging from new directions on approach to patients, proposals for comprehensive care, deeper understanding of the physical, mental and social domains of traffic accident victims, and actions directed towards their collective care.
References
- World Health Organization; Association for Safe International Road Travel. Faces behind figures: voices of road traffic crash victims and their families. Genebra: OMS; 2007.
- Departamento Nacional de Trânsito. Estatísticas gerais sobre trânsito. Brasília: DENATRAN; 1997.
- Marin L; Queiroz, MS. A atualidade dos acidentes de trânsito na era da velocidade: uma visão geral. Cad Saude Publica. 2000;16(1):7-21.
- Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Impacto da violência na saúde dos brasileiros. Brasília; 2005. Portuguese.
- Minayo, MCS. Violência: um problema para a saúde dos brasileiros. In: Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Impacto da violência na saúde dos brasileiros. Brasília; 2005. p. 9-42. Portuguese.
- Cavalcante, FG; Morita, PA; Rodrigues, S. Sequelas invisíveis dos acidentes de trânsito: o transtorno de estresse pós-traumático como problema de saúde pública. Cienc Saude Colet. 2009;14(5):1763-72.
- Oliveira, NLB; Sousa, RMC. Diagnóstico de lesões e qualidade de vida de motociclistas, vítimas de acidentes de trânsito. Rev Lat Am Enfermagem. 2003;11(6):749-56.
- Santos, JLG; Garlet, ER; Figueira, RB; Lima, SBS; Prochnow, AG. Acidentes e Violências: caracterização dos atendimentos no pronto-socorro de um hospital universitário. Saude Soc. 2008;17(3):211-8.
- Thomas, CS. Psychological consequences of traumatic injury. Br J Psychiatry. 2002;180(5):392-3.
- Gonçalves, F; Morita, PA; Haddad, S. Sequelas invisíveis dos acidentes de trânsito: o transtorno de estresse pós-traumático como problema de saúde pública. Brasília: IPEA; 2007. Available from:http://tinyurl.com/h6fhk4k
» http://tinyurl.com/h6fhk4k - The WHOQOL group. The World Health Organization quality of life assessment (WHOQOL): development and general psychometric properties. Soc Sci Med. 1998;46(12):1569-85.
- The WHOQOL group. The development of the World Health Organization quality of life assessment instrument (WHOQOL). In: Orley, J; Kuyken, W. Quality of life assessment: international perspectives. Heidelberg (Germany): Springer Verlag; 1994. p. 41-60.
- Rosemberg, M. Society and the adolescent self-image. Princeton (NJ): Princeton University Press; 1965.
- Bampi ,LNS; Guilhem, D; Lima, DD Qualidade de vida em pessoas com lesão medular traumática: um estudo com o WHOQOL-bref. Rev Bras Epidemiol. 2008;11(1):67-77.
- Fleck, MPA; Lima, AFBS; Louzada, S; Schestasky, G; Henriques, A; Borges, VR; et al Associação entre sintomas depressivos e funcionamento social em cuidados primários de saúde. Rev Saude Publica. 2002;36(4):431-8.
- Lima, AFBS. Qualidade de vida em pacientes do sexo masculino dependentes de álcool {master´s thesis}. Porto Alegre (Brazil): Universidade Federal do Rio Grande do Sul; 2001. Portuguese.
- Lianza, S; Casalis, MEP; Greve, JMDA; Eichberg, R. A lesão medular. In: Lianza S (Org.). Medicina de Reabilitação. 3rd ed. Rio de Janeiro: Sociedade Brasileira de Medicina Física e de Reabilitação; 2001. p. 299-322. Portuguese.
- Sousa, RMC; Koizumi, MS. As vítimas de traumatismo crânio-encefálico seis meses após o trauma. Acta Paul Enferm. 1998;11(1):63-78.
- Muñoz-Céspedes, JM; Paúl-Lepedriza, N; Pelegrín-Valero, C; Tirapu-Ustarroz, J. Factores de pronóstico en los traumatismos craneoencefálicos. Rev Neurol. 2001;32(4):351-64.
- Oliveira, NLB; Sousa, RMC. Retorno à atividade produtiva de motociclistas vítimas de acidentes de trânsito. Acta Paul Enferm. 2006;19(3):284-9.
- Avanci, JQ; Assis, SG; Santos, NC; Oliveira, RVC. Adaptação transcultural de escala de auto-estima para adolescentes. Psicol Reflex Crit. 2007;20(3):397-405
- Fleck, MPO instrumento de avaliação de qualidade de vida abreviado da Organização Mundial da Saude (WHOQOL-100): características e perspectivas. Cien Saude Colet. 2000;5(1):33-8.
- Alves, ALA; Salim, FM; Martinez, EZ; Passos, ADC; De Carlo, MMRP; Scarpelini, S; et al. Qualidade de vida de vítimas de trauma seis meses após a alta hospitalar. Rev Saude Publica. 2009;43(1):154-60.
- Mesquita Filho, M; Jorge, MHPM. Características da morbidade por causas externas em serviço de urgência. Rev Bras Epidemiol. 2007;10(4):579-91.
- Gawryszewski, VP; Coelho, HMM; Scarpelini, S; Zan, R; Jorge, MHPM; Rodrigues, EMS. Perfil dos atendimentos a acidentes de transporte terrestre por serviços de emergência em São Paulo, 2005. Rev Saude Publica. 2009;43(2):275-82.
- Ferreira, PCS; Tavares, DMS; Martins, NPF; Rodrigue,s LR; Ferreira, LA. Características sociodemográficas e hábitos de vida de idosos com e sem indicativo de depressão. Rev Eletr Enf. 2013;15(1):197-204.
- Shaw, BA; Liang, J; Krause, N. Age and race differences in the trajectories of self-esteem. Psychol Aging. 2010;25(1):84-94.
- Collins, AL; Smyer, MA. The resilience of self-esteem in late adulthood. J Aging Health. 2005;17(4):471-89.
- Robins, RW; Trzesniewski, KH; Tracy, JL; Gosling, SD; Potter, J. Global self-esteem across the life span. Psychol Aging. 2002;17(3):423-34.
- Gove, WR; Ortega, ST; Style, CB. The maturational and role perspectives on aging and self through the adult years: An empirical evaluation.AJS.1989;94(5):1117-45.
- Simmen-Janevska, K; Brandstätter,V; Maercker, A. The overlooked relationship between motivational abilities and posttraumatic stress: a review. Eur J Psychotraumatol. 2012;3.
- Magalhães, SHT; Loureiro, SR. Acidentes de trânsito e variáveis psicossociais - uma revisão da literatura. Medicina(Ribeirão Preto). 2007;40(3):345-51.
- Ritcher, J; Schawarz, M; Bauer, B. Personality characteristics determine health-related quality of life as an outcome indicator of geriatric inpatient rehabilitation. Curr Gerontol Geriatr Res. 2008:474618.
- Almeida, ALJ; Guimarães, RB. O lugar social do fisioterapeuta brasileiro. Fisioter Pesqui. 2009:16(1):82-8.
Publication Dates
-
Publication in this collection
Oct-Dec 2016
History
-
Received
12 May 2014 -
Accepted
09 Nov 2015