Abstracts
The aim of this study was to assess the influence of different light-emitting diodes (LED) light-curing devices for bonding orthodontic brackets, using the shear bond strength and analysis of adhesive remnant index (ARI). Crowns from 60 bovine incisors received brackets bonded with Transbond XT. Specimens were divided into 4 groups (n=15) according to the light-curing procedures: HL = control, halogen light; OR = Ortholux LED; UL = Ultraled XP, and RD = Radii LED. All light-curing procedures were performed for 40 s. Shear bond strength test was evaluated using an universal testing machine at a crosshead speed of 0.5 mm/min. Data were analyzed statistically by ANOVA and Tukey's test. The ARI scores were evaluated with a stereoscopic magnifying glass and analyzed statistically by Kruskal-Wallis test. A significance level of 5% was set for all analyses. Shear bond strength means in MPa and standard deviations were 9.82 (3.28), 12.70 (3.35), 9.04 (2.80) and 11.22 (2.36) for HL, OR, UL and RD, respectively. OR presented the highest shear bond strength mean value. HL differed significantly (p<0.05) from Groups OR and RD. However, these groups did not differ significantly from each other (p>0.05). Regarding the ARI scores, no statistically significant difference was observed (p>0.05) among the groups. In conclusion, Ortholux LED and Radii LED units provided the highest values of bracket adhesive strength.
shear strength; orthodontic brackets; visible light
O objetivo deste estudo foi avaliar a influência de diferentes aparelhos de luz tipo LED na colagem de bráquetes ortodônticos, através do teste de resistência ao cisalhamento e do Índice de Remanescente do Adesivo (IRA). Coroas de 60 incisivos bovinos receberam a colagem de bráquetes com compósito Transbond XT. A amostra foi dividida em 4 grupos (n=15) de acordo com os seguintes tipos de fotoativação: HL: controle, luz halógena; OR= Ortholux LED; UL= Ultraled XP e RD= Radii LED. Todas as fotoativações foram realizadas por 40 s. O teste de resistência ao cisalhamento foi realizado em máquina universal de ensaios mecânicos à velocidade de 0,5 mm/min. Os dados foram analisados estatisticamente pelo ANOVA e teste de Tukey. Os escores do IRA foram avaliados em lupa estereoscópica e analisados estatisticamente pelo teste de Kruskal-Wallis. O nível de significância de 5% foi adotado para todas as análises. Os valores médios (MPa) e o desvio-padrão do teste de resistência ao cisalhamento foram 9,82 (3,28), 12,70 (3,35), 9,04 (2,80) e 11,22 (2,36) para o grupo HL, OR, UL e RD, respectivamente. O grupo OR apresentou os maiores valores médios de resistência ao cisalhamento. O grupo HL diferiu significativamente (p<0,05) dos grupos OR e RD. Entretanto, este dois grupos não diferiram estatisticamente entre si (p>0,05). Quanto ao escores do IRA, nenhuma diferença estatística significante foi observada (p>0,05) entre os grupos. Concluiu-se que as unidades de luz Ortholux LED e Radii LED proporcionaram maiores valores de resistência adesiva aos bráquetes.
Evaluation of different LED light-curing devices for bonding metallic orthodontic brackets
Corina Maia de Souza PintoI; José Tarcísio Lima FerreiraII; Mírian Aiko Nakane MatsumotoII; Maria Cristina BorsattoII; Raquel Assed Bezerra da SilvaII; Fábio Lourenço RomanoII
IUnifal - Federal University of Alfenas, Alfenas, MG, Brazil
IIDepartment of Pediatric Clinic, Preventive and Community Dentistry, Ribeirão Preto Dental School, USP - University of São Paulo, Ribeirão Preto, SP, Brazil
Correspondence Correspondence: Prof. Dr. Fábio Lourenço Romano, Departamento de Clínica Infantil, Odontologia Preventiva e Social, Faculdade de Odontologia de Ribeirão Preto, USP, Avenida do Café, S/N, Monte Alegre, 14040-904 Ribeirão Preto, SP, Brasil. Tel: +55-16-3602-4146. Fax: +55-16-3602-4102. e-mail: fabioromano@forp.usp.br
ABSTRACT
The aim of this study was to assess the influence of different light-emitting diodes (LED) light-curing devices for bonding orthodontic brackets, using the shear bond strength and analysis of adhesive remnant index (ARI). Crowns from 60 bovine incisors received brackets bonded with Transbond XT. Specimens were divided into 4 groups (n=15) according to the light-curing procedures: HL = control, halogen light; OR = Ortholux LED; UL = Ultraled XP, and RD = Radii LED. All light-curing procedures were performed for 40 s. Shear bond strength test was evaluated using an universal testing machine at a crosshead speed of 0.5 mm/min. Data were analyzed statistically by ANOVA and Tukey's test. The ARI scores were evaluated with a stereoscopic magnifying glass and analyzed statistically by Kruskal-Wallis test. A significance level of 5% was set for all analyses. Shear bond strength means in MPa and standard deviations were 9.82 (3.28), 12.70 (3.35), 9.04 (2.80) and 11.22 (2.36) for HL, OR, UL and RD, respectively. OR presented the highest shear bond strength mean value. HL differed significantly (p<0.05) from Groups OR and RD. However, these groups did not differ significantly from each other (p>0.05). Regarding the ARI scores, no statistically significant difference was observed (p>0.05) among the groups. In conclusion, Ortholux LED and Radii LED units provided the highest values of bracket adhesive strength.
KeyWords: shear strength, orthodontic brackets, visible light
RESUMO
O objetivo deste estudo foi avaliar a influência de diferentes aparelhos de luz tipo LED na colagem de bráquetes ortodônticos, através do teste de resistência ao cisalhamento e do Índice de Remanescente do Adesivo (IRA). Coroas de 60 incisivos bovinos receberam a colagem de bráquetes com compósito Transbond XT. A amostra foi dividida em 4 grupos (n=15) de acordo com os seguintes tipos de fotoativação: HL: controle, luz halógena; OR= Ortholux LED; UL= Ultraled XP e RD= Radii LED. Todas as fotoativações foram realizadas por 40 s. O teste de resistência ao cisalhamento foi realizado em máquina universal de ensaios mecânicos à velocidade de 0,5 mm/min. Os dados foram analisados estatisticamente pelo ANOVA e teste de Tukey. Os escores do IRA foram avaliados em lupa estereoscópica e analisados estatisticamente pelo teste de Kruskal-Wallis. O nível de significância de 5% foi adotado para todas as análises. Os valores médios (MPa) e o desvio-padrão do teste de resistência ao cisalhamento foram 9,82 (3,28), 12,70 (3,35), 9,04 (2,80) e 11,22 (2,36) para o grupo HL, OR, UL e RD, respectivamente. O grupo OR apresentou os maiores valores médios de resistência ao cisalhamento. O grupo HL diferiu significativamente (p<0,05) dos grupos OR e RD. Entretanto, este dois grupos não diferiram estatisticamente entre si (p>0,05). Quanto ao escores do IRA, nenhuma diferença estatística significante foi observada (p>0,05) entre os grupos. Concluiu-se que as unidades de luz Ortholux LED e Radii LED proporcionaram maiores valores de resistência adesiva aos bráquetes.
INTRODUCTION
Bonding of orthodontic brackets started being employed in Orthodontics in the 1960's by using the enamel acid etching technique (1,2). At that time, only auto-polymerizing materials were available. With the introduction of light-activated adhesive systems, orthodontists could have sufficient time to position the bracket on enamel surface and remove the excess material. This evolution has allowed the emergence of several other bonding methods using different composites and light-curing devices.
Regarding light-curing devices, quartz-tungsten halogen (QTH) lamps have been long predominated in the market (3,4). However, other light sources were introduced aiming to improve light curing and clinical work. Halogen light-curing units have been used in Orthodontics for many years and their important characteristics, such as the wide-spectrum action, allow any resin material to be light-cured in different shapes, thus making bracket debonding and damage more difficult. Also, halogen light-curing units are easy to use and have a low-cost maintenance, being widely employed as controls in several scientific studies (4). Devices using xenon plasma arc, argon laser, and light-emitting diodes (LED) have been developed (5), all differing from each other in terms of energy source, wavelength variation, and light intensity (3,6-8).
Mills (7) was the first to suggest the use of LED in Orthodontics. After Mills' work, more potent devices have emerged in order to increase efficacy of photo-activation and decrease polymerization time, thus fulfilling professional requirements, reducing chair time, and providing more comfort to patient (3,8-10). LED-based light sources have advantages, such as small size, less weight, ergonomy, reduced heat and noise generation, longer life source of radiation, low power consumption (use of rechargeable batteries), and light emission spectrum with total camphorquinone absorption (3,4,8-12). Despite these interesting and innovative characteristics, it is important to know if this type of light can keep the mechanical properties of the restorative materials and photo-activate adhesive materials used for the boding of orthodontic brackets. In addition, the use of LED-based light sources in clinical applications needs further scientific grounds.
The aim of this study was to assess the influence of different light-emitting diodes (LED) light-curing devices for bonding orthodontic brackets, using the shear bond strength and analysis of adhesive remnant index (ARI).
MATERIAL AND METHODS
Sixty healthy bovine permanent lower incisors were used for study. After extraction, the teeth were cleaned, stored in a plastic container with distilled water, and stored at 4ºC. All procedures regarding specimen preparation were performed according to the TR 11405 protocol specification established by the International Organisation for Standardisation (ISO) (13).
After removal from storage, the teeth were centrally inserted into PVC tubes (dimensions: 27 x 22 x 0.15, Amanco, Joinville, SC, Brazil) containing chemically activated acrylic resin (Jet Clássico, São Paulo, SP, Brazil), with their buccal faces perpendicular to the tube base (Fig. 1). The buccal faces of the teeth were subjected to prophylaxis with fluoride-free extra-fine pumice stone and water slurry on rubber cups for 10 s, then washed and dried for the time. Next, the enamel surfaces were etched with 37% phosphoric acid (Dentsply Ind. e Com. Ltda., Petrópolis, RJ, Brazil) for 30 s, washed and dried for approximately 20 s.
Sixty metallic brackets (Victory Series, MBT system; 3M Unitek, Monrovia, CA, USA) for lower central incisor (reference 017-982) were bonded to the teeth using Transbond XT composite (3M Unitek) according to the manufacturer's recommendations (Fig. 1). All bonding procedures were performed by the same operator, who used a pair of pliers (Ortoply, Philadelphia, PA, USA), and the excess material was removed with a sharp explorer (Duflex, Juiz de Fora, MG, Brazil). Specimens were divided into 4 groups of 15 teeth/brackets, according to the light-curing unit used: HL (Control) = halogen light-curing unit (XL 2500; 3M ESPE, St. Paul, MN, USA); OR = Ortholux LED (3M Unitek; Unitek); UL - Ultra LED XP (Dabi Atlante, Ribeirão Preto, SP, Brazil), and RD - Radii LED (SDI, Victoria, Australia). Each bracket bonding was photo-activated with a distance of 1 mm between bracket base and light-curing device for 40 s, that is, 10 s for each side of the bracket. Light intensity of each device was measured prior to each photo-activation cycle using a curing radiometer (Demetron, Danbury, CT, USA) (Table 1). After photo-activation, the specimens were stored in distilled water at 37ºC for 24 h.
All specimens were submitted to shear bond strength test in auniversal testing machine (model 4411; Instron, Norwood, MA, USA) at crosshead speed of 0.5 mm/min, with the active chisel tip put on the upper part of the bracket base (Fig. 1). The results were obtained in kgf (Kilogram-force), converted into N (Newton), and divided by the bracket base area (10.58 mm2), thus rendering bond strength values in MPa.
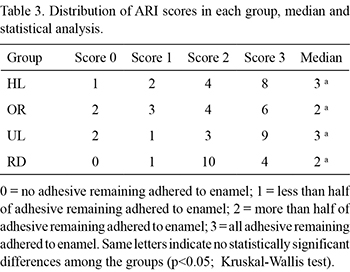
After debonding, the ARI from each specimen was evaluated by using a stereoscopic magnifying glass (Carl Zeiss, Goettingen, Germany) at ×10 magnification. The amount of resin material adhered to enamel after bracket removal was classified according to ARI scores established by Artun and Bergland (14): 0 = no adhesive remaining adhered to enamel; 1 = less than half of adhesive remaining adhered to enamel; 2 = more than half of adhesive remaining adhered to enamel; 3 = all adhesive remaining adhered to enamel.
The data on shear bond strength were submitted to ANOVA and Tukey's test , whereas the ARI score data were assessed by the Kruskal-Wallis test. A significance level of 5% was set for all analyses.
RESULTS
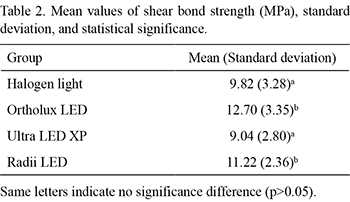
Shear bond strength data (in MPa), standard deviation, and statistical analysis are presented in Table 2. Group OR presented the highest shear bond strength of all groups. There was statistically significant difference (p<0.05) between group HL and groups OR and RD, which in turn did not differ significantly from each other (p>0.05). There was no statistically significant difference (p>0.05) between groups HL and UL.
ARI data, median and statistical analysis are presented in Table 3. No statistically significant difference (p>0.05) was found in the ARI scores among the four groups (Table 3).
DISCUSSION
Studies using shear bond strength tests are frequently difficult to be compared because of several variables such as type of light sources, exposure time, adhesive system used, enamel characteristics, and different methodological approaches. In order to minimize the influence of these variables in the present study, the control group received the same procedures applied to the experimental groups according to the most acceptable methodologies used in the literature (ISO TR 11405) (13).
Previous studies (4,5-10,12,15-18) have demonstrated that LED devices display equal or even superior performance compared to halogen light devices for 40-s photo-activation time. In this study, groups OR and RD showed higher shear bond strengths than groups HL and UL, although this latter group had a mean value similar to that of the former (Table 2).
On the other hand, Üsümez et al. (17) found significantly lower values for LED devices compared to halogen light units for photo-activation time of 10 s. Silta et al. (19) found significant differences compared to halogen and LED units at different of polymerization times (20 s, 10 s and 6 s); the shorter the curing time, lower the shear bond strength. Marquezan et al. (20) found no significant differences in the bond strengths when using the new Whitening Lase Ortho curing light for 40 s for a half arch compared to conventional halogen and LED curing lights used for 20 s per tooth. The results obtained by these authors differ from those of the present study, possibly due to the longer exposure time (40 s).
In the present study, the light intensity of all curing devices was measured using a radiometer (Table 1). The irradiance of Ultra LED XP unit (150 mW/cm2) was found to be lower than that produced by other devices (Table 1) and lower than that recommended in other studies (300 mW/cm2) for achieving an adequate polymerization (21). Power variation among the light-curing devices can justify the differences in shear bond strength values. However, the shear bond strength means obtained from all light sources overcame the values proposed by Reynolds (22) (5.9 to 7.8 MPa), suggesting that it is not necessary to use high power for curing adequately the composite underneath the bracket. Additionally, low irradiation intensity has the advantage of producing less heat on the tooth surface, thus decreasing the risks to pulp (8). Interestingly, it should be emphasized that the irradiance values provided by the manufacturers do not correspond to those measured with a curing radiometer (Table 1).
After debonding, the enamel surfaces to which the bracket was attached were divided according to ARI scores established by Artun and Bergand (14). Those scores quantify the remaining material on enamel as assess the area where fracture occurred during the shear bond strength test. In the same way as reported by Silta et al. (19), no significant differences were found among the groups. The highest median values found were in groups HL (control) and UL (Table 3).
The majority of fractures observed after bracket debonding occurred at the bracket-composite interface, predominantly ARI score 3 (all adhesive remaining on enamel). In group RD, ARI score 2 was the most frequently observed (more than half of the adhesive remaining on enamel). ARI score 0 was not observed in none of the specimens from group RD. ARI classification indicated that, regardless of the type of light-curing device, most of the material remained adhered to tooth after the bracket debonding. This type of failure suggests that the weakest link in the adhesive chain was between bracket base and composite, thus not affecting the dental surface at all. These results are also corroborated by previous studies (12,17), as no significant differences in ARI scores were observed between halogen light and LED units.
In conclusion, the highest values of shear bond strength were obtained with Ortholux and Radii LED units. The light sources tested in the present study (halogen and LED) were effective for photo-activation during bracket bonding. Most fractures observed after bracket debonding occurred at the bracket-composite interface, with adhesive remaining adhered to enamel.
Further research is needed to evaluate these and other LED devices before their use in Orthodontics and other dental specialities can be indicated in reliable manner.
Accepted April 4, 2011
- 1. Buonocore M. A simple method of increasing the adhesion of acrylic filing materials to enamel surfaces. J Dent Res 1955;34:849-853.
- 2. Newman GV. Bonding plastic orthodontic attachments to tooth enamel. J New Jersey Dent Soc 1964;35:346-358.
- 3. Mills RW, Jandt KD, Ashworth SH. Dental composite depth of cure with halogen and blue light emitting diode technology. Br Dent J 1999;186:388-391.
- 4. Stansbury JW. Curing dental resins and composite by polymerization. J Esthet Dent 2000;12:300-308.
- 5. Martinelli J, Pires-de-Souza FCP, Casemiro LA, Tirapelli C, Panzeri H. Abrasion resistance of composites polymerized by light-emitting diodes (LED) and halogen light-curing units. Braz Dent J 2006;17:29-33.
- 6. Correr AB, Sinhoreti MAC, Sobrinho LC, Tango RN, Schneider LFJ, Consani S. Effect of the increase of energy density on Knoop hardness of dental composites light-cured by conventional QTH, LED and xenon plasma arc. Braz Dent J 2005;16:218-224.
- 7. Mills RW. Blue light emitting diodes-another method of light curing? Br Dent J 1995;178:169.
- 8. Price RB, Felix CA, Andreou P. Evaluation of a second-generation LED curing light. J Can Dent Assoc 2003;69:666.
- 9. Kurachi C, Tuboy AM, Magalhães DV, Bagnato VS. Hardness evaluation of dental composite polymerized with experimental LED-based devices. Dent Mater 2001;17:309-315.
- 10. Layman W, Koyama T. A Clinical comparison of LED and halogen curing units. J Clin Orthod 2004;38:385-387.
- 11. Christensen GJ. The curing light dilemma. J Am Dent Assoc 2002;133:761-763.
- 12. Dunn WJ, Taloumis LJ. Polymerization of orthodontic resin cement with light-emitting diode curing units. Am J Orthod Dentofacial Orthop 2002;122:236-241.
- 13. Internationatal Organization for Standardization. Guidance on testing of adhesion to tooth structure. ISO/TC106/SC 1 N236, Resolution 61. - CD TR 11405, Trieste, October 1994.
- 14. Artun J, Bergland S. Clinical trials with crystal growth conditioning as an alternative to acid-etch enamel pretreatment. Am J Orthod 1984;85:333-340.
- 15. Teshima W, Nomura Y, Tanaka N, Urabe H, Okazaki M, Nahara Y. ESR study of camphoroquinone/amine photoiniciator systems using blue light-emitting diodes. Biomaterials 2003;24:2097-2103.
- 16. Tsai PC, Meyers IA, Walsh LJ. Depth of cure and surface microhardness of composite resin cured with blue LED curing lights. Dent Mater 2004;20:364-369.
- 17. Maruo IT, Godoy-Bezerra J, Saga AY, Tanaka OM, Maruo H, Camargo ES. Effect of etching and light-curing time on the shear bond strength of a resin-modified glass ionomer cement. Braz Dent J 2010;21:533-537.
- 18. Rêgo EB, Romano FL. Shear bond strength of metallic brackets photo-activated with light-emitting diode (LED) at different exposure times. J Appl Oral Sci 2007;15:412-415.
- 19. Silta YT, Dunn WJ, Peters CB. Effect of shorter polymerization times when using the latest generation of light-emitting diodes. Am J Orthod Dentofacial Orthop 2005;128:744-748.
- 20. Marquezan M, Lau T, Rodrigues C, Sant'Anna E, Ruellas A, Marquezan M, et al.. Shear bond strengths of orthodontic brackets with a new LED cluster curing light. J Orthod 2010;37:37-42.
- 21. Barghi N, Berry T, Hatton C. Evaluating intensity ouput of curing lights in private dental offices. J Am Dent Assoc 1994;125:992-996.
- 22. Reynolds IR. A review of direct orthodontic bonding. Br J Orthod 1975;2:171-178.
Correspondence:
Publication Dates
-
Publication in this collection
10 June 2011 -
Date of issue
2011