Abstract
The aim of the study was to evaluate canal preparation in primary molars with hand files, ProTaper Next and Self-Adjusting File (SAF) by 2D and 3D micro-computed tomography (micro-CT) analysis. Canals of 24 primary molars were prepared with hand files (HF), ProTaper Next (PTN) and SAF (n=8/group). The teeth were scanned before and after root canal preparation and the pre- and postoperative micro-CT images were reconstructed. Changes in 2D (area, perimeter, roundness, minor and major diameter) and 3D [volume, surface area, structure model index (SMI)] morphological parameters, as well as canal transportation and lateral perforations were evaluated (Kruskal-Wallis and ANOVA; a=0.05). SAF presented smaller changes in minor diameter, volume and surface area compared with HF and PTN (p<0.05). PTN presented more circular canals after preparation. 3D analysis revealed greater transportation in HF. PTN and SAF presented more centered canal preparation, especially in curved areas. SAF and HF presented, respectively, the lowest (0.05±0.02 and 0.07±0.04) and highest (0.14±0.11 and 0.29±0.17) apical transportation. There were fewer lateral perforations in SAF (4.2%) and PTN (7.7%) than in HF (47.8%) (p<0.05). In primary molars, mechanical preparation showed better shaping ability than hand files, promoting more centered preparations and lower occurrence of lateral perforations and canal transportation. Clinical Relevance: Manual instrumentation is still reported as the main choice in the primary teeth preparation; however, studies have shown limitations in its use. The morphological characteristics of primary teeth and the limited knowledge of shaping procedures in these teeth using mechanical preparation become a challenge for clinical practice and might impair the predictability of endodontic treatment.
Key Words:
primary teeth; root canal preparation; micro-computed tomography; self-adjusting file; rotary system.
Resumo
Este estudo avaliou o preparo do canal radicular em molares decíduos com sistema manual e mecanizado [ProTaper Next e Self-Adjusting File (SAF)], por meio de parâmetros morfológicos bi (2D) e tridimensionais (3D) em microtomografia computadorizada (micro-CT). Canais radiculares de 24 molares decíduos foram preparados com limas manuais (M), ProTaper Next (PTN) e SAF (n=8/grupo). Os dentes foram escaneados antes e após o preparo do canal radicular e as imagens de micro-CT pré e pós-operatória foram reconstruídas. As mudanças nos parâmetros morfológicos 2D (área, perímetro, circularidade, menor e maior diâmetro) e 3D [volume, área de superfície, índice de estrutura do modelo (SMI)], bem como o transporte do canal radicular e a presença de perfurações laterais foram avaliadas (Kruskal-Wallis and ANOVA; a=0.05). SAF apresentou menores mudanças no diâmetro menor, volume e área de superfície quando comparado com M e PTN (p<0.05). PTN mostrou canais mais circulares após o preparo. A análise 3D revelou maior transporte para o grupo M. PTN e SAF mostraram maior centralização do preparo do canal radicular, especialmente em áreas de curvatura. SAF e M apresentaram, respectivamente, o menor (0,05±0,02 e 0,07±0,04) e o maior (0,14±0,11 e 0,29±0,17) transporte apical. Foi possível observar menor porcentagem de perfurações laterais para os grupos SAF (4,2%) e PTN (7,7%) comparados ao grupo M (47,8%) (p<0.05). Conclui-se que o preparo mecanizado dos canais radiculares em molares decíduos, apresentou melhor capacidade de modelagem do que as limas manuais, promovendo preparos mais centralizados e menor ocorrência de perfurações laterais e transporte do canal.
Introduction
In cases of primary molars with irreversibly inflamed or necrotic pulp, the endodontic treatment is considered as a conservative therapy, since it maintains these teeth until their physiological exfoliation. The maintenance of primary teeth contributes to mastication, phonation, and aesthetics, and avoids development of deleterious oral habits. Furthermore, the maintenance of primary teeth prevents changes in chronology and eruption sequence of permanent teeth 11 Pinheiro, SL; Araujo, G; Bincelli, I; Cunha, R; Bueno, C. Evaluation of cleaning capacity and instrumentation time of manual, hybrid and rotary instrumentation techniques in primary molars. Int Endod J 2012;45:379-385.,22 Cleghorn, BMB; Boorberg, NB; Christie, WH. Primary human teeth and their root canal systems. Endod Topics 2012;23: 6-33..
Manual instrumentation is still reported as the main choice in the primary teeth preparation, but studies have shown limitations to its use, with the possibility of ledge formation, perforations, dentin compaction and instrument fracture 33 Silva, LA; Leonardo, MR; Nelson Filho, P; Tanomaru, JM. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child (Chic) 2004;71:45-47.. On the other hand, rotary instrumentation dramatically reduces the working time, which is a very interesting aspect to consider for pediatric patients 11 Pinheiro, SL; Araujo, G; Bincelli, I; Cunha, R; Bueno, C. Evaluation of cleaning capacity and instrumentation time of manual, hybrid and rotary instrumentation techniques in primary molars. Int Endod J 2012;45:379-385.,33 Silva, LA; Leonardo, MR; Nelson Filho, P; Tanomaru, JM. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child (Chic) 2004;71:45-47.,44 Kumme,r TR; Calvo, MC; Cordeiro, MM; de Sousa Vieira, R; de Carvalho Rocha, MJ. Ex vivo study of manual and rotary instrumentation techniques in human primary teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105: e84-92.,55 Nazari, Moghaddam, K; Mehran, M; Farajian Zadeh, H. Root canal cleaning efficacy of rotary and hand files instrumentation in primary molars. Iran Endod j 2009;4:53-57.,66 Azar, MR; Safi, L; Nikaein, A. Comparison of the cleaning capacity of Mtwo and Pro Taper rotary systems and manual instruments in primary teeth. Dent Res J(Isfahan) 2012;9:146-151.,77 Seraj, B; Ramezani, G; Ghadimi, S; Mosharrafian, SH; Motahhary, P; Safari, M. In-vitro comparison of instrumentation time and cleaning capacity between endodontic hand piece and manual preparation techniques in primary molar teeth. Minerva Stomatol2013;62:17-22.,88 Katge, F; Patil D; Poojari, M; Pimpale, J; Shitoot, A; Rusawat, B. Comparison of instrumentation time and cleaning efficacy of manual instrumentation, rotary systems and reciprocating systems in primary teeth: an in vitro study. J Indian Soc Pedod Prev Dent 2014;32:311-316.,99 Selvakumar, H; Anandhan, V; Thomas, E; Swaminathan, K; Vijayakumar, R. Evaluation of canal transportation and centering ability of K 3 (0.02%) and K 3 (0.04%) with hand K files in primary teeth using spiral computed tomography. J Indian Soc Pedod Prev Dent 2014;32:286-291.,1010 Poornima, PDP; Nagaveni, NB; Roopa, KB; Bharath, K; Neena, IE. Volumetric analysis of hand and rotary root canal instrumentation and filling in primary teeth using Spiral Computed Tomography - an in vitro study. Int J Paediatr Dent 2016;26:193-198..
When planning and deciding on the cleaning and shaping protocol for primary teeth, their morphological characteristics must be considered 11 Pinheiro, SL; Araujo, G; Bincelli, I; Cunha, R; Bueno, C. Evaluation of cleaning capacity and instrumentation time of manual, hybrid and rotary instrumentation techniques in primary molars. Int Endod J 2012;45:379-385.,1111 Ahmed, HM. Anatomical challenges, electronic working length determination and current developments in root canal preparation of primary molar teeth. Int Endod J 2013;46:1011-1022., especially for posterior teeth, which have shorter and more curved roots, thinner dentin walls and ectopic surface resorption and a root canal system (RCS) characterized by a ribbon-shaped morphology 1212 Fumes, AC; Sousa-Neto, MD; Leoni, GB; Versian,i MA; da Silva, LA; da Silva, RA; et al.. Root canal morphology of primary molars: a micro-computed tomography study. Eur Arch Paediatr Dent 2014;15:317-326.. It is therefore important to choose instruments that maintain the original canal shape without producing deviations and provide a uniform removal of dentin from the canal walls.
A recent study 1212 Fumes, AC; Sousa-Neto, MD; Leoni, GB; Versian,i MA; da Silva, LA; da Silva, RA; et al.. Root canal morphology of primary molars: a micro-computed tomography study. Eur Arch Paediatr Dent 2014;15:317-326., evaluating the primary molar teeth anatomy suggested that Self-Adjusting File (SAF) instrument could be an alternative for cleaning and shaping these teeth, since the proposal of this instrument is its tridimensional adaptation to the root canal walls producing uniform removal around the root canal perimeter, as opposed to only preparing the canal’s central portion with a round shape 1313 Siqueira, JF Jr.; Alves, FR; Almeida, BM; de Oliveira, JC; Rocas, IN. Ability of chemomechanical preparation with either rotary instruments or self-adjusting file to disinfect oval-shaped root canals. J Endod 2010;36: 1860-1865.,1414 Paque, F; Peters, OA. Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molars with the self-adjusting file. J Endod 2011;37: 517-521.,1515 Versiani, MA; Pecora, JD; de Sousa Neto ,MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002-1007.,1616 Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066.,1717 Metzger, Z; Teperovich, E; Zary, R; Cohen, R; Hof, R. The self-adjusting file (SAF). Part 1: respecting the root canal anatomy--a new concept of endodontic files and its implementation. J Endod 2010;36:679-690..
At the same time, ProTaper Next (PTN) emerged as a system designed to combine the most proven performance features from the past with the most recent technological advancements. This system is claimed to simplify rotary shaping procedures by reducing the number of files to 33 Silva, LA; Leonardo, MR; Nelson Filho, P; Tanomaru, JM. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child (Chic) 2004;71:45-47. significant design features, including progressive percentage tapers on a single file, M-wire technology and the offset design 1818 Ruddle, CJ; Machtou, P; West, JD. The shaping movement: fifth-generation technology. Dent Today 2013;32:6-9.. To the best authors’ knowledge, there are no studies evaluating ProTaper Next system in the preparation of root canals of primary teeth.
Cleaning and shaping of the RCS of primary teeth has been traditionally evaluated by destructive methods that do not provide a three-dimensional analysis of the specimens, such as clearing technique, Indian ink injection 33 Silva, LA; Leonardo, MR; Nelson Filho, P; Tanomaru, JM. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child (Chic) 2004;71:45-47.,55 Nazari, Moghaddam, K; Mehran, M; Farajian Zadeh, H. Root canal cleaning efficacy of rotary and hand files instrumentation in primary molars. Iran Endod j 2009;4:53-57.,77 Seraj, B; Ramezani, G; Ghadimi, S; Mosharrafian, SH; Motahhary, P; Safari, M. In-vitro comparison of instrumentation time and cleaning capacity between endodontic hand piece and manual preparation techniques in primary molar teeth. Minerva Stomatol2013;62:17-22.,88 Katge, F; Patil D; Poojari, M; Pimpale, J; Shitoot, A; Rusawat, B. Comparison of instrumentation time and cleaning efficacy of manual instrumentation, rotary systems and reciprocating systems in primary teeth: an in vitro study. J Indian Soc Pedod Prev Dent 2014;32:311-316. and serial sectioning into root slices 44 Kumme,r TR; Calvo, MC; Cordeiro, MM; de Sousa Vieira, R; de Carvalho Rocha, MJ. Ex vivo study of manual and rotary instrumentation techniques in human primary teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105: e84-92.. Moreover, two recent studies 99 Selvakumar, H; Anandhan, V; Thomas, E; Swaminathan, K; Vijayakumar, R. Evaluation of canal transportation and centering ability of K 3 (0.02%) and K 3 (0.04%) with hand K files in primary teeth using spiral computed tomography. J Indian Soc Pedod Prev Dent 2014;32:286-291.,1010 Poornima, PDP; Nagaveni, NB; Roopa, KB; Bharath, K; Neena, IE. Volumetric analysis of hand and rotary root canal instrumentation and filling in primary teeth using Spiral Computed Tomography - an in vitro study. Int J Paediatr Dent 2016;26:193-198. showed the use of computed tomography (CT) in the assessment of root canal preparation of primary teeth. Is noteworthy that although there are no studies that assess the biomechanical preparation in primary teeth using micro-computed tomography (micro-CT), this methodology has been commonly used for this purpose in permanent teeth, as it allows a three-dimensional non-invasive assessment of the RCS and root canal preparation 1212 Fumes, AC; Sousa-Neto, MD; Leoni, GB; Versian,i MA; da Silva, LA; da Silva, RA; et al.. Root canal morphology of primary molars: a micro-computed tomography study. Eur Arch Paediatr Dent 2014;15:317-326.,1414 Paque, F; Peters, OA. Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molars with the self-adjusting file. J Endod 2011;37: 517-521.,1515 Versiani, MA; Pecora, JD; de Sousa Neto ,MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002-1007.,1616 Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066..
Considering the morphological characteristics of primary teeth, the concept of minimum and uniform removal of dentin from canal walls and the limited knowledge of shaping procedures in primary teeth for a more predictable endodontic treatment, the aim of this study was to evaluate qualitatively and quantitatively the preparation of root canals of primary molars with hand files, ProTaper Next and SAF, using micro-CT scanning.
Material and Methods
Selection and Preparation of Specimens
For sample size calculation, SigmaPlot 11.0 statistical software (Systat Software Inc., San Jose, CA, USA) was used based on the following pre-established parameters from a pilot study. For both morphometric data and transportation variables, the minimum detectable difference (MDD) between the means equal to 0.90 and 0.70 and variation coefficient equal to 0.50 and 0.40, respectively. An alpha-type error of 0.05, power beta of 0.8 and number of groups of 2 were considered. With these results, the estimated minimum sample per group was found to be 7 specimens for morphometric data and 8 for transportation analysis. Therefore, after Ethics Committee approval, 24 primary mandibular molars with physiological root resorption limited to the apical third were selected from a pool of extracted teeth and stored in 0.1% thymol solution until the moment of use.
After washing in running water, coronal opening was performed on the occlusal surface using round diamond burs (#1012; KG Sorensen, Barueri, SP, Brazil) and tapered carbide burs with non-cutting tip (Endo-Z; Dentsply Maillefer), in high rotation, aiming to obtain an trapezoidal shape. After that, the root canals were irrigated with 5 mL of 1% NaOCl and, to facilitate the positioning of the tooth during experimental steps, a self-curing resin custom-made mold for each tooth was made. Apical patency was confirmed by inserting a size 10 K-file (Dentsply Maillefer) into the root canal until its tip was visible at the apical foramen and the working length (WL) was set 1.0 mm shorter of this measure. Size 15 and 20 hand files were used at the WL to create a glide path 1515 Versiani, MA; Pecora, JD; de Sousa Neto ,MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002-1007.,1616 Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066.. A single experienced operator performed all preparations.
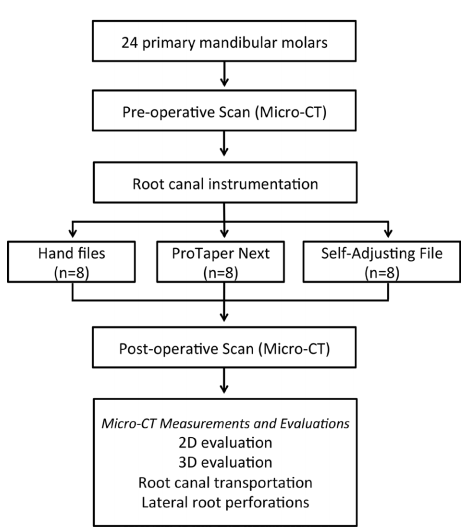
The specimens were scanned using a micro-CT scanner (SkyScan 1174v2; Bruker-micro-CT, Kontich, Belgium) operated at 50 kV, 800 mA (0.5-mm Al filter) and isotropic resolution of 16.7 µm. The scanning was performed by 180° rotation around the vertical axis with a rotation step of 1° 1212 Fumes, AC; Sousa-Neto, MD; Leoni, GB; Versian,i MA; da Silva, LA; da Silva, RA; et al.. Root canal morphology of primary molars: a micro-computed tomography study. Eur Arch Paediatr Dent 2014;15:317-326.,1515 Versiani, MA; Pecora, JD; de Sousa Neto ,MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002-1007.,1616 Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066.. Subsequently, these 24 teeth were matched to create eight groups of three based on the morphological aspects of the root canals (volume, surface area and 3D model). Then, one tooth from each group was randomly assigned to one of the 3 experimental groups (n=8) according to the root canal instrumentation technique: hand files (HF), ProTaper Next rotary system (PTN; Dentsply Maillefer) and Self-Adjusting File system (SAF) (ReDent Nova, Ra’anana, Israel) (Fig. 1).

Root Canal Preparation with Hand Files
The root canals were instrumented manually using crown-down technique with K files (Dentsply Maillefer) up to a #50 size file. Canals were irrigated with 1% NaOCl 1 mm shorter at each instrument change, using a total of 20 mL.
Root Canal Preparation with ProTaper Next System (PTN)
PTN files were powered by X-Smart™ endodontic micromotor (Dentsply/Maillefer) at a rotational speed of 300 rpm and 200 g/cm torque with in-and-out pecking motion combined with brushing action. Initially was used the Protaper Universal SX and next were used Protaper Next X1, X2 and X3 files. Canals were irrigated with 1% NaOCl 1 mm shorter at each instrument change, using a total of 20 mL.
Root Canal Preparation with SAF
A 1.5-mm diameter SAF instrument was operated to the WL with an in-and-out motion using a vibrating handpiece (GentlePower Lux 20LP; KaVo, Biberach, Germany) combined with a RDT3 head (ReDent-Nova) at a frequency of 83.3 Hz (5000 rpm) and amplitude of 0.4 mm for a total time of 4 min per canal. During the procedure, a continuous irrigation with 1.0% NaOCl with flow rate of 5 mL/min was applied by a special irrigation apparatus (VATEA, ReDent-Nova).
Micro-CT Measurements and Evaluations
The teeth were scanned again after canal preparation using the same parameters described for the preoperative analysis. The pre- and postoperative images were reconstructed using NRecon v.1.6.6.0 software (Bruker-micro-CT) and superimposed using a co-registration tool of DataViewer v.1.5.0 software (Bruker-micro-CT). CTAn v.1.14.4.1+ software (Bruker-micro-CT) was used for the 2D evaluation of the root canals at 1 mm from the apical foramen (area, perimeter, roundness, major diameter and minor diameter) and 3D evaluation of the canals from the cement enamel junction to the apex (volume, surface area and structure model index). The structure model index (SMI) involves a measurement of surface convexity in a 3D structure. An ideal plate, cylinder and sphere have SMI values of 0, 3, and 4, respectively 1212 Fumes, AC; Sousa-Neto, MD; Leoni, GB; Versian,i MA; da Silva, LA; da Silva, RA; et al.. Root canal morphology of primary molars: a micro-computed tomography study. Eur Arch Paediatr Dent 2014;15:317-326.,1515 Versiani, MA; Pecora, JD; de Sousa Neto ,MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002-1007.,1616 Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066.. The mean increase (Δ) of each 2D and 3D parameter was calculated by subtracting the postoperative values from the preoperative values. Color-coded root canal models (green indicating preoperative and red indicating postoperative canal surfaces) enabled qualitative comparison of the matched root canals before and after shaping using CTVol v.2.2.3.0 software (Bruker-micro-CT) 1515 Versiani, MA; Pecora, JD; de Sousa Neto ,MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002-1007.,1616 Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066..
Root canal transportation (in mm) was calculated by the mean difference between the centers of gravity for each apical slice before and after canal preparation. The size of the lateral root perforations (in mm) after preparation of each canal was also evaluated using CTAn v.1.14.4.1+ software (Bruker-micro-CT), according to the following classification: (a) absent, (b) than 1 mm, (c) between 1 and 2 mm and (d) larger than 2 mm. A single experienced operator performed all micro-CT analyses.
Statistical Analysis
After normality assumptions (Shapiro-Wilk test) and homogeneity of the variance (Levene test) were verified, the pre- and postoperative results for the 2D and 3D parameters were compared using paired-t test. The mean increase (Δ) of each parameter was compared among the groups by one-way ANOVA and post hoc Tukey’s test, and the lateral perforations scores were compared using Kruskal-Wallis and Dunn’s tests. SPSS v17.0 for Windows software (SPSS Inc., Chicago, IL, USA) was employed for all analyses with the level of statistical significance set at 5%. Kappa test was utilized to determinate the intra-examiner agreement (Kappa ≥ 0.85).
Results
The results of the 2D and 3D quantitative analysis are presented in Table 1. The preoperative analysis showed no statistically significant difference among the canals (p>0.05). The paired-t test showed that all the canal preparation techniques increased significantly the area, minor diameter, volume and surface area of the mesial and distal canals. SAF group presented the smallest mean increase of area, minor diameter, volume and surface area of the mesial and distal canal compared with HF and PTN groups (p<0.05). No significant difference was found among the groups regarding the major diameter (p>0.05). The shape (roundness) of both mesial and distal canals had greater alteration in the PTN group (p<0.05).
In the pre-preparation qualitative analysis (green), the 3D models showed the complexity of the RCS in primary molars with isthmuses and flattened areas (Fig. 2A). The changes in canal shape, shown by overlapping of unprepared canals (green) and prepared areas (red), showed an increase in canal contouring in all groups, being possible to observe greater transportation in HF group compared with the PTN and SAF groups, which exhibited more centered preparations, particularly in curved areas (Fig. 2B). A more uniform removal of dentin mass along the canal perimeter was observed in the SAF group. HF and PTN groups showed a more accentuated dentin removal from the inner canal walls towards the furcation region (danger area) (Figs. 2C and 2D)

Representative 2D and 3D reconstructions of the internal and external anatomy of the primary mandibular first molars before and after root canal preparation with hand, ProTaper Next and SAF files. (A) Preoperative 3D models of the internal root canal anatomy. (B) Buccal view of superimposed 3D models before (green) and after (red) root canal preparation. (C) Apical view of superimposed 3D models before (green) and after (red) root canal preparation. (D) Representative cross-sections of the superimposed root canals before (green) and after (red) preparation at the middle (m) and apical (a) thirds.

Distribution (%) of lateral perforations after root canal preparation with hand, ProTaper Next and SAF files. Different letters mean statistically significant difference (p<0.05).
SAF group showed lower apical transportation than HF group (p<0.05) and PTN group had intermediate values (Table 2). Lateral perforations were less frequent (p<0.05) in SAF (4.2%) and PTN (7.7%) groups compared with HF group (47.8%) (Fig. 3). SAF and PTN groups presented lateral perforations smaller than 1 mm while the HF groups presented lateral perforations larger than 2 mm (Fig. 3). Figure 4 exhibits irregularities and thinner dentin walls due to physiological root resorption before canal preparation, and the location and extent of perforations after biomechanical preparation.

Apical view of 3D models and representative cross-sections of groups HF, PTN and SAF showing irregularities and thinner dentin walls due to physiological root resorption before canal preparation, and the location and extent of perforations observed after canal preparation (black arrows).
Discussion
It is important to evaluate the action of different instruments on root canal geometry in different roots and tooth groups for endodontic treatment in primary teeth. Therefore, the objective of this study was to evaluate root canal preparation in primary mandibular molars with hand, ProTaper Next and SAF files, using micro-CT analysis.
Micro-CT analysis is a high-cost, labor-intensive and time-consuming methodology, which presents a steep learning curve to get the required expertise to extract quantitative data 1919 De-Deus, G; Marins, J; Neves A A de; Reis, C; Fidel, S, Versiani MA; et al.. Assessing accumulated hard-tissue debris using micro-computed tomography and free software for image processing and analysis. J Endod 2014;40:271-276.. Then, to ensure the internal validity of the experiment, the experienced and calibrated operator performed all micro-CT analyses.
Micro-CT scanning is a non-invasive and non-destructive technique that allows an accurate assessment of morphological characteristics of the RCS and the impact of the alterations occurred during the different phases of the endodontic treatment. While it is currently the methodology used in ex vivo studies of canal preparation in permanent teeth 1414 Paque, F; Peters, OA. Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molars with the self-adjusting file. J Endod 2011;37: 517-521.,1515 Versiani, MA; Pecora, JD; de Sousa Neto ,MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002-1007.,1616 Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066.,2020 Metzger, Z; Zary, R; Cohen, R; Teperovich, E; Paque, F. The quality of root canal preparation and root canal obturation in canals treated with rotary versus self-adjusting files: a three-dimensional micro-computed tomographic study. J Endod 2010;36:1569-1573.,2121 Zhao, D; Shen, Y; Peng, B; Haapasalo, M. Root canal preparation of mandibular molars with 3 nickel-titanium rotary instruments: a micro-computed tomographic study. J Endod 2014;40:1860-1864., the review of literature shows few studies using micro-CT to evaluate changes in the root canals of primary teeth after instrumentation.
Variations in canal geometry before shaping procedures seem to have more influence on the changes observed after preparation than the instrumentation techniques per se 1616 Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066.,2222 De Deus, G. Research that matters - root canal filling and leakage studies. Int Endod J2012;45:1063-1064.. Therefore, in the present study, attempts were made to create a reliable baseline, thus ensuring the comparison of groups for preoperative morphologic parameters.
SAF had the lowest mean increase in area, the minor diameter, volume and surface area in both mesial and distal canals. These findings corroborate previous studies in permanent teeth that showed lower dentin removal values with SAF compared with rotary instruments 1414 Paque, F; Peters, OA. Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molars with the self-adjusting file. J Endod 2011;37: 517-521.,1515 Versiani, MA; Pecora, JD; de Sousa Neto ,MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002-1007.,1616 Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066.,1717 Metzger, Z; Teperovich, E; Zary, R; Cohen, R; Hof, R. The self-adjusting file (SAF). Part 1: respecting the root canal anatomy--a new concept of endodontic files and its implementation. J Endod 2010;36:679-690.,1818 Ruddle, CJ; Machtou, P; West, JD. The shaping movement: fifth-generation technology. Dent Today 2013;32:6-9. and that instruments with different geometrical features produce preparations with different dimensions 2323 Ruddle, CJ. Nickel-titanium rotary instruments: current concepts for preparing the root canal system. Aust Endod J 2003;29:87-98.,2424 Peters, OA O. Current challenges and concepts in the preparation of root canal systems: a review. J Endod2004;30:559-567.,2525 Peters, OA; Paque, F. Current developments in rotary root canal instrument technology and clinical use: a review. Quintessence Int 2010;41:479-488.. SAF is a hollow, compressible instrument, with a thin abrasive layer on its surface, which expands inside the root canal and circumferentially removes a thin layer of dentin with a back-and-forth grinding motion 1717 Metzger, Z; Teperovich, E; Zary, R; Cohen, R; Hof, R. The self-adjusting file (SAF). Part 1: respecting the root canal anatomy--a new concept of endodontic files and its implementation. J Endod 2010;36:679-690.. This results in a preparation with a cross-section similar to the original canal, but only slightly larger 1717 Metzger, Z; Teperovich, E; Zary, R; Cohen, R; Hof, R. The self-adjusting file (SAF). Part 1: respecting the root canal anatomy--a new concept of endodontic files and its implementation. J Endod 2010;36:679-690.,2626 Metzger, Z; Teperovich, E; Cohen, R; Zary, R; Paque, F; Hulsmann, M. The self-adjusting file (SAF). Part 3: removal of debris and smear layer-A scanning electron microscope study. J Endod 2010;36:697-702.. On the other hand, the metallic structure and cutting efficiency of hand files and Protaper Next may explain their higher dentin removal capacity compared with SAF.
The mean increase in major diameter did not differ among groups possibly due to the shape of the root canals in primary molars 1212 Fumes, AC; Sousa-Neto, MD; Leoni, GB; Versian,i MA; da Silva, LA; da Silva, RA; et al.. Root canal morphology of primary molars: a micro-computed tomography study. Eur Arch Paediatr Dent 2014;15:317-326. as the flattened regions usually remain untouched by the instruments 2727 Keleş, A; Alcin, H; Kamalak, A; Versiani, MA. Oval-shaped canal retreatment with self-adjusting file: a micro-computed tomography study. Clin Oral Investig 2014;8:1147-1153..
The cross-sectional shape of the root canal in the apical third was evaluated using the morphometric parameter of roundness 1515 Versiani, MA; Pecora, JD; de Sousa Neto ,MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002-1007.,1616 Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066.. Roundness was more affected by ProTaper Next, which may be related to the fact that these instruments present increasing percentage taper in the apical portion.
Although PTN presented greater mean increases in the quantitative parameters of the root canal geometry compared with SAF, and greater removal of dentin from the canal walls, as seen in the 3D models, canal preparation with PTN also resulted in fewer occurrences of lateral perforations and intermediate behavior in apical transportation. These are important concerns during preparation of primary teeth because of the thinner dentin walls, especially in the danger zone, due to the permanent tooth germ. The manufacturer recommends the use of SAF for 4 min 1717 Metzger, Z; Teperovich, E; Zary, R; Cohen, R; Hof, R. The self-adjusting file (SAF). Part 1: respecting the root canal anatomy--a new concept of endodontic files and its implementation. J Endod 2010;36:679-690. and Protaper Next presents a reduced number of instruments compared with its predecessor, Universal Protaper 1818 Ruddle, CJ; Machtou, P; West, JD. The shaping movement: fifth-generation technology. Dent Today 2013;32:6-9.. The chairside team is also relevant in pediatric dentistry as it allows faster procedures while maintaining the quality and safety, in addition to reducing fatigue for the patient and the professional 44 Kumme,r TR; Calvo, MC; Cordeiro, MM; de Sousa Vieira, R; de Carvalho Rocha, MJ. Ex vivo study of manual and rotary instrumentation techniques in human primary teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105: e84-92..
In addition to these factors, the 3D models also showed larger deviations in the manual instrumentation group compared with PTN and SAF groups, which exhibited more centered preparations, especially in areas of curvature. Recent studies assessing canal preparation with ProTaper Next instruments in permanent teeth showed lower transportation by these instruments compared with other rotary Ni-Ti systems 2020 Metzger, Z; Zary, R; Cohen, R; Teperovich, E; Paque, F. The quality of root canal preparation and root canal obturation in canals treated with rotary versus self-adjusting files: a three-dimensional micro-computed tomographic study. J Endod 2010;36:1569-1573.. These files are made of a special NiTi alloy called M-Wire and incorporate a variable taper design and a unique offset mass of rotation, which improves the strength and flexibility along its active part 1818 Ruddle, CJ; Machtou, P; West, JD. The shaping movement: fifth-generation technology. Dent Today 2013;32:6-9.,2828 Pereira, ES; Peixoto, IF; Viana, AC; Oliveira, II; Gonzalez, BM; Buono, VT; et al.. Physical and mechanical properties of a thermomechanically treated NiTi wire used in the manufacture of rotary endodontic instruments. Int Endod J2012;45:469-674.. This may have contributed to the shaping ability of this instrument especially in the curved areas, since the primary molars have curvatures in both mesial and distal roots 1212 Fumes, AC; Sousa-Neto, MD; Leoni, GB; Versian,i MA; da Silva, LA; da Silva, RA; et al.. Root canal morphology of primary molars: a micro-computed tomography study. Eur Arch Paediatr Dent 2014;15:317-326.. Previous studies report that endodontic instruments manufactured with M-alloy wire are more flexible than those manufactured with conventional Ni-Ti alloy 2929 Ye, J; Gao, Y. Metallurgical characterization of M-Wire nickel-titanium shape memory alloy used for endodontic rotary instruments during low-cycle fatigue. J Endod 2012;38:105-107.,3030 Schafer, E. Root canal instruments for manual use: a review. Endod Dent Traumatol 1997;13:51-64., which in turn are more flexible than the stainless steel hand instruments, which have reduced flexibility 3131 Schafer, E; Schulz-Bongert, U; Tulus, G. Comparison of hand stainless steel and nickel titanium rotary instrumentation: a clinical study. J Endod 2004;30:432-435.. In the present study, the manual instrumentation did not maintain the original canal anatomy and caused a greater incidence of lateral perforations and apical transportation. Such results in numerous studies in permanent teeth contraindicate these instruments for preparation of teeth with accentuated root curvature 2424 Peters, OA O. Current challenges and concepts in the preparation of root canal systems: a review. J Endod2004;30:559-567.,3131 Schafer, E; Schulz-Bongert, U; Tulus, G. Comparison of hand stainless steel and nickel titanium rotary instrumentation: a clinical study. J Endod 2004;30:432-435..
In primary teeth, mechanical instrumentation showed better results than manual instrumentation, producing more centered preparations and a smaller number of lateral perforations and canal transportation. Comparing to the mechanical systems, SAF produced a more homogeneous preparation of primary root canals.
References
-
1Pinheiro, SL; Araujo, G; Bincelli, I; Cunha, R; Bueno, C. Evaluation of cleaning capacity and instrumentation time of manual, hybrid and rotary instrumentation techniques in primary molars. Int Endod J 2012;45:379-385.
-
2Cleghorn, BMB; Boorberg, NB; Christie, WH. Primary human teeth and their root canal systems. Endod Topics 2012;23: 6-33.
-
3Silva, LA; Leonardo, MR; Nelson Filho, P; Tanomaru, JM. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child (Chic) 2004;71:45-47.
-
4Kumme,r TR; Calvo, MC; Cordeiro, MM; de Sousa Vieira, R; de Carvalho Rocha, MJ. Ex vivo study of manual and rotary instrumentation techniques in human primary teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105: e84-92.
-
5Nazari, Moghaddam, K; Mehran, M; Farajian Zadeh, H. Root canal cleaning efficacy of rotary and hand files instrumentation in primary molars. Iran Endod j 2009;4:53-57.
-
6Azar, MR; Safi, L; Nikaein, A. Comparison of the cleaning capacity of Mtwo and Pro Taper rotary systems and manual instruments in primary teeth. Dent Res J(Isfahan) 2012;9:146-151.
-
7Seraj, B; Ramezani, G; Ghadimi, S; Mosharrafian, SH; Motahhary, P; Safari, M. In-vitro comparison of instrumentation time and cleaning capacity between endodontic hand piece and manual preparation techniques in primary molar teeth. Minerva Stomatol2013;62:17-22.
-
8Katge, F; Patil D; Poojari, M; Pimpale, J; Shitoot, A; Rusawat, B. Comparison of instrumentation time and cleaning efficacy of manual instrumentation, rotary systems and reciprocating systems in primary teeth: an in vitro study. J Indian Soc Pedod Prev Dent 2014;32:311-316.
-
9Selvakumar, H; Anandhan, V; Thomas, E; Swaminathan, K; Vijayakumar, R. Evaluation of canal transportation and centering ability of K 3 (0.02%) and K 3 (0.04%) with hand K files in primary teeth using spiral computed tomography. J Indian Soc Pedod Prev Dent 2014;32:286-291.
-
10Poornima, PDP; Nagaveni, NB; Roopa, KB; Bharath, K; Neena, IE. Volumetric analysis of hand and rotary root canal instrumentation and filling in primary teeth using Spiral Computed Tomography - an in vitro study. Int J Paediatr Dent 2016;26:193-198.
-
11Ahmed, HM. Anatomical challenges, electronic working length determination and current developments in root canal preparation of primary molar teeth. Int Endod J 2013;46:1011-1022.
-
12Fumes, AC; Sousa-Neto, MD; Leoni, GB; Versian,i MA; da Silva, LA; da Silva, RA; et al.. Root canal morphology of primary molars: a micro-computed tomography study. Eur Arch Paediatr Dent 2014;15:317-326.
-
13Siqueira, JF Jr.; Alves, FR; Almeida, BM; de Oliveira, JC; Rocas, IN. Ability of chemomechanical preparation with either rotary instruments or self-adjusting file to disinfect oval-shaped root canals. J Endod 2010;36: 1860-1865.
-
14Paque, F; Peters, OA. Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molars with the self-adjusting file. J Endod 2011;37: 517-521.
-
15Versiani, MA; Pecora, JD; de Sousa Neto ,MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002-1007.
-
16Versiani, MA; Leoni, GB; Steier, L; De-Deus, G; Tassani, S; Pécora, JD; et al.. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file Reciproc WaveOne and ProTaper Universal systems. J Endod 2013;39:1060-1066.
-
17Metzger, Z; Teperovich, E; Zary, R; Cohen, R; Hof, R. The self-adjusting file (SAF). Part 1: respecting the root canal anatomy--a new concept of endodontic files and its implementation. J Endod 2010;36:679-690.
-
18Ruddle, CJ; Machtou, P; West, JD. The shaping movement: fifth-generation technology. Dent Today 2013;32:6-9.
-
19De-Deus, G; Marins, J; Neves A A de; Reis, C; Fidel, S, Versiani MA; et al.. Assessing accumulated hard-tissue debris using micro-computed tomography and free software for image processing and analysis. J Endod 2014;40:271-276.
-
20Metzger, Z; Zary, R; Cohen, R; Teperovich, E; Paque, F. The quality of root canal preparation and root canal obturation in canals treated with rotary versus self-adjusting files: a three-dimensional micro-computed tomographic study. J Endod 2010;36:1569-1573.
-
21Zhao, D; Shen, Y; Peng, B; Haapasalo, M. Root canal preparation of mandibular molars with 3 nickel-titanium rotary instruments: a micro-computed tomographic study. J Endod 2014;40:1860-1864.
-
22De Deus, G. Research that matters - root canal filling and leakage studies. Int Endod J2012;45:1063-1064.
-
23Ruddle, CJ. Nickel-titanium rotary instruments: current concepts for preparing the root canal system. Aust Endod J 2003;29:87-98.
-
24Peters, OA O. Current challenges and concepts in the preparation of root canal systems: a review. J Endod2004;30:559-567.
-
25Peters, OA; Paque, F. Current developments in rotary root canal instrument technology and clinical use: a review. Quintessence Int 2010;41:479-488.
-
26Metzger, Z; Teperovich, E; Cohen, R; Zary, R; Paque, F; Hulsmann, M. The self-adjusting file (SAF). Part 3: removal of debris and smear layer-A scanning electron microscope study. J Endod 2010;36:697-702.
-
27Keleş, A; Alcin, H; Kamalak, A; Versiani, MA. Oval-shaped canal retreatment with self-adjusting file: a micro-computed tomography study. Clin Oral Investig 2014;8:1147-1153.
-
28Pereira, ES; Peixoto, IF; Viana, AC; Oliveira, II; Gonzalez, BM; Buono, VT; et al.. Physical and mechanical properties of a thermomechanically treated NiTi wire used in the manufacture of rotary endodontic instruments. Int Endod J2012;45:469-674.
-
29Ye, J; Gao, Y. Metallurgical characterization of M-Wire nickel-titanium shape memory alloy used for endodontic rotary instruments during low-cycle fatigue. J Endod 2012;38:105-107.
-
30Schafer, E. Root canal instruments for manual use: a review. Endod Dent Traumatol 1997;13:51-64.
-
31Schafer, E; Schulz-Bongert, U; Tulus, G. Comparison of hand stainless steel and nickel titanium rotary instrumentation: a clinical study. J Endod 2004;30:432-435.
Publication Dates
-
Publication in this collection
Jul-Aug 2017
History
-
Received
22 Feb 2017 -
Accepted
09 May 2017