
Abstract
The aim of this study was to evaluate Knoop hardness of different shades of a resin cement light-cured directly or through ceramic discs, measured 15 min or 24 h after light exposure, and at different depths. Specimens of a commercial resin cement (Variolink Veneer) in seven shades, were fabricated in an elastomeric mold, covered with a mylar strip, a 0.7 mm thick ceramic disc (IPS e.max Press) was placed and the cement was light-activated for 20 s using a blue LED (Radii-Cal). The cured resin cement specimens were transversely wet-flattened to their middle portion and microhardness (Knoop) values were recorded at 15 min after light exposure and after deionized water storage at 37 ºC for 24 h. Five indentations were made in the cross-sectional area at 100 and 700 μm depths from the top surface. Ten specimens were made for each test conditions. Data were submitted to ANOVA split-plot design (shade, post-cure time, mode of activation and depth), followed by Tukey post hoc test (α=0.05). Significant differences for shade (p<0.0001), mode of activation (p<0.001), post-cure time (p<0.0001) and depth (p<0.0001) were detected. No significant interactions (p>0.05) were found, except for shade x post-cure time (p<0.0045) and mode of activation x post-cure time (p<0.0003). Resin cement shade has a significant effect on Knoop hardness. Indirect activation through a ceramic material reduced significantly Knoop hardness. Hardness Knoop significantly increased after 24 h in all cements shades compared to values obtained after 15 min. Resin cement depth significantly reduced Knoop hardness.
Key Words:
ceramics; dental materials; hardness; resin cements; polymerization
Resumo
O objetivo deste estudo foi avaliar a dureza Knoop de diferentes cores de um cimento resinoso fotoativado diretamente ou através da interposição de um disco de cerâmica, medindo 15 min ou 24 h após exposição à luz, em diferentes profundidades. Amostras do cimento resinoso (Variolink Veneer) em sete cores foram fabricados num molde de elastômero, coberto com tira de poliéster, seguido de um disco cerâmico (IPS e.max Press) com 0.7 mm de espessura e fotoativado por 20 s com o aparelho LED (IPS e.max Press). O cimento resinoso fotoativado foi transversalmente desgastado na porção média e os valores de microdureza Knoop foram obtidos após 15 min após exposição à luz e após armazenagem em água deionizada à 37 °C por 24 h. Cinco penetrações foram feitas na secção transversal à 100 e 700 μm da superfície de topo. Dez amostras foram confeccionadas para cada condição de teste. Os dados foram submetidos à Análise de Variância em esquema de parcelas subdivididas (cor, tempo pós-ativação, modo de ativação e profundidade), seguido pelo teste de Tukey post hoc (α=0,05). Diferença significante para a cor (p<0,0001), modo de ativação (p<0,001), tempo pós-ativação (p<0,0001) e profundidade (p<0,0001) foi detectada. Nenhuma interação significante foi encontrada (p>0,05), exceto para a interação cor x tempo pós-ativação (p<0,0045) e modo de ativação x tempo pós-ativação (p<0,0003). A cor do cimento resinoso teve significante efeito na dureza Knoop. A ativação indireta através do material cerâmico reduziu significativamente a dureza Knoop. A dureza Knoop aumentou significativamente após 24 h em todas as cores do cimento comparados aos valores obtidos após 15 min. A profundidade do cimento resinoso reduziu significativamente os valores de dureza Knoop.
Introduction
Interest in dental ceramics has increased in restorative dentistry, mostly because of the excellent esthetic and mechanical properties of these type products. However, brittleness and susceptibility to fracture are major disadvantages of their use11 Lawn, BR; Pajares, A; Zhang, Y; Deng, Y; Polack, MA; Lloyd, IK; et al.. Materials design in the performance of all-ceramic crowns. Biomaterials 2004;25:2885-2892. . In order to minimize these deficiencies and strengthen all-ceramic restorations, adhesive cementation of these materials with resin cement has been suggested22 Groten, M; Pröbster, L. The influence of different cementation modes on the fracture resistance of feldspathic ceramic crowns. Int J Prosthodont 1997;10:169-177.. Clinically, the success of ceramic depends, to a great extent, on the quality of resin cement cure.
These cements are classified according to their activation mode: chemical, photo or dual curing33 Reges, RV; Moraes, RR; Correr, AB; Sinhoreti, MAC; Correr, Sobrinho, L; Piva, E; et al.. In-depth polymerization of dual-cured resin cement assessed by hardness. J Biomater Appl 2008;23:85-96.. Light-cured cements offer the clinical advantages of extended working time, setting on demand and improved color stability44 Pegoraro, TA; Silva, NRFA; Carvalho, RM. (2007) Cements for use in esthetic dentistry. Dent Clin North Am 2007;51:453-471. . After cementation, an adequate polymerization of resin cement is necessary to obtain high and stable bond strengths. Inadequate polymerization is associated with lower color stability, poor mechanical properties, and increased water sorption and solubility55 Janda, R; Roulet, JF; Latta, M; Rüttermann, S. Water sorption and solubility of contemporary resin-based filling materials. J Biomed Mater Res B Appl Biomater 2007;82:545-551.,66 Dall’Magro, E; Sinhoreti, MA; Correr, AB; Consani, RL; Sicoli, EA; Mendonça, MJ; et al.. Effect of different modes of light modulation on the bond strength and Knoop hardness of a dental composite. Braz Dent J 2008;19:334-340.. Previous investigators have reported that intervening restorative ceramics between the light curing unit (LCU) and resin cement might promote a significant attenuation of light reaching the photo-curable cement, and compromise the photo-activation of the luting material77 Blackman, R; Barghi, N; Duke, E. Influence of ceramic thickness on the polymerization of light-cured resin cement. J Prosthet Dent 1990;63:295-300.,88 Jung, H; Friedl, KH; Hiller, KA; Haller, A; Schmalz, G. Curing efficiency of different polymerization methods through ceramic restorations. Clin Oral Investig 2001;5:156-161.. The level of this attenuation is dependent on characteristics of the restorative material (shade, crystalline structure, thickness and opacity), which may interfere with light transmittance and, as result, produce inadequate cement polymerization99 Uctasli, S; Hasanreisoglu, U; Wilson, HJ. The attenuation of radiation by porcelain and its effect on polymerization of resin cements. J Oral Rehabil 1994;21:565-575.,1010 Pazin, MC; Moraes, RR; Gonçalves, LS; Borges, GA; Sinhoreti, MAC; CorrerSobrinho, L. Effects of ceramic thickness and curing unit on light transmission through leucite-reinforced material and polymerization of dual-cured luting agent. J Oral Sci 2008;50:131-136.,1111 Kilinc, E; Antonson, SA; Hardigan, PC; Kesercioglu, A. The effect of ceramic restoration shade and thickness on the polymerization of light- and dual-cure resin cements. Oper Dent 2011;36:661-669..
In addition, polymerization of the resin cement may also be influenced by characteristics of the cement as well: shade, chemical composition and filler particle size1212 Shortall, AC. How light source and product shade influence cure depth for a contemporary composite. J Oral Rehabil 2005;32:906-911.,1313 Reges, RV; Costa, AR; Correr, AB; Piva, E; Puppin-Rontani, RM; Sinhoreti, MAC; et al.. Effect of light-curing units, post-cured time and shade of resin cement on Knoop hardness. Braz Dent J 2009;20:410-413.. These factors may interfere with the depth of cure of the resin cement and can be associated with the physical properties and satisfactory clinical performance of the restoration33 Reges, RV; Moraes, RR; Correr, AB; Sinhoreti, MAC; Correr, Sobrinho, L; Piva, E; et al.. In-depth polymerization of dual-cured resin cement assessed by hardness. J Biomater Appl 2008;23:85-96.. Some studies have evaluated the effect of indirect activation or the depth of polymerization of different shades of resin cement77 Blackman, R; Barghi, N; Duke, E. Influence of ceramic thickness on the polymerization of light-cured resin cement. J Prosthet Dent 1990;63:295-300.,88 Jung, H; Friedl, KH; Hiller, KA; Haller, A; Schmalz, G. Curing efficiency of different polymerization methods through ceramic restorations. Clin Oral Investig 2001;5:156-161.,1111 Kilinc, E; Antonson, SA; Hardigan, PC; Kesercioglu, A. The effect of ceramic restoration shade and thickness on the polymerization of light- and dual-cure resin cements. Oper Dent 2011;36:661-669.,1212 Shortall, AC. How light source and product shade influence cure depth for a contemporary composite. J Oral Rehabil 2005;32:906-911.,1414 Leloup, G; Holvoet, PE; Bebelman, S; Devaux, J. Raman scattering determination of the depth of cure of light-activated composites: influence of different clinically relevant parameters. J Oral Rehabil 2002;29:510-515.. However, little is known about the combined influence of different resin cement shades and indirect light-activation through a restorative ceramic.
Therefore, the aim of this study was to evaluate the microhardness (Knoop hardness number - KHN) of different shades of a commercial light-cured resin cement (Variolink Veneer) with the material light-activated either through or without a ceramic restoration present and tested either after 15 min or 24 h. The hypotheses tested were: 1) Knoop hardness would similar for different cement shades; 2) Knoop hardness of all resin shades would not significantly different between cement shades; 2) Knoop hardness of all resin shades would not significantly different between post-cured measurement times (15 min and 24 h); 3) The Knoop hardness of resin cement specimens would not significantly different between use of either cement polymerization activated mode light cure (direct or indirect); and44 Pegoraro, TA; Silva, NRFA; Carvalho, RM. (2007) Cements for use in esthetic dentistry. Dent Clin North Am 2007;51:453-471. There would not significant difference Knoop hardness at different depths of resin cement (100-700 μm depth).
Material and Methods
Ten discs (10 mm diameter by 0.9 mm thick) were fabricated in a lithium disilicate glass ceramic (IPS e.max Press, shade HT A1, Ivoclar Vivadent, Schaan, Liechtenstein), according to manufacturer’s instructions. The resulting discs were submitted to a sequential wet polishing SiC abrasive papers (320, 400, 600 and 1200 grit; Norton SA, São Paulo, SP, Brazil) in a water-cooled automatic polisher (APL4; Arotec, Cotia, SP, Brazil) in order to obtain a final 10 mm diameter of 0.7 mm thickness. Specimens were ultrasonically cleaned in distilled water for 10 min and dried with compressed air. The thickness of the disc was measured using a digital caliper (Mitutoyo Corporation, Tokyo, Japan), with an accuracy of 0.01 mm.
A commercial light-cured veneer luting resin cement (Variolink Veneer, Ivoclar), was cured in seven shades. The radiopaque shades are Low Value (LV -1, -2 and -3) and High Value (HV +3), while shades that are not radiopaque consist of Medium Value (MV 0) and High Value (HV +1 and HV +2), according to manufacturer’s information. The colors corresponding to High Value render brighter and white surfaces, with HV+3 corresponding to an opaque having the lowest translucency (about 5%). The MV0 shade is the most neutral and presents the highest translucency (about 50%). The colors of Low Value present a warm, yellow-reddish tinge, and LV -3 has a low translucency (about 9%).
Resin cement was dispensed directly into an elastomeric mold (5 mm in diameter by 1 mm thickness, Express putty - 3M ESPE, St. Paul, MN, USA). A transparent polyester strip was then placed over the filled mold and manual downward pressure was applied, using a microscope slide, to force the cement to obtain the shape of the mold and to remove excess material. The microscope slide was removed and a ceramic disc was placed on the polyester strip, over the resin cement. The underlying resin cement was exposed to a light curing unit (LCU) directly through the ceramic (indirect mode - I), for 20 s, using a blue LED photocuring light (Radii-cal, SDI Limited, Bayswater, Victoria, Australia) having an irradiance of 1,200 mW/cm2 as measured using a curing radiometer (Model 100, Demetron Research Corporation, Danbury, CT). The light guide end was in contact with the surface of the ceramic during exposure. Figure 1 shows the experimental setup of the study.

Schematic diagram of the experimental setup. Resin cement (Variolink Veneer) was inserted into the elastomeric mold, a polyester strip was placed over the filled mold, the ceramic disc was positioned over the resin cement and a light curing unit was placed onto the ceramic surface for photo-activation of the underlying resin cement.
Twenty specimens were fabricated for each resin cement shade. Half of the specimens were tested for microhardness 15 min after light exposure and the remaining specimens were evaluated after 24 h of deionized water storage at 37 °C in light-proof containers. Twenty additional specimens for each resin cement shade were fabricated by light-activation without the ceramic disc present (direct mode - D), half of which had microhardness evaluated 15 min following light exposures and half after 24 h.
In order to obtain a smooth and plane surface for microhardness testing, the polymerized cement specimens were attached to an acrylic resin dye (Buehler, Lake Bluff, IL, USA) using sticky wax and were then transversely wet-cut using a series of SiC abrasive papers (320, 400, 600 and 1200 grit, Norton SA) in a water-cooled automatic polisher (APL4; Arotec). Knoop microhardness measurements were performed using a microhardness tester (HMV-2; Shimadzu Corp., Tokyo, Japan) under a load of 50 g applied for 15 s. Five indentations were made in the cross-sectional area at depths of 100 and 700 μm from the top surface (Fig. 2). The average value of the five readings was recorded as the Knoop hardness for that specific specimen at the given depth. Microhardness of the resin cement top surface layer was not tested, because it is known to have a lower extent of polymerization, due to oxygen inhibition and would yield lower hardness values33 Reges, RV; Moraes, RR; Correr, AB; Sinhoreti, MAC; Correr, Sobrinho, L; Piva, E; et al.. In-depth polymerization of dual-cured resin cement assessed by hardness. J Biomater Appl 2008;23:85-96..
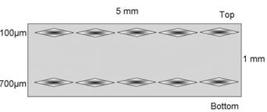
Diagram of the cross-sectional area of the flatted, polished cement specimen for Knoop hardness readings at different depths.
Exploratory data analyses were performed prior to applying an analysis of variance (ANOVA) split-plot design. The preliminary results by the Kolmogorov-Smirnov test indicated the data were normally distributed (p>0.05). The ANOVA tested the effect of the major factors of cement shade (at 7 levels), post-cure time (2 levels) and mode of activation (2 levels), as well as their interaction terms.
In addition, the effect of cement depth (2 levels) was examined with respect to the other major factors, as well as their interaction terms. Where appropriate, post-hoc, pair wise comparisons of means was tested using the Tukey test (SAS Institute Inc., Cary, NC, USA, version 9.3). All statistical testy was performed at a pre-set alpha of 0.05.
Results
The mean values of Knoop hardness are shown in Table 1. Significant influences of resin cement shades (p<0.0001), modes of activation (p<0.001), post-cure times (p<0.0001), and depths (p<0.0001) were detected. There were no significant interactions (p>0.05), except between shade x post-cure time (p<0.0045), and between modes of activation x post-cure time (p<0.0003).
When shades were compared, the mean Knoop hardness of MV0 was significantly greater than all other shades (p<0.05). The HV +3 shade demonstrated lower hardness values (p<0.05), regardless of the cement depth, mode of activation or post-cured time. No significant differences in hardness were found among the shades LV -1, LV -2, and HV +2 (p>0.05), or among the shades HV +2, HV +3, and LV -2 (p>0.05) in all conditions.
For all cements shades, there was a significant increase in Knoop hardness 24 h following light curing, compared to that at 15 min (p<0.05), for the same conditions of the direct and indirect curing methods and for all cement depths. All cements shades demonstrated a statistically significant higher Knoop hardness when exposed using direct as opposed to the indirect mode. When the effect of cement depth was analyzed, the hardness at 100 μm was significantly greater than at 700 μm (p<0.05), for the same conditions of the direct and indirect curing methods and post-cure time.
Discussion
The first hypothesis, which stated that Knoop hardness is not different among the different cement shades was rejected. The results showed that higher values for Knoop hardness were obtained for the shade MV0, with a statistically significant difference when compared to other shades. The HV+3 shade showed lower hardness values. Comparison of hardness values among shades at 15 min and a 24 h post light exposure showed that the values of MV0>HV+1>LV-1>LV-3=HV+2=LV-2>HV+3 (p<0.05), regardless of the mode of activation, post-cure time or cement depth. Thus, each cement shade might require a specific activation strategy in order to maximize hardness. A reliable polymerization depends on the light dispersion within of the material and an adequate amount of light is required to obtain high polymerization1414 Leloup, G; Holvoet, PE; Bebelman, S; Devaux, J. Raman scattering determination of the depth of cure of light-activated composites: influence of different clinically relevant parameters. J Oral Rehabil 2002;29:510-515.. Others showed a relationship between depth of cure and translucency of resin cement. Opaque cement shades may not cure adequately, because of the increase in light absorption by the pigments and because of the decreased capacity for light to penetrate into the composite, decreasing the hardness of the cement33 Reges, RV; Moraes, RR; Correr, AB; Sinhoreti, MAC; Correr, Sobrinho, L; Piva, E; et al.. In-depth polymerization of dual-cured resin cement assessed by hardness. J Biomater Appl 2008;23:85-96.,1212 Shortall, AC. How light source and product shade influence cure depth for a contemporary composite. J Oral Rehabil 2005;32:906-911.,1515 Guiraldo, RD; Consani, S; Consani, RLX; Berger, SB; Mendes, WB; Sinhoreti, MAC. Light energy transmission through composite influenced by material shades. Bull Tokyo Dent Coll 2009;50:183-190.. Another study detected that the more translucent the resin cement, the higher is the hardness1515 Guiraldo, RD; Consani, S; Consani, RLX; Berger, SB; Mendes, WB; Sinhoreti, MAC. Light energy transmission through composite influenced by material shades. Bull Tokyo Dent Coll 2009;50:183-190.. According to the author, this results can be explained by the fact that transparent resin cements absorb more light, and the depth of polymerization of these cements is higher than for the opaque cements.
In the present study, two post-cure times, 15 min and 24 h, were evaluated. The results indicated that the second hypothesis was not accepted. All resin cements shades showed a significant increase in Knoop hardness after 24 h, relative to values at 15 min, for the same conditions of the direct and indirect curing methods, and at all cement depths. Although the polymerization of light-activated resin cement occurs within the first 10 to 15 minutes, the cure can continue to increase until 24 h after light activation1616 Yan, YL; Kim, YK; Kim, K-H; Kwon, T-Y. Changes in degree of conversion and microhardness of dental resin cements. Oper Dent 2010;35:203-210.. A significant amount of free radicals remain trapped within the matrix after the end of irradiation, allowing continued formation of polymer chains, which increases the hardness values. The “post-activation” reaction can continue, because there are free radicals available and monomers present having sufficient mobility1717 Watts, DC; McNaughton, V; Grant, AA. The development of surface hardness in visible light-cured posterior composites. J Dent 1986;14:169-174. . This increase in cure is clinically important because an adequate polymerization of resin cement must be rapidly obtained for the material to withstand immediate loading from chair side adjustments and occlusal forces and must also present adequate biocompatibility33 Reges, RV; Moraes, RR; Correr, AB; Sinhoreti, MAC; Correr, Sobrinho, L; Piva, E; et al.. In-depth polymerization of dual-cured resin cement assessed by hardness. J Biomater Appl 2008;23:85-96..
In relation to the mode of activation, the direct mode showed higher hardness values than the indirect mode at both of the two post-cure times and among all cements shades. The results indicate that the third hypothesis was rejected. This finding is due to light attenuation caused by the placement of the intervening ceramic material. Others showed that this decrease in light might influence polymer development primary by decreasing double bond conversion, because polymerization is dependent on the radiant exposure to cause free radical formation1818 Halvorson, RH; Erickson, RL; Davdson, CL. Energy dependent polymerization of resin-based composite. Dent Mater 2002;18:463-469.. In addition, indirect polymerization activation reduces the level of irradiance to the luting material and the resulting polymer network development might be affected by decreasing the monomer conversion and also by interfering with the type and degree of cross-linking1919 Schneider, LF; Moraes, RR; Cavalcante, LM; Sinhoreti, MA; CorrerSobrinho, L. Cross-link density evaluation through softening tests: effect of ethanol concentrations. Dent Mater 2008;24:199-203. .
The results of the present work are in agreement with those of a previous study, which found higher hardness values when using the direct activation mode in relation to the indirect mode77 Blackman, R; Barghi, N; Duke, E. Influence of ceramic thickness on the polymerization of light-cured resin cement. J Prosthet Dent 1990;63:295-300.. However, some studies have found no significant difference between direct and indirect activation modes and interposing a ceramic disc of 0.7-1010 Pazin, MC; Moraes, RR; Gonçalves, LS; Borges, GA; Sinhoreti, MAC; CorrerSobrinho, L. Effects of ceramic thickness and curing unit on light transmission through leucite-reinforced material and polymerization of dual-cured luting agent. J Oral Sci 2008;50:131-136., 1-20)20 Runnacles, P; Correr, GM; Baratto, F Filho; Gonzaga, CC; Furuse, AY. Degree of conversion of a resin cement light-cured through ceramic veneers of different thicknesses and types. Braz Dent J 2014;25:38-42. or 2- mm thickness1111 Kilinc, E; Antonson, SA; Hardigan, PC; Kesercioglu, A. The effect of ceramic restoration shade and thickness on the polymerization of light- and dual-cure resin cements. Oper Dent 2011;36:661-669.. Another study showed that sufficient light energy was probably delivered to both surfaces of the specimens and consequently no significant influence in hardness occurred, or as result of the additional chemical curing effect that compensates for lower light levels of the bottom cement layers1010 Pazin, MC; Moraes, RR; Gonçalves, LS; Borges, GA; Sinhoreti, MAC; CorrerSobrinho, L. Effects of ceramic thickness and curing unit on light transmission through leucite-reinforced material and polymerization of dual-cured luting agent. J Oral Sci 2008;50:131-136.. Dual-cured resin cements are indicated to compensate for the attenuation of light caused by interposition of an indirect restorative material and to ensure adequate polymerization of the resin cement2121 Lee, IB; Um, CM. Thermal analysis on the cure speed of dual cured resin cements under porcelain inlays. J Oral Rehabil 2001;28:186-197.. The results of this study suggest that, for all resin cement shades, insufficient light energy for polymerization was delivered to the specimens during indirect activation. Increasing the exposure time of the resin cement may result in higher hardness values2222 AlShaafi, MM; AlQahtani, MQ; Price, RB. Effect of exposure time on the polymerization of resin cement through ceramic. J Adhes Dent 2014;16:129-135..
When the factor of cement depth was analyzed, the hardness at 100 μm was significantly greater than at 700 μm. Thus, the fourth hypothesis was rejected. These findings are in agreement with those of previous studies, which also found higher hardness values within the top 100 μm than at the bottom 700 μm33 Reges, RV; Moraes, RR; Correr, AB; Sinhoreti, MAC; Correr, Sobrinho, L; Piva, E; et al.. In-depth polymerization of dual-cured resin cement assessed by hardness. J Biomater Appl 2008;23:85-96.,2323 Puppin-Rontani, RM; Dinelli, RG; de Paula, AB; Fucio, SB; Ambrosano, GM; Pascon, FM. In-depth polymerization of a self-adhesive dual-cured resin cement. Oper Dent 2012;37:188-194.. During photoactivation, the incident light is attenuated with increasing depth from the irradiated surface, as a result of absorption and scattered by the fillers and resin components, reducing the curing effectiveness and thus hardness values as the depth increases1717 Watts, DC; McNaughton, V; Grant, AA. The development of surface hardness in visible light-cured posterior composites. J Dent 1986;14:169-174. ,2424 Rueggeberg, F. Contemporary Issues in Photocuring. Compend Contin Educ Dent Suppl 1999;Supplement 25:4-15.. Other studies have shown that only 25% of light striking the top surface of the composite is available at 1 mm depth2424 Rueggeberg, F. Contemporary Issues in Photocuring. Compend Contin Educ Dent Suppl 1999;Supplement 25:4-15. and similar attenuation might be caused by interposition of an indirect restorative material88 Jung, H; Friedl, KH; Hiller, KA; Haller, A; Schmalz, G. Curing efficiency of different polymerization methods through ceramic restorations. Clin Oral Investig 2001;5:156-161.. Although film thickness of 700 μm might not be suitable for luting purposes, the depth of polymerization of resin cements may indicate their polymerization potential. In a clinical situation, light attenuation caused by an indirect restorative material could be worsened by low irradiance levels of the light curing device. Moreover, shades, opacities and thicknesses of the indirect restorations may also interfere33 Reges, RV; Moraes, RR; Correr, AB; Sinhoreti, MAC; Correr, Sobrinho, L; Piva, E; et al.. In-depth polymerization of dual-cured resin cement assessed by hardness. J Biomater Appl 2008;23:85-96.,2525 Salameh, Z; Tehini, G; Ziadeh, N; Ragab, HA; Berberi, A; Aboushelib, MN. Influence of ceramic color and translucency on shade match of CAD/CAM porcelain veneers. Int J Esthet Dent 2014;9:90-97.. Thus, additional studies need to be performed that vary the light source intensity and exposure times as well as the color and thickness of overlaying ceramic, to gain even further insights into these clinically important parameters. In addition, actual clinical studies using these variables need to be performed to place clinical relevance on the laboratory findings.
In summary, the results showed that the resin cement shade and the presence of a ceramic indirect restoration have a significant effect on the Knoop hardness of resin cement. Cement Knoop hardness significantly increases after 24 h in all cements shades, relative to immediate values of the light-curing (15 min). Cement Knoop hardness significantly decreased with depth (from 100 to 700 μm) for all cement shades and activation modes.
References
-
1Lawn, BR; Pajares, A; Zhang, Y; Deng, Y; Polack, MA; Lloyd, IK; et al.. Materials design in the performance of all-ceramic crowns. Biomaterials 2004;25:2885-2892.
-
2Groten, M; Pröbster, L. The influence of different cementation modes on the fracture resistance of feldspathic ceramic crowns. Int J Prosthodont 1997;10:169-177.
-
3Reges, RV; Moraes, RR; Correr, AB; Sinhoreti, MAC; Correr, Sobrinho, L; Piva, E; et al.. In-depth polymerization of dual-cured resin cement assessed by hardness. J Biomater Appl 2008;23:85-96.
-
4Pegoraro, TA; Silva, NRFA; Carvalho, RM. (2007) Cements for use in esthetic dentistry. Dent Clin North Am 2007;51:453-471.
-
5Janda, R; Roulet, JF; Latta, M; Rüttermann, S. Water sorption and solubility of contemporary resin-based filling materials. J Biomed Mater Res B Appl Biomater 2007;82:545-551.
-
6Dall’Magro, E; Sinhoreti, MA; Correr, AB; Consani, RL; Sicoli, EA; Mendonça, MJ; et al.. Effect of different modes of light modulation on the bond strength and Knoop hardness of a dental composite. Braz Dent J 2008;19:334-340.
-
7Blackman, R; Barghi, N; Duke, E. Influence of ceramic thickness on the polymerization of light-cured resin cement. J Prosthet Dent 1990;63:295-300.
-
8Jung, H; Friedl, KH; Hiller, KA; Haller, A; Schmalz, G. Curing efficiency of different polymerization methods through ceramic restorations. Clin Oral Investig 2001;5:156-161.
-
9Uctasli, S; Hasanreisoglu, U; Wilson, HJ. The attenuation of radiation by porcelain and its effect on polymerization of resin cements. J Oral Rehabil 1994;21:565-575.
-
10Pazin, MC; Moraes, RR; Gonçalves, LS; Borges, GA; Sinhoreti, MAC; CorrerSobrinho, L. Effects of ceramic thickness and curing unit on light transmission through leucite-reinforced material and polymerization of dual-cured luting agent. J Oral Sci 2008;50:131-136.
-
11Kilinc, E; Antonson, SA; Hardigan, PC; Kesercioglu, A. The effect of ceramic restoration shade and thickness on the polymerization of light- and dual-cure resin cements. Oper Dent 2011;36:661-669.
-
12Shortall, AC. How light source and product shade influence cure depth for a contemporary composite. J Oral Rehabil 2005;32:906-911.
-
13Reges, RV; Costa, AR; Correr, AB; Piva, E; Puppin-Rontani, RM; Sinhoreti, MAC; et al.. Effect of light-curing units, post-cured time and shade of resin cement on Knoop hardness. Braz Dent J 2009;20:410-413.
-
14Leloup, G; Holvoet, PE; Bebelman, S; Devaux, J. Raman scattering determination of the depth of cure of light-activated composites: influence of different clinically relevant parameters. J Oral Rehabil 2002;29:510-515.
-
15Guiraldo, RD; Consani, S; Consani, RLX; Berger, SB; Mendes, WB; Sinhoreti, MAC. Light energy transmission through composite influenced by material shades. Bull Tokyo Dent Coll 2009;50:183-190.
-
16Yan, YL; Kim, YK; Kim, K-H; Kwon, T-Y. Changes in degree of conversion and microhardness of dental resin cements. Oper Dent 2010;35:203-210.
-
17Watts, DC; McNaughton, V; Grant, AA. The development of surface hardness in visible light-cured posterior composites. J Dent 1986;14:169-174.
-
18Halvorson, RH; Erickson, RL; Davdson, CL. Energy dependent polymerization of resin-based composite. Dent Mater 2002;18:463-469.
-
19Schneider, LF; Moraes, RR; Cavalcante, LM; Sinhoreti, MA; CorrerSobrinho, L. Cross-link density evaluation through softening tests: effect of ethanol concentrations. Dent Mater 2008;24:199-203.
-
20Runnacles, P; Correr, GM; Baratto, F Filho; Gonzaga, CC; Furuse, AY. Degree of conversion of a resin cement light-cured through ceramic veneers of different thicknesses and types. Braz Dent J 2014;25:38-42.
-
21Lee, IB; Um, CM. Thermal analysis on the cure speed of dual cured resin cements under porcelain inlays. J Oral Rehabil 2001;28:186-197.
-
22AlShaafi, MM; AlQahtani, MQ; Price, RB. Effect of exposure time on the polymerization of resin cement through ceramic. J Adhes Dent 2014;16:129-135.
-
23Puppin-Rontani, RM; Dinelli, RG; de Paula, AB; Fucio, SB; Ambrosano, GM; Pascon, FM. In-depth polymerization of a self-adhesive dual-cured resin cement. Oper Dent 2012;37:188-194.
-
24Rueggeberg, F. Contemporary Issues in Photocuring. Compend Contin Educ Dent Suppl 1999;Supplement 25:4-15.
-
25Salameh, Z; Tehini, G; Ziadeh, N; Ragab, HA; Berberi, A; Aboushelib, MN. Influence of ceramic color and translucency on shade match of CAD/CAM porcelain veneers. Int J Esthet Dent 2014;9:90-97.
Publication Dates
-
Publication in this collection
Jan-Feb 2018
History
-
Received
17 Apr 2017 -
Accepted
02 Aug 2017


