Abstract
The aim of this paper is to systematically review the literature to estimate the overall prevalence of xerostomia/hyposalivation in epidemiological studies. An electronic search was carried out up to February 2018 with no language restrictions. A total of 5760 titles were screened and just twenty-nine papers were included in review and the meta-analysis after a two independently reviewers applied the selection criteria. Data were extracted from PubMed and Web of Science databases. Eligibility criteria included original investigations from observational population-based studies that reported the prevalence of xerostomia or data that allowed the calculation of prevalence of xerostomia and/or hyposalivation. Studies conducted in samples with specific health conditions, literature reviews, case reports and anthropological studies, as conferences or comments were excluded. Sample size, geographic location of the study, study design, age of the studied population, diagnosis methods, and evaluation criteria used to determine xerostomia e/or hyposalivation were extracted for meta-analysis and meta-regression. Multivariate meta-regression analysis was performed to explore heterogeneity among studies. The overall estimated prevalence of dry mouth was 22.0% (95%CI 17.0-26.0%). Higher prevalence of xerostomia was observed in studies conducted only with elderly people. Despite diverse approaches to the condition’s measurement, just over one in four people suffer from xerostomia, with higher rates observed among older people. Moreover, the measurement methods used currently may over- or underestimate xerostomia. These findings highlight the need for further work on existing and new clinical measure and will be useful to determine which one is more reliable in clinical and epidemiological perspectives.
Key Words:
xerostomia; dry mouth; hyposalivation; global prevalence; salivary function
Resumo
O objetivo do estudo é revisar sistematicamente a literatura afim de estimar a prevalência global de xerostomia/hiposalivação em estudos epidemiológicos. Uma busca eletrônica foi conduzida até Fevereiro de 2018 sem restrições de linguagem. Um total de 5760 títulos foram inicialmente identificados e somente vinte e nove artigos foram incluídos na revisão e meta-análise após dois revisores independentes aplicarem os critérios de seleção. Os artigos foram extraídos das bases de dados PubMed/Medline e Web of Science. Os critérios de elegibilidade incluíram investigações originais de estudos observacionais de base populacional os quais reportaram a prevalência de xerostomia ou dados que permitissem o cálculo da prevalência de xerostomia e/ou hiposalivação. Estudos realizados em populações com condições de saúde específicas, revisões de literatura, relato de casos e estudos antropológicos, assim como, conferências ou comentários foram excluídos. Tamanho amostral, localização geográfica aonde foi realizado o estudo, desenho do estudo, idade da população estudada, métodos de diagnóstico e o critério de avaliação para determiner xerostomia e/ou hiposalivação foram extraídos para a meta-análise e metaregressão. Análise de meta-regressão multípla foi realizada para explorar a heterogeneidade entre os estudos. A prevalência global estimada de boca seca foi de 22.0% (95%IC 17.0-26.0%). Uma maior prevalência de xerostomia foi observada em estudos realizados exclusivamente em populações idosas. Apesar de diferentes abordagens utilizadas para mensurar as condições de interesse, cerca de uma em quatro pessoas é acometida por xerostomia, com taxas mais elevadas sendo observadas na população idosa. Além disso, os métodos de mensuração podem ter super- ou subestimado os valores de xerostomia. Os achados do presente estudo salientam a necessidade de mais estudos acerca das existentes e novas formas de avaliação clínica, os quais serão úteis para determinar qual é a mais confiável para as perspectivas clínicas e epidemiológicas.
Introduction
Xerostomia and hyposalivation are two distinct and independent phenomena, which may manifest alone or in combination 11 Johansson AK1, Johansson A, Unell L, Ekbäck G, Ordell S, Carlsson GE. Self-reported dry mouth in Swedish population samples aged 50, 65 and 75 years. Gerodontology 2012;29:e107-e115.. Xerostomia is defined as the subjective sensation of dry mouth and it is diagnosed through self-report 22 Castrejon-Perez RC, Borges-Yáñez SA, Gutiérrez-Robledo LM, Ávila-Funes JA. Oral health conditions and frailty in Mexican community-dwelling elderly: a cross sectional analysis. BMC Public Health 2012;12:773.. On the other hand, hyposalivation refers to an objectively measured low salivary flow 33 Alaraudanjoki V, Laitala ML, Tjäderhane L, Pesonen P, Lussi A, Ronkainen J. Influence of Intrinsic Factors on Erosive Tooth Wear in a Large-Scale Epidemiological Study. Caries Res 2016;50:508-516.. Either dry mouth situations may negatively affect oral health-related quality of life 44 Thomson WM, Poulton R Broadbent, JM Al-Kubaisy S. Xerostomia and medications among 32-year-olds. Acta Odontol Scand 2006;64:249-254.,55 Benn AM, Broadbent JM, Thomson WM. Occurrence and impact of xerostomia among dentate adult New Zealanders: findings from a national survey. Aust Dent J 2015;60:362-367. and may cause oral health problems such as halitosis, impaired chewing and swallowing, and difficulties in prosthesis retention 66 Ichikawa K, Sakuma S, Yoshihara A, Miyazaki H, Funayama S, Ito K, et al. Relationships between the amount of saliva and medications in elderly individuals. Gerodontology 2011;28:116-120.. There is evidence that lower salivary flow increases the risk of dental caries, due to an absence of the physical cleaning action and buffering capacity of saliva 77 Iwasaki M, Yoshihara A, Ito K, Sato M, Minagawa K, Muramatsu K. Hyposalivation and dietary nutrient intake among community-based older Japanese. Geriatr Gerontol Int 2016;16:500-507.. This increasing risk is not exclusive of elderly and can occur in early age, specially in asthmatic patients under treatment.
Epidemiological studies of dry mouth situations from the last two decades have shown prevalence estimates ranging from 1% 88 Reichart PA. Oral mucosal lesions in a representative cross-sectional study of aging Germans. Community Dent Oral Epidemiol 2000;28:390-398. to 62% 11 Johansson AK1, Johansson A, Unell L, Ekbäck G, Ordell S, Carlsson GE. Self-reported dry mouth in Swedish population samples aged 50, 65 and 75 years. Gerodontology 2012;29:e107-e115.. The high variability in estimates has been attributed to variations in measurement methods, populations investigated, sample representativeness, study design, and the age of individuals evaluated 99 Thomson WM. Issues in the epidemiological investigation of dry mouth. Gerodontology. 2005;22:65-76.. Despite the research effort, much remains unanswered about the epidemiology of dry mouth. Even xerostomia that is measured through self-report 22 Castrejon-Perez RC, Borges-Yáñez SA, Gutiérrez-Robledo LM, Ávila-Funes JA. Oral health conditions and frailty in Mexican community-dwelling elderly: a cross sectional analysis. BMC Public Health 2012;12:773.,1010 Gilbert GH, Heft MW, Duncan RP. Mouth dryness as reported by older Floridians. Community Dent Oral Epidemiol 1993;21:390-397., there are methodological differences, whereby some studies report only the presence or absence of dry mouth 77 Iwasaki M, Yoshihara A, Ito K, Sato M, Minagawa K, Muramatsu K. Hyposalivation and dietary nutrient intake among community-based older Japanese. Geriatr Gerontol Int 2016;16:500-507.,1111 Hochberg MC, Tielsch J, Munoz B, Bandeen-Roche K, West SK, Schein OD. Prevalence of symptoms of dry mouth and their relationship to saliva production in community dwelling elderly: the SEE project. Salisbury Eye Evaluation. J Rheumatol 1998;25:486-491.,1212 Jacobsson LT, Axell TE, Hansen BU, Henricsson VJ, Lieberkind K, Lilja B, et al. Dry eyes or mouth - an epidemiological study in Swedish adults, with special reference to primary Sjogren’s syndrome. J Autoimmun 1989; 2:521-527. and others investigate the frequency of such a sensation 55 Benn AM, Broadbent JM, Thomson WM. Occurrence and impact of xerostomia among dentate adult New Zealanders: findings from a national survey. Aust Dent J 2015;60:362-367.,1313 Anttila SS, Knuuttila ML, Sakki TK. Depressive symptoms as an underlying factor of the sensation of dry mouth. Psychosom Med 1998;60:215-218.,1414 Ekback G; Astrom AN; Klock K; Ordell S; Unell L. Variation in subjective oral health indicators of 65-year-olds in Norway and Sweden. Acta Odontol Scand 2009;67:222-232.. New approaches use scales, such as the Xerostomia Inventory (XI) developed and tested by Thomson et al. 1515 Thomson WM; Chalmers JM; Spencer AJ; Ketabi M. The occurrence of xerostomia and salivary gland hypofunction in a population-based sample of older South Australians. Spec Care Dentist 1999;19:20-23., which includes a battery of seven xerostomia questions used by Locker 1616 Locker, D. Dental status, xerostomia and the oral health-related quality of life of an elderly institutionalized population. Spec Care Dent 2003 23:86-93. or a nine-item battery of questions on dry mouth-related symptoms and behaviors 1717 So JS, Chung SC, Kho HS; Kim YK; Chung JW. Dry mouth among the elderly in Korea: a survey of prevalence, severity, and associated factors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:475-483..
Hyposalivation is diagnosed through the assessment of salivary flow, which may be evaluated by collecting the fluid from individual salivary glands (or pairs of glands) and; also, total salivary flow may be evaluated by collecting whole saliva. The latter method is more common 99 Thomson WM. Issues in the epidemiological investigation of dry mouth. Gerodontology. 2005;22:65-76.. However, there is a lack of consensus in the literature about which salivary flow rate indicates hyposalivation, ranging from less than 0.1mL/min unstimulated saliva 1515 Thomson WM; Chalmers JM; Spencer AJ; Ketabi M. The occurrence of xerostomia and salivary gland hypofunction in a population-based sample of older South Australians. Spec Care Dentist 1999;19:20-23. to 0.8 mL/min stimulated saliva 1818 Narhi TO Ainamo, A; Meurman, JH. Salivary yeasts, saliva, and oral mucosa in the elderly. J Dent Res 1993;72:1009-1014..
There is evidence of health conditions and risk behavior being determinants of xerostomia and hyposalivation. Increasing age has been reported as a risk marker for xerostomia 1111 Hochberg MC, Tielsch J, Munoz B, Bandeen-Roche K, West SK, Schein OD. Prevalence of symptoms of dry mouth and their relationship to saliva production in community dwelling elderly: the SEE project. Salisbury Eye Evaluation. J Rheumatol 1998;25:486-491.,1919 Kongstad, J; Ekstrand, K; Qvist, V; Christensen, LB; Cortsen, B; Gronbaek, M; et al. Findings from the oral health study of the Danish Health Examination Survey 2007-2008. Acta Odontol Scand 2013;71:1560-1569.. Chronic diseases such as diabetes, autoimmune diseases, especially Sjögren’s Syndrome 1212 Jacobsson LT, Axell TE, Hansen BU, Henricsson VJ, Lieberkind K, Lilja B, et al. Dry eyes or mouth - an epidemiological study in Swedish adults, with special reference to primary Sjogren’s syndrome. J Autoimmun 1989; 2:521-527., and polypharmacy 1010 Gilbert GH, Heft MW, Duncan RP. Mouth dryness as reported by older Floridians. Community Dent Oral Epidemiol 1993;21:390-397.,2020 Osterberg, T; Birkhed, D; Johansson, C; Svanborg, A. Longitudinal study of stimulated whole saliva in an elderly population. Scand J Dent Res 1992;100:340-345.,2121 Thomson WM. Subjective Aspects of Dry Mouth, in: Carpenter, Guy. (Ed.), Dry Mouth. A Clinical Guide on Causes, Effects and Treatments. 2015. Springer, Heidelberg, pp 103-115. are recognized as major dry mouth associations. Not only polypharmacy, but specific medicines favor the occurrence of xerostomia and hyposalivation, especially inhaled antiastmatic drugs 2222 Ryberg, M; Moller, C; Ericson, T. Saliva composition and caries development in asthmatic patients treated with beta-2 adrenoceptor agonists: A 4-year follow-up study. Scand J Dent Res 1991; 99:212-8.. The action of such medicines, even in early ages can significantly affect salivary flow. Considering the widespread occurrence of asthma since childhood 2323 Global Global Initiative for Asthma (GINA), Global Strategy for Asthma Management and Prevention. 2017. and the impact of its therapy in dry mouth, the effects of it therapy in a long-term are not clear and it must be considered in all ages as well.
A previous systematic review evaluating the prevalence of xerostomia in population samples was published in 2006 2424 Orellana, MF; Lagravere, MO; Boychuk, DG; et al. Prevalence of xerostomia in population-based samples: a systematic review. J Public Health Dent 2006,66;152-158.. However, that study included only estimates for xerostomia. Moreover, the study did not use a meta-analysis, so it was unable to obtain an overall prevalence estimate for xerostomia. Many epidemiological studies on dry mouth have been published since then.
This paper presents a systematic review of the literature on the prevalence of xerostomia and hyposalivation in order to obtain a global combined prevalence estimate for dry mouth, and to determine the factors behind the considerable variability in prevalence estimates.
Material and Methods
This systematic review was organized using the PRISMA statement and it was based on the following review question: “What is the estimated worldwide prevalence of xerostomia/hyposalivation?”
Eligibility Criteria
Original investigations from observational studies that reported the prevalence of xerostomia were included. Only population-based studies with representative samples, according to the Critical Appraisal Checklist for prevalence studies recommended by the Joanna Briggs Institute, were considered for this review. As a qualifying condition, all selected studies should have clearly reported the prevalence of xerostomia and/or hyposalivation or have included data allowing its calculation.
Studies conducted in samples with specific health conditions (asthma, cancer, depression, paralysis, syndromes - including Sjögren’s Syndrome, and similar convenience samples) were excluded, as were literature reviews, case-control studies, retrospective studies, case reports, anthropological studies, in vitro and in situ studies, and comments or conference abstracts. Articles in other languages than English, Spanish, Portuguese, French or German were excluded.
Search Strategy
An electronic search was performed in the PubMed and Web of Science databases, with no initial date and language restrictions. Keywords included the following MeSH and free terms: (Xerostomia(Mesh)) OR (Xerostomia (all)) OR (Dry Mouth(all)) OR (Mouth Dryness(all)) OR (Hyposalivation(all)) AND Epidemiologic Studies(Mesh)) AND (Cross-Sectional Studies(Mesh)) AND (Longitudinal Studies(Mesh)) AND (Cohort Studies(Mesh)), which are presented in Table 1 in several combinations.
Reports were managed using the EndNote X7.4 software (Thomson Reuters, New York, NY, USA). Duplicate reports were excluded. Two reviewers (GOC and ERS) independently screened titles and abstracts, based on the aforementioned criteria. The screened lists were compared and differences were discussed and resolved by consensus. If there was no consensus, a third examiner was asked to decide on the inclusion or exclusion of the study. The same two reviewers also screened full text manuscripts. Reference lists from the eligible papers were reviewed according to the eligibility criteria. Gray Literature was not screened.
Critical Appraisal
The Critical Appraisal Checklist for prevalence and incidence studies recommended by the Joanna Briggs Institute was employed. The same reviewers independently evaluated each study and answered ‘Yes’, ‘No’, or ‘Unclear’ for each of the 9 items of the instrument. Disagreements were resolved by reaching consensus through discussion.
Data Extraction and Data Analysis
Information extracted from the studies included sample size, geographic location, study design, age of the studied population, diagnosis methods, and evaluation criteria used to define xerostomia and/or hyposalivation. Prevalence rates for xerostomia/hyposalivation were also collected (or calculated, if necessary). In case of missing data, the authors were contacted up by e-mail. When more than one method for measuring dry mouth was employed, prevalence rate of hyposalivation was included in the meta-analysis for dry mouth. Prevalence rates were categorized according to the age of the participants (adults or elders), when more than one available, the highest was used; however, when such information was not available, studies were grouped into mixed population (adults and elders). Considering that cohort studies could showed prevalences of xerostomia or hyposalivation in more than 1 time, it was established the use of the most recent values of prevalences.
The estimated global prevalence of dry mouth was calculated using fixed- and random-effect models. When heterogeneity was present (I2>50% or chi-square p value<0.05), the random-effect model was favored 2525 DerSimonian, R; Laird, N. Meta-analysis in clinical trials, Control Clin Trials 1986;7:177-188.. The same criteria were adopted for individual meta-analysis of xerostomia and hyposalivation information of each study. Additionally, meta-regression and subgroup analyses were conducted to investigate sources of between-study variability for each criterion. Characteristics were included in a multivariate meta-regression model. Variable selection was performed using the backward stepwise approach. Variables with p value<0.20 remained in the final model, but only those with p value<0.05 were considered significant in the final adjusted model. Explained heterogeneity was obtained from the adjusted R2 of the final model. Subgroup analysis was also conducted for each methodological variable included in the final meta-regression model. Sensitivity analyses were conducted to estimate the influence of each study on the pooled results. Funnel plot and the Egger test were used to test for any potential publication bias 1717 So JS, Chung SC, Kho HS; Kim YK; Chung JW. Dry mouth among the elderly in Korea: a survey of prevalence, severity, and associated factors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:475-483.. All analyses were performed using the Stata 14.1 software (StataCorp, College Station, TX, USA).
Results
Electronic searches revealed 5760 studies. From those, 1346 were excluded for being duplicates. A total of 4414 articles were submitted to title and abstract screening and 114 of them remained for full-text evaluation, from which 85 were excluded after appraisal (Fig. 1, Table 2). A total of 29 articles met the inclusion criteria, among these articles, 26 reported the prevalence of xerostomia or data on it and 14 reported the prevalence of hyposalivation or data on it. One study was included twice in the meta-analysis, because it presented separate data for different populations under study 1414 Ekback G; Astrom AN; Klock K; Ordell S; Unell L. Variation in subjective oral health indicators of 65-year-olds in Norway and Sweden. Acta Odontol Scand 2009;67:222-232..

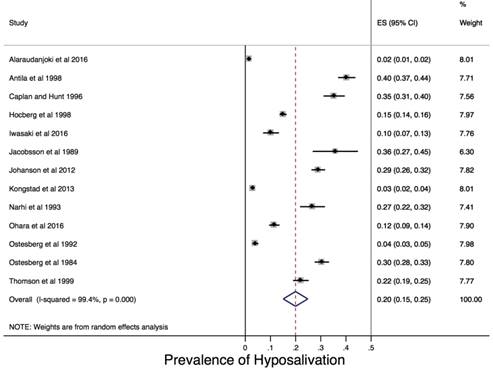
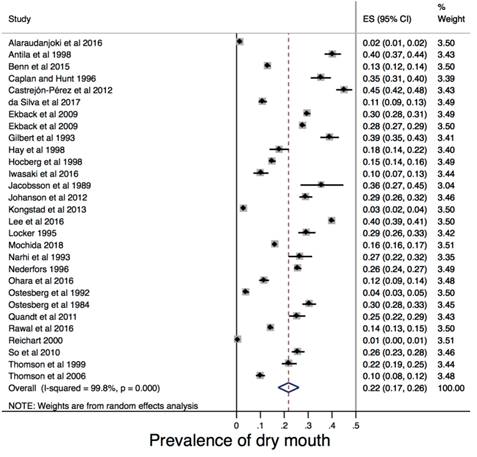
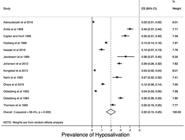
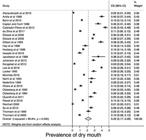
The overall prevalence of xerostomia was estimated to be 23.0% (95%CI 18.0-28.0%), with high heterogeneity among studies (I2 99.8%; chi square p value<0.001; Fig. 2). The overall prevalence of hyposalivation was estimated to be 20.0% (95%CI 15.0 - 25.0%) with high heterogeneity among studies (I2 99.4%; chi square p value<0.001; Fig. 3). The overall prevalence of dry mouth (xerostomia or hyposalivation) was estimated to be 22.0% (95%CI 17.0-26.0%), also with high heterogeneity among studies (I2 99.8%; chi square p-value<0.001; Fig. 4).

The final meta-regression analysis explained about 16% of the between-study variability.
Table 3 presents the main characteristics of the included studies. Some studies presented weaknesses under critical appraisal (Table 4), as follows: two studies 1212 Jacobsson LT, Axell TE, Hansen BU, Henricsson VJ, Lieberkind K, Lilja B, et al. Dry eyes or mouth - an epidemiological study in Swedish adults, with special reference to primary Sjogren’s syndrome. J Autoimmun 1989; 2:521-527.,2626 Hay, EM, Thomas, E; Pal, B; Hajeer, A; Chambers, H; Silman, AJ. Weak association between subjective symptoms or and objective testing for dry eyes and dry mouth: results from a population based study. Ann Rheum Dis 1998;57:20-24. did not use an adequate sample frame for the target population, two studies 77 Iwasaki M, Yoshihara A, Ito K, Sato M, Minagawa K, Muramatsu K. Hyposalivation and dietary nutrient intake among community-based older Japanese. Geriatr Gerontol Int 2016;16:500-507.,2727 Ohara, Y; Hirano, H; Yoshida, H. Prevalence and factors associated with xerostomia and hyposalivation among community-dwelling older people in Japan. Gerodontology 2016;33:20-27. did not have an adequate sample size or were unclear, one study 33 Alaraudanjoki V, Laitala ML, Tjäderhane L, Pesonen P, Lussi A, Ronkainen J. Influence of Intrinsic Factors on Erosive Tooth Wear in a Large-Scale Epidemiological Study. Caries Res 2016;50:508-516. did not describe their participants and the setting in detail, one study 2828 Caplan, DJ; Hunt, RJ. Salivary flow and risk of tooth loss in an elderly population. Community Dent Oral Epidemiol 1996;24:68-71. did not conduct the data analysis with sufficient coverage of the identified sample did not avoid coverage bias in data analysis, one study 1212 Jacobsson LT, Axell TE, Hansen BU, Henricsson VJ, Lieberkind K, Lilja B, et al. Dry eyes or mouth - an epidemiological study in Swedish adults, with special reference to primary Sjogren’s syndrome. J Autoimmun 1989; 2:521-527. did not use an appropriate statistical analysis, and one study 77 Iwasaki M, Yoshihara A, Ito K, Sato M, Minagawa K, Muramatsu K. Hyposalivation and dietary nutrient intake among community-based older Japanese. Geriatr Gerontol Int 2016;16:500-507. did not have a sufficient participation rate.
Tables 5 and 6 shows the subgroup analysis according to the variables retained in the final adjusted meta-regression models. A higher prevalence estimate for dry mouth was noted in studies conducted with older people only and in studies conduceted in Americas (Table 5). Table 6 presents overall prevalence estimates for xerostomia and hyposalivation separately. Considerating age group, the higher prevalence values were 27.2% for xerostomia in studies conducted with older people only; and 26.0% for hyposalivation in studies considering adults people only. The heterogeneity of the studies for each outcome was higher than 99.0%.
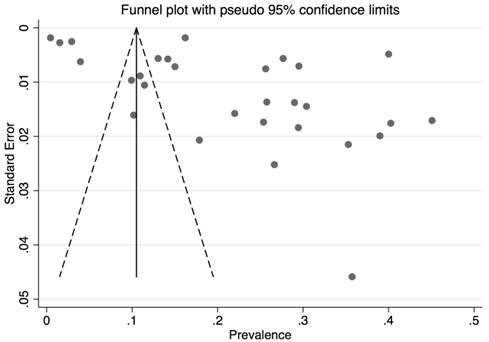
The Egger test revealed the presence of publication bias (p-value=0.007), which was confirmed by the metafunnel analysis (Fig. 5). Sensitivity analysis demonstrated that the omission of any study would not significantly modify the estimated prevalence of dry mouth (Fig. 6).


Estimated prevalence of dry mouth and confidence interval with random effect after the omission of the study.
Discussion
This meta-analysis of findings from epidemiological studies on dry mouth has found the overall estimated prevalence of dry-mouth from population-based studies tov be 22.0% (95%CI 17.0-26.0). Xerostomia and hyposalivation are two phenomena that may negatively affect the oral health of individuals and their quality of life 44 Thomson WM, Poulton R Broadbent, JM Al-Kubaisy S. Xerostomia and medications among 32-year-olds. Acta Odontol Scand 2006;64:249-254.,55 Benn AM, Broadbent JM, Thomson WM. Occurrence and impact of xerostomia among dentate adult New Zealanders: findings from a national survey. Aust Dent J 2015;60:362-367.,1313 Anttila SS, Knuuttila ML, Sakki TK. Depressive symptoms as an underlying factor of the sensation of dry mouth. Psychosom Med 1998;60:215-218.. Dry mouth impairs oral function, chewing, and swallowing 2929 Lee, YS; Kim, HG; Moreno, K. Xerostomia among older adults with low income: nuisance or warning? J Nurs Scholarsh 2016;48:58-65.. Considering oral diseases, evidences from different study designs researches highlight the impact of salivary problems in caries experience 3030 Ranganath, L; Shet, R; Rajesh, A; Saliva: a powerful diagnostic tool for minimal intervention dentistry. J Contemp Dent Pract 2012;13:240-245.,3131 Mazzoleni, S; Stellini, E; Cavaleri, E; Angelova Volponi, A; Ferro, R; Fochesato Colombani, S. Dental caries in children with asthma undergoing treatment with short-acting beta2-agonists. Eur J Paediatr Dent 2008;9:132-138.. Moreover, a recent study showed that dry mouth could influence the occurrence of halitosis and consequently affect oral health-related quality of life 3232 Silva, MF; Leite, FRM; Ferreira, LB; Pola, NM; Scannapieco FA; Demarco FF, et al. Estimated prevalence of halitosis: a systematic review and meta-regression analysis. Clin Oral Invest 2018;2247-55.. Besides oral manifestations, these problems may result in more general effects, including loss of appetite, malnutrition, impaired interpersonal communication and social interactions, and perhaps even depression, thereby negatively affecting the daily lives of sufferers 44 Thomson WM, Poulton R Broadbent, JM Al-Kubaisy S. Xerostomia and medications among 32-year-olds. Acta Odontol Scand 2006;64:249-254.,55 Benn AM, Broadbent JM, Thomson WM. Occurrence and impact of xerostomia among dentate adult New Zealanders: findings from a national survey. Aust Dent J 2015;60:362-367..
When only xerostomia was considered the overall prevalence in the studies considered in this review ranged from 0.01% 88 Reichart PA. Oral mucosal lesions in a representative cross-sectional study of aging Germans. Community Dent Oral Epidemiol 2000;28:390-398. to 45% 22 Castrejon-Perez RC, Borges-Yáñez SA, Gutiérrez-Robledo LM, Ávila-Funes JA. Oral health conditions and frailty in Mexican community-dwelling elderly: a cross sectional analysis. BMC Public Health 2012;12:773.. For hyposalivation, the prevalence rate ranged from 0.02% 33 Alaraudanjoki V, Laitala ML, Tjäderhane L, Pesonen P, Lussi A, Ronkainen J. Influence of Intrinsic Factors on Erosive Tooth Wear in a Large-Scale Epidemiological Study. Caries Res 2016;50:508-516. to 40% 1313 Anttila SS, Knuuttila ML, Sakki TK. Depressive symptoms as an underlying factor of the sensation of dry mouth. Psychosom Med 1998;60:215-218.. For both situations, ageing seems to be determinant of its occurrence, studies have shown what appears to be an increase in the prevalence of dry mouth with increasing age. Diverse factors have been investigated to clarify the potential association of age with such oral conditions. However, most studies were conducted in samples of older people and no population-based studies were conducted in children or adolescents sample. Moreover, a few studies conducted in both populations of young adults and older adults have found prevalence differences between them. Thomson et al. 1515 Thomson WM; Chalmers JM; Spencer AJ; Ketabi M. The occurrence of xerostomia and salivary gland hypofunction in a population-based sample of older South Australians. Spec Care Dentist 1999;19:20-23. found a prevalence of 20% of xerostomia in an older population and 10% in an adult population 44 Thomson WM, Poulton R Broadbent, JM Al-Kubaisy S. Xerostomia and medications among 32-year-olds. Acta Odontol Scand 2006;64:249-254.. Similar findings were observed by Benn et al. 55 Benn AM, Broadbent JM, Thomson WM. Occurrence and impact of xerostomia among dentate adult New Zealanders: findings from a national survey. Aust Dent J 2015;60:362-367. in a nationally representative sample, in which the prevalence of xerostomia was 5% in the 18-24 age group and 26% in those aged 75 years or older, but there was not a consistent age gradient. These findings provide further evidence that xerostomia, even in divergent proportions, could not affect only older people, and that perhaps the lack of knowledge of its occurrence by young adults is because younger age groups have become aware of it only over the last decade or so. Hence, it is difficult to establish age-standardized population prevalences of dry mouth and what kind factors really modify salivary conditions in young population.
There is evidence that the association with age is not just due to the aging process itself. Aging is associated with increases in comorbid chronic medical conditions, which consequently increases the use of medications. Many of the drugs taken are associated with lower salivary flow 1010 Gilbert GH, Heft MW, Duncan RP. Mouth dryness as reported by older Floridians. Community Dent Oral Epidemiol 1993;21:390-397.,1111 Hochberg MC, Tielsch J, Munoz B, Bandeen-Roche K, West SK, Schein OD. Prevalence of symptoms of dry mouth and their relationship to saliva production in community dwelling elderly: the SEE project. Salisbury Eye Evaluation. J Rheumatol 1998;25:486-491.,1717 So JS, Chung SC, Kho HS; Kim YK; Chung JW. Dry mouth among the elderly in Korea: a survey of prevalence, severity, and associated factors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:475-483.,2727 Ohara, Y; Hirano, H; Yoshida, H. Prevalence and factors associated with xerostomia and hyposalivation among community-dwelling older people in Japan. Gerodontology 2016;33:20-27.,3333 Locker, D, Xerostomia in older adults: a longitudinal study. Gerodontology1995;12:18-25.. In this context, an interesting observation was the association between the number of medications taken and the prevalence of xerostomia (34-36). The prevalence of xerostomia is usually higher in individuals who take more than one medication 44 Thomson WM, Poulton R Broadbent, JM Al-Kubaisy S. Xerostomia and medications among 32-year-olds. Acta Odontol Scand 2006;64:249-254.,3737 Nederfors,T; Isaksson, R; Mornstad, H; et al. Prevalence of perceived symptoms of dry mouth in an adult Swedish population-relation to age, sex and pharmacotherapy. Community Dent Oral Epidemiol1997;25: 211-216.. Factors such as changes in saliva quality, underlying diseases, and medications should be considered as the cause of higher subjective perception of dry mouth with aging 1616 Locker, D. Dental status, xerostomia and the oral health-related quality of life of an elderly institutionalized population. Spec Care Dent 2003 23:86-93.. Not only polypharmacy but specific drugs present salivary flow and quality adverse effects. Antiasthmatic drugs were suggested as the main mediator of high risk of dental caries in asthmatic children and adolescent due to its high impact on salivary conditions. Even few months using inhaled β2-agonist and corticosteroids could decrease significantly the salivary flow rate, increase dental plaque index, and decrease salivary pH 3838 Tootla, R; Toumba, KJ; Duggal, MS. An evaluation of the acidogenic potential of asthma inhalers. Arch Oral Biol 2004;49:275-283.,3939 Sag, C; Ozden, FO; Acikgoz G. The effects of combination treatment with a long-acting b2-agonist and a corticosteroid on salivary flow rate, secretory immunoglobulin A, and oral health in children and adolescents with moderate asthma: a 1-month, single-blind clinical study. Clin Ther 2007;29:2236-2242.,4040 Osterberg, T; Landahl, S; Hedegard, B. Salivary flow, saliva, pH and buffering capacity in 70-year-old men and women. Correlation to dental health, dryness in the mouth, disease and drug treatment. J Oral Rehabil 1984;11:157-170., all of these consequences favor dental caries. Finally, the long-term effect of this group of medicines in salivary aspects is not known, and identify asthmatic population that used inhaled medicines in the past could be an alternative to understand life-course effects of medication on salivary flow rate.
This study has several strengths that should be considered. The first one is the inclusion of population-based studies only, excluding studies that investigated clinical or other biased samples, then the common occurrence of dry mouth in general population could be evaluated. Secondly, the analytical approach used, including the meta-analysis, allowed estimating the global prevalence of xerostomia. Such methodology has already been used to estimate the global prevalence of halitosis 3232 Silva, MF; Leite, FRM; Ferreira, LB; Pola, NM; Scannapieco FA; Demarco FF, et al. Estimated prevalence of halitosis: a systematic review and meta-regression analysis. Clin Oral Invest 2018;2247-55. and its use here by regarding dry mouth highlights the importance of the approach for obtaining global estimates of the impact of major oral conditions. The high heterogeneity found in all meta-regressions conducted evidence the lack of a standard criteria for population-based studies aiming to assess salivary conditions. However, we used meta-regression as a tool to explain heterogeneity in prevalence among studies. Although there was no statistical association, a considerable amount of heterogeneity were explained after considering age-groups and geographic location of the studies as potential sources of heterogeneity. Finally, the studies included showed high quality, since just six studies of all included do not fulfill all items as “yes” in the JBI critical appraisal checklist.
Besides the strengths stated, our findings should be interpreted with caution. Firstly, the Egger test and the funnel plot revealed publication bias, although the main databases for the outcome had been searched and an extensive search had been conducted this could suggest a lack of information of unpublished studies or grey literature. Even though, a great variety of studies were screened (4,414 articles). Moreover, the chosen databases included the main peer reviewed journals of the field and probably all high-quality population-based salivary studies were included in our research. Secondly, even adopting strategies to collect detailed information of all studies, as send e-mail to authors, eight potential articles were excluded due not provide prevalence data, and it is not clear their influence on the overall result. Moreover, language restriction was applied and some specific countries prevalences were not considered, but only three articles were excluded by such reason, being in Hebrew, Chinese and Hungarian. Finally, we cannot fully explain the heterogeneity found based on the included variables. Hence we encourage the development of further studies addressing other potential sources of heterogeneity in salivary research.
The studies included were conducted mostly in high-income countries, except for one study in Mexico. Considering that the occurrence of chronic diseases and aging are rather socially determined, and social inequality manifests differently and perhaps more acutely in poorer countries, it is possible that the overall dry mouth prevalence estimate may have been different had more data from those countries been available. It is also important to emphasize the need for more information from prospective cohort studies, including from younger populations 3434 Rawal Hoffman, HJ; Bainbridge, KE. Prevalence and Risk Factors of Self-Reported Smell and Taste Alterations: Results from the 2011-2012 US National Health and Nutrition Examination Survey (NHANES). Chem Senses 2016;41,69-76. and consider the high presence of specific chronic diseases, such asthma that could influence xerostomia through medicines, in order to better understand the history of dry mouth and its effects 99 Thomson WM. Issues in the epidemiological investigation of dry mouth. Gerodontology. 2005;22:65-76..
Another important factor to consider is that the estimated prevalence rate highly depends on the method used to measure dry mouth. Xerostomia is not necessarily accompanied by lower salivary flow rate 77 Iwasaki M, Yoshihara A, Ito K, Sato M, Minagawa K, Muramatsu K. Hyposalivation and dietary nutrient intake among community-based older Japanese. Geriatr Gerontol Int 2016;16:500-507.,1010 Gilbert GH, Heft MW, Duncan RP. Mouth dryness as reported by older Floridians. Community Dent Oral Epidemiol 1993;21:390-397.,1313 Anttila SS, Knuuttila ML, Sakki TK. Depressive symptoms as an underlying factor of the sensation of dry mouth. Psychosom Med 1998;60:215-218.. In this context, Thomson et al. 1515 Thomson WM; Chalmers JM; Spencer AJ; Ketabi M. The occurrence of xerostomia and salivary gland hypofunction in a population-based sample of older South Australians. Spec Care Dentist 1999;19:20-23. reported that xerostomia and hyposalivation occurred together in only 6% of their overall sample, and that this was equivalent to only one in six of the 36% of individuals who had either condition. The measurement methods used may over- or underestimate xerostomia, a fact widely discussed by Thomson et al. 2121 Thomson WM. Subjective Aspects of Dry Mouth, in: Carpenter, Guy. (Ed.), Dry Mouth. A Clinical Guide on Causes, Effects and Treatments. 2015. Springer, Heidelberg, pp 103-115.. These findings emphasize the need for further work on existing and new clinical measures, including the most recent ones working with scales for epidemiological use to measure the prevalence of xerostomia. Alternatively, researchers may be required to reach a consensus on which of the many currently available measures should be used.
There is still much to find out about dry mouth and its associations 4141 Mochid,a Y; Yamamoto, T; Fuchida, S; Aida, J; Kondo, K. Does poor oral Health status increase the risk of falls?: The JAGES project longitudinal study. Plos One2018;13:e0192251.. Despite diverse approaches to the condition’s measurement, just over one in four people in adult age or older suffer from xerostomia, with higher rates observed among elderly.
References
-
1Johansson AK1, Johansson A, Unell L, Ekbäck G, Ordell S, Carlsson GE. Self-reported dry mouth in Swedish population samples aged 50, 65 and 75 years. Gerodontology 2012;29:e107-e115.
-
2Castrejon-Perez RC, Borges-Yáñez SA, Gutiérrez-Robledo LM, Ávila-Funes JA. Oral health conditions and frailty in Mexican community-dwelling elderly: a cross sectional analysis. BMC Public Health 2012;12:773.
-
3Alaraudanjoki V, Laitala ML, Tjäderhane L, Pesonen P, Lussi A, Ronkainen J. Influence of Intrinsic Factors on Erosive Tooth Wear in a Large-Scale Epidemiological Study. Caries Res 2016;50:508-516.
-
4Thomson WM, Poulton R Broadbent, JM Al-Kubaisy S. Xerostomia and medications among 32-year-olds. Acta Odontol Scand 2006;64:249-254.
-
5Benn AM, Broadbent JM, Thomson WM. Occurrence and impact of xerostomia among dentate adult New Zealanders: findings from a national survey. Aust Dent J 2015;60:362-367.
-
6Ichikawa K, Sakuma S, Yoshihara A, Miyazaki H, Funayama S, Ito K, et al. Relationships between the amount of saliva and medications in elderly individuals. Gerodontology 2011;28:116-120.
-
7Iwasaki M, Yoshihara A, Ito K, Sato M, Minagawa K, Muramatsu K. Hyposalivation and dietary nutrient intake among community-based older Japanese. Geriatr Gerontol Int 2016;16:500-507.
-
8Reichart PA. Oral mucosal lesions in a representative cross-sectional study of aging Germans. Community Dent Oral Epidemiol 2000;28:390-398.
-
9Thomson WM. Issues in the epidemiological investigation of dry mouth. Gerodontology. 2005;22:65-76.
-
10Gilbert GH, Heft MW, Duncan RP. Mouth dryness as reported by older Floridians. Community Dent Oral Epidemiol 1993;21:390-397.
-
11Hochberg MC, Tielsch J, Munoz B, Bandeen-Roche K, West SK, Schein OD. Prevalence of symptoms of dry mouth and their relationship to saliva production in community dwelling elderly: the SEE project. Salisbury Eye Evaluation. J Rheumatol 1998;25:486-491.
-
12Jacobsson LT, Axell TE, Hansen BU, Henricsson VJ, Lieberkind K, Lilja B, et al. Dry eyes or mouth - an epidemiological study in Swedish adults, with special reference to primary Sjogren’s syndrome. J Autoimmun 1989; 2:521-527.
-
13Anttila SS, Knuuttila ML, Sakki TK. Depressive symptoms as an underlying factor of the sensation of dry mouth. Psychosom Med 1998;60:215-218.
-
14Ekback G; Astrom AN; Klock K; Ordell S; Unell L. Variation in subjective oral health indicators of 65-year-olds in Norway and Sweden. Acta Odontol Scand 2009;67:222-232.
-
15Thomson WM; Chalmers JM; Spencer AJ; Ketabi M. The occurrence of xerostomia and salivary gland hypofunction in a population-based sample of older South Australians. Spec Care Dentist 1999;19:20-23.
-
16Locker, D. Dental status, xerostomia and the oral health-related quality of life of an elderly institutionalized population. Spec Care Dent 2003 23:86-93.
-
17So JS, Chung SC, Kho HS; Kim YK; Chung JW. Dry mouth among the elderly in Korea: a survey of prevalence, severity, and associated factors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:475-483.
-
18Narhi TO Ainamo, A; Meurman, JH. Salivary yeasts, saliva, and oral mucosa in the elderly. J Dent Res 1993;72:1009-1014.
-
19Kongstad, J; Ekstrand, K; Qvist, V; Christensen, LB; Cortsen, B; Gronbaek, M; et al. Findings from the oral health study of the Danish Health Examination Survey 2007-2008. Acta Odontol Scand 2013;71:1560-1569.
-
20Osterberg, T; Birkhed, D; Johansson, C; Svanborg, A. Longitudinal study of stimulated whole saliva in an elderly population. Scand J Dent Res 1992;100:340-345.
-
21Thomson WM. Subjective Aspects of Dry Mouth, in: Carpenter, Guy. (Ed.), Dry Mouth. A Clinical Guide on Causes, Effects and Treatments. 2015. Springer, Heidelberg, pp 103-115.
-
22Ryberg, M; Moller, C; Ericson, T. Saliva composition and caries development in asthmatic patients treated with beta-2 adrenoceptor agonists: A 4-year follow-up study. Scand J Dent Res 1991; 99:212-8.
-
23Global Global Initiative for Asthma (GINA), Global Strategy for Asthma Management and Prevention. 2017.
-
24Orellana, MF; Lagravere, MO; Boychuk, DG; et al. Prevalence of xerostomia in population-based samples: a systematic review. J Public Health Dent 2006,66;152-158.
-
25DerSimonian, R; Laird, N. Meta-analysis in clinical trials, Control Clin Trials 1986;7:177-188.
-
26Hay, EM, Thomas, E; Pal, B; Hajeer, A; Chambers, H; Silman, AJ. Weak association between subjective symptoms or and objective testing for dry eyes and dry mouth: results from a population based study. Ann Rheum Dis 1998;57:20-24.
-
27Ohara, Y; Hirano, H; Yoshida, H. Prevalence and factors associated with xerostomia and hyposalivation among community-dwelling older people in Japan. Gerodontology 2016;33:20-27.
-
28Caplan, DJ; Hunt, RJ. Salivary flow and risk of tooth loss in an elderly population. Community Dent Oral Epidemiol 1996;24:68-71.
-
29Lee, YS; Kim, HG; Moreno, K. Xerostomia among older adults with low income: nuisance or warning? J Nurs Scholarsh 2016;48:58-65.
-
30Ranganath, L; Shet, R; Rajesh, A; Saliva: a powerful diagnostic tool for minimal intervention dentistry. J Contemp Dent Pract 2012;13:240-245.
-
31Mazzoleni, S; Stellini, E; Cavaleri, E; Angelova Volponi, A; Ferro, R; Fochesato Colombani, S. Dental caries in children with asthma undergoing treatment with short-acting beta2-agonists. Eur J Paediatr Dent 2008;9:132-138.
-
32Silva, MF; Leite, FRM; Ferreira, LB; Pola, NM; Scannapieco FA; Demarco FF, et al. Estimated prevalence of halitosis: a systematic review and meta-regression analysis. Clin Oral Invest 2018;2247-55.
-
33Locker, D, Xerostomia in older adults: a longitudinal study. Gerodontology1995;12:18-25.
-
34Rawal Hoffman, HJ; Bainbridge, KE. Prevalence and Risk Factors of Self-Reported Smell and Taste Alterations: Results from the 2011-2012 US National Health and Nutrition Examination Survey (NHANES). Chem Senses 2016;41,69-76.
-
35da Silva, L; Kupek ,E; Peres, KG. General health influences episodes of xerostomia: a prospective population-based study. Community Dent Oral Epidemiol 2017;45:153-159.
-
36Quandt, SA; Savoca, MR; Leng, X; et al. Dry mouth and dietary quality in older adults in North Carolina. J Am Geriatr Soc 2011;59:439-445.
-
37Nederfors,T; Isaksson, R; Mornstad, H; et al. Prevalence of perceived symptoms of dry mouth in an adult Swedish population-relation to age, sex and pharmacotherapy. Community Dent Oral Epidemiol1997;25: 211-216.
-
38Tootla, R; Toumba, KJ; Duggal, MS. An evaluation of the acidogenic potential of asthma inhalers. Arch Oral Biol 2004;49:275-283.
-
39Sag, C; Ozden, FO; Acikgoz G. The effects of combination treatment with a long-acting b2-agonist and a corticosteroid on salivary flow rate, secretory immunoglobulin A, and oral health in children and adolescents with moderate asthma: a 1-month, single-blind clinical study. Clin Ther 2007;29:2236-2242.
-
40Osterberg, T; Landahl, S; Hedegard, B. Salivary flow, saliva, pH and buffering capacity in 70-year-old men and women. Correlation to dental health, dryness in the mouth, disease and drug treatment. J Oral Rehabil 1984;11:157-170.
-
41Mochid,a Y; Yamamoto, T; Fuchida, S; Aida, J; Kondo, K. Does poor oral Health status increase the risk of falls?: The JAGES project longitudinal study. Plos One2018;13:e0192251.
Publication Dates
-
Publication in this collection
Nov-Dec 2018
History
-
Received
17 May 2018 -
Accepted
06 June 2018