Abstracts
Uveitis is a common disease in dogs with a multitude of causes, one of them being ehrlichiosis. This article reviews several uveitis etiologies, as well as the important aspects of canine ehrlichiosis, including its diagnosis and the main ophthalmic signs presented in these cases. It also reports the therapy that should be used.
canine; chorioretinitis; hyphema; uveitis; Ehrlichia canis
As uveítes, que se constituem em oftalmopatias comuns entre os cães, decorrem de inúmeras causas. Em nosso meio, destaca-se a erliquiose. Este artigo discute as várias causas da enfermidade ocular, bem como aspectos importantes da enfermidade parasitária, incluindo os sinais, o diagnóstico e o tratamento.
canino; corioretinite; hifema; uveíte; Ehrlichia canis
REVIEW
CLINIC AND SURGERY
Uveitis in dogs infected with Ehrlichia canis
Uveíte em cães infectados com Ehrlichia canis
Arianne Pontes OriáI; Patrícia Mendes PereiraI; José Luiz LausII,1 1 Autor para correspondência.
IGraduate Students, Veterinary College, São Paulo State University (UNESP), Jaboticabal, SP, Brazil
IIProfessor, DVM, PhD, Veterinary College, UNESP-Jaboticabal, Via de Acesso Prof. Paulo Donato Castellane s/n, 14884-900, Jaboticabal, SP, Brazil. E-mail: jllaus@fcav.unesp.br. Tel: 55 16 32092626 Fax: 55 16 32024275
ABSTRACT
Uveitis is a common disease in dogs with a multitude of causes, one of them being ehrlichiosis. This article reviews several uveitis etiologies, as well as the important aspects of canine ehrlichiosis, including its diagnosis and the main ophthalmic signs presented in these cases. It also reports the therapy that should be used.
Key words: canine, chorioretinitis, hyphema, uveitis, Ehrlichia canis.
RESUMO
As uveítes, que se constituem em oftalmopatias comuns entre os cães, decorrem de inúmeras causas. Em nosso meio, destaca-se a erliquiose. Este artigo discute as várias causas da enfermidade ocular, bem como aspectos importantes da enfermidade parasitária, incluindo os sinais, o diagnóstico e o tratamento.
Palavras-chave: canino, corioretinite, hifema, uveíte, Ehrlichia canis.
INTRODUCTION
In this review article, we describe the anatomy and physiology of the uveal tract, the clinical signs and pathophysiological mechanisms of uveitis, the diseases known to cause uveitis in dogs, the history and pathogenesis of ehrlichiosis, the clinical signs and diagnosis of ehrlichiosis and the treatment for ehrlichiosis and uveitis.
ANATOMY AND PHYSIOLOGY OF THE UVEAL TRACT
Uveitis refers to the inflammation of the uveal tract, which is the vascular and pigmented coat of the eye (HAKANSON & FORRESTER, 1990). The uveal tract or uvea is deeply located on the sclera, where it attaches itself. It consists of three zones: choroid, ciliary body and iris (HAKANSON & FORRESTER, 1990). The iris controls the intensity of the light that penetrates to the posterior segment of the eye. The ciliary body promotes visual accommodation, the production of the aqueous humor, and has an important role in the regulation of intraocular pressure (IOP) (COLLINS & MOORE, 1999).
Visual accommodation is accomplished using the ciliary body muscles. In uveitis, these muscle spasm cause intense pain to the animal (HAKANSON & FORRESTER, 1990). The aqueous humor helps maintain intraocular pressure, which can be affected by circadian variations, contraction of the extraocular muscles, intraocular inflammation, changes to osmotic and blood pressures (under the influence of median arterial pressure and central venous pressure) and by topical and systemic drugs, among other factors (SLATTER, 1990). Inflammation of the anterior uvea leads to a reduction in the active secretion of the aqueous humor, lowering intraocular pressure (COOK & PEIFFER, 1997). The obstruction of the trabecular meshwork by inflammatory debris can delay or obstruct its drainage, increasing the intraocular pressure (BANKS, 1992).
The anterior uvea is the site of the blood-aqueous barrier, which prevents the access of proteins and blood cells into intraocular fluid (HAKANSON & FORRESTER, 1990). Changes in these functions may result in the reduction or loss of vision. Therefore, changes in the anterior uvea are of great clinical significance (COLLINS & MOORE, 1999). The choroid or posterior uvea is the most important vascular portion of the eye and is the largest nutrition source for the dogs retina and also has a fundamental importance to heat dissipation, which is created by light reactions (BISTNER, 1996).
It is worth noting that the uvea has a highly inflammatory reaction in dogs (HAKANSON & FORRSTER, 1990). During the inflammatory process, capillary permeability is increased, causing cells and proteins to migrate to the aqueous humor and vitreous, resulting in an increased inflammatory response and the deposition of antigen-antibody complexes (HAKANSON & FORRESTER, 1990).
UVEITIS
Uveitis is described as a group of diseases of endogenous or exogenous origin (BISTNER et al., 1996). It is a complex inflammatory process clinically characterized by alterations to vascular permeability and cell infiltration (POWELL, 2002). It is not a simple nosologic entity and therefore should be treated as an ocular manifestation of different systemic diseases. Uveitis should be differentiated from other ocular afflictions that also cause pain and hyperemia. One should be attentive and thorough when distinguishing between various types and causes of uveitis (HAKANSON & FORRESTER, 1990).
Uveitis can be classified into anterior uveitis (iridocyclitis), posterior uveitis (choroiditis) and panuveitis (COLLINS & MOORE, 1999; POWELL, 2002).
Some of the clinical signs of anterior uveitis are conjunctival hyperemia, ciliary flush, corneal edema, presence of keratic precipitates, miosis, flare, Rubeosis iridis, iris color change, hyphema, anterior and posterior synechiae, cataract and reduction of the intraocular pressure. Acute posterior uveitis can be observed as hyporeflective lesions on the tapetal fundus, which can lead to retinal detachment. In the non-tapetal fundus, alterations can be seen as whitish-grayish spots (HAKANSON & FORRESTER, 1990). The healing process in these spots results in areas of hyperreflectivity and pigment deposition on the tapetal and non-tapetal regions, respectively (HAKANSON & FORRESTER, 1990; POWELL, 2002).
The pathophysiological mechanisms in which systemic infections can lead to uveitis are the direct destruction of the uveal tissues by infectious agents or the presence of immune-mediated events associated with infectious agents, including all four of the classical hypersensitivity responses (I, II, III, and IV) (FISCHER & EVANS, 2002). Many endogenous causes of uveitis have been recognized as bacterial (Brucella canis, Borrelia burgdorferi), fungal (Blastomyces dermatitidis, Cryptococcus neoformans, Histoplasma capsulatum), parasitic (Dirofilaria immitis, Diptera spp. (fly larvae), ocular larva migrans (Toxocara and Baylisascaris spp.), protozoan (Leishmania donovani, Toxoplasma gondii), rickettsial (Ehrlichia canis or Ehrlichia platys, Rickettsia rickettsii), viral (adenovirus, herpesvirus, distemper), idiopathic (trauma, toxemia, corneal ulceration), neoplastic and paraneoplastic disorders (hyperviscosity syndrome, primary and secondary neoplasia, granulomatous meningoencephalitis), metabolic disorders (phacolytic uveitis diabetic cataract), coagulopathy and immune-mediated disorders (vasculitis, cataract - lens induced or phacolytic uveitis, lens trauma phacoclastic uveitis and uveodermatologic syndrome) (POWELL, 2002).
EHRLICHIOSIS HISTORY AND PATHOGENESIS
Due to its severity, the ehrlichiosis is considered one of the most potentially fatal disease in domestic and wild dogs (PYLE, 1980). Ehrlichia canis belongs to the Rickettsiaceae family, which is a small, gram-negative coccoid bacterium that parasitizes circulating monocytes intracytoplasmically in clusters called morulae (HARRUS et al., 1997; WANER et al., 1999). The disease is transmitted by the tick Rhipicephalus sanguineus (MARTIN, 1999).
The disease was first identified as a specific entity in Algeria in 1935. Since then, it has been recognized worldwide (HARRUS et al., 1997). In Brazil, canine ehrlichiosis was first diagnosed by COSTA in Belo Horizonte in 1973, and later in Curitiba by KAVINSKI in 1988.
The pathogenesis of ehrlichiosis begins with an incubation period of 8 to 20 days; which is followed by acute, subclinical and chronic phase of the disease (HARRUS et al., 1997; NEER, 1998). During the acute phase, the parasite enters the bloodstream and the lymphatic system and stays in mononuclear phagocyte cells of the spleen, liver and lymph nodes, where it will replicate (HARRUS et al., 1997). These cells spread the rickettsias to other organs that interact with endothelial cells to induce a vasculitis (HARRUS et al., 1997).
Evidence that immunogenic mechanisms play a role in the pathogenesis of ehrlichiosis includes histological findings of extensive plasma cell infiltration of various parenchymal organs and perivascular cuffing of vessels in the lungs, kidneys, spleen, meninges and ocular tissues (HARRUS et al., 1996; HARRUS et al., 1997). Positive direct antiglobulin and autoagglutination tests in infected animals, as well as persistent hypergammaglobulinemia in all stages of the disease, also indicates immunogenic mechanism (HARRUS et al., 1996; HARRUS et al., 1997). The demonstration of antiplatelet antibodies in dogs experimentally infected with Ehrlichia canis further supports the theory that the disease may have an immunopathologic component (WANER et al., 1995; HARRUS et al., 1997).
EHRLICHIOSIS - CLINICAL AND OCULAR SIGNS
The clinical signs of the acute phase may be mild and non-specific and may include: depression, lethargy, moderate weight loss, anorexia, fever, lymphadenomegaly, splenomegaly, superficial bleeding, vomiting, nasal and ocular serous or purulent discharge, ataxia and dyspnea (SWANGO et al., 1989; WANER et al., 1999). These signs will usually decrease spontaneously within one to four weeks, but dogs can remain sub-clinically infected (SWANGO et al., 1989). Immunocompetent dogs are capable of eliminating the parasite during the sub-clinical phase (time frame of months to years), but some dogs develop the chronic phase of the disease, which could be moderate to severe (GOULD et al., 2000). The clinical signs of this phase include depression, weakness, anorexia, weight loss, peripheral edema, anemia, fever, bleeding due to platelet reduction, secondary bacteriologic infections, pneumonia, glomerulonephritis, arthritis, reproduction disorders, neurological signs and ocular alterations (HARRUS et al., 1997).
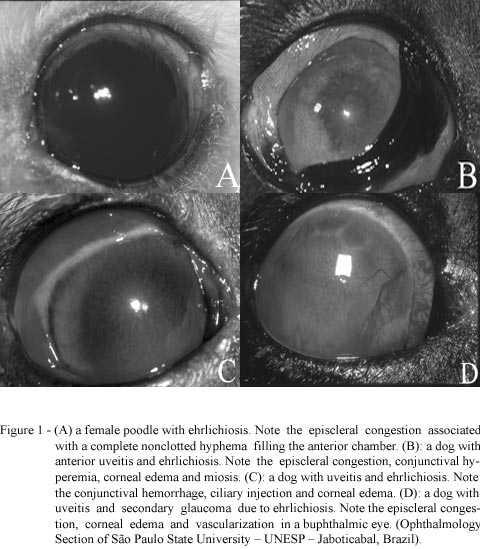
The ocular signs may be present in all phases of the disease (MARTIN 1999) and involve almost every structure of the eye (RISTIC et al., 1972; COLLINS & MOORE, 1999). The severity of the ocular involvement varies from patient to patient (STILES, 2000) (Figure 1). Experimentally, the ocular lesions have been present during the acute states, with 50% of the inoculated dogs developing ocular lesions (MARTIN, 1999). The prevalence of ocular lesions in naturally occurring cases ranges from 10% to 15% (MARTIN, 1999). The ocular findings include conjunctival hemorrhages, episcleral congestion, anterior chamber flare, Rubeosis iridis, miosis, corneal edema, keratic precipitates, hypopyon, hyphema and reduced intraocular pressure (GLAZE & GAUNT, 1986; HARRUS et al., 1998; CLERC & LAFORGE, 1999; STILES, 2000). Inflammatory debris can obstruct the trabecular meshwork to induce secondary glaucoma and annular posterior synechiae will result in iris bombé formation (COLLINS & MOORE, 1999). If the posterior segment is involved, then papilledema and chorioretinitis can be seen (GLAZE & GAUNT, 1986). Severe thrombocytopenia causes retinal hemorrhages and hyphema, and conjunctival petechiae may be seen in the chronic phase of the disease (SWANSON, 1990; GLAZE & GAUNT, 1986). Frequent hemorrhage may induce secondary retinal detachment (EVERMANN, 1998; MARTIN, 1999). Optic neuritis, retinal blood vessel engorgement and papillary hemorrhage may also be present (MARTIN, 1999; STILES, 2000). Tortuosity of retinal blood vessels has been recorded along with chorioretinal lesions characterized by centrally pigmented hyperreflective areas (HARRUS et al., 1997). An unusual and infrequently observed ocular lesion is bilateral subconjunctival melting scleral lesions that result in perforation and uveal tract prolapse (MARTIN & STILES, 1998; MARTIN, 1999; STILES, 2000).
ELLETT et al. (1973) and CLERC & LA FORGE, (1999) reported that dogs experimentally infected with Ehrlichia canis develop engorged retinal vessels during the initial fever stage. This phase is followed by the regression of the vascular engorgement, with simultaneous development of perivascular lesions on the tapetal and non-tapetal fundus. Later, the lesions will reduce in size, becoming discrete, or they are substituted by areas of intense hyperreflectivity the same as observed on progressive retinal atrophy (PRA), but without the typical vascular attenuation (ELLETT et al., 1973; MARTIN, 1990).
In a recent study, from the 88 animal eyes studied that had positive serology for Ehrlichia canis, 63 presented exclusively uveitis, distributed into iridocyclitis, posterior uveitis and panuveitis; 22 presented uveitis and secondary glaucoma, and the remaining three were phthisical. Ocular discharge was observed in 45.4% of the dogs; there was episcleral congestion in 69.3%, ciliary injection in 28.4%, corneal edema in 61.3%, keratic preciptates in 18.1%, flare in 22.7%, hyphema in 10.2%, iris edema in 36.3%, Rubeosis iridis in 25%, iris pigmentation and retinal detachment in 11.3%, tortuous retinal vessels in 27.2%, hemorrhage in 12.5% and retinal hyperreflexia in 9% of the cases (ORIÁ, 2001).
EHRLICHIOSIS DIAGNOSIS
The diagnosis of ehrlichiosis is done through serology (indirect immunofluorescent antibody assay and dot-blot ELISA), associated with clinical signs and laboratory results, wherein thrombocytopenia, hematological abnormalities (anemia, leukopenia, lymphopenia) and serum abnormalities (hypoalbuminemia, hypergammaglobulinemia) are apparent. Another way to make a diagnosis is by verifying the presence of morulae in the cytoplasm of mononuclear cells on blood smears. They are present during the acute phase of the disease, however they can be difficult to find (HARRUS et al., 1997).
Serological evaluation is necessary in all cases where infection is suspected (EVERMANN, 1998). The indirect immunofluorescent antibody test (IFA) has rarely been used, because it requires specialized laboratory services (CADMAN et al., 1994). However, values for the dot-blot enzyme linked immunoassay technique (DBELIA) have been correlated with serological titers obtained by the IFA test (CADMAN et al., 1994). Using the Immunocomb test (Biogal) based on the DBELIA technique, it is possible to determine IgG antibodies specific for the organism (CASTRO, 1997; ORIÁ, 2001).
Monoclonal gammopathy and hypoalbuminemia have been seen in canine ehrlichiosis, although polyclonal gammopathy, followed by hypoalbuminemia are more commonly found (MICHELS, 1995; PERILLE, 1991). Platelet dysfunction can contribute to ocular hemorrhages, when a high concentration of paraproteins is present (HARRUS et al., 1998). The most common clinical manifestations of monoclonal gammopathy are hemorrhages and hyperviscosity syndrome. An elevation in protein concentrations has been linked to the genesis of oncotic pressure elevation, leading to hypervolaemia (HARRUS et al., 1998).
The elevation of oncotic pressure, as well as secondary isquemic alterations and hyperviscosity, could cause a hypertensive retinopathy and hyphema (HARRUS et al., 1998; KOMAROMY, 1999). It also includes the deposition of immune complexes on the vascular wall, and vasculitis, which is seen as a lymphoplasmacytic perivascular cuffing (HARRUS, 1998). Ocular hemorrhage can be due to an increase in the oncotic pressure and vasculitis, as well as thrombocytopenia and platelet dysfunction (HARRUS et al., 1998).
TREATMENT EHRLICHIOSIS AND UVEITIS
The key to the treatment is to maintain the visual ability of the patient. The specific therapy for ehrlichiosis is doxycycline (5 to 10mg/kg every 12 hours, orally, for 21 days) and/or imidocarb dipropionate (5mg/kg, subcutaneously, with an interval of 15 days minimum) (FISCHER, 2002). With regard to the tick-control, the use of fipronil on a monthly basis has proved to be an effective prevention and treatment for dogs in areas endemic to canine monocytic ehrlichiosis (DAVOUST et al., 2003).
Drugs that can control inflammation are essential. Corticosteroids (systemic and local) are the most common group of drugs used in cases of uveitis, especially prednisone. Whenever necessary, non-steroidal anti-inflammatories (NSAIDs) can be used alone as an alternative to corticosteroids (POWELL, 2002), or in combination with them, in order to maximize the anti-inflammatory effects of the therapy. Also, the use of NSAIDs should be avoided when coagulopaties or intraocular hemorrhage are present (POWELL, 2002), which are not uncommon in cases of ehrlichiosis. The use of systemically NSAIDs should be done cautiously because of their interference with platelet function and the possibility of persistent or recurrent bleeding. A good alternative is the use of oral carprofen because it has a minimal effect on the platelet function (COLLINS & MOORE, 1999). There are also vedaprofen and meloxicam on the local market, which can be used with good results.
Cyclopegics and mydriatics, such as atropine sulfate at 1%, have been recommended in cases of anterior uveitis in order to prevent the formation of synechia and to reduce the ciliary spasms leading to local pain relief. However, one should be very careful because of the possibility of compromising the iridocorneal angle, causing obstruction, since mydriasis can promote increase of intraocular pressure, leading to glaucoma. If glaucoma is already present, a topical carbonic anhydrase inhibitor, such as dorzolamide HCL (2% ophthalmic solution) or brinzolamide (1% ophthalmic suspension) should be used, to reduce the production of aqueous humor. Seletive and nonseletive b-adrenergic blocking agents can be added to this protocol, like timolol maleate (0.5% to 4%), metipranolol or betaxolol hydrochloride for having additive effects on the decrease of the intraocular pressure, when used in combination with a carbonic anhydrase inhibitor. Topical antibiotics have little penetration into the anterior chamber, so a systemic antibiotic therapy is recommended, whenever necessary (FISCHER & EVANS, 2002). The dipivefrin is a sympathomimetic agent usually used on the treatment of glaucoma. In patients with uveitis that are susceptible to or already have glaucoma, its use is very beneficial. Under these circumstances, the hypotensive effects of the drug are desirable in order to reduce the IOP and the mydriatic effects to prevent the formation of posterior synechiae (COLLINS & MOORE, 1999).
The prognosis depends on the lesions severity. In cases of a medium to moderate degree, the prognosis is favorable. Severe cases have a guarded prognosis. The eye should be re-evaluated within the first 24 to 48 hours following treatment. If secondary conditions develop as a result of the uveitis (glaucoma, hyphema, intense pain), the prognosis is guarded to poor (POWELL, 2002). The prognosis also becomes guarded in cases where there is no improvement of the clinical signs, such as in animals that develop bone marrow aplasia.
CONCLUSION
Ehrlichiosis is endemic in our region. It is very difficult to control, because there are no campaigns to inform the public how to control the spread of ticks. Therefore, it is important to draw attention to the fact that ehrlichiosis can cause uveitis in several cases and it could manifest itself without a definite pattern. The goals of treatment in these cases are to identify and treat ehrlichiosis thoroughly, control the ocular inflammation and to promote pain relief.
Recebido para publicação 29.05.03
Aprovado em 29.10.03
- BANKS, J.W. Olho e ouvido. In: Histologia veterinária aplicada São Paulo : Manole, 1992. Cap.28, p.589-600.
- BISTNER, S.; SHAW, D.; RIIS, R.C. Disease of the uveal tract (part I). In: GLAZE, M.B. The compendium collection: ophthalmology in small animal practice New Jersey : Veterinary Learning Systems, 1996. p.161-185.
- CADMAN, H.F. et al. Comparison of the dot-blot enzyme linked immunoassay with immunofluorescence for detecting antibodies to Ehrlichia canis Veterinary Record, v.8, p.362, 1994.
- CASTRO, M.B. Avaliação das alterações hematológicas, imunológicas e anatomopatológicas na infecção aguda experimental de cães por Ehrlichia canis (DONATIEN & LESTOQUARD, 1935) Moshkovski 1945 1997. 69f. Dissertação (Mestrado em Patologia Veterinária) - Curso de Pós-graduação em Medicina Veterinária, Universidade Estadual Paulista.
- CLERC, B.; LAFORGE, H. Ocular manifestations of systemic disease. In: ETTINGER, S.J.; FELDMAN, E.C. Textbook of veterinary internal medicine Philadelphia : Saunders, 1999. V.1. Cap.78, p.524-532.
- COLLINS, B.K.; MOORE, C.P. Disease and surgery of the canine anterior uvea. In: GELATT, K.N. Veterinary ophthalmology Philadelphia : Lippincott Williams & Wilkins, 1999. Cap.22, p.755-796.
- COOK, C.S.; PEIFFER JR., R.L. Clinical basic science. In: PEIFFER JR., R.L; PETERSEN-JONES, S.M. Small animal ophthalmology Philadelphia : Saunders, 1993. p.1-12.
- COSTA, J.O. Ehrlichia canis infection in dog in Belo Horizonte - Brazil. Arquivos Escola Veterinária UFMG, Belo Horizonte, v.25, p.199-200, 1973.
- DAVOUST, B. et al. Assay of fipronil efficacy to prevent canine monocytic ehrlichiosis in endemic areas. Veterinary Parasitology, v.112, p.91-100, 2003.
- ELLETT, E.W.; PLAYTER, R.F.; PIERCE, K.R. Retinal lesions associated with induced canine Ehrlichiosis: a preliminary report. Journal of the American Animal Hospital Association, v.9, p.214-218, 1973.
- EVERMANN, J.F. Laboratory diagnosis of viral and rickettsial infections. In: GREENE, C.E. Infectious diseases of the dog and cat Philadelphia : Saunders, 1998. Cap.28, p.1-6.
- FISCHER, C.A.; EVANS, T. Uveitis: ocular manifestations of systemic diseases in dogs. In: RIIS, R.C. Small animal ophthalmology secrets Philadelphia : Hanley & Belfus, 2002. Cap.29, p.184-191.
- GLAZE, M.B.; GAUNT, S.D. Uveitis associated with Ehrlichia platys infection in a dog. Journal of the American Veterinary Medical Association, v.188, p.916-917, 1986.
- GOULD, D.J. et al. Canine monocytic ehrlichiosis presenting an acute blindness 36 months after importation into the UK. Journal of Small Animal Practice, v.41, p.263-265, 2000.
- HAKANSON, N.; DRU FORRESTER, S. Uveitis in the dog and cat. Veterinary Clinics of North America Small Animal Practice, v.20, n.3, p.715-735, 1990.
- HARRUS, S. et al. Kinetics of serum antiplatelet antibodies in experimental acute canine ehrlichiosis. Veterinary Immunology and Immunopathology, v.5, p.13-20, 1996.
- HARRUS, S.; BARK, H.; WANER, T. Canine monocytic ehrlichiosis an update. Compendium on Continuing Education for the Practicing Veterinarian, v.5, n.1, p.9-16, 1997.
- HARRUS, S. et al. Acute blindness associated with monoclonal gammopathy induced by Ehrlichia canis infection. Veterinary Parasitology, v.78, n.31, p.155-160, 1998.
- KAVINSKI, L.C. Ocorrência de um caso de erliquiose canina em Curitiba - PR. Revista do Setor de Ciências Agrárias v.10, p.217-219, 1988.
- KOMAROMY, A.M. et al. Hyphema. Part I. Pathophysiologic considerations. Compendium on Continuing Education for the Practicing Veterinarian; v.21, p.1064-1069, 1999.
- MARTIN, C.L. Ocular infections. In: GREENE, C.E. Infectious diseases of the dog and cat Philadelphia : Saunders, 1990. Cap.13, p.209.
- MARTIN, C.L. Ocular manifestations of systemic disease. In: GELATT, K.N. Veterinary ophthalmology Philadelphia : Lippincott Williams & Wilkins, 1999. Cap.37, p.1408-1409.
- MARTIN, C.L.; STILES, J. Ocular infections. In: GREENE, C.E. Infectious diseases of the dog and cat Philadelphia : Saunders, 1998. Cap.28, p.658-671.
- MICHELS, G.M., et al. Hypergammaglobulinemia in a dog. Journal of the American Veterinary Medical Association, v.207, p.567-570, 1995.
- NEER, T.M. Canine monocytic and granulocytic ehrlichiosis. In: GREENE, C.E. Infectious diseases of the dog and cat Philadelphia : Saunders, 1998. Cap.28, p.139-147.
- ORIÁ, A.P. Correlação entre uveítes, achados de patologia clínica, sorológicos (Reação de imunofluorescência indireta e Dot-blot ELISA) e de anatomopatologia do bulbo do olho, em animais da espécie canina, natural e experimentalmente infectados pela Ehrlichia canis 2001. 69f. Dissertação (Mestrado em Cirurgia Veterinária) Curso de Pós-graduação em Cirurgia Veterinária, Universidade Estadual Paulista, Campus de Jaboticabal.
- PERILLE, A.L.; MATUS, R.E. Canine ehrlichiosis in six dogs with persistently increased antibody titers. Journal of Veterinary Internal Medicine, v.195, p.195-198, 1991.
- POWELL, C.C. Uveitis in general. In: RIIS, R.C. Small animal ophthalmology secrets Philadelphia : Hanley & Belfus, 2002. Cap.28, p.177-183.
- PYLE, R.L. Canine ehrlichiosis. Journal of the America Veterinary Medical Association, v.177, n.12, p.1197-1199, 1980.
- RISTIC, M. et al. Sorological diagnosis of tropical canine pancytopenia by indirect immunofluorescence. Infection and Immunity, v.6, p.226-231, 1972.
- SLATTER, D. Uvea. In: Fundamentals of veterinary ophthalmology 3.ed. Philadelphia : Saunders, 1990. Cap.12, p.338-364.
- STILES, J. Canine rickettsial infections. Veterinary Clinics of North America. Small Animal Practice, v.30, p.1135-1149, 2000.
- SWANGO, L.J.; BANKEMPER, K.W.; KONG, L.I. Bacterial, rickettsial, protozoal and miscellaneous infection. In: ETTINGER, S.J. Textbook of veterinary internal medicine Philadelphia : Saunders, 1989. Cap.46. p.265-297.
- SWANSON, J.F. Ocular manifeststions of systemic diseases in the dog and cat. Veterinary Clinics of North America. Small Animal Practice, v.20, n.3, p.849-867, 1990.
- WANER, T. et al. Demonstration of serum antiplatelet antibodies in experimental acute canine ehrlichiosis. Veterinary Immunology and Immunopathology, v.48, p.177-182, 1995.
- WANER, T. et al. Canine monocytic ehrlichiosis an overview. Israel Veterinary medical Association, v.54, n.4, p.1-8, 1999.
Publication Dates
-
Publication in this collection
30 Aug 2004 -
Date of issue
Aug 2004
History
-
Received
29 May 2003 -
Accepted
29 Oct 2003