Abstracts
The aim of this research was to evaluate economic costs of respiratory and circulatory diseases in the municipality of Cubatão, in the state of São Paulo, Brazil. Data on hospital admissions and on missed working days due to hospitalization (for age group 14 to 70 years old) from the database of Sistema Único de Saúde (SUS - Brazilian National Health System) were used. Results: Based on these data, it was calculated that R$ 22.1 million were spent in the period 2000 to 2009 due to diseases of the respiratory and circulatory systems. Part of these expenses can be directly related to the emission of atmospheric pollutants in the city. In order to estimate the costs related to air pollution, data on Cubatão were compared to data from two other municipalities that are also located at the coast side (Guarujá and Peruíbe), but which have little industrial activity in comparison to Cubatão. It was verified that, in both, average per capita costs were lower when compared to Cubatão, but that this difference has been decreasing in recent years.
Atmospheric Pollution; Health Costs; Cubatão; Cardiorespiratory Diseases
O objetivo básico do trabalho foi avaliar os custos econômicos relacionados às doenças dos aparelhos respiratório e circulatório no município de Cubatão (SP). Para tanto, foram utilizados dados de internação e dias de trabalho perdidos com a internação (na faixa dos 14 aos 70 anos de idade), na base de dados do Sistema Único de Saúde (SUS). Resultados: A partir dos dados levantados, calculou-se o valor total de R$ 22,1 milhões gastos no período de 2000 a 2009 devido às doenças dos aparelhos circulatório e respiratório. Parte desses gastos pode estar diretamente relacionada à emissão de poluentes atmosféricos no município. Para se estimar os custos da poluição foram levantados dados de outros dois municípios da Região da Baixada Santista (Guarujá e Peruíbe), com menor atividade industrial em comparação a Cubatão. Verificou-se que, em ambos, as médias de gastos per capita em relação às duas doenças são menores do que em Cubatão, mas que essa diferença vem diminuindo sensivelmente nos últimos anos.
Poluição atmosférica; custos de saúde; Cubatão; doenças cardiorrespiratórias
ARTICLES
Economic cost of air pollution in Cubatão - SP based on health expenses related to diseases of the respiratory and circulatory systems
Flávio TayraI; Helena RibeiroII; Adelaide de Cássia NardocciIII
IEconomista. Doutor em Ciências Sociais e Pós-doutorado em Saúde Pública pela USP. Professor da FEI e consultor econômico. Endereço: Rua Dr. Nicolau de Souza Queiroz, 167, ap. 502, CEP 04105-000, São Paulo, SP, Brasil. E-mail: ftayra@usp.br
IIGeógrafa. Livre-docente em Saúde Pública. Professora titular do Departamento de Saúde Ambiental da Faculdade de Saúde Pública da Universidade de São Paulo. Endereço: Av. Dr. Arnaldo, 715, CEP 01246-904, São Paulo, SP, Brasil. E-mail: lena@usp.br
IIIFísica. Livre-docente em Saúde Pública. Professora associada do Departamento de Saúde Ambiental da Faculdade de Saúde Pública da Universidade de São Paulo. Endereço: Av. Dr. Arnaldo, 715, CEP 01246-904, São Paulo, SP, Brasil. E-mail: nardocci@usp.br
ABSTRACT
The aim of this research was to evaluate economic costs of respiratory and circulatory diseases in the municipality of Cubatão, in the state of São Paulo, Brazil. Data on hospital admissions and on missed working days due to hospitalization (for age group 14 to 70 years old) from the database of Sistema Único de Saúde (SUS - Brazilian National Health System) were used. Results: Based on these data, it was calculated that R$ 22.1 million were spent in the period 2000 to 2009 due to diseases of the respiratory and circulatory systems. Part of these expenses can be directly related to the emission of atmospheric pollutants in the city. In order to estimate the costs related to air pollution, data on Cubatão were compared to data from two other municipalities that are also located at the coast side (Guarujá and Peruíbe), but which have little industrial activity in comparison to Cubatão. It was verified that, in both, average per capita costs were lower when compared to Cubatão, but that this difference has been decreasing in recent years.
Keywords: Atmospheric Pollution; Health Costs; Cubatão; Cardiorespiratory Diseases.
Introduction
Despite the advances in the control of pollutant emissions related to the industrial activity, it is still an important source of air pollution. The analysis of the economic and social development that industry enables usually does not take into account the cost-benefit balance of the activities, and does not include the short and long term cost associated with the increase in deaths and diseases that is caused by pollution.
Diverse studies have reported a significant association between pollution levels and morbidity and mortality markers. In these studies, particle pollution has been associated with worse pulmonary function, increased respiratory symptoms (Schwartz, 1994; Ostro, 1998; Desqueyroux and Momas, 1999) and with the increment in hospital admissions due to respiratory diseases (Sunyer and col., 1997; Gouveia and Fletcher, 2000) and cardiovascular diseases (Zanobetti and col., 2000; Poloniecki and col., 1997). The increase in daily mortality has also been reported in many countries (Anderson and col., 1996; Daumas and col., 2004; Toulomi and col., 1996), and it may be associated with particle pollution, even when the average concentrations are within the international standards for air quality (Momas and col., 1993).
Calculating the economic costs associated with pollution in this case, air pollution is an action of great importance for decision-making as, by means of specific techniques, it enables to construct indicators that subsidize the adoption of the most efficient options. In this sense, the basic purpose is to measure the utilized inputs (costs) and the obtained results (effects). Thus, the aim of such measurement is that of optimization, either through the minimization of costs to obtain the same results, or through the maximization of results at the lowest cost. Essentially, therefore, economic assessments are technical procedures that support strategic and managerial decisions.
In light of what was presented above, this study aimed to calculate the economic cost associated with respiratory and cardiovascular diseases related to air pollution in the municipality of Cubatão, which is located in the Metropolitan Region of the Baixada Santista, in the State of São Paulo (Southeastern Brazil).
Methodology
The majority of the analyzes that estimate the social cost of pollution use the damage-function method (DF), in which the following relationships are estimated: policy and emissions, emissions and air quality, air quality and exposure, exposure and physical damages, and physical damages and monetary value (Delucchi, 2000; Delucchi and col., 2002; Gangadharan and Valenzuela, 2001; Garber and col., 1996; Garber and Phelps, 1997; Krupnick and col., 1996; Pearce and Markandya, 1987). However, all these stages and particularly the assessment stage contain a reasonable amount of uncertainty, and as a result, the estimates of the socioeconomic cost of air pollutant emissions have proved to be highly variable, and many times, conflicting (Murphy and Delucchi, 1998; McCubbin and Delucchi, 1999; Quah and Boon, 2003).
Generally speaking, the valuation methods can be divided between those of demand function and those of production function (Seroa da Motta and Mendes, 1995). In the case of the production function methods, the environmental resource has a value, because it contributes as input or substitute in the production of a private good or service. Due to this relation, it is possible to use the prices of private goods and services so that the monetary value of the environmental resource is estimated (Seroa da Motta, 1995). These methods are the most used ones in the valuation of nonmarket goods, because they employ techniques that are simpler to apply, as goods that already exist in the market are used as shadow price.
The marginal productivity method is capable of establishing relations between a given production function and possible alterations to a particular environmental good or service, observing the correlation between these variables and constructing a dose-response function (DR).
The health costs associated with diseases of the respiratory and circulatory systems (related, among other reasons, to air pollution) can be classified into four categories:
1) Medical expenses associated with the treatment of diseases;
2) Missed working days resulting from the disease;
3) Expenses to avoid or prevent (preventive expenses) and activities associated with attempts to mitigate the disease; and
4) Disutility associated with the symptoms and leisure opportunities lost due to the disease.
In view of the difficulties in estimating the portions referring to the two last items, we calculated the health cost associated with air pollution by adding total hospital expenses (per age group and per event) to the value of the missed working days due to the disease, based on the average salaries in the region.
Hospital expenses were calculated and the number of missed working days due to hospitalizations was estimated, based on data from Datasus, of the Sistema Único de Saúde (SUS Brazilian National Health System), surveyed in the portal of the Health Department of the State of São Paulo. Data on mortality by causes were provided by Fundação Seade, of the Government of the State of São Paulo.
In this stage of the research, hospitalization expenses due to the main causes (ICDs) were surveyed, as well as deaths, emphasizing the respiratory and cardiovascular causes. This survey fulfilled two objectives: to detect the main causes of death in the municipality, and also, the trend of such causes in the 2000 2009 decade. With a variation in the data, the number of missed working days due to hospital admissions was also calculated for those in the age group 14-70 years, so that it was possible to measure the costs related to absences from work, a portion that is not included in the data of Sistema Único de Saúde. With these data, it was possible to obtain the direct and indirect costs related to hospitalizations due to respiratory and cardiovascular diseases in Cubatão in the period from 2000 to 2009.
Income data were surveyed from the calculation of the average effective yield of the employed population (Pastore, 1994), calculated by Pesquisa Mensal do Emprego (PME Monthly Employment Research), of IBGE Instituto Brasileiro de Geografia e Estatística (Brazilian Institute of Geography and Statistics). All the values were discounted to present value (January 2010), based on the average of IPCA (Extended National Consumer Price Index, also of IBGE) to the years under analysis.
To attribute value to the missed working day, we used the mean of the 2009 average monthly labor income, for overall Brazil, as the research is carried out only in metropolitan regions and the average of the Metropolitan Region of São Paulo was higher than the national average. These data were obtained from IBGE's PME, and the average was divided by 30 (number of days).
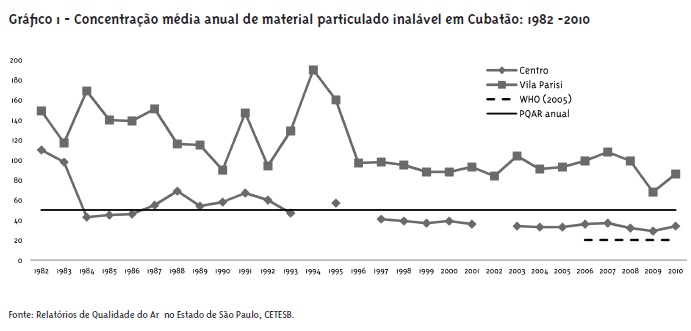
From 1970 to 1980, Cubatão's economic growth reached a level of 4.43% per year, and in 1985, its industrial production represented approximately 3% of the national GDP, with industries of the petrochemical, steel and fertilizer sectors. On the other hand, in 1984, its industries released approximately 1,000 daily tons of pollutants into the air, and the air pollution levels reached values that were absolutely critical. Since then, dozens of programs and actions have been developed with the aim of reducing the industrial emissions. In 2010, according to Companhia de Tecnologia de Saneamento Ambiental(CETESB - Environmental Sanitation Technology Company), Cubatão had 230 priority industrial sources of fossil fuels emission and combustion, which released annually into the atmosphere 3.4x103 tons of carbon monoxide CO, 1.1x103 tons of hydrocarbons HC, 7.62x103 tons of nitrogen oxides NOx, 15.8x103 of sulfur oxides SOx and 3.06x103 tons of particulate matter (CETESB, 2011).
Despite the efforts that have been undertaken and the systematic reduction in the emission of pollutants in the last decades in Cubatão, the air quality standards are frequently exceeded. Graph 1 shows the average annual concentrations of particulate matter, measured in the monitoring stations located in the central region and in the industrial area of Cubatão, from 1982 to 2010, as well as the values of the air quality standard defined by CETESB and the standard recommended by the World Health Organization in 2005 (WHO, 2005).
Results
Causes of death in the municipality
At Cubatão, the respiratory causes represent the fourth cause of death. Air pollution is related to the increase in respiratory problems. However, in the studied decade, the diseases of the circulatory system were the main cause of death in the city. Between 2000 and 2009, 1,436 deaths were registered due to this cause, representing 23.4% of the cases. They were followed by external causes (17.9%) and cancer (13.3%). Respiratory system diseases were responsible for 10.7% of the deaths, as shown by Graph 2.
In the period under analysis, the causes of death in the municipality presented a relative stability. In absolute figures, the total number of deaths decreased from 699 in 2000 to 659 in 2008. The circulatory system diseases represented 19.9% of the deaths in 2000 and reached 26.6% in 2008. Those related to the respiratory system represented 9.6% in 2000 and reached 11.5% in 2008. In terms of percentages, both presented an increasing trend (Graph 2).
Respiratory deaths
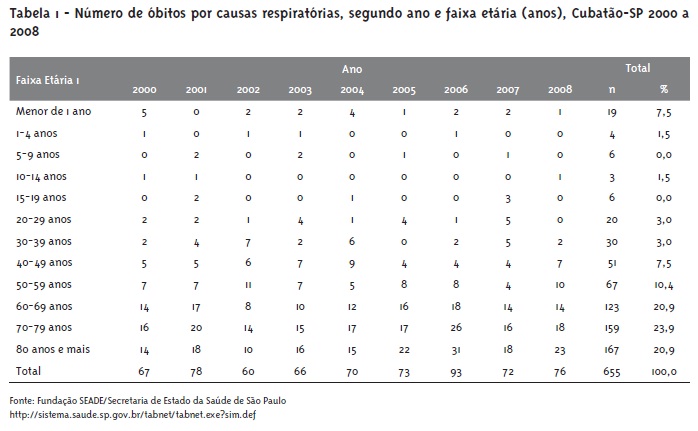
Deaths caused by respiratory diseases in children have greater impact among those younger than 1 year (7.5%). However, people older than 60 years represent 65.7% of the deaths related to this cause, which indicates an age-related situation of vulnerability, as shown in Table 1.
Despite the oscillations, a slight reduction in the mortality rate by respiratory causes can be perceived in the municipality of Cubatão. In 2000, the rate was 61.9 per 100 thousand inhabitants; it reached 76.9 in 2007 and, in 2008, it was 59.5 per 100 thousand inhabitants. On the other hand, in the age group of children younger than 1 year, the decline was quite significant: it was 234.7 in 2000 and decreased to 49.7 in 2008 (Graph 3).
Hospitalizations
In terms of percentages, pregnancy, delivery and puerperium are the main cause of hospitalization through Sistema Único de Saúde (SUS) in Cubatão. They rank first in the authorizations for hospitalizations of the SUS (23.8%), followed by the causes related to diseases of the respiratory system, which represent 11.2% and are responsible for the highest number of days of stay in hospitals. Injuries and external causes are the third most important chapter in terms of number of hospitalizations, followed by diseases related to the circulatory system, with 8% (Graph 4).
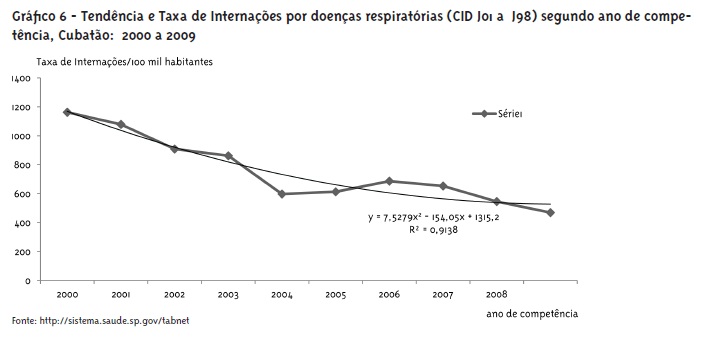
Hospitalization rates due to respiratory diseases present a sharp decline trend, both for men and for women, as presented in Graphs 5 and 6.
Costs associated with the diseases
Although they are the fourth main hospitalization cause, the diseases of the circulatory system have the main share in the values paid by the SUS (18.3% of the total), being followed by those related to pregnancy and delivery. The diseases of the respiratory system, the second main hospitalization cause, are the third in terms of paid monetary values.
In monetary values, between 2000 and 2009 the SUS spent R$ 59.2 million in the municipality. The diseases of the circulatory system consumed R$ 10.9 million and represent 18.3% of the resources. The diseases of the respiratory system, in turn, corresponded to expenses of R$ 6.9 million (11.6%).
The share of the circulatory diseases in the total value paid by the SUS, in relative terms, reached its peak in 2003 (21.7%). The respiratory diseases had their largest share in 2001, when they reached 13.9%, as shown in Graph 7.
Although they have a lower number of hospitalizations and a smaller share in terms of value paid, the diseases of the respiratory system exceed those of the circulatory system in number of days at the hospital. The treatments can be simpler or less expensive, but they demand more days of hospitalization.
Expenses by age group
The longer hospitalization time caused by the respiratory diseases affects mainly children younger than 1 year, who account for 24% of the total of resources spent on hospitalization. The children younger than 14 years (including those younger than 1 year) account for 51.4% of the total spent due to this cause.
In the case of the circulatory diseases, the situation is different, because their costs are concentrated mainly on the age group 40 70 years, which absorb 65% of the expenses, as can be seen on Tables 2 to 5.
The days of stay at the SUS units totaled 424.5 thousand between 2000 and 2009. The respiratory system diseases generated the largest period of stay, being responsible for 56.9 thousand days in the period, although they rank third in the paid authorizations for hospital admissions.
Calculating the economic cost of the disease
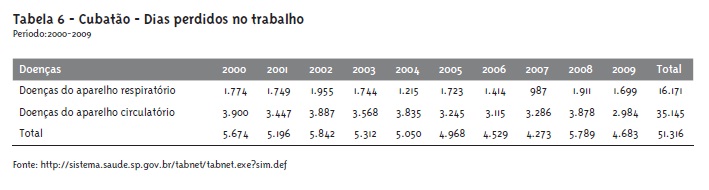
As seen in the previous item, despite the longer stay due to the respiratory system diseases, the highest number of missed working days is due to the causes of the circulatory system, which affect people in an age group in which they are more involved in the labor market.
As was already mentioned in the methodology, the value per missed day was calculated based on the 2009 average monthly income for overall Brazil. These data were obtained from the Monthly Employment Research (PME) of IBGE; they were divided by 30 (number of days) and multiplied by the hospitalization days. It is a conservative calculation, as absences from work may have occurred before or after the hospitalizations, due to the same episode of disease.
Due to this aspect, the cost of missed working days due to diseases of the circulatory system is much higher than that of the diseases of the respiratory system, which has represented, since the beginning of the decade, a share that is sometimes inferior to 50% (Table 6).
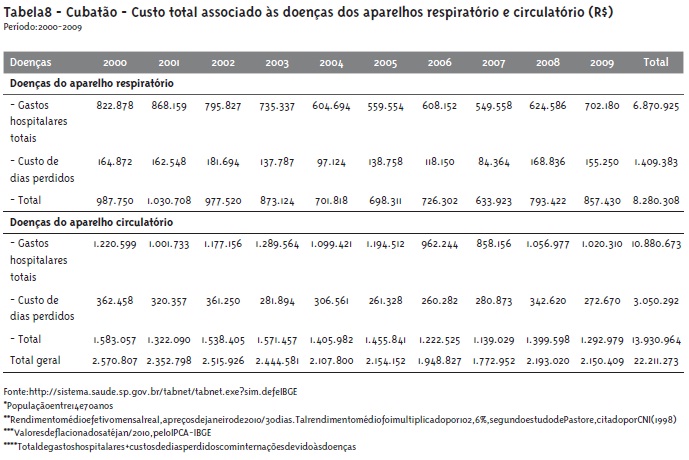
The health cost associated with hospitalizations due to diseases of the circulatory and respiratory systems was also calculated, adding the total hospital expenses (per age group and per event, concentrated on respiratory and cardiovascular morbidity) to the value of the missed working days due to the disease, which was based on the average salaries (Table 7). Based on such premises and data, we arrived at the total cost of R$ 22.1 million.
Total cost of the circulatory and respiratory diseases
Based on the surveyed data, we arrived at the total value of R$ 22.1 million spent in the period from 2000 to 2009 due to the diseases of the circulatory and respiratory systems (Table 8). The respiratory diseases accounted for costs of R$ 8.3 million, while the costs of the circulatory diseases were R$ 13.9 million.
It should be highlighted that when the total costs were discounted to present value, they showed a slight deceleration in relation to the beginning of the decade, a fact that was also demonstrated by the decreasing trend in the number of hospitalizations due to respiratory causes. In 2000, R$ 2.57 million were spent per year, while this value was reduced to R$ 2.15 million in 2009.
Estimating the economic cost of pollution
The presented costs, related to circulatory and respiratory diseases in the municipality of Cubatão, represent an expressive sum and had a decreasing trend in the last 10 years. Nevertheless, it is important to highlight that the economic costs associated with air pollution represent only a part of such costs, as even in cities with little or no industrial activity and low volume of vehicle traffic, that is, with low rate of pollutant emission, records of cases of such diseases and their inherent costs are verified.
To estimate the associated economic costs, hospitalization data from two adjacent municipalities were surveyed and compared. These municipalities do not have air pollution monitoring stations but present neither the industrialization history nor industries of pollutant potential like Cubatão. One city is very close: Guarujá, a tourist resort whose predominant economic activity are the services; the other, Peruíbe, is a little farther and also has low industrial activity compared to Cubatão. All three are coastal municipalities and were selected to control for the climate factor.
The per capita expenses related to hospitalizations due to respiratory and circulatory problems were calculated. In 2000, the per capita expense with hospitalizations due to circulatory diseases in Cubatão was R$ 10.82 per inhabitant. In Guarujá it was R$ 8.48 and in Peruíbe, it was much lower (R$ 4.70). From 2007 onwards, however, this relationship was reversed and Peruíbe started to have an average per capita expense that was higher than that of Cubatão (in 2009, it was R$ 10.58, compared to R$ 7.69 of Cubatão). Nevertheless, regarding the average of the last 10 years, the per capita expense in Cubatão was higher than that of the two other cities (Graph 8).
The same relationship can be observed in relation to hospitalizations due to diseases of the respiratory system. In 2000, while Cubatão had an average per capita expense of R$ 7.30, in Peruíbe this value was of R$ 4.06 and in Guarujá, it reached R$ 6.46. Generally speaking, the expenses gradually decreased during the decade and, in 2007, Peruíbe started to present a value that was higher than that of Cubatão. Concerning the average of the last 10 years, the per capita expense in Cubatão is still higher than that of the two other municipalities, as shown in Graph 9.
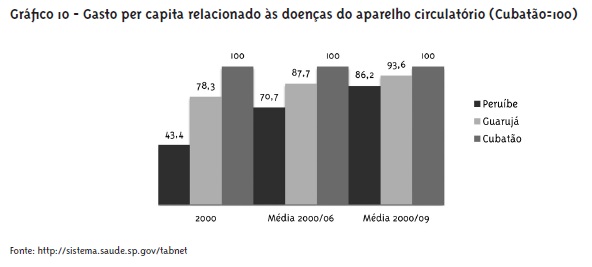
Another way of observing the evolution of the per capita expenses due to the two diseases is by verifying the proportion of each municipality in relation to the municipality under focus. In 2000, the per capita expense due to diseases of the circulatory system in Peruíbe represents only 43% of what was verified in Cubatão, while in Guarujá it represented 78%. Between 2000 and 2006, this difference gradually decreased and Peruíbe reached 71% and Guarujá, 88%. Regarding the average of the last 10 years, there was an even higher decrease, with Peruíbe reaching a per capita expense equivalent to 86% of that of Cubatão, while the one of Guarujá was of 94% (Graph 10).
In relation to the respiratory diseases, the difference between Peruíbe and Guarujá compared to Cubatão has also been decreasing but, on the average of the period 2000 to 2009, the per capita expenses related to respiratory hospitalizations, comparatively, were of 82% and 92%, respectively. Graph 11 shows these proportions.
These differences in relation to the city of Cubatão can be attributed to the greater emission of pollutants (deduced from its larger industrial activity). Based on estimates, the lowest indexes that were verified were applied (namely, for Peruíbe, 86% for diseases of the circulatory system and 82% for diseases of the respiratory system), as a discount factor for the costs of Cubatão. The costs associated with pollution would be: 14% for diseases of the circulatory system and 18% for diseases of the respiratory system. Based on the previous item, the costs of pollution, in Cubatão, measured by their impacts based on hospitalizations, calculated from statistics of the SUS, were of R$ 3.44 million between 2000 and 2009.
Discussion and Conclusions
We observed, in the figures surveyed from 2000 to December 2009, a clear trend of decline in the number of hospitalizations occurred in the city of Cubatão. From 2000 to 2009, 8,799 hospitalizations due to respiratory diseases were registered in the Sistema de Informação Hospitalar (SIH-SUS Hospital Information System), and the majority (56.6%) of the patients was of the male sex. The hospitalization rate decreased from 1,162 hospitalizations per 100 thousand inhabitants to 469 in 2009, that is, it was reduced by 2.5 times. This decrease in the number of hospitalizations may be related to the greater control of air pollution in recent years and to the better resolvability of the cases of the disease before the need of hospitalization.
The rate is higher for the group of children younger than five years, followed by the group of individuals older than 60 years. From 2000 to 2009, the decrease in the number and rate of hospitalizations occurred predominantly in children younger than five years. And there is a trend of decline in the coming years.
The rate of mortality by respiratory diseases has remained constant, revolving around 60 deaths/100 thousand inhabitants. However, the most affected age groups were those of individuals older than 50 years and children younger than 1 year. It is important to highlight that, from 2000 to 2009, the decrease was of almost five times among children younger than 1 year.
Based on neighboring cities, and calculating the average per capita expense due to the two diseases, it was estimated that the costs directly related to air pollution in the city for the period 2000 to 2009 were R$ 3.44 million. These costs are quite conservative, as they were calculated from data available in public databases and did not cover other items that are taken into account in valuation studies, mentioned in the methodology. The costs per outpatient clinic assistances and per treatments performed at home were also not surveyed, as these data were not available. The costs of diseases of people who do not resort to the Brazilian National Health System for treatment were also not surveyed, due to the same reasons.
Therefore, it is recommended to the health sector that efforts are undertaken so as to amplify the collection, systematization and availability of assistance data, in order to enhance the knowledge of the impacts on health and on the deriving costs, enabling to take positions and to define more consistent policies and programs.
References
- ANDERSON, H. R. et al. Air pollution and daily mortality in London: 1987-92. British Medical Journal, London, v. 312, p. 665-9, 1996.
- COMPANHIA AMBIENTAL DO ESTADO DE SÃO PAULO. Qualidade do ar no Estado de São Paulo 2010 São Paulo: CETESB, 2011. Disponível em: http://www.cetesb.sp.gov.br/ar/qualidade-do-ar/31-publicacoes-e-relatorios Acesso em: 12 mar. 2011.
- DAUMAS, R. P.; MENDONÇA, G. A. S.; PONCE-DE-LEÓN, A. P. de. Poluição do ar e mortalidade em Idosos no município do Rio de Janeiro: análise de série temporal. Cadernos de Saúde Pública, Rio de Janeiro, v. 20, n. 1, p. 311-9, fev. 2004.
- DELUCCHI, M. A. Environmental externalities of motor vehicle use in the US. Journal of Transport Economics and Policy, Claverton Down, v. 34, p. 135-68, 2000.
- DELUCCHI, M.; McCUBBIN, D. R.; MURPHY, J. The health and visibility cost of air pollution: a comparison of estimation methods. Journal of Environmental Management, Berkeley, v. 64, p. 139-52, 2002.
- DESQUEYROUX, H.; MOMAS, I. Pollution atmosphérique et santé: une synthèse des études longitudinales de panel publiées de 1987 a 1998. Revue d'Epidemiologie et de Sante Publique, Issy les Moulineaux, v. 47, p. 361-75, 1999.
- GANGADHARAN, L.; VALENZUELA, R. Interrelationship between income, health and environment: Extendy the environmental Kuznets Curve hypothesis. Ecological Economics, Hanover, v. 36, p. 513-35, 2001.
- GARBER R, A. M.; PHELPS, C. E. Economics foundations of cost-effectiveness analysis. Journal of Health Economics, York, v. 16, p. 1-31, 1997.
- GARBER, A. M. et al. Theoretical foundations of cost-effectiveness analysis. In: GOLD, M. R. et al. Cost-effectiveness in health and medicine Oxford: Oxford University Press, 1996.
- GOUVEIA N.; FLETCHER, T. Respiratory diseases in children and outdoor air pollution in Sao Paulo, Brazil: a time series analysis. Journal of Occupational and Environmental Medicine, Chicago, v. 57, p. 477-83, 2000.
- KRUPNICK, A. et al. The value of health benefits from ambient air quality improvements in central and Eastern Europe: an exercise in benefit transfer. Environmental and Resource Economics, Washington , v. 7, n. 4, p. 307-22, 1996.
- McCUBBIN, D. R.; DELUCCHI, M. A. The health costs of motor vehicle related air pollution. Journal of Transport Economics and Policy, Claverton Down, v. 33, p. 253-86, 1999.
- MOMAS, I. et al. Urban atmospheric pollution and mortality: analysis of epidemiological studies published between 1980 and 1991. Revue d'Epidemiologie et de Sante Publique, Issy les Moulineaux, v. 41, p. 30-43, 1993.
- MURPHY, J. J.; DELUCCHI, M. A. A review of the literature on the social cost of motor vehicle use. Journal of Transportation and Statistics, Washington, v. 1, p. 15-42, 1998.
- OSTRO, B. Estimating the health effects of air pollutants: a method with an application to Jakarta. Policy Research Working Paper 1301 New York: The World Bank, 1998.
- PASTORE, J. Encargos sociais no Brasil e no exterior: uma avaliação crítica. Brasília: Sebrae, 1994.
- PEARCE, D.; MARKANDYA, A. An appraisal of the economic value of environmental improvement and the economic cost of environmental damage London: University College of London. Department of Economics, 1987. (Internal paper).
- POLONIECKI, J. D. et al. Daily time series for cardiovascular hospital admissions and previous day's air pollution in London, UK. Journal of Occupational and Environmental Medicine, Chicago, v. 54, p. 535-40, 1997.
- QUAH, E.; BOON, T. L. The economic cost o fair pollution on health in Singapore. Journal of Asian Economics, Bologna, v. 14, p. 73-90, 2003.
- SCHWARTZ, J. Air pollution and daily mortality: a review and meta analysis. Environ Res, Maryland Heights, v. 64, p. 36-52, 1994.
- SEROA DA MOTTA, R.; MENDES, A. P. Custos da saúde associados à poluição de ar no Brasil. Pesquisa e Planejamento Econômico, Rio de Janeiro, v. 25, n. 5, abr. 1995.
- SEROA DA MOTTA, R. Contabilidade ambiental: teoria, metodologia e estudos de casos no Brasil, Rio de Janeiro: Instituto de Pesquisa Econômica Aplicada, 1995.
- SUNYER, J. et al. Urban air pollution and emergency admissions for asthma in four European cities: the APHEA Project. Thorax, London, v. 52, p. 760-5, 1997.
- TOULOMI, G.; SAMOLI, E.; KATSOUYANNI, K. Daily mortality and "winter type" air pollution in Athens, Greece a time series analysis within the APHEA project. Journal of Epidemiology & Community Health, London, v. 50, p. 47-51, 1996.
- WORLD HEALTH ORGANIZATION. Air quality guidelines for particulate matter, ozone, nitrogen dioxide and sulfur dioxide: global update 2005. Geneva: WHO, 2005.
- ZANOBETTI, A.; SCHWARTZ, J.; DOCKERY, D. W. Airborne particles are a risk factor for hospital admissions for heart and lung disease. Environ Health Perspect, North Carolina, v. 108, p. 1071-7, 2000.


Publication Dates
-
Publication in this collection
24 Oct 2012 -
Date of issue
Sept 2012
History
-
Received
05 Oct 2011 -
Accepted
12 Apr 2012