
Summary
Objective:
the aim of this study was to investigate the addition of elastography to the BI-RADS® lexicon for the classification of breast lesions.
Methods:
a total of 955 consecutive patients who were subjected to breast percutaneous biopsy from January 2010 to December 2012 were retrospectively assessed. Overall, 26 patients who did not present with masses on conventional ultrasound were excluded. The patients were classified according to the fifth edition of the breast imaging and reporting data system (BI-RADS®) lexicon, which includes elastographic findings. The BI-RADS®classification is based on the same classification principles that have been suggested by the author, which classify lesions as soft, intermediate, or hard.
Results:
the addition of elastographic findings to the BI-RADS® lexicon improved the sensitivity (S), specificity (SP), and diagnostic accuracy (DA) of ultrasound in the assessment of breast lesions, which increased from 93.85, 72.07, and 76.64 to 95.90, 80.65, and 91.39%, respectively.
Conclusion:
these findings suggest that the addition of elastography to the BIRADS ® lexicon will improve the SP and DA of ultrasound in the screening of breast lesions.
Keywords:
ultrasonography; interventional; breast diseases; adenocarcinoma; breast cyst; breast ductal carcinoma; breast neoplasms
Resumo
Objetivo:
investigar o impacto da adição da descoberta da elastografia das lesões mamárias à classificação segundo o léxico BI-RADS®.
Métodos:
estudo retrospectivo com 955 pacientes consecutivas, submetidas à biópsia mamária percutânea no período de janeiro de 2010 a dezembro de 2012. Foram excluídas 26 pacientes que apresentaram lesão não nodular ao ultrassom convencional. As lesões foram classificadas conforme proposta da 5ª edição do léxico BI-RADS®, que inclui os achados de elastografia. A classificação BI- -RADS® é baseada nos mesmos critérios propostos pelo autor, que classifica as lesões como macias, intermediárias e rígidas.
Resultados:
a adição dos achados da elastografia ao léxico BI-RADS® melhorou a sensibilidade (S), a especificidade (E) e a acurácia diagnóstica (AD) do ultrassom na avaliação das lesões mamárias, de 93.85, 72.07 e 76.64% para 95.90, 80.65 e 91.39%, respectivamente.
Conclusão:
os achados sugerem que a adição dos achados da elastografia ao léxico BI-RADS® pode melhorar a S, a E e a AD do ultrassom no rastreamento de lesões mamárias.
Palavras-chave:
ultrassonografia de intervenção; doenças mamárias; adenocarcinoma; cisto mamário; carcinoma ductal de mama; neoplasias da mama
Introduction
The fifth edition of the breast imaging and reporting data system (BI-RADS®), an ultrasound atlas, was updated to include the assessment of the elasticity of breast lesions using elastography.
Elastography was developed as an additional tool for ultrasound studies in the 1990s.1 The first corresponding clinical studies were conducted in the early 2000s, and elastography was eventually included in the latest edition of the BI-RADS® lexicon. The addition of elastography to the lexicon aimed to improve the specificity (SP) of ultrasound, because low SP is currently a major barrier to the wide application of ultrasound in clinical practice. This study assessed the elasticity of breast lesions, using elastography combined with conventional findings that are suggested in the BI-RADS® lexicon. In addition, this study investigated the impact of elastography in routine testing.
Methods
A total of 955 patients who were referred to the Computed Tomography Center (CTC – Centro de Tomografia Computadorizada, São Paulo, SP, Brazil) for percutaneous biopsy of breast nodules from January 2010 to December 2012 were retrospectively and consecutively assessed. All of the patients signed an informed consent form. Institutional review board approval was not required.
Overall, 26 patients who did not present with nodular lesions on ultrasound before biopsy were excluded.
A total of 929 lesions were included in the study. The lesions were assessed using ultrasound and elastographic techniques that have been previously described by the author.
Both the conventional and elastographic studies were performed by two radiologists with 6 and 17 years of experience in breast imaging, respectively. Examinations were performed using a Sonix SP (Ultrasonix Medical Corporation, Vancouver, Canada) US system and a 5–14-MHz multi-frequency linear probe. For the elastography study, special software was used for the Ultrasonix system, version 3.0.2 (Beta1), upgraded to the commercial version 2.6.
The lesions were first classified according to the BI-RADS® lexicon and, then, classified based on the elastographic findings. Using the BI-RADS® lexicon criteria, the masses were classified according to their shape, orientation, margin, echo pattern, posterior acoustic features, and vascularity. Using the elastographic criteria, the lesions were classified as soft, intermediate, or hard22 ACR BI-RADSTM Atlas. 5.ed. [cited 2014 jan 25]. Available at: http://www.acr.org/Quality-Safety/Resources/BIRADS.
http://www.acr.org/Quality-Safety/Resour...
(Figure 1). The techniques that were used in the elastographic classification have been previously described.33 Fleury EF, Fleury JC, Piato S, Roveda Jr D. New elastographic classification of breast lesions during and after compression. Diagn Interv Radiol. 2009; 15(2):96-103.,44 Fleury EF, Fleury JC, Olibeira VM, Rinaldi JF, Piato S, Roveda Jr D. Proposal of the systematization of the elastographic study of mammary lesions through ultrasound scan. Rev Assoc Med Bras. 2009; 55(2):192-6. The final classification of the lesions was based on the BI-RADS® ultrasound assessment categories and the elastographic findings (Table 1).
A combination of the classification principles that have been suggested by the authors and the definitions in the BI-RADS®.
The final classification of breast lesions after the addition of elastographic findings (soft, intermediate, or hard) to the BI-RADS® classification.
The positive predictive value (PPV), negative predictive value (NPV), sensitivity (S), SP, and diagnostic accuracy (DA) of the BI-RADS® classification, with and without the elastographic data, were determined and compared.
Results
Table 2 describes the final results of the BI-RADS® classification, with and without the elastographic data. In addition, Table 2 describes the distribution of the lesions according to both systems of classification and the distribution of false positive (FP), false negative (FN), true positive (TP), and true negative (TN) results. The PPV, NPV, S, SP, and DA results for the ultrasound-based BI-RADS®classification were 47.16, 97.78, 93.85, 72.07, and 76.64%, respectively. The corresponding results for the BI-RADS® classification combined with the elastographic data were 56.84, 98.67, 95.90, 80.65, and 91.39%, respectively.
Frequency of the BI-RADS® categories for the lesions that were classified with (BI-RADS® Elastography) and without (BI-RADS®) elastographic findings. True positive (TP), true negative (TN), false positive (FP), and false negative (FN) findings. The positive predictive value (PPV), the negative predictive value (NPV), the sensitivity, the specificity, and the diagnostic accuracy of each method were assessed.
Discussion
The introduction of elastographic findings into the BI-RADS® lexicon serves as an additional tool to improve the SP and DA of ultrasound in the screening of breast lesions. The low SP of current ultrasound techniques has led to a large number of FP results, which often necessitate diagnostic biopsies. The low SP of ultrasound hinders its use in the routine diagnostic screening of breast lesions.
Elastography requires the coupling of specific software and an ultrasound device to assess the softness of tissue in areas of interest. This method is based on the assumption that benign lesions tend to be softer than malignant lesions. Elastography software is currently included in most commercial ultrasound devices; however, this software has not been standardized. This software may be used for a qualitative assessment of lesions, which is based on the visual evaluation of changes in color in the area of interest; however, this type of assessment is subjective. In a quantitative assessment, the degree of hardness in a lesion is estimated using objective data. Compressions to induce the required deformation may be performed manually or using specific probes, such as acoustic radiation force impulse (ARFI) and shear-wave imaging.55 Ko KH, Jung HK, Kim SJ, Kim H, Yoon JH. Potential role of shear-wave ultrasound elastography for the differential diagnosis of breast non-mass lesions: preliminary report. Eur Radiol. 2014; 24(2):305-11.,66 Barr RG, Zheng Z. Shear-wave elastography of the breast: value of a quality measure and comparison with strain elastography. Radiology. 2015; 275(1):45-53.
Even with the introduction of these new technologies, there seems to be a convergence in the literature to adopt the qualitative criteria for the evaluation of breast masses as a standard, rather than quantitative criteria. The reason for this is that ultrasound is, in essence, a subjective method of image interpretation, which depends on the experience and training of the examiner. Lesions deeper than 2 cm are less accurately characterized by means of shear-wave elastography.77 Hooley RJ, Scoutt LM, Philpotts LE. Breast ultrasonography: state of the art. Radiology. 2014; 268(3):642-59.
The latest edition of the BI-RADS® atlas includes elastographic findings, and lesions are classified as soft, intermediate, or hard. This classification is based on the same principles that were suggested by the authors, in 2008.
Table 2 shows that most (482, 51.9%) of the lesions in the patients who were referred to our center for percutaneous biopsies were classified as category 3 (most likely benign), according to the BI-RADS® lexicon. The risk of malignancy in category 3 lesions is low (less than 2%), and these lesions are typically fibroadenomas. Patients with category 3 lesions are often subjected to percutaneous biopsy for a clearer diagnosis or because of patient anxiety.
In a 2009 study, the authors described variations in the elastographic findings for fibroadenomas, which exhibit a highly variable presentation, due to their histological complexity. Fibroadenomas include both soft and hard lesions. It was observed that the most indolent fibroadenomas (hypocellular with collagen) appeared softer on elastographic assessment, whereas the complex and hypercellular lesions were harder.88 Fleury EF, Rinaldi JF, Piato S, Roveda Jr D. Appearance of breast masses on sonoelastography with special focus on the diagnosis of fibroadenomas. Eur Radiol. 2009; 19(6):1337-46. Elastography allows for an unequivocal diagnosis in complicated cysts.99 Fleury EF, Rinaldi JF, Piato S, Fleury JC, Roveda Jr D. Features of cystic breast lesions at ultrasound elastography. Radiol Bras. 2008; 41(3):167-72.Because of the inclusion of elastographic data in the BI-RADS®lexicon, in this study, a large number of lesions that would have been classified as BI-RADS® category 3 (most likely benign and soft) were reclassified as BI-RADS® category 2 (benign). Patients with benign lesions would be referred back to screening. The number of lesions that were classified as category 3 decreased from 483 to 256, i.e., a decrease of approximately 47%. In addition, the number of lesions that were classified as category 2 consequently increased from 59 to 344, i.e., an increase of approximately 483%. The lesions with intermediate elasticity should remain in category 3, whereas hard lesions should be reclassified as BI-RADS® category 4a, i.e., lesions that would require further diagnostic elucidation.
Elastography may impact lesions that are classified as BI-RADS®category 4a, which include lesions that meet most of the criteria for benign lesions, but would benefit from further investigation with diagnostic methods or short-term follow-up. The classification of soft lesions would shift from category 4a to category 3, for which short-term follow-up (usually 6 months) is recommended. The risk of malignancy in lesions that are classified in the BI-RADS® lexicon as category 4a varies from 2-10%. The inclusion of elastographic findings would not significantly impact the recommendations that are suggested in the BI-RADS® atlas for lesions that are classified as categories 4b, 4c, and 5. In such cases, the morphology of the lesions is considered the most relevant criterion when malignancy is suspected, and the elastographic findings do not impact the recommendations in the BI-RADS® lexicon. Clinical reports suggest that certain histological tumor types appear soft on elastography, such as high-grade ductal carcinoma, mucinous carcinoma, and papilliferous carcinoma. In such cases, the lesion morphology or growth pattern is significantly suspicious, and morphology is the decisive criterion for classification.
The results of this study demonstrate that the use of elastography as recommended in the latest edition of the BI-RADS® lexicon improved the SP and DA of ultrasound, which increased from 72.0 to 80.65% and from 76.64 to 91.39%, respectively. The S of this method did not significantly change (increased from 93.85 to 95.90%).
A limitation of this study is that this analysis was conducted at a single center for breast cancer patients. Further studies are needed to validate the results.
The use of elastographic findings according to the recommendations in the latest edition of the BI-RADS® lexicon may improve the SP and DA of ultrasound in the screening of breast cancer. Therefore, use of ultrasound as a screening and diagnostic method for this condition may increase.
-
Study conducted at Faculdade de Ciências Médicas da Santa Casa de São Paulo, São Paulo, SP, Brazil
References
-
1Ophir J, Céspedes I, Ponnekanti H, Yazdi Y, Li X. Elastography: a quantitative method for imaging the elasticity of biological tissues. Ultrason Imaging. 1991; 13(2):111-34.
-
2ACR BI-RADSTM Atlas. 5.ed. [cited 2014 jan 25]. Available at: http://www.acr.org/Quality-Safety/Resources/BIRADS.
» http://www.acr.org/Quality-Safety/Resources/BIRADS -
3Fleury EF, Fleury JC, Piato S, Roveda Jr D. New elastographic classification of breast lesions during and after compression. Diagn Interv Radiol. 2009; 15(2):96-103.
-
4Fleury EF, Fleury JC, Olibeira VM, Rinaldi JF, Piato S, Roveda Jr D. Proposal of the systematization of the elastographic study of mammary lesions through ultrasound scan. Rev Assoc Med Bras. 2009; 55(2):192-6.
-
5Ko KH, Jung HK, Kim SJ, Kim H, Yoon JH. Potential role of shear-wave ultrasound elastography for the differential diagnosis of breast non-mass lesions: preliminary report. Eur Radiol. 2014; 24(2):305-11.
-
6Barr RG, Zheng Z. Shear-wave elastography of the breast: value of a quality measure and comparison with strain elastography. Radiology. 2015; 275(1):45-53.
-
7Hooley RJ, Scoutt LM, Philpotts LE. Breast ultrasonography: state of the art. Radiology. 2014; 268(3):642-59.
-
8Fleury EF, Rinaldi JF, Piato S, Roveda Jr D. Appearance of breast masses on sonoelastography with special focus on the diagnosis of fibroadenomas. Eur Radiol. 2009; 19(6):1337-46.
-
9Fleury EF, Rinaldi JF, Piato S, Fleury JC, Roveda Jr D. Features of cystic breast lesions at ultrasound elastography. Radiol Bras. 2008; 41(3):167-72.
Publication Dates
-
Publication in this collection
Jul-Aug 2015
History
-
Received
08 Dec 2014 -
Accepted
19 Feb 2015

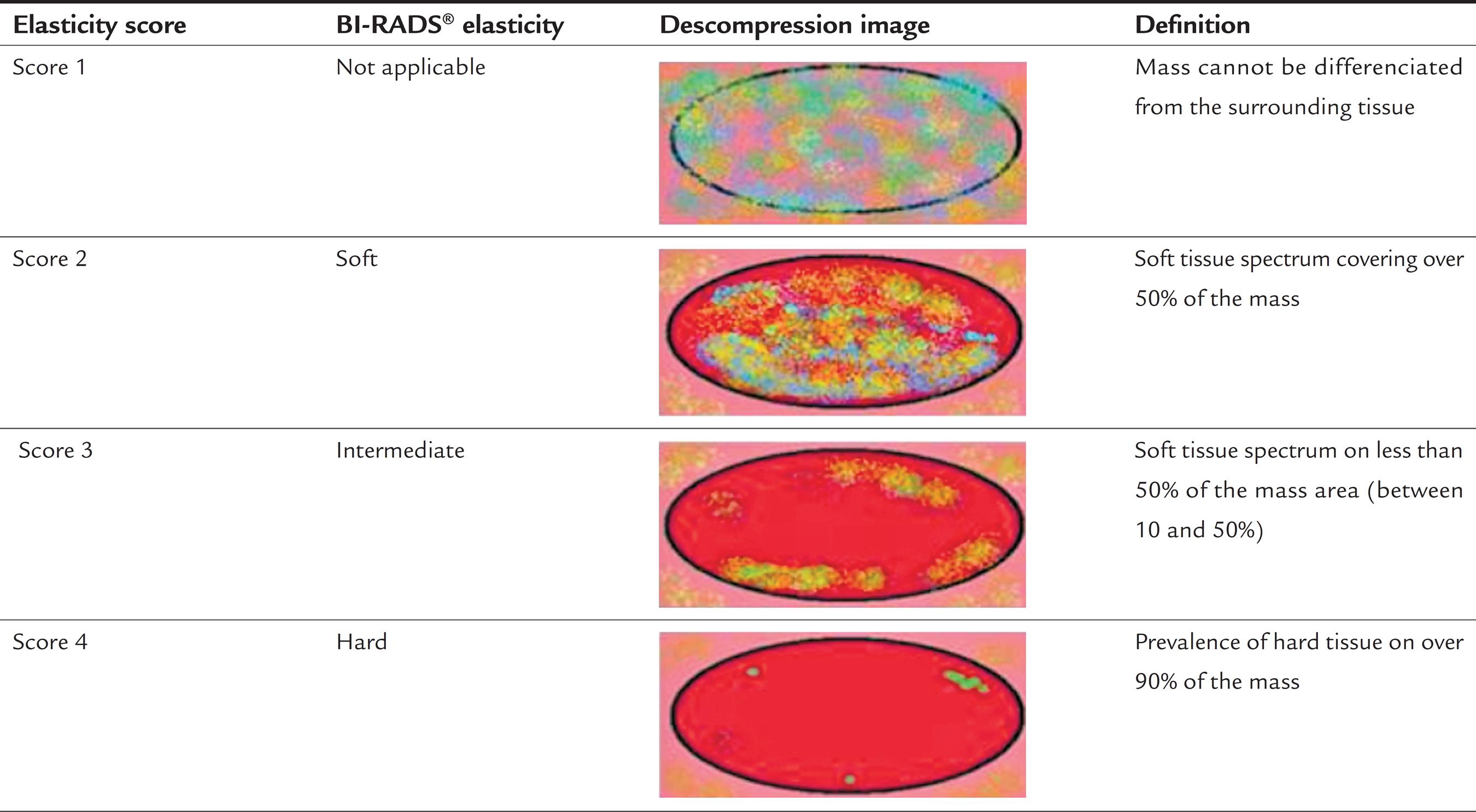 Image courtesy of author.
Image courtesy of author.