Abstracts
In this article we examine advertising material for erectile dysfunction drugs in order to analyse the discourses of pharmaceutical marketing. Embedded within a cycle that both contributes to, and feeds from, existing notions, advertisements directed towards doctors deploy new ideas related to nosological categories, while at the same time re-enforcing traditional gender/sexuality paradigms. Male sexuality, traditionally represented as "wild" and "unruly", is (re)normalised. The biomedicalized "new man", sexually potent, confident and stiff, is a hybrid of body and technology, found in the dissolving boundary between nature and culture.
Biomedicalization; Masculinities; Gender; Sexuality; Advertising
Neste artigo utilizamos material publicitário de drogas para tratamento da "disfunção erétil" para analisar os discursos do marketing farmacêutico. Num ciclo de realimentação, as propagandas voltadas aos médicos veiculam novas concepções relacionadas a categorias nosológicas, enquanto reforçam noções tradicionais de gênero/sexualidade. A sexualidade masculina, tradicionalmente representada como "selvagem", "incontrolável", é (re)normatizada. O "novo homem" biomedicalizado, sexualmente potente, confiante e rígido é um produto híbrido corpo-tecnologia, na fronteira esfumaçada entre natureza e cultura.
Biomedicalização; Masculinidades; Gênero; Sexualidade; Propaganda
Man with a Capital 'M'. ideas of masculinity (Re)Constructed in Pharmaceutical Marketing
Ilivifaro@gmail.com:CLAM/IMS/UERJ
IIliliankc@gmail.com:CLAM/IMS/UERJ
IIIfabiola.rohden@gmail.com ?:CLAM. UFRGS
IVjane.russo@gmail.com:CLAM/IMS/UERJ
ABSTRACT
In this article we make use of marketing material for medication for the treatment of 'erectile dysfunction' to analyse pharmaceutical marketing discourses. In a feedback cycle, the advertisements, intended for doctors, both carry new conceptions related to nosological categories, at the same time as traditional notions of gender/sexuality. Masculine sexuality, traditionally represented as 'wild', or 'uncontrollable', is (re)normatised. The 'new man', biomedicalised, sexually potent, confident, and rigid, is a hybrid body/technology product at the vague frontier between nature and culture.
Key words: Biomedicalisation (biomedicalization); masculinity; gender; sexuality; advertising.
The time has come to show the capital M at the heart of every Brazilian Man.
(Advertising for the medication Helleva®, produced by Cristália Laboratories).
INTRODUCTION
In this article, we will analyse advertising material and announcements aimed at doctors, of four pharmaceutical companies, for the treatment of so-called "masculine sexual dysfunctions". The material was collected in ethnography undertaken in two congresses, one for sexology and the other for sexual medicine.
Until the end of the 1990s, the medical treatments available for impotence, such as injections in the penis right before intercourse or penial implants, all had in common an invasive character. The attempts at establishing direct connections between the serum levels of testosterone and masculine sexual dysfunctions were inconclusive. In 1991, the launching of sildenafil citrate
Some decades prior, the classic studies of Masters and Johnson had constructed a model of comprehension of human sexual activity, the "cycle of sexual response", conceived as 'psycho-physiological', placing in one side the psychogenetic causes and the organic causes, such as diabetes, on the other. From a practical point of view, the mode of intervention available, only involved the 'psycho' element or compartment (Masters & Johnson, 1966, 1970; Giami, 2009b, p.640). In 1977, Helen Kaplan reelaborated this model and proposed a version that is used up until the present day as a reference: a cycle composed of three successive psycho-physiological phases, that is, desire, excitation and orgasm (Kaplan, 1977). These studies caused a dislocation of standard ideas of impotence and frigidity to that of 'sexual dysfunction', by way of the discrimination and normatisation of the 'phases of the sexual response cycle'. This movement configures what Faro (2009a, p. 10-11) conceived of as the "psychomedicalisation" of sexuality.
The public injection of phenoxibenzamine by Dr. Giles Brindley into his own penis at a urology conference, in 1983, has been a performance transformed into the origin myth in the history of interventions into impotence (Rohden, 2009, p. 98; Marshall & Katz, 2002, p. 54). Beyond the conspicuous erection, it has reinforced the concept of male arousal as a 'physiological event', disassociated from the psychological component of sexual desire. We can understand this bizarre 'inaugural moment' as a landmark signifying the biomedicalisation of masculine sexual activity. One sees, throughout the 1980s, an increase in the amount of research and scientific articles about masculine sexual dysfunctions and their treatment, which implied an important inflexion for the field of clinical sexology. In the first place, the psychogenic conception of impotence was downplayed in favour of a predominantly organic conception. As such, it has been necessary a change in the diagnostic category itself that, according to the analysis of Lakoff (2005), needed to become "operationable". The category of impotence, with its heavy symbolic weight and tendency to absorb the subject as a whole, was gradually abandoned in favour of the term 'erectile dysfunction', defined as
The persistent incapacity to attain or maintain sufficient rigidity in the erection to have sexual relations. The degree of erectile dysfunction is variable and can be situated between a partial reduction of penial rigidity and an incapacity to maintain an erection, and the total absence of erection. This definition is limited to the erectile capacity of the penis and does not include libidinal problems, and problems with ejaculation or orgasm. (Krane et al., 1989, apud Giami, 2009b, p. 641).
The increase in the number of studies about masculine sexuality during the 1980s within a generally medicalised framework (Giami, 2009b; Faro, 2008), contributed in a marked fashion to the construction of a technological frame conducive to biomedicalisation.
The development of pharmacological technologies destined for the 'resolution' of a new nosological category (ED) has a double aspect: to simultaneously respond to the constructed and consolidated demand of this very category as a 'medical problem' to be 'resolved', clearly showing the circularity of the process of medicalisation/biomedicalisation. We would be, therefore, facing the co-construction of technologies and consumers: new molecules, and 'real' or 'potential' patients with ED. This contemporary focus on the male and the reduction of masculine sexuality to the erection embody the process of biomedicalisation of sexuality in the late 20th century.
By way of a more general problematisation that mixes sexuality and age as fundamental dimensions of the modern subject, Barbara Marshall and Stephen Katz (2002), amongst others, highlight the importance of lifestyle cultures at the end of the last century. These cultures, by emphasizing health, activity, and the avoidance of ageing, were part of a broader process, which gave birth to a vast field of studies and interventions regarding the penetrative capacity of the masculine sexual organ. According to the authors, the great novelty is that one goes from a conception that admits the decline of sexual life across the passage of time, and in which one even judges negatively sexual activity in old age, to another, in which one is obliged to have good sexual performance until the end of one's life. Beyond this, sexual activity is advocated as the very necessary condition for a healthy life, and erectile capacity would define virility throughout the course of masculine life (Marshall & Katz, 2002; Marshall, 2006).
The important argument raised by the bibliography regarding this theme is that it was initially necessary to transform erectile dysfunction into a problem, in order to show that this could affect any man, at any stage of life. Equally, according to this logic, it was emphasised that a drug capable of 'resolving' or 'preventing' this difficulty was already available. In this sense, Viagra would be part of the group of so-called life-style drugs or comfort medicines, intended to improve individual performance; a market clearly in expansion. Furthermore Pfizer also invested in promoting the idea of erectile dysfunction as an acceptable topic for public discussion, which would lead to a greater search for treatment on the part of patients (Lexchin, 2006).
According to Meika Loe (2001) the development of this new material and cultural technology was related to the propagation of an idea of masculinity in crisis, illustrated especially through the metaphor of the erection. The notion that the erection, a symbol of virility and masculine identity, is effectively unstable and subject to various types of mishaps seems to increasingly gain attention. Furthermore, it is precisely to combat this lack of control or uncertainty regarding the masculine body that the industry offers a resource like Viagra, which would guarantee the expectation of an always improved performance (Grace et al, 2006).
As Brigeiro and Maksud point out, Viagra was launched in Brazil on the 1st of June, 1998 and "no other medicine had been dealt with by the Brazilian print media with the same level of interest and variety of approaches, being dealt with in diverse sections and columns" (Brigeiro & Maksud, 2009, p. 74). The analysis of the advertising campaigns for Viagra in various countries has shown how the medication transformed itself into something intended to improve sexual performance without restriction to a specific group.
The idea of a 'crisis of masculinity' has been used to explain, not just the emergence of erectile dysfunction as a medical issue, but also the 'incredible success' of the drugs produced to treat it.
At the same time, the medicalisation of reproduction (and of the female body) led to the release onto the market of the birth control pill, a biotechnological event that had profound consequences in the transformations mentioned above. According to Loe, the pill, by removing obstacles that sustained a double sexual morality, transformed women into "critical consumers of masculine performance" (Loe, 2004, p.13), increasing the anxiety of heterosexual men regarding the traditional definitions of masculinity. Developing further this line of inquiry, Loe affirms that the new reproductive technologies from the middle of the 20th century were precursors for sexual pharmacology. According to Loe, the new oral contraceptives served as catalysts and barometers of the changes in social attitude regarding science, technology, and medicine. By having as their objective a body and lifestyle transformation of its users (and not a cure for a disease), they could be considered the first lifestyle drugs in the field of sexuality. For this author, the Viagra era represents the emergence of a masculinity recovery movement based on a drug, and the re-emergence of the male body as a locus of confidence and control through an intense investment (financial and scientific) in the restoration or improvement of "masculine sexual potential" (Op. Cit.).
The strictly organic definition of sexual potency, leaving aside affective, social, or moral definitions, removes it from the struggles regarding definitions of gender. It is as if urologists (and the pharmaceutical industry) had provided the disorientated men a way by which masculine potency, by being translated into purely physical terms as erectile potency, could be 'improved'. In this manner, masculine (re)empowering necessarily implies the biomedicalisation of masculine sexuality, resulting in important transformations in the very definition of this sexuality.
A new facet of this phenomenon, especially visible in the Brazilian case, is the way ED is being used as a 'decoy' for public policy in programs of prevention for chronic conditions in men (Carrara et al., 2009). This issue was made explicit by the then Health Minister José Gomes Temporão, whose declaration on the matter produced innumerable, highly significant jokes.
Rohden (2009) points out the role of the gender differences in the configuration of the field of sexual medicine, considering that the prevailing perspective reduces the sexual experience of men to the anatomic-physical norm of erection, most of the time considered only in the context of heterosexual relations. In the masculine case, the model of Masters & Johnson, according to which sexuality is viewed as the combination of bio-psycho-socio elements and as something that has to do with the couple, is left aside. Men are presented as individualised beings by way of a description of their corporal economy, and deprived of interiority (when compared to women). When it comes to women, the description tends to include relational issues, especially those regarding the moral-affective quality of the couple. Beyond this, in their case, a paradoxical key for our comprehension is added. If, on one hand, there is an insistent reference to the supposed complexity of feminine sexuality, which would be more influenced by affective and relational issues, on the other hand there is the constant recourse to the masculine model, be it "basic" research about feminine sexuality or as the standard for investments in diagnosis and treatment of the female 'dysfunctions'.
In this article, via the analysis of the advertising of drugs for ED intended for doctors, we propose to explore what certain forms of biomedicalisation reveal about the (re)construction of masculinity.
As Elaine Rabello shows,
(...) [A]dvertising does not create values, but rather uses those that are already circulating in the society and reformulates them for presentation to the public through advertising. Owing to this, the media becomes a useful vehicle for the comprehension of what the society legitimates as a desirable lifestyle. In this way, it is of interest to the pharmaceutical industry to give a name and a substrate to the desire for total wellbeing and performance through the process of reification, attributing materiality to a brand or product which, being swallowed, can enter the body (the stage of the experiences of wellbeing and productivity) and "produce" the desired "health" effects, thanks to science, to technology, and thanks to who, obviously, makes all of this available in the form of a product (Rabello, 2010, p. 31).
In the same way the presuppositions regarding masculinity inform the marketing of drugs for ED, the distinct substances whose 'actions' manifest themselves differently in terms of the promised erection indicate what would be the 'desirable' attributes for 'adequate' masculine performance. This performance would possibly be the summation of all the attributes associated to these substances. At the same time, the number of requirements for such a qualification shows it to be an unattainable ideal: 'complete' masculinity which, according to these parameters, reveals itself in the final analysis to be a mission impossible to achieve. One of the roles played by the marketing consists precisely in the incessant incitement of the search for this ideal, with many very often unsubtle promises.
MATERIAL AND DISCUSSION
Our empirical data was constituted by leaflets obtained in observations undertaken in the two congresses, one of sexology and the other of sexual medicine; the XI Brazilian Congress of Human Sexuality, Recife, 2007 and the X Congress of the Latin American Society of Sexual Medicine, Florianópolis, 2009, respectively. The second event is part of the implantation and development of sexual medicine, an area that has sought to affirm itself as autonomous in relation to sexology. In the field of studies/interventions into sexuality, it situates itself in the most radical stream of the biomedical paradigm, and has established a hegemonic relation with clinical sexology:
One can perceive that the supporters of sexual medicine, in the great majority urologists, tend to apply pressure to what until then had functioned as a more dispersed field in terms of definitions and demarcations of boundaries, in order to transform it into a body with clearer frontiers between the different attributions and functions (doctors practice medicine, psychologists practice psychotherapy, educators practice/orient sexual education). From this point of view the designation "sexologist" or "sexology", which seems to refer naturally to the period of implantation of the field and to a moment of greater dispersion of definitions and frontiers, is abandoned in the name of more precise designations, which concentrate specialties also clearly demarcated (Russo et al, 2011, p. 134).
Russo et al. (Op. cit.) propose a map of the studies and interventions into sexuality, which helps to contextualize the congresses studied in these ethnographies. The authors suggest that sexology and sexual medicine, that have a medico-psychological perspective in common, correspond to parts of a more ample aggregate that gathers different kinds of knowledge and of interventions into sexuality. This broader field is also composed by approaches centred on political activism and by studies developed by the social/anthropological sciences. Sexology appears as a term which has been losing prestige, with the tendency to be superseded, and refers to a field which structured itself along two subfields, clinical and educational sexology. While the educational subfield positioned itself in the interface between the three approaches of the field of knowledge and interventions regarding sexuality, having conceptions now more political and social, now more biological, clinical sexology, just as with sexual medicine, characterises itself by the naturalising presuppositions of the medico-psychological vision (Op. cit., p.134).
Congresses and events play an important role in the constitution and institutionalisation of this field, especially because it is an area that tends to be ignored in undergraduate and graduate courses.
Information packs in couché paper were obtained, with four colour printing and quite luxurious productions. There was a fairly constant pattern in these packs: on the first page was an attention grabbing headline, with a strong border, graphics on the next page and, on the last page, information in small lettering with diverse bibliographical references.
We worked with the advertising of four drugs: Viagra® (sildenafil citrate) of Pfizer, Cialis® (tadalafil) of Eli Lilly from Brazil, Levitra® (vardenafil) of Bayer Schering Pharma, and Helleva® (lodenafil carbonate), of Cristália Chemical Products and Pharmaceuticals Ltd., whose slogan transformed itself into the epigraphy of, and inspired the title of this study. The informational material of Levitra included advertising for Nebido®. Cialis, Levitra, Helleva, and Viagra are drugs for ED. Nebido, with a testosterone base, aims at treating hypogonadism or 'androgen deficiency in the aging male' - ADAM.
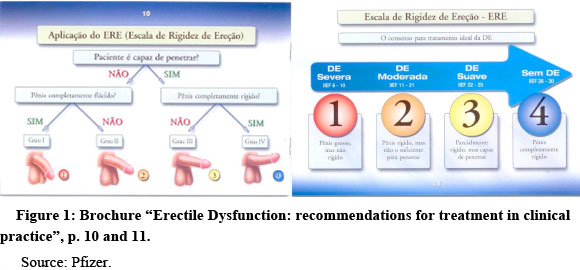
The anatomical illustrations of penises were accompanied on the opposite page by the specification of the "Scale of Hardness of the Erection (SHE): 1st Degree - severe ED: thick penis but not rigid; 2nd degree - moderate ED: rigid penis, but not sufficient for penetration; 3rd degree - mild ED: partially rigid, but still able to penetrate; 4th degree - without ED: penis totally rigid".
One of the brochures for Viagra (entitled "Hardness is the aim") illustrated, in a manner so as to leave no margin for doubt, the 'degree of hardness of the erection' (Figure 2). Rectangles of an increasing size, arranged from left to right, contained the following images: 1st degree - water; 2nd degree - sand; 3rd degree - braided straw, and 4th degree - a blue wooden board, with the wood grain drawn in.
By contrast, BSP also distributed copies of urologists' papers, with authors' photos and a complete bibliography, in which clinical cases were presented. One of these leaflets, although dealing exclusively with the use of Levitra, nevertheless had an advertisement for Nebido at the end: a double page spread in which the term ADAM featured prominently, accompanied by an asterisk in which the acronym was spelled out didactically as "androgenic deficiency of the ageing male". Another leaflet, dealing with diabetes, discussed the lowering of testosterone levels, recommending Nebido while also featuring an advertisement for the drug. A different brochure entitled "Sexual health as a gateway for male health" dealt exclusively with testosterone deficiency, for which the 'tried and true' therapeutic choice was Nebido.
Comparing Pfizer and PSB's materials, the simplicity of the former when compared to the complexity of the latter is noticeable, which included detailed academic format articles. A hypothesis for this difference is that Pfizer was manufacturing a product that was already in a stage of stabilisation
Beyond a strategy of 'scientifically' legitimising the efficacy of the drugs, there was a battle underway for dominance of the market, in which a drug's 'qualities' were compared to those of its competitors. Pfizer's talking points were 'hardness', and the fact that Viagra was the first drug approved for ED, as we can see in the slogans found in their promotional brochures: "Hardness is important" and "Only Viagra is Viagra" were added to the image of the blue rhomboid pill strangely balanced on one of its corners, that is, 'standing up'. Various double-entendres and ambiguous images were scattered throughout the promotional material: "Viagra, sildenafil citrate. A solid relationship with hardness"; a stone sculpture of an embracing couple. The predominant colour used was blue, a 'masculine' colour and the colour of the marketed pill, indicating that with extreme hardness everything becomes 'blue'.
Cialis is currently the bestselling iPDE5
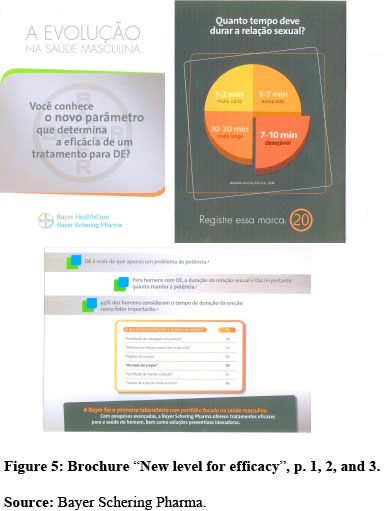
Commensurate with the stage of diffusion, the emphasis of Levitra's campaign was on its "novelty" in establishing a "new level of efficacy for ED treatment" in this way prolonging the "duration of sexual intercourse". In one of the drug's brochures a pie chart, divided in four segments, specified and standardised the ideal duration: "1-2 minutes (too short); 3-7 minutes (adequate); 10-30 minutes (too long); 7-10 minutes (desirable)". This last slice was slightly detached from the rest, to prevent any possible misinterpretation of the chart (Figure 5).
If Pfizer subtly emphasised Viagra's status as the first ever treatment for ED ("Only Viagra is Viagra"),
Another BSP brochure established the equation "Couple's satisfaction = longer duration of sexual intercourse = new parameter for efficacy". In a pedagogic illustration of the process of creating a technological framework favourable to several of their products, their slogan emphasised how "Levitra® prolongs the duration of sexual intercourse up to three times longer in patients with ED both with or without comorbidities" (our emphasis). As a bonus, was the promise that the drug would have a '3 in 1' role: by satisfying its claim of prolonging "up to three times longer the duration of sexual intercourse" (our emphasis), a 'too short' episode of intercourse of 1-2 minutes, following the previously mentioned pie chart on the desired length for sexual intercourse (Figure 5), would reach the 3-6 minute 'adequate' band, nearly arriving at a 'desirable' intercourse of 7-10 minutes. From this, we can hypothesize that, at this stage of the drug's promotion, it could also reach premature ejaculators. Even those in the 'adequate' band could be 'upgraded' to 'desirable', in a potential use of Levitra as an enhancement or lifestyle drug (Azize, 2006).
Following the logic of their competitors' avant-garde advertisements, Helleva
When compared to the promotional material for Viagra and Levitra, both quite discreet in their promises for a conspicuous masculinity, Helleva was quite explicit: "It is time to show the capital M at the heart of each and every Brazilian Man" was the slogan that accompanied the capital H,
According to the graphs that compared the rate of absorption of the drug when taken on an empty stomach or when taken with alcohol, use in conjunction with alcohol or food would not interfere with the drug's absorption. On the contrary, the performance of the drug would actually improve in these cases. This was presented as an advantage, in stark contrast with Viagra, which needs to be taken on an empty stomach to be effective.
The image of a cake with white icing and colourful sugar chips, with a capital H instead of the traditional birthday candle (or the cherry on top), found in the third page of Helleva's brochure is pregnant with meanings: it can be related to the association between the use of Helleva and celebration, the possibility of having a sexual feast after a gastronomic one, the feast of having your capital M (capital H in the original) optimised and not be let down at the 'key' moment.
Presenting the drug as innovative was compatible with Helleva still being in its promotional phase, while being the "first synthetic product developed in Brazil" which would give the drug a certain seniority and credibility in Brazil. Cristália's main slogan is "Innovation is in our DNA. Cristália is the Brazilian-owned pharmaceutical company that invests more in research, development, and innovation", a slogan that features prominently on their website, alongside the information that the company received the FINEP
In a public announcement published in the O Estado de São Paulo newspaper, Temporão
Thus, the collaboration between Cristália/FIOCRUZ suggests that, if the project to which Carrara et al. referred was to be implemented, Helleva could be the chosen drug. The National Policy of Men's Health could significantly help turn this possibility into a reality, helping to promote and popularise Helleva on the Brazilian market.
FINAL REMARKS
We are dealing with a broader uninterrupted feedback cycle of which the studied material represents an 'instant', an example. The cycle departs from lay and traditional presuppositions of gender and sexuality which, translated in medical terms (medicalisation), transform themselves into normatised domains that can and, especially, should be 'corrected'. The functions 'corrected' by the biomedical interventions produce new expectations, models, and possibilities, that is to say, new bodies reconfigured by pharmacological technologies (biomedicalisation). New bodies also produce new norms and ideals which, appropriated by the lay public, construct parallel pathways of drug consumption by way of self-prescription. As much the medical prescriptions as self prescribing reinforce biomedicalisation, since they work from the understanding of a bodily activity codified in medical terms and which, in this manner, is open to pharmacological interventions. This cycle produces a technological frame in which the use of pharmaceuticals stops being merely 'acceptable' and becomes 'desirable'. Each new medication is integrated into this cycle, reinforcing the technological frame in which 'men's health' and 'masculinity' are constantly reconstructed and resignified.
One seeks the legitimation of products and of the 'necessity' for their use through the invocation of 'scientificity', backed up by scientific articles that reveal the dissolution of the boundaries between academic production, research, and industrial development.
As Alain Giami shows, in the absence of critical medical training regarding themes related to sexual function, "the pharmaceutical industry controls in an almost exclusive manner the information and the training of doctors" (Giami, 2009b, p. 69). In this way, in respect to the prescriptions for ED, doctors occupy a similar place to lay people, partly consequent on an academic education which does not include the critical evaluation of scientific articles (Camargo Jr., 2003).
In Brazil, the advertisement of this type of medication (the so-called ethical drug) is forbidden, it can only be advertised to doctors (in congresses or in scientific publications). That explains in part the fact that this propaganda, directed toward professionals, makes use of the normal marketing arsenal. In other words, one uses with the doctor common sense images and conceptions similar to the ones used with lay-persons. One has the impression that the industry intends to 'sell' the product to the professional for their personal use. In other terms, despite the aim of the advertisement being to instigate the doctor to prescribe, its language and the images used make it seems that the real aim is to sell the medication itself.
The colloquial language used in all the information packs, for "exclusive circulation amongst doctors", grabbed our attention. In the advertising kits for Cialis, we note on the last page, in capital letters, the recommendation "Don't forget to speak with your patient", explaining in detail what to say:
+ With Cialis your patient does not need to schedule to take the tablet immediately before sexual relations.
+ Cialis has up to 36 hours of efficacy, that is to say, your patient can take it at lunch on Friday and will be safe to have sexual relations, at any time, up until Sunday morning.
+ Cialis can be taken with fatty foods and alcoholic drinks in moderate quantities.
+The erection only occurs through sexual stimulation.
+It is not recommended for a patient who is using organic nitrates. (Cialis Information pack, p.4)
Backed up by the absence of critical medical training regarding the theme, the choice of topics to be 'clarified' seemed to place the agency of the professional in second place. The ready made explanation which the laboratory suggests the doctor should provide the patient presupposes a professional that is no more than an intermediary between the industry and the consumer.
According to Azize, the discourses which circulate "between the lay public, the pharmaceutical laboratories, and biomedical professionals (promote) the idea of a 'super-health', generating a new objective and new uses for the medications", constructing what the same author calls "lifestyle medications" (Azize, 2006, p.121). Regarding our specific object, the pharmaceuticals for ED, Faro points out that:
Pro-sexual drugs offer an enhancement for sexuality, something that would make the body function better, which would bring completion to sexual function. It is not an illness that can be cured by a medication, but a function, which will be potentialised with a pill (Faro, 2009b, p. 18).
At the same time in which the drugs 'guarantee' performance, they produce a diversity of anxieties, present or future, in relation to the 'quality' and duration of an erection. As Chris Wienke carefully analysed, the self-response questionnaire on the Levitra site carries to the inevitable conclusion that, if the person does not have any of the listed problems, they may still "wish to speak with their doctor about some worry regarding their erectile quality" (Wienke, 2006, p.62).
The advertising for Viagra makes plain, including visually, an ideal of masculinity which requires (to be attained with absolute security) the use of pharmaceuticals, as shown in the graphic in which the fourth stage of erection ("completely hard and totally rigid") is represented by the unappealingly obvious blue wooden board. That is to say, the advertising simultaneously exploits masculine insecurity and 'expectations', by offering a 'magic pill', reinforcing the idea of a male sexuality always ready for sex, translated in the readiness of the "completely hard" penis to penetrate. In this sense, we arrive at the point of an 'optimised' masculinity. The '4th stage of erection' assumes, automatically, as Vares and Braun show, "all male sexuality (…) codified as always potentially suboptimal and capable of being improved" (Vares & Braun, 2006, p.328). In other terms, "the presentation of Viagra operates a paradoxical relationship in which one has to overcome the loss of virility without demolishing its symbolic content (to the contrary, while reinforcing it)" (Brigeiro & Maksud, 2009, p.79). The desirable duration of the normalised erection should be between 7 and 10 minutes, no more and no less. The equation "Satisfaction of the couple = greater duration of sexual relation = new parameter of efficiency" shows the notion of sexual relations as heteronormative ("Get better at having sex with your partner")
'Responsible masculinity' is used by the BSP campaign, which is in agreement with the already mentioned National Policy of Men's Health. It is what the first phrase of the advertising material for Levitra indicates: "THE EVOLUTION in Masculine Health". On the interior page, the idea is reinforced: "Bayer was the first laboratory with a portfolio focused on masculine health. With advanced research Bayer Schering Pharma offers effective treatments for the health of men as well as innovative preventative solutions". The 'responsible man' takes care of his physical and economic health, according to our national product, Helleva, which declares that: "Big results, small costs, just how a man likes it". In a clear paradox with the strategy of the Ministry of Health of using ED as a hook to talk about other conditions, such as hypertension and diabetes, the advertising material of Helleva underlines, amongst its qualities, the fact of being still more efficient "after meals rich in lipids and also after the consumption of alcohol".
The pharmacological effect of a guaranteed and sustained erection produces 'confident masculinity': "It's time to show the capital H that's at the heart of every Brazilian man". The implicit conception of male sexuality centred on the erection as unstable leads to the notion that without medication all male sexuality is uncertain. The resolution of this 'fragility' is sought in a concrete solution: a pill that will eliminate uncertainty. "Confidence stamped on the box" and also "Security with a capital H". Or, according to Eli Lilly: "Freedom of choice which only Cialis offers", "Cialis is highly effective for up to 36 hours". Without questioning the equation masculinity = erection, one starts by managing the fragility, guaranteeing the erection. Male sexuality, traditionally represented as 'wild', 'instinctive', and 'uncontrollable' is normatised and rationalised. Paradoxically, it is by way of sophisticated pharmacological technology that one offers to men the return of their 'primordial' characteristics, of their 'true sexual nature', of their 'liberty' and 'confidence'. Molecules and behaviours are mixed in a naturalised continuum. Constructing a masculinity in whose centre is the maintenance of the sexually potent man, confident, rigid and effective, we find a hybrid product as much body as technology, 'super-natural', on the definitively misty border between nature and culture.
REFERENCES
- Angell, M. A verdade sobre os laboratórios farmacêuticos Rio de Janeiro, Record, 2007.
- Azize, R. Saúde e estilo de vida: divulgação e consumo de medicamentos em classes médias urbanas. In: Leitão, D.; Lima, D.; Machado, R. P. (orgs.) Antropologia e consumo: diálogos entre Brasil e Argentina Porto Alegre, AGE, 2006, pp.119-137.
- Bijker, W. E. The social construction of Bakelite: towards a theory of invention. In: Bijker, W.E.; Hughes, T. & Pinch, T.J. (eds.) The social construction of technological systems. New directions in the sociology and history of technology. Cambridge, MIT Press, 1987, pp.159-187.
- __________. Do not despair: there is life after constructivism. Science, technology & human values vol.18, nº 1, Thousand Oaks, CA, Winter 1993, pp.113-138.
- Brigeiro, M. e Maksud, I. Aparição do Viagra na cena pública brasileira: discursos sobre corpo, gênero e sexualidade na mídia. Revista Estudos Feministas, Florianópolis, vol.17, nº 1, 2009, pp.71-88.
- Camargo Jr., K. R. Sobre palheiros, agulhas, doutores e o conhecimento médico: a epistemologia intuitiva dos clínicos. In: Camargo Jr., K. R. Biomedicina, saber e ciência: uma abordagem crítica. São Paulo, Hucitec, 2003, pp.147-185.
- Carrara, S.; Russo, J. e Faro, L. A política de atenção à saúde do homem no Brasil: os paradoxos da medicalização do corpo masculino. Physis. Revista de Saúde Coletiva, vol.19, nº 3, 2009, pp.659-678.
- Clarke, A.; Mamo, L.; Fishman, J.; Shim, J.; Fosket, J. Biomedicalization: Technoscientific Transformations of Health, Illness, and U.S. Biomedicine. American Sociological Review, vol. 68, April, 2003, pp.161-194.
- Connell, R. W. La organización social de la masculinidad. In: Valdéz, T. & Olivarría, J. (eds) Masculinidad/es: - p poder y crisis Santiago, Chile, Isis Ediciones de las mujeres/FLACSO, nº 24, 1997,pp.31-48.
- Conrad, P. The medicalization of society: on the transformation of human conditions into treatable disorders. Baltimore, The Johns Hopkins Press, 2007.
- Faro, L. As disfunções sexuais femininas no periódico. Archives of Sexual Behavior. Dissertação de mestrado em Saúde Coletiva, Instituto de Medicina Social, UERJ, Rio de Janeiro, 2008.
- __________. Contornos da medicalização da sexualidade feminina no século XXI: disfunções sexuais femininas num periódico científico. Trabalho apresentado no 33º Encontro Anual da ANPOCS, Caxambu, 2009a. Disponível em: http://www.encontroanpocs.org.br/2009/. Acesso em: 15/12/2009.
- __________. A medicalização das disfunções sexuais femininas no contexto da farmacologização da sexualidade. Trabalho apresentado no XIV Congresso Brasileiro de Sociologia, Rio de Janeiro, 2009b. Disponível em: Acesso em: 22/06/2010.
- Fleck, L. Genesis and Development of a Sientific Fact. Chicago and London, The University of Chicago Press, 1979.
- Giami, A. Ethnographie d"une conférence médico-scientifique: l'influence de l'industrie pharmaceutique dans le champ de la sexologie. Revue Sociologie / Santé, nº 30, 2009a, pp.187-210.
- __________. Da impotência à disfunção erétil. Destinos da medicalização da sexualidade. Physis. Revista de Saúde Coletiva vol. 19, nº 3, Rio de Janeiro, 2009b, pp.637-658.
- Grace, V.; Potts, A.; Gavey, N. & Vares, T. The Discursive Condition of Viagra. Sexualities, vol. 9, nº 3, London, Thousand Oaks e New Delhi, SAGE Publications, 2006, pp.295-314.
- Kaplan, H. A nova terapia do sexo Rio de Janeiro, Nova Fronteira, 1977.
- Krane, R., Goldstein, I. e Saenz de Tejada, I. Impotence. The New England Journal of Medicine, vol. 321, nº 24, 1989, pp.1648-1659.
- Lakoff, A. Pharmaceutical Reason: kKnowledge and Value in Global Psychiatry. Cambridge MA, Cambridge University Press, 2005.
- Lexchin, J. Bigger and Better: How Pfizer Redefined Erectile Dysfunction. Plosmedicine, vol. 3, nº 4, 2006, pp.1-4.
- Loe, M. Fixing broken masculinity: Viagra as a technology for the production of gender and sexuality. Sexuality and culture, vol. 5, nº 3, 2001, pp.97-125.
- __________. The rise of Viagra - how the little blue pill changed sex in America. New York, New York University Press, 2004.
- __________. The Viagra blues: embracing or resisting the Viagra body. In: Rosenfeld, D. e Faircloth, C. (orgs.) Medicalized Masculinities. Philadelphia, Temple University Press, 2006.
- Mamo, L. & Fishman, J. Potency in all the right places: Viagra as a technology of the gendered body. In: Body and society, vol.7, nº 4, London, Thousand Oaks and New Delhi, SAGE Publications, 2001, pp.13-35.
- Marshall, B. Hard science: gendered construction of sexual dysfunction in the Viagra age. Sexualities, vol. 5, nº 2, London, Thousand Oaks and New Delhi, SAGE Publications, 2002, pp.131-158.
- __________. The New Virility: Viagra, Male Aging and Sexual Function. Sexualities, vol. 9, nº 3, London, Thousand Oaks and New Delhi, SAGE Publications, 2006, pp.345-362.
- __________ & Katz, S. Forever Functional: Sexual Fitness and the Ageing Male Body. Body & Society, vol. 8, nº 4, London, Thousand Oaks and New Delhi, SAGE Publications, 2002, pp.43-70.
- Masters, W. & Johnson, V. Human sexual response. Boston, Little, Brown, 1966.
- __________. Human sexual inadequacy. Boston, Little, Brown, 1970.
- Mulhall, J., et alii Erectile Dysfunction: Monitoring Response to Treatment in Clinical Practice - Recommendations of an International Study Panel. Journal of Sexual Medicine, nº 4, 2007, pp.448-464.
- Oudshoorn, N. Beyond the Natural Body: An Archeology of Sex Hormones London, Routledge, 1994.
- Pinch, T. J. & Bijker, W. E. The social construction of facts and artifacts: Or how the sociology of science and the sociology of technology might benefit each other. In: Bijker, W.E., Hughes, T. & Pinch, T.J. (eds). The social construction of technological systems: new directions in the sociology and history of technology. Cambridge, MIT Press, 1987, pp.17-50.
- Rabello, E. T. Representações sociais mobilizadas pela propaganda televisiva de medicamentos: intersecções entre ciência, saúde e práticas de consumo. Dissertação de mestrado em Saúde Coletiva. PPGSC do Instituto de Medicina Social UERJ, Rio de Janeiro, 2010.
- Rohden, F. Uma ciência da diferença: sexo e gênero na medicina da mulher. Rio de Janeiro, Editora FIOCRUZ, 2001.
- __________. Diferenças de gênero e medicalização da sexualidade na criação do diagnóstico das disfunções sexuais. Revista Estudos Feministas, vol.17, nº 1, Florianópolis, 2009, pp.89-109.
- Rosenfeld, D. & Faircloth, C. A. Introduction: Medicalized Masculinities: The Missing Link? In: Rosenfeld, D. & Faircloth, C.A. (eds.) Medicalized Masculinities Philadelphia, Temple University Press, 2006, pp.1-20.
- Russo, J. et alii Sexualidade, ciência e profissão no Brasil. Rio de Janeiro, CEPESC, 2011.
- SBU - Sociedada Brasileira de Urologia. Disfunção Erétil: Tratamento com Drogas Inibidoras da Fosfodiesterase Tipo 5. Projeto Diretrizes (Associação Médica Brasileira e Conselho Federal de Medicina), 2006. Disponível em: http://www.projetodiretrizes.org.br/5_volume/16-Disfun5.pdf. Acesso em 15/06/2010
- Tiefer, L. The Viagra phenomenon. Sexualities, vol.9, nº 3. London, Thousand Oaks and New Delhi, SAGE Publications, 2006, pp.273-294.
- Vares, T. & Braun, V. Spreading the Word, but What Word is That? Viagra and Male Sexuality in Popular Culture. Sexualities, vol. 9, nº 3, London, Thousand Oaks and New Delhi, SAGE Publications, 2006, pp.315-332.
- Wienke, C. Sex in the Natural Way: The Marketing of Cialis and Levitra. In: Rosenfeld, D. & Faircloth, C.A. (eds.) Medicalized Masculinities. Philadelphia, Temple University Press, 2006, pp.45-64.
[10]
[11]
[12]
[13]
[14]
[15]
[16]
[17]
[18]
[19]
[20]
[21]
[22]
[23]
[24]
[25]
[26]
[27]

[28]
[29]
[30]
[31]
[32]
[33]
[34]
Publication Dates
-
Publication in this collection
11 July 2013 -
Date of issue
June 2013
History
-
Received
27 July 2011 -
Accepted
25 Apr 2012