Abstracts
The authors report a case of hereditary palmoplantar keratoderma, Unna-Thost type, demonstrating some atypical features when compared to descriptions found in the literature. The case study also includes pseudoainhum on both fifth toes. The authors describe other hereditary palmoplantar keratodermas that may also present with pseudoainhum, and demonstrate the basic clinical criteria that they share.
ainhum; keratoderma, palmoplantar
Os autores relatam um caso de ceratodermia palmoplantar hereditária de Unna-Thost, de apresentação clínica atípica, bem como complicação do tipo estrangulamento ainhumóide no quinto dedo de ambos os pés. Os autores citam ainda outras ceratodermias palmoplantares hereditárias que podem cursar com pseudo-ainhum, bem como os critérios clínicos básicos que diferenciam essas manifestações.
ainhum; ceratodermia palmar e plantar
CASE REPORT
Unna-Thost type palmoplantar keratoderma associated with pseudoainhum - A case report* * Work done at Padre Bento Hospital Complex Dermatology Service, Guarulhos, São Paulo State.
Luciana Valentini de Melo CesariniI; José Roberto Pereira PegasII; Vítor Manuel Silva dos ReisIII; Helena MüllerIV; Marco Antônio de OliveiraV; Mário Cezar PiresVI
IAssistant physician, Padre Bento Hospital Complex Dermatology Service of Guarulhos (CHPBG), Master's degree, certified Specialist by Brazilian Society of Dermatology (SBD)
IIAssistant physician, Padre Bento Hospital Complex Dermatology Service of Guarulhos (CHPBG), Master's Degree, certified Specialist by Brazilian Society of Dermatology (SBD)
IIIAssistant physician, The Clinics' Hospital Dermatology Service (FMUSP), Ph.D., certified Specialist by Brazilian Society of Dermatology (SBD)
IVMedical pathologist, Head of clinic, Adjunct Professor of Pathological Anatomy, Santa Casa de Sao Paulo Medical Faculty
VStudent-physician, CHPBG
VIHead Physician, Padre Bento Hospital Complex Dermatology Service of Guarulhos (CHPBG), Ph.D., certified Specialist by Brazilian Society of Dermatology (SBD)
Correspondence Correspondence to Luciana Valentini de Melo Cesarini Rua Dr Diogo de Faria, 929 / 141 - Vila Clementino 04037-003 São Paulo SP Tel./Fax: (11) 5083-8222 E-mail: lucivalmel@uol.com.br
SUMMARY
The authors report a case of hereditary palmoplantar keratoderma, Unna-Thost type, demonstrating some atypical features when compared to descriptions found in the literature. The case study also includes pseudoainhum on both fifth toes. The authors describe other hereditary palmoplantar keratodermas that may also present with pseudoainhum, and demonstrate the basic clinical criteria that they share.
Key-words: ainhum; keratoderma, palmoplantar.
INTRODUCTION
Palmoplantar keratodermas (PPK) make up a complex and heterogeneous group of diseases that are genetically determined and characterized by keratinization disturbances.1
The classification of keratodermas is based on the clinical condition, which takes account of lesion morphology, the genetic inheritance model, age of onset, presence or absence of lesions localized beyond the transgressive palmoplantar regions, and involvement of more than one ectodermic structure.2
Recently, a new classification for PPK was proposed which covers not only the clinical aspect of lesions, but also the histopathologic and molecular alterations involved. From this classification, three groups or clinical forms resulted, which may be called diffuse, focal and punctuated.3
The term 'ainhum', from Angolan origin, means 'to saw'. It is characterized by formation of fibrous constricting bands usually around the fifth toe. These are uni- or bilateral, and may lead to amputation of the affected toe. The manifestation is described as affecting all races and regions worldwide, though it occurs with greatest frequency among Negroid males.4 Other pathologies deserve attention as they may also present with fibrous constriction ring formations similar to those of true ainhum, but which are termed pseudoainhum.
Among the genodermatoses that may present with pseudoainhum, one finds intrauterine forms termed congenital pseudoainhum or amniotic band syndrome. These may present with constriction band formations around the trunk, limbs and toes, which tend to undergo intrauterine amputation.4
Other acquired diseases have also been described in the literature. These may be associated with pseudoainhum, such as porokeratosis of Mibelli,5 erythropoietic protoporphyria,6 scleroderma,7,8 psoriasis,9 plica neuropathica,10 infectious processes like Hanseniasis,11 tertiary syphilis, and other phenomena like Raynaud's disease, diabetes mellitus, syringomyelia, and, finally, facticious pseudoainhum caused by the hair-thread tourniquet syndrome around the digit.4
Pseudoainhum may occur also as a complication in some hereditary palmoplantar keratodermas.
CASE REPORT
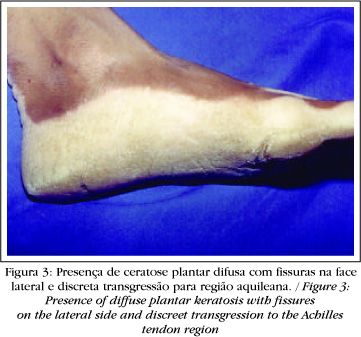
A 48-year-old male melanoderm patient, born in the city of Minas Gerais, Minas Gerais state, and living in Sao Paulo, São Paulo state. He reported the onset of lesions on the hand and feet at age 15. Two years later there emerged a constriction ring around the fifth right toe that grew progressively (Figure 1). A year later, a similar process occurred on the contralateral toe. The dermatological examination revealed diffuse palmoplantar keratosis (Figure 2) with fissures on the lateral sides of both feet (Figure 3). The keratosis showed limited areas of transgression on the anterior side of the wrist and Achilles tendon region. The base of the fifth digit of both feet was shown to be surrounded by a fibrous ring. The right-side lesion was accompanied with edema, pain and fetid suppurative material, which was the reason why he was led to seek specialized medical assistance. Also seen were ungual alterations like thickening without dystrophy. Hair and teeth showed no alterations.
By means of a genealogical investigation spanning three generations, which included 25 known family relatives, six additional cases of PPK were detected: four brothers, the father and the paternal grandfather's sister (Heredogram). Radiological examinations were carried out of the dental arch and hands, which did not exhibit any abnormalities; of the right foot, which showed bone resorption of the proximal phalange of the fifth toe; of the left foot, which showed a fracture of the proximal phalange with signs of resorption and osteoporosis of the fifth toe. The wrist biopsy over the keratosis area revealed non-specific alterations, such as orthohyperkeratosis with moderate acanthosis. The patient studied in this paper initially received treatment with oral antibiotics and local care at the focus of infection on his right foot. Yet a week after being interned, spontaneous disarticulation occurred followed by strangulation and amputation of the fifth right toe. Medical surgery was not required.
DISCUSSION
Unna-Thost PPK is classified as a hereditary form of palmoplantar keratoderma. In 1962, in his monograph on acrokeratoses, Osvaldo Costa considered it to be the main representative of all types of palmoplantar keratosis. It was described by Thost in 1880 as a form of palmoplantar ichthyosis. Meanwhile, it befell to Unna to classify it as a variant of keratoderma in 1883.12
Some authors have considered it a classic dermatological example of regular dominant inheritance. There exist reports on the involvement being present in up to six generations. Authors in Croatia have described isolated cases of the precocious or late-onset emergence of the disease, which may be related to genetic factors, such as spontaneous mutation, reduced expression and incomplete penetrance.13,14 The genetic analysis of families with palmoplantar keratoderma, Unna-Thost type, has allowed medical researchers to observe alterations present in the filaments of keratin type II gene (codified as 12q11-13). No definitive mutations were observed in the families analyzed.15

Clinically, Unna-Thost PPK is characterized by symmetrical keratosis circumscribed to the palms and soles. Absence of pruritus can be attested, and palmoplantar hyperhidrosis is a frequent symptom. When there is no such symptom, the disease leads to hardening and drying of the corneal layer, which ends up producing grooves and deep fissures. When intense, the keratosis may reach the lateral edges of the feet and hands. In some cases, at the shifting point between the diseased skin and healthy skin, a red-bluish colored band can be verified as beginning at the outer edge of the palms and quickly reaching the center and inner sides of the fingers and toes. Still, these are not obligatory signs.12,16
The onset of the disease virtually always takes place during the first year of life. It may also appear in adolescence and even in adulthood. There is no predilection for race, though incidence is slightly higher in men. The disease is related to the influence of climatic factors. Worsening of the clinical condition or increasing relapses occurs during the cold periods of the year. With respect to complications, the following has been described: fungal and/or bacterial infection in the fissures and folds of the joints, occasioning a characteristic odor; inflammation and pain, which makes walking and manual work difficult and even impossible. Lymphangitic processes, dyshidrotic eczema, onychomycosis, and blister formation are other related alterations.12,17,18
The histopathologic alterations in Unna-Thost PPK are non specific. They typically lack epidermolysis, which is an important factor of differentiation from Vorner's epidermolytic palmoplantar keratoderma. Despite its hereditary pattern and the similar clinical alterations to Unna-Thost PPK, the latter keratoderma shows typical histopathologic alterations, such as vacuolar alterations of the granular layer. Such alterations were not found in the case studied for this paper.
Treatment of palmoplantar keratodermas, prior to the availability of aromatic retinoids, used to be based on the use of topical keratolytic agents. These did not demonstrate satisfactory results on the long term. Systemic retinoids, such as etretinate and, more recently, acitretinate, have been used on severe and diffuse forms of palmoplantar keratodermas either in association with a mutilating character or not. In various cases, it has proved to have a good therapeutic response19-22 in spite of it presenting some adverse effects, such as increased cutaneous fragility and sensitivity, which has contributed to discontinuing treatment in many cases. At this point in time, genic therapy remains only a theoretical perspective due to the extreme difficulty of repairing the transformed allele.15
Pseudoainhum may occur in association with hereditary palmoplantar keratodermas (Table 1). It is more frequent in those having a mutilating character, such as Vohwinkel's disease, with autosomal dominant inheritance, and Meleda's disease, with recessive autosomal inheritance.
At the outset of studying the present case, the authors sought to insert the patient in the diffuse palmoplantar keratosis group, which presents with ainhum strangulation, as is the case with Vohwinkel's palmoplantar keratoderma mutilans, which also appears as diffuse symmetric PPK, whose inheritance pattern was dominant. Nonetheless, there were no other typical characteristics of the disease found, such as the honeycomb pattern of keratosis, and 'starfish' shaped lesions on the dorsal aspect of the hand or fingers.12,22-24
Meleda's disease (or, mal de Meleda) differs from the present case owing to its resemblance with recessive autosomal inheritance PPK. It has a more severe clinical condition, transgressive lesions at the palmoplantar regions and lifelong progressive lesions.12,20,21
Moncorps12 described the clinicomorphological variations of Unna-Thost PPK in 1931, by distinguishing the following: a) exclusive involvement of the hands and feet, absence of symmetry; b) transgressions to neighboring areas; c) simultaneous appearance of hyperkeratosis or other cutaneous modifications over the rest of the body; d) alteration of the cutaneous annexes (hairs and nails) and of the mucosas; e) dental, musculoskeletal, psychological and endocrinal alterations.
Moreover, the appearance of constriction corneal rings in the Unna-Thost disease was first cited by Hetch in 1930. It was later called the ainhum-like form of Unna-Thost keratoderma by Argelles Casals.12
The authors conclude that the presence of clinicomorphological characteristics and dominant inheritance, in association with some variations observed by Moncorps, and finally the rare association of constriction corneal rings all contribute to terming this case an atypical clinical form of Unna-Thost type PPK, in which the presence of the ainhum-like strangulation should be emphasized.

REFERENCES
Received in September, 20th of 2001
Approved by the Consultive Council and accepted for publication in May, 24th of 2002
- 1. Rickman L, Simrak D, Stevens HP, et al. N-terminal delection in a desmossomal cadherin causes the autossomal dominant skin disease striate palmoplantar keratoderma. Hum Mol Gen 1999; 8:971-6.
- 2. Christiano AM. Frontiers in keratodermas: pushing the envelope. Trends Genetic 1997; 13:227-233.
- 3. Stevens HP et al: Linkage of an American pedigree with palmoplantar keratoderma and malignancy (palmoplantar ectodermal dysplasia type III) to 17q24. Literature survey and proposed update classification of the palmoplantar keratodermas. Arch Dermatol 1996;132,640-51.
- 4. Burgdorf WHC: Ainhum e Pseudoainhum; in Fitzpatrick TB, Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, et al: Dermatology in General Medicine, ed.5. New York, Mc Graw-Hill, 1999:1208-9.
- 5. Ramesh V, Misra RS, Mahaur BS. Pseudoainhum in porokeratosis of Mibelli. Cutis 1992; 49(2): 129-30.
- 6. Christopher AP, Grattan CE, Cowan MA. Pseudoainhum and erytropoietic protoporphyria. Br J Dermatol 1988;118(1):113-6.
- 7. Park BS, Hyun-Cho K, Youn JI, Chung JH. Pseudoainhum associated with linear scleroderma [letter] Arch Dermatol 1996; 132(12):1520-1.
- 8. Tajima S, Suzuki Y, Inazumi T. A case of atypical localized scleroderma presenting with pseudoainhum: treatment with tranilast an anti-fibrotic agent [letter]. Acta Derm Venereol 1996; 76(2): 162.
- 9. McLaurin CI. Psoriasis presenting with peudoainhum. J Am Acad Dermatol 1982; 7(1): 130-2.
- 10. Diestelmeier MR & Rodman OG. Pseudoainhum associated with plica neuropathica. Cutis 1981; 28(6): 629-30.
- 11. Gibbs RC & Frank SB. Keratoma Hereditaria Mutilans (Vohwinkel). Arch Derm 1966; 94: 619-25.
- 12. Costa OG. Acroceratoses (ceratodermias palmo-plantares). Tese. Belo Horizonte: Minas Gerais (MG), 1962.
- 13. Kansky A, Stanimirovic A, Basta- Juzbasic A. Isolated cases of palmo plantar Keratoderma, Unna-Thost type. Cutis 1992; 49:406-8.
- 14. Yang JM, Lee S, Kang HJ et al Mutations in the 1A rod domain segment of the keratin 9 gene in epidermolytic palmoplantar keratoderma. Acta Derm Venereol 1998;78:412-16.
- 15. Ratnavel RC, Griffiths WAD. The inherent palmoplantar keratodermas. Br J Dermatol 1997;137:485-90.
- 16. Sampaio SAP, Rivitti EA. Alterações Hereditárias da Queratinizaçã. In: Dermatologia. São Paulo, Artes Médicas, 1998:765-86.
- 17. Gamborg NP. The prevalence of dermatophyte infeccions in Heraditary palmo plantar Keratoderma. Acta Derm Venereal 1983; 63: 439-41.
- 18. Gamborg NP. Dermatophyte Infeccions in Hereditary palmo plantar Keratoderma. Frequency and Therapy. Dermatologica 1984; 168:238-41.
- 19. Paug AFICS, Orange AP, Verzevki VD, Stolz E. Succesful Treatment of Keratoderma Hereditaria Mutilans with na Aromatic Retinoid. Arch Dermatol 1981; 117: 225-28.
- 20. Brambiella L, Pigatto PD, Boneschi V, Altomare GF, Finzi AF. Unusual cases of Meleda treated with Aromatic Retinoid Etretinate. Dermatologica 1984; 168: 283-86.
- 21. Bergman R, Bitterman DO, Fartasch M, Gershon BR, Friedman BR. Mal de Meleda- Keratoderma with pseudo-ainhum. Br J dermatol 1993; 128: 207-12.
- 22. Bell M, Hoede N, Schopf RE. Pseudo-ainhum in Vohwinkel disease- Keratoderma Hereditarium Mutilans. Hautarzt 1993; 44:738-41.
- 23. Cole RD, McCauley M, Way BH. Vohwinkel Keratoma Hereditaria Mutilans. Int. J. Dermatol 1984; 23:131-4.
- 24. Medina S, Alonso ML, Freire P, Elias LM, Ledo A. Síndrome de Vohwinkel: a proposito de dos casos asociados a sordera. Med Cut 1992; 20:232-36.
- 25. Stevens HP, Leigh IM: Keratoderma of palms and soles. In: Fitzpatrick TB, Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA et al Dermatology in General Medicine,ed 5. New York, McGraw-Hill, 1999:603-13.
Publication Dates
-
Publication in this collection
03 June 2004 -
Date of issue
Feb 2004
History
-
Received
20 Sept 2001 -
Accepted
24 May 2002