Abstracts
Rosai-Dorfman disease, otherwise known as sinus histiocytosis with massive lymphadenopathy, is a non-Langerhans cell histiocytosis with a benign course and unknown etiology. It was described in 1969 as a painless cervical lymph node enlargement in association with fever, weight loss and sweating. Extranodal disease has been reported in 43% of cases, with involvement of multiple organs. Purely extranodal Rosai-Dorfman disease has been already reported, including forms restricted to the skin. This paper reports a case of purely cutaneous Rosai-Dorfman disease, which is of interest in view of the rarity of this condition.
Histiocytosis; Non-Langerhans-cell histiocytosis; Sinus histiocytosis
A doença de Rosai-Dorfman, também denominada histiocitose sinusal com linfadenopatia maciça, é histiocitose de células não Langerhans, idiopática e de curso benigno. Descrita em 1969, caracteriza-se por linfadenomegalia não dolorosa, sendo a cadeia cervical a mais envolvida, além de febre, perda de peso e sudorese. O envolvimento extranodal ocorre em 43% dos casos, em que múltiplos sítios podem ser acometidos. Já foram descritos casos exclusivamente extranodais, inclusive formas limitadas à pele. Relata-se um caso de doença de Rosai-Dorfman extranodal cutânea pura, devido à raridade dessa apresentação clínica.
Histiocitose; Histiocitose de células não Langerhans; Histiocitose sinus
CASE REPORT
Cutaneous Rosai-Dorfman disease - a case report*Josie da Costa EirasI; Antônio Pedro Mendes SchettiniII; Livia Lima de LimaIII; Liana Hortência Miranda TubillaIV; Rosa Maria Libório de OliveiraV
IPhysician currently participating in the Residency Program in Dermatology at the Alfredo da Matta Foundation, Manaus, AM, Brazil
IIDermatologist, Alfredo da Matta Foundation. Master's degree in Tropical Pathology awarded by the Federal University of Amazonas, Manaus, AM, Brazil
IIIPhysician currently participating in the Residency Program in Dermatology at the Alfredo da Matta Foundation, Manaus, AM, Brazil
IVPhysician, Alfredo da Matta Foundation, Manaus, AM, Brazil
VDermatologist, Municipal Health Department, Manaus, AM, Brazil
Mailing address
ABSTRACT
Rosai-Dorfman disease, otherwise known as sinus histiocytosis with massive lymphadenopathy, is a non-Langerhans cell histiocytosis with a benign course and unknown etiology. It was described in 1969 as a painless cervical lymph node enlargement in association with fever, weight loss and sweating. Extranodal disease has been reported in 43% of cases, with involvement of multiple organs. Purely extranodal Rosai-Dorfman disease has been already reported, including forms restricted to the skin. This paper reports a case of purely cutaneous Rosai-Dorfman disease, which is of interest in view of the rarity of this condition.
Keywords: Histiocytosis; Non-Langerhans-cell histiocytosis; Sinus histiocytosis
INTRODUCTION
Rosai-Dorfman disease, also known as sinus histiocytosis with massive lymphadenopathy, is a non- Langerhans cell histiocytosis first described in 1965 by Destombes and recognized as a distinct clinicopathological entity by Rosai and Dorfman in 1969. 1-8
It is characterized clinically by a massive, bilateral, painless cervical lymphadenopathy, usually in association with fever, weight loss, night sweats, leukocytosis with neutrophilia, increased erythrocyte sedimentation rate and polyclonal gammopathy. 1,2,8-10
Although less common, other lymph node chains such as the axillary, inguinal, paraaortic or mediastinal chains may be affected. 8,11 Extranodal involvement occurs in 43% of cases, either in association with lymph node involvement or otherwise. 4,7,9,10 Various affected sites have been described such as the nasal and paranasal cavities, eyes and retro-orbital tissue, central nervous system, bones and skin, among others. 2,6
Purely extranodal cutaneous forms have already been reported; however, they occur rarely, with only 85 cases having been described up to 2006 in reports or short series, thus justifying the present case report. 10-15
CASE REPORT
A 26-year old female domestic servant, skin photo type III, reported the appearance of a lesion one year prior to consultation, following an insect bite. The lesion grew progressively on the medial surface of her right arm, with occasional pain and pruritus. The patient reported no systemic symptoms such as fever, malaise or weight loss. General physical examination was normal and there was no sign of lymph node enlargement. Dermatological examination showed a non-infiltrated, brownish plaque with clear borders and irregular contours measuring 6 cm, with pink tuberosities of around 0.5 cm in diameter on the surface (Figure 1). Laboratory tests, chest xrays of the facial sinuses and long bones, and abdominal ultrasonography were all within normal limits and anti-HIV serology was negative.
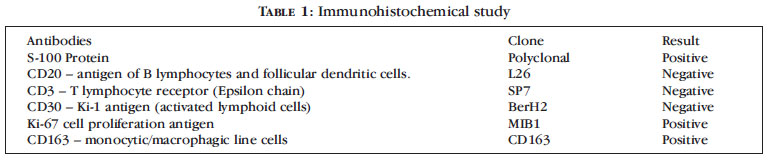
A skin biopsy was performed, which showed dermal inflammatory infiltrate composed essentially of histiocytes with large cytoplasm, vesicular nuclei and evident nucleoli, with emperipolesis (Figure 2). Lymphocytes, neutrophiles, rare eosinophiles and giant cells of the Langhans type were also found. Immunohistochemistry revealed diffuse S-100 protein expression in the histiocyte cells (Figure 3) as well as positivity for Ki-67 and CD163 and negativity for CD20, CD3 and CD30 (Table 1).
A diagnosis of exclusively cutaneous Rosai-Dorfman disease was made, with complete surgical resection of the plaque five months prior to the present report.
DISCUSSION
The term cutaneous Rosai-Dorfman disease is used exclusively for the forms of the disease in which involvement is restricted to the skin in order to differentiate it from sinus histiocytosis with massive lymphadenopathy in which there is systemic involvement of multiple sites including the skin. 2,4,13,15 Extranodal forms occur in 43% of cases, the skin being the most common site. Around 10% of patients have skin lesions and in 3% the disease is limited exclusively to the skin. 1,9
The etiology of the disease remains unknown despite some reports that the systemic form of the disease coexists with herpesvirus hominis-6 and 8 (HHV6 and 8) and Epstein-Barr virus (EBV) infection. Investigators have also attempted to demonstrate this association in small series of cases in the cutaneous forms of the disease; however, results have been var-ied, with the majority testing negative. 5,13 The finding of polyclonal gammopathy strengthens the hypothesis of a reactive process against infectious agents. 2
Contrary to the systemic form, which affects principally children and young adults and which shows no preference for gender or ethnic group, the purely cutaneous form of the disease is slightly more common in older age-groups, in women and in nonblack ethnic groups. 1,3,4,6,11,12
Clinically, it presents with papules, nodules, plaques, masses or tumors of a brownish- or yellowish-erythematous color, varying in size from less than 1 cm to 30 cm, either localized or disseminated. The most common sites affected are, in order of decreasing frequency, the trunk, head, neck, lower and upper extremities. 13 The lesions may occasionally resemble psoriasis or acne. 11
Histopathology shows a proliferation of histiocytic cells of large cytoplasm and vesicular nuclei, sometimes with evident nucleoli. The presence of preserved inflammatory cells surrounded by a clear halo may be noticed inside the cytoplasm of these histiocytes, this phenomenon being referred to as emperipolesis. Immunohistochemistry was positive for S-100 protein, CD68 and CD163 and negative for CD1a. Electronic microscopy showed no signs of Birbeck granules. 4,6,7,10 Although emperipolesis is not pathognomonic for this condition, its occurrence in large histiocytes that express S-100 protein determines a diagnosis of Rosai-Dorfman disease. 10,15
Clinical and histopathological differential diagnoses include other histiocytic disorders such as malignant histiocytosis, hemophagocytic syndromes, reticulohistiocytoma of the skin and Langerhans cell histiocytosis as well as large-cell lymphoma, Hodgkin's lymphoma, melanoma and metastatic carcinoma. 4,11
Cases in which the disease is limited to the skin often fail to present any laboratory abnormalities, often progress benignly and are self-limiting, with no need for more aggressive interventions, treatment being indicated only for symptomatic or systemic cases. Therapeutic options include corticosteroids, thalidomide, ·-interferon, cryosurgery, radiotherapy, chemotherapy and surgical excision, among others.7,12,13
As a consequence of the progressive growth, the distressing appearance of the lesion and the absence of any systemic involvement, the patient was submitted to surgical excision and is currently being followed-up to monitor any possible recurrence or progression to systemic disease.

ACKNOWLEDGEMENTS
The authors gratefully acknowledge the collaboration of Dr. Carlos E. Bacchi, Director and Pathologist at the Consultoria em Patologia Laboratory, Botucatu, São Paulo, Brazil, in performing the immunohistochemical study and supplying the photomicrographs.
REFERENCES
- 1. Luz FB, Gaspar AP, Kalil-Gaspar N, Ramos-e-Silva M. Os histiócitos e as histiocitoses não Langerhans em Dermatologia. An Bras Dermatol. 2003;78:99-118.
- 2. Pitamber HV, Grayson W. Five cases of cutaneous Rosai-Dorfman disease. Clin Exp Dermatol. 2003;28:17-21.
- 3. Cheng SP, Jeng KS, Liu CL. Subcutaneous Rosai-Dorfman disease: is surgical excision justified? J Eur Acad Dermatol Venereol. 2005;19:747-50.
- 4. Salim A,Williamson M, Barker F, Hughes J. Steroid responsive cutaneous Rosai-Dorfman disease associated with uveitis and hypothyroidism. Clin Exp Dermatol. 2002;27:277-9.
- 5. Ortonne N, Fillet AM, Kosuge H, Bagot M, Frances C, Wechsler J. Cutaneous Destombes-Rosai-Dorfman disease: absence of detection of HHV-6 and HHV-8 in skin. J Cutan Pathol 2002:29:113-8.
- 6. Grabczynska SA, Toh CT, Francis N, Costello C, Bunker CB. Rosai-Dorfman disease complicated by autoimmune haemolytic anaemia: case report and review of a multisystem disease with cutaneous infiltrates. Br J Dermatol. 2001;145:323-6.
- 7. Wang KH, Chen WY, Liu HN, Huang CC, Lee WR, Hu CH. Cutaneous Rosai-Dorfman disease: clinicopathological profiles, spectrum and evolution of 21 lesions in six patients. Br J Dermatol. 2006;154:277-86.
- 8. Menzel C, Hamscho N, Dobert N, Grunwald F, Kovacs AF, Wolter M, et al. PET imaging of Rosai-Dorfman disease: correlation with histopathology and ex-vivo beta-imaging. Arch Dermatol Res. 2003;295:280-3.
- 9. Van Zander J. Cutaneous Rosai-Dorfman disease. Dermatol Online J. 2004;10:12.
- 10. Weitzman S, Jaffe R. Uncommon Histiocytic Disorders: the non-Langerhans cell histiocytoses. Pediatr Blood Cancer. 2005;45:256-64.
- 11. Uniyal SK, Beena KR, Ramesh V, Mukherjee A. Cutaneous Rosai-Dorfman disease preceding inguinal lymphadenopathy. Int J Dermatol. 2002; 41:404-6.
- 12. Child FJ, Fuller LC, Salisbury J, Higgins EM. Cutaneous Rosai-Dorfman disease. Clin Exp Dermatol. 1998;23:40-2.
- 13. Frater JL, Maddox JS, Obadiah JM, Hurley MY. Cutaneous Rosai-Dorfman disease: comprehensive review of cases reported in the medical literature since 1990 and presentation of an illustrative case. J Cutan Med Surg. 2006;10:281-90.
- 14. Brenn T, Calonje E, Granter SR, Leonard N, Grayson W, Fletcher CD, et al. Cutaneous Rosai-Dorfman disease is a distinct clinical entity. Am J Dermatopathol. 2002;24:385-91.
- 15. Wang KH, Cheng CJ, Hu CH, Lee WR. Coexistence of localized Langerhans cell histiocytosis and cutaneous Rosai-Dorfman disease. Br J Dermatol. 2002;147:770-4.
Publication Dates
-
Publication in this collection
02 Dec 2010 -
Date of issue
Oct 2010
History
-
Accepted
22 Sept 2008 -
Received
13 Aug 2008