Abstracts
BACKGROUND: Telepathology is considered a good alternative for a second opinion consultation. Its implementation is desirable, but studies to confirm its practical application are required. OBJECTIVES: To evaluate the reproducibility of histopathologic diagnoses of skin diseases obtained through digital photomicrographs compared with conventional microscopy. METHODS: We evaluated the surgical specimens of 135 patients using an optical microscope. After 4 weeks, the same consultants independently evaluated a total of 1,738 digital photomicrographs obtained from the histopathological slides. We estimated the overall rate of intra and interobserver agreement, and the Kappa coefficient was obtained with the categorization of the skin diseases: neoplastic skin diseases, infectious-contagious skin diseases and non-infectious-contagious skin diseases. RESULTS: Consultant 1 obtained an agreement of 88.1% (95% CI = 81.5% - 93.1%) between conventional microscopy and images. Consultant 2 obtained an agreement of 80.7% (95% CI = 73.1% - 87%). The interobserver agreement for the microscopy analysis was 81.5% (95% CI = 73.9% - 87.6%). The same analysis using microphotography showed an agreement of 85.9% (95% CI = 78.9% - 91.3%). The Kappa coefficient, which evaluated the categorized skin diseases, was 98.6% for Consultant 1, 93.1% for Consultant 2, 95.8% for interconsultant analyses of images and 95.9% for interconsultant analyses using conventional optical microscopy. All of these values are considered optimal. CONCLUSION: The evaluation of microphotographs shows a good level of reproducibility when compared to traditional microscopy and, therefore, is a viable option for a second opinion consultation in dermatopathology
Dermatology; Diagnosis, computer-assisted; Reproducibility of results; Telepathology
FUNDAMENTOS: A telepatologia é considerada boa alternativa para consultas de segunda opinião. Sua implementação é desejável, mas estudos que confirmem sua aplicação prática são necessários. OBJETIVOS: Analisar a concordância entre os diagnósticos histopatológicos de dermatoses feitos com base em microfotografias digitais em comparação com a microscopia convencional. MÉTODOS: As lâminas de 135 pacientes foram avaliadas por dois consultores por meio de microscópio. Após quatro semanas, os mesmos consultores avaliaram 1.738 microfotografias digitais obtidas dessas lâminas. Estimou-se a taxa geral de concordância intraobservadores e interobservadores e obteve-se o índice Kappa com a categorização das dermatoses: dermatoses neoplásicas, dermatoses infectocontagiosas e não infectocontagiosas. RESULTADOS: A concordância do Consultor 1, que analisou lâminas ao microscópio versus imagens, foi de 88,1% (IC 95% = 81,5% - 93,1%). O Consultor 2 obteve concordância de 80,7% (IC 95% = 73,1% - 87%). A concordância interconsultores ao microscópio foi de 81,5% (IC 95% = 73,9% - 87,6%). A mesma análise por meio de microfotografias mostrou concordância de 85,9% (IC 95% = 78,9% - 91,3%). O índice Kappa, que avalia as dermatoses categorizadas, foi de 98,6% para o Consultor 1, de 93,1% para o Consultor 2, de 95,8% para interconsulta por imagens e de 95,9% para interconsultas ao microscópio óptico. Todos esses valores são considerados ótimos. CONCLUSÃO: A avaliação das microfotografias apresentou ótimo nível de reprodutibilidade quando comparada à microscopia tradicional, sendo uma opção viável para consultas de segunda opinião em dermatopatologia
Dermatologia; Diagnóstico por computador; Reprodutibilidade dos testes; Telepatologia
INVESTIGATION
Reproducibility of histopathologic diagnosis of skin diseases by digital photomicrographs versus conventional optical microscopy*
Fernanda Almeida SchettiniI; Luiz Carlos Lima FerreiraII; Antonio Pedro Mendes SchettiniIII; Romildo Torres CameloIV
IMedicine student, Federal University of Amazonas (UFAM) - Manaus (AM), Brazil
IIPhD in Pathology - Associate Professor of Pathology, Federal University of Amazonas (UFAM) - Manaus (AM), Brazil
IIIMSc - Dermatopathologist, Alfredo da Matta Foundation (FUAM) - Manaus (AM), Brazil
IVSpecialist in Pathology - Pathologist, Amazonas' Center for Cancer Control Foundation - Manaus (AM), Brazil
Mailing address
ABSTRACT
BACKGROUND: Telepathology is considered a good alternative for a second opinion consultation. Its implementation is desirable, but studies to confirm its practical application are required.
OBJECTIVES: To evaluate the reproducibility of histopathologic diagnoses of skin diseases obtained through digital photomicrographs compared with conventional microscopy.
METHODS: We evaluated the surgical specimens of 135 patients using an optical microscope. After 4 weeks, the same consultants independently evaluated a total of 1,738 digital photomicrographs obtained from the histopathological slides. We estimated the overall rate of intra and interobserver agreement, and the Kappa coefficient was obtained with the categorization of the skin diseases: neoplastic skin diseases, infectious-contagious skin diseases and non-infectious-contagious skin diseases.
RESULTS: Consultant 1 obtained an agreement of 88.1% (95% CI = 81.5% - 93.1%) between conventional microscopy and images. Consultant 2 obtained an agreement of 80.7% (95% CI = 73.1% - 87%). The interobserver agreement for the microscopy analysis was 81.5% (95% CI = 73.9% - 87.6%). The same analysis using microphotography showed an agreement of 85.9% (95% CI = 78.9% - 91.3%). The Kappa coefficient, which evaluated the categorized skin diseases, was 98.6% for Consultant 1, 93.1% for Consultant 2, 95.8% for interconsultant analyses of images and 95.9% for interconsultant analyses using conventional optical microscopy. All of these values are considered optimal.
CONCLUSION: The evaluation of microphotographs shows a good level of reproducibility when compared to traditional microscopy and, therefore, is a viable option for a second opinion consultation in dermatopathology.
Keywords: Dermatology; Diagnosis, computer-assisted; Reproducibility of results; Telepathology
INTRODUCTION
The continuing progress in the field of information and communications technology has enabled the emergence of telemedicine, which was initially contemplated as a link between health care facilities located in areas of difficult geographical access and those located in more developed regions, with greater power of resolving health issues. Telepathology is a branch of telemedicine defined as the practice of pathology at a distance through the visualization of microscopic images sent for consultation on a computer screen rather than direct analysis of the slides under a microscope.1 Telepathology, therefore, combines knowledge of medical informatics and digital images with telecommunication resources, with various uses such as telediagnosis, teleconsultation and tele-education.2
The term telepathology was first used in the editorial of the medical journal "Human Pathology" in 1986.3 Initially, it was believed that images of anatomopathological examinations analyzed on the screen of a monitor connected to a computer would have low resolution quality and that its use would not be effective as an object of study or a diagnostic tool. However, the systematic use of personal computers in health care facilities, the decreasing costs of equipment, the advances in the technology of resolution of digital photographic images and the demonstration of the advantages of telepathology workstations in articles published in the specialized literature have demonstrated the effectiveness of the method. 4
Just as pathology, dermatology also uses the method of image analysis for diagnosis of skin diseases. As in other applications of telemedicine, the goal is to provide high quality dermatological care more efficiently by moving information about the patient rather than moving the patient. 5
Using relatively simple equipment, dermatologists and pathologists can quickly transmit microscopic images photographed in a certain location to remote centers. Image transfer can occur in dynamic systems (real-time systems) and in static image systems (images are stored and analyzed later). The first method allows consultation via a robotic microscope, which can be controlled by the pathologist consulted. The equipment used in robotic systems is relatively expensive and requires data transmission networks of high performance. The method of storing and analyzing images at a later time allows us to transmit images captured by a digital camera as an electronic mail file and to analyze them at opportune time. This system has lower cost and is easy to apply. However, some studies addressing the validity of both systems suggest that telepathology with static image may be less accurate. 6
Review work such as that by MASSONE et al. (2008)7 has shown that the use of teledermatopathology is already integrated into the routine of specialized centers in the forms of teleconsultation and teleteaching, being an instrument that can be used to integrate developed countries with developing countries, thus improving the quality of health services. RAO & LOMBARDI (2009)8 have demonstrated that efforts dedicated to broadening the use of telemedicine have already shown positive effects in developing countries. These countries with inadequate health care should incorporate telemedicine into their health system. This way they can even have the aid of volunteer doctors from other countries.
In Brazil, there are few studies on telepathology or digital pathology. In general, these studies most often focus on the author's personal experience or on the institutional experience regarding the use of telepathology workstations. The criteria used for evaluating the results are diagnostic accuracy, specificity and sensitivity of digital samples, in addition to direct observation of percentage rates of agreement or disagreement between intraobserver (optical microscope slides) and interobserver diagnoses (virtual microscopy, remote). The results normally lead to the conclusion that telepathology is an important diagnostic tool as well as it helps to connect the services of surgery and anatomic pathology of a hospital in real time. 9
In 2002, the Federal Council of Medicine of Brazil (CFM) officially recognized the rendering of services through Telemedicine, Resolution No. 1.643/2002, based on the declaration of Tel Aviv (1999), which determined responsibility and ethical rules necessary for the use of tele-assistance. 10
The state of Amazonas has a vast geographical area, low population density, and access to municipalities occurs mainly by boat. This geographic isolation, among other causes, complicates the settling of professionals within the state; therefore, patients who need tests that are a little more complex, such as skin biopsies, need to go to the capital of the state, which usually implies high financial and social costs. Similarly, the isolation of the state capital in relation to the main urban centers, which are generally located in the south and southeast of the country, hinders the exchange of experiences among professionals working in this area, thus making second opinion consultations almost laborious. Telepathology seems to be a viable alternative to overcome these limitations.
This study was conducted with the objective of evaluating the reliability of a static method of telepathology using low-cost resources that are basically already available at health care units, contributing to the foundation and implementation of this technology.
MATERIALS AND METHODS
We developed a cross-sectional descriptive study based on the analysis of photomicrographs of inflammatory and neoplastic skin diseases and compared the results obtained with the analysis of slides under optical microscope. We got a sample from all of the 3,110 histopathological examinations performed on patients treated at Alfredo da Matta Foundation in 2007 and which were processed in the laboratory of dermatopathology of the Foundation. When calculating the sample size, we considered the population of patients who had been biopsied, the expected sensitivity of 90% with a sampling error of 5% and 95% reliability, totaling histopathological examinations of 135 patients. The sample was composed using a table of random numbers. We included only cases with definite diagnosis. When a randomly selected number corresponded to a biopsy without diagnostic definition (descriptive reports), it was substituted for the next number in the table. The slides for the selected patients were removed from the file and evaluated by a doctor, here called observer, specializing in dermatopathology, who confirmed the previous diagnosis having access to the slides and medical records. After that, photomicrographs were taken of each slide, following this scheme: each slide was divided by two vertical and two horizontal imaginary axes. Photographs were then obtained from each of the quadrants with the objective lenses in the following magnification powers: 4x, 10x and 40x. Two pathologists, called consultants, received the photographed images, stored on CD-ROM, and made the diagnosis. They also had access to the clinical data available in the original medical examination request, in case they needed them. The consultants considered a primary and a secondary diagnostic possibility, taking notes of difficulties in analyzing the slides in relation to poor quality of photos, necessity of pictures of other fields, lack of magnification and blurring. Four weeks later, the consultants received the slides corresponding to the images sent and provided a primary and a secondary diagnosis (differential). Photomicrographs were obtained by the observer using a Zeiss microscope and an Olympus digital camera with 5.0 megapixel maximum resolution. The images were compressed into JPEG (Joint Photographic Expert Group) files and stored on a CD-ROM for analysis by the two consultants.
We used the Kappa coefficient (k) to assess the level of agreement between the consultants. This test evaluates whether the agreement obtained is higher than it would be expected by chance. The following Kappa values will be considered: above 0.7 = excellent agreement, values between 0.4 and 0.7 = moderate agreement, and values under 0.4 = poor agreement. 11
RESULTS
Out of the 135 patients participating in the study, 73 were male (54.5%), while 61 were female patients (45.5%). Only one patient could not have his/her gender evaluated due to lack of information. The patients' mean age was 51 years, ranging from a minimum of nine years old to a maximum of 100 years old.
Due to technical problems with the slides, 24 of them had to be discarded and replaced by an equal number, keeping the number of the original sample. 1,738 photomicrographs were obtained of the histopathological slides of the patients needed for the sample, the equivalent of an average of 12.87 photomicrographs per case. The number of photomicrographs ranged from 5 to 29 per patient, according to the need established by the observer based on the size of the tissue sample on the slide being analyzed.
The skin diseases evaluated in the study group are listed according to frequency in Table 1. It is worth emphasizing that each consultant offered a primary diagnosis for the analysis of the slides and one for the analysis of the photomicrographs. Furthermore, they had the option of offering a secondary diagnosis for each situation, when they considered it necessary. Therefore, the total citations of skin diseases were 612.
It was found that when comparing the diagnoses obtained by examining slides under a microscope and those obtained from images of these same slides, an observer obtained a rate of 88.1% (95% CI = 81.5% - 93.1%) and the other obtained 80.7% (95% CI = 73.1% - 87%).
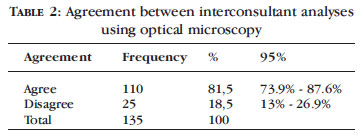
An evaluation of the level of agreement between the two consultants in relation to the diagnoses established by analyzing the slides under an optical microscope showed a value of 81.5% (95% CI = 73.9% - 87.6%) (Table 2).
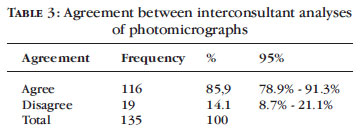
The agreement between the two consultants when the diagnoses were established by analyzing photomicrographs was 85.9% (95% CI = 78.9% 91.3%), as shown in Table 3.
Table 4 lists, in order of frequency, the skin diseases that generated the highest number of discrepancies between the consultants.
Table 5 shows the agreement and Kappa coefficient among the different types of analyses performed when the skin diseases were categorized into three groups: Neoplastic Skin Diseases, Infectious-Contagious Skin Diseases, and Non-Infectious-Contagious Skin diseases.
DISCUSSION
The present study used a sample of 135 patients. The number of patients included was a little higher than that used by other similar studies. Among the dermatoses evaluated, there was a predominance of neoplasms and infectious-contagious diseases, representing the profile of the skin diseases diagnosed in the institution where the work was conducted. It was16 observed that Consultant 1's agreement rate in relation to analysis of the slides under an optical microscope and image analysis was 88.1% (95% CI = 81.5% - 93.1%). Similarly, Consultant 2's agreement rate was 80.7% (95% CI = 73.1% - 87%) concerning the analysis of slides under an optical microscope and images. These results are considered optimal, since the two consultants carried out an independent evaluation and the readings of the slides under a microscope and the images were done at different times so as not to influence, even if unintentionally, the evaluation. These results provide consistency to the study, since they show that the two consultants demonstrate good performance on carrying out the diagnoses independently of one another.
Agreement between Consultant 1 and Consultant 2 when they analyzed the slides under an optical microscope was 81.5% (CI = 73.9% - 87.6%). This concordance rate is also considered optimal and demonstrates that the selected slides presented good reading quality, allowing the tissue characteristics of each diagnosis to be observed. Studies evaluating interconsultant diagnosis do not always show good concordance, given the different professional experience of each consultant. In the current study, this limitation may have been overcome by the fact that the two consultants have extensive experience in dermatopathology and follow schools with similar diagnostic parameters.
Interconsultant concordance for the analysis of photomicrographs was high: 85.9% (CI = 78.9% 91.3%), which demonstrates that the systematic collection of photomicrographs, storage of images and their subsequent analysis on computer screens make the diagnosis via this method feasible. It was found that among the dermatoses generating discordance, 27.1% of them consisted of the leprosy spectrum. The criteria for the histopathological classification of leprosy are not consensual yet, and this may have contributed negatively to the occurrence of this discordance.
The Kappa coefficient is used in most studies that evaluate agreement between diagnoses, for it is an adjusted indicator of agreement that takes into account agreement due to a chance factor. The level of reproducibility of the diagnoses obtained in this study by optical microscopy analysis versus the analysis of digital photomicrographs was assessed by the Kappa coefficient. In order for this analysis to be performed, it was necessary to categorize the diseases into three groups: neoplastic skin diseases, infectious-contagious skin diseases, non-infectious-contagious skin diseases. The rates observed were 98.6% for Consultant 1 (p <0.001 (z test), 93.1% for Consultant 2 (p <0.001 (z test), 95.8% for interconsultant analysis of images, and 95.9% (p <0.001 (z test) for interconsultant analysis using optical microscopy.
In general, the concordance rates and Kappa coefficient observed in this study are similar to those observed by LEINWEBER et al. (2006)14 (Kappa: 80% to 93%), although these authors evaluated only lesions of melanocytic neoplasia. WINOKUR et al. (2000)13 also concluded in their study that there was 90% accuracy in diagnoses. These authors used only 99 digital images of 29 different organs in their study group. BERMAN et al. (1997)12 obtained 84% of agreement comparing image analysis with conventional microscopy; however, they used only one consultant at different times.
The results of this study were above those found by PICCOLO et al. (2002)1 and MASSONE et al. (2007).15 However, different methodologies were used, with the number of consultants going up to 12, which prevents a comparative analysis.
CONCLUSION
A - Agreement between the two consultants who analyzed skin diseases under an optical microscope was 81.5% (95% CI = 73.9% - 87.6%); while it was 85.9% (CI 95% = 78.9% - 91.3%) when using digital photomicrographs, with these values being interpreted as optimal.
B - The Kappa coefficient observed in the evaluation of slides containing dermatoses categorized into neoplastic skin diseases, infectious-contagious skin diseases and non-infectious-contagious skin diseases under an optical microscope between two consultants was 95.9% (p <0.001 (z test). The same coefficient obtained by image analysis was 95.8% (p <0.001 (z test). These values are considered optimal.
C - The results obtained allow us to conclude that the analysis of images of slides containing skin diseases (tele-dermatopathology) is an effective method which reliably reproduces the results obtained by means of traditional analysis under an optical microscope.

REFERENCES
- 1. Piccolo D, Soyer HP, Burgdorf W, Talamini R, Peris K, Bugatti L, et al. Concordance between telepathologic diagnosis and conventional histopathologic diagnosis. Arch Dermatol. 2002;138:53-8.
- 2. Burg G, Hasse U, Cipolat C, Kropf R, Djamei V, Soyer HP, et al. Teledermatology: Just cool or a real tool? Dermatology. 2005;210:169-73.
- 3. Chao LW, Enokihara MY, Silveira, PSP, Gomes SR, Böhm, GM. Telemedicine model for training non-medical persons in the early recognition of melanoma. J Telemed Telecare. 2003;9:S4-7.
- 4. Borges MR. Telepatologia: definição, histórico, modalidades, vantagens e desvantagens do uso da patologia digital como ferramenta diagnóstica de alta tecnologia [Tese]. Rio de Janeiro (RJ): Pontifícia Universidade Católica do Rio de Janeiro; 2004.
- 5. Pak HS. Teledermatology and teledermatopathology. Semin Cutan Med Surg. 2002;21:179-89.
- 6. Borges MR. Telepatologia: Nova ferramenta diagnóstica e importante elo tecnológico entre as áreas da patologia e clínicas médica e cirúrgica. Cad Bras Med. 2005;18:7-11.
- 7. Massone C, Wurm EM, Hofmann-Wellenhof R, Soyer HP. Teledermatology: An update. Semin Cutan Med Surg. 2008;27:101-5.
- 8. Rao B, Lombardi A. Telemedicine: Current status in developed and developing countries. J Drugs Dermatol. 2009;8:371-5.
- 9. Miot HA, Paixão MP, Wen CL. Teledermatologia - passado, presente e futuro. An Bras Dermatol. 2005;80:523-32.
-
10Ctsistema.com [Internet]. Conselho Federal de Medicina. Resolução CFM no 1.643/2002. [acesso 22 Ago. 2009]. Disponível em: http://www.ctsistemas.com.br/documentos/TELEMEDICINA.pdf
- 11. Fletcher R, Fletcher S. Epidemiologia Clínica: Elementos Essenciais. 4 ed. Porto Alegre: Artmed; 2006. p. 57-67.
- 12. Berman B, Elgart GW, Burdick AE. Dermatopathology via a still-image telemedicine system: diagnostic concordance with direct microscopy. Telemed J. 1997;3:27-32.
- 13. Winokur TS, McClellan S, Siegal GP, Redden D, Gore P, Lazenby A, et al. A prospective trial of telepathology for intraoperative consultation (frozen sections). Hum Pathol. 2000;31:781-5.
- 14. Leinweber B, Massone C, Kodama K, Kaddu S, Cerroni L, Haas J, et al. Teledermatopathology: a controlled study about diagnostic validity and technical requirements for digital transmission. Am J Dermatopathol. 2006;28:413-6.
- 15. Massone C, Peter Soyer H, Lozzi GP, Di Stefani A, Leinweber B, Gabler G, et al. Feasibility and diagnostic agreement in teledermatopathology using a virtual slide system. Hum Pathol. 2007;38:546-54.
-
16Fundação Alfredo da Mata. Boletim Epidemiológico. (Folheto de circulação interna). Manaus: Fundação Alfredo da Mata; jan/dez. 2005.
Publication Dates
-
Publication in this collection
21 June 2011 -
Date of issue
June 2011
History
-
Received
22 Feb 2010 -
Accepted
18 Aug 2010