Abstracts
BACKGROUND: Atopic Dermatitis is a disease which has increased during the past years despite our improved understanding of it. OBJECTIVE: To assess the impact of Atopic Dermatitis in the quality of life of children and teenagers and their family. METHOD: A descriptive cross-sectional method with prospective data collection of 50 children and teenagers diagnosed with Atopic Dermatitis ranging in age from 5-16 years. Fifty parents and/or guardians answered the quality of life questionnaires The Children's Dermatology Life Quality Index and Family Dermatitis Impact Questionnaire. The socio-demographic and clinical variables were evaluated by a clinical record chart designed specifically for the research and socioeconomic standardized questionnaire by the Brazilian Association of Research Enterprises, which evaluates assets acquired and the educational level of the head of the household. RESULTS: Thirty-five out of the 50 patients were female (70%), and 28 (56%) of them were from social class C. The Questionnaire Children's Dermatology Life Quality Index showed that 19 (38%) patients ranged from 7 to 12 points (moderate impact of atopic dermatitis) and 17 patients (34%) ranged from 13 to 30 points (high impact of atopic dermatitis). The Family Dermatitis Impact Questionnaire revealed that 15 (30%) families had scores between 7 and 12 points and 22 families (44%) scored between 13 and 30 points. CONCLUSION: The results show that there is a very high impact on the QoL for atopic dermatitis patients and their families. This makes us suggest the importance of including the quality of life study in clinical evaluations.
Adolescent; Brazil; Child; Dermatitis; Preschool; Quality of life
FUNDAMENTOS: A dermatite atópica é uma doença cuja prevalência vem aumentando nos últimos anos apesar do conhecimento crescente sobre a mesma. OBJETIVO: Avaliar a qualidade de vida das crianças e adolescentes com dermatite atópica e de suas famílias. MÉTODO: Estudo transversal descritivo com coleta prospectiva de dados de 50 crianças e adolescentes de 5 a 16 anos, com diagnóstico de DA e 50 pais ou responsáveis dos mesmos através da utilização de dois questionários de qualidade de vida, o Qualidade de Vida na Dermatologia Infantil e o Impacto da Dermatite Atópica na Família. As variáveis sócio-demográficas e clínicas foram avaliadas por uma ficha clínica elaborada especificamente para a pesquisa, os aspectos socioeconômicos, pelo questionário padronizado da Associação Brasileira de Empresas de Pesquisa, que avalia bens adquiridos e o grau de instrução do chefe da família. RESULTADOS: Havia 35/50 (70%) pacientes do sexo feminino; 28(56%) da classe social C. Através do questionário Qualidade de Vida na Dermatologia Infantil observou-se que: 19 (38%) pacientes ficaram na faixa de 7 a 12 pontos (impacto moderado da dermatite atópica) e 17 (34%), na faixa de 13 a 30 pontos (impacto elevado da dermatite atópica). Pelo questionário Impacto da Dermatite Atópica na Família observou-se: 15 (30%) famílias apresentaram escores entre 7 e 12 pontos e 22 (44%) entre 13 e 30 pontos. CONCLUSÃO: Os resultados mostram que a repercussão da doença na vida dos pacientes com dermatite atópica e de suas famílias é alta, o que nos faz sugerir que seria importante inserir o estudo da qualidade de vida na avaliação clínica dos mesmos.
Adolescente; Brasil; Criança; Dermatite atópica; Pré-Escolar; Qualidade de vida
INVESTIGATION
Quality of life in children and teenagers with atopic dermatitis* * Work performed at the Instituto de Dermatologia Professor Rubem David Azulay - Santa Casa da Misericórdia do Rio de Janeiro - Rio de Janeiro (RJ), Brazil.
Qualidade de vida das crianças e adolescentes com dermatite atópica
Cláudia Soïdo Falcão do AmaralI; Maria de Fátima Bazhuni Pombo MarchII; Clemax Couto Sant'AnnaIII
ISpecialist In Allergy and Immunology by the Brazilian Association of Allergy and Immunopathology - Associação Brasileira de Alergia e Imunopatologia (ASBAI). Chief of the Allergy and Immunology Service of the Instituto de Dermatologia Professor Rubem David Azulay - Santa Casa da Misericórdia do Rio de Janeiro - Rio de Janeiro (RJ), Brazil
IIPhD in Medicine by the Universidade Federal do Rio de Janeiro (UFRJ) - Assistant Professor of the Instituto de Puericultura e Pediatria Martagão Gesteira - Universidade Federal do Rio de Janeiro (IPPMG-UFRJ) - Rio de Janeiro (RJ), Brazil
IIIPhD in Medicine by the Universidade Federal do Rio de Janeiro (UFRJ) - Assistant Professor of the Instituto de Puericultura e Pediatria Martagão Gesteira - Universidade Federal do Rio de Janeiro (IPPMG-UFRJ) - Rio de Janeiro (RJ), Brazil
Mailing address Mailing address: Cláudia Soïdo Falcão do Amaral Rua Coronel Moreira César, 26 sala 711 - Icaraí 24230 060 Niterói RJ E-mail: csfamaral@ig.com.br
ABSTRACT
BACKGROUND: Atopic Dermatitis is a disease which has increased during the past years despite our improved understanding of it.
OBJECTIVE: To assess the impact of Atopic Dermatitis in the quality of life of children and teenagers and their family.
METHOD: A descriptive cross-sectional method with prospective data collection of 50 children and teenagers diagnosed with Atopic Dermatitis ranging in age from 5-16 years. Fifty parents and/or guardians answered the quality of life questionnaires The Children's Dermatology Life Quality Index and Family Dermatitis Impact Questionnaire. The socio-demographic and clinical variables were evaluated by a clinical record chart designed specifically for the research and socioeconomic standardized questionnaire by the Brazilian Association of Research Enterprises, which evaluates assets acquired and the educational level of the head of the household.
RESULTS: Thirty-five out of the 50 patients were female (70%), and 28 (56%) of them were from social class C. The Questionnaire Children's Dermatology Life Quality Index showed that 19 (38%) patients ranged from 7 to 12 points (moderate impact of atopic dermatitis) and 17 patients (34%) ranged from 13 to 30 points (high impact of atopic dermatitis). The Family Dermatitis Impact Questionnaire revealed that 15 (30%) families had scores between 7 and 12 points and 22 families (44%) scored between 13 and 30 points.
CONCLUSION: The results show that there is a very high impact on the QoL for atopic dermatitis patients and their families. This makes us suggest the importance of including the quality of life study in clinical evaluations.
Keywords: Adolescent; Brazil; Child; Dermatitis, atopic; Preschool; Quality of life
RESUMO
FUNDAMENTOS: A dermatite atópica é uma doença cuja prevalência vem aumentando nos últimos anos apesar do conhecimento crescente sobre a mesma.
OBJETIVO: Avaliar a qualidade de vida das crianças e adolescentes com dermatite atópica e de suas famílias.
MÉTODO: Estudo transversal descritivo com coleta prospectiva de dados de 50 crianças e adolescentes de 5 a 16 anos, com diagnóstico de DA e 50 pais ou responsáveis dos mesmos através da utilização de dois questionários de qualidade de vida, o Qualidade de Vida na Dermatologia Infantil e o Impacto da Dermatite Atópica na Família. As variáveis sócio-demográficas e clínicas foram avaliadas por uma ficha clínica elaborada especificamente para a pesquisa, os aspectos socioeconômicos, pelo questionário padronizado da Associação Brasileira de Empresas de Pesquisa, que avalia bens adquiridos e o grau de instrução do chefe da família.
RESULTADOS: Havia 35/50 (70%) pacientes do sexo feminino; 28(56%) da classe social C. Através do questionário Qualidade de Vida na Dermatologia Infantil observou-se que: 19 (38%) pacientes ficaram na faixa de 7 a 12 pontos (impacto moderado da dermatite atópica) e 17 (34%), na faixa de 13 a 30 pontos (impacto elevado da dermatite atópica). Pelo questionário Impacto da Dermatite Atópica na Família observou-se: 15 (30%) famílias apresentaram escores entre 7 e 12 pontos e 22 (44%) entre 13 e 30 pontos.
CONCLUSÃO: Os resultados mostram que a repercussão da doença na vida dos pacientes com dermatite atópica e de suas famílias é alta, o que nos faz sugerir que seria importante inserir o estudo da qualidade de vida na avaliação clínica dos mesmos.
Palavras-chave: Adolescente; Brasil; Criança; Dermatite atópica; Pré-Escolar; Qualidade de vida
INTRODUCTION
Atopic dermatitis (AD) is a chronic relapsing inflammatory disease of the skin characterized by intensely pruritic and eczematous lesions. The location usually depends on the age of the patient. It is predominant in childhood but can occur at any age.1
Its prevalence has increased in recent decades. The reasons for this increase are not well established, however it is believed that in addition to individual genetic predisposition, environmental factors, pollutants, exposure to allergies and infections, might be involved. 2
The diagnosis is made by the morphology and distribution of skin lesions, associated with personal or family history of atopy. Usually the clinical criteria used is the one by Hanifin and Rajka.3
In most cases, AD is associated with other atopic diseases such as asthma and allergic rhinitis which characterizes the genetic predisposition of these individuals to exaggeratedly synthesize Immunoglobulin E (IgE) specific for various antigens, especially for those inhaled.4,5 The sensitivity to allergens through the skin seems to predispose patients to atopic respiratory diseases.6
It has been shown that there is a common physiological path among severe AD, asthma and allergic rhinitis confirming the multiple factors in its etiology. 7
The concepts of quality of life (QoL) and quality of life related to health (HRQoL) are used to define treatment and evaluate the cost / benefit of the procedures employed in the health sector. 8-10
The instruments used to measure QoL questionnaires are based on data collected to assess physical, psychological and patient intervention results.11,12 This method has been widely used, especially in chronic diseases that often cause great impact on the lives of patients and their families.11,13
AD is one of the diseases responsible for the negative impact on the patients QoL.14
Several aspects of the patient's life may be affected by AD, such as clothing worn, bath duration, continuous use of emollients, family and social life, ability to practice sports, sleep or study and, depending on age, sex and professional life. The patients frequently experience significant psychological changes that often develop into severe depression.14,15 In fact, AD causes changes in the QoL of the patient and family socially, emotionally and financially. The overload of caring for patients with AD may lead to conflicts between parents and healthy siblings which alters the family's structure.16,17
The treatment of AD is uncommon not only due to the difficulty in relation to the clinical aspects, but also because of the financial investment that the parents have to make to maintain long-term care, which many times makes it hard for the families to continue with the treatment.
Our objective was to assess how AD affects the QoL of children, teenagers and their families.
METHODS
The study was cross-sectional, descriptive, with prospective data collection taken from patients that were accompanied through the program at the Dermatology Service Center at the Santa Casa da Misericórdia of Rio de Janeiro, during the period of January 2009 to September 2010. The samples were taken from patients treated at the Allergy and Immunology Clinic of Dermatology, the Pediatric Dermatology Center, and the General Dermatology Center.
We included children and teenagers from 5 to 16 years of age diagnosed with AD according to the criteria of Hanifin and Rajka, as well as from input from the parents of these patients. We excluded children and teenagers with chronic diseases, and those with allergies due to cognitive impairment, illiterate, those who had used any relief medication the week prior to the study and those who refused to answer.3
Data collection was performed at the Allergy and Immunology Dermatology service. To obtain the data, we used medical records with questions about the variables of interest, personal and family history of atopic conditions, age of onset and clinical features to confirm the diagnosis of AD. The socio-economic data was obtained through standardized questionnaire from the Brazilian Association of Research Companies (ABEP) that evaluates the amount of goods purchased and the educational level of household heads by scoring from zero to forty-six, and the respondents were distributed into eight economic classes: A1, A2, B1, B2, C1, C2, D and E. The measurement of QoL was performed using two questionnaires: The Children's Dermatology Life Quality Index - CDLQI)18 and the Dermatitis Family Impact Questionnaire - DFI.19 The CDLQI and DFI questionnaires are of English origin and were validated in the UK. They were subsequently translated and culturally appropriated for use in Brazilian Portuguese. The CDLQI was recently validated in our setting. It is directed to the ages five to 16 years and can be completed by the patient.20 It consists of ten questions that assess symptoms and feelings, leisure, school and holidays, family relationships, sleep and treatment. All questions are related to the weeks preceding its application; each question is assigned a score from zero to three points. The result ranges from zero (minimum) to 30 (maximum).
The DFI was designed to be answered by parents or guardians. It consists of ten questions, all related to the week prior to its application. The score assigned to each response and the final sum is obtained similarly to the questionnaire CDLQI. Even though it had been translated and appropriated culturally to the Portuguese used in Brazil, it was not validated for our population sample.12 In both questionnaires, the higher the score, the worse the reflection of AD for the patient and family.
The AD was classified according to clinical forms: children - up to two years (mainly characterized by the involvement of the face and also the neck, forehead, trunk and extensor surface of limbs); youth-from two to 12 years (longer lesions, xerosis, scaly and lichenification, mainly affecting the popliteal saddle and antecubital folds, neck, wrist and ankles); adult - twelve years on, the location of the lesions on flexural areas with xerosis is predominant.
The descriptive analysis was presented in tables as mean ± SD and median (minimum - maximum) for numeric data, and frequency (n) and percentage (%) for categorical data.
Inferential analysis consisted of the following methods:
For comparison of categorical variables sociodemographic and atopy, we applied the x2 test or the Fisher exact test, and chronological age (in years) and diagnosis (in months) between three tracks of the score (0 to 6, 7 to 12 and 13 to 30 points), we used one-way ANOVA or Kruskal-Wallis, respectively; 21
The comparison of scores CDLQI and DFI (in points) between socio-demographic variables and atopy in two categories were analyzed using the Mann-Whitney test and the Spearman correlation coefficient was used to measure the association between the QoL scores.
Nonparametric methods were used because the scores did not show normal distribution (Gaussian distribution) due to rejection of the hypothesis of normality according to Kolmogorov-Smirnov test. The criteria for determining significance were set at 5%. Statistical analysis was performed with SAS® System software version 6.11 (SAS Institute Inc., Cary, North Carolina).
The project was Approved by the Ethics Committee of the Santa Casa da Misericórdia of Rio de Janeiro on January 12, 2009 (CEP 002/09; FR 238078; CAAE - 0018.0.346.000-08).
RESULTS
We selected 52 patients and their 52 parents or guardians. Two patients were excluded because their parents refused to participate, leaving 50 patients. The clinical data, the social profile and the scores of the questionnaires CDLQI and DFI are described in table 1. The patients were divided into two groups according to age: 5 to 9 years of age and 10 to 16 years of age. The score from the questionnaires CDLQI and DFI were divided into 4 categories according to the intensity of the impact due to the AD in the life of those interviewed: 0 to 1 points (no impact upon the life of the patient), 2 to 6 points (moderate impact), 7 to 12 and 13 to 30 points (high impact). It is important to say that the point range was taken from the CDLQI questionnaire; in our work we decided to also use this same point range for the analysis of the DFI questionnaire.
The main symptoms reported were itching in 50 patients (100% of cases), dry skin in 49 patients (98%) and lichenification in 32 patients (64%).
The most common locations for the eczematous lesions were: antecubital folds in 37 patients (74%) and popliteal saddle in 40 patients (80%), extensive surface of arms in 43 patients (86%), legs in 42 patients (84%) and thighs in 31 patients (62%). The neck and trunk were also cited in the spotlight, respectively involving 29 patients (58%) and 27 patients (54%).
The descriptive analysis of socio-demographic variables and atopy by age of CDLQI (F1:0-6; F2: 7 to 12, F3: 13 to 30) are presented in table 2. The CDLQI score in points were divided into three groups for a better statistical analysis: F1: 0 to 6 points (none or small impact of AD in QoL), F2: 7 to 12 points (moderate impact), and F3: 13 to 30 points (high impact).
In relation to social class, according to the points obtained from the answers given to the specific questionnaire, the patients were divided into 6 different classes A2, B1 and B2 representing a higher social class financially, and C1 and C2, D representing a lower social class financially.
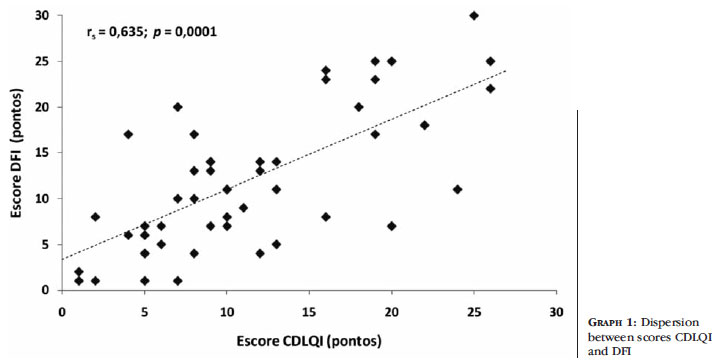
The correlation between the DFI and CDLQI analyzed by the Spearman correlation coefficient showed a significant relationship between CDLQI and DFI scores (r = 0.635, p = 0.0001, n = 50). This means that the higher the score the higher the expected value CDLQI score DFI (Graph 1).
DISCUSSION
This work developed in a dermatology referral center showed that AD extremely impairs the QoL of children and teenagers and their families.
In the questionnaire CDLQI, 38% of the patients AD had moderate effect on QoL and 34% considered very high effect. We found that 72% of the patients had significant effect on the QoL. In the questionnaire DFI, 30% of the AD patients' parents or guardians scored between seven and twelve points and 44% of them scored between thirteen to thirty points. No correlation was found between the intervals of the scores and the severity of the impact caused by the disease in the DFI questionnaire as we had seen with the CDLQI and what authors had published on the subject. However through analysis, it was determined that 74% of the families studied had negative impact on their family structure. The choice of these questionnaires in the present study was based on their use in several countries because they are well structured, comprehensive, reliable, and language adaptable.
In the questionnaire CDLQI, areas with the highest level of problems were related to symptoms and feelings, followed by problems in leisure, personal relationships, and school or vacation. Working with the results of the DFI questionnaire showed the important impact of the disease on the family's expenses, in fatigue or even exhaustion of parents, family relationships affected and compromised quality of sleep and leisure. Our study has shown the prevalence of these issues. The data reflects how the presence of a child with AD affects QoL leading to a high degree of family commitment.22
Our results call attention to the fact that the work had been done in an educational institution where it prioritizes the quality of care, clarification about the disease and the option of participation in the monthly support group carried out there. We decided to use two QoL questionnaires, like other authors, because the CDLQI measures the effect that the AD, especially in its severe form, causes in the patient's life and the DFI in the lives of family. There is however, a growing appreciation of such instruments in the literature.23
Graph 1 shows a correlation between the commitments that AD promotes in the life of the child, teenager and family life. The high impact of illness on the QoL of children and teenagers showed a direct correlation with the QoL of the family.
Although there is a greater knowledge of AD, it continues to promote these profound changes in QoL of patients.2,24
AD has been considered a disease of the highest impact with regard to social and psychological aspects. Studies comparing AD and other chronic diseases such as psoriasis, depression, hypertension and type 2 diabetes with the use of these questionnaires, CDLQI being one of them, show greater impact on QoL of AD then other diseases not only on the QoL of children and teenagers but also of adults.25 In adults, mental effects are also described.26
AD is most commonly found during the childhood years. Our greatest percentage (72%) aged from 10 to 16 years, and this is due to characteristics of the study site.
There was a female predominance (70% of the cases), similar to other studies.14 However, there are studies that show higher percentage in males.27 Our data showed that the score of CDLQI and DFI questionnaires were worse in men (p = 0.013 and p = 0.05 respectively) than in women. We did not find similar results in the literature used. We found that most women have a greater concern with their appearance and the clothing they wear.27
Our data shows a significant association with allergic rhinitis and asthma characterizing the tendency that the individual is genetically predisposed to develop other atopic diseases.28
The chronic characteristic of AD entails high expenses for its control, not only with regard to drug use, but also by frequent visits to the health services. Our study did not show a significant percentage difference between the high and low social classes, moderate impact scores (7-12 points) and high (13 to 30 points), both in the questionnaire CDLQI and in DFI. Thus, the economic status was not involved decisively in the natural evolution of the disease. The predominance of class C is expected because the trial was held at a public service with the targeted population being mostly poor. A Turkish study with 785 children showed a higher incidence of skin diseases, including AD, in children with poor working conditions.29 Another Austrian study, showed higher frequency of atopic diseases in adult patients with higher socio-economiccultural standard, residing in urban areas.30 There are many reports in the literature following this same trend.
CONCLUSION
In this study, the small sample size was a limitation. However, it is a representation that the service and the results are similar to those found in national and international literature that show the same negative impact that AD has on the patient's life as well as the life of his/her relatives.16,17 Even though this study was not the first one to be done, it was relevant to evaluate the QoL of our patients. It is believed that more studies on the QoL of an AD patient would be very beneficial as well as establishing multidisciplinary approaches to treatment strategies, adherence to treatment and better control of the disease.
Thanks to:
Professor David Rubem Azulay, Chief of Dermatology (Prof. Institute of Dermatology Rubem David Azulay) Santa Casa da Misericórdia of Rio de Janeiro by the possibility of the study and encouragement

Received on 12.11.11
Approved by the Advisory Board and accepted for publication on 30.01.2012.
Conflict of interests: None.
Financial Support: Masters Sponsorship - Grade 10 Pupil (Aluno Nota 10) - Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ). Part of the research.
- 1. Leung DYM. Atopic dermatitis: immunology and treatment with immune modulators. Clin Exp Immunol. 1997;107 Suppl 1:25-30.
- 2. Torres-Borrego J, Molina-Terán AB, Montes-Mendoza C. Prevalence and associated factos of allergic rhinitis and atopic dermatitis in children. Allergol Immunopathol (Madr). 2008;36:90-100.
- 3. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Dermatol Venereol (Stockh). 1980;Suppl 92:44-47.
- 4. Leite RMS, Leite AAC, Costa IMC. Dermatite atópica: uma doença cutânea ou uma doença sistêmica? A procura de respostas na historia da dermatologia. An Bras Dermatol. 2007;82:71-8.
- 5. Zheng T, Yu J, Oh MH, Zhu Z. The atopic march: progression from atopic dermatitis to allergic rhinitis and asthma. Allergy Asthma Immunol Res. 2011;3:67-73.
- 6. Fuiano N, Incorvaia C. The atopy patch test: is it time to redefine its significance? Ann Allergy Asthma Immunol. 2011;106:278-82.
- 7. Leung DY, Soter NA. Cellular and immunologic mechanisms in atopic dermatitis. J Am Acad Dermatol. 2001;44(1 Suppl):S1-S12.
- 8. Minayo MCS, Hartz ZMA, Buss PM. Qualidade de vida e saúde: um debate necessário. Cienc Saúde Coletiva. 2000;5:7-18.
- 9. Frisén A. Measuring health-related quality of life in adolescence. Acta Pediatr. 2007;96:963-8.
- 10. Dantas RAS, Sawada NO, Malerbo MB. Pesquisas sobre qualidade de vida: revisão da produção científica das universidades públicas do Estado de São Paulo. Rev Latino Am Enfermagem. 2003;11:532-8.
- 11. Grange A, Bekker H, Noyes J, Langley P. Adequacy of health-related quality of life measures in children under 5 years old: systematic review. J Adv Nurs. 2007;59:197-220.
- 12. Soreiffmann M, Weber MB, Fontes Neto PT, Mazzotti NG, Prati C, Barzenski B, et al. Tradução e adequação cultural para o português de questionários sobre qualidade de vida para pacientes portadores de dermatite atópica. Revista HCPA. 2005;25(Supl 1);1-251.
- 13. Klatchoian DA, Len CA, Terrei MT, Silva M, Itamoto C, Ciconelli MT, et al. Quality of life of children and adolescents from São Paulo: reliability and validity of the Brazilian version of the Pediatric Quality of Life Inventory TM version 4.0 Generic Core Scales. J Pediatr (Rio J). 2008;84:308-15.
- 14. Fontes Neto PTL, Weber MB, Fortes SD, Cestari TF. A Dermatite atópica na criança: uma visão psicossomática. Rev Psiqiatr RS. 2006;28:78-82.
- 15. Santos VS. Qualidade de Vida em Crianças e Adolescentes com Problemas de Saúde: conceptualização, medida e intervenção. Psic Saúde & Doenças. 2006;7:89-94
- 16. Fontes Neto PTL, Weber MB, Fortes SD, Cestari TF, Escobar GF, Mazzotti N, et al. Avaliação dos sintomas emocionais e comportamentais em crianças portadoras de dermatite atópica. Rev Psiquiatr Rio Gd Sul. 2005;27:279-91.
- 17. Beattie PE, Lewis-Jones MS. A comparative study of impairment of quality of life in children with skin disease and children with other chronic childhood diseases. Br J Dermatol. 2006;155:145-51.
- 18. Lapidus CS, Kerr PE. Social impact of atopic dermatitis. Med Health R I. 2001;84:294-5.
- 19. Lewis-Jones MS, Finlay AY. The Children's Dermatology Life Quality Index (CDLQI): initial validation and practical use. Br J Dermatol. 1995;132:942-9.
- 20. Lawson V, Lewis-Jones MS, Finlay AY, Reid P, Owen RG. The family impact of childhood atopic dermatitis: the Dermatitis Family Impact Questionnaire. Br J Dermatol. 1998;138:107-13.
- 21. Prati C, Comparin C, Boza JC, Cestari TF. Validação para o português falado no Brasil do instrumento Escore da Qualidade de Vida na Dermatologia Infantil (CDLQI). Med Cutan Iber Lat Am. 2010;38:229-33.
- 22. Hollander M, Wolfe DA. Nonparametric statistical methods. 2 ed. New York: John Wiley & Soni; 1999. 787 p.
- 23. Al Shobaili HA. The impact of childhood atopic dermatitis on the patient's family. Pediatr Dermatol. 2010;27:618-23.
- 24. Ben-Gashir MA, Seed PT, Hay RJ. Quality of life and disease severity are correlated in children with atopic dermatitis. Br J Dermatol. 2004;150:284-90.
- 25. Kiebert G, Sorensen SV, Revicki D, Fagan SC, Doyle JJ, Cohen J, et al. Atopic dermatitis is associated with a decrement in health-related quality of life. Int J Dermatol. 2002;41:151-8.
- 26. Coghi S, Bortoletto MC, Sampaio SA, Andrade Júnior HF, Aoki V. Quality of life is severely compromised in adult patients with atopic dermatitis in Brazil, especially due to mental components. Clinics (São Paulo). 2007;62:235-42.
- 27. Hon KL, Leung TF, Wong KY, Chow CM, Chuh A, Ng PC. Does age or gender influence quality of life in children with atopic dermatitis? Clin Exp Dermatol. 2008;33:705-9.
- 28. Spergel JM. From atopic dermatitis to asthma: the atopic march. Ann Allergy Asthma Immunol. 2010;105:99-106.
- 29. Inanir I, Sahin MT, Gündüz K, Dinc G, Türel A, Oztürkcan S. Prevalence of skin conditions in primary school children in Turkey: differences based on socioeconomic factor. Pediatr Dermatol. 2002;19:307-11.
- 30. Dorner T, Lawrence K, Rieder A, Kunze M. Epidemiology of allergies in Austria. Results of the first Austrian allergy report. Wien Med Wochenschr. 2007;157:235-42.
Publication Dates
-
Publication in this collection
01 Oct 2012 -
Date of issue
Oct 2012
History
-
Received
12 Nov 2011 -
Accepted
30 Jan 2012