Abstracts
An uncommon skin manifestation of Dermatitis Herpetiformis is palmar and plantar purpura. Dermoscopic examination is useful for any skin condition since it allows recognition of structures that are not discernible to the naked eye. A 22 year-old Caucasian man was admitted with excoriated lesions and pruritus. Petechial lesions could be seen on volar aspect of the digits on the hands and feet. Dermoscopy examination revealed erythematous and violaceous dots and erythematous and brown dots.
Celiac disease; Dermatitis herpetiformis; Dermoscopy; Purpura; Skin diseases, vesiculobullous
Púrpura palmar e plantar é uma manifestação cutânea incomum da Dermatite Herpetiforme. A dermatoscopia é útil para o exame dermatológico por permitir o reconhecimento de estruturas que ao olho nu não são perceptíveis. Doente caucasiano masculino de 22 anos que queixava-se de lesões escoriadas e prurido. Observouse na face volar dos dedos dos pés e das mãos lesões petequiais. O exame dermatoscópico revelou pontos eritematosos e violáceos, além de pontos eritematosos e marrons.
Dermatite herpetiforme; Dermatopatias vesiculobolhosas; Dermoscopia; Doença celíaca; Púrpura
INTRODUCTION
Dermatitis herpetiformis (DH) was initially described by Louis Duhring in 1884.11. Duhring LA. Landmark article, Aug 30, 1884: Dermatitis herpetiformis. By Louis A. Duhring. JAMA. 1983;250:212-6. DH most commonly presents as a symmetric, pruritic, papulovesicular eruption on the extensor surfaces of children and adults.22. McGovern TW, Bennion SD. Palmar purpura: an atypical presentation of childhood dermatitis herpetiformis. Pediatr Dermatol. 1994;11:319-22 , 33. Cunha PR, Barraviera SR. Autoimmune bullous dermatoses. An Bras Dermatol. 2009;84:111-24. An uncommon skin manifestation of DH is palmar and plantar purpura. The dominant hand often appears more involved, suggesting trauma as an etiologic factor.44. Bolotin D, Petronic-Rosic V. Dermatitis herpetiformis. Part I. Epidemiology, pathogenesis, and clinical presentation. J Am Acad Dermatol. 2011;64:1017-24.
Dermoscopic examination is a useful tool for visualization of any skin condition since it allows recognition of structures that are not discernible to the naked eye.
CASE REPORT
We report a clinical case where purpuric lesions on the hands of a patient with DH were examined under dermoscopy.
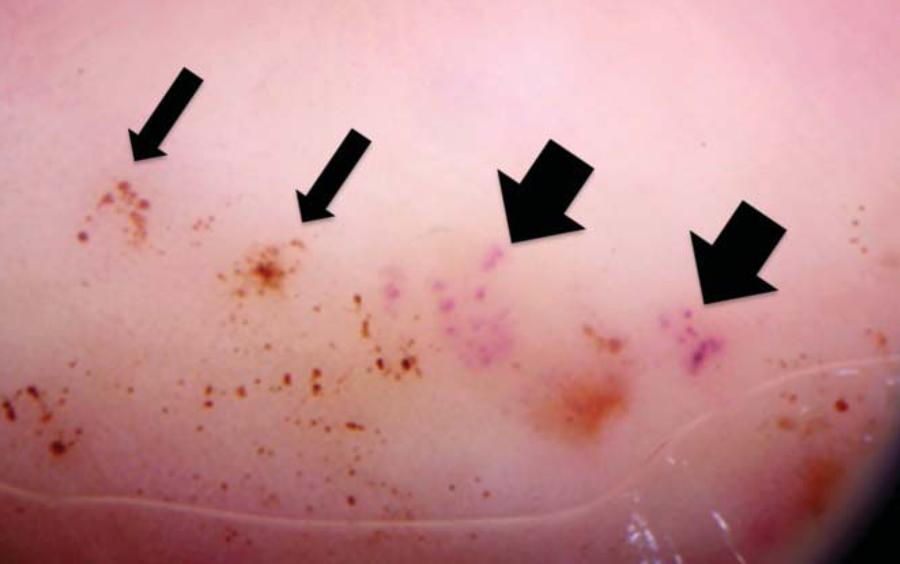
A 22 year-old Caucasian man with one and a half year history of generalized excoriated cutaneous lesions was admitted with intense pruritus. Numerous excoriated papules and crusts were distributed on the scalp, neck, dorsum, extensor surface of the limbs, in addition to the lumbar and intergluteal areas. Petechial lesions on the volar aspect of the digits of the hands and feet were visible (Figure 1). Dermoscopy examination (DermLite Photo; 3Gen) of the volar surface of the fingers revealed erythematous and violaceous dots (new petechial lesions) and erythematous and brown dots (old petechial lesions) (Figure 2). The patient's medical history included hypothyroidism. He presented no gastrointestinal symptoms. He was right-handed.
Dermatitis Herpetiformis. Under dermoscopy exam (DermLite Photo; 3Gen), erythematous and violaceous dots can be seen (New petechial lesions, thick arrows) and erythematous and brown dots (Old petechial lesions, thin arrows)
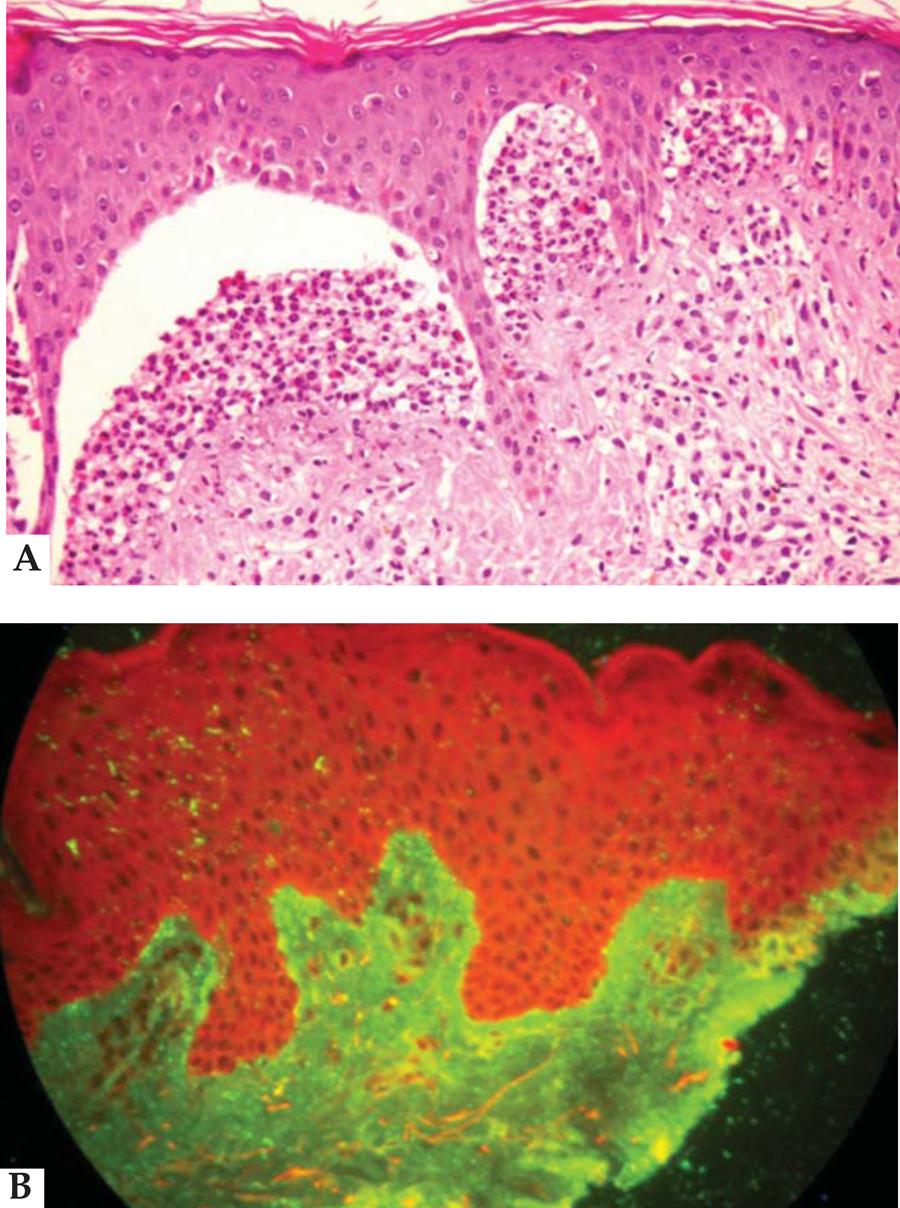
The vicinity of a purpuric lesion on the second finger of his right hand was biopsied. Hematoxilineosin stain revealed a subepidermal vesicle with neutrophils infiltrate in the dermal papillae (Figure 3A). Direct immunofluorescence exam of the apparently normal perilesional skin revealed granular IgA deposits on the upper dermis (Figure 3B). The serum level of anti-transglutaminase IgA antibodies was 18U/ml (ELISA, normal range: under 10U/ml) and G6PD was normal. Dapsone 100mg per os was initiated. After 3 days, there was no pruritus, and a glutenfree diet was accepted. On the 20th day of treatment, we saw only residual hyperpigmentated lesions.
Dermatitis Herpetiformis. A. (Hematoxylin and Eosin, 100x) subepidermal vesicle with neutrophilic infiltrate in the papillary dermis. B. (Direct immunofluorescence): IgA deposit in a granular pattern in the upper dermis
DISCUSSION
A Hungarian group presented a large series of children with DH displaying hemorrhagic palmar lesions, with the right palm and index finger more involved. Mechanical factors were thought to exacerbate the lesions, and the right-sided predominance could probably be ascribed to most patients being right-handed.55. Karpati S, Torok E, Kosnai I. Discrete palmar and plantar symptoms in children with dermatitis herpetiformis Duhring. Cutis. 1986;37:184-7.
The atypical palmar and plantar purpura presentation of DH has been reported in the literature by many authors. However, description of the dermoscopy examination has never been reported. Vazquez-Lopez et al recently revised the dermoscopic patterns of purpuric lesions, but did not describe lesions similar to those cited above.66. Vazquez-Lopez F, García-García B, Sanchez-Martin J, Argenziano G. Dermoscopic patterns of purpuric lesions. Arch Dermatol. 2010;146:938.
Our case suggests that dermatologists need to perform a careful dermoscopy exam of the hands and feet in order to find new clues in cases where DH is a possible diagnosis.
REFERENCES
-
1Duhring LA. Landmark article, Aug 30, 1884: Dermatitis herpetiformis. By Louis A. Duhring. JAMA. 1983;250:212-6.
-
2McGovern TW, Bennion SD. Palmar purpura: an atypical presentation of childhood dermatitis herpetiformis. Pediatr Dermatol. 1994;11:319-22
-
3Cunha PR, Barraviera SR. Autoimmune bullous dermatoses. An Bras Dermatol. 2009;84:111-24.
-
4Bolotin D, Petronic-Rosic V. Dermatitis herpetiformis. Part I. Epidemiology, pathogenesis, and clinical presentation. J Am Acad Dermatol. 2011;64:1017-24.
-
5Karpati S, Torok E, Kosnai I. Discrete palmar and plantar symptoms in children with dermatitis herpetiformis Duhring. Cutis. 1986;37:184-7.
-
6Vazquez-Lopez F, García-García B, Sanchez-Martin J, Argenziano G. Dermoscopic patterns of purpuric lesions. Arch Dermatol. 2010;146:938.
-
Financial funding: None
-
*
Work performed at the Dermatology Division of the Hospital das Clínicas of the University of São Paulo School of Medicine (HC-FMUSP) - São Paulo (SP), Brazil.
Publication Dates
-
Publication in this collection
Oct 2013
History
-
Received
27 Aug 2012 -
Accepted
04 Oct 2012