Abstract:
A patient with systemic involvement, initially treated as tuberculosis, is presented in this report. There were only two painful subcutaneous nodules, from which we arrived at the correct diagnosis of histoplasmosis. The patient was attended by several experts in the fields of infectious diseases, nephrology and internal medicine, but the diagnosis was only possible after dermatological examination and skin biopsy. This case values multidisciplinary interaction between dermatologists and other medical areas for diagnosis of cases with atypical manifestations.
Keywords:
Fungi; Histoplasmosis; Opportunistic infections
INTRODUCTION
Histoplasmosis is a disease caused by the dimorphic fungus Histoplasma capsulatum.11 Deepe GS. Histoplasma capsulatum. In: Mandell's, Douglas, and Buschett's principles and practice of infectious disease. Philadelphia: Churchill Livingstone; 2000. p. 2718-32. As there is a growing number of immunosuppressed individuals - a consequence of the use of immunosuppressive drugs, HIV infection or post-transplantation therapy -, this mycosis has become more common, with varied clinical manifestations and a wide spectrum of dermatological lesions.22 Cunha VS; Goldani LZ; Cestari TF. Manifestações mucocutâneas de histoplasmose na AIDS[tese].Porto Alegre (RS): Universidade Federal do Rio Grande do Sul; 2005.
This report describes a patient with systemic involvement, who was initially treated for tuberculosis. There were only two painful subcutaneous nodules, from which the correct diagnosis of histoplasmosis was reached.
CASE REPORT
The patient was referred by the infectologist for evaluation of subcutaneous nodules that appeared one year before. He had undergone kidney transplantation 15 years ago and was using prednisone (20 mg/day) and sodium mycophenolate (5.760 mg/day), besides propranolol and nifedipine for hypertension. The dermatological examination revealed two subcutaneous nodules measuring around 2 cm each, painful when pressed, with a firm consistency, barely delimited and adherent, covered by slightly swollen and erythematous, cyanotic skin on the right arm and near the elbow on the left forearm (Figure 1). There was no other noteworthy alteration on the skin or mucosae.
He also described history of fever, cough and weight loss, beginning simultaneously with the onset of the subcutaneous nodules. Although sputum cultures were negative for AFB, he was treated for tuberculosis because he continued to be febrile and with a TB-suggestive clinical condition and pulmonary image. The treatment for tuberculosis was suspended 40 days later, as there was no improvement and the patient remained febrile.
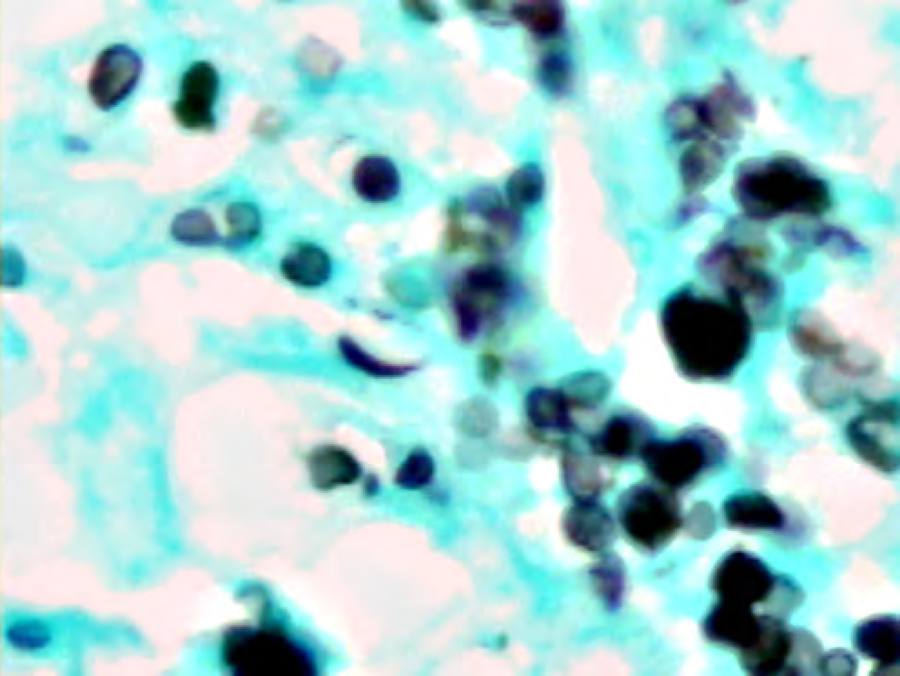
A biopsy of the nodule on the right arm was carried out and revealed cellular tissue with proliferation of macrophages and rare multinucleated giant cells, in addition to lymphoplasma neutrophilic infiltrate. Methenamine silver staining showed a great quantity of intracytoplasmatic microorganisms characteristic of H. capsulatum, sometimes forming hyphae and spores (Figures 2, 3 and 4). Finally, one year after the onset of symptoms, he received the diagnosis and treatment for disseminated histoplasmosis.
Histoplasmosis: anatomopathology. Chronic granulomatous inflammatory process with a great number of microorganisms showing Histoplasma capsulatum characteristics (Gomori)
DISCUSSION
Histoplasmosis is a systemic fungal infection that may vary from asymptomatic infection to disseminated disease with lethal outcome. The H. capsulatum is present in contaminated soil with faeces of birds or bats. Most of primary infections are asymptomatic. Factors like virulence of the agent, age group and basic disease contribute to the onset and intensity of symptoms, as the disease is related mainly to alterations in cellular immunity. Therefore, during investigation of cavitary and granulomatous pulmonary lesions, attention should be given also to the possibility of this infection.33 Lima MM, Costa FF, Fontenele LMAR, Albuquerque LM, Coriolano MWL, Carvalho MC. Histoplasmose disseminada com cavitação pulmonar, padrão miliar e acometimento laringotraqueobrônquico em paciente imunocompetente: relato de caso. RevSocBrasClín Méd. 2012;10:61-4.
It may be divided into the following clinical forms: a) histoplasmosis in normal host, subdivided into asymptomatic primary infection and acute pulmonary infection; b) chronic cavitary pulmonary histoplasmosis; c) histoplasmosis in the immunocompromised host, corresponding to acute or subacute disseminated histoplasmosis; and d) immunologically mediated disease.44 Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Doenças infecciosas e parasitárias: guia de bolso.3. ed. Brasília: Ministério da Saúde; 2004. 236p. Série B. Textos Básicos de Saúde.
Chronic disseminated histoplasmosis involves more frequently people older than 40 years of age, predominantly of the male gender. Usually, the patients have mild immune deficiencies produced by several factors like advanced age, alcoholism, diabetes mellitus, solid tumors, corticotherapy and lymphomas.44 Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Doenças infecciosas e parasitárias: guia de bolso.3. ed. Brasília: Ministério da Saúde; 2004. 236p. Série B. Textos Básicos de Saúde. The most important findings are asthenia, weight loss and lesions on the skin or mucosae.
The cutaneous lesions of histoplasmosis in the immunosuppressed patient are not diagnostic, as many other diseases share a similar morphology; for this reason systemic signs and symptoms should be valued, in order to reduce the number of possible differential hypotheses.55 Marques SA, Silvares MR, Camargo RM, Marques ME. Cutaneous histoplasmosis disclosing an HIV-infection.AnBrasDermatol. 2013;88:420-3. Mucosal lesions can be observed in around 90% of cases, are polymorphic, ulcerated or ulcerovegetative and are located on the tongue, the oral mucosa, the pharynx, the nasal septum and the larynx. Skin lesions are less frequent than mucosal lesions and appear in 10% of cases. They present as ulcers of sharp, deep borders, with granulomatous bottom, acneiform papules and ulcerated, pustular or nodular top.44 Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Doenças infecciosas e parasitárias: guia de bolso.3. ed. Brasília: Ministério da Saúde; 2004. 236p. Série B. Textos Básicos de Saúde.,66 Orsi AT, Nogueira L, Chrusciak-Talhari A, Santos M, Ferreira LC, Talhari S, et al. Histoplasmosis and AIDS co-infection. A Bras Dermatol. 2011;86:1025-6.
The reported case was revealed to be chronic disseminated histoplasmosis of cutaneous presentation without mucosal lesion, of difficult diagnosis. It was evaluated by several specialists from the areas of infectology, nephrology and internal medicine, but the diagnosis was possible only with dermatological examination and skin biopsy. This case values multidisciplinary interaction between dermatologists and specialists from other medical areas for the diagnosis of cases with atypical manifestation.
-
Financial Support: None.
-
*
Work carried out at Universidade do Oeste Paulista (Unoeste) - Presidente Prudente (SP), Brazil.
REFERENCES
-
1Deepe GS. Histoplasma capsulatum. In: Mandell's, Douglas, and Buschett's principles and practice of infectious disease. Philadelphia: Churchill Livingstone; 2000. p. 2718-32.
-
2Cunha VS; Goldani LZ; Cestari TF. Manifestações mucocutâneas de histoplasmose na AIDS[tese].Porto Alegre (RS): Universidade Federal do Rio Grande do Sul; 2005.
-
3Lima MM, Costa FF, Fontenele LMAR, Albuquerque LM, Coriolano MWL, Carvalho MC. Histoplasmose disseminada com cavitação pulmonar, padrão miliar e acometimento laringotraqueobrônquico em paciente imunocompetente: relato de caso. RevSocBrasClín Méd. 2012;10:61-4.
-
4Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Doenças infecciosas e parasitárias: guia de bolso.3. ed. Brasília: Ministério da Saúde; 2004. 236p. Série B. Textos Básicos de Saúde.
-
5Marques SA, Silvares MR, Camargo RM, Marques ME. Cutaneous histoplasmosis disclosing an HIV-infection.AnBrasDermatol. 2013;88:420-3.
-
6Orsi AT, Nogueira L, Chrusciak-Talhari A, Santos M, Ferreira LC, Talhari S, et al. Histoplasmosis and AIDS co-infection. A Bras Dermatol. 2011;86:1025-6.
Publication Dates
-
Publication in this collection
May-Jun 2016
History
-
Received
07 July 2014 -
Accepted
10 Nov 2014