Abstract
Linear IgA dermatosis is a rare subepidermal autoimmune blistering disease characterized by linear deposition of IgA along the basement membrane zone. In the last three decades, many different drugs have been associated with the drug-induced form of the disease, especially vancomycin. We report a case of vancomycin-induced linear IgA disease mimicking toxic epidermal necrolysis. The aim of this work is to emphasize the need to include this differential diagnosis in cases of epidermal detachment and to review the literature on the subject and this specific clinical presentation.
Keywords:
Linear IgA bullous dermatosis; Drug eruptions; Vancomycin
INTRODUCTION
Linear IgA dermatosis (LAD) is a rare autoimmune mucocutaneous blistering disease characterized immunohistopathologically by subepidermal blister and linear deposition of IgA along the basement membrane zone (BMZ) on direct immunofluorescence (DIF). It is classified as spontaneous and drug-induced (DI-LAD) forms.11 Chanal J, Ingen-Housz-Oro S, Ortonne N, Duong TA, Thomas M, Valeyrie-Allanore L, Lebrun-Vignes B, André C, Roujeau JC, Chosidow O, Wolkenstein P. Linear IgA bullous dermatosis: comparison between the drug-induced and spontaneous forms. Br J Dermatol. 2013;169:1041-8. Since the first publication about DI-LAD in 1981, more than one hundred cases have been reported associating different drugs with the disease, especially vancomycin. 22 Gabrielsen TO, Staerfelt F, Thune PO. Drug induced bullous dermatosis with linear IgA deposits along the basement membrane. Acta Derm Venereol. 1981;61:439-41.,33 Fortuna G, Salas-Alanis JC, Guidetti E, Marinkovich MP. A critical reappraisal of the current data on drug-induced linear immunoglobulin A bullous dermatosis: a real and separate nosological entity? J Am Acad Dermatol. 2012;66:988-94
Annular or polycyclic plaques and papules with blistering around the edges (string of pearls sign) is the classic presentation of LAD, occurring usually in childhood.44 Wojnarowska F, Venning VA. Immunobullous diseases. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's: Textbook of Dermatology. 8th ed. Oxford: Blackwell Publishing; 2010. p. 40.45-40.51. Development of LAD in adulthood can be clinically polymorphic, mimicking dermatitis herpetiformis (DH), bullous pemphigoid (BP), pemphigus vulgaris, erythema multiforme and toxic epidermal necrolysis (TEN).55 Kakar R, Paugh H, Jaworsky C. Linear IgA bullous disease presenting as toxic epidermal necrolysis: a case report and review of the literature. Dermatology. 2013;227:209-13.
DI-LAD tends to be more severe, extensive and atypical than spontaneous LAD. In a recent study with an expressive number of cases for a rare condition, the frequencies of mucosal involvement, presence of target or target-like lesions and the string of pearls sign did not differ between the two forms of the disease. However, Nikolsky's sign and large erosions were significantly more frequent in patients with DI-LAD.11 Chanal J, Ingen-Housz-Oro S, Ortonne N, Duong TA, Thomas M, Valeyrie-Allanore L, Lebrun-Vignes B, André C, Roujeau JC, Chosidow O, Wolkenstein P. Linear IgA bullous dermatosis: comparison between the drug-induced and spontaneous forms. Br J Dermatol. 2013;169:1041-8.
Few cases have been published of the rare and dramatic TEN-like clinical presentation of the disease.55 Kakar R, Paugh H, Jaworsky C. Linear IgA bullous disease presenting as toxic epidermal necrolysis: a case report and review of the literature. Dermatology. 2013;227:209-13. This report is justified by its iconographic exuberance, rarity and the need to include the disease in the differential diagnosis of patients with epidermal detachment.
CASE REPORT
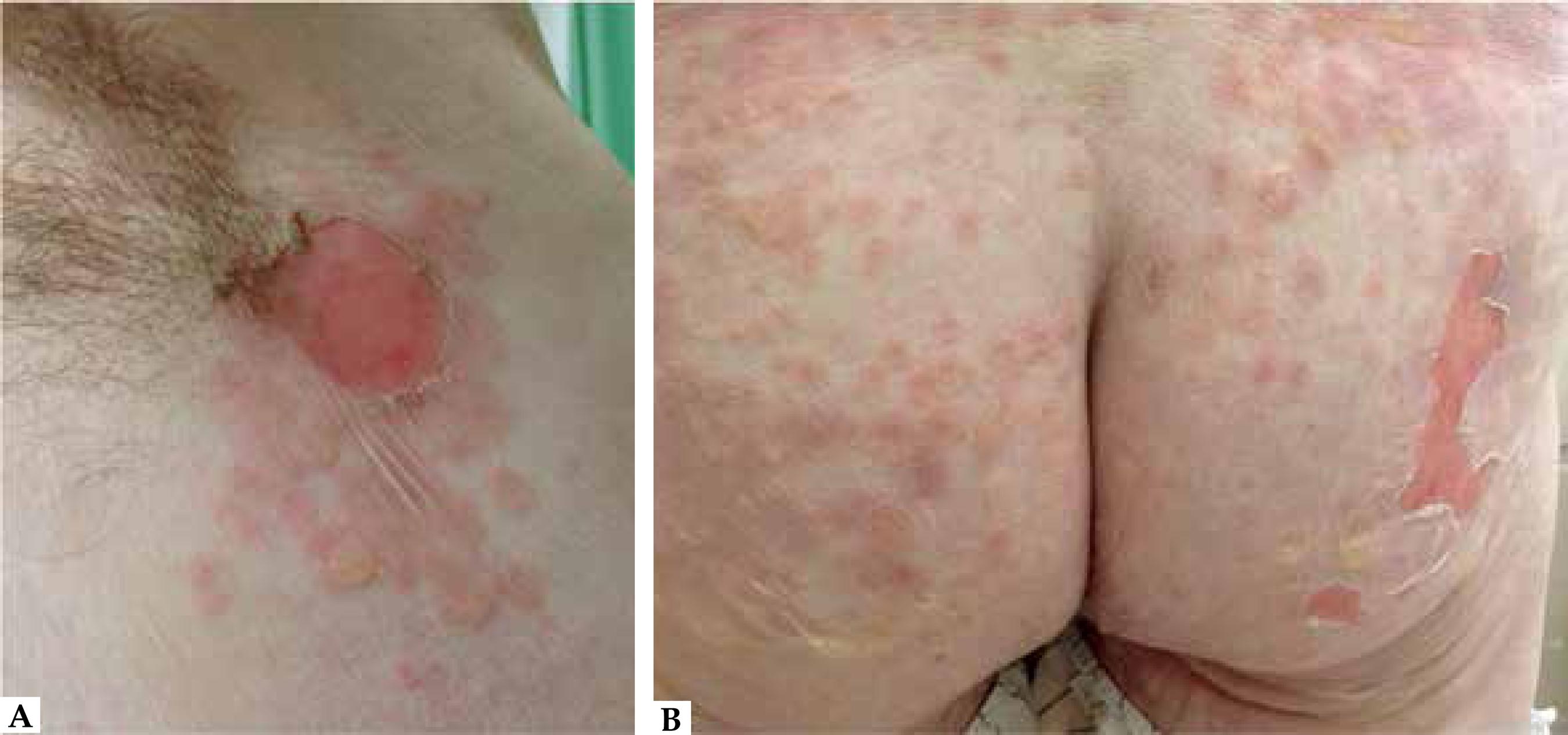
A 75-year-old male patient was hospitalized for surgical myocardial revascularization. Past medical history included high blood pressure, diabetes, dyslipidemia and ischemic stroke. In the previous three days, he had developed painful oral ulcers, tense and flaccid bullae and vesicles over the limbs and trunk. We also identified erosions on the buttocks and a positive Nikolsky's sign (Figures 1 and 2). Abrupt onset and rapid progression of the lesions were observed. The patient had been under empiric therapy with intravenous vancomycin and ceftriaxone since the day of the surgery, ten days before the lesions started to appear. The remaining drugs in use were enoxaparin, tramadol, amiodarone and medicines under continuous and chronic prescription (losartan, aspirin, propranolol, amlodipine, clonidine and simvastatin). The vancomycin level was 31.7 µg/ml, which is above the recommended therapeutic concentration (15-20 µg/ml).
A) Axillary region with flaccid bullae and erosion. B) Confluent flaccid blisters and vesicles with erosions and epidermal detachment on the buttocks
Considering the clinical picture and drug history, vancomycin-induced LAD was suspected. TEN and BP were considered in the differential diagnosis. Biopsy of an intact vesicle revealed subepidermal cleavage with neutrophilic infiltrate (Figure 3). DIF on perilesional skin demonstrated linear IgA deposition at the BMZ and negative IgG, IgM and C3 fluorescence (Figure 4).
Histopathology of an intact vesicle (hematoxylin and eosin). A and B) Subepidermal cleavage – 40x and 400x magnification; C) Neutrophilic infiltrate – 400x magnification
Direct immunofluorescence on perilesional skin revealing linear IgA deposition at the basement membrane zone
New lesions stopped appearing eight days after antibiotic discontinuation and administration of prednisone 0.5 mg/Kg/d. Complete healing was observed after twelve days. However, the patient died of sepsis and respiratory failure two weeks after total reepithelization of the skin.
DISCUSSION
Up to 2013, 16 cases of DI-LAD mimicking TEN had been reported. These cases were reviewed by Kakar et al., who found an average age of 69 years, variable mucous involvement (8/13), positive Nikolsky's sign in 8 out of 10 cases and affected body surface area ranging from 15%-90%. All surviving patients showed resolution of lesions two or more weeks after discontinuation of the putative drug. Six deaths were not attributable to DI-LAD itself, as in our case. Treatment of DI-LAD usually consists of discontinuation of the offending medication. In this review, however, six patients were also treated with dapsone, corticosteroid or intravenous immunoglobulin.55 Kakar R, Paugh H, Jaworsky C. Linear IgA bullous disease presenting as toxic epidermal necrolysis: a case report and review of the literature. Dermatology. 2013;227:209-13.
In the present report, chronology (onset of lesions 10 days after vancomycin introduction, and resolution 12 days after discontinuation) is compatible with the literature. In the cases associated with vancomycin reviewed by Fortuna et al., latency period ranged from 2 to 21 days and clinical remission occurred 1 to 21 days after drug discontinuation.33 Fortuna G, Salas-Alanis JC, Guidetti E, Marinkovich MP. A critical reappraisal of the current data on drug-induced linear immunoglobulin A bullous dermatosis: a real and separate nosological entity? J Am Acad Dermatol. 2012;66:988-94
The DIF pattern presented by our patient is classic in LAD, but C3 and IgM deposits can also be found in association with IgA. LAD histopathology is not specific and may be similar to DH and BP. A subepidermal blister with neutrophilic infiltrate is the most common description, but the infiltrate can be eosinophilic, mimicking BP.44 Wojnarowska F, Venning VA. Immunobullous diseases. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's: Textbook of Dermatology. 8th ed. Oxford: Blackwell Publishing; 2010. p. 40.45-40.51.
Identification of the target antigens by immunoblotting has been performed in a few cases of DI-LAD. Different molecular weight proteins of the BMZ have been implicated (83-, 97-, 130-, 210-, 230-, 285- (LAD285), 180Kda; NC16a domain of BP180; type VII collagen; α3 subunit of laminin-332).66 Zenke Y, Nakano T, Eto H, Koga H, Hashimoto T. A case of vancomycin-associated linear IgA bullous dermatosis and IgA antibodies to the a3 subunit of laminin-332. Br J Dermatol. 2014;170:965-9.,77 Tashima S, Konishi K, Koga H, Hashimoto T. A case of vancomycin-induced linear IgA bullous dermatosis with circulating IgA antibodies to the NC16a domain of BP180. Int J Dermatol. 2014;53:e207-9. Because of the multiple possible antigens involved, indirect immunofluorescence on salt-split skin can be positive on the epidermal side, dermal side or both.44 Wojnarowska F, Venning VA. Immunobullous diseases. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's: Textbook of Dermatology. 8th ed. Oxford: Blackwell Publishing; 2010. p. 40.45-40.51.,88 Willsteed E, Bhogal B, Black M, McKee P, Wojnarowska F. Use of 1M NaCl split skin in the indirect immunofluorescence of the linear IgA bullous dermatoses. J Cutan Pathol. 1990;17:144-8.
DI-LAD pathogenesis has not been completely elucidated yet. Implicated drugs can cause disruption of self-tolerance by a hapten-mediated process or by structurally modifying proteins at the BMZ. Triggering events such as infections may act as co-factors.99 Klein PA, Callen JP. Drug-induced linear IgA bullous dermatosis after vancomycin discontinuance in a patient with renal insufficiency. J Am Acad Dermatol. 2000;42:316-23.
In 2012, Fortuna et al. reviewed the literature in journals indexed in PubMed and selected 52 cases of DI-LAD. Out of the total, 46.2% were related to vancomycin and 53.8% to other substances, especially captopril, trimethoprim/sulfamethoxazole, phenytoin and diclofenac.33 Fortuna G, Salas-Alanis JC, Guidetti E, Marinkovich MP. A critical reappraisal of the current data on drug-induced linear immunoglobulin A bullous dermatosis: a real and separate nosological entity? J Am Acad Dermatol. 2012;66:988-94 Chart 1 contains an updated list of drugs associated with LAD.11 Chanal J, Ingen-Housz-Oro S, Ortonne N, Duong TA, Thomas M, Valeyrie-Allanore L, Lebrun-Vignes B, André C, Roujeau JC, Chosidow O, Wolkenstein P. Linear IgA bullous dermatosis: comparison between the drug-induced and spontaneous forms. Br J Dermatol. 2013;169:1041-8.
Despite the considerable number of studies reporting association between LAD and medications, there is poor evidence of causality in the majority of them. Diagnosis usually relies on chronology and previously published cases. However, as these patients are often exposed to many concurrent medications, establishing a cause-effect relationship may be challenging. Challenge-de-challenge-rechallenge testing protocol should be the gold-standard procedure, but is not always feasible because of ethical and operational aspects.33 Fortuna G, Salas-Alanis JC, Guidetti E, Marinkovich MP. A critical reappraisal of the current data on drug-induced linear immunoglobulin A bullous dermatosis: a real and separate nosological entity? J Am Acad Dermatol. 2012;66:988-94 A reasonable option is the use of internationally accepted algorithms for causality assessment in adverse drug reactions (ADR), such as Naranjo algorithm (Chart 2).1010 Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239-45.
Naranjo algorithm for causality assessment between a drug and possible related adverse reactions
In the case we presented, vancomycin was considered to have induced LAD due to chronological plausibility, a Naranjo score of 4 (possible ADR) and previous conclusive reports on this reaction.
This report aims to draw attention to the possibility of LAD in cases of suspected TEN and to emphasize the need for a biopsy and DIF in all of them. The list of medications implicated in DI-LAD development has grown in recent years, but one has to be cautious in establishing causality. The use of algorithms to estimate the probability of ADR can aid in establishing a diagnosis.
-
*
Work performed at the Universidade Federal de São Paulo (UNIFESP) - São Paulo-SP - Brazil.
-
Financial Support: None
References
-
1Chanal J, Ingen-Housz-Oro S, Ortonne N, Duong TA, Thomas M, Valeyrie-Allanore L, Lebrun-Vignes B, André C, Roujeau JC, Chosidow O, Wolkenstein P. Linear IgA bullous dermatosis: comparison between the drug-induced and spontaneous forms. Br J Dermatol. 2013;169:1041-8.
-
2Gabrielsen TO, Staerfelt F, Thune PO. Drug induced bullous dermatosis with linear IgA deposits along the basement membrane. Acta Derm Venereol. 1981;61:439-41.
-
3Fortuna G, Salas-Alanis JC, Guidetti E, Marinkovich MP. A critical reappraisal of the current data on drug-induced linear immunoglobulin A bullous dermatosis: a real and separate nosological entity? J Am Acad Dermatol. 2012;66:988-94
-
4Wojnarowska F, Venning VA. Immunobullous diseases. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's: Textbook of Dermatology. 8th ed. Oxford: Blackwell Publishing; 2010. p. 40.45-40.51.
-
5Kakar R, Paugh H, Jaworsky C. Linear IgA bullous disease presenting as toxic epidermal necrolysis: a case report and review of the literature. Dermatology. 2013;227:209-13.
-
6Zenke Y, Nakano T, Eto H, Koga H, Hashimoto T. A case of vancomycin-associated linear IgA bullous dermatosis and IgA antibodies to the a3 subunit of laminin-332. Br J Dermatol. 2014;170:965-9.
-
7Tashima S, Konishi K, Koga H, Hashimoto T. A case of vancomycin-induced linear IgA bullous dermatosis with circulating IgA antibodies to the NC16a domain of BP180. Int J Dermatol. 2014;53:e207-9.
-
8Willsteed E, Bhogal B, Black M, McKee P, Wojnarowska F. Use of 1M NaCl split skin in the indirect immunofluorescence of the linear IgA bullous dermatoses. J Cutan Pathol. 1990;17:144-8.
-
9Klein PA, Callen JP. Drug-induced linear IgA bullous dermatosis after vancomycin discontinuance in a patient with renal insufficiency. J Am Acad Dermatol. 2000;42:316-23.
-
10Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239-45.
Publication Dates
-
Publication in this collection
Sep-Oct 2016
History
-
Received
25 Apr 2015 -
Accepted
27 May 2015